")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Prevalence and Determinants of COVID-19 Vaccine Hesitancy Among the Ethiopian Population: A Systematic Review
Authors Yehualashet DE , Seboka BT , Tesfa GA , Mamo TT , Yawo MN , Hailegebreal S
Received 26 March 2022
Accepted for publication 25 July 2022
Published 29 July 2022 Volume 2022:15 Pages 1433—1445
DOI https://doi.org/10.2147/RMHP.S368057
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Delelegn Emwodew Yehualashet,1 Binyam Tariku Seboka,1 Getanew Aschalew Tesfa,1 Tizalegn Tesfaye Mamo,1 Mulugeta Namaro Yawo,1 Samuel Hailegebreal2
1School of Public Health, Dilla University, Dilla, Ethiopia; 2School of Public Health, Arba Minch University, Arba Minch, Ethiopia
Correspondence: Delelegn Emwodew Yehualashet, School of Public Health, Dilla University, Dilla, Ethiopia, Tel +251 976061907, Email [email protected]
Introduction: Although vaccination is the most effective way to end the COVID-19 pandemic, there are growing concerns that vaccine hesitancy may undermine its effectiveness. In Ethiopia, vaccine hesitancy forms a major challenge to the uptake of COVID-19 vaccines. This systematic review examined the prevalence and determinants of the COVID-19 vaccine hesitancy among the Ethiopian population.
Methods: A systematic search of articles was conducted in PubMed, EBSCO, Google Scholar, and Semantic Scholar. Studies that evaluated the prevalence and determinants of COVID-19 vaccine hesitancy in Ethiopia were included. The identified determinants of COVID-19 vaccine hesitancy were analyzed based on the frequency of occurrence in the included studies.
Results: The overall COVID-19 vaccine hesitancy level in the Ethiopian population ranged from 14.1% to 68.7%. The high COVID-19 vaccine hesitancy rate observed in this study was due to contextual factors, individual factors, and vaccine-specific factors. Young age, female sex, living in rural areas, lack of adequate information, and lower education are the most common contextual determinants of the COVID-19 vaccine hesitancy. Lack of awareness about the COVID-19 vaccine, low risk of COVID-19, poor adherence to COVID-19 prevention strategies, and negative attitude towards the COVID-19 vaccine are the most frequently reported personal factors. Common vaccine-specific determinants of COVID-19 vaccine hesitation are the side effects of the vaccine and doubts about its effectiveness of the vaccine.
Conclusion: Our review showed that COVID-19 vaccine hesitancy remains highly prevalent and varied across regions of Ethiopia, with a wide variety of factors associated with it. Potential interventions on the benefits of vaccination and the adverse effects of vaccine rejection are crucial to enhance COVID-19 vaccine uptake among the Ethiopian population.
Keywords: COVID-19, vaccine, hesitancy, acceptance, systematic review, Ethiopia
Introduction
Coronavirus disease 2019 (COVID-19) is an infectious disease caused by the novel coronavirus (SARS-CoV-2) and was first identified in December 2019 in Wuhan, China.1 The World Health Organization (WHO) declared COVID-19 as a global pandemic on 11 March 2020.2 The virus infects millions of people and kills millions since its inception.3 Vaccines effectively reduce the risk of serious illness and death from COVID-19. The COVID-19 vaccine is also safe and has a low risk of serious adverse events.4–6
Vaccines provide great protection in terms of public health, however, to be successful, the vaccine level must be high.7 Especially relevant in the context of the current COVID-19 epidemic, high vaccination coverage rates are needed to provide indirect protection to society as a whole, bring society back to a normal way of life, and to re-open the world economy to the general population.8 High vaccination rates are also important in achieving herd immunity to reduce the spread of COVID-19 and to create a lower risk of infection in the general population and those most susceptible to transmission.8–10
The success of the COVID-19 vaccination program depends on the proportion of people who prefer to be vaccinated, and recent estimates suggest that up to 70% of the population may need to be vaccinated to end the current epidemic.11 COVID-19 vaccines need to be released as quickly as possible to bring the public back to normal as soon as possible. However, vaccine hesitancy poses a major threat to the effectiveness of the vaccine in preventing disease and death from COVID-19.12,13 Studies conducted in 2021 show that between 40% and 50% of respondents worldwide are reluctant to receive the COVID-19 vaccine with wide variations across countries.14,15 In Ethiopia, a survey found that only 31% of the general population was willing to receive the COVID-19 vaccine.16
The WHO defines vaccine hesitancy as “delay in acceptance or rejection of safe vaccines despite the availability of vaccine services”.17 COVID-19 vaccine hesitancy is thought to be a multi-factor event influenced by a range of factors. It includes cognitive, psychological, socio-demographic, political, and cultural factors and varies among different populations.18 Numerous studies have shown that public concern about the safety and/or side effects of COVID-19 vaccines, widespread misinformation about COVID-19 vaccines, and distrust in governments are the factors contributing to the growing hesitancy toward COVID-19 vaccines.19–22 Overcoming vaccine hesitancy is complex, so no single intervention can be completely resolved, especially in the case of COVID-19 where the evidence for effective strategies to address it is currently limited.23 Hence, a multi-component approach tailored to the local population is required to effectively address vaccine hesitancy.23 Accordingly, it is essential to understand the proportion and determinants of the COVID-19 vaccine hesitancy to inform policymakers and formulate direct intervention measures that can successfully combat the COVID-19 pandemic.
Despite the growing literature, examining the prevalence and determinants of the COVID-19 vaccine in Ethiopia, limited comprehensive evidence has been presented to provide an in-depth and systematic summary of important factors driving vaccine hesitancy specific to the Ethiopian population. This systematic review aimed to examine the proportion of COVID-19 vaccine hesitancy and its associated factors among the Ethiopian population. This review provides valuable insights for policymakers to design and implement targeted and holistic interventions to combat the COVID-19 epidemic in Ethiopia. It helps and facilitates the planning of vaccination campaigns to improve the uptake of the COVID-19 vaccine. Furthermore, our result can not only increase COVID-19 vaccine coverage but also improve the readiness of the existing health system for routine and emergency vaccination.
Methods
A systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.24 By using these guidelines, we have developed a search strategy and eligibility criteria before review. Then, the search was conducted through a two-step selection process based on the pre-defined eligibility criteria and evaluated the returned articles. After identifying studies relevant to this review, relevant data were collected from each study. Details of the review process are provided below.
Research Questions
- What is the proportion of COVID- 19 vaccine hesitancy among the Ethiopian population?
- What are the determinants of COVID-19 vaccine hesitancy among the Ethiopian population?
Information Sources and Search Strategy
PubMed, EBSCO, Google Scholar, and Semantic Scholar were searched by using the following search strategy: (“COVID-19” OR “SARS-CoV-2” OR “corona virus disease 2019” OR “nCOV” OR “2019-nCOV”) AND (“vaccine” OR “vaccination”) AND (“acceptance” OR “willingness” OR “intention” OR “hesitancy”) AND (“associated factors” OR “determinant factors”) AND (“Ethiopia”).
Eligibility Criteria
The inclusion criteria for this systematic review were peer-reviewed journal articles, survey studies done among the Ethiopian population (general population, health care workers, teachers, students, drivers, lactating mothers, adults, bankers, pregnant women, and patients), studies that investigated the prevalence and/or determinants of COVID-19 vaccine hesitancy/acceptance/willingness, and studies published in English until January 18, 2022. Unpublished manuscripts (preprints), non-empirical studies, articles studying vaccine hesitancy other than COVID-19 disease, studies conducted in other countries, and articles that did not report the outcome of interest were excluded from the present systematic review.
