")
Back to Journals » Infection and Drug Resistance » Volume 12
Prevalence and predictors of occult hepatitis C virus infection among Egyptian patients who achieved sustained virologic response to sofosbuvir/daclatasvir therapy: a multi-center study
Authors Mekky MA , Sayed HI, Abdelmalek MO, Saleh MA , Osman OA, Osman HA , Morsy KH , Hetta HF
Received 11 September 2018
Accepted for publication 13 December 2018
Published 22 January 2019 Volume 2019:12 Pages 273—279
DOI https://doi.org/10.2147/IDR.S181638
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Eric Nulens
Mohamed A Mekky,1 Hani I Sayed,2 Mohamed O Abdelmalek,1 Medhat A Saleh,3 Osman A Osman,1 Heba A Osman,4 Khairy H Morsy,5 Helal F Hetta6,7
1Department of Tropical Medicine and Gastroenterology, Assiut University Hospital, Assiut, Egypt; 2Center for Management of Viral Hepatitis, Ministry of Health, Assiut, Egypt; 3Department of Public Health and Community Medicine, Assiut University, Assiut, Egypt; 4Department of Tropical Medicine and Gastroenterology, South Valley University Hospital, Qena, Egypt; 5Department of Tropical Medicine and Gastroenterology, Sohag University Hospital, Sohag, Egypt; 6Department of Medical Microbiology and Immunology, Faculty of Medicine, Assiut University, Assiut, Egypt; 7Department of Internal Medicine, University of Cincinnati Medical Center, Cincinnati, OH, USA
Background: Occult hepatitis C virus (HCV) infection (OCI) is characterized by the detection of HCV-RNA in non-serum reservoirs, such as peripheral blood mononuclear cells (PBMCs) and/or hepatocytes with undetectable HCV-RNA or antibodies in the serum. In this study, we tried to evaluate the prevalence and possible predictors of OCI in patients who achieved sustained virologic response (SVR) post sofosbuvir/daclatasvir (SOF/DCV) therapy.
Patients and methods: A cross-sectional multicenter study was designed to enroll 1,280 HCV-infected patients who received SOF (400 mg) plus DCV (60 mg) once daily ± ribavirin regimen for 12 weeks and achieved SVR 12 weeks post treatment. They were randomly recruited from three dedicated Egyptian centers for management of HCV. Real-time PCR was performed to detect HCV-RNA in serum and PBMCs and to evaluate the different risk factors pertaining to the existence of OCI.
Results: HCV-RNA was detected in PBMCs of 50 (3.9%) of them. All OCI cases exhibited significant fibrosis score and raised pre-treatment alanine aminotransferase (ALT) levels. Logistic regression analysis comparing OCI with non-OCI revealed that high pre-treatment viral load, raised ALT, advanced fibrosis score, prolonged prothrombin time, low albumin, Child B score, antiviral experienced patients, and raised bilirubin are the most significant predictor for the possibility of OCI presence with Odds Ratio as 7.03, 5.13, 4.4, 2.68, 2.52, 1.9, 1.5, and 1.2, respectively.
Conclusion: In spite of its remote possibility, OCI post SOF/DCV therapy may be present in some cases, and this may entail a re-auditing for the definition of SVR by dual testing in both serum and PBMCs.
Keywords: Occult, hepatitis C, Direct acting, Sofosbuvir
Introduction
The landscape of hepatitis C virus (HCV) management has evolved substantially since the emergence of interferon (INF)-based regimens and the subsequent all-oral treatment protocols with several waves of guidelines to tailor the best regimen.1–3 The optimal goal of all these guidelines is to achieve a sustained virologic response (SVR) which is defined as an undetectable HCV-RNA, using a sensitive assay (typically with a lower limit of 25 IU/mL), 12 weeks after completion of therapy (SVR12).1 The use of direct acting antiviral drugs (DAAs), especially the second generation with sofosbuvir (SOF)-based regimens, markedly improves the SVR rates.4 In Egypt, the real-life experience of using SOF plus daclatasvir (DCV), as adopted by the National Committee for the Control of Viral Hepatitis, proved to be a successful regimen with SVR rates approaching 95%.5,6
The concept of SVR was appraised with the emergence of a relatively new entity of detecting replicating viral genomic particles at extra-hepatic compartments, such as in peripheral blood mononuclear cells (PBMCs), hepatic tissue, or even in colonic mucosa.1,7–10 Thereafter, the term occult C infection (OCI) was raised and represents the greatest challenge against the argument of SVR.
