")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 11
Prevalence and Associated Factors of Macrosomia Among Newborns Delivered in University of Gondar Comprehensive Specialized Hospital, Gondar, Ethiopia: An Institution-Based Cross-Sectional Study
Authors Adugna DG , Enyew EF, Jemberie MT
Received 28 October 2020
Accepted for publication 10 December 2020
Published 16 December 2020 Volume 2020:11 Pages 495—503
DOI https://doi.org/10.2147/PHMT.S289218
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Dagnew Getnet Adugna, Engidaw Fentahun Enyew, Molla Taye Jemberie
Department of Human Anatomy, School of Medicine, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
Correspondence: Dagnew Getnet Adugna
Department of Human Anatomy, School of Medicine, College of Medicine and Health Science, University of Gondar, P.O. Box: 196, Gondar, Ethiopia
Tel +251 932223887
Email [email protected]
Background: Macrosomia is defined as a birth weight of newborns ≥ 4000 grams irrespective of gestational age. It is becoming a burning public health issue in most developing countries and contributes to maternal and newborn complications. Though macrosomia has been increasing in Ethiopia, evidence about its magnitude and associated factors is limited yet. Therefore, this study aimed to assess the prevalence and associated factors of macrosomia among newborns delivered at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia.
Methods: An institution-based cross-sectional study was carried out from February 23rd to April 23rd, 2020. A total of 491 mothers and their newborns were included in the study. The data were collected by interviewing the mothers and reviewing their charts using a structured questionnaire. The outcome variable was newborn birth weight. Data were entered using Epi-data version 4.6 and analyzed using STATA version 14 software. Bivariable and multivariable binary logistic regression were used to identify the factors associated with macrosomia.
Results: The prevalence of macrosomia was 7.54%. Gestational age ≥ 40 weeks (adjusted odds ratio (AOR) = 4.1 (95% CI = 1.7– 9.7)), diabetes mellitus (AOR=5.5 (95% CI = 1.2– 25)), previous history of macrosomia (AOR = 3.7 (95% CI = 1.4– 10)), and male sex (AOR = 3.4 (95% CI = 1.3– 8.7)) were significantly associated with macrosomia.
Conclusion: In the current study, the prevalence of macrosomia was relatively high. The study revealed that maternal diabetes mellitus, higher gestational age, history of macrosomia, and male newborns were the predictors of macrosomia. Thus, obstetric caregivers should give attention to early detection and management of mothers with diabetes mellitus, history of macrosomia, and gestational age of ≥ 40 weeks during pregnancy to prevent macrosomia and its complications.
Keywords: macrosomia, birth weight, newborns, pregnancy, associated factors, Ethiopia
Background
Fetal birth weight is a significant measure of a mother’s and newborn’s nutritional status and maybe the determinant of the newborn’s survival and future health, growth, and development.1 Macrosomia is the term used to describe a fetus or a newborn with very high body weight. There is no popular agreement among researchers and obstetricians on the definition of macrosomia. Although birth weight (BW) greater than 4000, 4200, or 4500 gram have been used as a definition of a macrosomic newborn in various studies,2,3 the most accepted definition is the BW of newborns greater than or equal to 4000 gram.4 Most researchers in low and middle-income countries describe macrosomia as a BW of newborns 4000 gm and above irrespective of gestational age (GA), and it affects both maternal and neonatal health outcomes adversely.5–7
Worldwide, macrosomia affects 3–15% of all pregnancies.8 In developed countries, the prevalence of macrosomia ranges from 5% to 20% at all births,4 although there has been a rise of 15–25% in the last two decades. Research in 23 developing countries across Asia, Africa, and Latin America found that the prevalence of macrosomia varied widely from 0.5% in India to 14.9% in Algeria.9 Based on the findings of two studies, the macrosomia rate in Chad was reported as 7.6%10 and 11.8% in Iran.11 Findings from recent studies have also shown that macrosomia prevalence in Ethiopia ranges from 6.7% to 19.1%.12,13 As a result, the different prevalence rates among different countries may be due to several causative factors investigated in various studies.8,10,11,13–20
Many risk factors have been identified in the causation of macrosomia. These include maternal age; multiparity, gestational age (GA), previous macrosomic baby, ethnicity, male child sex, and the difference in socio-demographic factors.7,9,12,19,21–29 Factors such as pre-gestational body mass index (BMI), weight gain during pregnancy, and pre-existing diabetes mellitus (DM) and gestational diabetes (GDM) are recognized as independent factors for macrosomia.7,26,30–32
Macrosomia is a growing public health problem in most developing countries and it directly or indirectly contributes to maternal and neonatal morbidity and mortality.6,7 This is due to the higher prevalence of diabetes and obesity in reproductive-aged women in developing countries.9,33 It is known that macrosomia is associated with a variety of maternal and newborns complication such as perineal injury, cesarean section, postpartum hemorrhage, prolonged labor, birth asphyxia, shoulder dystocia, brachial plexus injury, and skeletal injury, stillbirth, hypoglycemia.7,9,21,34,35 Additionally, macrosomic infants are prone to certain cancers,24 obesity, hypertension, and type-II DM later in adulthood.36 Adverse maternal and neonatal health outcomes due to macrosomia may result in increased maternal and neonatal risks in developing countries due to the limited availability of obstetrical and newborn basic emergency care.35
Macrosomia is becoming a crucial public health issue in Ethiopia. However, there are limited researches in developing countries like Ethiopia in general and no study in the study area in particular which determines the prevalence of macrosomia and its associated factors. The aim of the present study is, hence, to assess the prevalence and associated factors of macrosomia among newborns delivered at the University of Gondar Comprehensive Specialized Hospital.