Screening and Selection
The identified articles were selected in two stages. The first step involves screening all article titles and abstracts based on eligibility criteria, followed by reviewing the full text of articles with similar criteria. Initially, two independent reviewers examined all titles and abstracts for eligible articles. Disputes regarding exclusions between the two reviewers were resolved through discussions. Finally, all the reviewers individually evaluated the full text of each article and made a final selection of articles to be included.
Outcome of Interest
In this systematic review, the primary outcome was the prevalence of the COVID-19 vaccine hesitancy, which was reported in the included studies. The secondary outcome was determinants of COVID-19 vaccine hesitancy, which has been reported in included studies.
Data Extraction and Analysis
Studies that met the inclusion criteria were further analyzed and the following items were extracted from each study: authors, year of publication, study period, data collection method, target population, study design, sample size, prevalence, and determinants of COVID-19 vaccine hesitancy. The Strategic Advisory Group of Experts (SAGE) determinants of vaccine hesitancy model25 was used to categorize the determinants. Using this model, the determinants of COVID-19 vaccine hesitancy were categorized into three groups: contextual factors, individual/group factors, and vaccine/vaccination-related factors. Finally, the factors were analyzed according to the frequency of occurrences in the studies.
Quality Assessment
Quality was assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Analytical Cross-Sectional Study.26 There are nine criteria in the checklist to assess the quality of cross-sectional studies. Each item in the evaluation criterion is represented by “yes”,“no”, “unclear” or “not available”. The score is one (1) for yes and zero (0) for the rest. A quality score is calculated for each article by dividing the total score by the total possible score. Each article is classified as low quality (<50%), medium quality (50–69%), or high quality (≥7 0%).
Results
Study Selection
The selection process and relevant eligibility criteria are presented in Figure 1. A total of 1801 articles were identified for initial screening. Of this, 903 articles were excluded due to duplication. Following the removal of the duplicates, the titles and abstracts of 898 articles were evaluated for eligibility. Leaving 824 articles based on title and abstract screening, 74 articles were retained for full-text screening. Subsequently, 54 studies were excluded after the full-text screening. Finally, 20 articles have been included in the present systematic review.
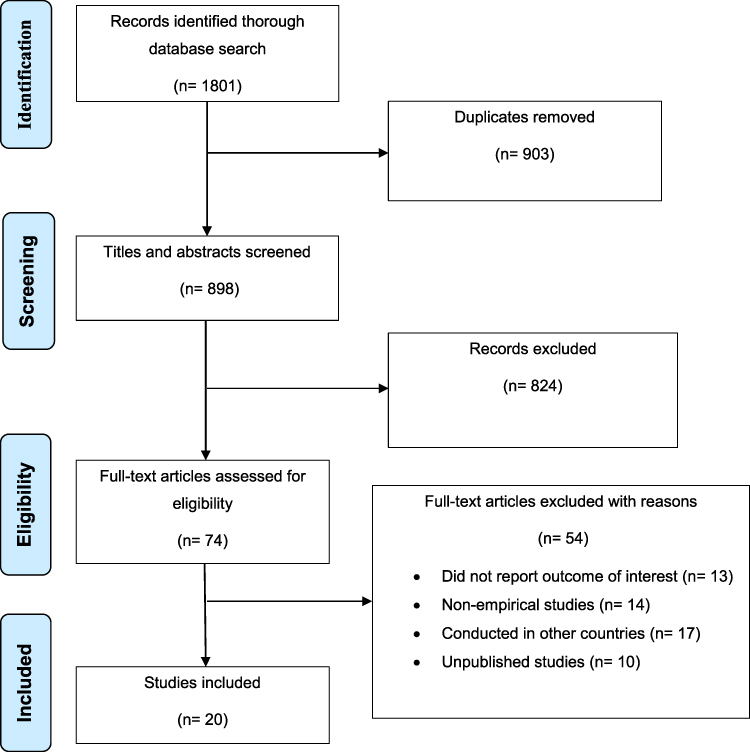 |
Figure 1 PRISMA flow chart of study selection process for systematic review of the prevalence and determinants of COVID-19 vaccine hesitancy among the Ethiopian population. Notes: Adapted from: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71.24 Creative Commons Attribution (CC BY 4.0) license (https://creativecommons.org/licenses/by/4.0/legalcode). |
