")
Back to Journals » Vascular Health and Risk Management » Volume 16
Prevalence and Outcomes of Thrombophilia in Patients with Acute Pulmonary Embolism
Authors Obaid M, El-Menyar A , Asim M, Al-Thani H
Received 9 December 2019
Accepted for publication 21 February 2020
Published 9 March 2020 Volume 2020:16 Pages 75—85
DOI https://doi.org/10.2147/VHRM.S241649
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Munzir Obaid,1 Ayman El-Menyar,2,3 Mohammad Asim,2 Hassan Al-Thani1
1Department of Surgery, Hamad General Hospital (HGH), Doha, Qatar; 2Department of Surgery, Clinical Research, Trauma and Vascular Surgery Section, HGH, Doha, Qatar; 3Department of Clinical Medicine, Weill Cornell Medical School, Doha, Qatar
Correspondence: Ayman El-Menyar
Weill Cornell Medical College, Consultant Clinical Research, Trauma Surgery, Hamad General Hospital, Doha, Qatar
Tel +974 44394029
Fax +974 44394031
Email [email protected]
Background: We aimed to study the prevalence and outcomes of thrombophilia in acute pulmonary embolism.
Methods: A retrospective observational study was conducted to include patients with a radiologically confirmed diagnosis of PE screened for thrombophilia from May 2011 to February 2015. Data included patients’ demographics; clinical presentation, risk factors, laboratory investigations, management, and outcome were analyzed and compared in patients with and without thrombophilia.
Results: A total of 227 cases of PE were included in the study, of which 108 (47.6%) had thrombophilia. The most frequent coagulopathic abnormality included deficiency of protein S, protein C, and antithrombin III and hyperhomocysteinemia. Only seven out of 79 patients were found to have factor V Leiden. PE patients diagnosed with thrombophilia were 10 years younger in age and peaked in the age range 30– 39 years. Prior history of DVT (p=0.001) and PE (p=0.001) were the main significant risk factors in the thrombophilia group. The frequency of different risk categories of clinical probability scores did not differ significantly among those with and without thrombophilia. Pulmonary hypertension was a common complication in the thrombophilia group (P=0.009). Medications used included warfarin (74.7%), enoxaparin (73.9%), and heparin (55.4%). The overall mortality rate was 8.4%, and was non-significantly higher in the non-thrombophilia group.
Conclusion: Deficiencies of protein S, protein C, and antithrombin III are the leading causes of thrombophilic defects. Patients with hereditary thrombophilia are at increased risk of acute PE, particularly among young individuals. Therefore, early detection of thrombophilic defects together with other unprovoked risk factors could reduce the risk of recurrent VTE.
Keywords: pulmonary embolism, thrombophilia, risk factors, thromboembolism, outcome
Introduction
Acute pulmonary embolism (PE) is basically a detrimental form of venous thromboembolism (VTE) with an approximate 90-day fatality rate of 15–20%.1,2 It occurs in about one-third of patients with VTE3 and remains a cause of cardiovascular death.4 Therefore, appropriate risk-stratification based on primary predisposing factors is crucial for the discrimination and aggressive management of high-risk individuals. It has been suggested that the occurrence of VTE necessitates interaction among various clinical, acquired, and inherited risk factors.5 PE risk factors such as advanced age, cancer, immobility, recent trauma, surgery, or hospitalization can be identified in 50% of cases.6,7 However, in as many as 20 to 50% of the idiopathic cases, unprovoked PE can be explained by inherited thrombophilia.8,9
Inherited thrombophilia is a genetic predisposition to venous thromboembolism which may occur due to a single dominant abnormality or combinations of multiple milder defects.10
To date, various genetic traits are identified which influence the coagulation function and in turn contribute to the overall risk of VTE, namely protein C, protein S, and antithrombin deficiencies, and the point mutations in factor V Leiden.8 Among the general population, the frequency of hereditary thrombophilia ranges from 4 to 5% for factor V Leiden, from 0.2 to 0.4% for deficiency of protein C, is 0.2% for protein S, and is 0.02% for antithrombin.11
Thrombophilic disorders are of two types which are characterized by coagulation abnormality with loss of function and the other with gain of function.12 A metaanalysis showed that the VTE risk is increased in patients with natural anticoagulant deficiency.13 Contemporary research suggests that thrombophilia might result from a combination of genetic and environmental risk factors.10 The aim of the current study is to determine the frequency of thrombophilic risk factors in patients diagnosed with acute pulmonary embolism.
Methods
Between May 2011 and February 2015, patients who presented with acute PE confirmed by CTPA were retrospectively identified from the radiology database, and the relevant clinical information was retrieved from the medical records at Hamad General Hospital. All adult patients admitted for the management of acute PE and screened for thrombophilia were included in the study. Clinically suspected patients with PE who were not confirmed by CT imaging or were not screened for thrombophilia markers were excluded from the study. The collected data from the patients’ medical records included demographics, clinical presentation, predisposing factors, radiologic imaging, routine laboratory findings, D-dimers, cardiac troponin level, management, and detailed notes for in-hospital course, hospital length of stay, complications (leg pain, swelling, ulcers, and pulmonary hypertension), and outcome. Patients were followed up for routine clinical care as per the standard clinical practice. Screening for thrombophilia includes testing for deficiency of antithrombin (AT III), protein S (PS), and protein C (PC), hyperhomocysteine, antiphospholipid syndrome (APS), lupus anticoagulant, factor V Leiden, and systemic lupus erythematosus (SLE). PE was defined radiologically as the presence of an endoluminal central filling defect partially or completely occluding the pulmonary arteries. The severity of clinical presentation in patients with PE was assessed by clinical probability scores such as the simplified Wells score, revised Geneva score, and simplified pulmonary embolism severity index (PESI). The Institutional Review Board (IRB# 15139/15) of the Hamad Medical Corporation has approved and granted exempt status for this retrospective study.