Occult C was considered when HCV-RNA was detectable in PBMCs, and/or liver tissue after repeated serum HCV-RNA–non-reactivity by sensitive assays (ranging between 52 and 1,000 vge or 10 and 615 IU/mL).2 Literature defined two different forms of OCI; the cryptogenic form in which patients have no anti-HCV antibodies, and the secondary form in which patients have anti-HCV antibodies and had cleared HCV infection either spontaneously or after therapy.11,12 The assessment of OCI among patients who received antiviral regimens was investigated in many clinical scenarios; such as in patient with spontaneously cleared virus,13 in hemodialysis patients,14 in liver transplant settings,15 and also in patients with treatment-induced SVR, but data in this context were conflicting, with some studies finding genomic and anti-genomic HCV-RNA in PBMCs,1 while others did not.2 The presence of post-treatment viral particles in patients with SVR may carry a potential risk for disease relapse, disease progression, and/or a hidden re-infection foci that may affect the disease epidemiologic pattern and distribution.
Therefore, we herein, aimed to determine the prevalence of OCI in PBMCs among patients who achieved SVR12 after DAAs and to determine the different predictors of OCI existence.
Patients and methods
Patients’ recruitment and study design
Between January 2017 and December 2017, a cross-sectional study was designed to enroll randomly selected patients in whom SVR12 was achieved at three dedicated Viral Hepatitis Management Centers in three different governorates; Assiut, Sohag, and Qena at Upper Egypt. Randomization was done through computer-based random allocation software that randomly selected cases from the pool within a specified time using patients’ ID number. All patients received a combination of SOF; 400 mg plus DCV; 60 mg once daily ± ribavirin (RBV) regimen for 12 weeks and achieved SVR12. Patients were either treatment naive or experienced to previous Interferon/RBV regimen. All patients had compensated liver cirrhosis as assessed by Fibroscan (EchoSens, Paris, France) prior to treatment.
All the following data were assessed at the pre-treatment phase in all patients: body mass index calculation, serum aspartate aminotransferase (IU/L), serum alanine aminotransferase (ALT, IU/L), serum albumin, serum bilirubin, serum alpha-fetoprotein, prothrombin time and concentration, international normalized ratio, blood urea, and serum creatinine. Also, liver stiffness score measurements were done by Fibroscan® (EchoSens) in kilopascals (kPa) with the following scaling: scores less than 7.4 kPa were equal to F0-F2, 9.5–12.4 kPa were equal to F3, and 14.5 kPa or greater were equal to F4 on METAVIR pathologic scoring system.16,17
RNA isolation from plasma and PBMCs
Automatic extraction of viral RNA from thawed plasma was done according to the manufacturer’s protocol using the QIAamp1 Viral RNA Mini-Kit (cat#1048147, QIAGEN1, Qiagen, Hilden, Germany). Separation of PBMCs from blood was done using Ficoll Hypaque (Lonza, Verviers, Belgium) according to the manufacturer’s instructions then lysed by lysis buffer provided in the kits, then automated extraction of the total RNA from lysed PBMCs was performed according to the manufacturer’s protocol using QIAamp1 RNA Blood Mini-Kits (cat#52304, QIAGEN1, Qiagen).