Methods
Study Setting
The study area, University of Gondar Comprehensive Specialized Hospital, is located in the Central Gondar zone, Amhara Regional State, Northwest Ethiopia. Gondar is found at a distance of 745km from Addis Ababa, the capital of Ethiopia. University of Gondar Comprehensive Specialized Hospital is one of the largest teaching hospitals in the Amhara Region, and providing service for more than 7.2 million people in Gondar town and the catchment area. The maternity division of the hospital is composed of antenatal care (ANC) clinic, postnatal ward, and delivery wards. It has midwives, senior obstetricians, residents, general practitioners, and support staff. Based on the hospital administrators’ report for 2019/20, about 9900 childbirths were attended at the University of Gondar Comprehensive Specialized Hospital.
Study Design and Period
An institution-based cross-sectional study was conducted from February 23rd to April 23rd, 2020.
Source and Study Population
The source population was all mother-newborn pairs in the University of Gondar Comprehensive Specialized Hospital and the study population was those randomly selected mother-newborn pairs during the study period.
Inclusive and Exclusive Criteria
All mothers who delivered live newborns at the University of Gondar Comprehensive Specialized Hospital during the study period were included in the study and those mothers who were too critically ill to speak were excluded.
Sample Size Determination and Sampling Procedure
The sample size was calculated using a single population proportion formula by considering confidence level (95%), a margin of error = 3%, and 11.86% of prevalence taken from the previous study done in Hawassa, Ethiopia.28 By adding a 10% non-response, the final sample size was 491. A systematic random sampling technique was employed to select study participants. The client registration book of two months before the data collection time was reviewed and then the total numbers of deliveries during a data collection time were estimated (1650 deliveries per two months). To determine the sampling interval (K), the total expected number of all births during the study period (1650) was divided by the sample size (491) to give 3. To select the first participant, the lottery method was used. Then every 3rd record was selected to form the sample.
Variables of the Study
Dependent variable: macrosomia.
Independent variables
Socio-demographic factors: maternal age, religion, residence, educational status, occupational status, family number, and income.
Obstetrics and medical factors: parity, GA, maternal pre-existing DM and GDM, previous macrosomic delivery, previous history of stillbirth, pre-eclampsia, polyhydramnios, and low level of physical activity.
Newborn related factor: sex of newborns.
Data Collection Procedure and Tools
The data were collected by interviewing the mothers and reviewing their charts using a structured questionnaire. The questionnaire was prepared and utilized after reviewing relevant literature. It was first developed in English then translated into Amharic and translated-back into English for appropriateness and easiness in approaching study participants. The BW of a newborn was measured within an hour of delivery by using a beam balance scale accurate to 100gm. The last normal menstrual period (LNMP) was confirmed from both her chart and through the interview. GA was estimated based on her LNMP and using chart review Ultrasound reports.
Data Quality Control
The training was provided for data collectors on techniques of data collection. Before data collection, the questionnaire was pretested; and necessary adjustment was done accordingly. The data collectors were supervised daily by the principal investigator, and the collected data were checked for completeness, consistency, accuracy, and clarity before entry.
Data Processing and Analysis
The collected data were coded, entered into Epidata version 4.6, and exported to STATA version 14 software for analysis. Descriptive statistics like percentages, proportions, and mean was used. The results were presented using tables, text, and charts. A Chi-square test was done for categorical variables to check the assumptions. For the associated factors, binary logistic regression analysis was done since the outcome variable is binary. Both bi-variable and multivariable binary logistic regression analysis was employed. Model fitness was assessed using the Hosmer-Lemeshow test. Variables with a p-value of less than 0.2 in the bi-variable logistic regression were considered for the multivariable logistic regression analysis. In the multivariable logistic regression, Adjusted Odds Ratio (AOR) with 95% confidence interval was used to declare the factors significantly associated with macrosomia.
