")
Back to Journals » Nutrition and Dietary Supplements » Volume 12
Prevalence and Associated Factors of Stunting Among Children Aged 6–59 Months in Delanta District; North East Ethiopia
Authors Tadesse SE , Mekonnen TC
Received 5 November 2019
Accepted for publication 15 February 2020
Published 25 February 2020 Volume 2020:12 Pages 41—48
DOI https://doi.org/10.2147/NDS.S237407
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gary Johanning
Sisay Eshete Tadesse, Tefera Chane Mekonnen
Department of Public Health, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia
Correspondence: Sisay Eshete Tadesse Email [email protected]
Background: Under-nutrition among under-five children is a global public health problem. Sub-Saharan Africa and South Asia were the home for three-fourth of the world’s stunted children. There is a disparity in the prevalence and associated factors of under-nutrition across regions and cities.
Objective: To assess the prevalence and associated factors of stunting among children 6– 59 months in Delanta district.
Methods: A community-based cross-sectional study design was conducted among 342 systematically selected children aged 6– 59 months from April to May 2017 G.C. The sample size was calculated by single population proportion formula. Data were collected by a structured questionnaire, SECA weight measurement, and height measuring board. After collection, data were entered into Epi data version 3.1 for cleaning and transferred to SPSS version 24.0 for analysis. Anthropometric data were analyzed using WHO Anthro 2005 software. Descriptive statistics were done and the result was reported by frequency, percentile, and mean ± standard deviation. Variables having a p-value < 0.25 in bivariable binary logistic regression were transported to multivariable binary logistic regression to identify factors associated with stunting. In multivariable model, the statistical significance was declared by using adjusted odds ratio with 95% confidence interval and a p-value < 0.05.
Results: The mean age of the study participants was 25.12± 15.45 months. The prevalence of stunting was 22.1% (95% CI: 17.6, 26.5). Late initiation of breastfeeding (AOR=2.4; 95% CI: 1.2, 4.9), postnatal care (AOR=0.3, 95% CI: 0.1, 0.9), and repeated episodes of respiratory infection (AOR=4.9; 95% CI: 1.8, 12.8) were factors associated with stunting.
Conclusion and Recommendation: Stunting is a moderate public health problem. Late initiations of breastfeeding, not attending postnatal care and repeated respiratory infection were factors associated with stunting. So, strengthening implementation of baby-friendly hospital initiatives, strengthening of postnatal care service utilization and prevention and control of respiratory infection should be included in the prevention strategies of stunting.
Keywords: prevalence, stunting, associated factors, cross-sectional, Ethiopia and Delanta
Introduction
Under-nutrition is a condition which results from inadequate intake of one or more essential nutrients. Stunting is one of the three main indicators used to define under nutrition in under five children. It is a measure of chronic malnutrition and measured by length/height for age. It is a global public health challenge affecting 155 million under-five children.1 Africa region was the major contributor for stunted children for the globe, which accounts 59 million (37%). The trend in Africa region is increasing since 1990.2 In sub-Saharan Africa, annually more than 30% of under-five mortality is associated with under-nutrition.3 Stunting in early childhood is associated with impaired cognitive development, reduced school attainment, productivity loss, impaired reproductive performance and increased susceptibility to metabolic and cardiovascular diseases in later life.4–6 Young children who were stunted were 33% less likely to escape poverty.7 This consequence will result 4% to 11% of overall GDP losses in Africa and Asia.2
Stunting is a result of multifaceted interactions between various factors like chronic insufficient protein and energy intake, intrauterine growth retardation, lack of exclusive breastfeeding, inappropriate complementary feeding practices, short maternal stature, restricted fetal growth, frequent infection, food insecurity, water sanitation and hygiene, socio-demographic and economic factors.8–10
The World Health Assembly adopted a new target to reduce the number of stunted children under the age of 5 years by 40% in 2025. The Federal Government of Ethiopia has been working to reduce stunting to 26% by 2020. The most critical time to reduce childhood stunting is during 1000 days, from pregnancy to the end of a child second birthday. During this time, the child has increased nutritional needs to support rapid growth and development, is more susceptible to infections, sensitivity to biological programming and is totally dependent on others for nutrition, care, and social interactions. So this period is essential to intervene on creating stunting free generation.5,6
Although Ethiopia has achieved a remarkable reduction in under-five mortality in the last two decades, stunting is still a serious public health problem including the globe.11 Amhara regional state was the frontline contributor for the highest prevalence of stunting in Ethiopia. The annual reduction rate of stunting in the country is 2.3% which is below the target, i.e. 4.4%. This indicates as there is a broken bridge which hinders the pace rate of stunting reduction. Regardless of searching effort, there is limited evidence in the study area on the prevalence and contributing factors of stunting among 6–59 months old children. Therefore, the aim of this study was to assess the prevalence and associated factors of stunting among 6–59 months old children in Delanta district.