Detection of HCV-RNA in plasma and PBMCs by quantitative real-time PCR
Detection of HCV viral load in the plasma and PBMCs was performed with the Artus1HCV-RG RT-PCR Kit (cat no. 4518265, QIAGEN1, Qiagen) by standardized quantitative real-time PCR according to the manufacturer’s protocol, and amplification was done by the ABI 7500 Fast Real-Time PCR Thermal cycler (Applied Biosystems, Foster City, CA, USA). Negative and positive controls were obtained from healthy volunteers and HCV-infected patients, respectively.
Data analysis and ethical considerations
Frequencies, percentages, and means were used, as appropriate, for descriptive analysis. Univariate and multivariate logistic regression analyses were performed to assess the significant predictors of occult HCV persistence between groups. All statistical analyses was conducted by SPSS software for Windows, release 11(SPSS Inc., Chicago, IL, USA). A P-value<0.05 was considered significant.
The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by our Institutional Review Board, Assiut University College of Medicine (IRB No 17300010). An informed written consent was taken from the patients for participation in the study.
Results
Demographic and laboratory data of enrolled patients
A total of 1,280 patients (96.1% were males [n=1,100], mean age was 52.6±7.9 years) were recruited. Of them, 940 patients (76.4%) were treatment naïve and the remaining 26.5% were treatment experienced to INF/RBV. Cirrhosis was observed in 60% of patients (n=760). The basic demographic and laboratory data of patients are shown in Table 1.
