")
Back to Journals » Infection and Drug Resistance » Volume 14
Prevalence and Genetic Diversity of Clostridium perfringens Isolates in Hospitalized Diarrheal Patients from Central China
Authors Wang B, Dong W, Ma L, Dong Y , Wang S, Yuan Y, Ma Q, Xu J, Yan W , Nan J, Zhang Q , Xu W, Ma B, Chu Y, Zhang J, Li L, Li Y
Received 14 September 2021
Accepted for publication 30 October 2021
Published 15 November 2021 Volume 2021:14 Pages 4783—4793
DOI https://doi.org/10.2147/IDR.S338593
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Baoya Wang,1 Wenjuan Dong,2 Liyan Ma,3 Yonghui Dong,4 Shanmei Wang,1 Youhua Yuan,1 Qiong Ma,1 Junhong Xu,1 Wenjuan Yan,1 Jing Nan,1 Qi Zhang,1 Wenbo Xu,1 Bing Ma,1 Yafei Chu,1 Jiangfeng Zhang,1 Li Li,1 Yi Li1
1Department of Clinical Microbiology, Henan Provincial People’s Hospital, People’s Hospital of Zhengzhou University, and People’s Hospital of Henan University, Zhengzhou, 450003, Henan, People’s Republic of China; 2Department of Clinical Microbiology, Xicheng District Pingan Hospital, Beijing, 100035, People’s Republic of China; 3Department of Clinical Microbiology, Beijing Friendship Hospital, Capital Medical University, Beijing, 100050, People’s Republic of China; 4Department of Osteology, Henan Provincial People’s Hospital, People’s Hospital of Zhengzhou University, and People’s Hospital of Henan University, Zhengzhou, 450003, Henan, People’s Republic of China
Correspondence: Yi Li; Li Li
Department of Clinical Microbiology, Henan Provincial People’s Hospital, People’s Hospital of Zhengzhou University, and People’s Hospital of Henan University, Weiwu Road 5, Zhengzhou, 450003, Henan, People’s Republic of China
Tel +8637165580484
Fax +8637187160318
Email [email protected]; [email protected]
Objective: This study aimed to investigate the prevalence, genetic diversity and clinical characteristics of Clostridium perfringens isolates from hospitalized clinical diarrheal patients.
Methods: A prospective study was conducted on 1108 patients with diarrhea during hospitalization. Stool samples were cultured for C. perfringens, and the toxin genes were detected by PCR. The available clinical data of 112 patients were analyzed to study the clinical features of various isolates. Multi-locus sequence typing (MLST) was performed to assess phylogenetic relationship between different isolates.
Results: A total of 153 (13.8%) isolates were obtained from patients’ stools. C. perfringens type F (49.0%) was the major toxin type in the isolates, followed by type A (n = 59, 38.6%) and type C (n = 14, 9.2%). Patients older than 50 years and those with underlying diseases of cancer, hepatobiliary system, and ulcerative colitis (UC) were more predisposed to C. perfringens type F and type A infection than to type C. The patients infected with type C experienced more severe clinical symptoms compared to those with type A infection. There was a significant association between type FC and foodborne gastrointestinal (GI) diseases (p = 0.018), between type FP and antibiotic-associated diarrhea (AAD) (p < 0.001), and between type A and sporadic diarrhea (SD) (p < 0.001). Phylogenetic analysis indicated that type F isolates carrying a chromosomal cpe gene mainly belonged to ST77 (6/15 isolates). Type F isolates with cpe gene on a plasmid exhibited high genetic diversity.
Conclusion: High prevalence and considerable genetic diversity of C. perfringens type F were found in clinical diarrheal patients. Elderly people and patients with cancer, hepatobiliary diseases or UC, or suspected of having food poisoning (FP) may be targeted for routine testing of C. perfringens toxin genes and may benefit from early detection of C. perfringens type C isolates that cause more severe clinical symptoms.
Keywords: Clostridium perfringens, toxin type, clinical characteristics, prevalence, MLST
Introduction
Clostridium perfringens (C. perfringens) is an important pathogen, causing human gastrointestinal (GI) diseases, particularly in the hospital environment. Recently, subtypes of C. perfringens have been classified into seven toxin types (A through G) based on their ability to produce the major lethal toxins, alpha, beta, epsilon, iota, enterotoxin (CPE) and NetB.1 CPE encoded by cpe gene, is a 35-kDa polypeptide that binds to claudin receptors on enterocytes to form pores, disrupting the intercellular claudin tight junctions and causing intestinal disease symptoms.2 CPE-positive C. perfringens subtypes are responsible for causing food poisoning (FP) and non-foodborne gastrointestinal (GI) diseases such as AAD and SD.3–5 Type F represents the formerly called CPE-positive isolates of C. perfringens type A and produces CPA and CPE toxins. Recently, Azimirad et al reported that 13.3% of patients with AAD carried type F isolates, demonstrating the importance of type F in the development of AAD.4 Additionally, type F was reported as an essential infection source for asymptomatic carriers and foodborne diseases.6 Clostridium perfringens type C and type D also express CPE,1 and type C can cause enteric diseases characterized by vomiting, diarrhea, and abdominal cramps. Type C can also cause fatal intestinal necrosis in humans and other animals.7,8 Apart from CPE, beta2 toxin encoded by the cpb2 gene has been associated with enteric disease in humans and necrotic enteritis in chickens and many other animal species.7,9,10 A recent study suggested that beta2 toxin was significantly associated with children suffering from autism spectrum disorders (ASD).11
Multi-locus sequence typing (MLST) is a commonly used technique for the typing of human, animal and foodborne pathogens. An MLST scheme for C. perfringens was developed by Xiao et al, comparing nucleic acid sequences of eight housekeeping genes of C. perfringens isolates and analyzing phylogenetic relationship between different species.12 Two studies have shown that different toxin types of C. perfringens exhibited distinct genetic characteristics.6,13
C. perfringens is well known in many countries as the causative agent of several forms of enteric disease;4,14–16 however, the prevalence of enterotoxigenic C. perfringens isolates has not been systematically studied in hospitals in China. This study aimed to determine the prevalence, clinical characteristics, and molecular epidemiology of C. perfringens in hospitalized patients suffering from gastroenteritis, including foodborne GI diseases, AAD and SD, in the central region of China.