Statistical Analysis
Data were reported as proportion, mean (±standard deviation), median, and range, when applicable. Patients were categorized into two groups based on the thrombophilia screening (non-thrombophilia vs thrombophilia). Comparison between the two groups was done using the Pearson chi-square test for categorical variables and Student's t-tests for continuous variables. Yates’ corrected chi-square was used for categorical variables, if the expected cell frequencies were below 5. ANOVA test was used for different age groups in the cohort. In addition, descriptive statistics were also performed according to different thrombophilia tests to assess with respect to demographics, predisposing factors, and outcome. Data analysis was carried out using SPSS version 18 (SPSS Inc., Chicago, Illinois, USA).
Results
During the study period, 227 consecutive patients with a radiologically confirmed diagnosis of PE were enrolled in the study. Of them, 108 (47.6%) patients were found to have a hypercoagulable state that had at least one marker positive for thrombophilia. There were 125 (55.1%) males and the mean age of the study cohort was 50.6±16.9 years.
Characteristics and Clinical Presentation of PE Patients
PE patients diagnosed with thrombophilia were 10 years younger in age (45.2±13.9 vs 55.4±18.1; p=0.001) than those without thrombophilia (Table 1). In comparison to patients without thrombophilia, the vast majority of patients with thrombophilia were diagnosed with PE during an emergency department visit (p=0.001), presented with dyspnea (p=0.02) and chest pain (p=0.008), and had a prior history of DVT (p=0.001) and PE (p=0.001). On the other hand, the non-thrombophilia group was more likely to have an in-hospital diagnosis (p=0.001), have a history of surgery more than 24 h (p=0.01), be bedridden (p=0.002), and have coronary artery disease (p=0.001), myocardial infarction (p=0.02), trauma (p=0.008), and long bone fracture (p=0.005). There were no significant differences between the two groups with respect to clinical presentation, comorbidities such as diabetes, hypertension, and congestive heart failure, and other predisposing factors like hypercholesterolemia, pelvic fracture, and paraplegia.
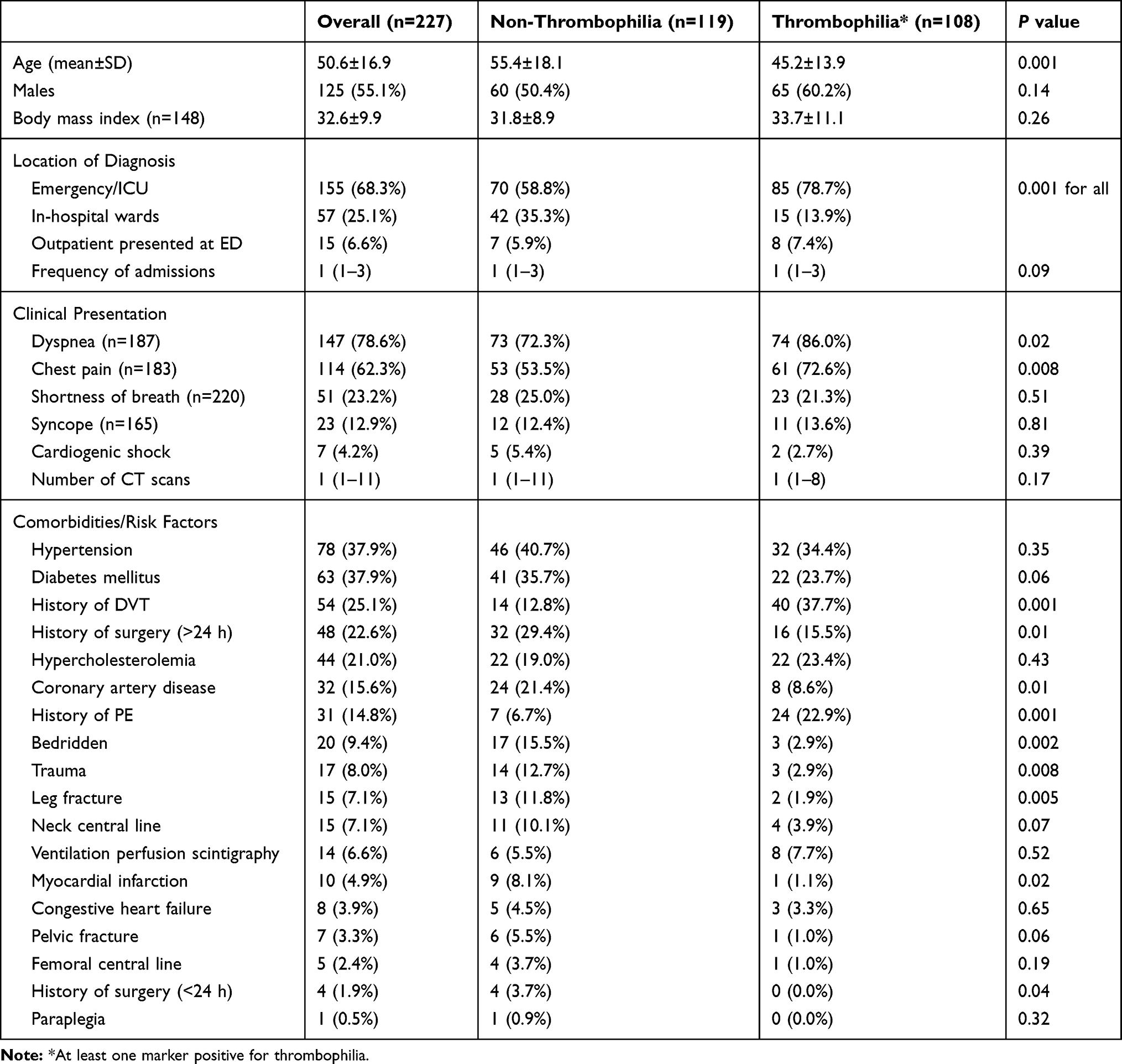 |
Table 1 Main Clinical Features and Risk Factors of Acute PE by Thrombophilia |
Table 2 compares the clinical probability scores. With respect to the clinical probability scores, the majority of subjects were in low probability (80.6%) using the simplified Wells score and of low risk using the revised Geneva score (94.3%) and simplified Pulmonary Embolism Severity Index (sPESI; 62.9%). The frequency of different risk categories of clinical probability scores did not differ significantly among those with and without thrombophilia.