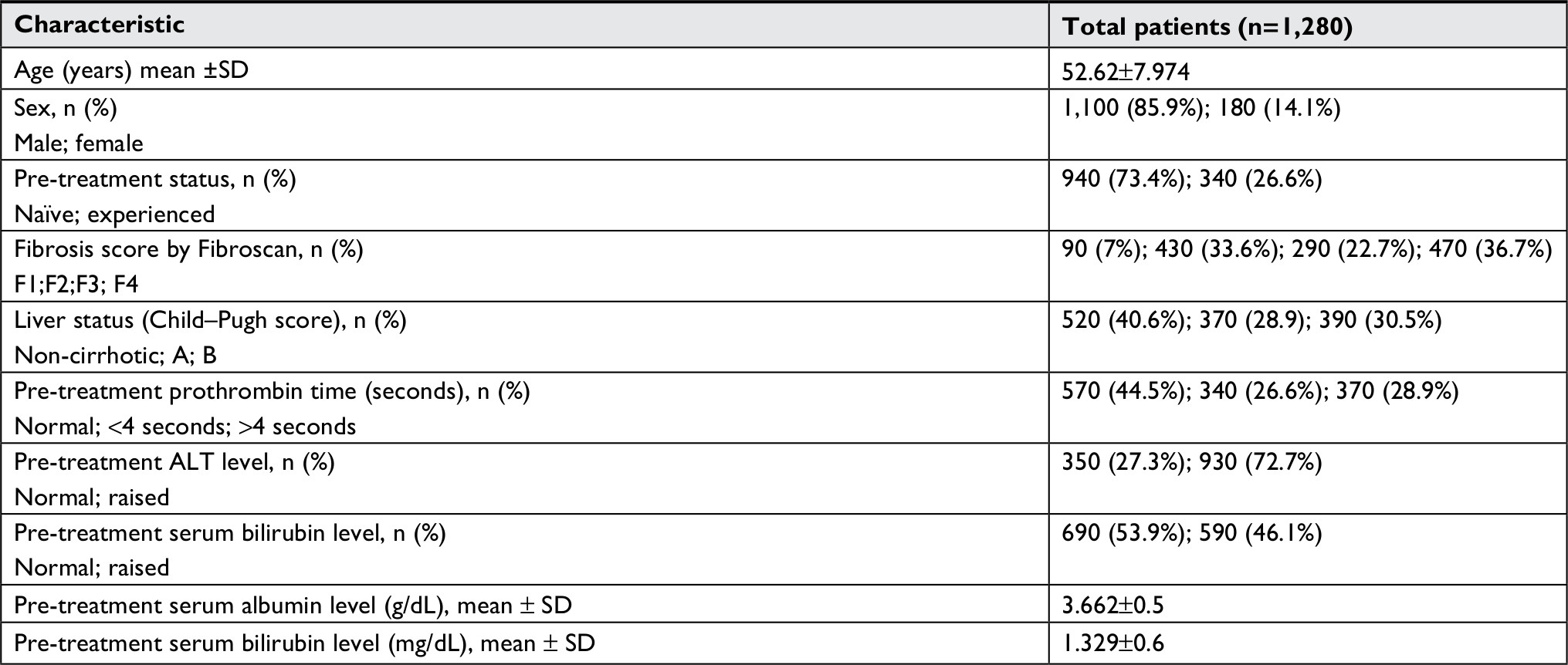 | Table 1 Demographic and laboratory characteristics of enrolled subjects |
Prevalence of OCI and characteristics
Among the 1,280 SVR patients, HCV-RNA was detected in PBMCs in 3.9% (n=50). Comparing positive and negative cases with OCI prior to therapy, there was a significant difference with regard to age (P=0.01), pre-treatment experience (P=0.001), pre-treatment prothrombin activity (P=0.01), pre-treatment serum bilirubin level (P=0.0001) and pre-treatment albumin level (P=0.001). However, we could not find any statistically significant difference with regard to gender, Fibroscan score pre-treatment viral load, and Child–Pugh score.
Post therapy (at SVR12), there was a statistical difference between two groups with regard to ALT levels (P=0.01), prothrombin activity (P=0.001) while, serum bilirubin and albumin levels did not show any statistical difference between two groups. The detailed comparison between positive and negative OCI cases is shown in Table 2.
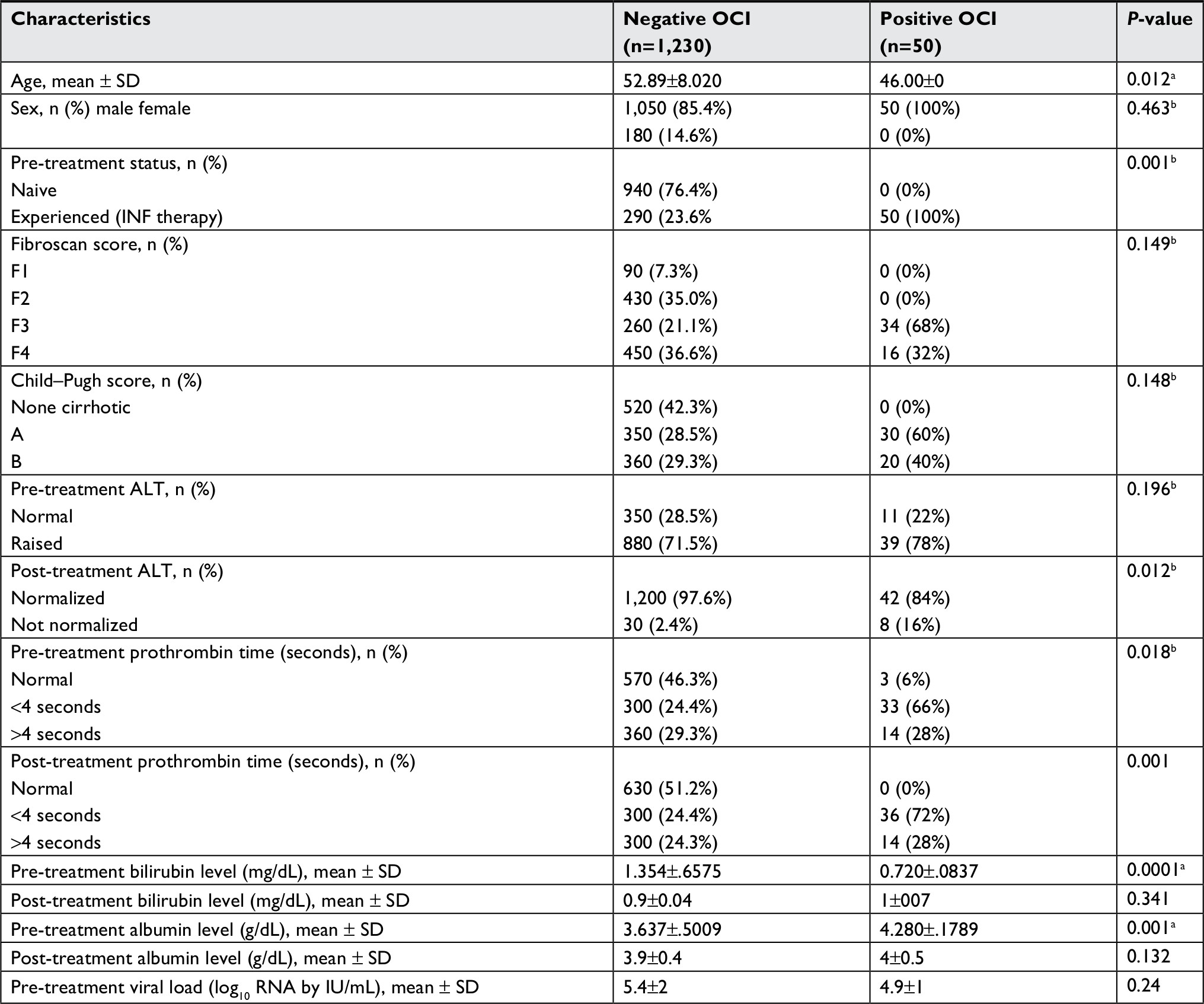 | Table 2 Univariate analysis of factors associated with the presence of OCI Notes: at-Test. bChi-squared test. Abbreviations: ALT, alanine aminotransferase; INF, interferon; OCI, occult C infection. |
Predictors of OCI among studied population
Logistic regression analysis for prediction of occult C revealed the following risk factors (OR): raised pre-treatment viral load (OR =7.03), raised ALT (OR =5.13), Fibroscan grade 4 (OR =4.4), abnormal prothrombin time 4–6 seconds (OR =2.68), low albumin (OR =2.52), Child B score (OR =1.9), previous treatment experience (OR =1.5), and raised bilirubin (OR =1.2) as shown in Table 3.
 | Table 3 Logistic regression analysis for potential risk factors for the existence of OCI Note: *the potential risk factor (predictor). Abbreviations: ALT, alanine aminotransferase; OCI, occult C infection. |
Discussion
The term OCI is now a challenging entity in the field of post hepatitis management and follow-up.11,18–21It is described when HCV-RNA is detectable in liver and/or PBMCs in patients with undetectable serum HCV-RNA.22 On the level of molecular pathology, it is well known that exposure of the intracellular HCV-RNA strands to the stress of antiviral therapy is associated with disappearance of the antisense strand that leads to interruption of the virus life cycle.18–21 Concordant clearance of intracellular HCV-RNA strands and hence, the whole virus particles from serum are a promising sign of cure. On the contrary, the persistence of the intra-PBMCs strands and its reappearance or the presence of non-responding antisense strand to antiviral therapy is a predictor of non-responder to therapy or relapse.18–20 Therefore, OCI may be considered as a hidden source for HCV recurrence or a remote source of re-infection in patients in whom SVR was assigned and now it is a debatable point of discussion, especially in localities with a high endemicity of HCV infection. From this respect, we tried to investigate the frequency of OCI in form of HCV persistence in the PBMCs in a relatively large well-defined cohort.