Methods and Materials
Study Design, Area, Period, Population, and Eligibility Criteria
A community-based cross-sectional study design was conducted among mother/caregivers that had 6–59 months old children who have been living in the selected Kebeles of Delanta district from April to May 2017. The district is found 494 km away from Addis Ababa, the capital of Ethiopia and about 312 km far from the capital of Amhara national regional state, Bahir Dar. It has 34 Kebeles and a total population of 143,881. Of these 70,253 (48.8%) were males and 71,756 (51.2%) were females. In the district, there are 19,481 under-five children. Mother/caregivers who were unable to communicate due to illness and children with physical deformity were excluded from the study.
Sample Size Calculation and Sampling Techniques
Single population proportion formula was used to determine the sample size. The sample size was calculated by considering the following assumptions; 95% confidence interval, 5% margin of error and prevalence of stunting (28.2%).12 Therefore, after adding 10% non-response rate, the total sample size was 342.
From the total 34 Kebeles, 10 were randomly selected and included in the study. Number of study participants was assigned to each selected Kebele proportional to their population size. Then, the study participants were included in the study using systematic sampling technique. The first study participant was selected by lottery method. Then, study participants were included in the study following the Kth value, i.e. every 8th child was included in the study.
Operational/Standard Definition
Stunted: a child was classified as stunted when his/her length/height-for-age Z score of <−2SD of the WHO Growth Standard chart.13
Not stunted: a child was classified as not-stunted when his/her length/height-for-age Z score of ≥−2SD of the WHO Growth Standard chart.13
Data Collection Methods
Data were collected by face to face interview using a structured questionnaire and observational checklist adapted from previous relevant literatures. Three groups of participants’ characteristics were gathered, namely socio-demographic and economic (Maternal age, marital status, maternal education, maternal occupation, family size, family income, age of child and sex of child), health-care related factors (birth spacing, antenatal care, place of delivery, postnatal care, immunization, and childhood illness), child feeding practice (ever breastfeeding, early initiation of breastfeeding, colostrum feeding, duration of exclusive breastfeeding, timely initiation of complementary feeding and frequency of feeding), and WASH (sources of drinking water, presence of toilets, hand washing at critical times and solid waste disposal) related factors.
For children aged 6–24 months, length was measured in a recumbent position to the nearest 0.1 cm using a standard lying board with a detachable sliding foot piece and weight was measured to the nearest 10 gm. While for children aged 25–59 months, height was measured in a standing position to the nearest 0.1 cm using a standard vertical board with a detachable sliding headpiece. Height of mother/caregivers was measured in a standing position to the nearest 0.1 cm using a standard vertical board with a detachable sliding headpiece. Weight of mother/caregivers was measured. Six BSc nurses and two health officers were participated in the data collection.
Data Quality Assurance
The questionnaire was translated to Amharic and retranslated back to English for consistency. Pre-test was conducted on 5% of the sample size at Kutaber district. Two-day training was given for data collectors and a supervisor on the overall data collection procedure. On spot supervision was made to check and correct incomplete questionnaire. The overall data collection process was controlled by the principal investigator. The child height and weight were measured without shoes, hats, and hair ornaments. During measurement, their occipital, shoulders, buttocks, and heels were touched with the vertical surface of the stadiometer. Weight was measured using SECA, model 874102159, serial number 5874269114011 weight measurement scale. The scale was made zero for each measurement.
Data Analysis
After coding the data were entered into Epi Data version 3.1 for cleaning and exported to SPSS version 20.0 and WHO Anthro 2005 software for analysis. Anthropometric data were analyzed by using WHO Anthro 2005. Descriptive statistics were computed and the result was reported using mean ± standard deviation, tables, graphs, frequencies, and percentages. Then, bivariable binary logistic regression was performed and variables with p<0.25 were transported to multivariable logistic regression to identify factors associated with stunting among children aged 6–59 months. Finally, multivariable binary logistic regression model was done to identify factors associated with stunting. A p-value<0.05 and adjusted odds ratio with its 95% confidence interval were used to declare the statistically significant associations.
Ethical Clearance
Ethical clearance was obtained from College of Medicine and health sciences, Wollo University. Letter of permission was obtained from Delanta district health office and selected Kebeles. This study was conducted in accordance with the Helsinki Declaration and written informed consent was obtained from mother/caregivers. Participants were informed as participation was on a voluntary basis. The data collection procedure was anonymous for keeping the confidentiality of any information. Those mother/caregivers with malnourished children were counseled and linked to outpatient therapeutic feeding and safety net program.