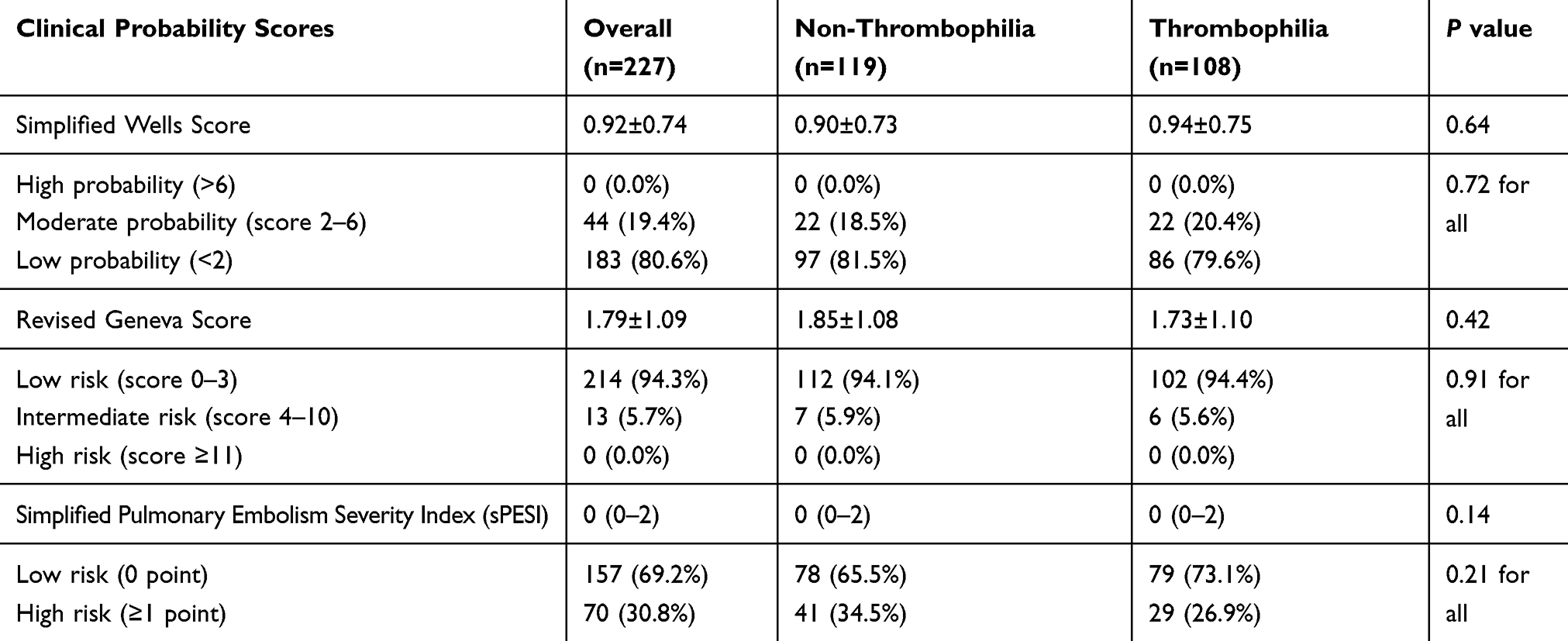 |
Table 2 Comparison of Clinical Probability Scores |
Hereditary Defects or Deficiency
The deficiencies of protein S (56.2%), protein C (51.7%), and antithrombin III (44.8%) and hyperhomocysteinemia (42.7%) were the most frequent hypercoagulopathic defects in our cohort. Only seven out of 79 patients (8.9%) were found to have factor V Leiden (Figure 1). The occurrence of thrombophilia according to different age groups in patients with acute PE is given in Figure 2. Thrombophilia showed an inverted bell-shaped curve with age groups which peaked in the age group of 30–39 years.
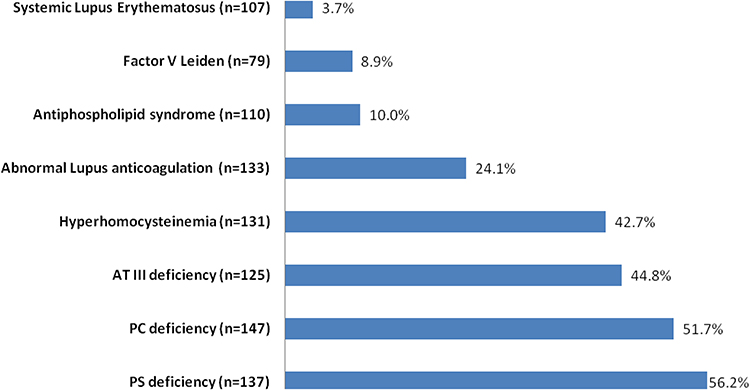 |
Figure 1 Distribution of thrombophilic disorders in patients with acute PE. |
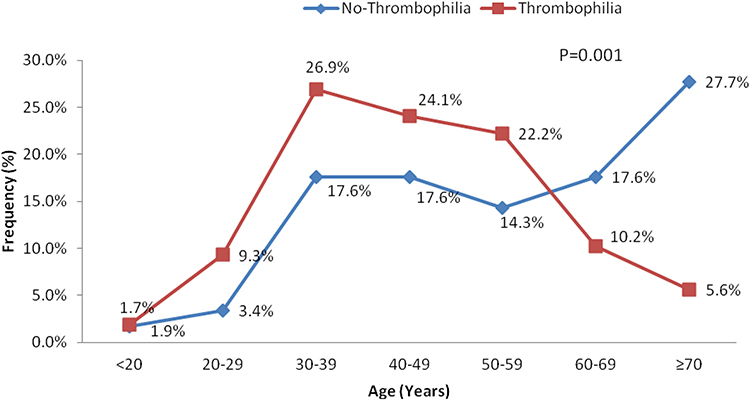 |
Figure 2 Occurrence of thrombophilia according to different age groups in patients with acute PE. |
Table 3 shows the comparison of management and outcome based on thrombophilia status.
