")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 9
Prevalence and perception of smoking habits among the Palestinian population in the Gaza Strip
Authors Eldalo A
Received 27 February 2016
Accepted for publication 12 May 2016
Published 15 July 2016 Volume 2016:9 Pages 297—301
DOI https://doi.org/10.2147/JMDH.S107346
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ahmed S Eldalo
Department of Pharmacology and Toxicology, College of Pharmacy, Taif University, Taif, Kingdom of Saudi Arabia
Background: The Gaza Strip is a densely populated place with ~2 million inhabitants in an area of 365 km2. The aim of this study was to determine the smoking prevalence in the Gaza Strip and to identify the perception of the Palestinian population on smoking.
Method: A cross-sectional study was conducted in the Gaza Strip, Palestinian territories, during the period from June to September 2014. Convenient sampling method was adopted. A structured pretested questionnaire was used.
Results: A total of 600 adults aged 15 years or older completed the questionnaires with a response rate of 83.3%. The prevalence rate of smoking was 26.3%, with a significantly higher rate among males (31%) than females (6.9%) (P<0.001). The mean starting age was 17.4±3.9 years. The study revealed that influence of friends is the major reason for initiation of smoking and the most influential factor in convincing smokers to quit was the family. Smokers’ knowledge about smoking risks motivates them to try stop smoking (64.9%) or desire to stop smoking (65.2%).
Conclusion: The study revealed that tobacco use is significantly prevalent in the Gaza Strip. The author recommends rapid antismoking campaigns with stress on the family role and massive intervention programs to encourage young people to change their behavior toward smoking.
Keywords: smoking, prevalence, perception, Gaza Strip
Introduction
The Gaza Strip is a narrow piece of land lying on the eastern coast of the Mediterranean Sea. Its position is on the cross road from Africa to Asia. The Gaza Strip is a highly crowded place, home to approximately 2 million people, with an area of 365 km2. The coastal area along the Eastern Mediterranean Sea is ∼40 km long.1
Tobacco harms nearly every organ of the body. It is the leading preventable cause of early deaths in many developed countries and is considered as one of the most important public health problems.2 The global tobacco epidemic is predicted to kill 10 million people every year over the next 2–3 decades, and the vast majority of these deaths will occur in developing countries.3 According to the Palestinian Central Bureau of Statistics, the smoking rate in the Gaza Strip was estimated to be as follows: smokers 18 years and older comprised 27.5% in 2000, decreasing to 25.3% in 2006 and 22.5% in 2010.4 Tobacco use can be controlled, at least in public places. In many countries, tobacco use in public places is banned. This prohibition would at least decrease the rates of second-hand smoking and risks associated with smoking.5 The Palestinian Legislative Council Public Health Law states that, “The ministry should take the suitable measures to limit the harm created by the spread of smoking”.6 In a study carried out in the Gaza City, smoking inside public places contributed to serious unsafe levels of indoor air quality in these areas.7 To the best of our knowledge only one study is available related to tobacco use among Palestinian population in the Gaza Strip7 due to known difficult situations. There was a need to find out the current prevalence of tobacco use and its related behavior among residents in this area. This study was conducted to determine the smoking prevalence and the perception of smoking among the Palestinian population in the Gaza Strip.
Materials and methods
Study design and study area
A cross-sectional survey was conducted in all Gaza Governorates, Gaza Strip, Palestinian territories, during the period from June to September 2014.
Target population
All Palestinians (>15 years old) residing in the Gaza Strip at the time of the study were included.
Sampling technique and sample size
Based on a power analysis, a sample of ∼400 participants were needed for power >0.90 to detect a moderate effect in the multiple regression analysis at 5% level of significance.8 A convenient method of sampling was adopted, and a total of 720 adults were invited to participate.
Data collection
Participants were met in public places such as supermarkets, public markets, hospitals, and universities. Verbal informed consent was obtained from each participant. A self-administered questionnaire was used to collect data. A pilot study was carried out in a similar area for validity testing of the contents, but the obtained results were not included in the study.
The questionnaire composed of four sections. The first part was to collect data on participants’ demographic characteristics for both current smokers and nonsmokers. The second part was designed to collect data on smokers’ attitude toward smoking. The third part was designed as a Likert scale to determine the knowledge, attitude, and practice about smoking including the main reasons for starting smoking and the person who is convincing them to quit smoking. The last part was designed to assess nonsmoker participants on their opinions about smoking and their attitude toward smoking.
