")
Back to Journals » Infection and Drug Resistance » Volume 15
Prevalence and Multi-Drug Resistance of Streptococcus pneumoniae Infection Among Presumptive Tuberculosis Adult Cases at Dilla University Referral Hospital, Dilla, Ethiopia
Authors Kaloro Halala B, Ali MM , Ormago MD
Received 17 June 2022
Accepted for publication 19 August 2022
Published 5 September 2022 Volume 2022:15 Pages 5183—5191
DOI https://doi.org/10.2147/IDR.S375343
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Benyiam Kaloro Halala,1 Musa Mohammed Ali,2 Moges Desta Ormago2
1Referral Hospital, Dilla University, Dilla, Ethiopia; 2School of Medical Laboratory Science, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia
Correspondence: Moges Desta Ormago, Email [email protected]
Introduction: Streptococcus pneumoniae is the leading cause of community-acquired pneumonia in Africa. The simultaneous occurrence of both infections leads to delayed diagnosis and inadequate treatment. The study aimed to determine the prevalence, antimicrobial susceptibility pattern and associated factors of Streptococcus pneumoniae infection among presumptive Tuberculosis adult cases at Dilla University Referral Hospital, Dilla, Ethiopia.
Methods: An institution-based cross-sectional study was conducted on 422 presumptive TB cases visiting TB clinic at Dilla University Referral Hospital from April to June 2021. Following the Bartlett’s criteria, the accepted sputum samples were cultured on Blood agar plate and chocolate agar plate. Streptococcus pneumoniae was identified and confirmed by typical colony morphology, alpha-hemolysis, gram staining, optochin susceptibility and bile solubility tests. Antimicrobial susceptibility test was done by using the Kirby-Bauer disc diffusion method. Semi-structured questionnaires were used to collect data. Bivariate and multivariate logistic regression analyses were done by using SPSS version 23.0, computer software.
Results: The overall prevalence of S. pneumoniae in presumptive tuberculosis adult cases was 21.4% (95% CI: 17.7– 25.5). S. pneumoniae has a high level of resistance to penicillin (74.1%), tetracycline (78.7%) and Trimethoprim-sulfamethoxazole (46%). Multidrug resistance was observed in 46.1% of bacterial isolates. Being primary education, more than five family size and one or two rooms in the house had more likely to cause S. pneumoniae infection.
Conclusion: This study revealed a relatively high prevalence of multidrug resistance of Streptococcus pneumoniae infection. Primary educational status, living in a crowded family, below two rooms in the house, had a significant association with S. pneumoniae infection.
Keywords: S. pneumoniae, antimicrobial susceptibility, tuberculosis, Dilla, Ethiopia
Introduction
Tuberculosis and pulmonary pneumonia are both lower respiratory tract infections that affect almost all classes of people mostly in developing countries.1 Pneumonia can be spread in the nose or throat and can infect the lungs if they are inhaled. They may also spread via airborne droplets from a cough or sneeze. In addition, pneumonia may spread through contact and blood, especially during and after birth.2,3 S. pneumoniae (pneumococcus) is a major cause of the disease, ranging from uncomplicated respiratory tract infections to severe invasive pneumococcal disease (IPD).4
Streptococcus pneumoniae (S. pneumoniae) is the major cause of morbidity and mortality in the world.5,6 It contributes to 120 million new pneumonia infections worldwide, 14 million of which were severe enough to require hospitalization.7 Surveillance data on S. pneumoniae infections are few if available to health care providers1. S. pneumoniae (pneumococcus) is a major cause of disease, ranging from uncomplicated respiratory tract infections to severe invasive pneumococcal disease (IPD).2 Studies in Hawassa, Ethiopia, reported that among commonest microbes causing pneumonia, the proportion of S. pneumoniae was 6%8 and 18.1%, and another study in Addis Ababa, Ethiopia, showed the proportion of S. pneumoniae was 18.5%.9
Tuberculosis in men is caused by Mycobacterium tuberculosis, and according to the 2021 global TB report, ten million people were estimated to have TB cases, and 1.3 million TB deaths were among HIV-negative and 214,000 TB deaths were among HIV-positive people every year though TB drugs are effective and given freely to patients in developing countries including Ethiopia.10
Antimicrobial-resistant strains of Streptococcus pneumoniae have become one of the greatest challenges to global public health today, and inappropriate use of antibiotics and high level of antibiotic use are probably the main factors driving the emergence of resistance worldwide. The susceptibility of penicillin (61.7%) to S. pneumoniae globally was the lowest one of all antibiotics in the TEST panel. Africa, Asia, and the Middle East were the sources of isolates with 43.5%, 29.9%, and 20.7% susceptibility, respectively.11 Study in two regions of Ethiopia showed that of the 57 isolates, 17.5% were fully resistant to penicillin, and multidrug resistance (MDR) was seen in 33.3% isolates.12