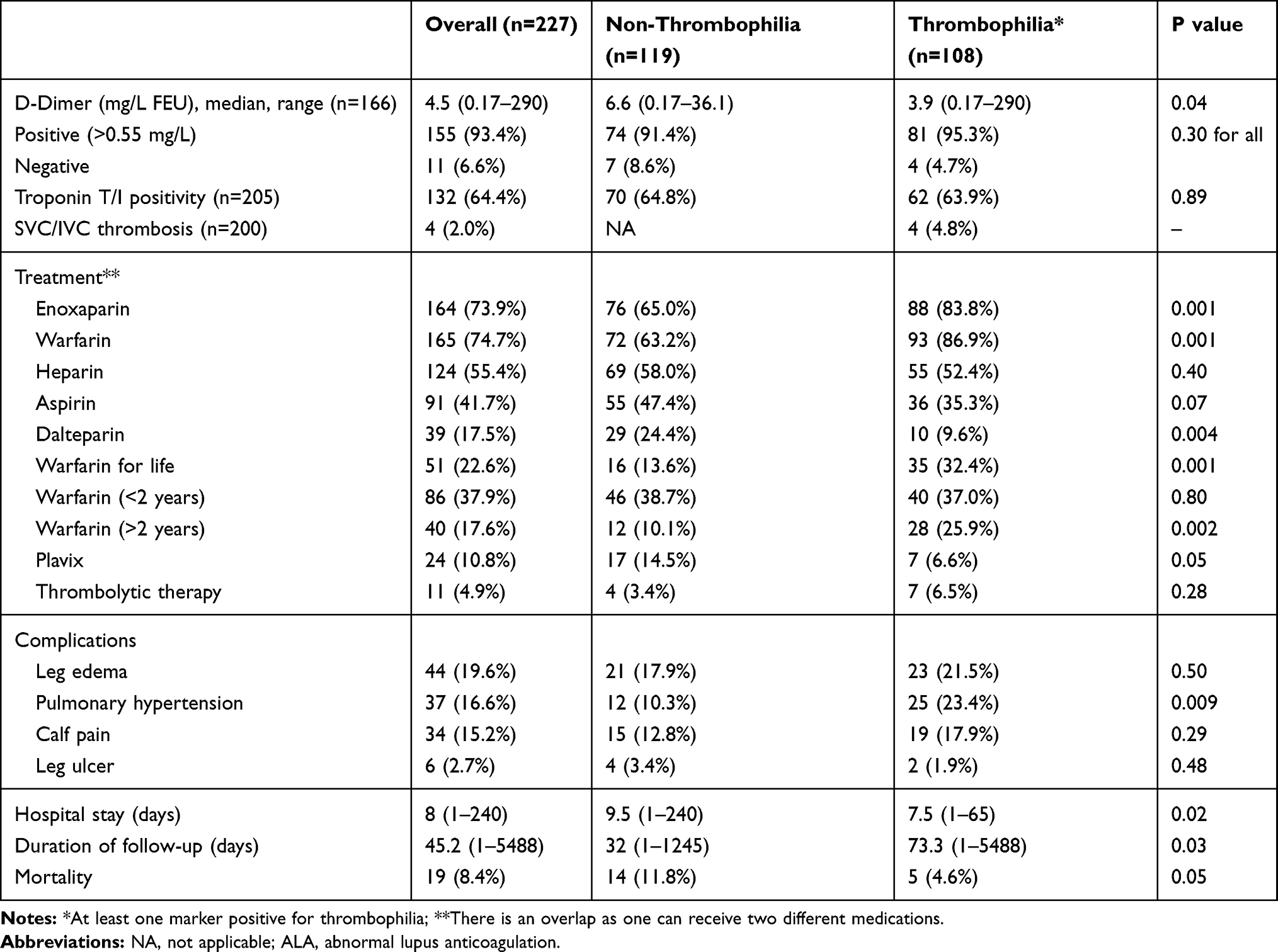 |
Table 3 Comparison of Management and Outcome |
The median D-dimer value was lower among patients in the thrombophilia group as compared to those in the non-thrombophilia group (p=0.04). Cardiac troponin was tested in 205 patients; of which 132 (64.4%) were found to have positive findings with no significant difference between the two groups. The most frequently used medications were warfarin (74.7%), enoxaparin (73.9%), heparin (55.4%), and aspirin (41.7%). PE patients with thrombophilia were frequently treated with enoxaparin (83.8% vs 65.0%, p=0.001) and warfarin (86.9% vs 63.2%, p=0.001) when compared to the non-thrombophilic group. A significantly higher proportion of patients with thrombophilia were treated with warfarin for more than 2 years (p=0.002) as well as continued warfarin for their lifetime (P=0.001). Antiplatelet treatment such as aspirin (47.4% vs 35.3%; p=0.07) and clopidogrel (14.5% vs 6.6%; P=0.05) was non-significantly higher in the non-thrombophilia than thrombophilia group. Almost 50% of patients were treated with heparin, with no significant difference between the two groups. However, PE patients in the non-thrombophilia group were more likely to be treated with dalteparin as compared to the thrombophilia group (24.4% vs 9.6%; p=0.004) respectively. Thrombolytic therapy was used only in 11 patients; 7 (6.5%) of them had thrombophilia.
The most common post-thrombotic complications were leg edema (19.6%), pulmonary hypertension (16.6%), and calf pain (15.2%). Patients in the thrombophilia group were more likely to develop pulmonary hypertension (23.4% vs 10.3%; p=0.009). Patients without thrombophilia were found to have a prolonged median length of stay as compared to those with thrombophilia (p=0.02). The overall all-cause mortality rate was 8.4% (19 patients), and the mortality rate was non-significantly higher in the non-thrombophilia group compared to the thrombophilia group.
Table 4 shows the presentation of the main clinical features of the thrombophilic group. Patients with APS were found to be the youngest with mean age 38.2±11.7 years, whereas patients with factor V Leiden were more likely to be older with mean age 51.4±14.3 years.