The study was revised and approved by the Committee of Pharmacy Practice Research Unit (PPRU), College of Pharmacy, Taif University, Kingdom of Saudi Arabia.
Data analysis and statistical tests
Data were processed using Statistical Package for Social Sciences Version 16 (SPSS Inc., Chicago, IL, USA). Mean and frequencies as percentages were used to describe variables. Chi-square test was used to determine the association between the demographic characteristics and participants’ knowledge and perception. P-value <0.05 was considered statistically significant.
Results
A total of 600 participants completed the questionnaires with a response rate of 83.3%; their ages ranged from 15 years to 77 years old, with a mean ± SD of 30.15±12.6. There were 158 (26.3%) smokers among the participants. Male respondents were dominant (484; 80.7%). Prevalence rate among males was significantly higher (150; 31%) than that in females (8; 6.9%) (P<0.001), while there was no significant difference between respondents with high or low monthly incomes (P=0.259) (Table 1).
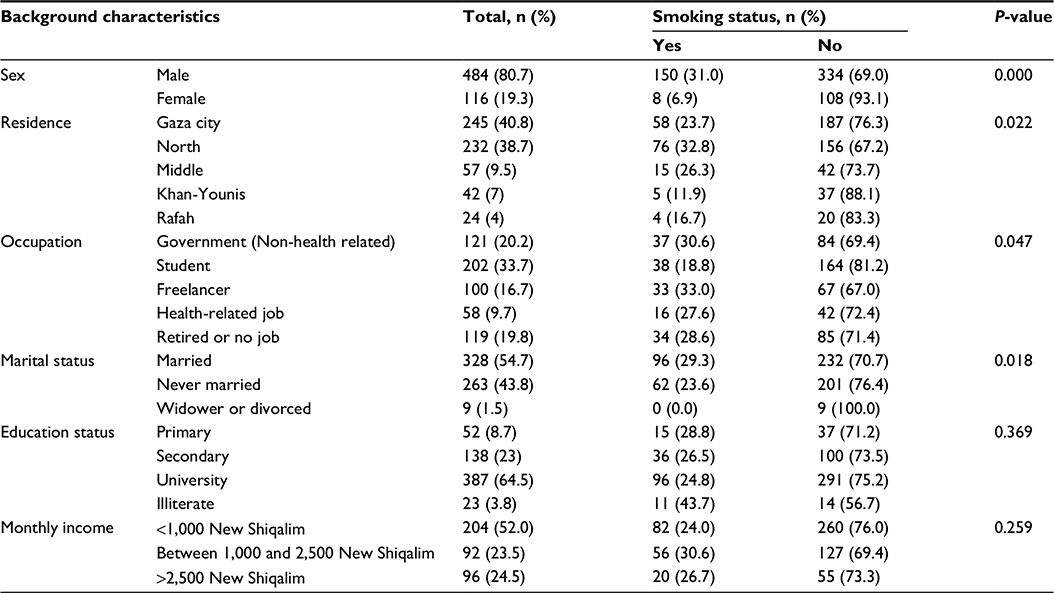 | Table 1 Demographic characteristics and smoking status of the participants (n=600) |
This study revealed that smoking habit was started at an early age from 7 years to 30 years old, with a mean ± SD of 17.4±3.9. The majority of smokers (133; 84.1%) were used to smoking cigarettes, while 45 (28.4%) used the water pipe (shisha) for tobacco smoking. Half of smokers (68; 50.4%) consumed 11–20 cigarettes a day, while 39 (28.9%) used ten cigarettes or less and eleven (8.1%) smoked >30 cigarettes a day. Regarding the number of cigarettes consumed daily, there was no significant association observed neither between participants’ sex (P=0.74) nor between their educational level (P=0.08). Regarding correlation with occupation, less than half (42.9%) of medical staff and 6.5% of students consumed 21–30 cigarettes, while 7.1% of medical staff and 54.8% of students consumed ten cigarettes or less (P<0.001). The monthly income also affected the number of cigarettes; 37.7% of participants with monthly income <1,000 New Shiqalim consumed ten cigarettes or less and 8.7% of them consumed 21–30 cigarettes, while 21.1% of smokers with monthly income >2,500 New Shiqalim consumed ten cigarettes or less and 31.6% of them consumed 21–30 cigarettes per day (P=0.02). A higher proportion of participants (41; 27.7%) smoked their first cigarette within 1 hour after waking up, and 27 (18.2%) of them started smoking in the early morning on an empty stomach.