Characteristics of Included Studies
A total of 20 cross-sectional studies published up to January 18, 2022, were analyzed in this review. Most studies have been conducted on health workers. The paper questionnaire is a commonly used data collection tool in the included studies. The largest sample size was 1184 and the smallest sample size was 323. More than half of the studies were conducted in the SNNPR (n = 7) and Amhara regions (n = 6) in Ethiopia. Further details of the included studies are shown in Table 1.
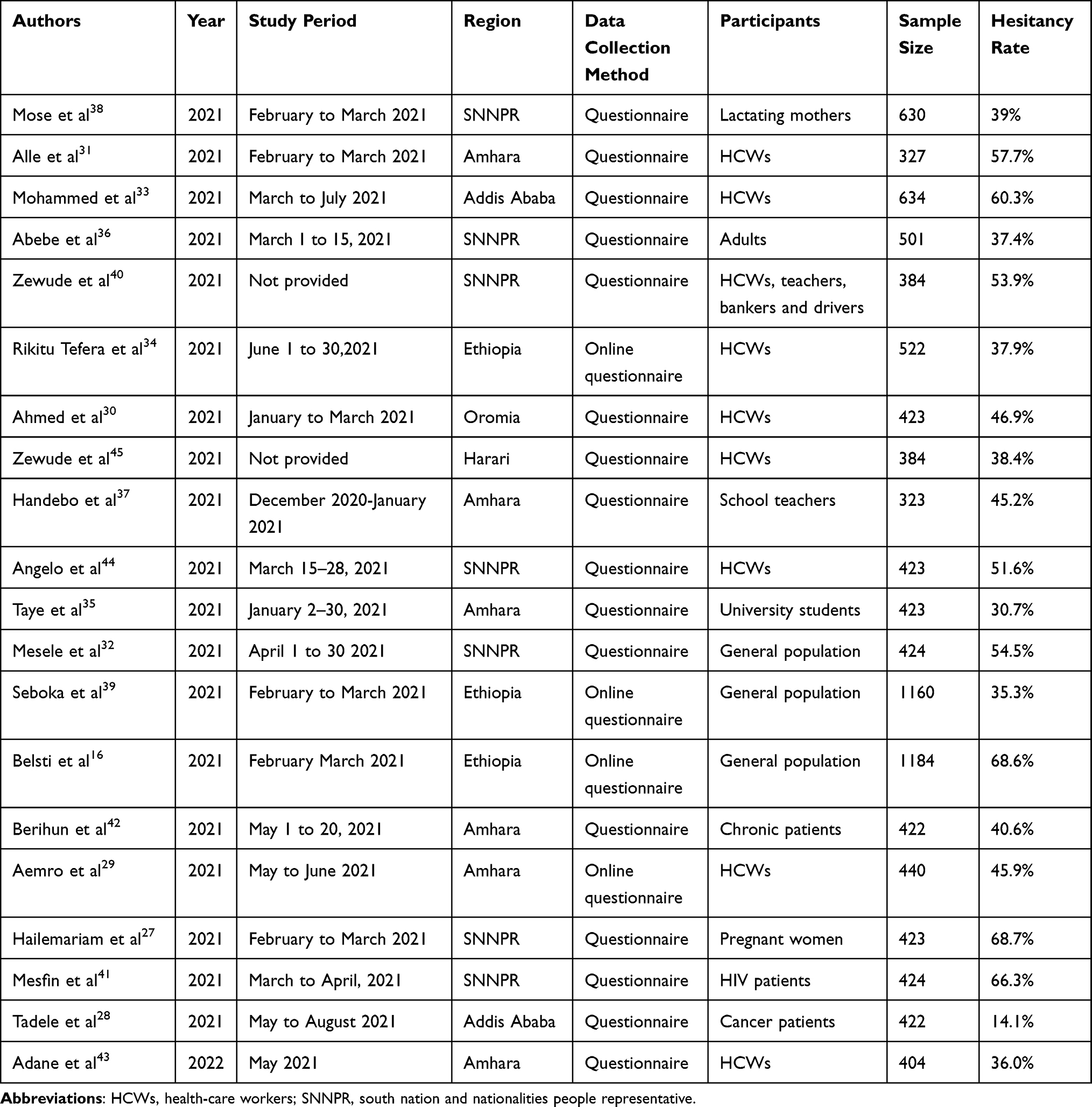 |
Table 1 Characteristics of Studies Included in the Systematic Review of Prevalence and Determinants of COVID-19 Vaccine Hesitancy in Ethiopia, 2022 |
COVID-19 Vaccine Hesitancy Rate in Ethiopia
The proportion of COVID-19 vaccine hesitancy from different parts of Ethiopia is presented in Table 1. The highest level of COVID-19 vaccine hesitancy was reported among pregnant women in SNNPR (68.7%)27 and the lowest level of COVID-19 vaccine hesitancy was recorded among cancer patients in Addis Ababa (14.1%).28
Determinants of COVID-19 Vaccine Hesitancy in Ethiopia
Contextual Factors
A total of 12 factors were identified under contextual determinants of COVID-19 vaccine hesitancy (Table 2). Among the contextual factors being young appeared in seven of the 20 studies (35%).29–35 Lower educational status appeared in six of the 20 studies (30%).16,27,36–39 Lack of adequate information on COVID-19 vaccination appeared in four of the 20 studies (20%).28,32,39,40 Being females,16,39,41 living in rural areas,16,27,38 and religious beliefs,16,30,37 each appeared in three of the 20 studies (15%). Lack of trust in government33,40 and being only academic staff in university hospitals34,36 appeared in two of the 20 studies (10%). Four factors, namely: being married,16 not having health insurance,42 being a non-health science student,35 and unclear information by public health authorities,29 each appeared in one of the 20 articles (5%).
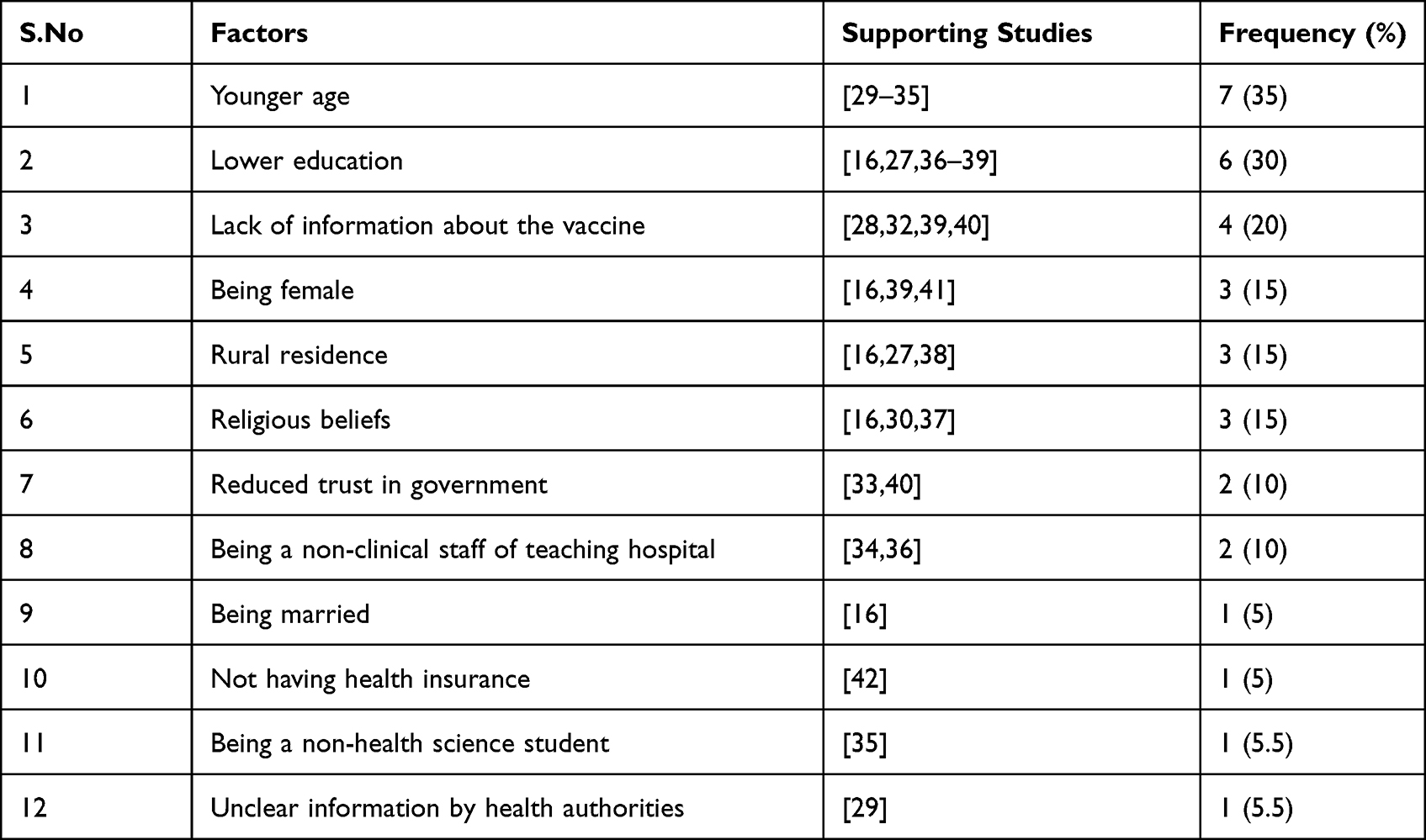 |
Table 2 Contextual Determinants of COVID-19 Vaccine Hesitancy in Ethiopia |
Individual Factors
Ten factors were identified for the individual determinants of COVID-19 vaccine hesitancy (Table 3). Among the ten factors under this category poor knowledge about the COVID-19 vaccine27,30,35,36,38,41,42 and low perceived risk of being infected with COVID-1928–30,32,37,43,44 appeared in seven of the 20 studies (35%). Poor compliance with COVID-19 prevention measures27,29,35,38,44 and negative attitude towards COVID-19 vaccine30,40,42–44 appeared in five of the 20 studies (25%). Not having a history of chronic illness appeared in three of the 20 studies (15%).36,41,44 Not having close relatives or friends diagnosed with COVID-1939,42 and not having COVID-19 infection experience28,34 appeared in two of the 20 studies (10%). Three factors, namely: believing that other non-vaccine preventive mechanisms are sufficient to prevent COVID-19 infection,45 belief in having adequate natural immunity,45 and lesser trust in science,33 each appeared in one of the 20 articles (5%).