Result
Socio-Demographic and Economic Factors
A total of 336 mother/caregivers with their children were included in the study, making a response rate of 98.2%. Slightly more than two-third 236 (70.2%) of them were rural residents. Three-fourth 253 (75.3%) of mothers/caregivers was housewife. Two hundred sixty-six (79.2%) of mother/caregivers were married. The mean age of children was 25.12±15.45 months. Regarding their sex, 173 (51.5%) were male while the rest (48.5%) were females (Table 1).
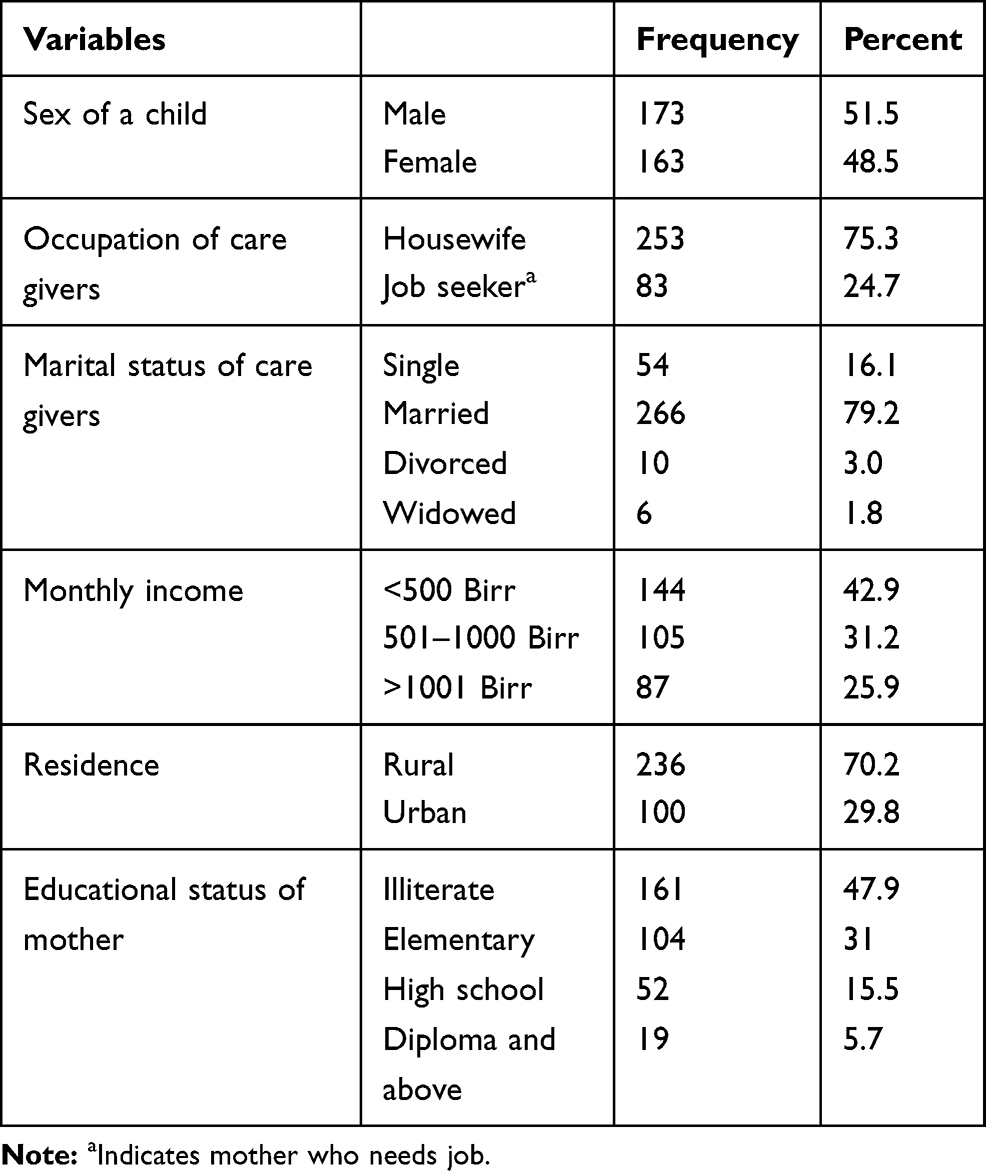 |
Table 1 Socio-Demographic and Economic Characteristics of Study Population, Delanta District, 2017 |
Health-Related Factors
One hundred forty (41.7%) of mother/caregivers practiced birth spacing. Three-fourth of 258 (76.8%) of the respondents were attended antenatal care follow-up. Only one-third 111 (33%) of mother/caregivers were delivered at health facility. More than three-fourth 267 (79.5%) of under five children were found on the right track of immunization. With respect to infection, slightly higher than one-third 123 (36.6%) of 6–59 months old children were not affected by infection in the last 2 weeks (Table 2).