Materials and Methods
Sample and Clinical Data Collection
Fecal samples were collected from 1108 patients suffering from diarrhea and admitted to Henan Provincial People’s Hospital, Zhengzhou, China between Oct 2018 and Oct 2019. The samples were tested for C. difficile and C. perfringens. C. difficile toxin genes (tcdB, cdt, and tcdc deletion at nucleotide 117) from fecal samples were detected by GeneXpert C. difficile PCR assay (Cepheid Inc., USA). The available medical records of 112 patients with fecal samples positive for C. perfringens, were reviewed for age, gender, clinical profile, underlying disease, procedures performed and results of laboratory tests.
Culture and Identification of C. perfringens Isolates
The freshly collected stool specimens were delivered within 2 h of collection to a clinical microbiology laboratory to test for the presence of C. perfringens. After shock treatment with 95% alcohol, stool specimens were cultured anaerobically on 5% sheep blood agar plates at 37°C for 24 h. The colonies suspected to be belonging to C. perfringens were identified by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF-MS) (Bruker Daltonics GmabH, Billerica, MA, USA). Isolates were maintained in cooked-meat medium with glycerol (30%) at −80°C for further studies.
PCR Amplification of Toxin Genes
Bacterial genomic DNA was extracted from the colonies growing on 5% sheep agar plates using a Bacterial Genomic DNA Extraction Kit (Cat. No. 9763, Takara, Japan). Plasmid DNA was purified from the pure bacterial cultures using E.Z.N.A. Plasmid Mini Kit I (Cat. No. D6942, Omega, USA). The genomic and plasmid DNA were stored at −20°C till used for PCR experiments.
The toxin genes cpa, cpb, cpb2, etx, iap, cpe and netB were amplified by PCR using specific primer pairs1,17 (Table 1). DNA amplification by PCR was carried out in a reaction volume of 25 μL with 3 μL of template DNA (200 ng/μL), 1.5 μL each of 10 pmol/μL forward and reverse primers, 6.5 μL of water, and 12.5 μL of 2× Multiplex PCR Mix. The PCR was performed using a Bio-Rad T100 system (USA) using the following program: Initial denaturation step of 5 min duration at 95°C, followed by 35 cycles of 30 s at 94°C, 1 min at 50 °C, and 1 min at 72°C. The final extension was performed for 10 min at 72°C. The PCR products (4 μL) were visualized by electrophoresis on a 2% agarose gel with a 2000-bp ladder (DL2000, Takara, Japan) as the molecular size marker. The type B isolate C. perfringens ATCC 3626 was used as a positive control for cpa, cpb and etx genes. Isolates SM101 and ATCC 13124 were used as positive and negative controls, respectively, for cpe gene.
 |
Table 1 Primers Used for PCR Amplifications in This Study |
MLST Analysis
MLST typing was performed as described previously.12 In brief, eight loci (colA, groEL, sodA, plc, gyrB, sigK, pgk and nadA) were amplified by PCR and the PCR products were sequenced by using a 3730 XL DNA Analyzer (Applied Biosystems, USA). DNA sequences were submitted to a public C. perfringens MLST database (https://pubmlst.org/organisms/clostridium-perfringens) to obtain the sequences type (ST). New alleles and STs were deposited in the C. perfringens MLST database. The phylogenetic trees were constructed from the concatenated sequences by the maximum likelihood method, using a Tamura-Nei model in MEGA version 7.0 software.18
Statistical Analysis
Data were excluded from analyses if complete data sets were not obtained for a particular case. Statistical analyses were performed by IBM SPSS Software Version 20.0 (IBM, Armonk, NY). Clinical data were analyzed by the chi-square or Fisher’s exact test. A p-value of less than 0.05 was considered as statistically significant. Categorical variables were reported as frequencies and percentages, normally distributed continuous variables were reported as means and standard deviations (SDs) and non-normally distributed continuous variables as medians and interquartile ranges (IQRs).
Results
Prevalence of Toxin Genes and Toxin Types
A total of 153 C. perfringens isolates were collected from 1108 diarrheal stool samples. C. difficile pathogens were also detected in six specimens (3.9%) positive for C. perfringens. A total of 132 toxigenic C. difficile isolates were detected out of all stool samples by the GeneXpert C. difficile PCR assay. The cpa gene was detected in all isolates, cpe in 55.6% (85/153), cpb in 9.2% (14/153), and cpb2 in 3.3% (5/153) of the positive samples. The genes etx, iap, or netB were not detected in any of the isolates. C. perfringens type F (positive for cpa and cpe genes) was the main toxin type, accounting for 49.5% (75/153) of all isolates, followed by type A (cpa-positive), which was found in 38.6% (59/153) of the isolates. The type C isolates were grouped into two subtypes, type C-1 and type C-2, based on their toxin genes. Ten isolates carrying cpa, cpb and cpe genes were assigned to type C-1, and four isolates carrying cpa and cpb genes were assigned to type C-2. In addition, two isolates (positive for cpa and cpb2 genes) belonged to type H1, and three isolates (positive for cpa, cpe and cpb2 genes) were classified as type H213 (Table 2).