Table 2 illustrates the attitude of smokers toward smoking and its relation to their sex, education level, and occupation. The majority (101; 65.2%) of smokers had the desire to stop smoking. There was a significant association between the desire to stop smoking and education level (P=0.041); participants with a university education level were less desirable to stop smoking (65.6%) than participants with a primary education level (73.3%). Moreover, 65.3% of males and 62.5% of females had a desire to stop smoking (P=0.024). About one-third (33.8%) of smokers admitted that there were antismoking committee services in the country. Astonishingly, 68 (43.9%) of smokers recommended smoking to their relatives and friends who became smokers.
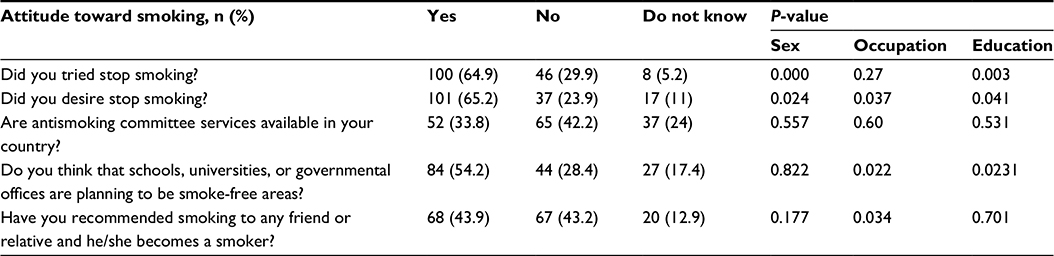 | Table 2 Smoker participants’ attitude toward smoking |
According to the smokers’ perception, the main causes of their smoking were influenced by friends (119; 78.8%), followed by imitating popular figures (85; 56.7%). There was no significant difference between the occupation and friend causes of smoking (P=0.37). Smokers thought that the most influential factor in convincing them to quit smoking was their family (90; 60%), while the teachers were the least ones (52; 34.7%) (Table 3).
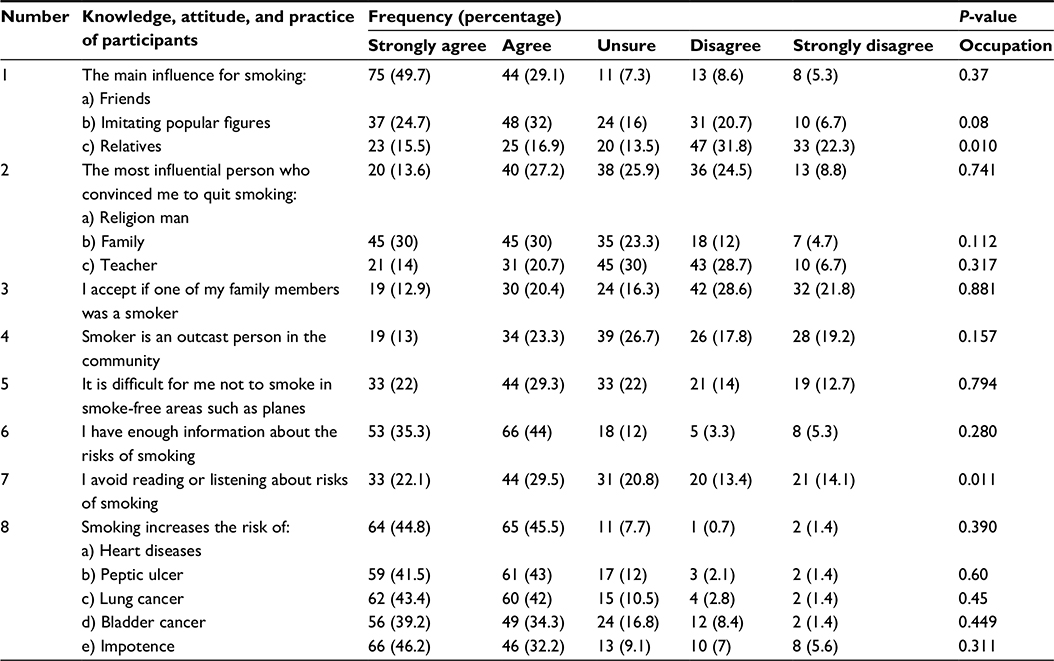 | Table 3 Knowledge, attitude, and practice of smoker participants about smoking (Likert scale application) |
Regarding the nonsmoker participants, most of them were either never smoking (327; 75.3%) or trying to smoke (287; 66%). There was a significant difference between occupation and education level with a past history of smoking. The majority of them (354; 81.2%) did not accept if one of their family members to be a smoker, but more than half (255; 58.5%) admitted that they are never annoyed by smokers around them as shown in Table 4.
