")
Back to Journals » Journal of Pain Research » Volume 16
Prevalence and Correlates of Depression and Anxiety in Patients with Functional Anorectal Pain
Authors Dong L , Sun T, Tong P, Guo J, Ke X
Received 3 December 2022
Accepted for publication 24 January 2023
Published 26 January 2023 Volume 2023:16 Pages 225—232
DOI https://doi.org/10.2147/JPR.S400085
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Liping Dong,1,2 Ting Sun,2 Ping Tong,2 Jia Guo,3 Xiaoyan Ke1
1Affifiliated Nanjing Brain Hospital, Nanjing Medical University, Nanjing, People’s Republic of China; 2Department of Clinical Psychology, Yangzhou University Affiliated Northern Jiangsu People’s Hospital, Yangzhou, People’s Republic of China; 3Department of Proctology of Traditional Chinese Medicine, Yangzhou University Affiliated Northern Jiangsu People’s Hospital, Yangzhou, Jiangsu, People’s Republic of China
Correspondence: Xiaoyan Ke, Child Mental Health Research Center, the Affiliated Brain Hospital of Nanjing Medical University, 264 Guangzhou Road, Nanjing, Jiangsu, 210029, People’s Republic of China, Tel +8613305176562, Fax +8602982296194, Email [email protected]
Purpose: Patients with functional anorectal pain (FAP) often experience psychological distress, impaired quality of life, increased healthcare utilisation, and even suicidal tendencies. However, limited data exists on the psychological correlates of FAP in Chinese patients. Therefore, this study aimed to examine the prevalence of depression, anxiety, and related psychosocial factors in Chinese patients with FAP.
Methods: We used a cross-sectional research design and recruited 100 patients with FAP from SuBei Hospital’s multidisciplinary clinic for pelvic floor disorders between January and December 2021. Information on patients’ demographic and disease characteristics was also collected. Depressive and anxiety symptoms were assessed using the Patient Health Questionnaire Depression (PHQ-9) and the Generalised Anxiety Disorder Questionnaire (GAD-7). Multiple logistic regression analysis was used to examine factors associated with depression and anxiety.
Results: The prevalence of depressive and anxiety symptoms among patients with FAP was 55% and 46%, respectively. Being a woman, specific marital status (single, divorced, separated, or widowed), longer FAP duration, and sleep disturbance were significantly associated with an increased risk of depressive symptoms. Additionally, specific marital status (single, divorced, separated, or widowed), sleep disturbance, and high Visual Analogue Scale scores were associated with anxiety symptoms.
Conclusion: Depressive and anxiety symptoms are prevalent in patients with FAP. Several socio-demographic and clinical predictors have been identified. There is a need for psychologists to be involved in the treatment of patients with FAP. Thus, multidisciplinary treatment may be the optimal treatment strategy.
Keywords: functional anorectal pain, depression, anxiety, multidisciplinary treatment
Introduction
Functional anorectal pain (FAP) is a non-organic idiopathic pain in the anus or rectum. This obscure disorder was first described over 100 years ago.1 Clinically, the main manifestations are discomfort, burning pain, tingling pain, and foreign body sensation. However, clinical and subsequent examinations fail to identify any pathological processes.2 Rome III, a diagnostic criterion for functional bowel disorders, classifies FAP into proctalgia fugax and chronic proctalgia.3 The prevalence of chronic proctalgia is 2% to 5%,4 while the prevalence of proctalgia fugax ranges from 8% to 18% in community studies.5 However, its actual prevalence appears to be higher.6 FAP is more common in women2,7 and is challenging to diagnose, owing to its unknown aetiology and complex symptoms. The disease has a particular lesion location and multiple complex adjacent organs, such as the urinary system, reproductive system, rectoanal canal, and pelvic floor muscle tissue,2 making treatment very difficult. Patients with FAP often experience psychological distress, such as depression and anxiety, impaired quality of life,8 increased health care utilization,9 and suicidal tendencies.10
FAP is a branch of functional gastrointestinal disease. It is well established that psychological symptoms are widespread in functional gastrointestinal diseases.11,12 A systematic review demonstrated that patients with irritable bowel syndrome (IBS) have three-fold increased probability of developing either anxiety or depression, compared with healthy individuals.13 Symptoms of psychological distress are common in IBS patients. A study reported that up to 60% of people with IBS have major psychosocial disorders, including mental or personality disorders, life stress, a history of abuse, and chronic pain behaviours.14 Depression, anxiety, and somatisation are more common in women than in men.15 However, few recent studies exist on the psychological factors involved in anorectal pain. This suggests that clinicians do not pay sufficient attention to the psychological problems associated with anorectal pain. Furthermore, this may be a possible factor in poor treatment response to the disease.