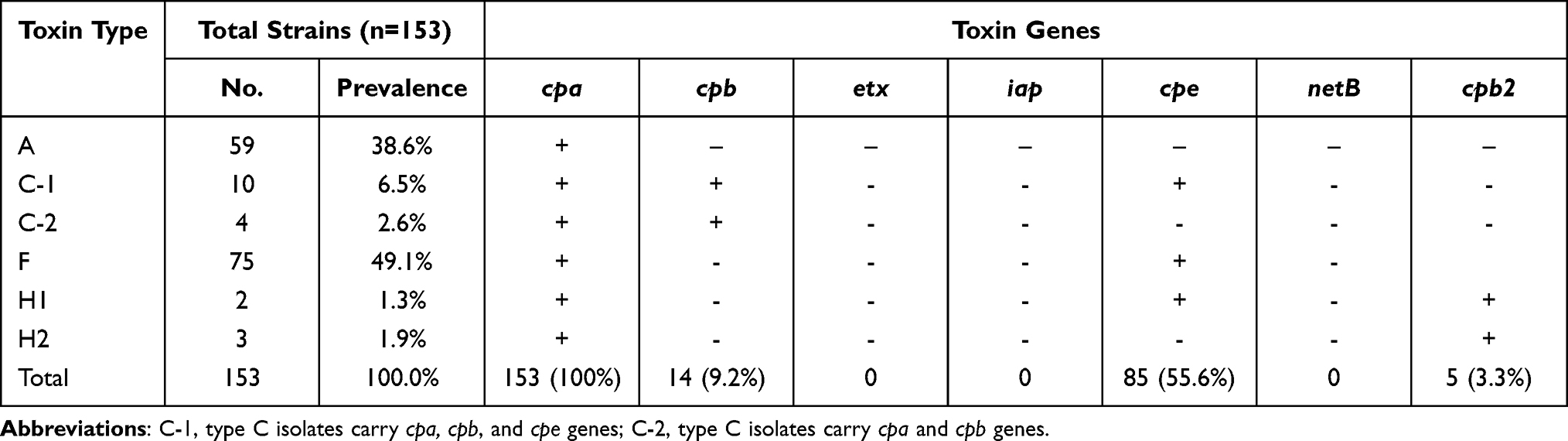 |
Table 2 Prevalence of C. Perfringens Isolates and Toxin Gene Profiles |
Association of Toxin Types of C. perfringens with GI Diseases
The 153 patients positive for C. perfringens infection suffered from three types of gastroenteritis (GI) diseases: foodborne GI diseases, AAD and SD. The food borne GI diseases were caused by type F (12/18), type C (3/18), type A (2/18) and type H2 (1/18) isolates. The 12 type F isolates could be further divided into five Fc (cpe gene on chromosome) and seven Fp (cpe gene on plasmid) types. AAD was mainly caused by type FP isolates (30/48 cases), but a small number of patients were also found to be infected with type FC (5/48), type C (5/48), type A (7/48) and type H2 (1/48). SD was caused mainly by types A (50/87), and Fp (23/87); however, a small number of patients were also found to be infected with type Fc (5/87), type C (6/87) and type H1 (3/87). Type FP was found at higher frequency in AAD, compared to foodborne GI diseases and SD (62.5% versus 38.9% and 26.4%, p < 0.001), and type A was more prevalent in SD, compared to food borne GI diseases and AAD (57.5% versus 11.1% and 14.6%, p < 0.001). Type FC had a higher rate in foodborne GI diseases, compared to AAD and SD (27.8% versus 10.4% and 5.7%, p < 0.001), There was no significant association between other types (type C, type H1 and type H2) and the three GI diseases (p > 0.05) (Table 3).
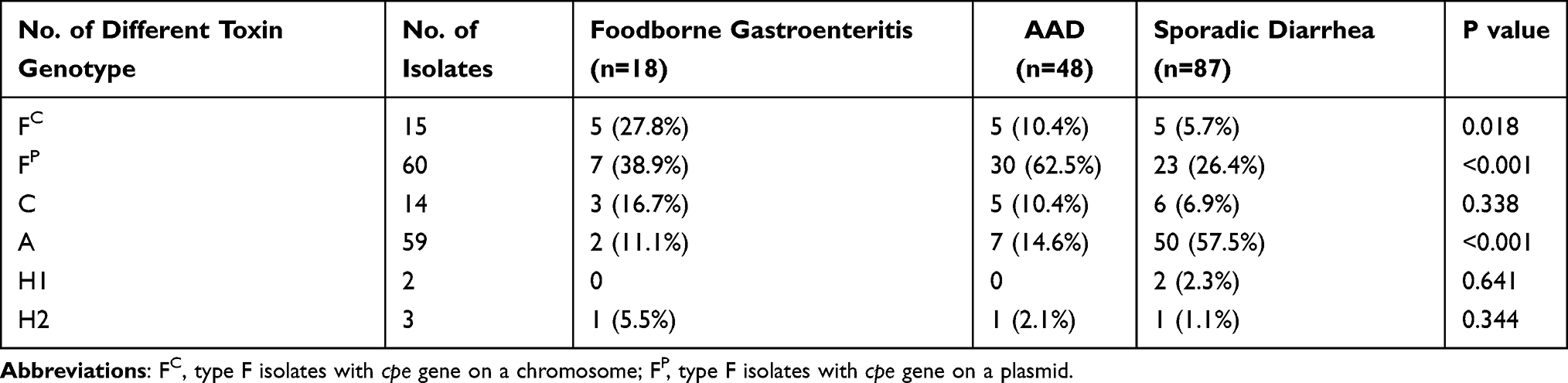 |
Table 3 Disease Caused by Different Toxin Types of C. Perfringens Isolates |
Clinical Features of Toxin Types of Infected C. perfringens Patients
The data for age, gender, length of hospitalization, underlying diseases and results of laboratory investigations were obtained from the available medical records of 112 patients. C. perfringens infection was more common in the elderly patients and the patients older than 50 years were mainly infected with C. perfringens type F (39/60, 65.0%), type C (7/11, 63.6%) and type A (30/41, 73.2%). The age range of patients infected with type F (1–83 years) and type A (8–90 years) was broader as compared to that of type C (20–79 years). The ratio of male to female patients and the average period of hospitalization in type F, type C and type A infected patients were not different. Type F patients mainly suffered from malignancy (19/60, 31.7%), hepatobiliary disease (13/60, 21.7%) and ulcerative colitis (UC) (11/60, 18.3%). The main underlying diseases in type A patients were malignancy (16/41, 38.1%), hepatobiliary disease (10/41, 23.8%), cerebral infarction (7/41, 16.7%) and cardiovascular diseases (7/41, 16.7%). The numbers of type C patients were relatively small, the clinical course of type C patients was more severe. In type F and type C patients, C-reactive protein and Procalcitonin (ng/mL) were higher than type A patients (p < 0.05) (Table 4). Type C patients also had a higher incidence of fever (6/13, 54.5%), compared to type F (20/20, 30%) and type A 7/41, 16.6%) patients (p < 0.05). WBC count and fecal occult blood were similar in the three groups (Table 4). The mean length of hospitalization of patients suffering from foodborne GI disease was shorter (5.7± 2.3 days) than for those with AAD (34 ±15.6 days) or SD (11 ± 7.6 days) (p < 0.01). Similarly, patients suffering from foodborne GI disease and AAD had more serious C. perfringens infection and required a much longer duration of antibiotic treatment compared to those with SD (data not shown).