Ethical Considerations
Ethical approval and clearance for this study were obtained from the Ethical Review Committee of the School of Medicine, College of Medicine and Health Sciences, University of Gondar with an approval number (Ref. No.1858/02/2020). An official letter was submitted to the University of Gondar Comprehensive Specialized Hospital, Medical Director Offices. Permission was obtained from the University of Gondar Comprehensive Specialized Hospital, Department of Gynecology and Obstetrics. After explaining the objective and the importance of the study, written informed consent was obtained from each participant. Confidentiality was maintained. This study was conducted in accordance with the Declaration of Helsinki. University of Gondar Ethical Review Committee approved participants under the age of 18 years to provide informed consent on their own behalf, and the informed consent included the publication of anonymised responses.
Results
Socio-Demographic Characteristic of the Study Participants
A total of 491 study participants were involved in the study with a response rate of 100%. The mean age of the mothers was 28.23 (±5.33) years, ranging from 16 to 45 years. Majority 383 (78%) were urban residents. In addition, 461 (93.89%) of the mothers were married, 289 (58.86%) had secondary education, and 236 (48.07%) were housewives. Regarding the income of the study participants, 376 (76.58%) of mothers had an average monthly income between 1211 and 8970 Ethiopian Birr (Table 1).
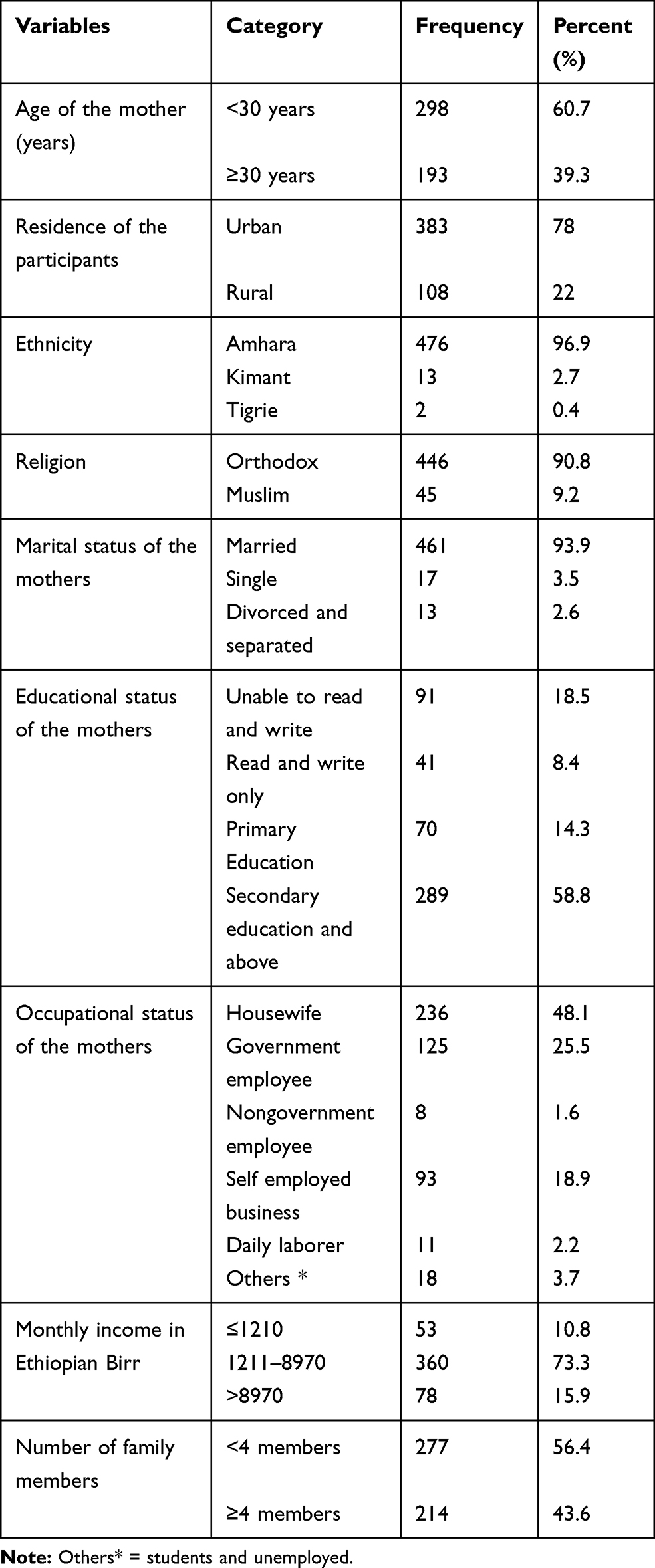 |
Table 1 Socio-Demographic Characteristics of the Study Participants |
Obstetric and Medical Characteristics of Mothers
Out of 491 mothers, most 470 (95.72%) had ANC follow-up and 363 (77.23%) of them had at least four visits during their course of pregnancy. Concerning pregnancy status, 358 (72.91%) of pregnancy was wanted and planned. Majority 435 (88.59%) of women gave birth to between 37 and 42 weeks of gestation, and 305 (62.12%) were multiparous. Fifty-four mothers (11%) had pre-eclampsia, and 15 (3.05%) had DM (pre-existing and GDM) of which 13 (86.67%) had GDM. Out of 491 interviewed mothers, 57 (11.61%) had a history of cesarean section, and 41 (8.35%) had a prior history of macrosomic baby delivery (Table 2).