Mortality due to pneumonia is strongly linked to poverty-related factors such as undernutrition, lack of safe drinking water and sanitation, indoor and outdoor air pollution, and inadequate access to health care.13,14 A timely diagnosis of pneumonia is an essential step in the prevention process of the disease. X-ray and laboratory identification of the causative agent is the confirmatory tools to certainly establish the diagnosis of pneumonia.15 While these are largely unaffordable in resource-poor settings like Ethiopia16 and it cannot be assumed that all respiratory symptoms have bacterial pneumonia and should receive antibiotics, the data indicate a big gap between the rich and the poor in the treatment of symptoms of pneumonia, receiving care for pneumonia symptoms from a healthcare provider. Furthermore, in sub-Saharan Africa, where most deaths from pneumonia occur, only 47% of children with pneumonia symptoms are taken for care, with the lowest proportions in Western and Central Africa.14
However, Ethiopia is among the highest burden of pneumonia.17 Co-infection with tuberculosis (TB) and bacteria has not been widely reported. Although the superadded bacterial infection can occur in TB patients, the simultaneous occurrence of both infections leads to delayed diagnosis and inadequate treatment. Tubercular-bacterial co-infection needs to be considered, especially if TB occurs in atypical pulmonary or extra-pulmonary locations.18 Hence, information on Streptococcus pneumonia infection and drug susceptibility patterns are very important for the proper selection and use of antibiotic agents. Therefore, this study aimed to determine the prevalence and multi-drug resistance of Streptococcus pneumoniae Infection among Presumptive Tuberculosis Adult Cases at Dilla University Referral Hospital, Dilla, Ethiopia.
Materials and Methods
Study Setting
The study was conducted at Dilla University Referral Hospital (DURH) from April to June 2021. The Hospital is found in Dilla town which is the capital city of Gedeo zone, South Nations Nationalities and People Region (SNNPR), and it is located at 5°27´ N latitude and 38°8´ to 38°30´ east longitude with an elevation of 1570m above sea level. The town is 365 km far away from Addis Ababa and is located on the main road from Addis Ababa to Nairobi at the eastern edge of the Rift valley. Dilla University Hospital in its laboratory diagnostic department provides microbiological analysis including bacterial culture, identification and drug susceptibility testing from clinical samples. Patients visiting the outpatient department of the hospital with signs and symptoms suggestive of TB or with CXR abnormalities suggestive of TB were bacteriologically confirmed by using Xpert MTB/RIF assay.
Study Design and Participants
A facility-based cross-sectional study design was conducted among presumptive tuberculosis adult patients attending DURH. Since there was no previous study in the area, sample size was determined by considering the following: prevalence of Streptococcus pneumoniae infection = 50%, margin of error = 5%, 95% confidence level = 95%, and non-response rate = 10%. Accordingly, the total sample size was 422.
Systematic random sampling technique was applied to select 422 respondents for interview. The interval (K) was obtained by dividing the total number of patients attending the medical OPD for LRTI during the study period by sample size. According to information found from the database of DURH, the average daily patient flow due to LRTI at OPD is 19. The study period took 3 months, which contain 66 days and 19 times 66 gives 1254. Therefore, the total patient flow during the study period is 1254.
K = 1254/422 = 2.9≈ 3
One of the first three presumptive tuberculosis cases was selected by a simple random sampling method. So, every 3rd presumptive tuberculosis case who came to the adult OPD in the study period was recruited until the required amount of sample was attained.
Data Collection and Laboratory Processing
Socio-demographic and clinical data were collected by trained nurses through face-to-face interviews with the patient using a semi-structured questionnaire from 422 respondents whose sputum samples fulfill Bartlett’s criteria on Grams stain. Single sputum samples were collected using dry, sterile, leak-proof, translucent, and screw-capped plastic containers with a capacity of 30 mL and brought to the Microbiology Laboratory of Dilla University Referral Hospital for laboratory processing.