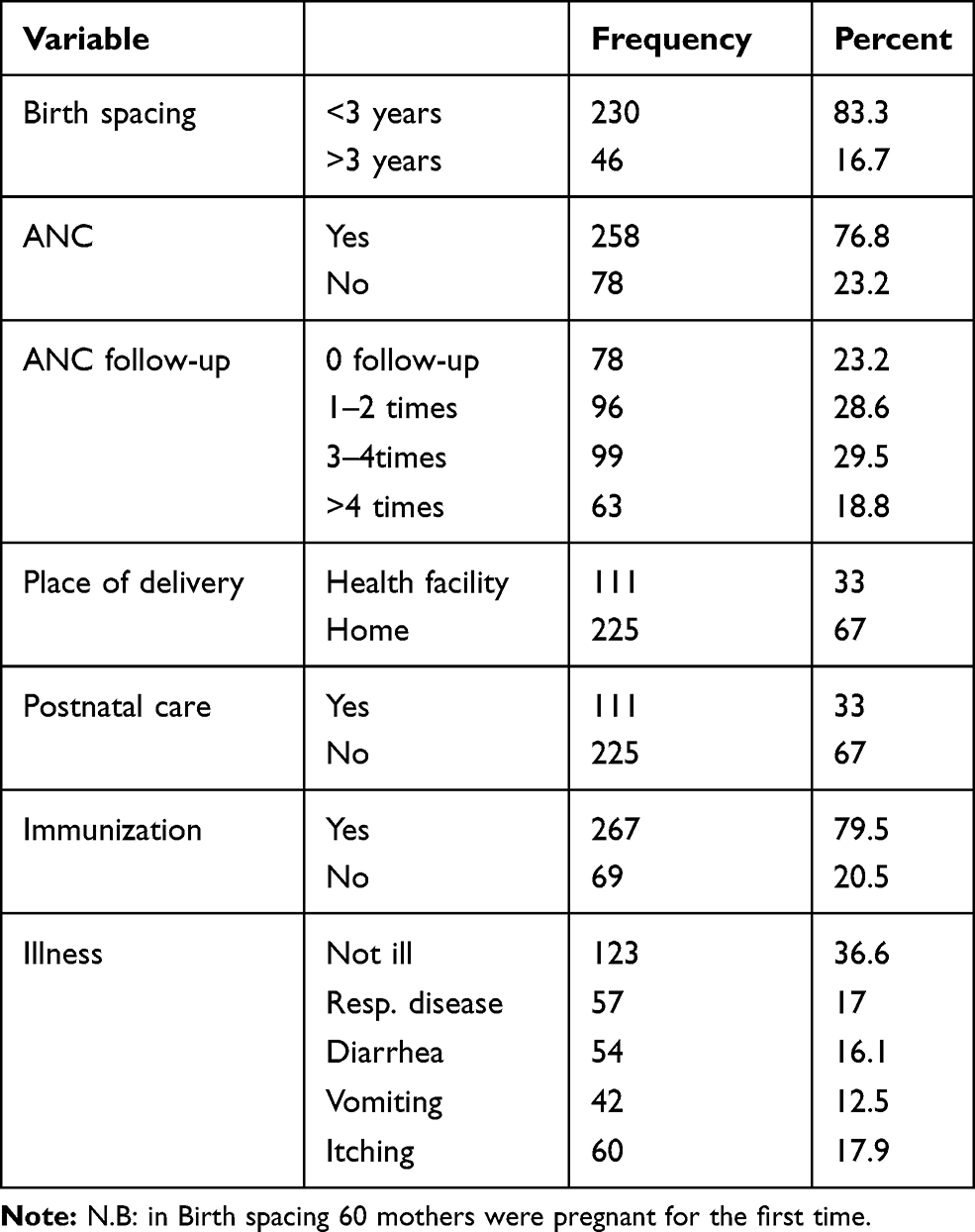 |
Table 2 Health-Care Related Factors of Stunting Among Children Aged 5–59 Months, Delanta District, 2017 |
Child Feeding Practices
More than half 188 (56.2%) of mother/caregivers initiated breastfeeding within 1 hr after birth. Slightly lower than one-third 106 (31.5%) of mother/caregivers practiced prelacteal feeding. The mean frequency of breastfeeding per day was 8.5±1.9. About 312 (92.9%) of mother/caregivers start complementary feeding exactly at 6 months of age, while 30 (8.9%) mother/caregivers initiate complementary food beyond 6 months (Table 3).