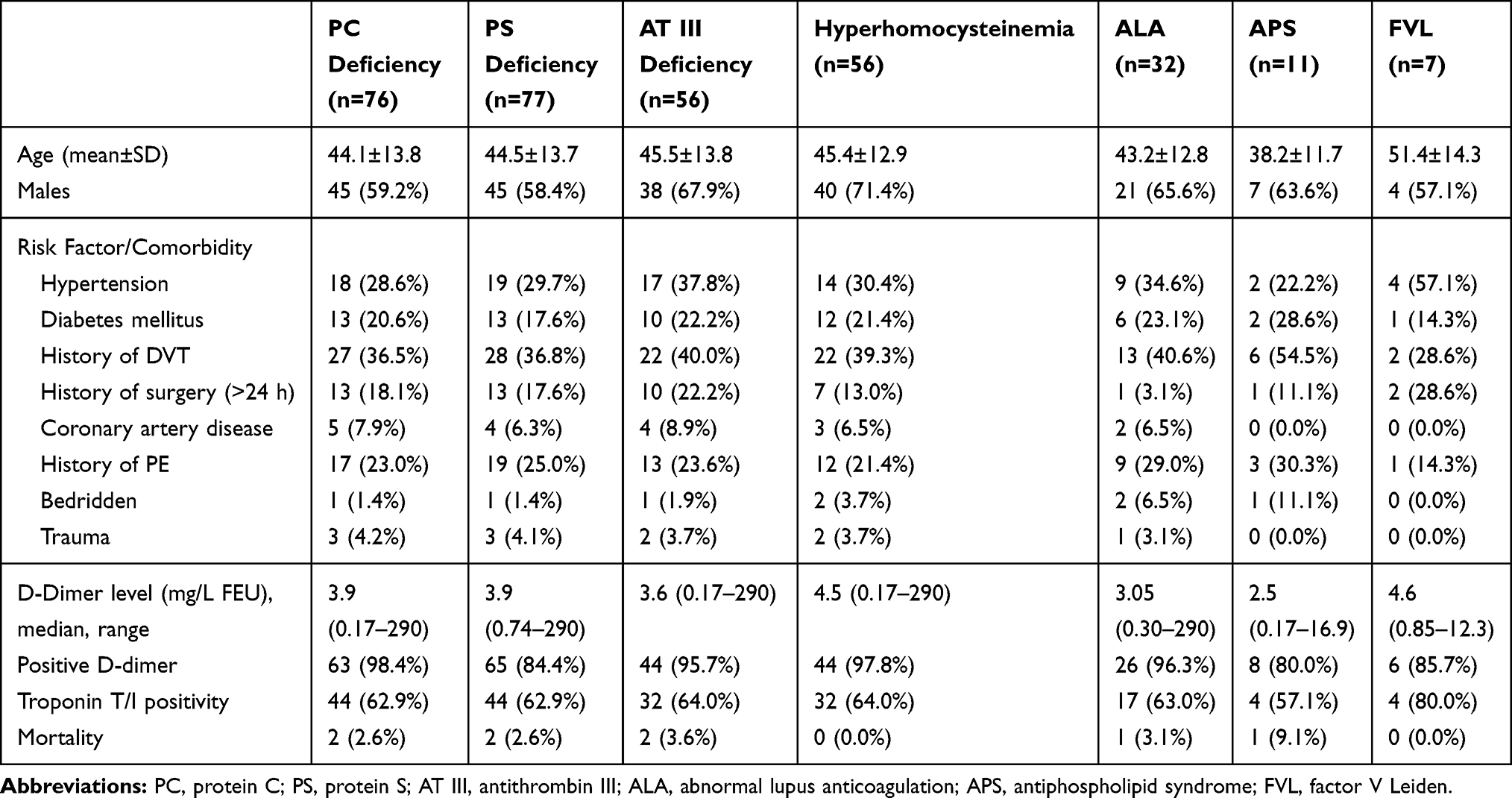 |
Table 4 Presentation of Main Clinical Features of the Thrombophilic Defects |
Male gender predominated among all of the groups with thrombotic disorders and was most frequent in patients with hyperhomocysteinemia (71.4%). History of DVT was most common in patients with AT III deficiency and hyperhomocysteinemia. Recurrent PE was more evident in those with lupus anticoagulant, antiphospholipid syndrome, and PS deficiency. However, thrombophilia defects were observed in less than 10% in bedridden, trauma and cardiac patients.
Positive D-dimer (>0.5 mg/L) was observed in more than 80% and it reached up to 98.4% in PC deficiency. Moreover, cardiac troponin positivity was observed in more than 60% of patients with different thrombophilic defects (80% in FVL). There was no mortality in patients with hyperhomocysteinemia and FVL. However, the mortality was lower among groups with different thrombophilic defects.
Discussion
The present study showed that nearly half of patients with acute PE had thrombophilic defects and the majority of them were diagnosed at an emergency department visit. The thrombophilic group was more likely to have a prior history of VTE. With respect to the clinical probability scores, the majority of subjects fell under the low-risk group. The frequency of thrombophilia peaked in the age group of 30–39 years. The risk of pulmonary hypertension is high in our cohort (16.6%) with a significant difference between the study groups (23% in patients with thrombophilia vs 10% in non-thrombophilia). This finding needs further evaluation.