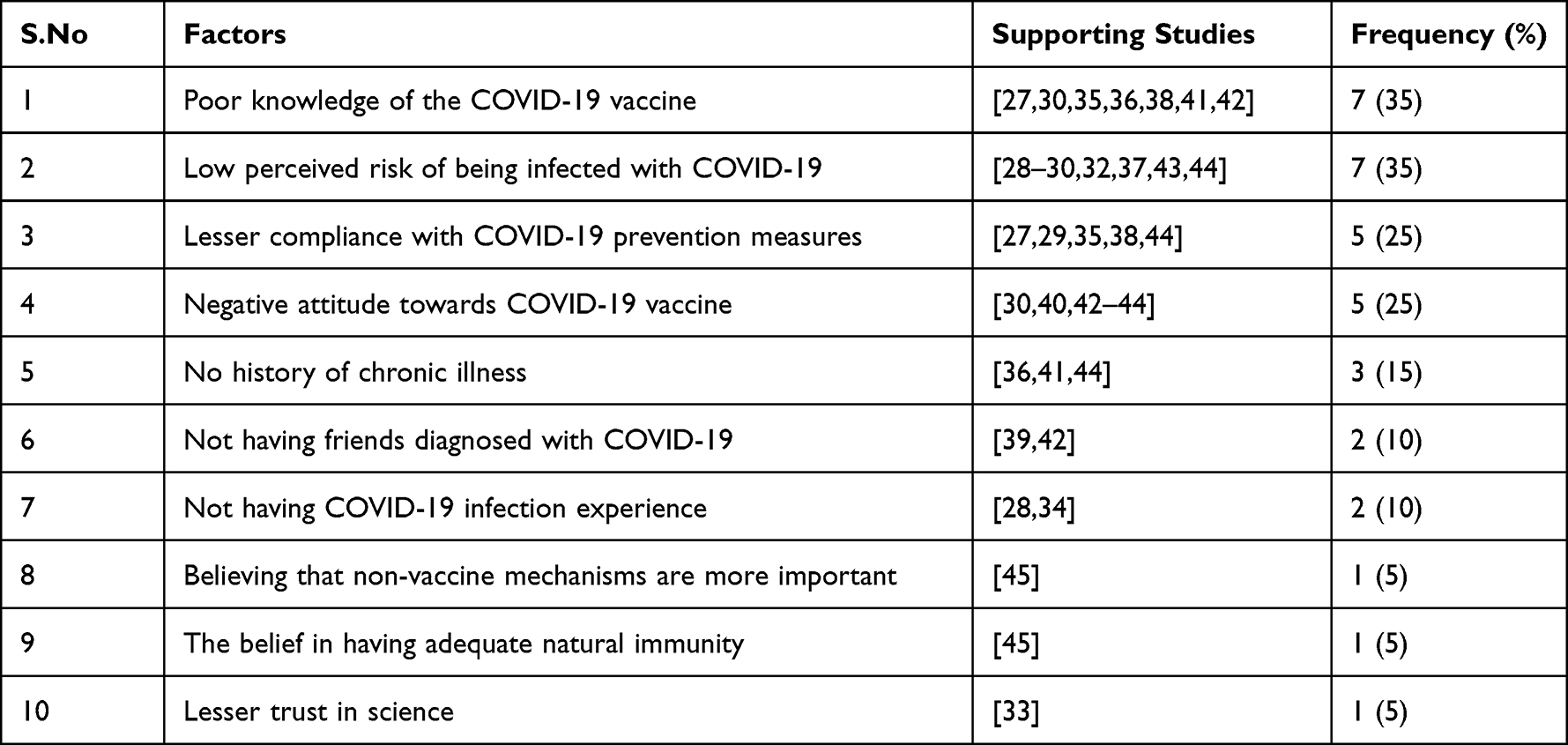 |
Table 3 Individual/Group Related Determinants of COVID-19 Vaccine Hesitancy in Ethiopia |
Vaccine Related Factors
A total of 3 factors were identified under vaccine-related determinants of COVID-19 vaccine hesitancy (Table 4). Among the three factors under this category concern about the safety and/or side effect of the vaccine appeared in six of the 20 studies (30%).29,33,37,39,40,45 Doubts about the effectiveness of the vaccine appeared in four of the 20 studies (20%).32,37,40,45 Lack of advocacy for COVID-19 vaccination from health professionals appeared in one of the 20 studies (5%).38
 |
Table 4 Vaccine/Vaccination-Related Determinants of COVID-19 Vaccine Hesitancy in Ethiopia |
Quality of Included Studies
The JBI critical appraisal checklist for analytical cross-sectional studies included the following eight criteria. (#1) Was the criteria for inclusion in the sample clearly defined? (#2) Were the study subjects and the setting described in detail? (#3) Was the exposure measured validly and reliably? (#4) Were objective, standard criteria used for measurement of the condition? (#5) Were confounding factors identified? (#6) Were strategies to deal with confounding factors stated? (#7) Were the outcomes measured validly and reliably? (#8) Was appropriate statistical analysis used? Based on the above criteria, the quality score of included studies is given in (Table 5). Of the included studies, 15 were rated as high quality, five as moderate quality, and no studies were rated as poor quality.
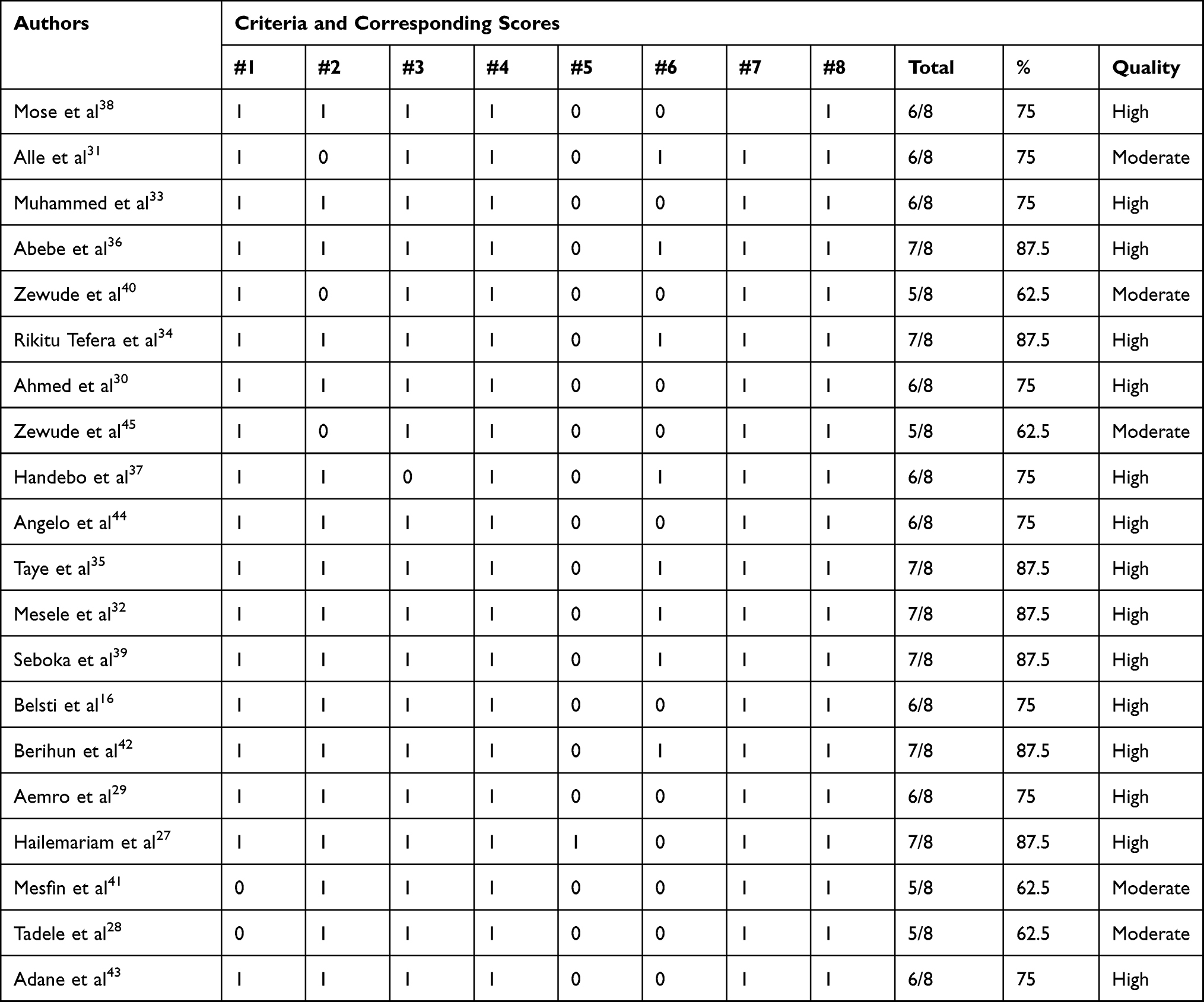 |
Table 5 Quality Assessment Results of the Included Studies Using the JBI Critical Appraisal Checklist for Analytical Cross-Sectional Studies |
Discussion
In this review, we examined the proportion and determinants of COVID-19 vaccine hesitancy in Ethiopia. The overall proportion of COVID-19 vaccine hesitancy ranged from 14.1% to 68.7%, as reported in Addis Ababa and SNNPR, respectively. This finding suggests that vaccine hesitancy poses a serious challenge to COVID-19 pandemic management and control. Many countries are developing vaccines to protect their populations from the current COVID-19 pandemic.46 The widespread use of the COVID-19 vaccine is believed to boost herd immunity and protect the population from COVID-19.47 However, with this high level of COVID-19 vaccine resistance, the current COVID-19 pandemic is becoming increasingly difficult to manage and control. Therefore, the establishment of educational resources should be implemented to improve the use of the COVID-19 vaccine to make the population aware of its safety, the importance of the vaccine, and the adverse effects of vaccine rejection.
In this study, the proportion of the COVID-19 vaccine hesitancy in the general population in Ethiopia ranged from 35% to 68%. Similarly, previous studies show that between 40% and 50% of the world’s population are reluctant to receive the COVID-19 vaccine, with variations in different countries.14,15 In addition, our results were similar to another study conducted in Germany, with 42.5% of the participants reporting that they were hesitant to vaccinate against COVID-19.48 On the contrary, the acceptance rate of the COVID-19 vaccine was observed to be high in the USA (81%)49 and the Chinese population (91.3).50 This can be attributed to differences in the spread and burden of the COVID-19 pandemic between countries. In addition, the variation can be explained by differences in awareness of the severity of COVID-19 and access to healthcare. This discrepancy may also be due to differences in respondents’ local traditions, cultures, and beliefs about the benefits and risks of the COVID-19 vaccine. For example, the Chinese population had strong beliefs about the effectiveness of the COVID-19 vaccine, as 89.5% thought the vaccine was an effective way to prevent and control COVID-19.50 This positive attitude towards COVID-19 vaccination and the perceived major pandemic impact may explain the high acceptance of the COVID-19 vaccine among the Chinese population compared to the Ethiopian population.