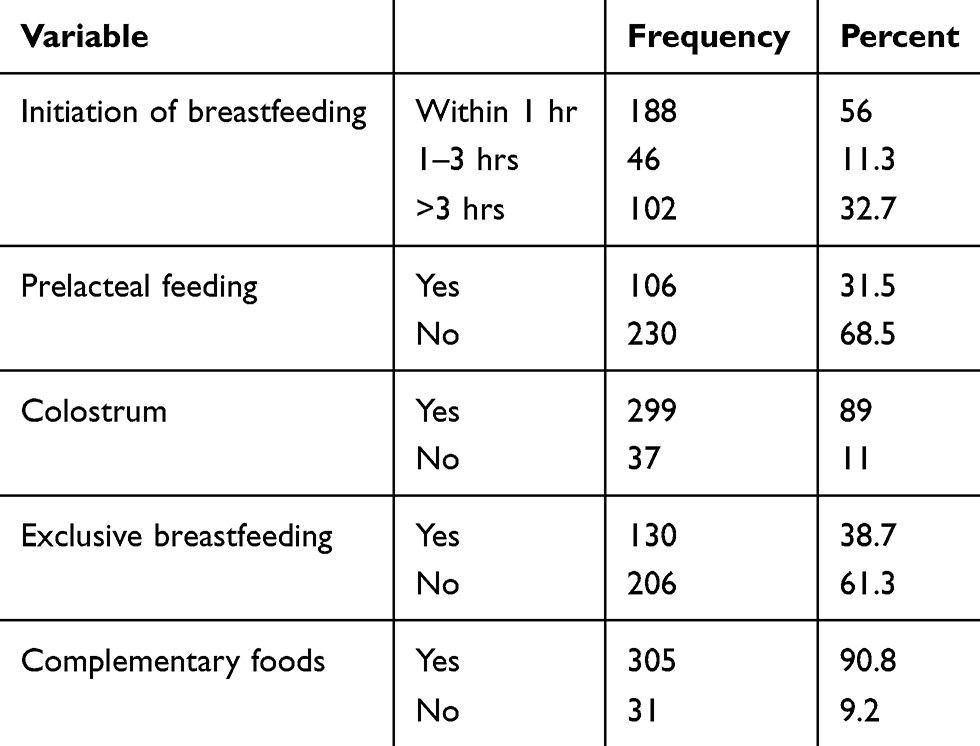 |
Table 3 Infant and Young Child Feeding Practices of Children Aged 6–59 Months, Delanta District, 2018 |
Prevalence of Stunting
The overall prevalence of stunting among children aged 6–59 months in Delanta district was 22.1% (95% CI: 17.6, 26.3). Among this, about 12.1% (95% CI: 9.1, 16.3) were moderately stunted while 8.6% (95% CI: 5.7, 11.8) were severely stunted (Figure 1).
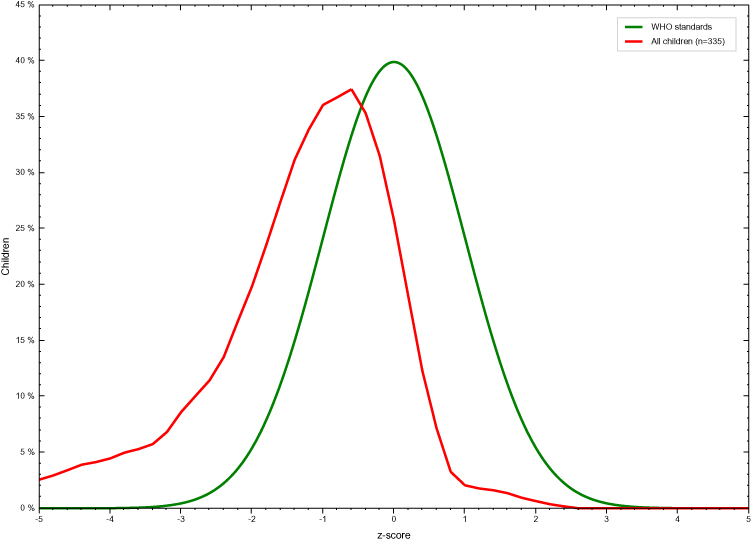 |
Figure 1 Length/Height for age distribution among 6–59 months old children in Delanta district, North East Ethiopia, 2017 G.C. |
The prevalence of stunting was higher among boys 28.3% (95% CI: 21.6, 35.0) than girls 15.4% (95% CI: 9.9–21.0) (Figure 2).
