")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Prevalence and Factors Associated with Delayed Initiation of Antiretroviral Therapy Among People Living with HIV in Nekemte Referral Hospital, Western Ethiopia
Authors Bayisa L , Tadesse A , Reta MM, Gebeye E
Received 12 June 2020
Accepted for publication 28 August 2020
Published 24 September 2020 Volume 2020:12 Pages 457—465
DOI https://doi.org/10.2147/HIV.S267408
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Lami Bayisa,1 Abilo Tadesse,1 Mebratu Mitiku Reta,1 Ejigu Gebeye2
1Department of Internal Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Institute of Public Health, University of Gondar, Gondar, Ethiopia
Correspondence: Abilo Tadesse Email [email protected]
Background: Ethiopia has adopted the “Universal Test and Treat” strategy to its national policy in 2016 to put all people living with HIV/AIDS (PLHIV) on antiretroviral therapy (ART) regardless of their World Health Organization (WHO) clinical stage or CD4 cell count level. A significant percentage of PLHIV start therapy has been delayed despite the availability of ART, which results in poor treatment outcomes including HIV-related morbidity and mortality, and continued HIV transmission.
Methods: This cross-sectional study was conducted to determine the magnitude and associated factors of delayed ART initiation among PLHIV at ART Clinic, Nekemte Referral hospital, Western Ethiopia between January 1, 2020 and March 31, 2020 for the time period of January 1, 2016 to December 31, 2019. A consecutive sampling method was used to recruit 417 study subjects. The collected data were entered into Epi data version 3.1 and exported to STATA version 14 for statistical analysis. Logistic regression analysis was used to identify associated factors with delayed ART initiation among PLHIV. P-values< 0.05 were used to declare significant association.
Results: A total of 417 PLHIV were included in the study. The mean age of study subjects was 33.49 (SD± 9.81) years. The majority of participants attended formal education (77%) and were urban dwellers (82%). One-third (34%) of them initiated ART delayed, beyond 7 days of confirmed HIV diagnosis. Subjects with normal nutritional status (BMI=18.5– 24.9kg/m2) (AOR=3.12, 95% CI=1.29– 7.57; P=0.012), CD4 count ≥ 351cells/mm3 (AOR=2.89, 95% CI=1.27– 6.58; P=0.011), tuberculosis (TBC) co-infection (AOR=2.76, 95% CI=1.13– 6.70; P=0.025), use of traditional treatment (AOR=4.03, 95% CI=2.03– 8.00; P< 0.001) and did not know other ART user(s) (AOR=2.86, 95% CI=1.52– 5.37; P=0.001) were significantly associated with delayed ART initiation.
Conclusion: Early HIV testing mechanisms and timely linkage to HIV care by advocating “Test-and-Treat” should be strengthened.
Keywords: PLHIV, antiretroviral therapy, Western Ethiopia
Background
By the end of 2019, there were 37.9 million people living with HIV infections worldwide, two-thirds of them in sub-Saharan Africa. Two million people were newly infected with HIV and 770,000 people died of AIDS-related causes. Two-thirds of eligible individuals accessed antiretroviral therapy worldwide. In 2018, more than half a million people were estimated to be living with HIV/AIDS in Ethiopia. Two-thirds of eligible individuals were put on ART.1,2
In 2015, the joint United Nations Program on HIV/AIDS set the Fast-Track target to reduce new HIV infections and HIV-related deaths to fewer than 500,000 in 2020 and end the HIV epidemic worldwide by 2030. The Fast-Track targets include the 90-90-90 strategy: 90% of people living with HIV know their status, 90% who know their HIV status access ART, and 90% of people receiving ART have suppressed viral loads. Since then, the World Health Organization has declared the “Universal Test and Treat” by endorsing initiation of ART within 7 days of confirmed HIV diagnosis. Ethiopia initiated “Test and Treat” in 2016 and committed to reducing new adult HIV infections by 50% by 2020 and to ending AIDS as a public health threat by 2030. Despite ART benefit in “treat all” policy, challenges remain in PLHIV to ensure timely access to HIV care from resource poor settings.3–9
Challenges to HIV care in PLHIV include, but are not restricted to, individual-level, clinical, and health facility-related factors. Individual-level factors contributing to delayed ART initiation included low literacy status, poor economic status, and rural residence. Working functional status, TBC co-infection, and high baseline CD4 count were among a few clinical predictors of delayed ART initiation. As well, health facility type, distance from ART center, perceived confidentiality of HIV records, and perceived home-based care affected timing of ART initiation.14–28
This study is the first of its kind at national-level to determine the magnitude and associated factors of delayed ART initiation among PLHIV after WHO endorsed “Universal Test and Treat” strategy.