Our review also indicated that the proportion of COVID-19 vaccine hesitancy among healthcare workers in Ethiopia ranged from 36% to 60.3%. The result of this study was in line with a previous systematic review which reported the proportion of COVID-19 vaccine hesitancy as 49%.51 This implies that a considerable proportion of healthcare workers were hesitant towards the COVID-19 vaccine, which hinder their recommendation of vaccination to their patients. Evidence shows that the attitude of the healthcare workers toward the COVID-19 vaccine was found to influence their intention to suggest the vaccine to their patients and the general population.52 This problem is alarming due to the position of health care workers at the forefront in combating the spread and impact of the COVID-19 epidemic, which puts them at risk of infection.53–55 Therefore, health workers need to be involved in future priority education so that they can influence the use of vaccines and be approved by the population.
The widespread prevalence of COVID-19 vaccine hesitancy observed in our study is due to the following factors: contextual factors, individual factors, and vaccine-specific factors. Younger age, being females, living in rural areas, lack of adequate information, and lower education were common contextual factors associated with COVID-19 vaccine hesitancy. Poor knowledge about the COVID-19 vaccine, lower self-perceived risk of infection with COVID-19, poor adherence to COVID-19 prevention rules, and negative attitude towards COVID-19 vaccine were most frequently mentioned individual and group related factors associated with increased COVID-19 vaccine hesitancy. Common vaccine/vaccination-specific determinants included concerns about the safety and/or side effects of the vaccine and worries about the effectiveness of the vaccine.
Being young was the most frequently mentioned determinant of COVID-19 vaccine hesitancy. This is in line with previous systematic reviews of COVID-19 vaccine hesitancy.56–60 This increase in the hesitancy of the COVID-19 vaccine among young people may be due to the WHO announcement about groups at high risk of COVID-19 infection and death. The WHO has declared that the COVID-19 pandemic is more prevalent and worse for older people than for younger ones. This leads to younger participants being more hesitant than older participants.61 This finding also means that older people may have more responsibility and accountability towards themselves and their families. Therefore, an in-depth understanding of the potential factors influencing adolescents’ hesitancy to take the COVID-19 vaccine and their vaccine intent will contribute to the development and implementation of effective methods to promote the COVID-19 vaccine in this group.
Our review also confirmed that females were more hesitant to the COVID-19 vaccine. This is consistent with the findings of various systematic reviews,56–60 which identified being females as one of the most frequently reported factors associated with increased COVID-19 vaccine hesitancy. Studies conducted in Bangladesh and Vietnam also reported higher COVID-19 vaccine hesitancy among female respondents.62,63 The main reasons may be the apparent low-risk perception of COVID-19, high beliefs of conspiracy-related theories about the pandemic in women than men,64 and concerns about the safety of vaccination during pregnancy and lactation.65
The current study also identified a low level of education as a major determinant of COVID-19 vaccine hesitancy. This is in line with the findings of some systematic reviews,57,58,66 which identified a low level of education among commonly cited determinants of COVID-19 vaccine hesitancy. In a US study, high levels of hesitancy against the COVID-19 vaccine were shown in people with limited education.67 This may be because more educated people have better access to vaccine information and can understand information about the benefits and safety of the COVID-19 vaccine; on the contrary, the uneducated are more likely to be misinformed about the vaccine. Thus, individuals should be aware of herd immunity, vaccine safety, and how vaccines can help people return to their daily lives.