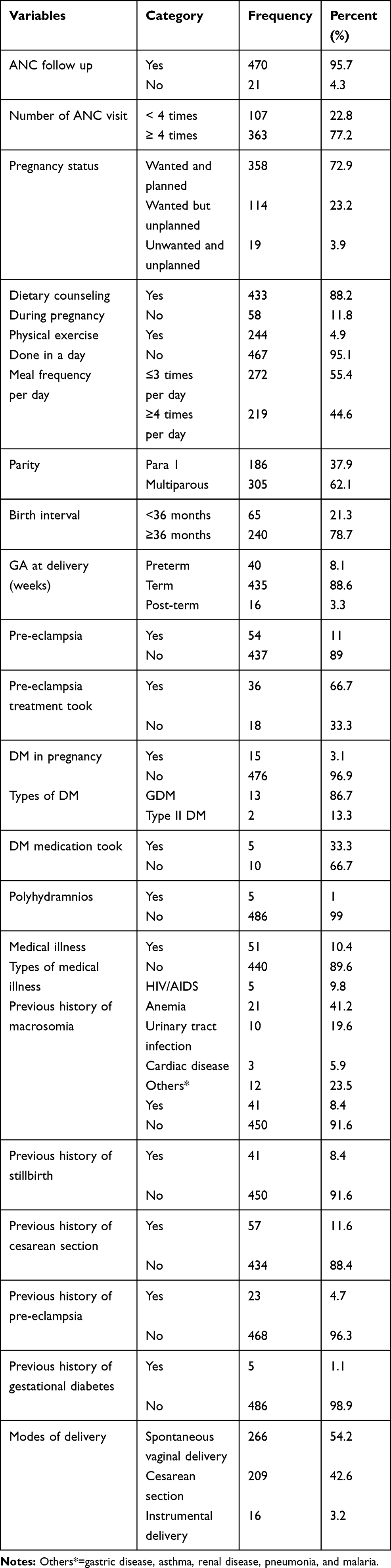 |
Table 2 Obstetric and Medical Characteristics of the Mothers Delivered at the University of Gondar Comprehensive Specialized Hospital, Northwest, Ethiopia 2020 (n=491) |
Characteristics of Newborns
The mean BW of the newborns was 3028.2±579.1gram. Regarding the sex of newborns, 275 (56.01%) were male and 216 (43.99%) were females with a ratio of 1.27:1, respectively (Table 3).