Gram’s Stain
Quality of sputum samples was checked macroscopically for color, volume, viscosity, and odor and microscopically based on Bartlett’s criteria, and any positive score (sum of + and – values assigned) on Gram’s stain was considered an acceptable result to be cultured.19
Cultivation and Identification of Isolates
The purulent part of the accepted sputum samples was cultured on Blood agar plate (Oxoid, Hampshire, UK) and chocolate agar plate (Oxoid, Hampshire, UK) with a sterile wire loop and incubated in CO2 enriched atmosphere at 37°C for 24 hours. Streptococcus pneumoniae was then identified and confirmed by typical colony morphology, alpha-hemolysis, gram staining, optochin susceptibility and bile solubility tests.20
Antibiotic Susceptibility Testing
The disk diffusion method (Kirby–Bauer) was carried out using Muller Hinton agar (Oxoid, Hampshire, UK) supplemented with 5% sheep’s blood for fastidious organisms as recommended by the Clinical and Laboratory Standard Institute (CLSI, 2020). Similar pure colonies were sub-cultured into the nutrient broth, mixed, and incubated for 2–6 hours at 35–37°C.21 The suspension was evenly inoculated onto Mueller–Hinton agar. Antibiotics tested include trimethoprim-sulfamethoxazole (SXT) (1.25/23.75μg), erythromycin (ERY) (15μg), vancomycin (VAN) (30μg), tetracycline (TTC) (30μg), chloramphenicol (CHL) (30μg) and clindamycin (CLM) (2μg). The zone of inhibition was measured after 18–24 hours of incubation at 35–37°C and interpreted as susceptible, intermediate, or resistant.22
Quality Control
The consistency of the questionnaire was assured by pre-testing 5% of the questionnaires before the actual data collection. For quality control, a reference strain S. pneumoniae ATCC 49619 was used. Before use, all culture media were tested for sterility.
Data Entry and Analysis
Entry, cleaning and analysis of data were done by using SPSS version 23 software. Descriptive statistics were done using frequency and percentage to present the findings in the form of graphs and tables. Variables with a p-value <0.25 on bivariate analysis were selected for multivariate analysis. The multivariate analysis was used to determine the association between covariates and the outcome variables. Odds ratio (OR) with 95% CIs calculated from the multivariate logistic regression adjusting for possible confounding (AOR) was used to determine the presence and strength of the association between dependent and independent variables, and P-values <0.05 was considered as a cut point.