Table 5 shows the review of studies based on VTE and thrombophilia.14–22 In the current literature, the frequency of hereditary thrombophilia varies possibly due to socio-ethnic diversity, and also depends upon the diagnostic modalities used in the different clinical settings.23 It has been reported that almost 40% of VTE can be explained by activated protein C (APC) resistance which is caused by mutation in factor V (factor V Leiden).24,25 Only 5–10% of the thrombophilic cases are associated with deficiency of AT, PC, and/or PS.21 Contrary to the previous reports, deficiencies of AT-III, PC, and PS and hyperhomocysteinemia were the most frequent hereditary thrombophilia subtypes in our cohort. As shown in Table 5, the published data suggest inconsistency in the occurrence of VTE among males and females.3 In the present study the proportion of males was slightly higher than females, which is consistent with an earlier study from our center and in the region.26,27 Also, PE patients with thrombophilia were more likely to be younger and more frequently had a history of recurrent VTE than those without thrombophilia. Notably, there is a steep decline in the frequency of hereditary thrombophilia with age in our cohort, which is also evident from findings of the MAISTHRO registry suggesting that this could be attributed to the decrease in frequency of genetic defects and deficiency of PC or PS in individuals that developed an initial VTE event at an advanced age.28
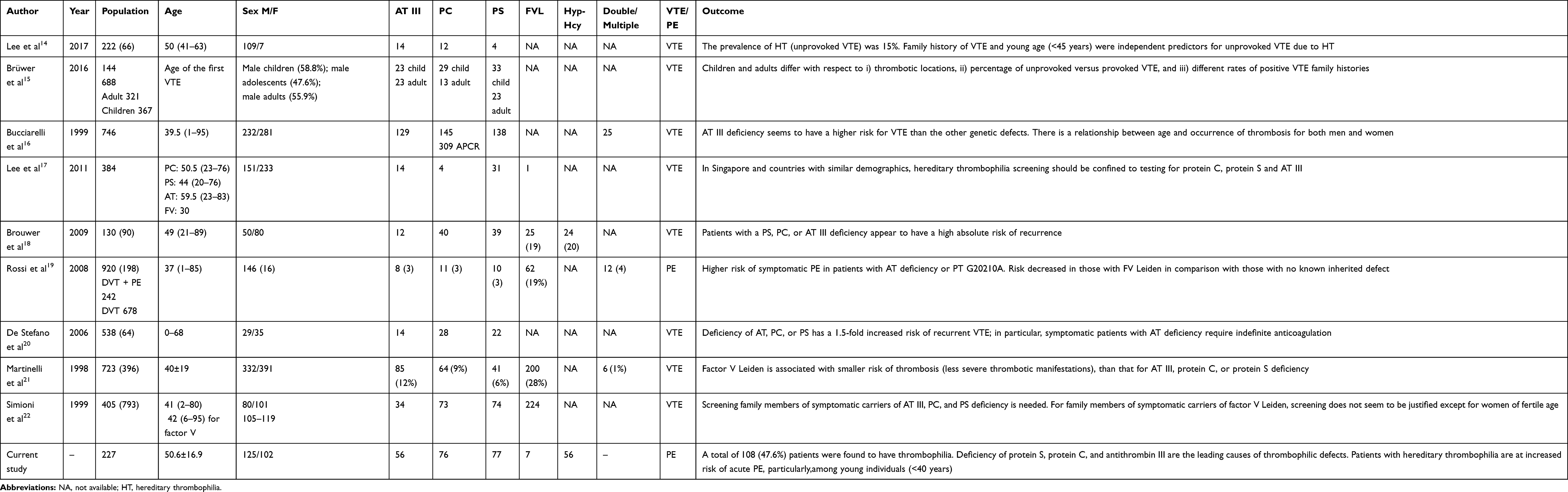 |
Table 5 Review of Literature for VTE and Thrombophilia |
Evidence suggests that around 10% of in-hospital mortalities are related to PE which often remains undiagnosed prior to death.13 Therefore, it is necessary to initiate early thromboprophylaxis in high-risk patients. In the present study, there is a higher predilection between PE diagnosed in the emergency department or in the ICU and thrombophilia.
Although hereditary thrombophilia and mainly deficiencies of PC and PS are known to have higher risk for myocardial infarction (MI),29 in our study the incidence of MI was significantly lower in the thrombophilia group. Notably, comorbidities were more frequent in the non-thrombophilia group.
Among various prognostic scorings, the sPESI is considered the most useful and validated tool to predict mortality in patients with PE.30 With respect to clinical probability scores, the majority of subjects were in low probability or risk and often have a better prognosis and there is no observed association of thrombophilia with the predicted risk of mortality in PE patients in the current study.
Moreover, in patients with acute PE, increased levels of cardiac troponin indicate the right ventricular strain which might be related to the higher risk of severe PE.31 In the current study, elevated cardiac troponin showed no significant association with thrombophilia and the risk of mortality.
Douketis et al32 suggested that PE patients are four times more likely to die due to recurrent VTE. Notably, in our cohort, patients with hereditary thrombophilia had longer treatment course due to increased risk of recurrence and about one-third continued to use anticoagulant for their lifetime. For unprovoked PE, the optimal treatment duration remains unknown and treatment could be extended beyond 3 months of duration.33 Lifetime continuation of anticoagulant in patients with lowrisk of bleeding was also recommended by some authors; particularly in males with second unprovoked PE and/or positive D-dimer testing after 1 month of stopping anticoagulant therapy.34
Chronic thromboembolic pulmonary hypertension is one of the serious complications of acute PE, which is observed in 16.6% of cases in our cohort. Also, we observed a significant association of pulmonary hypertension with hereditary thrombophilia. Our findings are in accordance with an earlier prospective study of 314 cases with acute PE.35
An earlier study suggested that deficiencies of PC or PS and AT III, and antiphospholipid antibodies are associated with an increased risk of recurrent VTE.28 In our study, 38% of patients presented with recurrent DVT and 23% had a prior history of PE; this is in agreement with earlier studies which demonstrated that patients with thrombophilia are at increased risk of recurrent VTE, which ranges between 36% and 62%.20,36 There is no association between family history of thrombosis and the risk of recurrent thrombosis in patients without protein C, protein S, or antithrombin deficiency.37
The overall mortality rate in our cohort was 8.4%, and the mortality rate was non-significantly higher in the non-thrombophilia group compared to the thrombophilia group. Consistent with our findings, a European Prospective Cohort on Thrombophilia identified no association of familial thrombophilia with the risk of mortality, irrespective of prior history of thrombosis.38 This could be explained by the fact that patients with familial thrombophilia are better aware of the symptoms of VTE, which increases the chances of early diagnosis and management; thereby conferring lower risk of complications and mortality.