Methods
Study Design and Period
An institution-based cross-sectional study was conducted at ART Clinic, Nekemte Referral Hospital, Western Ethiopia between January 1, 2020 and March 31, 2020 for the time period of January 1, 2016 to December 31, 2019.
Study Setting
The hospital is located in Western Ethiopia, which is 321 km away from the capital, Addis Ababa. The hospital has more than 295 beds and gives services to a catchment population of three million people. The hospital provides integrated ART services and currently about 3500 PLHIV were on treatment and of them nearly 1500 PLHIV were tested and initiated ART after “Test and Treat” strategy was implemented. HIV testing strategies in the ART center were voluntary counseling and testing (VCT) and provider-initiated testing and counseling (PITC). The HIV treatment cascade in the ART center was adopted from the WHO model that outlines the steps of care that PLHIV go through from initial diagnosis to achieving viral suppression. The cascade embraces linking and retaining of PLHIV in HIV care after confirmed HIV diagnosis. Rapid ART will be initiated in those retained in HIV care. Achieving viral suppression is the goal of ART.
Study Subjects and Variables
The source population was PLHIV on ART who had follow-up at ART Clinic, Nekemte Referral hospital. The study population was PLHIV who had follow-up at ART Clinic, Nekemte Referral hospital, aged 18 years and above, and initiated ART between January 1, 2016 and December 31, 2019. Individuals whose date of HIV diagnosis and ART initiation were not recorded were excluded from the study.
Study Variables
Dependent variable: Delayed initiation of ART.
Independent variables: 1) Socio-demographic characteristics include age, sex, religion, level of education, marital status, occupation, income level, and residence; 2) Clinical characteristics include base line CD4 count, WHO clinical stage, functional status, nutritional status, TB/HIV co-infection, and HIV testing approach; 3) Behavioral factors include alcohol use, use of traditional treatment, and knew ART user(s).
Sample Size and Sampling Procedure
The sample size was determined using a single population proportion formula with the assumption of 95% confidence level, 5% margin of error, and taking 50% magnitude of delayed ART initiation. The consecutive sampling method was used to recruit 417 study subjects among those who initiated ART between January 1, 2016 and December 31, 2019.
Data Collection Instrument and Procedures
Data were collected through an investigator administered pre-designed questionnaire. The questionnaire was prepared in English and translated into local languages, Amharic and Afan Oromo, for data collection and then re-translated back to English with maintaining its consistency. The patients’ charts were retrieved by using the patients’ registration number from the database. Patients were interviewed to obtain socio-demographic data. Relevant medical history and laboratory parameters were obtained from patients’ HIV intake and follow-up care form. One supervisor (BSc Nurse) and two data collectors (Clinical Nurses) participated in the data collection process. Quality of data was ensured through training and supervising of data collectors.
Data Analysis
Data were entered into a computer using EPI data version 4.4.1 statistical program. Data were cleaned and exported to STATA windows version 14.0 for analysis. Patient characteristics were reported as counts (percentages) for categorical variables, and mean with standard deviation for continuous variables. Both bi-variable and multi-variable logistic regression analyses were used to identify associated factors with delayed ART initiation. Those variables with a P-value<0.2 in the bi-variable analysis were exported to multi-variable analysis to control the possible effect of confounders. Adjusted odds ratio (AOR) with 95% confidence interval (CI) and P-value<0.05 were used to select significantly associated variables with delayed ART initiation.