 |
Figure 2 Length/Height for age distribution by sex among 6–59 months old children in Delanta Woreda, North East Ethiopia, 2017 G.C. |
Factors Associated with Stunting Among Children Aged 6–59 Months Old
The result of multivariable logistic regression model showed that children who initiated breastfeeding more than 3 hrs after delivery were almost 2 times more likely to be stunted as compared to those children who initiated breastfeeding within 1 hr after delivery (AOR=2.4; 95% CI: 1.2, 4.9). Those mother/caregivers who follow postnatal care were 70% less likely to have stunted child as compared to those who did not follow postnatal care (AOR=0.3, 95% CI: 0.1, 0.8). Children who were repeatedly affected by respiratory infection were almost five times more likely to become stunted as compared to those children who were not ill (AOR=4.9; 95% CI: 1.8, 12.8) (Table 4).
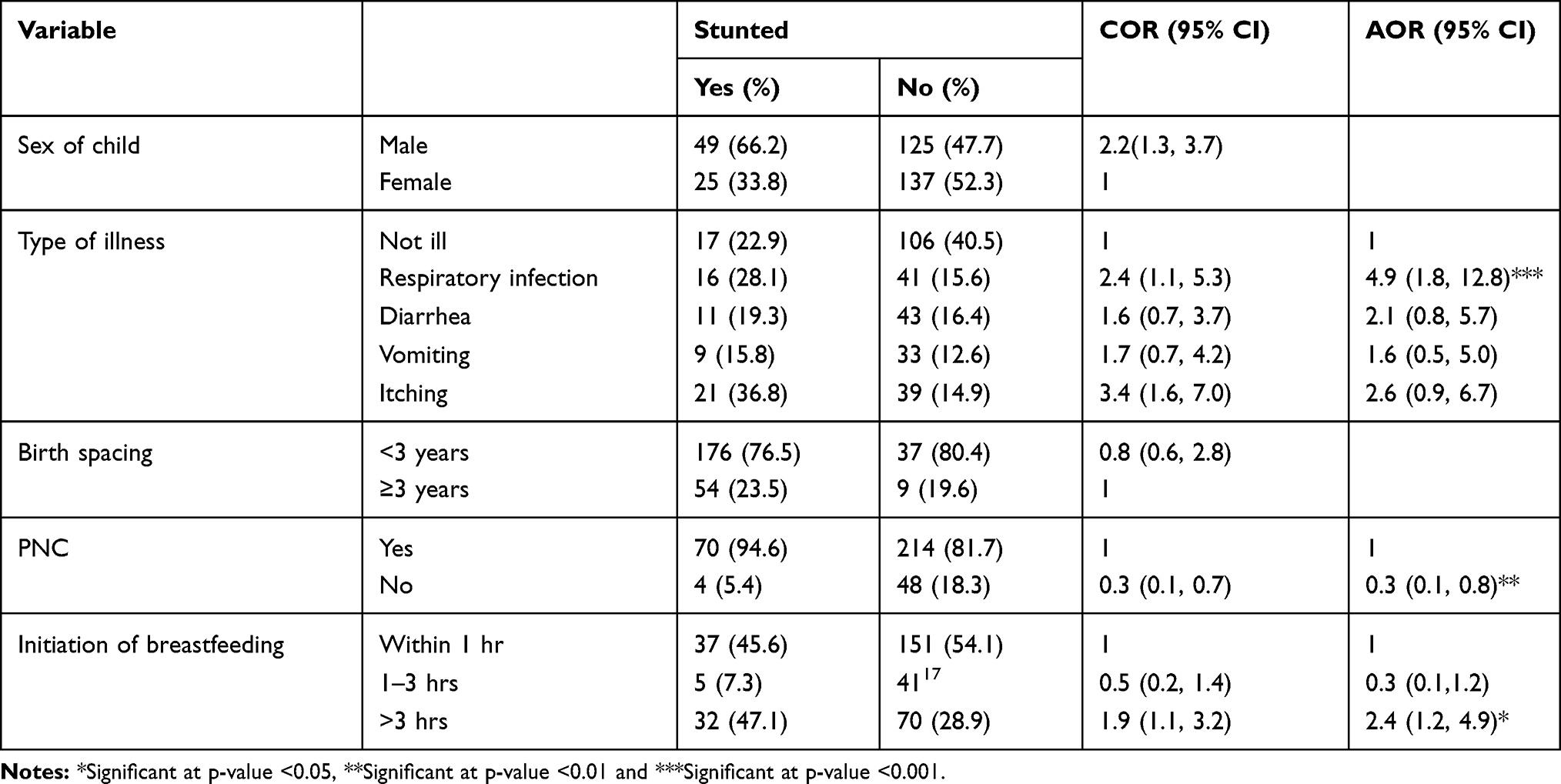 |
Table 4 Factors Associated Stunting Among 6–59 Months Old Children, Delanta District, North Eastern Ethiopia, 2017 G.C |
Discussion
To be effective in the prevention of chronic malnutrition among under-five children in Ethiopia in general and in the study area in particular, there appears a need to investigate the prevalence and contributing factors of chronic malnutrition. Hence, this study tried to assess the prevalence and associated factors of chronic malnutrition among children aged 6–59 months in Delanta district. The prevalence of stunting among 6–59 months old children was 22.1%. This finding is similar with a study done in Somali region, Ethiopia.14 While it was lower than the national (38%) prevalence of stunting.11 It is also lower than studies conducted in Bule Hora (47.6%) and Jimma Arjo (41.4%).15,16 But, it is higher than studies conducted in Somali region and Bangladesh.17,18 This inconsistency might be due to the exclusion of under-six-month-old children. The distribution of stunting was higher among boys (28.9%) than girls (14.7%). This is in line with studies conducted in sub-Saharan Africa.19 Though the actual cause for the difference was not well recognized, it is assumed that boys are more likely to be influenced by environmental stress than girls.
This study revealed that respiratory infection was associated with the development of stunting. Those children who were repeatedly affected by respiratory infection were nearly 5 times more likely to become stunted when compared to their counterparts. This finding was similar with a study done in other part of the world,19,20 which stated that respiratory infection during childhood contributes to malnutrition by impairing height gain over a longer period of time. It is also believed that a child needs to recover from weight loss before resuming linear growth, which contributes to reduction in catch-up growth. Recurrent weight faltering which is associated with multiple episodes of respiratory infection may lead to linear growth faltering.20 However, in areas where there are inadequate dietary intake and high rates of infectious diseases, the process of catch-up growth may not be possible. Therefore, respiratory tract infection will lead to a decreased appetite and malabsorption which is associated with a high level of stunting among children.