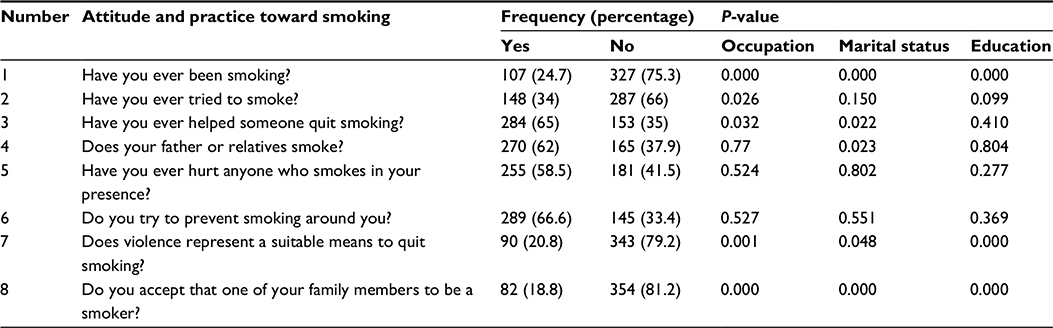 | Table 4 Attitude and practice of nonsmoker participants toward smoking |
Discussion
The prevalence of smoking in this study was found to be 26.3%. This was higher than the 2010 estimation by The Palestinian Central Bureau of Statistics.4 It was high compared to the median prevalence rate of 17.5% in a review article reported in Saudi Arabia.9 Prevalence among female smokers was significantly lower than that in males; the prevalence of female smokers has traditionally been low due to the Eastern Mediterranean Region’s conservative cultural and social values, in compliance with a study in Turkey with the same conditions, which showed that females were found to be smoking less than males.10 Studies in Western countries showed high prevalent smoking rate among girls and boys.11,12 In this study, the monthly income did not affect the smoking use habit but it affected the number of cigarettes per day. This was in a disagreement with Mikko 2005 study, which reported that smoking was more common among those with lower income and lower education.13
The study revealed that influence of friends was the major reason for starting smoking; this is in agreement with studies conducted in Malaysia14 and Saudi Arabia.15 Other studies from Spain16 and Japan17 that were carried out among school students showed increased smoking rates by the influence of having smoker friends. This finding may motivate parents to advise their children to avoid smokers’ company to avoid the negative effects of smoking hazards and to decrease the possibility of being smokers.
The most influential factor that is urging smokers to quit smoking was their family members’ advice; this finding was in agreement with a Saudi Arabian study.15 The concept of family in Mediterranean societies has conceived the house as the center and the meeting place for all family members. The family is considered the cornerstone of life for father, mother, and child.18 This was confirmed by the finding of nonsmoker participants since the majority of them (81.2%) did not accept their family members to be a smoker.
The results revealed that smokers’ information about the hazards of smoking was good, but knowledge about this information was not to accepted level; Asian studies reported that children’s knowledge about the risk of smoking does not encourage them not to smoke.19 Their knowledge about smoking hazards motivates them to try stop smoking (64.9%) or desire to stop smoking (65.2%). This was also declared by the nonsmoker participants. The majority of them (81.2%) did not accept their family member to smoke.
This study had some limitations. The proportional convenience sample was not as perfect as the ambition, since 79.5% of the sample was from Gaza and North governorates. This was due to obstacles faced by the author during data collection.