Therefore, this study aimed to investigate the prevalence of, and factors associated with depression and anxiety in Chinese outpatients with FAP. To the best of our knowledge, this is the first study to investigate the prevalence of and factors associated with depression and anxiety in patients with FAP.
Materials and Methods
Methods
This cross-sectional study explored the prevalence and correlates of depression and anxiety among patients with FAP. The study was conducted at the SuBei Hospital’s multidisciplinary clinic for pelvic floor disorders between January and December 2021. A total of 100 outpatients with FAP were enrolled in the study.
Participants
The inclusion criteria were as follows: (1) all patients older than 18 years who met the Rome III diagnostic criteria for FAP; (2) having a FAP diagnosis based on anal finger examination, perianal ultrasound, colonoscopy, and pelvic MRI; (3) no apparent cognitive dysfunction; and (4) consenting to participate in the study.
The exclusion criteria were: (1) patients with anal fissures, anal fistulas, complicated haemorrhoids, perianal abscesses, or tumours; (2) patients with different associated organic diseases (including known spinal lesions and primary nervous system disease); and (3) under 18 years of age.
This study was approved by the Ethics Committee of Subei Hospital and was performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants before enrolment.
Questionnaire
Information on patients’ demographic and disease characteristics (including age, sex, marital status, level of education, monthly income, job status, smoking, alcohol consumption, and sleep disturbances) was collected. Disease characteristics included the following: disease duration of FAP and history of anal surgery.
Depressive symptoms were assessed using the Patient Health Questionnaire Depression (PHQ-9), a convenient and effective tool for detecting depressive symptoms.16 The PHQ-9 includes nine questions, each of which can be scored from 0 to 3. The total score ranged from 0 to 27, and patients with a score ≥ 5 were identified as having depressive symptoms.17 Anxiety symptoms were assessed using the Generalized Anxiety Disorder Questionnaire (GAD-7).18 The GAD-7 includes seven questions, each of which can be scored from 0 to 3. The total score ranged from 0 to 21, and patients with a score ≥ 5 were identified as having anxiety symptoms.17
All participants completed a 10 cm Visual Analogue Scale (VAS) to evaluate pain intensity. The VAS score ranged from 0 (“absence of symptom”) to 10 (“maximum intensity of symptoms”).
Statistical Analysis
Demographic data were expressed in terms of frequency and percentages. Participants were grouped according to the presence of depression or anxiety. Chi-square tests were used for categorical variables, while t-tests were used for continuous variables. Multivariate logistic regression was used to identify the participants’ characteristics associated with depressive or anxiety symptoms. The odds ratios and 95% confidence intervals were estimated. All data were analysed using SPSS software (version 26.0; SPSS, Inc., Chicago, IL, USA). Statistical significance was set at p < 0.05.
Results
Demographic and Clinical Characteristics of Study Participants
A total of 100 patients with FAP were recruited during data collection. Of these, 55 participants (55.0%) had depressive symptoms and 46 participants (46.0%) had anxiety symptoms.
In the present study, 41% of participants were 40–59 years old, while 33% of participants were older than 60 years. Most of the participants were women (77%), married (81.0%), and employed (55.0%). Additionally, a minority of participants reported having a low level of education (42%), a low monthly income (30%), and sleep disturbances (42.0%). Nearly 87% of the participants were non-smokers and 90% were non-drinkers. Moreover, 67% of the participants had a long disease duration (> three months), and 11% had a history of anal surgery. The mean VAS score of the participants was 3.70 (SD = 2.51) (Table 1).