In the current study, OCI was detected in about 4% of patients, in whom, SVR12 was assigned. It was noted that all of them were experienced to prior IFN treatment failure. Conflicting results were found in literature. Abd Alla et al reported a high prevalence of OCI among treatment experienced and naive cases.23 Also, in the study of Khadr et al, secondary OCI was found in about 25% of cases treated with SOF/DCV.24 But, this study was criticized by the small sample size (40 patients). In the study of Radkowski et al they tested OCI after INF-based therapy and found positive OCI in PBMC in most of their patients and even on long-term follow-up post SVR.25
Also, Cavalheiro et al, emphasized the same concept in post-INF therapy.26 With the era of DAAs, re-evaluation of the existence of OCI post treatment was also detected in the study of Yousif et al, who tested OCI among different regimens of all-oral treatment and found a relatively higher prevalence of OCI (about 12%).27 On the other hand, others could not find any detectable HCV genomic RNA in their plasma or PBMCs; such as Maylin et al, study in which they tested 156 successfully treated immune-competent patients with INF-based therapy.28 Likewise, Bernardin et al tested HCV viremia in PBMCs of anti-HCV-positive/HCV-RNA-negative blood donors who had spontaneously or therapeutically cleared their plasma viremia found that the clearance of HCV from PBMC was relatively complete in both.29
In the current study, OCI was tested in the immediate phase of post SVR achievement (SVR12), which made the possibility of re-infection or a new infection somewhat impossible. In their interesting study, Ibarra et al documented the impaired cellular uptake of RBV into PBMCs with time. This may provide an explanation for the question why PBMCs could become a reservoir of HCV, especially with INF/RBV therapy and then the subsequent relapse, and treatment failure.30
Studies tackled this issue summarized the possible mechanism of OCI by the replication of HCV quasispecies in the PBMCs and then become as reservoir for virus.31
With regard to the clinical relevance of patients with positive OCI, all positive OCI cases were cirrhotic with a significant fibrosis score (F3 or F4) and also abnormal liver function tests, especially raised ALT prior to treatment. These findings were also reported in other studies of Rahman et al and Sood et al, which found a definite percentage of OCI that occurs more often in patients with overt cirrhosis.32,33 Elmasry et al examined the occurrence of OCI in HCV-infected liver transplant recipients who achieved SVR with recent DAAs and found an altered aminotransferase levels in 11% of their patients.34 However, their results may be influenced by the effect of immunosuppressive regimens as they tested OCI in post-liver transplant settings.
Our study proposed a strong recommendation of testing OCI in those with SVR as a routine part of post-treatment workup. Dual testing for both conventional PCR in the serum and PBMCs may be an essential endpoint for the precision of SVR. The need for a tailored protocol for retreatment of such patients with OCI may need further intense research.
Study limitations
This study has some limitations. First, the lack of sequential and serial follow-up by testing HCV-RNA in PBMCs post SVR24 in some patients. This weakness is considered and ongoing new study, by the same authors, is now on plan to test OCI post SVR24 in different treatment protocols and different patients’ inclusions. Second, the lack of simultaneous testing OCI in liver tissue may be considered as a weak point. However, performing liver biopsy is difficult both technically and ethically to be applied in such study design. The third weakness is the lack of genotype testing. Genotype testing was not mandated in the Egyptian protocol for treating HCV and was not considered as a prerequisite for enrolling patients. Moreover, most of studies testing HCV genotype documented genotype 4 as the main genotype in Egypt.35
Conclusion
In spite of its remote possibility, OCI post SOF/DCV therapy may be present in some cases, and this may entail a re-auditing for the definition of SVR by dual testing in both serum and PBMCs.
Acknowledgments
We would like to thank the patients and volunteers enrolled on this study. We appreciate the cooperation of all staff members in viral hepatitis management centers in Assiut, Sohag, and Qena in Upper Egypt for their help with sample collection. We gratefully acknowledge the Medical Research Center, Faculty of Medicine, Assiut University, for supporting with research equipment. Finally, we appreciate the support of the department members of internal medicine, division of digestive diseases, viral immunology laboratory, University of Cincinnati, OH, USA
This research was funded by Egyptian government scholarship for Helal F Hetta and by the Grant Office, Faculty of Medicine, Assiut University.
Disclosure
The authors report no conflicts of interest in this work.