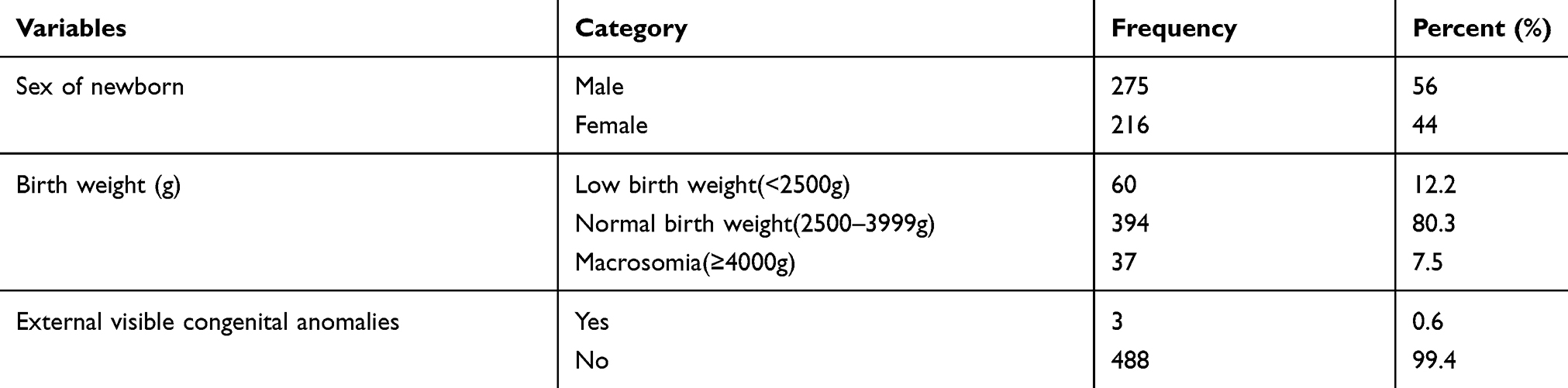 |
Table 3 Newborn Characteristics of the Study Participants at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia 2020 (n=491) |
Prevalence of Macrosomia
The prevalence of macrosomia was 7.5% (95% CI: 5.5, 10.2%) and is presented in Table 3. Among the macrosomic babies, there were more male babies (n = 30, 81.1%) compared to female (n = 7, 18.9%).
Factors Associated with Macrosomia
In bivariable analysis: maternal age ≥30 years, being Muslim religion, average monthly income, GA ≥ 40 weeks, multiparity, pre-eclampsia, DM, polyhydramnios, previous history of macrosomia, previous history of stillbirth, and sex of newborn were statistically significant at a p-value of 0.2. However, in the multivariable model, only GA ≥ 40 weeks, maternal DM, previous history of macrosomia, and male newborns were statistically significant associated factors with macrosomia.
Mothers having a GA of ≥40 weeks were 4.1 times more likely to delivered macrosomic newborns than their counterparts (AOR= 4.1 (95% CI: 1.7–9.7)). The odds of being macrosomic in babies born from DM mothers were 5.5 times greater than the odds of macrosomia in non-DM mothers (AOR =5.5, 95% CI (1.2–25)). Mothers who had a previous history of macrosomic baby were 3.7 times more likely to deliver a macrosomic baby as compared to their counterparts (AOR =3.7, 95% CI (1.4–10)). Likewise, being male increased the risk of having macrosomia by 3.4 compared to females (AOR =3.4, 95% CI (1.3–8.7)) (Table 4).
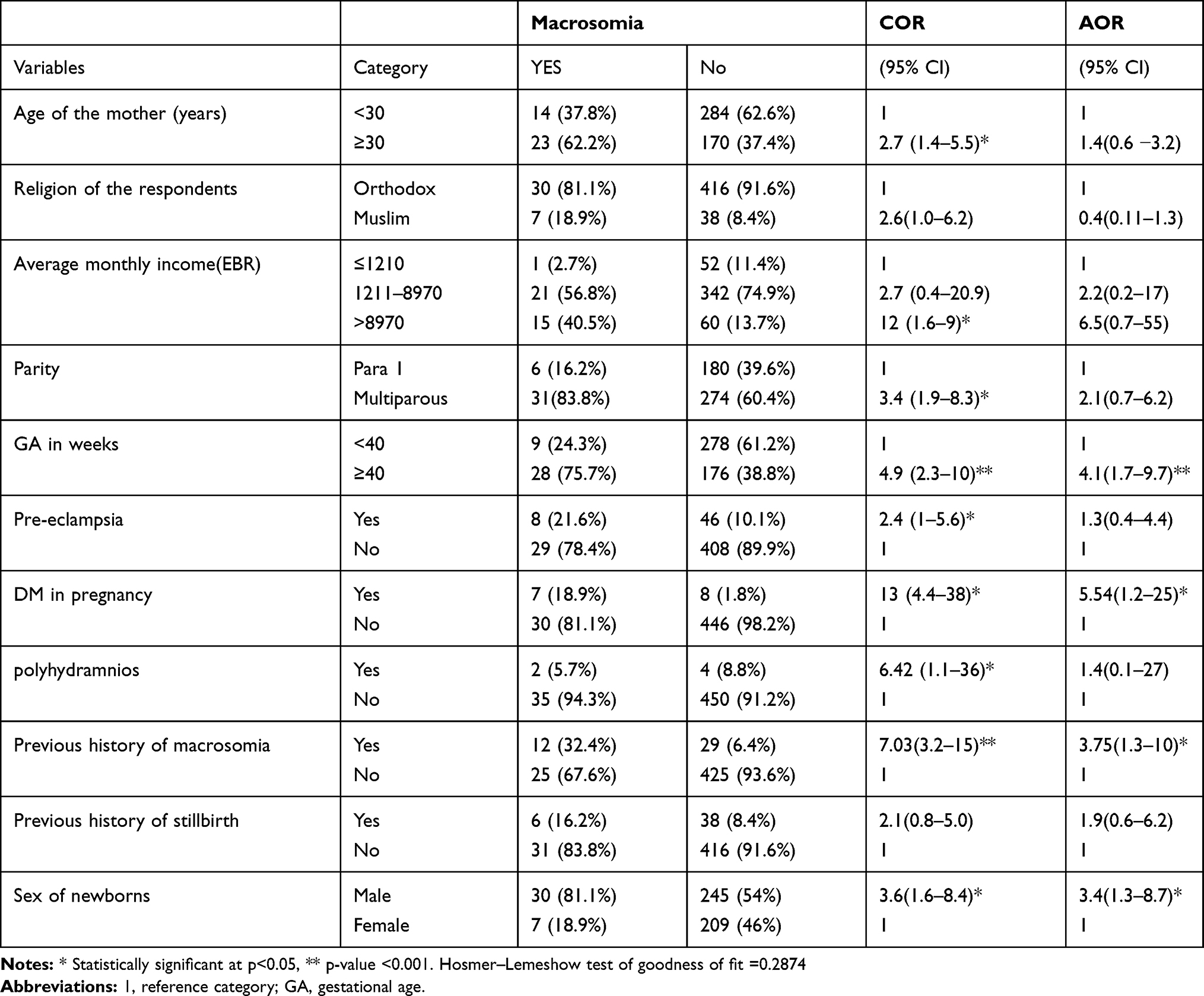 |
Table 4 Factors Associated with Macrosomia Among (n =491) Newborns Delivered at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia 2020 |
Discussion
This study was aimed to assess the prevalence and associated factors of macrosomia among newborns delivered at the University of Gondar Specialized Comprehensive Hospital. In this study, the prevalence of macrosomia was found to be 7.54%. The present study was in line with previous studies in Saudi Arabia,32 Turkey,16 China,14 Ghana,15 Chad,19 and Ethiopia.13 On the other hand, the finding of this study was lower than the study conducted in Iran11 and Algeria.10 This variation may be due to racial and ethnic differences15,37 and also may be due to geographical variation of factors among a different area that has been documented in various studies.14,26 As well, this finding was also lower than the study conducted in Ethiopia.12 The difference could be because methodological, in a way that, the previous study considered only singleton term live-birth deliveries which increase the prevalence of macrosomia. This variation may also be associated with the difference in the socio-economic status of the mothers and the study area. However, our finding was higher than the findings reported in China,18 Saudi Arabia,20 and Iran.17 The possible reasons for the discrepancy could be the difference in socio-demographic characteristics, health service system, and the way of treating mothers during follow-up care, study area, and study time.