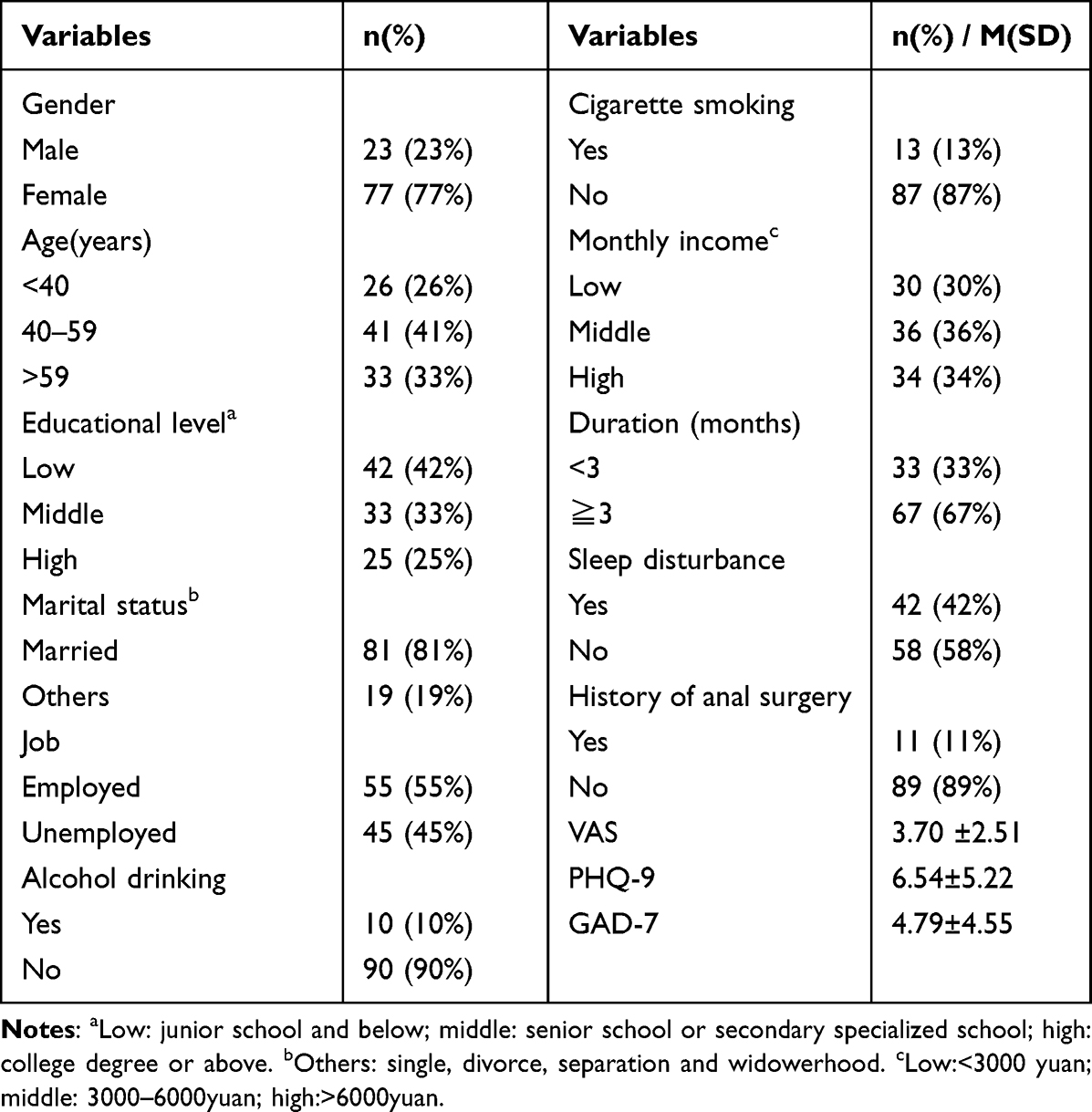 |
Table 1 Demographic and Disease Characteristics of Participants (n = 100) |
Univariate Analysis
Univariate analysis showed that being a woman, low educational level, specific marital status (single, divorced, separated, or widowed), disease duration, alcohol consumption, and sleep disturbance were significantly related to depression symptoms. Additionally, in the univariate analysis, female sex, poor marital status, sleep disturbances, and high VAS scores were associated with anxiety symptoms. The additional details are provided in Table 2.