Ethical Considerations
Ethical clearance was obtained from the Institutional Review Board (IRB) of College of Medicine and Health Sciences, University of Gondar. A formal letter of permission was obtained from Nekemte Referral hospital administrative body. Study subjects were recruited only after informed written consent was obtained from them. All data obtained were treated confidentially.
Definition of Terms
Delayed ART initiation was defined as receiving ART at any time after 7 days of post-HIV diagnosis in those who have no opportunistic infections (OIs).5,7 For those diagnosed and found to have both HIV and OI(s) at the same time, delayed ART initiation was defined as ART initiation after 2 months following anti-TBC regimen started,5,10 ART initiation after 4 weeks following amphotericin B–based regimen or after 6 weeks following fluconazole based regimen started for Cryptococcal meningitis,5,11 or ART initiation after 2 weeks following Pneumocystis jirovecii pneumonia (PCP) treatment started.12
Functional status is defined by WHO, working as able to perform usual work inside or outside home; ambulatory as able to perform Activity of Daily Living (ADL) but not able to work; bedridden as not able to perform ADL.
Traditional healing refers to health practices, approaches, knowledge, and beliefs incorporating plant, animal, and mineral-based medicines, spiritual therapies, manual techniques, and exercises, applied singularly or in combination to treat, diagnose, and prevent illnesses or maintain well-being.13
Results
Socio-Demographic Characteristics of Study Participant
A total of 417 PLHIV were included in the study. The mean age of study subjects was 33.49 (SD±9.81) years. The majority of participants were females (55%), married (57%), and Christian by religion (54%). Most respondents attended formal education (77%) and were urban dwellers (82%) (Table- 1).
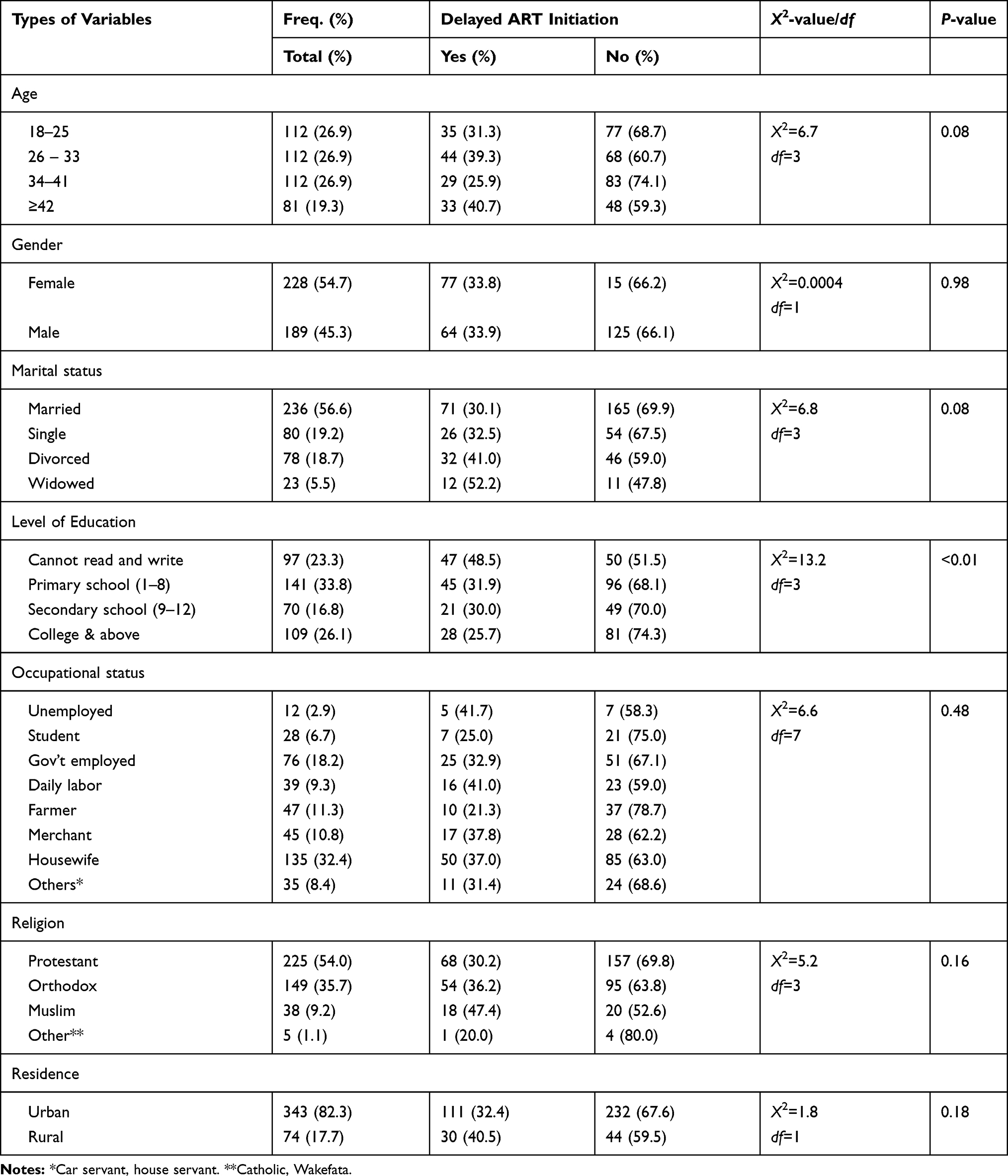 |
Table 1 Socio-Demographic Characteristics of PLHIV Attending ART Services at Nekemte Referral Hospital, Western Ethiopia, January 1–March 31, 2020 (n=417) |
Clinical Characteristics of Study Participants