Results
Socio-Demographic, Environmental and Behavioral Characteristics
A total of 416 presumptive tuberculosis adult cases were participated with a response rate of 98.6%. The mean age was 27.3 (±9.6). Two hundred one (48.3%) were in the 18–24-year age category, 230 (55.3%) were males, 274 (65.9%) were urban dwellers, 210 (50.5%) were single and 77 (18.5%) were illiterate. Regarding environmental and behavioral characteristics, the majority 289 (69.5%) were living in a Mud/soil floor house, 295 (70.9%) had at least two windows, 27 (6.5%) had ever used any tobacco products, 14 (3.4%) were smoke cigarettes in last 30 days and 71 (17.1%) had ever drunk alcohol (Table 1)
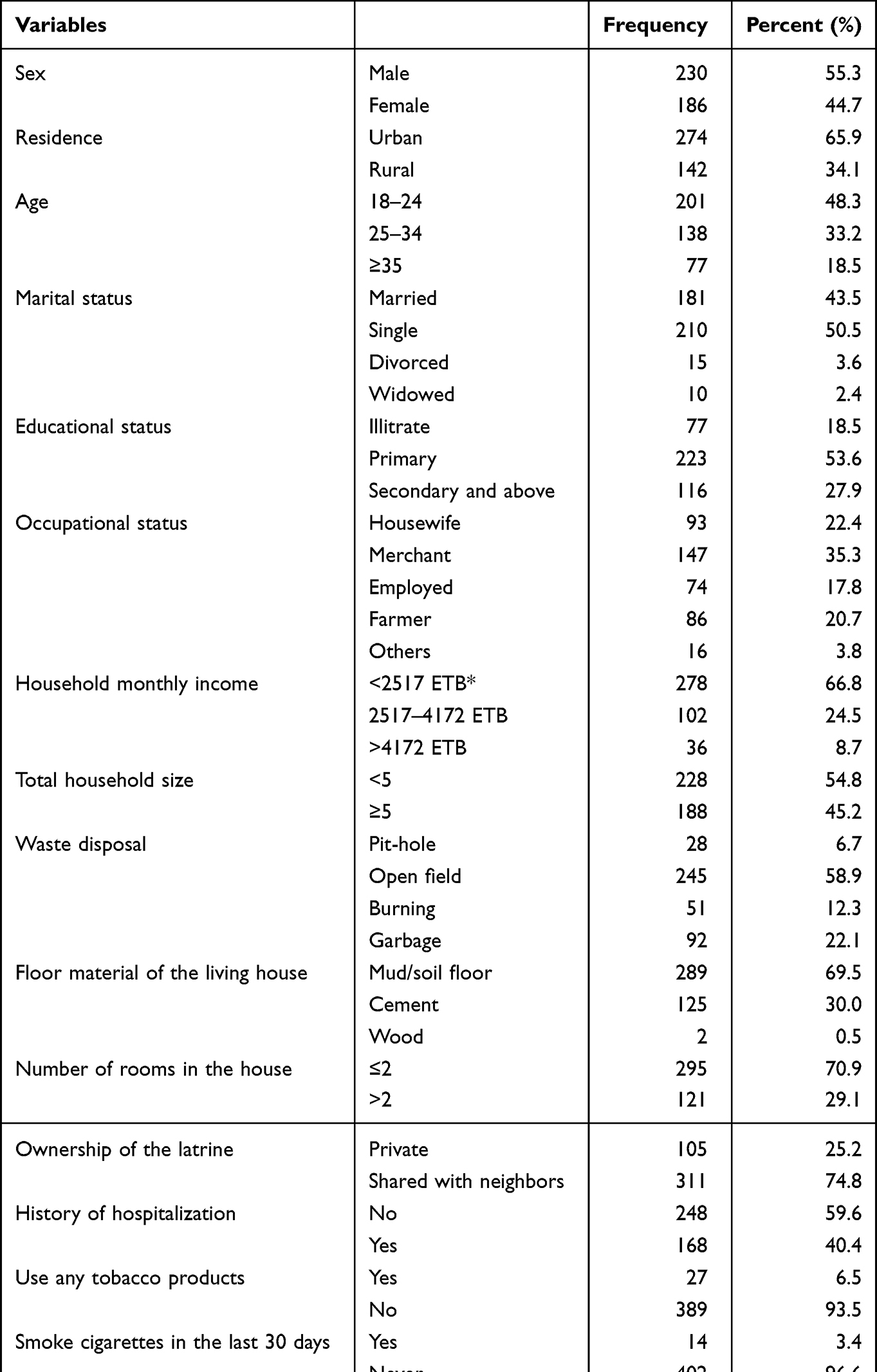 |
Table 1 Socio-Demographic, Environmental and Behavioral Characteristics of Presumptive Tuberculosis Adult Cases at Dilla University Referral Hospital, Dilla, Ethiopia, 2021 (n = 416) |
The Prevalence and Antimicrobial Susceptibility Pattern of S. pneumoniae
The overall prevalence of S. pneumoniae in presumptive tuberculosis adult cases was 89 (21.4%) (95% CI: 17.7–25.5). The prevalence of S. pneumoniae among illiterate participants (29.9%) was higher than participants with primary education (20.2%) and S. pneumoniae infection among participants living in one or two rooms in the house (27.5%) were fourfold higher than participants living in more than two rooms in the house (6.6%).
Twenty-three (25.8%) isolates of S. pneumonia were susceptible to all of the antibiotics tested, 16 (18%) were resistant to one antimicrobial agent, 9 (10.1%) were resistant to two antimicrobial agents and 41 (46.1%) were resistant to three or more antimicrobial agents (multi-drug resistant). S. pneumoniae isolates were resistant to erythromycin 43 (48.3%), trimethoprim-sulfamethoxazole 36 (40.4%), tetracycline 36 (40.4%) and susceptible to clindamycin 76 (85.4%) and chloramphenicol 73 (82%) (Table 2).
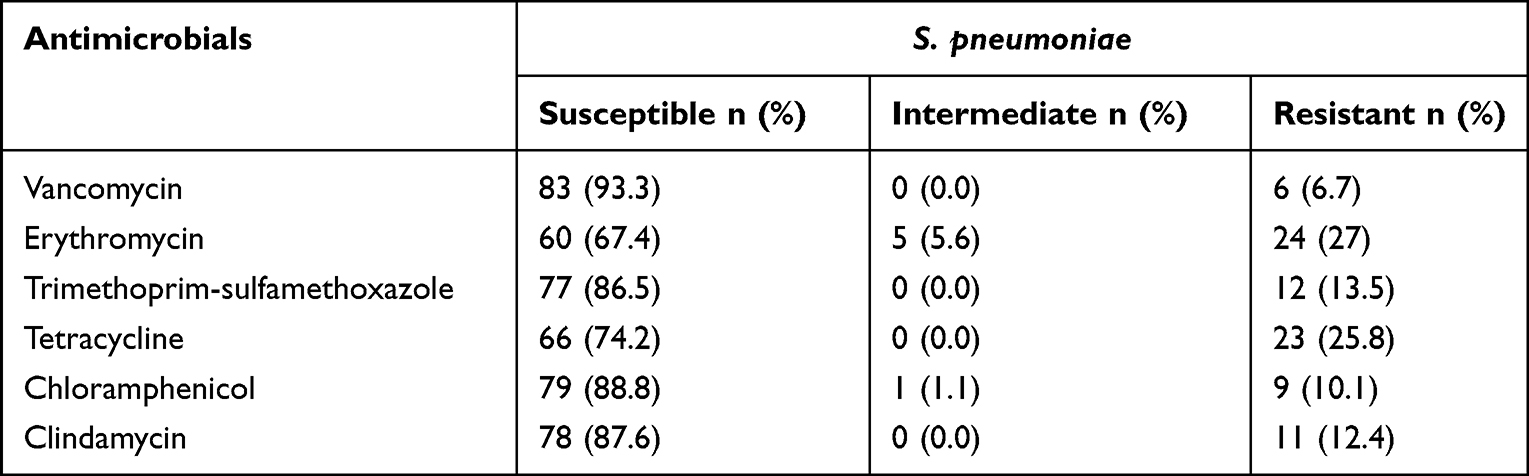 |
Table 2 Antimicrobial Susceptibility Pattern of S. pneumoniae Isolates from Sputum Samples Collected from Presumptive Tuberculosis Adult Cases at Dilla University Referral Hospital, Dilla, Ethiopia, 2021 (n = 89) |
Associated Factors of S. pneumoniae Infections