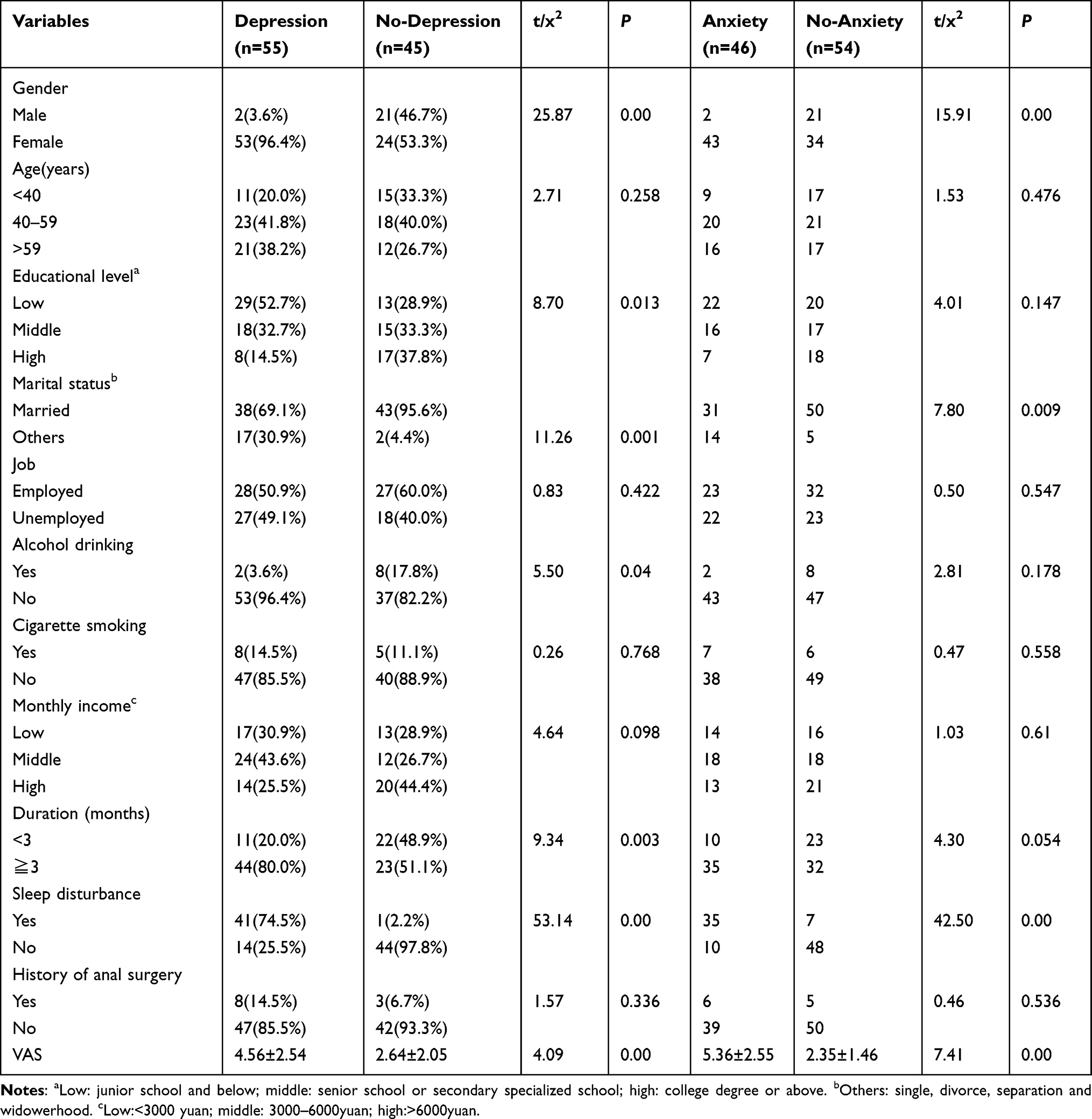 |
Table 2 Univariate Analysis of Risk Factors for Depressive and Anxiety Symptoms |
Multivariate Logistic Regression Analysis
The risk factors for depressive symptoms were assessed by multiple logistic regression analyses. As shown in Table 3, independent predictors of depressive symptoms included female sex, poor marital status, longer disease duration, and sleep disturbances. In addition, being married, shorter disease duration, and having good sleep quality could lower the risk of depression.
 |
Table 3 Multiple Logistic Regression Analysis of Risk Factors for Depressive Symptoms |
Multiple logistic regression analysis also identified marital status, sleep disturbances, and higher VAS scores as positive predictors of anxiety symptoms. Good sleep quality and lower VAS scores were negative (protective) factors (Table 4).