Most study subjects had working functional status (83%). Two-thirds of participants (64%) had early stage HIV infection (clinical stage I and II). The mean CD4 count was 321 (SD±221) cells/mm3, and less than half (44%) had CD4 count >446 cells/mm3. Two-thirds (62%) had normal nutritional status (body mass index (BMI)=18.5–24.9 kg/m2) and were screened for HIV by PITC (58%). Ten percent of respondents were co-infected with TBC (Table-2).
 |
Table 2 Clinical Characteristics of PLHIV Attending ART Services at Nekemte Referral Hospital, Western Ethiopia, January 1–March 31, 2020 (n=417) |
Behavior-Related Characteristics
The majority (60%) of study subjects visited traditional healer(s) before they enrolled into HIV care. Less than half (42%) of participants knew other ART user(s). Two-thirds (59%) used alcohol as substance before knowing their HIV status.
Health Facility-Related Characteristics
Most study subjects (82%) came from the catchment area of the ART center. The majority (58%) of PLHIV were enrolled into HIV care via PITC.
Delayed Antiretroviral Therapy Initiation
Among a total of 417 study subjects who commenced ART, 34% of participants initiated ART delayed, beyond 7 days of confirmed HIV diagnosis. Among delayed initiators, 80% of them initiated 8 days to 8 weeks, the remaining 20% started after 8 weeks. Nearly half (46%) of TBC co-infected cases started ART delayed (after 2 months).
Factors Associated with Delayed Antiretroviral Therapy Initiation
Binary logistic regression was done to determine the association between each independent variable with delayed antiretroviral therapy initiation. On multivariable binary logistic regression analysis, subjects with normal nutritional status (BMI=18.5–24.9 kg/m2) (AOR=3.12, 95% CI=1.29– 7.57; P=0.012), CD4 count ≥351 cells/mm3 (AOR=2.89, 95% CI=1.27–6.58; P=0.011), TBC co-infection (AOR=2.76, 95% CI=1.13–6.70; P=0.025), use of traditional treatment (AOR=4.03, 95% CI=2.03–8.00; P<0.001), and did not know other ART user(s) (AOR=2.86, 95% CI=1.52–5.37; P=0.001) were significantly associated with delayed ART initiation. Delayed antiretroviral therapy initiation was 59% (AOR=0.41, 95% CI=0.18–0.91; P=0.03) lower among those who came from out of the catchment area of ART center (Table 3).