The odds of having a stunted child among mother/caregivers who initiated breast milk after 3 hrs of delivery were almost 2 times higher than those who initiated within 1 hr. This result was consistent with other studies from Gurage zone and Tigray region.21,22 This could be because early initiation of breastfeeding within 1 hr is an important contributor for successful breastfeeding through increased secretion and production of breast milk which will provide sufficient nutrient including colostrum (which provide the first natural immunity) for the growing baby. While late initiation of breastfeeding is associated with a decreased breast milk secretion which will contribute for increased prevalence of stunting among children aged 6–59 months.
Those mother/caregivers who follow postnatal care service were 70% less likely to have stunted child as compared to those mother/caregivers who did not follow their postnatal care. This might be because during postnatal care follow-up mother will gate nutrition education from health-care providers about optimum child feeding practice which can be applied for the growing baby. This may have a positive impact on the physical growth of a child.
Limitation of the Study
Since the study was cross-sectional, it was difficult to examine any potential temporal relationships; it may be affected by recall bias among respondents when answering questions related to events happening in the past.
Conclusion and Recommendation
In the study area, the prevalence of stunting is a moderate public health problem. Late initiation of breastfeeding, not utilizing postnatal care service and repeated episodes of respiratory infection were factors associated with stunting. Hence, strengthening baby-friendly hospital initiatives and promotion of breastfeeding, improving postnatal care services utilization and prevention and control of respiratory infections should be included in stunting prevention strategies among children aged 6–59 months.
Abbreviations
ANC, Antenatal Care; AOR, Adjusted Odds ratio; CI, Confidence Interval; COR, Crude Odds ratio; PNC, Postnatal Care; UNICEF, United Nation Children’s Emergency Fund; WHO, World Health Organization.
Consent for Publication
Consent for publication is secured from study participants.
Acknowledgment
We would like to acknowledge Wollo University for funding this research. We want also to thank mother/caregivers who provide information, data collectors and Delanta health office for their full support and cooperation during the data collection process.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. WHO U, Mathers C. Global Strategy for Women’s, Children’s and Adolescents’ Health (2016-2030). Vol. 9. Organization; 2016.
2. Horton S, Steckel RH. Malnutrition: global economic losses attributable to malnutrition 1900–2000 and projections to 2050. How Much Have Global Problems Cost the Earth? A Scorecard from 1900 to;2050. 247–272.