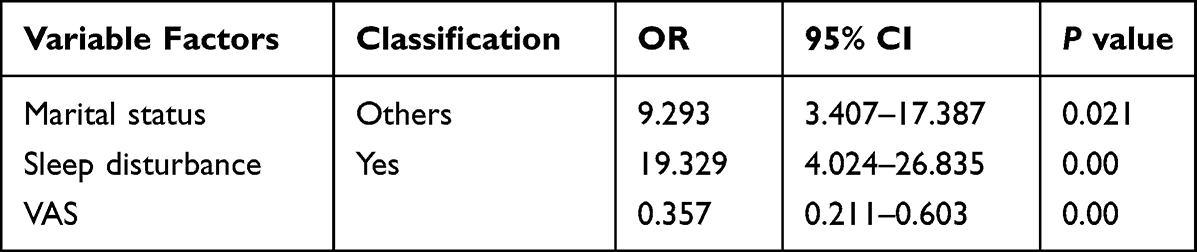 |
Table 4 Multiple Logistic Regression Analysis of Risk Factors for Anxiety Symptoms |
Discussion
In the present study, 55% of the patients with FAP were screened positively for depressive symptoms using the PHQ-9, whereas 46% of the patients with FAP were screened positively for anxiety symptoms using the GAD-7. These findings indicate that depressive and anxiety symptoms are common among patients with FAP. To date, inadequate attention has been paid to depressive and anxiety symptoms in anorectal clinics, and comparative studies have been scarce. A study reported that the prevalence of depression and anxiety was 25% and 73%, respectively, using a 63-item checklist devised by one of the authors.19 A recent study using the Beck Depression Inventory and State and Trait Anxiety Inventory in the Chinese population revealed that 92.7% of patients with chronic idiopathic anal pain reported symptoms of psychological disturbance.20 The results of our study were different from those of the aforementioned studies, which may be related to the different sample sizes, research objectives, and applicable assessment tools. Furthermore, we found that female participants were more likely to have depressive and anxiety symptoms than male participants. This was consistent with previous reports,20 indicating that there may be a sex difference in depression and anxiety in patients with FAP. Although symptoms of depression and anxiety are widespread in such patients, very few receive antidepressant or anxiolytic treatment. One possible reason for not receiving treatment was that patients and clinicians erroneously believed it was normal to feel depressed or anxious when suffering from the disease.21 Another possible cause is social stigma. Many people consider it shameful to receive psychological treatment in China.
Regarding sex, being a woman was significantly associated with depression and anxiety. Generally, depression, anxiety, and somatisation are more common in women than in men.15 A study of functional gastrointestinal disorders showed that, compared with healthy control patients, IBS patients were approximately three times more likely to have anxiety, which was more common in women than in men.13 Biological factors may have contributed to these differences. Sex-related differences in the prevalence of depression first appear after menarche and continue until perimenopause.22 There is also evidence that affective symptoms, such as depression, may be influenced by changes in ovarian hormone levels.23 However, the exact underlying mechanism remains unclear.
This study revealed that individuals with sleep disturbances were more likely to exhibit depressive and anxiety symptoms than those without sleep disturbances. Despite the paucity of findings on the relationship between sleep disturbances and depression/anxiety among patients with FAP, this finding is consistent with the theory that insomnia is associated with the risk of depression in the general population.24 A previous meta-analysis provided evidence that insomnia increased the risk of psychopathology and suggested that insomnia was a significant predictor of the onset of depression, anxiety, and other mental disorders.25 A study of an elderly population documented that depressive symptoms were uniquely related to higher levels of daytime dysfunction. In contrast, anxiety symptoms were related to decreased sleep quality and increased sleep latency.26 Moreover, previous studies established a bidirectional relationship between sleep problems and depression. Specifically, people with insomnia are at an increased risk of depression, and sleep disturbances are common in depressed patients.27 Our results suggest that sleep disturbances may be an essential predictor of depressive and anxiety symptoms in patients with FAP. Furthermore, improving sleep problems in patients with FAP may be clinically significant.