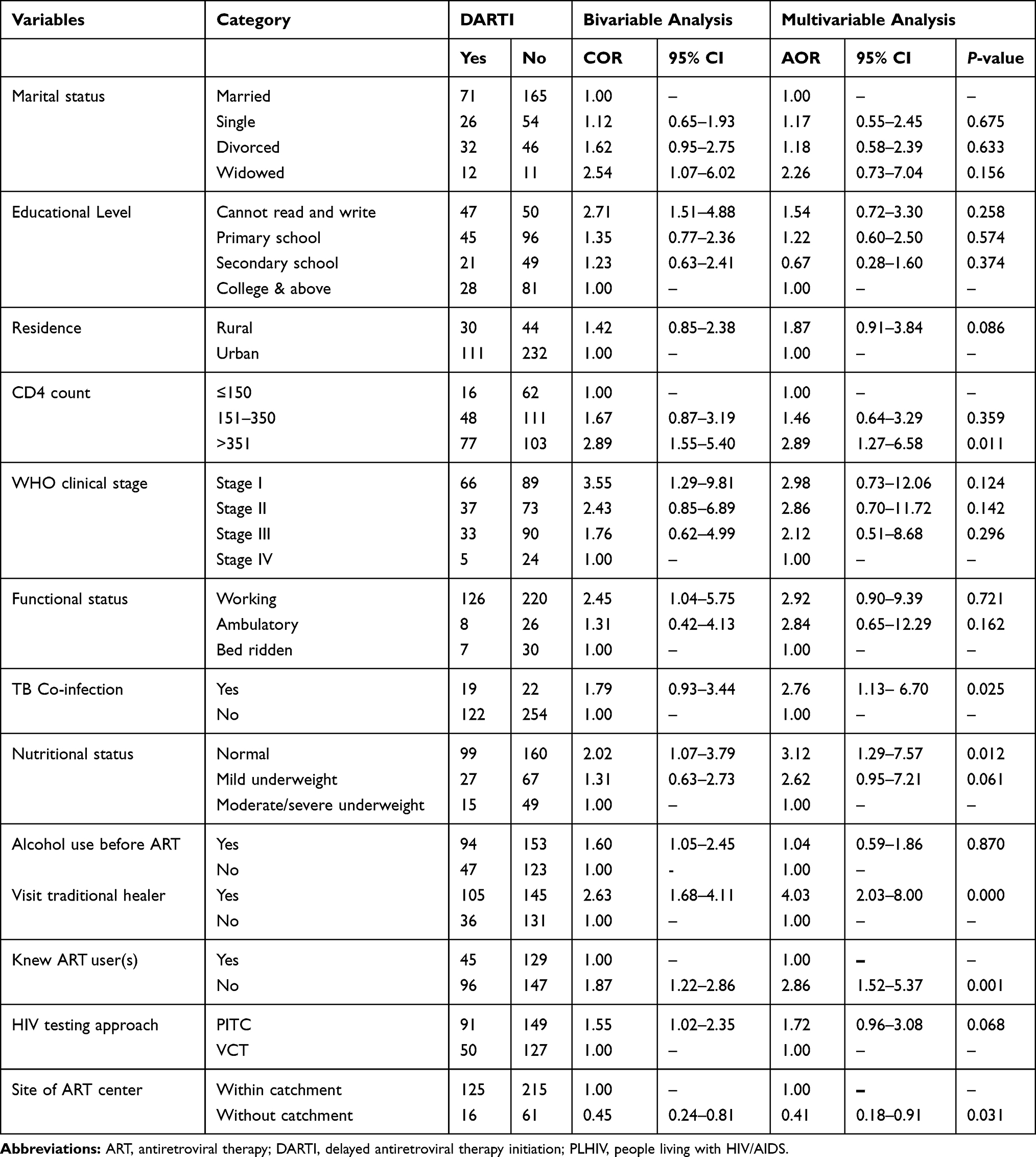 |
Table 3 Bivariable and Multivariable Analysis for Delayed Antiretroviral Therapy Initiation (DARTI) Among PLHIV on ART at Nekemte Referral Hospital, West Ethiopia, January 1–March 31, 2020 (n=417) |
Discussion
This is the first study in Ethiopia to report the promising result of the “Test and Treat” strategy for newly HIV infected patients. Two-thirds of study subjects initiated ART early, within 7 days, and nearly half (45%) initiated ART on the same day of confirmed HIV diagnosis. Recent analysis of routine data in Zimbabwe and South Africa revealed 72% and 67% of HIV positive patients, respectively, initiated ART within 7 days, and two-thirds (65% and 64%) initiated ART on the same day of enrollment into HIV care.16,17 This figure indicated better linkage to ART care to implement the “treat-all” strategy. Rapid ART initiation to all HIV positive individuals regardless of CD4 count level or WHO clinical stage improves a continuum (or cascade) of HIV care and reduces HIV-related morbidity and mortality, and curtails the spread of HIV infection.5,–7–9,14,15
At present, delayed ART initiation is defined as those who started ART after 7 days of enrollment into HIV care. Odds for delayed ART initiation were 3-fold higher in subjects with a CD4 count >351 cells/mm3 (A0R=2.89, 95% CI=1.27–6.58) as compared to those with a CD4 count <155 cells/mm3. Similar findings were reported from follow-up studies in other Sub-Saharan African countries.18–20 Patients with a higher CD4 count might feel “too healthy” to require ART. As well, odds for delayed ART initiation were 3-fold higher in subjects with normal nutrition status (BMI=18.5–24.9 kg/m2) (AOR=3.12, 95% CI=1.29–7.57) as compared to underweight individuals. Patients with normal nutritional status could have preserved immunity and might not be clinically ill, and deferred to take ART early.