The variables that had a P value <0.25 by bivariate analysis and became a candidate for multivariate analysis were residence, age, educational status, total household size, number of rooms in the house, ownership of the latrine, history of hospitalization and ever-drunk alcohol were found to be potentially associated with the prevalence of S. pneumoniae. In the multivariate analysis, the study participants who had primary educational status were about three times more frequently exposed to S. pneumoniae with [AOR = 2.95, 95% CI (1.39, 6.27)] as compared with secondary and above education. Family size of more than five [AOR = 1.85, 95% CI: (1.11, 3.08)] and two or fewer rooms in the house [AOR = 5.69, 95% CI: (2.59, 12.53)] had high odds of exposure to S. pneumoniae infection as compared to their counterparts. Furthermore, the study participants who shared a latrine with a neighbor also had about 2.5 times more frequently exposed to S. pneumoniae [AOR = 2.47, 95% CI (1.23, 4.97)] when it compared with those who had a private latrine (Table 3).
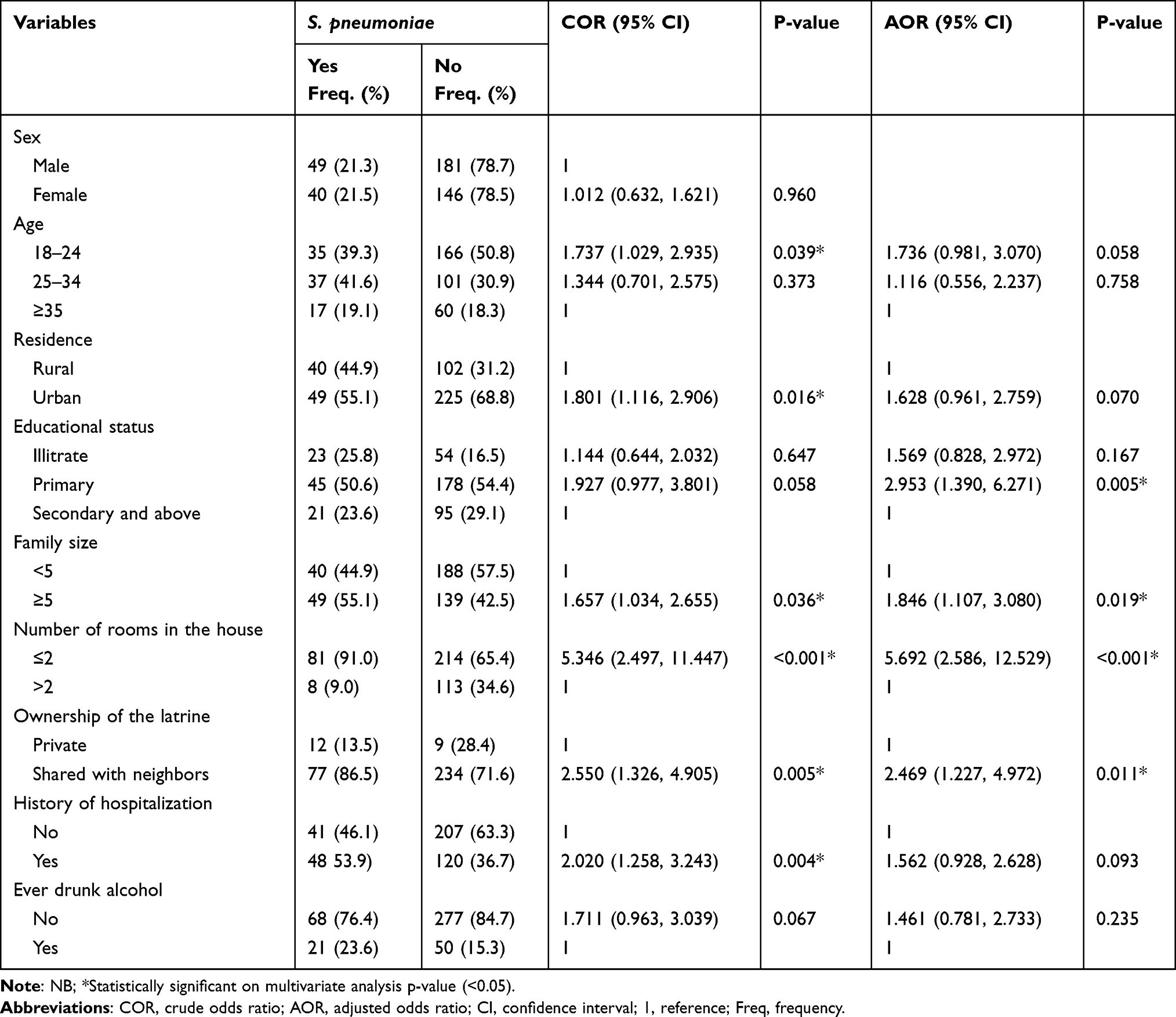 |
Table 3 Bivariate and Multivariate Logistic Regression Analyses of Factors Associated with S. pneumoniae Infection Among Presumptive Tuberculosis Adult Cases at Dilla University Referral Hospital, Dilla, Ethiopia, 2021 (n = 416) |
Discussion
The overall prevalence of S. pneumoniae infection in presumptive Tuberculosis adult cases at Dilla University Referral Hospital, Dilla, Ethiopia, was 89 (21.4%) (95% CI: 17.7–25.5). This study finding was comparable to results reported from Biratnagar, Nepal (21.3%),23 and Beira, Mozambique (23%).24 Our finding is higher than findings reported from Ekpoma, Nigeria (6.4%),1 Ogun state, Nigeria (8.8%),25 Sokoto, North-Western Nigeria (5.6%), and 7.3% in Kano teaching hospital, northern Nigeria.26 On the other hand, the finding of this study is lower than the one reported from Jimma, South-west Ethiopia (43%).27 The reason could be due to geographical distribution, sample size, educational background, and other socio-economic factors.
In this study, S. pneumoniae was sensitive to clindamycin (87.6%), vancomycin (93.3%), trimethoprim-sulfamethoxazole (86.5%), chloramphenicol (88.8%). The higher sensitivity of S. pneumoniae was reported in Hawassa, Ethiopia, for clindamycin (88.9%),28 and in Arsi, Ethiopia, for vancomycin (97.7%) and chloramphenicol (94.3%).29