We found that patients who had FAP for more than three months were significantly more likely to develop depressive symptoms. Chronic pain is considered pain expected to persist for more than one month after tissue healing or for at least three of the first six months of the healing process.28 Chronic pain and depression are frequently comorbid.29 Major depression (MDD) is the most common mental disorder associated with chronic pain. The prevalence of major depression is 30 to 40% among patients with chronic pain requiring treatment.30 The daily challenges of chronic pain often include reduced enjoyment of everyday activities, loss of function, role changes, and relationship difficulties.31 Uncertainty regarding the absence of pain or the possibility of worsening pain is accompanied by feelings of anxiety, depression and anger.32 Several mechanisms may explain the association between depression and anxiety and chronic pain. One possible explanation is that the positive correlation between depression and pain is mediated by many factors, including general somatization tendencies.33
Depression and anxiety were significantly higher among participants who were single, divorced, unmarried, and widowed, than among participants who were married. Marital status is a key social factor that affects depression and anxiety. One study examined whether marital functioning variables were related to psychological distress and chronic pain. The results showed that marital variables contributed significantly to depressive and anxiety symptoms, pain severity and physical disability.34 Previous research has repeatedly shown that married people have better mental health than single, separated, widowed or divorced people.35,36 Being married is a protective factor for depression, which is seen in Western and Asian populations.37 The results of the present study are consistent with these results.
This study also found that a high VAS score was significantly associated with an increased anxiety risk. In other words, pain intensity was associated with anxiety symptoms. A study of Latinx young adults showed that greater pain intensity was related to increased pain-related anxiety.38 Furthermore, a bidirectional relationship may exist between pain and stress. Pain has been shown to lead to anxiety, which can enhance pain.39 Previous experimental results have shown that those with higher trait anxiety responded to painful stimuli significantly with increased pain intensity and anxiety levels. In contrast, increased state anxiety led to higher pain scores among participants.40 A longitudinal study reported that a reduction in depression and anxiety significantly predicted a reduction in pain intensity during a graded telehealth intervention for chronic musculoskeletal pain.41 Our results suggest that alleviating anxiety symptoms may clinically alleviate pain in patients.
There are several limitations to this study. First, the cross-sectional design can only demonstrate associations between variables and depressive and anxiety symptoms, and no causal inferences can be made among the studied outcome variables. Second, the application of self-made scales may lead to social desirability and reporting biases, resulting in under- or over-reporting of actual conditions. Third, the sample size was not large enough and the samples were limited to one hospital, so the factors influencing clinical correlates were not sufficiently comprehensive. Multi-center and large sample studies are needed in the future.
Conclusion
This study explored the prevalence of depressive and anxiety symptoms among patients with FAP. Our findings indicate that depressive and anxiety symptoms are common among patients with FAP. We also investigated the related risk factors. Female sex, poor marital status, longer disease duration, and sleep disturbances were significantly associated with an increased risk of depressive symptoms. Additionally, specific marital status (single, divorced, separated or widowed), sleep disturbances, and high VAS scores were associated with anxiety symptoms. FAP is a complex disease. Symptoms of depression and anxiety are prevalent in patients with FAP. Clinicians should pay attention to psychological problems in patients with FAP. There is a need for psychologists to be involved in the treatment of patients with FAP. Multidisciplinary treatment may be a better treatment way. Our future research direction will focus on the effect of multidisciplinary team intervention on the treatment of patients with FAP.
Ethics Approval
Ethical approval was obtained by the Ethics Committee of SuBei Hospital. All participants gave written informed consent to participate in the study.
Acknowledgments
We would like to thank the study participants and all staff members involved in this study for their efforts in the data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Thompson WG. Proctalgia fugax. Dig Dis Sci. 1981;26(12):1121–1124. doi:10.1007/BF01295979
2. Atkin GK, Suliman A, Vaizey CJ. Patient characteristics and treatment outcome in functional anorectal pain. Dis Colon Rectum. 2011;54(7):870–875. doi:10.1007/DCR.0b013e318217586f
3. Ke MY, Zhao W. Application of Rome III diagnostic criteria on functional gastrointestinal disorders. Zhonghua Yi Xue Za Zhi. 2009;89(14):937–938.