In this study, nearly half (46%) of TBC co-infected HIV patients started ART delayed (after 2 months). Subjects who had tuberculosis co-infection were 3-fold more likely to delayed ART initiation as compared to their counterparts (AOR=2.76, 95% CI=1.13–6.70). This finding was in agreement with studies from Ethiopia and other developing countries. Various ART guidelines explained uncovering diagnosis of TBC delayed ART initiation by 2–8 weeks to avoid IRIS and minimize drug toxicities.5,7,10,21–23
Odds for delayed ART initiation were 4-fold higher in those who used traditional treatment (AOR=4.03, 95% CI=2.03–8.00), consistent with a report from Tigray, Ethiopia. Alternative treatment users might have poor healthcare-seeking behavior, and delayed to initiate ART.24 Those who did not know ART users were 3-fold more delayed for ART initiation as compared to those who knew ART users (AOR=2.86, 95% CI=1.52–5.37). Similarly, studies in South Africa and India showed patients having an HIV positive relative or friend were more likely to start ART early. Possible explanation includes having a relative or friend already on ART could help to be familiar with HIV care. As well, subjects who knew PLHIV who disclosed their HIV status to relatives or friends got better social support to ease stigma and discrimination.25,26 Surprisingly, subjects out of the catchment area were 59% less likely to have delayed ART initiation (AOR=0.41, 95% CI=0.18–0.91). In contrast, studies in Sub-Saharan Africa reported the distance from HIV care site to be associated with low engagement on HIV care.26–28 This clinical scenario could be explained by subjects who were distant from the HIV care site might have understood benefit of ART care, but might have low confidence to initiate ART in their locality.
Limitation of the Study
Data were cross-sectional, not longitudinal, preventing assessment of whether identified associated factors caused or resulted from delayed ART initiation. Selection bias might reduce the generalizability of the study.
Conclusions
One-third (34%) of study subjects initiated ART delayed, beyond 7 days of confirmed HIV diagnosis. Identified characteristics of patients with delayed ART initiation (DARTI) included normal nutritional status, higher CD4 count, TBC co-infection, use of traditional treatment, did not know other ART user(s) and site of ART center.