Consistent with the findings in many systematic reviews;57–59,66,68 living in rural areas was one of the most frequently reported determinants of COVID-19 vaccine hesitancy. Further, a study from Bangladesh reported that rural residents were more reluctant to vaccinate than those living in urban areas.62 The high prevalence of vaccination among urban dwellers can be explained as people living in urban areas have improved access to health care and are more exposed to different media than the rural population. In addition, compared with the urban community, rural communities may be reluctant to vaccinate because of certain cultural practices and religious beliefs that prevent vaccination.69
Poor knowledge of the COVID-19 vaccine was also an important factor associated with the growing hesitancy against the COVID-19 vaccine. This result is consistent with previous studies conducted in Southeast Asia and England.70,71 These findings are explained by having good knowledge of the COVID-19 vaccine will help people to know the benefits of the COVID-19 vaccine. Hence, improving public awareness of the benefits, efficacy, and safety of the COVID-19 vaccine is one of the strategies to achieve targeted vaccine coverage. To increase public awareness about the COVID-19 vaccination, there need to be frequent social campaigns that highlight the vaccine’s usefulness.
Poor adherence to COVID-19 prevention measures was one of the most frequently stated factors influencing COVID-19 vaccine hesitancy. Consistent with this, a high hesitancy of the COVID-19 vaccine was found among people who showed poor adherence to COVID-19 protection measures such as social isolation, face masking, and frequent hand washing.72 Our study found that low trust in the government and the actions they took, the health care response, and the information provided by health officials were associated with the rejection of the COVID-19 vaccine. Other studies have also reported a lack of trust in government/health officials as a factor in the COVID-19 vaccine reluctance.73,74 Evidence suggests that people who trust the government’s message are more likely to adhere to disease prevention practices. Therefore, the Ethiopian government and health authorities should work to build public trust and explicitly state the effectiveness of the vaccine, adverse effects, and safety through traditional media and other means.
The perception of a low risk of being infected with COVID-19 was found to be associated with COVID-19 vaccine hesitancy. This is consistent with studies conducted in Vietnam and South Italy.75,76 This is because people who find themselves at low risk are less concerned about getting infected with COVID-19. As a result, they will not fully participate in COVID-19 prevention strategies, including vaccination.77 Therefore, interventions with different communication methods should be implemented to explain the risk of COVID-19 to the population.
Concerns about the safety and side effects of the vaccines were recognized as a major determinant of COVID-19 vaccine hesitancy. This is in line with a study conducted among healthcare workers in Egypt.78 Another systematic review found that the main reasons for vaccine rejection were concerns about vaccine safety and efficacy.21 This is because hesitancy is largely caused by concerns about the safety, efficiency, and side effects of the vaccine. People who are unsure whether the side effects of the COVID-19 vaccine are tolerable or not are very reluctant to take this vaccine.79,80 Therefore, the provision of clear and scientifically valid information about the safety of the COVID-19 vaccine and its adverse outcomes should be a priority task for public health authorities. Since willingness to take the COVID-19 vaccine and its perceived safety and efficacy are strongly linked, it is important to build confidence in the vaccine. The high efficacy and safety of COVID-19 vaccines increase public confidence in the vaccines, thus reducing vaccine hesitancy. The government should continue to educate the public about the safety and side effects to boost confidence in vaccines. It is also important to understand how the implementation of public health measures affects vaccination hesitancy.
Overall, this review has briefly summarized the level of COVID-19 vaccine hesitancy among the Ethiopian population and associated factors. These findings will make a significant contribution to health policymakers, health authorities, researchers, health care providers, and the entire population. All relevant organs should be actively involved to overcome the COVID-19 vaccine hesitancy that can minimize the morbidity and mortality associated with this pandemic and halt this period of the pandemic. Identifying factors based on their frequency of occurrence in the literature can help policymakers prioritize effort levels for maximum effectiveness, and the results of this review should enable future studies to explore the significance and order of importance. In addition, public health authorities should encourage the uptake of the COVID-19 vaccine by providing reliable information about the COVID-19 vaccine. The population needs to be educated about the efficacy, benefits, and safety of the COVID-19 vaccine to increase acceptance rates of this vaccine. It is also imperative to disseminate better public health messages to raise awareness and change the negative attitudes of the population towards the COVID-19 vaccine. Furthermore, future studies may use our findings to explore strategies to address COVID-19 vaccine hesitancy in Ethiopia.
Strengths and Limitations
To our knowledge, our study is the first to bring together key factors of COVID-19 vaccine hesitancy across contextual, individual, and vaccine-specific effects among the Ethiopian population to shed light on the design of targeted intervention programs. Another strength of this review lies in the analysis of factors based on the frequency of occurrence in the literature, which facilitates the understanding of the most important factors causing COVID-19 vaccine hesitancy in Ethiopia. Despite its strength, our review has some limitations. Some of the studies included in this review were subject to selection bias because people required internet access to participate in the study and complete the survey. Moreover, the protocol for this review has not been prospectively registered in PROSPERO.
Conclusion
Overall, COVID-19 vaccine hesitancy is quite common and differs in different parts of Ethiopia. Younger age, being female, living in a rural area, lack of adequate information, and low education were the most common contextual determinants of COVID-19 vaccine hesitancy. Insufficient knowledge about the COVID-19 vaccine, low self-perceived risk of contracting COVID-19, poor adherence to COVID-19 prevention measures, and negative attitude toward the COVID-19 vaccine were the most frequently studied individual factors. Common vaccine-specific determinants included concerns about vaccine safety and side effects, and doubts about vaccine efficacy.
Healthcare managers should acknowledge the widespread prevalence of COVID-19 vaccine hesitancy in Ethiopian regions and be aware of the factors we identified when formulating policies regarding the COVID-19 vaccine. Although we present our identified factors as separate factors, each factor alone does not affect COVID-19 vaccine hesitancy. Therefore, understanding the relationships between our identified factors and knowing how our factors affect each population group is crucial to improving COVID-19 vaccine uptake and addressing vaccine hesitancy among the Ethiopian population.
Data Sharing Statement
The data used to support the findings of this study are included in the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Song F, Shi N, Shan F, et al. Emerging 2019 Novel Coronavirus (2019-nCoV) Pneumonia. Radiology. 2020;295(1):210–217. doi:10.1148/radiol.2020200274
2. WHO director-general’s opening remarks at the media briefing on COVID-19-11 March 2020. Available from: https://www.who.int/directorgeneral/speeches/detail/who-director-general-s-opening-remarks-at-The-media-briefing-on-covid-19—11march–2020.
3. Noh J, Danuser G. Estimation of the fraction of COVID-19 infected people in U.S. states and countries worldwide. PLoS One. 2021;16(2):e0246772. doi:10.1371/journal.pone.0246772
4. World Health Organization. Coronavirus disease (COVID-19): vaccines safety; 2021. Available from: https://www.who.int/news-room/q-a-detail/coronavirus-disease-(covid-19)-vaccines-safety.
5. Centers for Disease Control and Prevention. Vaccine safety and monitoring; 2021. Available from: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety.html.
6. Majeed A, Molokhia M. Vaccinating the UK against covid-19. BMJ. 2020;371:m4654. doi:10.1136/bmj.m4654
7. Betsch C, B€ohm R, Korn L, Holtmann C. On the benefits of explaining herd immunity in vaccine advocacy. Nat Hum Behav. 2017;1(3):1–6.
8. Dube E, Laberge C, Guay M, Bramadat P, Roy R, Bettinger JA. Vaccine hesitancy: an overview. Hum Vaccines Immunother. 2013;9(8):1763–1773.
9. Larson HJ, Jarrett C, Schulz WS, et al. Measuring vaccine hesitancy: the development of a survey tool. Vaccine. 2015;33(34):4165–4175.