Limitations
One limitation is the retrospective design which might influence the generalizability of our results and also the data obtained from a single center which limits the sample size. Another potential limitation is the timing of testing for thrombophilia. It is known that PS, PC, and AT III values can be misleadingly reduced due to consumption during the acute episode of VTE or during anticoagulant therapy.39 It is not clearly stated when blood samples were drawn, in particular, or the duration of symptoms and therapy used as this may overestimate or underestimate the prevalence of thrombophilia. However, based on our institutional guidelines we believed that all of the tests were performed after the initial presentation and in the absence of the anticoagulant, when possible. The analysis in our study was done based on the second result after 6 months. Finally, some of our patients were partially screened for thrombophilic defects, so there might be a possibility of underestimation of the true incidence of multiple thrombophilic risk factors. However, we believe that not every test that is available is necessary and thrombophilic testing should be customized on an individual basis.
In conclusion, deficiency of protein S, protein C, and antithrombin III isthe leading cause of thrombophilic defects in our cohort; however, the timing of measurement is crucial. Patients with hereditary thrombophilia are at increased risk of acute PE, particularly young individuals (<40 years). Importantly, one-third and one-fifth of DVTs and PEs respectively reoccur in the presence of thrombophilic risk factors and could therefore be prevented, if individuals are appropriately screened after a first VTE episode. Therefore, early detection of thrombophilic defects together with other unprovoked risk factors could reduce the risk of VTE in high-risk individuals. Furthermore, larger prospective studies are needed to confirm the findings of the present study.
Ethics Approval and Consent to Participate
This observational study has received expedited review and was approved by the Institutional Review Board (IRB#15139/15) at the Medical Research Center, Hamad Medical Corporation, Doha, Qatar. A waiver of consent was granted as there was no direct contact with subjects and data were anonymously and confidentially retrieved with compliance with the Declaration of Helsinki.
Consent for Publication
Approved by the Institutional Review Board (IRB#15139/15).
Data Sharing Statement
Data will be available upon request after approval and signing agreement with the medical research center.
Acknowledgments
We would like to thank all of the staff of the radiology department at Hamad General Hospital, for their contribution and support.
Author Contributions
MMO, AE, MA, and HA: all authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nagamalesh UM, Prakash VS, Naidu KCK, Sarthak S, Hegde AV, Abhinay T. Acute pulmonary thromboembolism: epidemiology, predictors, and long-term outcome – A single center experience. Indian Heart J. 2017;69:160–164. doi:10.1016/j.ihj.2016.08.010
2. Ceresetto JM. Venous thromboembolism in Latin America: a review and guide to diagnosis and treatment for primary care. Clinics (Sao Paulo). 2016;71:36–46. doi:10.6061/clinics/2016(01)07
3. White RH. The epidemiology of venous thromboembolism. Circulation. 2003;107(23 Suppl 1):I4–I8. doi:10.1161/01.CIR.0000078468.11849.66
4. Morrone D, Morrone V. Acute pulmonary embolism: focus on the clinical picture. Korean Circ J. 2018;48(5):365–381. doi:10.4070/kcj.2017.0314
5. Vossen CY, Conard J, Fontcuberta J, et al. Risk of a first venous thrombotic event in carriers of a familial thrombophilic defect. The European Prospective Cohort on Thrombophilia (EPCOT). J Thromb Haemost. 2005;3:459–464. doi:10.1111/jth.2005.3.issue-3
6. McRae S. Pulmonary embolism. Aust Fam Physician. 2010;39:462–466.
7. Moheimani F, Jackson DE. Venous thromboembolism: classification, risk factors, diagnosis, and management. ISRN Hematol. 2011;2011:124610. doi:10.5402/2011/124610
8. Merriman L, Greaves M. Testing for thrombophilia: an evidence-based approach. Postgrad Med J. 2006;82(973):699–704. doi:10.1136/pgmj.2006.048090
9. Canadian Agency for Drugs and Technologies in Health. Effectiveness of Factor V Leiden and Prothrombin Mutation Testing in Patients Presenting with a First Unprovoked Venous Thromboembolic Episode: A Systematic Review and Economic Analysis [Internet]. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; March, 2015. Available from http://www.ncbi.nlm.nih.gov/books/NBK361450/.
10. Khan S, Dickerman JD. Hereditary thrombophilia. Thromb J. 2006;4:15. doi:10.1186/1477-9560-4-15
11. Ali N, Ayyub M, Khan SA. High prevalence of protein C, protein S, antithrombin deficiency, and Factor V Leiden mutation as a cause of hereditary thrombophilia in patients of venous thromboembolism and cerebrovascular accident. Pak J Med Sci. 2014;30:1323–1326. doi:10.12669/pjms.306.5878
12. Crowther MA, Kelton JG. Congenital thrombophilic states associated with venous thrombosis: a qualitative overview and proposed classification system. Ann Intern Med. 2003;138:128–134. doi:10.7326/0003-4819-138-2-200301210-00014
13. Di Minno MN, Ambrosino P, Ageno W, Rosendaal F, Di Minno G, Dentali F. Natural anticoagulants deficiency and the risk of venous thromboembolism: a meta-analysis of observational studies. Thromb Res. 2015;135(5):923–932. doi:10.1016/j.thromres.2015.03.010
14. Lee SY, Kim EK, Kim MS, et al. The prevalence and clinical manifestation of hereditary thrombophilia in Korean patients with unprovoked venous thromboembolisms. PLoS One. 2017;12(10):e0185785. doi:10.1371/journal.pone.0185785
15. Brüwer G, Limperger V, Kenet G, et al. Impact of high risk thrombophilia status on recurrence among children and adults with VTE: an observational multicenter cohort study. Blood Cells Mol Dis. 2016;62:24–31. doi:10.1016/j.bcmd.2016.10.024
16. Bucciarelli P, Rosendaal FR, Tripodi A, et al. Risk of venous thromboembolism and clinical manifestations in carriers of antithrombin, protein C, protein S deficiency, or activated protein C resistance: a multicenter collaborative family study. Arterioscler Thromb Vasc Biol. 1999;19(4):1026–1033. doi:10.1161/01.ATV.19.4.1026
17. Lee LH, Liu TC, Kuperan P, et al. Hereditary thrombophilia in an unselected cohort of venous thrombosis patients in Singapore. J Clin Pathol. 2011;64:814–817. doi:10.1136/jclinpath-2011-200018
18. Brouwer JL, Lijfering WM, Ten Kate MK, Kluin-Nelemans HC, Veeger NJ, van der Meer J. High long-term absolute risk of recurrent venous thromboembolism in patients with hereditary deficiencies of protein S, protein C or antithrombin. Thromb Haemost. 2009;101(1):93–99. doi:10.1160/TH08-06-0364
19. Rossi E, Za T, Ciminello A, Leone G, De Stefano V. The risk of symptomatic pulmonary embolism due to proximal deep venous thrombosis differs in patients with different types of inherited thrombophilia. Thromb Haemost. 2008;99:1030–1034. doi:10.1160/TH08-02-0069
20. De Stefano V, Simioni P, Rossi E, et al. The risk of recurrent venous thromboembolism in patients with inherited deficiency of natural anticoagulants antithrombin, protein C and protein S. Haematologica. 2006;91:695–698.