Recommendations
Early HIV testing mechanisms and timely linkage to HIV care by advocating “Test-and-Treat” should be strengthened. Intensive counseling should be reinforced to subjects who had predictive health-related characteristics towards delayed ART initiation.
Abbreviations
ART, antiretroviral therapy; ADL, activity of daily living; AOR, adjusted odds ratio; BMI, body mass index; BSc, Bachelor of Science; COR, crude odds ratio; CI, confidence interval; DARTI, delayed ART initiation; EARTI, early ART initiation; HIV, Human Immunodeficiency Virus; IRIS immune reconstitution inflammatory syndrome; OIs, opportunistic infections; PCP, Pneumocystis jirovecii pneumonia; PLHIV, people living with HIV/AIDS; PITC, provider initiated testing and counseling; SD, standard deviation; TBC, tuberculosis; UTT, universal test and treat; VCT, voluntary counseling and testing; WHO, World Health Organization.
Data Sharing Statement
All data generated and analyzed are included in this research article.
Ethics Approval and Consent to Participate
Ethical approval was obtained from Institutional Review Board of College of Medicine and Health Sciences, University of Gondar. Formal letter of permission was obtained from Nekemte Referral hospital administrative body. Study subjects were recruited only after informed written consent was obtained. The research was conducted in accordance with the “Declaration of Helsinki”.
Acknowledgment
We are grateful to the study participants and their health personnel.
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Global HIV & AIDS statistics - 2019 fact sheet [Internet]. Available from: https://www.unaids.org/en/resources/fact-sheet.
2. Ethiopia [Internet]. Available from: https://www.unaids.org/en/regionscountries/countries/ethiopia.
3. Progress report 2016: prevent HIV, test and treat all: WHO support for country impact. Available from: https://apps.who.int/iris/handle/10665/251713.
4. Fast-Track Commitments to end AIDS by 2030-UNAIDS. Available from: https://www.unaids.org/sites/default/files/media_asset/fast-track-commitments_en.pdf.
5. Guidelines for managing advanced HIV disease and rapid initiation of antiretroviral therapy 2017. Available from: https://www.who.int/hiv/pub/guidelines/advanced-HIV-disease/en.
6. HIV prevention in ethiopia national road map; 2018. Available from: https://ethiopia.unfpa.org/sites/default/files/pub-pdf.
7. National guidelines for comprehensive HIV prevention, care and treatment. Available from: https://aidsfree.usaid.gov/sites/default/files/resources/ethiopia_art_guidelines_2017.pdf.
8. Ford N, Migonea C, Calmyc A, et al. Benefits and risks of rapid initiation of antiretroviral therapy. AIDS. 2018;32(1):17–23. doi:10.1097/QAD.0000000000001671
9. Nash D, Yotebieng M, Sohn AH. Treating all people living with HIV in sub-Saharan Africa: a new era calling for new approaches. J Virus Erad 2018;4(Suppl. 2):1–4.
10. TB/HIV considerations for antiretroviral use in patients with co-infections in adult and adolescent. ARV [Internet]. AIDS info. Available from: https://aidsinfo.nih.gov/guidelines/html/1/adult-and-adolescent-arv.
11. WHO. WHO: guidelines for the diagnosis, prevention and management of cryptococcal disease in HIV-infected adults, adolescents and children. Available from: http://www.who.int/hiv/pub/guidelines/cryptococcal-disease/en.
12. Castro JG, Morrison-Bryant M. Management of Pneumocystis jirovecii pneumonia in HIV infected patients: current options, challenges and future directions. HIV/AIDS. 2010;2:123–134.
13. Birhan W, Giday M, Teklehaymanot T. The contribution of traditional healers’ clinics to public health care system in Addis Ababa, Ethiopia: a cross-sectional study. J Ethnobiol Ethnomed. 2011;7(1):39. doi:10.1186/1746-4269-7-39
14. Mateo-Urdiales A, Johnson S, Nachega JB, Eshun-Wilson I. Rapid initiation of antiretroviral therapy for people living with HIV. Cochrane Database Syst Rev. 2018;2:CD012962.