The findings of the present study indicated that the GA of ≥40 weeks was significantly associated with macrosomia. Mothers having a GA of ≥40 weeks were 4.1 times more likely to be delivered macrosomic babies than mothers having a GA of <40 weeks. This finding was supported by the studies in Malaysia,26 Iraq,6 California,25 Ethiopia,28 Iran,17 Tanzania,7 and China.27 This may be because an advanced gestational age leads to large birth weight at delivery by permitting the growth process to continue in the uterus. And, this is to be expected as newborns gain weight around 150–200g near term.38
Our study also demonstrated that maternal DM significantly increased the risk of macrosomia in newborns. Mothers who had DM were 5.5 times more likely to have a macrosomic baby as compared to those who had no DM. This was in agreement with the study in Saudi Arabia,32 Malaysia,26 Iran,31,39 and Tanzania.7 The possible reason might be due to the pathophysiology of macrosomia. The pathophysiology of macrosomia is related to the underlying maternal or fetal conditions which are responsible for its development. In a diabetic mother, an impaired maternal glycemic control and high maternal serum glucose level which leads to hyperglycemia cause glucose to cross the placenta but the insulin does not cross. These results in fetal pancreas respond to hyperglycemia and secrete excessive insulin (hyperinsulinemia). Hyperglycemia in the fetus results in the stimulation of the secretion of insulin, insulin-like growth factors, growth hormone, and other growth factors, which in turn stimulate fetal tissue growth, deposition of fat, and glycogen in the fetus, resulting in macrosomia.40
Our finding also revealed that mothers having a previous history of macrosomic babies were at increased risk of having macrosomic newborns. Mothers who had a previous history of a macrosomic baby had 3.7 times increased risk of having a macrosomic baby than their counterparts. This finding was in agreement with studies in Chad,19 Cameron,29 Iran,11,31 Iraq,6 Tanzania,7 and Ethiopia.12,28 This may be due to an inherited genetic tendency of a mother to deliver macrosomic babies. This could be due to the greater maternal BMI at the time of conception, excessive weight gain between pregnancies as well as weight gain during pregnancy leading to recurrence of macrosomia.41
Furthermore, in this study macrosomia had a significant positive association with the sex of newborns. Being male was about 3.6 times more likely to be macrosomic as compared to being female. This is consistent with studies in Malaysia,26 China,14 Northern California,25 Cameron,29 and Ethiopia.28 Male newborns usually around 150–200g larger than female newborns of the same gestational age near term.38
Strength of the Study
The data were collected by trained professional midwives; and there were no similar studies conducted in the study area.