In our study, S. pneumoniae was resistant to erythromycin (27%) and tetracycline (25.8%). Resistant to S. pneumoniae was reported in Addis Ababa, Ethiopia, for erythromycin (40%)9 and Gonder, Ethiopia, for tetracycline (31.3%).30
The overall magnitude of multidrug resistance (MDR) was 46.1%. This result was higher than the previous studies which were conducted in Hawassa, Ethiopia (11.1%),28 Addis Ababa and Amhara region, Ethiopia (33.3%),12 and lower than other studies in Addis Ababa, Ethiopia (66.7%).9
This may be due to the wide use of this antibiotic in the communities because of its dose convenience, cost-effectiveness, easy availability in any pharmacy and the trend of sharing the drugs in the community. In addition to this, remarkable differences might have occurred because of the random use of antibiotics, the poor implementation of antibiotic policy and control in the study area may aggravate the situation.
History of hospitalization had a higher prevalence of S. pneumoniae infection (53.9%) among presumptive tuberculosis adult cases. This study result also agreed with the study report on S. pneumoniae infection and history of hospitalization in Hawassa, Southern Ethiopia (53.8%)31 and in Gondar University Hospital, Northwest Ethiopia (76.6%).30 This may be due to acquiring the infection from the hospital environment during management of the patient for different reasons of admission.
This study also showed that the study participants who had primary school participants were three times more likely to be exposed to S. pneumoniae than participants with secondary and above education. This study result was consistent with the study report in Mekelle Zone, Tigray, Northern Ethiopia32 and in Ogun State, Nigeria.25 The possible explanation for this may be that lower educational status was more exposed to environmental contaminants, like dust, animal dung, and lack of information.
In addition to this, presumptive tuberculosis adult cases from more than five family size had twice likely to be exposed to S. pneumoniae than those having less than five family size. This study result agreed with the study report from Wolaita-Sodo, Ethiopia.33 The possible reason for more likely to be exposed to S. pneumoniae infection is that high family size may increase the chance of the transmission of the S. pneumoniae among the family members.