15. Rosen S, Fox MP, Larson BA, et al. Accelerating the uptake of antiretroviral therapy initiation in Sub-Saharan Africa: an operations research agenda. PLoS Med. 2016;13(8):e1002106. doi:10.1371/journal.pmed.1002106
16. Rufu A, Chitimbire VTS, Nzou C, et al. Implementation of the ‘Test and Treat’ policy for newly diagnosed people living with HIV in Zimbabwe in 2017. Internal Union Tuber Lung Dis. 2018;8(21):145–150.
17. Lilian RR, Rees K, Mcintyre JA, Struthers HE, Peters RPH. Same-day antiretroviral therapy initiation for HIV-infected adults in South-Africa: analysis of routine data. PLoS One. 2020;15(1):e0227572. doi:10.1371/journal.pone.0227572
18. Fatukasi TV, Cole SR, Moore RD, et al. Risk factors for delayed antiretroviral therapy initiation among HIV-seropositive patients. PLoS One. 2017;12(7):e0180843.:
19. Teklu AM, Delele K, Abraha M, Belayhun B, Gudina EK, Nega A. Exploratory analysis of time from HIV diagnosis to ART start, factors and effect on survival: A longitudinal follow up study at seven teaching hospitals in Ethiopia. Ethiop J Health Sci. 2017;27(1):17–28. doi:10.4314/ejhs.v27i1.3S
20. Bor J, Chiu C, Ahmed S, et al. Failure to initiate HIV treatment in patients with high CD4 counts: evidence from demographic surveillance in rural South Africa. Trop Med Int Health. 2018;23(2):206–220. doi:10.1111/tmi.13013
21. Anlay DZ, Tiruneh BT, Dachew BA. Late ART Initiation among adult HIV patients at university of Gondar Hospital, Northwest Ethiopia. Afr Health Sci. 2019;19(3):2324–2334. doi:10.4314/ahs.v19i3.4
22. Gesesew H, Tsehayneh B, Massa D, Tesfay A, Kahasay H, Mwanri L. The prevalence and associated factors for delayed presentation for HIV care among tuberculosis/HIV co-infected patients in Southwest Ethiopia: a retrospective observational cohort. Cochrane Database Syst Rev. 2016;5(96):1–10. doi:10.1186/s40249-016-0099-8
23. Abay SM, Deribe K, Reda A, et al. The effect of early initiation of antiretroviral therapy in TB/HIV co-infected patients. A systematic review and meta-analysis. J Inter Assoc Provid AIDS Care. 2015;14(6):560–570. doi:10.1177/2325957415599210
24. Assen A, Molla F, Wondimu A, et al. Late presentation for diagnosis of HIV infection among HIV positive patients in South Tigray Zone, Ethiopia. BMC Public Health. 2016;16:558–564. doi:10.1186/s12889-016-3263-y
25. Alvarez-Uria G, Pakam R, Midde M, Naik PK. Predictors of delayed antiretroviral therapy initiation, mortality, and loss to follow up in HIV infected patients eligible for HIV treatment: data from an HIV cohort study in India [Internet]. Biomed Rest. 2013
26. Plazy M, Newell M-L, Orne-Gliemann J, Naidu K, Dabis F, Dray-Spira R. Barriers to antiretroviral treatment initiation in rural KwaZulu-Natal, South Africa. HIV Med. 2015;16:521–532. doi:10.1111/hiv.12253
27. Fox MP, Mazimba A, Seidenberg P, Crooks D, Sikateyo B, Rosen S. Barriers to initiation of antiretroviral treatment in rural and urban areas of Zambia: a cross-sectional study of cost, stigma, and perceptions about ART. J Int AIDS Soc. 2010;13:8–18. doi:10.1186/1758-2652-13-8
28. Kunihira NR, Nuwaha F, Mayanja R, Peterson S. Barriers to use of antiretroviral drugs in Rakai district of Uganda. Afr Health Sci. 2010;10(2):120–129.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.