21. Martinelli I, Mannucci PM, De Stefano V, et al. Different risks of thrombosis in four coagulation defects associated with inherited thrombophilia: a study of 150 families. Blood. 1998;92(7):2353–2358. doi:10.1182/blood.V92.7.2353
22. Simioni P, Sanson BJ, Prandoni P, et al. Incidence of venous thromboembolism in families with inherited thrombophilia. Thromb Haemost. 1999;81(2):198–202. doi:10.1055/s-0037-1614442
23. Pai N, Ghosh K, Shetty S. Cause of deep venous thrombosis and pulmonary embolism in young patients from India as compared with other ethnic groups. Blood Coagul Fibrinolysis. 2012;23:257–261. doi:10.1097/MBC.0b013e3283502961
24. De Stefano V, Finazzi G, Mannucci PM. Inherited thrombophilia: pathogenesis, clinical syndromes, and management. Blood. 1996;87(9):3531–3544. doi:10.1182/blood.V87.9.3531.bloodjournal8793531
25. Ridker PM, Hennekens CH, Lindpaintner K, Stampfer MJ, Eisenberg PR, Miletich JP. Mutation in the gene coding for coagulation factor V and the risk of myocardial infarction, stroke, and venous thrombosis in apparently healthy men. N Engl J Med. 1995;332(14):912–917. doi:10.1056/NEJM199504063321403
26. El-Menyar A, Nabir S, Ahmed N, Asim M, Jabbour G, Al-Thani H. Diagnostic implications of computed tomography pulmonary angiography in patients with pulmonary embolism. Ann Thorac Med. 2016;11(4):269–276. doi:10.4103/1817-1737.191868
27. Al Otair HA, Al-Boukai AA, Ibrahim GF, Al Shaikh MK, Mayet AY, Al-Hajjaj MS. Outcome of pulmonary embolism and clinico-radiological predictors of mortality: experience from a university hospital in Saudi Arabia. Ann Thorac Med. 2014;9:18–22. doi:10.4103/1817-1737.124420
28. Weingarz L, Schwonberg J, Schindewolf M, et al. Prevalence of thrombophilia according to age at the first manifestation of venous thromboembolism: results from the MAISTHRO registry. Br J Haematol. 2013;163:655–665. doi:10.1111/bjh.12575
29. Mahmoodi BK, Brouwer JL, Veeger NJ, van der Meer J. Hereditary deficiency of protein C or protein S confers increased risk of arterial thromboembolic events at a young age: results from a large family cohort study. Circulation. 2008;118(16):1659–1667. doi:10.1161/CIRCULATIONAHA.108.780759
30. Shafiq A, Lodhi H, Ahmed Z, Bajwa A. Is the pulmonary embolism severity index being routinely used in clinical practice? Thrombosis. 2015;2015:175357. doi:10.1155/2015/175357
31. Becattini C, Vedovati MC, Agnelli G. Prognostic value of troponins in acute pulmonary embolism: a meta-analysis. Circulation. 2007;116:427–433. doi:10.1161/CIRCULATIONAHA.106.680421
32. Douketis JD, Kearon C, Bates S, Duku EK, Ginsberg JS. Risk of fatal pulmonary embolism in patients with treated venous thromboembolism. JAMA. 1998;279:458–462. doi:10.1001/jama.279.6.458
33. Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S–e496S. doi:10.1378/chest.11-2301
34. Kearon C, Akl EA. Duration of anticoagulant therapy for deep vein thrombosis and pulmonary embolism. Blood. 2014;123(12):1794–1801. doi:10.1182/blood-2013-12-512681
35. Pengo V, Lensing AW, Prins MH, et al.; Thromboembolic Pulmonary Hypertension Study Group. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med. 2004;350(22):2257–2264. doi:10.1056/NEJMoa032274
36. van den Belt AG, Sanson BJ, Simioni P, et al. Recurrence of venous thromboembolism in patients with familial thrombophilia. Arch Intern Med. 1997;157(19):2227–2232. doi:10.1001/archinte.1997.00440400077009
37. Hron G, Eichinger S, Weltermann A, et al. Family history for venous thromboembolism and the risk for recurrence. Am J Med. 2006;119(1):50–53. doi:10.1016/j.amjmed.2005.04.043
38. Pabinger I, Vossen CY, Lang J, et al. Mortality and inherited thrombophilia: results from the European Prospective Cohort on Thrombophilia. J Thromb Haemost. 2012;10(2):217–222. doi:10.1111/j.1538-7836.2011.04573.x
39. Stevens SM, Woller SC, Bauer KA, et al. Guidance for the evaluation and treatment of hereditary and acquired thrombophilia. J Thromb Thrombolysis. 2016;41(1):154–164. doi:10.1007/s11239-015-1316-1
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.