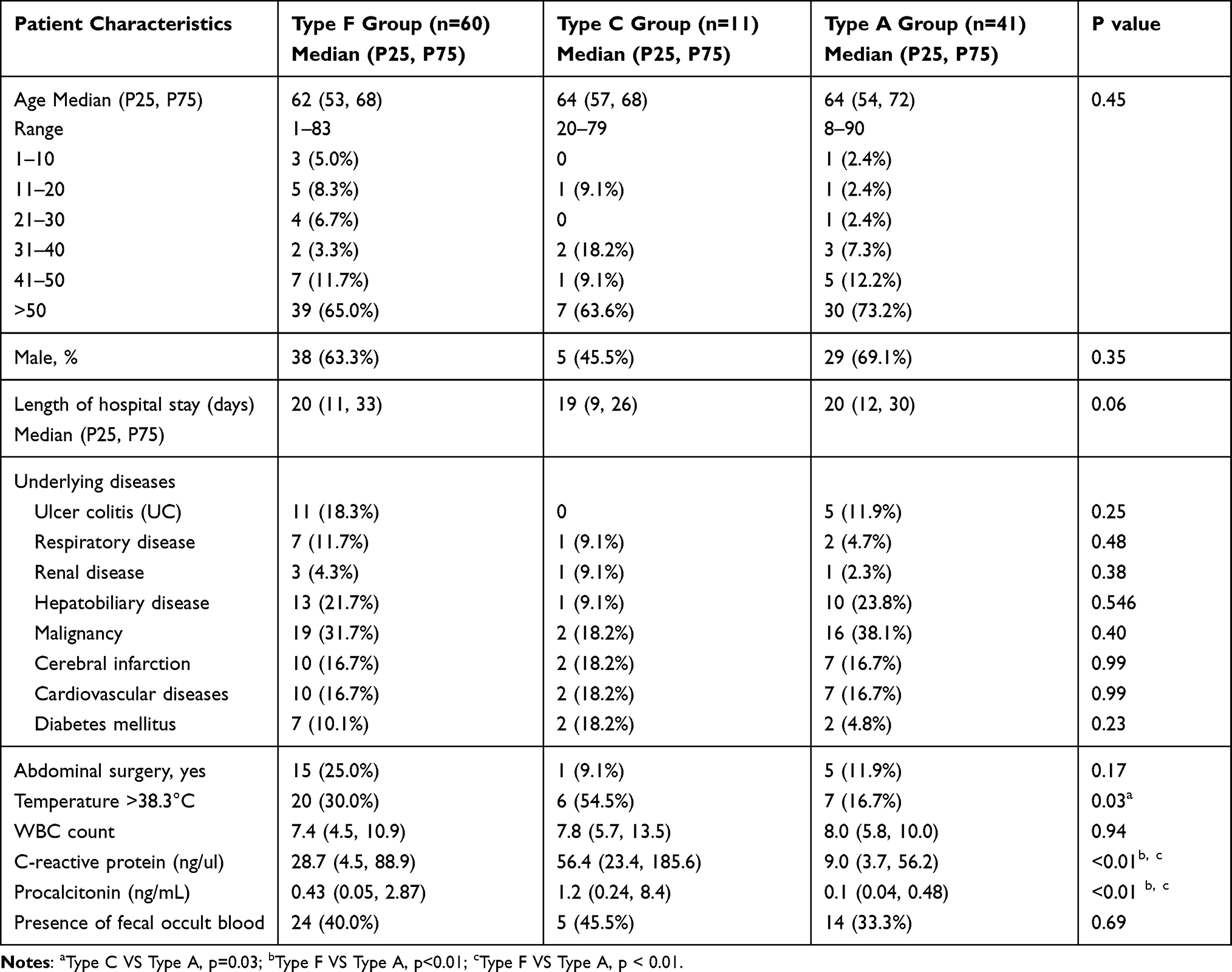 |
Table 4 Demographic and Clinical Characteristics in Different Toxin Types of C. Perfringens Groups |
Molecular Subtyping and Phylogenetic Analysis
Genotyping analysis by MLST revealed that out of 153 C. perfringens isolates, 143 exhibited a wide variety of sequence types (STs), including many new ST types. Ten isolates could not be characterized due to double peaks in the sequences of PCR products which could not be resolved despite repeated experiments. The sequences of new ST types, corresponding to new isolates of C. perfringens had been submitted to C. perfringens MLST database (Table S1). A total of 83 isolates were chosen and analyzed genetically (Table 5), which included all type F and type C isolates, and 2 type A isolates (cpb2-positive isolates). The profiles of STs and toxin genes in the remaining type A isolates were shown in supplementary results (Table S2). MLST phylogenetic analysis indicated that type FC isolates predominantly belonged to ST77 (6/15 isolates), which is more closely related to ST382, and the remaining 8 isolates grouped into a separate cluster. Six ST77 isolates were cultured from different wards and at different times, therefore ruling out the origination from a single source ward. In contrast, most of type FP isolates exhibited considerable diversity, and only 5 out of 48 isolates belonged to ST41. Type FP isolates were genetically divergent from type FC isolates. Similarly, type C and type A carrying cpb2 gene isolates were assigned into different ST types respectively, and had high genetic diversity between ST types (Figure 1).