Limitation of the Study
This study had some limitations: First, the cross-sectional nature of the study design may not show the cause and effect relationship. Secondly, the study did not address some factors such as high pre-pregnancy body mass index and weight gain during pregnancy.
Conclusion
The prevalence of macrosomia in this study was relatively high. The presence of DM, previous history of macrosomia, GA of 40 weeks and above, and male sex were significant factors associated with macrosomia. So, obstetric caregivers should give attention to early detection and management of mothers with DM, previous macrosomia, and GA of ≥40 weeks during their ANC visit to prevent macrosomia and its associated complications.
Abbreviations
ANC, Antenatal Care; AOR, Adjusted Odds Ratio; BMI, Body Bass Indexed; BW, birth weight; CI, Confidence Interval; COR, Crude Odds Ratio; DM, Diabetes Mellitus; GA, Gestational Age; GDM, Gestational Diabetes Mellitus; HIV/AIDS, Human Immune Virus/Acquired Immune Deficiency Syndrome; LNMP, Last Normal Menstrual Period; STATA, statistics/data analysis.
Data Sharing Statements
All data and materials of this study are available and can be accessed with a reasonable request from the corresponding author with the email address of “[email protected]”.
Acknowledgments
We would like to acknowledge all study participants and data collectors for their great contributions to the success of this study. We would also like to thank the University of Gondar for providing us ethical clearance and financial supports.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors declare that they have no conflicts of interest for this work.
References
1. Gage TB, Fang F, O’Neill E, DiRienzo G. Maternal education, birth weight, and infant mortality in the United States. Demography. 2013;50(2):615–635. doi:10.1007/s13524-012-0148-2
2. Zhang X, Decker A, Platt RW, Kramer MS. How big is too big? The perinatal consequences of fetal macrosomia. Am J Obstet Gynecol. 2008;198(5):517. doi:10.1016/j.ajog.2007.12.005
3. Boulet SL, Alexander GR, Salihu HM, Pass M. Macrosomic births in the United States: determinants, outcomes, and proposed grades of risk. Am J Obstet Gynecol. 2003;188(5):1372–1378. doi:10.1067/mob.2003.302
4. Henriksen T. The macrosomic fetus: a challenge in current obstetrics. Acta Obstet Gynecol Scand. 2008;87(2):134–145. doi:10.1080/00016340801899289
5. Wondie T, Jara D, Ayana M. Factors associated with macrosomia among neonates delivered at Debre Markos Referral Hospital, Northwest Ethiopia, 2014: a case-control study. J Diabetes Metab. 2014;5(468):2.
6. Jasim SK, Al-Momen H, Majeed BA, Hussein MJ. Rate of Fetal Macrosomia with Maternal and Early Neonatal Complications in Internally Moved People Affected by Violence. Health Sci. 2018;7(7):141–146.
7. Said AS, Manji KP. Risk factors and outcomes of fetal macrosomia in a tertiary center in Tanzania: a case-control study. BMC Pregnancy Childbirth. 2016;16(1):243.
8. Asplund CA, Seehusen DA, Callahan TL, Olsen C. Percentage change in antenatal body mass index as a predictor of neonatal macrosomia. Ann Family Med. 2008;6(6):550–554.
9. Koyanagi A, Zhang J, Dagvadorj A, et al. Macrosomia in 23 developing countries: an analysis of a multicountry, facility-based, cross-sectional survey. Lancet. 2013;381(9865):476–483.
10. Mai A, Abbassia D. The prevalence of fetal macrosomia at the specialized hospital of gynecology and obstetrics of Sidi Bel Abbes (West Of Algeria). J Nutr Food Sci. 2014;4(3):1.