4. Rao SS, Paulson J, Mata M, et al. Clinical trial: effects of botulinum toxin on Levator ani syndrome--a double-blind, placebo-controlled study. Aliment Pharmacol Ther. 2009;29(9):985–991. doi:10.1111/j.1365-2036.2009.03964.x
5. Drossman DA, Li Z, Andruzzi E, et al. U.S. householder survey of functional gastrointestinal disorders. Prevalence, sociodemography, and health impact. Dig Dis Sci. 1993;38(9):1569–1580. doi:10.1007/BF01303162
6. Bharucha AE, Wald A, Enck P, et al. Functional anorectal disorders. Gastroenterology. 2006;130(5):1510–1518. doi:10.1053/j.gastro.2005.11.064
7. Christiansen J. Chronic idiopathic anal pain. Eur J Surg. 1998;164(2):83–88. doi:10.1080/110241598750004724
8. Heymen S, Wexner SD, Gulledge AD. MMPI assessment of patients with functional bowel disorders. Dis Colon Rectum. 1993;36(6):593–596. doi:10.1007/BF02049867
9. Bharucha AE, Lee TH. Anorectal and pelvic pain. Mayo Clin Proc. 2016;91(10):1471–1486. doi:10.1016/j.mayocp.2016.08.011
10. Rao SS, Bharucha AE, Chiarioni G, et al. Functional anorectal disorders. Gastroenterology. 2016;150:1430–1442.e4. doi:10.1053/j.gastro.2016.02.009
11. Bulut Çakmak B, Özkula G, Işıklı S, et al. Anxiety, depression, and anger in functional gastrointestinal disorders: a Cross-sectional observational study. Psychiatry Res. 2018;268:368–372. doi:10.1016/j.psychres.2018.06.046
12. Ballenger JC, Davidson JR, Lecrubier Y, et al. Consensus statement on depression, anxiety, and functional gastrointestinal disorders. J Clin Psychiatry. 2001;62(Suppl 8):48–51.
13. Zamani M, Alizadeh-Tabari S, Zamani V. Systematic review with meta-analysis: the prevalence of anxiety and depression in patients with irritable bowel syndrome. Aliment Pharmacol Ther. 2019;50(2):132–143. doi:10.1111/apt.15325
14. Drossman DA, McKee DC, Sandler RS, et al. Psychosocial factors in the irritable bowel syndrome. A multivariate study of patients and nonpatients with irritable bowel syndrome. Gastroenterology. 1988;95(3):701–708. doi:10.1016/s0016-5085(88)80017-9
15. Blanchard EB, Keefer L, Galovski TE, et al. Gender differences in psychological distress among patients with irritable bowel syndrome. J Psychosom Res. 2001;50(5):271–275. doi:10.1016/s0022-3999(01)00207-0
16. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
17. Li Z, Hao Y, Han Y, et al. Prevalence and associated physical symptoms of depressive and anxiety symptoms in neurology outpatient clinic. J Neurol Neurosurg Psychiatry. 2019;90(11):1286–1287. doi:10.1136/jnnp-2018-320130
18. Spitzer RL, Kroenke K, Williams JB, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
19. Pilling LF, Swenson WM, Hill JR. The psychologic aspects of proctalgia fugax. Dis Colon Rectum. 1965;8(5):372–376. doi:10.1007/BF02627263
20. Mao W, Liao X, Wu W, et al. The clinical characteristics of patients with chronic idiopathic anal pain. Open Med. 2017;12:92–98. doi:10.1515/med-2017-0015
21. Kanner AM, Barry JJ. Barry JJ The impact of mood disorders in neurological diseases: should neurologists be concerned. Epilepsy Behav. 2003;4(Suppl 3):S3–13. doi:10.1016/j.yebeh.2003.08.018
22. Halbreich U, Kahn LS. Role of estrogen in the aetiology and treatment of mood disorders. CNS Drugs. 2001;15(10):797–817. doi:10.2165/00023210-200115100-00005
23. Oinonen KA, Mazmanian D. Mazmanian D Effects of oral contraceptives on daily self-ratings of positive and negative affect. J Psychosom Res. 2001;51(5):647–658. doi:10.1016/s0022-3999(01)00240-9