References
Ghany MG, Strader DB, Thomas DL, Seeff LB. Diagnosis, management, and treatment of hepatitis C: an update. Hepatology. 2009;49(4):1335–1374. | ||
Omata M, Kanda T, Wei L, et al. APASL consensus statements and recommendations for hepatitis C prevention, epidemiology, and laboratory testing. Hepatol Int. 2016;10(5):681–701. | ||
Mekky MA, Abdel-Malek MO, Osman HA, et al. Efficacy of ombitasvir/paritaprevir/ritonavir/ribavirin in management of HCV genotype 4 and end-stage kidney disease. Clin Res Hepatol Gastroenterol. Epub 2018 Aug 27. | ||
Crespo J, Calleja JL, Fernández I, et al. Real-world effectiveness and safety of oral combination antiviral therapy for hepatitis C virus genotype 4 infection. Clin Gastroenterol Hepatol. 2017;15(6):e941:945–949. | ||
Elsharkawy A, Fouad R, El Akel W, et al. Sofosbuvir-based treatment regimens: real life results of 14 409 chronic HCV genotype 4 patients in Egypt. Aliment Pharmacol Ther. 2017;45(5):681–687. | ||
Omar H, El Akel W, Elbaz T, et al. Generic daclatasvir plus sofosbuvir, with or without ribavirin, in treatment of chronic hepatitis C: real-world results from 18 378 patients in Egypt. Aliment Pharmacol Ther. 2018;47(3):421–431. | ||
Castillo I, Rodríguez-Iñigo E, López-Alcorocho JM, Pardo M, Bartolomé J, Carreño V. Hepatitis C virus replicates in the liver of patients who have a sustained response to antiviral treatment. Clin Infect Dis. 2006;43(10):1277–1283. | ||
Hetta HF, Mekky MA, Khalil NK, Nassar MI, Ahmed SH, et al. Extra-hepatic infection of hepatitis C virus in the colon tissue and its relationship with hepatitis C virus pathogenesis. J Med Microbiol. 2016;65(8):703–712. | ||
Hetta HF, Mekky MA, Khalil NK, et al. Association of colonic regulatory T cells with hepatitis C virus pathogenesis and liver pathology. J Gastroenterol Hepatol. 2015;30(10):1543–1551. | ||
Hetta HF, Mehta MJ, Shata MTM. Gut immune response in the presence of hepatitis C virus infection. World J Immunol. 2014;4(2):52–62. | ||
Castillo I, Pardo M, Bartolomé J, et al. Occult hepatitis C virus infection in patients in whom the etiology of persistently abnormal results of liver-function tests is unknown. J Infect Dis. 2004;189(1):7–14. | ||
Pham TN, Macparland SA, Mulrooney PM, Cooksley H, Naoumov NV, Michalak TI. Hepatitis C virus persistence after spontaneous or treatment-induced resolution of hepatitis C. J Virol. 2004;78(11):5867–5874. | ||
Aboalam H, Rashed H-A, Mekky M, Nafeh H, Osman O. Prevalence of occult hepatitis C virus in patients with HCV-antibody positivity and serum HCV RNA negativity. J Curr Med Res Pract. 2016;1(2):12. | ||
Ali NK, Mohamed RR, Saleh BE, Alkady MM, Farag ES. Occult hepatitis C virus infection among haemodialysis patients. Arab J Gastroenterol. 2018;19(3):101–105. | ||
Keyvani H, Bokharaei-Salim F, Monavari SH, et al. Occult hepatitis C virus infection in candidates for liver transplant with cryptogenic cirrhosis. Hepat Mon. 2013;13(8):e11290. | ||
Bedossa P, Poynard T. An algorithm for the grading of activity in chronic hepatitis C. The METAVIR Cooperative Study Group. Hepatology. 1996;24(2):289–293. | ||
Ziol M, Handra-Luca A, Kettaneh A, et al. Noninvasive assessment of liver fibrosis by measurement of stiffness in patients with chronic hepatitis C. Hepatology. 2005;41(1):48–54. | ||
Zaghloul H, El-Sherbiny W. Detection of occult hepatitis C and hepatitis B virus infections from peripheral blood mononuclear cells. Immunol Invest. 2010;39(3):284–291. | ||