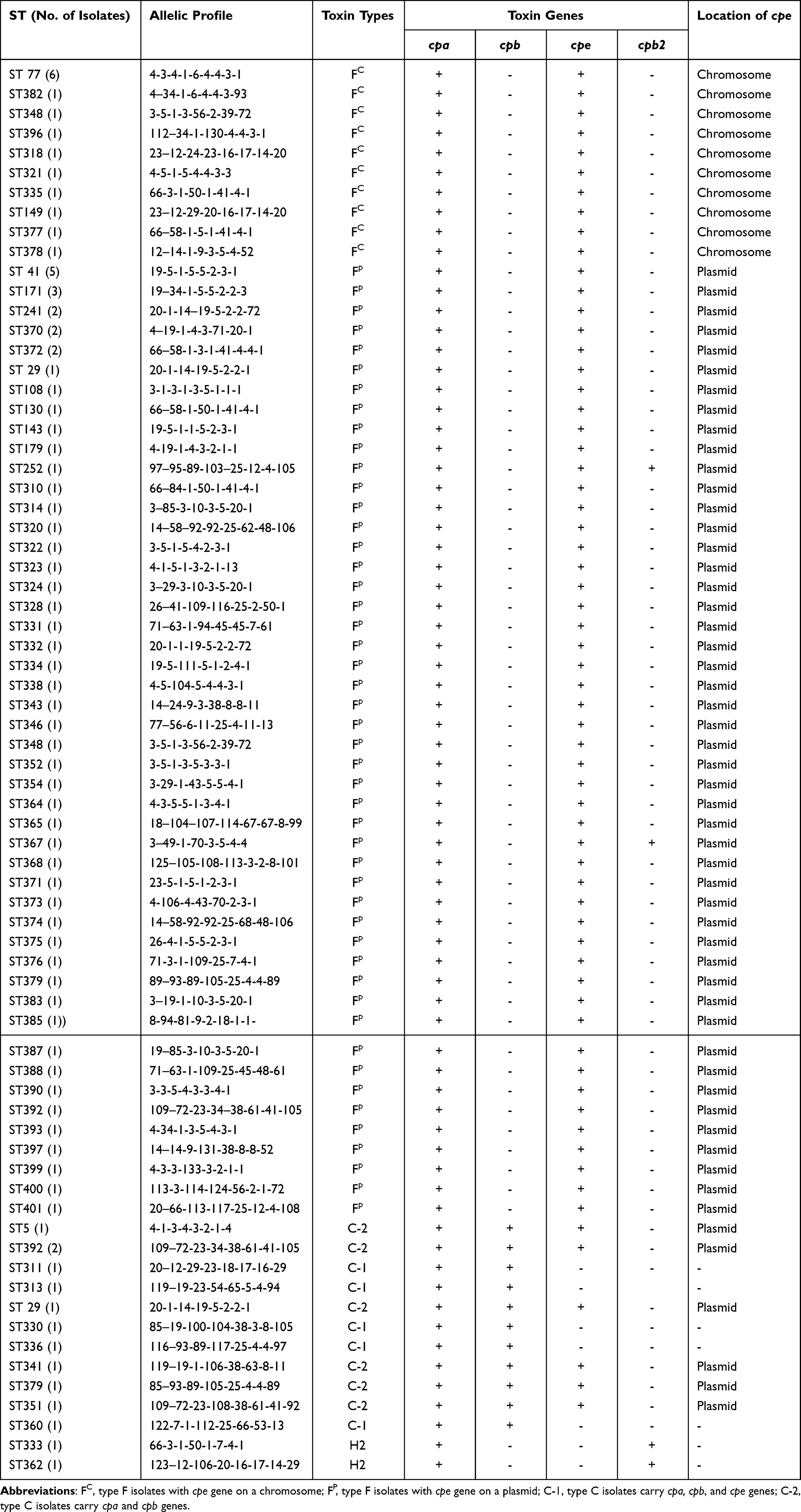 |
Table 5 Sequence Types (ST) and Toxin Gene Profiles of C. Perfringens Isolates |
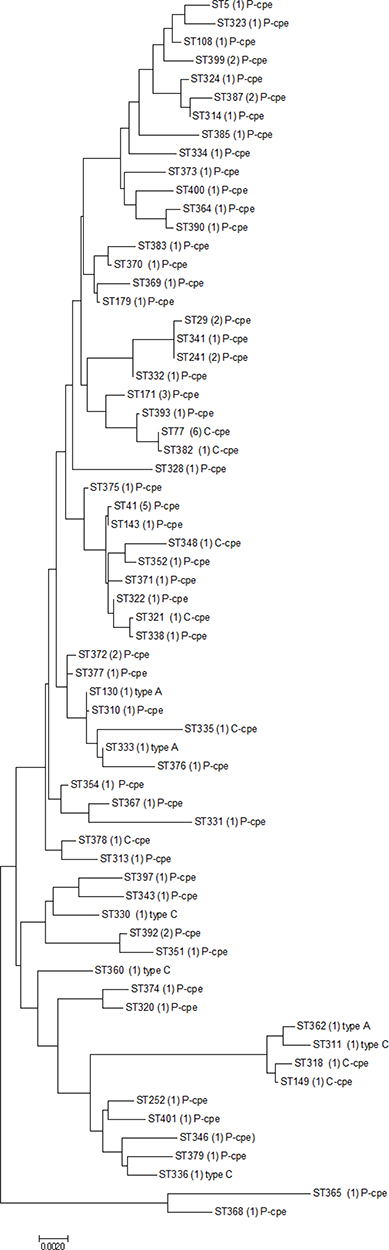 |
Figure 1 Phylogenetic analysis of several toxin types (Fc, Fp, C and A carrying cpb2 gene) of C. perfringens isolates created by the maximum likelihood method based on composite sequences of eight housekeeping gene fragments using MEGA 7.0 software. |
Discussion
To our knowledge, this is the first in-depth investigation of fecal carriage of C. perfringens in clinical diarrheal patients in central China. We have reported the clinical features associated with infection by various subtypes of C. perfringens and molecular characterization and genetic diversity of various isolates. In this study, we found a high prevalence of C. perfringens type FC infections in patients with foodborne GI diseases and C. perfringens type FP were mostly associated with non-foodborne GI diseases. This observation is similar to recent reported studies.4,19 Most C. perfringens type F isolates carrying cpe gene on the chromosome (FC) caused food poisoning, some of them also caused AAD and SD. Likewise, most type F isolates carrying cpe gene on a plasmid (FP) caused AAD, but a significant number of these isolates also caused food poisoning GI diseases and SD. Thus, C. perfringens type F isolates were a significant cause of AAD, food poisoning GI disease and SD diseases. Interestingly, we also observed that patients with AAD had longer hospital stays and duration of antibiotic treatments and more serious of C. perfringens infections. This finding supports a significantly pathogenic role of C. perfringens in AAD.