Limitation of the Study
As the patient him/herself collects the sputum, it was difficult to avoid contamination. Since participants may forget some information asked, there might be a recall bias.
Conclusions
Multi-drug resistance of Streptococcus pneumoniae infection in presumptive tuberculosis adult cases was prevalent. Therefore, culture and susceptibility test is vital for appropriate management of Streptococcus pneumoniae infection of the lower respiratory tract in the study area.
Abbreviations
LRTI, Lower respiratory tract infection; MDR-TB, Multi-Drug Resistant Tuberculosis; OPD, Outpatient department; SPSS, Statistical Package for Social Science; TB, Tuberculosis; WHO, World Health Organization.
Data Sharing Statement
The data that support the findings of this study will be available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Before initiation of the study, ethical clearance was obtained from the Institution Review Board Hawassa University College of Medicine and Health Sciences (Ref. No IRB/126/13). Participants were recruited after informed written consent was obtained. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The authors would like to thank Hawassa University College of Medicine and Health Sciences and School of Medical Laboratory Science and Dilla University Referral Hospital for the material and reagent supply that made the study possible. We acknowledge all data collectors for their cooperation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that there are no competing interests.
References
1. Agwu E, Ohihion A, Agba M, et al. Incidence of Streptococcus pneumoniae infections among patients attending tuberculosis clinics in Ekpoma, Nigeria; 2006.
2. Wei M, Zhao Y, Qian Z, et al. Pneumonia caused by Mycobacterium tuberculosis. Microbes Infect. 2020;22(6–7):278–284. doi:10.1016/j.micinf.2020.05.020
3. Zhang Z, Sng L, Yong Y, et al. Delays in diagnosis and treatment of pulmonary tuberculosis in AFB smear-negative patients with pneumonia. Int J Tuberc Lung Dis. 2017;21(5):544–549. doi:10.5588/ijtld.16.0667
4. Lim TK, Siow WT. Pneumonia in the tropics. Respirology. 2018;23(1):28–35. doi:10.1111/resp.13137
5. Aston SJ. Pneumonia in the developing world: characteristic features and approach to management. Respirology. 2017;22(7):1276–1287. doi:10.1111/resp.13112
6. Marangu D, Zar HJ. Childhood pneumonia in low-and-middle-income countries: an update. Paediatr Respir Rev. 2019;32:3–9. doi:10.1016/j.prrv.2019.06.001
7. Lee H-M, Park I-H, Shin J-M, et al. XXIV world allergy congress 2015.
8. Daka D, Loha E, Giday A. Streptococcus pneumonia and antimicrobial resistance, Hawassa referral hospital, South Ethiopia. J Med Lab Diagn. 2011;2(3):27–30.
9. Nurahmed N, Kedir S, Fantahun S, et al. Bacterial profile and antimicrobial susceptibility patterns of lower respiratory tract infection among patients attending selected health centers of Addis Ababa, Ethiopia. Egypt J Chest Dis Tuberc. 2020;69(2):399.
10. World Health Organization. Global Tuberculosis Report. Geneva: World Health Organization; 2021.
11. Zhang Z, Chen M, Ying Y, Pan S, Liu Y. Antimicrobial susceptibility among Streptococcus pneumoniae and Haemophilus influenzae collected globally between 2015 and 2017 as part of the Tigecycline Evaluation and Surveillance Trial (TEST). Dovepress Infect Drug Resist. 2019;2019(12):1209–1220. doi:10.2147/IDR.S203121
12. Sharew B, Moges F, Yismaw G, et al. Antimicrobial resistance profile and multidrug resistance patterns of Streptococcus pneumoniae isolates from patients suspected of pneumococcal infections in Ethiopia. Ann Clin Microbiol Antimicrob. 2021;20(1):1–7. doi:10.1186/s12941-021-00432-z
13. Karami M, Hosseini SM, Hashemi SH, et al. Prevalence of nasopharyngeal carriage of Streptococcus pneumoniae in children 7 to 14 years in 2016: a survey before pneumococcal conjugate vaccine introduction in Iran. Hum Vaccin Immunother. 2015;15(9):2178–2182. doi:10.1080/21645515.2018.1539601
14. World Health Organization. Fact Sheet on Pneumonia Provides Key Facts and Information on Streptococcus pneumoniae. World Health Organization; 2019.
15. Were DW, Qazi DS. The Context and Key Problems of Pneumonia Diagnosis in Low Resource Settings. World Health Organization; 2014.