Conclusion
The study revealed that the epidemic of smoking habit was imminent in the Gaza Strip. The author recommends rapid and intensive antismoking campaigns stressing on the family role. Massive intervention programs to encourage young people for changing their behavior toward smoking were also recommended. Further research is needed to explore the determinants of tobacco use and effective ways to reduce tobacco consumption among the population of the Gaza Strip.
Acknowledgments
The author highly appreciates the hard work of data entry that was carried out by Mariam M Aldalo and Omaima M Al-Sheikh-Khalil. The author declares that he did not receive any financial reimbursements for conducting or publishing this article.
Disclosure
The author reports no conflicts of interest in this work.
References
Abualtayef MT, Abd Rabou AFN, Abu Foul AA, Ghabayen SM, Elsinwar HM. Microbial water quality of coastal recreational water in the Gaza Strip, Palestine. Nusantara Biosci. 2014;6(1):26–32. | ||
U.S. Department of Health and Human Services [webpage on the Internet]. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2014. Available from: http://ash.org/wp-content/uploads/2014/01/full-report.pdf. Accessed February 6, 2014. | ||
Maziak W, Ward K, Soweid R, Eissenberg T. Tobacco smoking using a water-pipe: are-emerging strain in a global epidemic. Tob Control. 2004;13(4):327–333. | ||
The Palestinian Central Bureau of Statistics. Percentage of Individuals 18 Years Old and over Who Smoke. Public Health Indicators; 2010. Available from: http://www.pcbs.gov.ps/Portals/_PCBS/Downloads/book1941.pdf. Accessed February 2015. | ||
Habibzadeh F. Non-communicable diseases in the Middle East. Lancet. 2013;381:279. | ||
Palestinian Legislative Council [webpage on the Internet]. Public Health Law No. (20) for the Year 2004 AD 2004. Available from: www.hdip.org/public%20health%20law%20English.pdf. Accessed March 2, 2013. | ||
Abuelaish I, Seidenberg AB, Kennedy RD, Rees VW. Second-hand smoke and indoor air quality in public places in Gaza city. EMHJ. 2013;19(5):447–451. | ||
Pourhoseingholi MA, Vahedi M, Rahimzadeh M. Sample size calculation in medical studies. Gastroenterol Hepatol Bed Bench. 2013;6(1):14–17. | ||
Bassioni MM. Review article: smoking in Saudi Arabia. Saudi Med J. 2009;30(7):876–888. | ||
Uncu Y, Irgil E, Karadag M. Smoking patterns among primary school students in Turkey. Sci World J. 2006;6:1667–1673. | ||
Baugh JC, Srinivasan SR, Sklov MC, Berenson GS, Hunter SM. Developmental trends of first cigarette smoking experience of children. The Bogalusa Heart Study. Am J Publ Health. 1982;72(10):1161–1164. | ||
Rawhone RG, Keeling CA, Jenkins A, Guz A. Cigarette smoking among secondary children in 1975. J Epidemiol Community Health. 1978;32(1):53–58. | ||
Laaksonen M, Rahkonen O, Karvonen S, Lahelma E. Socioeconomic status and smoking analysing inequalities with multiple indicators. Eur J Public Health. 2005;15(3):262–269. | ||
Naing NN, Ahmad Z, Musa R, Hamid FR, Ghazali H, Bakar MH. Factors related to smoking habits of male adolescents. Tob Induc Dis. 2004;2(3):133–140. | ||
Eldalo AS. Smoking knowledge, attitude, and practice among Saudi Population. Life Sci J. 2014;11(10):82–85. | ||
Auba J, Villalbi JR. Tobacco and adolescents: influence of personal environment. Med Clin Barcelona. 1993;100(3):506–509. | ||
Kawabata T, Maruya N, Nakamura M. Smoking and alcohol drinking behavior among Japanese adolescents: results from ‘Japan knows your body study’. Nippon-Koshu-Eisei-Zasshi. 1991;38(12):885–899. | ||
Smith RM. The people of Tuscany and their families in the fifteenth century: medieval or Mediterranean? J Fam Hist. 1981;6(1):107–128. | ||
Fraser J. Combating addiction in developing countries. World Health Forum. 1995;16(3):267–269. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.