10. MacDonald NE. Vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33(34):4161–4164. doi:10.1016/j.vaccine.2015.04.036
11. Bartsch SM, O’Shea KJ, Ferguson MC, et al. Vaccine Efficacy Needed for a COVID-19 Coronavirus Vaccine to Prevent or Stop an Epidemic as the Sole Intervention. Am J Prev Med. 2020;59:493–503. doi:10.1016/j.amepre.2020.06.011
12. Hammer CC, Cristea V, Dub T, Sivelä J. High but slightly declining COVID-19 vaccine acceptance and reasons for vaccine acceptance, Finland April to December 2020. Epidemiol Infect. 2021;149:E123.
13. Kumari A, Ranjan P, Chopra S, et al. Knowledge, barriers and facilitators regarding COVID-19 vaccine and vaccination programme among the general population: a cross-sectional survey from one thousand two hundred and forty-nine participants. Diabetes Metab Syndr. 2021;15(3):987–992.
14. Institute of Global Health Innovation, Imperial College London. Covid-19: global attitudes towards a COVID-19 vaccine; 2021. Available from: https://www.imperial.ac.uk/media/imperial-college/institute-of-globalhealth-innovation/GlobalVaccineInsights_ICL-Covid-19-Behaviour-Tracker-EMBARGOED-00.01-04.02.2021.pdf.
15. Robinson E, Jones A, Daly M. International estimates of intended uptake and refusal of COVID-19 vaccines: a rapid systematic review and meta-analysis of large nationally representative samples. medRxiv. 2020. doi:10.1101/2020.12.01.20241729
16. Belsti Y, Gela YY, Akalu Y, et al. Willingness of Ethiopian Population to Receive COVID-19 Vaccine. J Multidiscip Healthc. 2021;14:1233–1243.
17. MacDonald NESAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33:4161–4164. doi:10.1016/j.vaccine.2015.04.036
18. Sallam M. Covid-19 vaccine hesitancy worldwide: a concise systematic review of vaccine acceptance rates. Vaccines. 2021;9(2):1–15.
19. Cerda AA, García LY. Hesitation and refusal factors in individuals’ decision-making processes regarding a coronavirus disease 2019 vaccination. Front Public Health. 2021;9(April):874.
20. Lazarus JV, Wyka K, Rauh L, et al. Hesitant or Not? The Association of Age, Gender, and Education with Potential Acceptance of a COVID-19 Vaccine: a Country-level Analysis. J Health Commun. 2020;25:799–807. doi:10.1080/10810730.2020.1868630
21. Lin C, Tu P, Beitsch LM. Confidence and Receptivity for COVID-19 Vaccines: a Rapid Systematic Review. Vaccines. 2020;9:16. doi:10.3390/vaccines9010016
22. Roozenbeek J, Schneider CR, Dryhurst S, et al. Susceptibility to misinformation about COVID-19 around the world. R Soc Open Sci. 2020;7:201199. doi:10.1098/rsos.201199
23. Jarrett C, Wilson R, O’Leary M, Eckersberger E; Larson HJSAGE Working Group on Vaccine Hesitancy. Strategies for addressing vaccine hesitancy - a systematic review. Vaccine. 2015;33:4180–4190. doi:10.1016/j.vaccine.2015.04.040
24. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:71.
25. World Health Organisation. Report of the SAGEWorking Group on Vaccine Hesitancy; 2014. Available from: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf.
26. Moola S, Munn Z, Tufanaru C, et al. Chapter 7: systematic reviews of etiology and risk. In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. JBI; 2020. Available from: https://synthesismanual.jbi.global.
27. Hailemariam S, Mekonnen B, Shifera N, et al. Predictors of pregnant women’s intention to vaccinate against coronavirus disease 2019: a facility-based cross-sectional study in southwest Ethiopia. SAGE Open Medicine. 2021;9:20503121211038454.
28. Tadele Admasu F. Knowledge and Proportion of COVID-19 Vaccination and Associated Factors Among Cancer Patients Attending Public Hospitals of Addis Ababa, Ethiopia, 2021: a Multicenter Study. Infect Drug Resist. 2021;14:4865–4876.
29. Aemro A, Amare NS, Shetie B, Chekol B, Wassie M. Determinants of COVID-19 vaccine hesitancy among health care workers in Amhara region referral hospitals, Northwest Ethiopia: a cross-sectional study. Epidemiol Infect. 2021;149:e225.
30. Ahmed MH, Kanfe SG, Jarso MH. Intention to receive vaccine against COVID-19 and associated factors among health professionals working at public hospitals in resource limited settings. PLoS One. 2021;16(7):e0254391.
31. Alle YF, Oumer KE. Attitude and associated factors of COVID-19 vaccine acceptance among health professionals in Debre Tabor Comprehensive Specialized Hospital, North Central Ethiopia; 2021: cross-sectional study. Virusdisease. 2021;32(2):1–7.
32. Mesele M. COVID-19 Vaccination Acceptance and Its Associated Factors in Sodo Town, Wolaita Zone, Southern Ethiopia: cross-Sectional Study. Infect Drug Resist. 2021;14:2361–2367.
33. Mohammed R, Nguse TM, Habte BM, Fentie AM, Gebretekle GB. COVID-19 vaccine hesitancy among Ethiopian healthcare workers. PLoS One. 2021;16(12):e0261125.
34. Rikitu Terefa D, Shama AT, Feyisa BR, et al. COVID-19 Vaccine Uptake and Associated Factors Among Health Professionals in Ethiopia. Infect Drug Resist. 2021;14:5531–5541.
35. Taye BT, Amogne FK, Demisse TL, et al. Coronavirus disease 2019 vaccine acceptance and perceived barriers among university students in northeast Ethiopia: a cross-sectional study. Clin Epidemiol Global Health. 2021;12:100848.
36. Abebe H, Shitu S, Mose A. Understanding of COVID-19 Vaccine Knowledge, Attitude, Acceptance, and Determinates of COVID-19 Vaccine Acceptance Among Adult Population in Ethiopia. Infect Drug Resist. 2021;14:2015–2025.
37. Handebo S, Wolde M, Shitu K, Kassie A. Determinant of intention to receive COVID-19 vaccine among school teachers in Gondar City, Northwest Ethiopia. PLoS One. 2021;16(6):e0253499.
38. Mose A. Willingness to Receive COVID-19 Vaccine and Its Determinant Factors Among Lactating Mothers in Ethiopia: a Cross-Sectional Study. Infect Drug Resist. 2021;14:4249–4259.
39. Seboka BT, Yehualashet DE, Belay MM, et al. Factors Influencing COVID-19 Vaccination Demand and Intent in Resource-Limited Settings: based on Health Belief Model. Risk Manag Healthc Policy. 2021;14:2743–2756.
40. Zewude B, Habtegiorgis T. Willingness to Take COVID-19 Vaccine Among People Most at Risk of Exposure in Southern Ethiopia. Pragmatic Observational Res. 2021;12:37–47.
41. Mesfin Y, Argaw M, Geze S, Zewdu BT. Factors Associated with Intention to Receive COVID-19 Vaccine Among HIV Positive Patients Attending ART Clinic in Southwest Ethiopia. Patient Prefer Adherence. 2021;15:2731–2738.
42. Berihun G, Walle Z, Berhanu L, Teshome D. Acceptance of COVID-19 Vaccine and Determinant Factors Among Patients with Chronic Disease Visiting Dessie Comprehensive Specialized Hospital, Northeastern Ethiopia. Patient Prefer Adherence. 2021;15:1795–1805.
43. Adane M, Ademas A, Kloos H. Knowledge, attitudes, and perceptions of COVID-19 vaccine and refusal to receive COVID-19 vaccine among healthcare workers in northeastern Ethiopia. BMC Public Health. 2022;22(1):128.