Beta toxin (encoded by cpb gene) is a pore-forming cytopathic toxin that can cause vascular necrosis, intestinal necrosis and systemic enterotoxaemia in humans and animals.7,20 A recent case report described how C. perfringens type C triggered a life-threatening acute hemorrhagic necrotizing enteritis (AHNE) with high mortality.21 In the present study, we found that in spite of the small number of C. perfringens type C isolates cultured from these patients, infection with these isolates was characterized by vomiting, abdominal cramps, bloody diarrhea and even necrosis of intestinal mucosa. Some C. perfringens type C isolates (C-1) carried three toxin genes (cpa, cpb. and cpe). The increased virulence of type C isolates might be due to the synergistic effect of several toxins such as beta toxin with CPE. In this study, the clinical features and laboratory findings confirmed that type C isolates caused more serious clinical symptoms than type A isolates.
Beta2 toxin encoded by plasmid-borne cpb2 gene was associated with food poisoning and AAD. Five isolates carrying cpb2 gene were detected in diarrheal patients in this study. In a similar study performed in Japan, cpb2 gene prevalence was only present at a low rate.13 However, the C. perfringens subtypes containing cpb2 gene have been found to play an important role in pre-term necrotizing enterocolitis (NEC).22,23 Additionally, cpb2 gene-positive C. perfringens isolates have also been found at higher rates in feces of autism spectrum disorder (ASD) children and infants aged <6 months.24–26 Another study demonstrated that beta 2 toxin contributed to necrotizing soft tissue infections in hospitalized patients.27 Further studies are required to investigate the pathogenic significance of beta 2 toxin produced by C. perfringens isolates in humans.
Patients older than 50 years-of-age were more likely to have C. perfringens infection. Similar results were reported in a study on C. perfringens infection in AAD patients from Iran.4 However, another study on C. perfringens infection in a community in England found an older average age for increased susceptibility.28 The possible reasons that patients older than 50-years were prone to C. perfringens infection include three different aspects: (1) the majority of these patients have more comorbid diseases and weakened immune system function which cause them to be more susceptible to C. perfringens infection; (2) the diversity of intestinal microbiota in these patients decreases and loss of colonization resistance may result in an increased risk for developing C. perfringens infection after the use of antimicrobial therapy;29 and (3) other therapeutic factors in these patients may impair colonization resistance, including surgery, cancer chemotherapy and invasive procedures that can lead to C. perfringens infection. The ratios of male to female and the length of hospital stay in the three groups of patients were similar to those reported in previous studies.4,30 Typically, C. perfringens food poisoning is a self-limiting disease lasting 12–24 h; mortality is uncommon.31 However, we found that patients in our study positive for C. perfringens food poisoning experienced diarrhea lasting for more than 24 h, and had to be given antibiotic therapy during hospitalization. The most common underlying diseases in patients infected with both C. perfringens type F and type A, in decreasing order of prevalence, were cancers, especially GI tumors requiring chemotherapy and radiation therapy, hepatobiliary diseases, cerebral infarction and cardiovascular diseases. This finding is in agreement with the results of a previous study.4 Interestingly, we observed that patients with diseases of the hepatobiliary system such as decompensated liver cirrhosis and cholecystitis, were at greater risk of developing C. perfringens type F and type A infections. The main reasons are perhaps an imbalance in the enteric microbiota, alterations of the intestinal barrier, probably due to portal hypertension, and reticuloendothelial system dysfunction in these patients.32,33 We found that a subset of patients infected with C. perfringens type F and A suffered from UC, confirmed by colonoscopy. These data are in disagreement with research by Aleksandra et al where the numbers of Crohn’s disease patients were higher than those of UC patients, but this may be attributed to the difference in the average age of the patients in these two studies.34 The average age of patients in our study was much higher than the average age of 11.7 years in their study. It is important to emphasize the impact of C. perfringens type A isolates on patients with decompensated liver cirrhosis and UC patients with dysfunctional intestinal epithelial barriers. C. perfringens type A isolates can easily penetrate the destroyed intestinal epithelial barriers, enter the vasculature and cause bacteremia.