3. Communication UDo. Tracking Progress on Child and Maternal Nutrition: A Survival and Development Priority. Unicef; 2009.
4. Sudfeld CR, McCoy DC, Danaei G, et al. Linear growth and child development in low-and middle-income countries: a meta-analysis. Pediatrics. 2015;135:e1266–e1275.
5. De Onis M, Dewey KG, Borghi E, et al. The World Health Organization’s global target for reducing childhood stunting by 2025: rationale and proposed actions. Matern Child Nutr. 2013;9:6–26. doi:10.1111/mcn.12075
6. Prendergast AJ, Humphrey JH. The stunting syndrome in developing countries. Paediatr Int Child Health. 2014;34(4):250–265. doi:10.1179/2046905514Y.0000000158
7. Burnett C, Valentini S, Cabreiro F, et al. Absence of effects of Sir2 overexpression on lifespan in C. elegans and Drosophila. Nature. 2011;477(7365):482. doi:10.1038/nature10296
8. Christian P. Maternal height and risk of child mortality and undernutrition. JAMA. 2010;303(15):1539–1540. doi:10.1001/jama.2010.469
9. Hoddinott J, Maluccio JA, Behrman JR, Flores R, Martorell R. Effect of a nutrition intervention during early childhood on economic productivity in Guatemalan adults. Lancet. 2008;371(9610):411–416. doi:10.1016/S0140-6736(08)60205-6
10. McCoy DC, Peet ED, Ezzati M, et al. Early childhood developmental status in low-and middle-income countries: national, regional, and global prevalence estimates using predictive modeling. PLoS Med. 2016;13(6):e1002034. doi:10.1371/journal.pmed.1002034
11. Macro O. Ethiopia Demographic and Health Survey, 2005. Addis Ababa: Central Statistical Authority; 2006.
12. Ayele G, Abera K, Damene H, Fikru T. Health Services, a Healthy Environment, and Malnutrition in Ethiopian Assessment and Analysis of Underlying Determinants of Malnutrition Addis Ababa University. Addis Ababa: Addis Ababa University; 2005.
13. De Onis MOA, Borghi E, Siyam A, Nishida C, Siekmann J. The new WHO child growth standards. Paediatr Croat. 2008;52(Supl 1):3–7.
14. Fikadu T, Assegid S, Dube L. Factors associated with stunting among children of age 24 to 59 months in Meskan district, Gurage Zone, South Ethiopia: a case-control study. BMC Public Health. 2014;14(1):800. doi:10.1186/1471-2458-14-800
15. Asfaw M, Wondaferash M, Taha M, Dube L. Prevalence of undernutrition and associated factors among children aged between six to fifty nine months in Bule Hora district, South Ethiopia. BMC Public Health. 2015;15(1):41. doi:10.1186/s12889-015-1370-9
16. Hailemariam TW, Nekemte E. Prevalence of underweight and its determinant factors of under two children in a rural area of western ethiopia. Food Sci Qual Manage. 2014;31.
17. Demissie S, Worku A. Magnitude and factors associated with malnutrition in children 6-59 months of age in pastoral community of Dollo Ado district, Somali region, Ethiopia. Sci J Public Health. 2013;1(4):175–183. doi:10.11648/j.sjph.20130104.12
18. Siddiqi MNA, Haque MN, Goni MA. Malnutrition of under-five children: evidence from Bangladesh. Asian J Med Sci. 2011;2(2):113–119. doi:10.3126/ajms.v2i2.3662
19. Wamani H, Peterson S, Tumwine JK, et al. Boys are more stunted than girls in sub-Saharan Africa: a meta-analysis of 16 demographic and health surveys. BMC Pediatr. 2007;7(1):17. doi:10.1186/1471-2431-7-17
20. Mwiru R, Spiegelman D, Hertzmark E, et al. Nutritional predictors of acute respiratory infections among children born to HIV-infected women in Tanzania. J Trop Pediatr. 2013;59(3):203–208. doi:10.1093/tropej/fmt004
21. Bantamen G, Belaynew W, Dube J. Assessment of factors associated with malnutrition among under five years age children at Machakel Woreda, Northwest Ethiopia: a case control study. J Nutr Food Sci. 2014;4(1):1.
22. Alemayehu M, Tinsae F, Haileslassie K, Seid O, Gebregziabher G, Yebyo H. Undernutrition status and associated factors in under-5 children, in Tigray, Northern Ethiopia. Nutrition. 2015;31(7–8):964–970. doi:10.1016/j.nut.2015.01.013
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.