16. Gebru T, Taha M, Kassahun W. Risk factors of diarrhoeal disease in under-five children among health extension model and non-model families in Sheko district rural community, Southwest Ethiopia: comparative cross-sectional study. BMC Public Health. 2014;14(1):395. doi:10.1186/1471-2458-14-395
17. Alamneh YM, Adane F. Magnitude and Predictors of Pneumonia among Under-Five Children in Ethiopia: A Systematic Review and Meta-Analysis. Journal of Environmental and Public Health. 2020;2020:1606783.
18. Arora AA, Krishnaswamy UM, Moideen RP, Padmaja MS. Tubercular and bacterial coinfection: a case series. Lung India. 2015;32(2):172–174. doi:10.4103/0970-2113.152645
19. Krishna S, Jabeen H, Jeer M. Correlation of sputum gram stain and sputum culture for respiratory tract infections in a tertiary care hospital, Ballari, India. Int J Curr Microbiol App Sci. 2017;6:3008–3012. doi:10.20546/ijcmas.2017.606.357
20. Cheesbrough M. District Laboratory Practical in Tropical Countries. New York: Cambridge University press Cambridge; 2006.
21. Bauer AW, Kirby WMM, Sherris JC, Turck M. Antibiotic susceptibility testing by a standardized single disk method. Am J Clin Pathol. 1966;45(4_ts):493–496. doi:10.1093/ajcp/45.4_ts.493
22. CLSI. Performance Standards for Antimicrobial Susceptibility Testing.
23. Mahato S, Sah H, Yadav S. Isolation of Streptococcus pneumoniae from the sputum samples and their antimicrobial resistance in Biratnagar. Nepal J Microbiol Exp. 2019;7(6):
24. Jeannet CB, Sara JB, Geoffrey CM, et al. Antimicrobial susceptibility of Streptococcus pneumoniae in adult patients with pneumococcal pneumonia in an urban hospital in Mozambique. BMC Res Notes. 2014;7(2):110. doi:10.1186/1756-0500-7-110
25. Samson E, Ajike A, Cletus U, Abiodun O. Prevalence of Streptococcus pneumoniae and Mycobacterium tuberculosis co-infection among HIV infected adult patients on HAART in Ogun State, Nigeria. Int J Virol AIDS. 2019;6:46.
26. Iliyasu Z, Babashani M. Prevalence and predictors of TB co-infection among HIV seropositive patients attending Aminu Kano teaching hospital, northern Nigeria. J Epidemiol. 2009;19:81–87. doi:10.2188/jea.JE20080026
27. Lema K, Murugan R, Tachbele E. Prevalence and associated factors of pneumonia among under-five children at public hospitals in Jimma zone, South West of Ethiopia, 2018. J Pulmonol Clin Res. 2018;2(1):25–31.
28. Gebre AB, Begashaw TA, Ormago MD. Bacterial profile and drug susceptibility among adult patients with community acquired lower respiratory tract infection at tertiary hospital, Southern Ethiopia. BMC Infect Dis. 2021;21(1):1–10. doi:10.1186/s12879-021-06151-2
29. Abaye G, Fekadu H, Haji K, Alemu D, Anjulo AA, Yadate DT. Prevalence and risk factors of pneumococcal nasopharyngeal carriage in healthy children attending kindergarten, in district of Arsi Zone, South East, Ethiopia. BMC Res Notes. 2019;12(1):1–6. doi:10.1186/s13104-019-4283-3
30. Anagaw B, Gezachew M, Biadgelgene F, et al. Antimicrobial susceptibility patterns of Streptococcus pneumoniae over 6 years at Gondar University Hospital, Northwest Ethiopia. Asian Pac J Trop Biomed. 2013;3(7):536–541. doi:10.1016/S2221-1691(13)60109-4
31. Haile AA, Gidebo DD, Ali MM. Colonization rate of Streptococcus pneumoniae, its associated factors and antimicrobial susceptibility pattern among children attending kindergarten school in Hawassa, southern Ethiopia. BMC Res Notes. 2019;12(1):1–7. doi:10.1186/s13104-019-4376-z
32. Adhanom G, Gebreegziabiher D, Weldu Y, et al. Species, risk factors, and antimicrobial susceptibility profiles of bacterial isolates from HIV-infected patients suspected to have pneumonia in Mekelle Zone, Tigray, Northern Ethiopia. Biomed Res Int. 2019;2019(2019):1–9. doi:10.1155/2019/8768439
33. Admasie A, Kumie A, Worku A. Children under five from houses of unclean fuel sources and poorly ventilated houses have higher odds of suffering from acute respiratory infection in Wolaita-Sodo, Southern Ethiopia: a case-control study. J Environ Public Health. 2018;2018:9320603. doi:10.1155/2018/9320603
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.