44. Angelo AT, Alemayehu DS, Dachew AM. Health care workers intention to accept COVID-19 vaccine and associated factors in southwestern Ethiopia, 2021. PLoS One. 2021;16(9):e0257109.
45. Zewude B, Belachew A. Intention to Receive the Second Round of COVID-19 Vaccine Among Healthcare Workers in Eastern Ethiopia. Infect Drug Resist. 2021;14:3071–3082.
46. Yoda T, Katsuyama H. Willingness to receive COVID-19 vaccination in Japan. Vaccines. 2021;9(1):48. doi:10.3390/vaccines9010048
47. Dodd RH, Cvejic E, Bonner C, et al. Willingness to vaccinate against COVID-19 in Australia. Lancet Infect Dis. 2021;21(3):318–319. doi:10.1016/S1473-3099(20)30559-4
48. Umakanthan S, Lawrence S. Predictors of COVID-19 vaccine hesitancy in Germany: a cross-sectional, population-based study. Postgrad Med J. 2022.
49. Mondal P, Sinharoy A, Su L. Sociodemographic predictors of COVID-19 vaccine acceptance: a nationwide US-based survey study. Public Health. 2021;198:252–259.
50. Wang J, Jing R, Lai X, et al. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines. 2020;8(3):87.
51. Luo C, Yang Y, Liu Y, et al. Intention to COVID-19 vaccination and associated factors among health care workers: a systematic review and meta-analysis of cross-sectional studies. Am J Infect Control. 2021;1:87.
52. Iguacel I, Maldonado AL, Ruiz-Cabello AL, et al. Attitudes of healthcare professionals and general population toward vaccines and the intention to Be vaccinated against COVID-19 in Spain. Front Public Health. 2021;9:879.
53. Nguyen LH, Drew DA, Graham MS, et al. Risk of COVID-19 among front-line health-care workers and the general community: a prospective cohort study. Lancet Public Health. 2020;5:e475–e483.
54. Shaukat N, Ali DM, Razzak J. Physical and mental health impacts of COVID-19 on healthcare workers: a scoping review. Int J Emerg Med. 2020;13:40.
55. Palamenghi L, Barello S, Boccia S, Graffigna G. Mistrust in biomedical research and vaccine hesitancy: the forefront challenge in the battle against COVID-19 in Italy. Eur J Epidemiol. 2020;35:785–788.
56. Aw J, Seng JJB, Seah SSY, Low LL. COVID-19 Vaccine Hesitancy-A Scoping Review of Literature in High-Income Countries. Vaccines. 2021;9:8.
57. Cascini F, Pantovic A, Al-Ajlouni Y, Failla G, Ricciardi W. Attitudes, acceptance and hesitancy among the general population worldwide to receive the COVID-19 vaccines and their contributing factors: a systematic review. EClinicalMedicine. 2021;40:101113.
58. Moola S, Gudi N, Nambiar D, et al. A rapid review of evidence on the determinants of and strategies for COVID-19 vaccine acceptance in low- and middle-income countries. J Glob Health. 2021;11:05027.
59. Robinson E, Jones A, Lesser I, Daly M. International estimates of intended uptake and refusal of COVID-19 vaccines: a rapid systematic review and meta-analysis of large nationally representative samples. Vaccine. 2021;39(15):2024–2034.
60. Yasmin F, Najeeb H, Moeed A, et al. COVID-19 Vaccine Hesitancy in the United States: a Systematic Review. Front Public Health. 2021;9:770985.
61. Williams SR. National routine adult immunisation programmes among World Health Organization Member States: an assessment of health systems to deploy COVID-19 vaccines. Eurosurveillance. 2021;26:2001195.
62. Abedin M, Islam MA, Rahman FN, et al. Willingness to vaccinate against COVID-19 among Bangladeshi adults: understanding the strategies to optimize vaccination coverage. PLoS One. 2021;16:e0250495. doi:10.1371/journal.pone.0250495
63. Huynh G, Tran TT, Nguyen HTN, Pham LA. COVID-19 vaccination intention among healthcare workers in Vietnam. Asian Pac J Trop Med. 2021;14:159–164. doi:10.4103/1995-7645.312513
64. Sallam M, Dababseh D, Yaseen A, et al. COVID-19 misinformation: mere harmless delusions or much more? A knowledge and attitude cross-sectional study among the general public residing in Jordan. PLoS One. 2020;15:e0243264.
65. Mohan S, Reagu S, Lindow S, Alabdulla M. COVID-19 vaccine hesitancy in perinatal women: a cross sectional survey. J Périnat Med. 2021;49:678–685.
66. Wang Y, Liu Y. Multilevel determinants of COVID-19 vaccination hesitancy in the United States: a rapid systematic review. Preventive Med Rep. 2021;1:101673.
67. Malik AA, McFadden SM, Elharake J, et al. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine. 2020;26:100495.
68. Ochieng C, Anand S, Mutwiri G, Szafron M, Alphonsus K. Factors Associated with COVID-19 Vaccine Hesitancy among Visible Minority Groups from a Global Context: a Scoping Review. Vaccines. 2021;9:12.
69. Assfaw YT. Determinants of Antenatal Care, Institutional Delivery and Skilled Birth Attendant Utilization in Samre Saharti District, Tigray, Ethiopia. Umeå: Umeå University; 2010.
70. Peretti-Watel P, Seror V, Cortaredona S; The COCONEL Group. A future vaccination campaign against COVID-19 at risk of vaccine hesitancy and politicization. Lancet Infect Dis. 2020;20:769–770. doi:10.1016/S1473-3099(20)30426-6
71. Sherman S, Smith L, Sim J, et al. COVID-19 vaccination intention in the UK: results from the COVID-19 Vaccination Acceptability Study (CoVAccS), a nationally representative cross-sectional. Available from: https://pubmed.ncbi.nlm.nih.gov/33242386/.
72. Paul E, Steptoe A, Fancourt D. Attitudes towards vaccines and intention to vaccinate against COVID-19: implications for public health communications. Lancet Reg Health Eur. 2021;1:100012.
73. Murphy J, Vallieres F, Bentall RP, et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat Commun. 2021;12:29.
74. Edwards B, Biddle N, Gray M, Sollis KCOVID-19. vaccine hesitancy and resistance: correlates in a nationally representative longitudinal survey of the Australian population. PLoS One. 2021;16:e0248892.
75. Ledda C. Attitudes of healthcare personnel towards vaccinations before and during the COVID-19 pandemic. Int J Environ Res Public Health. 2021;18:2703.
76. Huynh G, Tran TT, Nguyen HT, et al. COVID-19 vaccination intention among healthcare workers in Vietnam. Asian Pac J Trop Med. 2021;14:159.
77. Qattan A, Alshareef N, Alsharqi O, et al. Acceptability of a COVID-19 vaccine among healthcare workers in the Kingdom of Saudi Arabia. Front Med. 2021;8:83.
78. Fares S, Elmnyer MM, Mohamed SS. COVID-19 vaccination perception and attitude among healthcare workers in Egypt. J Prim Care Community Health. 2021;12:21501327211013303.
79. Biswas N, Mustapha T, Khubchandani J, et al. The nature and extent of COVID-19 vaccination hesitancy in healthcare workers. J Community Health. 2021;1–8.
80. Qunaibi E, Basheti I, Soudy M, et al. Hesitancy of Arab healthcare workers towards COVID-19 vaccination: a large-scale multinational study. Vaccines. 2021;9:446.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.