Based on the MLST scheme previously reported by Xiao et al,12 we observed a considerable genetic diversity in the C. perfringens isolates. The phylogenetic analysis indicated that most C. perfringens type FC isolates belonged to a single distinct cluster that evolved independently from C. perfringens type Fp isolates. Moreover, C. perfringens type Fp isolates do not have a common genetic background, which supports the idea of horizontal transfer of cpe gene among C. perfringens type FP strains via conjugation (cpe-positive to cpe-negative transfer).35 These results are similar to earlier studies that demonstrated a wide genetic diversity of C. perfringens type FP isolates.12,13 Our findings indicate that MLST assays can be used as tools to investigate the reservoirs and transmission among cpe-positive clinical isolates of C. perfringens.
The limitations of this study should be considered. Because there was not enough volume of stool specimens, we were only able to identify the toxigenic types of C. perfringens isolates using multiplex PCR, which is one of the diagnostic methods for ascertaining C. perfringens infection.17,36 Indeed, several studies reported that C. perfringens infection was diagnosed by detection of CPE toxin using ELISA, reversed passive latex agglutination (RPLA) and enzyme immunoassay (EIA) tests.28,37,38 Further experiments should be performed to detect the CPE toxin in stool specimens of patients.
Conclusions
We believe that testing for the cpe gene or CPE toxin should be included in the routine diagnosis of vulnerable patients over 50 years of age, or in patients with underlying diseases such as cancer, liver cirrhosis or ulcerative colitis. In addition, for patients younger than 50 years, if they are suspected of having food poisoning due to contaminated food, we also suggest screening them for cpe gene or CPE toxin. Lastly, our data add to the evidence base that despite its relatively low prevalence, C. perfringens type C can cause severe clinical symptoms in patients. Further studies are needed to carefully evaluate the potential role of C. perfringens type A in the etiology of diseases that involve violation of the intestinal barrier such as UC and spontaneous bacterial peritonitis in liver cirrhosis.
Data Sharing Statement
The datasets generated for this study are available from the corresponding author Pro Yi Li on request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Zhengzhou University (20190211). Adult patients wrote the informed consent and a parent or legal guardian of patients under 18 years of age provided informed consent prior to the molecular analysis described below. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We are grateful to my colleagues Xuhua Zhou and Wenning Yang who assisted with collection and identification of C. perfringens isolates.
Funding
This work was supported by the National Natural Science Foundation of China (82004169) and Joint Program of Henan Province and Chinese Health Committee (LHGJ20200016).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Rood JI, Adams V, Lacey J, et al. Expansion of the Clostridium perfringens toxin-based typing scheme. Anaerobe. 2018;53:5–10. doi:10.1016/j.anaerobe.2018.04.011
2. Eichner M, Augustin C, Fromm A, et al. In colon epithelia, Clostridium perfringens enterotoxin causes focal leaks by targeting claudins which are apically accessible due to tight junction derangement. J Infect Dis. 2017;217(1):147–157. doi:10.1093/infdis/jix485
3. Ghoneim NH, Hamza DA. Epidemiological studies on Clostridium perfringens food poisoning in retail foods. Rev Sci Tech. 2017;36(3):1025–1032. doi:10.20506/rst.36.3.2734
4. Azimirad M, Gholami F, Yadegar A, et al. Prevalence and characterization of Clostridium perfringens toxinotypes among patients with antibiotic-associated diarrhea in Iran. Sci Rep. 2019;9(1):7792. doi:10.1038/s41598-019-44281-5
5. Shrestha A, Uzal FA, McClane BA. Enterotoxic Clostridia: clostridium perfringens enteric diseases. Microbiol Spectr. 2018;6(5):10. doi:10.1128/microbiolspec.GPP3-0003-2017
6. Yanagimoto K, Uematsu K, Yamagami T, et al. The Circulation of type F Clostridium perfringens among humans, sewage, and ruditapes philippinarum (Asari Clams). Pathogens. 2020;9(8):669. doi:10.3390/pathogens9080669
7. Mehdizadeh Gohari I, Navarro AM, Li J, et al. Pathogenicity and virulence of Clostridium perfringens. Virulence. 2021;12(1):723–753.
8. Posthaus H, Kittl S, Tarek B, et al. Clostridium perfringens type C necrotic enteritis in pigs: diagnosis, pathogenesis, and prevention. J Vet Diagn Invest. 2020;32(2):203–212. doi:10.1177/1040638719900180
9. Fohler S, Klein G, Hoedemaker M, et al. Diversity of Clostridium perfringens toxin-genotypes from dairy farms. BMC Microbiol. 2016;16(1):199. doi:10.1186/s12866-016-0812-6
10. Derongs L, Druilhe C, Ziebal C, et al. Characterization of Clostridium perfringens isolates collected from three agricultural biogas plants over a one-year period. Int J Environ Res Public Health. 2020;17(15):5450. doi:10.3390/ijerph17155450
11. Al Radaideh AJ, Badran EF, Shehabi AA. Diversity of toxin genotypes and antimicrobial susceptibility of Clostridium perfringens isolates from feces of infants. Germs. 2019;9(1):28–34. doi:10.18683/germs.2019.1154
12. Xiao Y, Wagendorp A, Moezelaar R, et al. A wide variety of Clostridium perfringens type A food-borne isolates that carry a chromosomal cpe gene belong to one multilocus sequence typing cluster. Appl Environ Microbiol. 2012;78(19):7060–7068. doi:10.1128/AEM.01486-12
13. Matsuda A, Aung MS, Urushibara N, et al. Prevalence and genetic diversity of toxin genes in clinical isolates of clostridium perfringens: coexistence of alpha-toxin variant and binary enterotoxin genes (bec/cpile). Toxins. 2019;11(6):326. doi:10.3390/toxins11060326
14. Kim YJ, Kim SH, Ahn J, et al. Prevalence of Clostridium perfringens toxin in patients suspected of having antibiotic-associated diarrhea. Anaerobe. 2017;48:34–36. doi:10.1016/j.anaerobe.2017.06.015
15. Kiu R, Caim S, Painset A, et al. Phylogenomic analysis of gastroenteritis-associated Clostridium perfringens in England and Wales over a 7-year period indicates distribution of clonal toxigenic strains in multiple outbreaks and extensive involvement of enterotoxin-encoding (CPE) plasmids. Microb Genom. 2019;5(10):e000297.