24. Neckelmann D, Mykletun A, Dahl AA. Dahl AA Chronic insomnia as a risk factor for developing anxiety and depression. Sleep. 2007;30(7):873–880. doi:10.1093/sleep/30.7.873
25. Hertenstein E, Feige B, Gmeiner T, et al. Insomnia as a predictor of mental disorders: a systematic review and meta-analysis. Sleep Med Rev. 2019;43:96–105. doi:10.1016/j.smrv.2018.10.006
26. Yu J, Rawtaer I, Fam J, et al. Sleep correlates of depression and anxiety in an elderly Asian population. Psychogeriatrics. 2016;16(3):191–195. doi:10.1111/psyg.12138
27. Benca RM, Peterson MJ. Insomnia and depression. Sleep Med. 2008;9(Suppl 1):S3–9. doi:10.1016/S1389-9457(08)70010-8
28. Blyth FM, March LM, Brnabic AJ, et al. Chronic pain in Australia: a prevalence study. Pain. 2001;89(2–3):127–134. doi:10.1016/s0304-3959(00)00355-9
29. Bair MJ, Robinson RL, Katon W, et al. Depression and pain comorbidity: a literature review. Arch Intern Med. 2003;163(20):2433–2445. doi:10.1001/archinte.163.20.2433
30. Tyrer S. Psychiatric assessment of chronic pain. Br J Psychiatry. 1992;160:733–741. doi:10.1192/bjp.160.6.733
31. Levenson J. Textbook of Psychosomatic Medicine. Washington, DC: American Psychiatric Publishing; 2005.
32. Holmes A, Christelis N, Arnold C. Depression and chronic pain. Med J Aust. 2013;199(S6):S17–20. doi:10.5694/mja12.10589
33. Lerman SF, Rudich Z, Brill S, et al. Longitudinal associations between depression, anxiety, pain, and pain-related disability in chronic pain patients. Psychosom Med. 2015;77(3):333–341. doi:10.1097/PSY.0000000000000158
34. Cano A, Gillis M, Heinz W, et al. Marital functioning, chronic pain, and psychological distress. Pain. 2004;107(1–2):99–106. doi:10.1016/j.pain.2003.10.003
35. Jang SN, Kawachi I, Chang J, et al. Marital status, gender, and depression: analysis of the baseline survey of the Korean Longitudinal Study of Ageing (KLoSA). Soc Sci Med. 2009;69(11):1608–1615. doi:10.1016/j.socscimed.2009.09.007
36. Bulloch AG, Williams JV, Lavorato DH, et al. The relationship between major depression and marital disruption is bidirectional. Depress Anxiety. 2009;26(12):1172–1177. doi:10.1002/da.20618
37. Inaba A, Thoits PA, Ueno K, et al. Depression in the United States and Japan: gender, marital status, and SES patterns. Soc Sci Med. 2005;61(11):2280–2292. doi:10.1016/j.socscimed.2005.07.014
38. Zvolensky MJ, Kauffman BY, Shepherd JM, et al. Pain intensity, pain-related anxiety, and somatic and mental health symptoms: a test among latinx young adults. Psychol Health Med. 2021;26(3):289–297. doi:10.1080/13548506.2020.1764598
39. Koga K, Descalzi G, Chen T, et al. Coexistence of two forms of LTP in ACC provides a synaptic mechanism for the interactions between anxiety and chronic pain. Neuron. 2015;86(4):1109. doi:10.1016/j.neuron.2015.05.016
40. Tang J, Gibson SJ. A psychophysical evaluation of the relationship between trait anxiety, pain perception, and induced state anxiety. J Pain. 2005;6(9):612–619. doi:10.1016/j.jpain.2005.03.009
41. Scott EL, Kroenke K, Wu J, et al. Beneficial effects of improvement in depression, pain catastrophizing, and anxiety on pain outcomes: a 12-month longitudinal analysis. J Pain. 2016;17(2):215–222. doi:10.1016/j.jpain.2015.10.011
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.