de Marco L, Manzini P, Trevisan M, et al. Prevalence and follow-up of occult HCV infection in an Italian population free of clinically detectable infectious liver disease. PLoS One. 2012;7(8):e43541. | ||
Carreño V, Bartolomé J, Castillo I, Quiroga JA. New perspectives in occult hepatitis C virus infection. World J Gastroenterol. 2012;18(23):2887–2894. | ||
Idrees M, Lal A, Malik FA, et al. Occult hepatitis C virus infection and associated predictive factors: the Pakistan experience. Infect Genet Evol. 2011;11(2):442–445. | ||
Nicot F, Kamar N, Mariamé B, Rostaing L, Pasquier C, Izopet J. No evidence of occult hepatitis C virus (HCV) infection in serum of HCV antibody-positive HCV RNA-negative kidney-transplant patients. Transpl Int. 2010;23(6):594–601. | ||
Abd Alla MDA, El Awady MK. Hepatitis C virus RNA strands detection in peripheral blood mononuclear cells legitimizes virus eradication in negative serum PCR naïve and post-treatment patients. J Clin Transl Hepatol. 2017;5(1):1–8. | ||
Abu Khadr NA, Nouh HH, Hanafi NF, Asser SL, Hussain YA. Secondary occult hepatitis C virus infection (HCV) in chronic HCV patients after treatment with sofosbuvir and daclatasvir. Int J Curr Microbiol App Sci. 2018;7(1):1357–1365. | ||
Radkowski M, Gallegos-Orozco JF, Jablonska J, et al. Persistence of hepatitis C virus in patients successfully treated for chronic hepatitis C. Hepatology. 2005;41(1):106–114. | ||
Cavalheiro NP, Filgueiras TC, Melo CE, et al. Detection of HCV by PCR in serum and PBMC of patients with hepatitis C after treatment. Braz J Infect Dis. 2007;11(5):471–474. | ||
Yousif MM, Elsadek Fakhr A, Morad EA, et al. Prevalence of occult hepatitis C virus infection in patients who achieved sustained virologic response to direct-acting antiviral agents. Infez Med. 2018;26(3):237–243. | ||
Maylin S, Martinot-Peignoux M, Moucari R, et al. Eradication of hepatitis C virus in patients successfully treated for chronic hepatitis C. Gastroenterology. 2008;135(3):821–829. | ||
Bernardin F, Tobler L, Walsh I, Williams JD, Busch M, Delwart E. Clearance of hepatitis C virus RNA from the peripheral blood mononuclear cells of blood donors who spontaneously or therapeutically control their plasma viremia. Hepatology. 2008;47(5):1446–1452. | ||
Ibarra KD, Jain MK, Pfeiffer JK. Host-based ribavirin resistance influences hepatitis C virus replication and treatment response. J Virol. 2011;85(14):7273–7283. | ||
Attar BM, van Thiel D. A new twist to a chronic HCV infection: occult hepatitis C. Gastroenterol Res Pract. 2015;2015:579147. | ||
Rahman MZ, Ahmed DS, Masud H, et al. Sustained virological response after treatment in patients with chronic hepatitis C infection--a five year follow up. Bangladesh Med Res Counc Bull. 2013;39(1):11–13. | ||
Sood A, Midha V, Mehta V, et al. How sustained is sustained viral response in patients with hepatitis C virus infection? Indian J Gastroenterol. 2010;29(3):112–115. | ||
Elmasry S, Wadhwa S, Bang B-R, et al. Detection of occult hepatitis C virus infection in patients who achieved a sustained virologic response to direct-acting antiviral agents for recurrent infection after liver transplantation. Gastroenterology. 2017;152(3):e558:550–553. | ||
Ahmed OA, Safwat E, Khalifa MO, et al. Sofosbuvir plus daclatasvir in treatment of chronic hepatitis C genotype 4 infection in a cohort of Egyptian patients: an experiment the size of Egyptian village. Int J Hepatol. 2018;2018:9616234. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.