16. Mahamat Abdelrahim A, Radomski N, Delannoy S, et al. Large-scale genomic analyses and toxinotyping of clostridium perfringens implicated in foodborne outbreaks in France. Front Microbiol. 2019;10:777. doi:10.3389/fmicb.2019.00777
17. Baums CG, Schotte U, Amtsberg G, et al. Diagnostic multiplex PCR for toxin genotyping of Clostridium perfringens isolates. Vet Microbiol. 2004;100(1–2):11–16. doi:10.1016/S0378-1135(03)00126-3
18. Kumar S, Stecher G, Tamura K. MEGA7: molecular evolutionary genetics analysis version 7.0 for bigger datasets. Mol Biol Evol. 2016;33(7):1870–1874. doi:10.1093/molbev/msw054
19. Kobayashi S, Wada A, Shibasaki S, et al. Spread of a large plasmid carrying the cpe gene and the tcp locus amongst Clostridium perfringens isolates from nosocomial outbreaks and sporadic cases of gastroenteritis in a geriatric hospital. Epidemiol Infect. 2009;137(1):108–113. doi:10.1017/S0950268808000794
20. Nagahama M, Ochi S, Oda M, et al. Recent insights into Clostridium perfringens beta-toxin. Toxins. 2015;7(2):396–406. doi:10.3390/toxins7020396
21. Zeng S, Hin T, Fong CJ, et al. Acute hemorrhagic necrotizing enteritis: a case report and review of the literature. Ann Palliat Med. 2021;10(5):5853–5861. doi:10.21037/apm-20-1131
22. Sim K, Shaw AG, Randell P, et al. Dysbiosis anticipating necrotizing enterocolitis in very premature infants. Clin Infect Dis. 2015;60(3):389–397. doi:10.1093/cid/ciu822
23. Gao X, Yang Q, Huang X, et al. Effects of Clostridium perfringens beta2 toxin on apoptosis, inflammation, and barrier function of intestinal porcine epithelial cells. Microb Pathog. 2020;147:104379. doi:10.1016/j.micpath.2020.104379
24. Góra B, Gofron Z, Grosiak M, et al. Toxin profile of fecal Clostridium perfringens strains isolated from children with autism spectrum disorders. Anaerobe. 2018;51:73–77. doi:10.1016/j.anaerobe.2018.03.005
25. Alshammari MK, AlKhulaifi MM, Al Farraj DA, et al. Incidence of Clostridium perfringens and its toxin genes in the gut of children with autism spectrum disorder. Anaerobe. 2020;61:102114. doi:10.1016/j.anaerobe.2019.102114
26. Shaw AG, Cornwell E, Sim K, et al. Dynamics of toxigenic Clostridium perfringens colonisation in a cohort of prematurely born neonatal infants. BMC Pediatr. 2020;20(1):75. doi:10.1186/s12887-020-1976-7
27. Salamon D, Ochońska D, Wojak I, et al. Evidence for infections by the same strain of beta 2-toxigenic clostridium perfringens type A acquired in one hospital ward. Pol J Microbiol. 2019;68(3):323–329. doi:10.33073/pjm-2019-035
28. Forward LJ, Tompkins DS, Brett MM. Detection of Clostridium difficile cytotoxin and Clostridium perfringens enterotoxin in cases of diarrhoea in the community. J Med Microbiol. 2003;52(Pt 9):753–757.
29. Pilmis B, Le Monnier A, Zahar JR. Gut microbiota, antibiotic therapy and antimicrobial resistance: a narrative review. Microorganisms. 2020;8(2):269. doi:10.3390/microorganisms8020269
30. Mpamugo O, Donovan T, Brett MM. Enterotoxigenic Clostridium perfringens as a cause of sporadic cases of diarrhoea. J Med Microbiol. 1995;43(6):442–445.
31. Bintsis T. Foodborne pathogens. AIMS Microbiol. 2017;3(3):529–563. doi:10.3934/microbiol.2017.3.529
32. Lee NY, Suk KT. The role of the gut microbiome in liver cirrhosis treatment. Int J Mol Sci. 2020;22(1):199. doi:10.3390/ijms22010199
33. Albuquerque A, Macedo G. Spontaneous bacterial empyema in a cirrhotic patient due to Clostridium perfringens: case report and review of the literature. Gastroenterol Hepatol. 2013;36(2):69–71. doi:10.1016/j.gastrohep.2012.04.007
34. Banaszkiewicz A, Kądzielska J, Gawrońska A, et al. Enterotoxigenic Clostridium perfringens infection and pediatric patients with inflammatory bowel disease. J Crohns Colitis. 2014;8(4):276–281. doi:10.1016/j.crohns.2013.08.018
35. Brynestad S, Sarker MR, McClane BA, et al. Enterotoxin plasmid from Clostridium perfringens is conjugative. Infect Immun. 2001;69(5):3483–3487. doi:10.1128/IAI.69.5.3483-3487.2001
36. Wu J, Zhang W, Xie B, et al. Detection and toxin typing of Clostridium perfringens in formalin-fixed, paraffin-embedded tissue samples by PCR. J Clin Microbiol. 2009;47(3):807–810. doi:10.1128/JCM.01324-08
37. Rajkovic A, Jovanovic J, Monteiro S, et al. Detection of toxins involved in foodborne diseases caused by Gram-positive bacteria. Compr Rev Food Sci Food Saf. 2020;19(4):1605–1657. doi:10.1111/1541-4337.12571
38. Ishioka T, Aihara Y, Carle Y, et al. Contrasting results from two commercial kits testing for the presence of clostridium perfringens enterotoxin in feces from norovirus-infected human patients. Clin Lab. 2020;66(5). doi:10.7754/Clin.Lab.2019.190801
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.