11. Mardani M, Rossta S, Rezapour P. Evaluation of the prevalence of macrosomia and the maternal risk factors. Iranian J Neonatology IJN. 2014;5(3):5–9.
12. Tela FG, Bezabih AM, Adhanu AK, Tekola KB. Fetal macrosomia and its associated factors among singleton live-births in private clinics in Mekelle city, Tigray, Ethiopia. BMC Pregnancy Childbirth. 2019;19(1):219. doi:10.1186/s12884-019-2379-3
13. Mengesha HG, Wuneh AD, Weldearegawi B, Selvakumar DL. Low birth weight and macrosomia in Tigray, Northern Ethiopia: who are the mothers at risk? BMC Pediatr. 2017;17(1):144. doi:10.1186/s12887-017-0901-1
14. Li G, Kong L, Li Z, et al. Prevalence of Macrosomia and Its Risk Factors in China: A Multicentre Survey Based on Birth Data Involving 101 723 Singleton Term Infants. Paediatric Perinatal Epidemiology. 2014;28(4):345–350. doi:10.1111/ppe.12133
15. Abubakari A, Kynast-Wolf G, Jahn A. Prevalence of abnormal birth weight and related factors in Northern region, Ghana. BMC Pregnancy Childbirth. 2015;15(1):335. doi:10.1186/s12884-015-0790-y
16. Usta A, Usta CS, Yildiz A, et al. Frequency of fetal macrosomia and the associated risk factors in pregnancies without gestational diabetes mellitus. Pan Afr Med J. 2017;26.
17. Amini P, Maroufizadeh S, Hamidi O, Samani RO, Sepidarkish M. Factors associated with macrosomia among singleton live-birth: A comparison between logistic regression, random forest, and artificial neural network methods. Epidemiology Biostatistics Public Health. 2016;13:4.
18. Wong P, Wk TW. Risk factors and pregnancy outcomes of macrosomia: a retrospective cohort study. Hong Kong J Gynaecol Obstet Midwifery. 2018;18:18–23.
19. Madoue GB, Sile SN, Lhagadang F. Fetal macrosomia: risk factors, maternal and fetal outcomes in N’Djamena Mother and Child Hospital, Chad. South Sudan Med J. 2018;11(2):40–43.
20. Al-Qashar F, Al-Ghamdi M, Agab W, et al. Prevalence and outcomes of macrosomic infants born to non-diabetic mothers: A ten years’ experience at the tertiary care center. J Am Sci. 2016;12:12.
21. Salem W, Adler A, Lee C, Smith G. Maternal waist to hip ratio is a risk factor for macrosomia. BJOG. 2012;119(3):291–297.
22. Islam MR. Prevalence and Predictors of Macrosomia Newborn: Northern-Norwegian Mother-And-Child Study. Universitetet I Tromsø; 2012.
23. Ouzounian J, Hernandez G, Korst L, et al. Pre-pregnancy weight and excess weight gain are risk factors for macrosomia in women with gestational diabetes. J Perinatology. 2011;31(11):717–721. doi:10.1038/jp.2011.15
24. Lawlor D, Fraser A, Lindsay R, et al. Association of existing diabetes, gestational diabetes and glycosuria in pregnancy with macrosomia and offspring body mass index, waist and fat mass in later childhood: findings from a prospective pregnancy cohort. Diabetologia. 2010;53(1):89–97. doi:10.1007/s00125-009-1560-z
25. Stotland N, Caughey A, Breed E, Escobar G. Risk factors and obstetric complications associated with macrosomia. Int j Gynecol Obstetrics. 2004;87(3):220–226. doi:10.1016/j.ijgo.2004.08.010
26. Yadav H, Lee N. Factors influencing macrosomia in pregnant women in a tertiary care hospital in Malaysia. J Obstet Gynaecol Res. 2014;40(2):439–444. doi:10.1111/jog.12209
27. Cheng YW, Nicholson JM, Nakagawa S, Bruckner TA, Washington AE, Caughey AB. Perinatal outcomes in low-risk term pregnancies: do they differ by week of gestation? Am J Obstet Gynecol. 2008;199(4):
28. Biratu AK, Wakgari N, Jikamo B. Magnitude of fetal macrosomia and its associated factors at public health institutions of Hawassa city, southern Ethiopia. BMC Res Notes. 2018;11(1):888. doi:10.1186/s13104-018-4005-2
29. Nkwabong E, Tangho GRN. Risk factors for macrosomia. j Obstetrics Gynecol India. 2015;65(4):226–229. doi:10.1007/s13224-014-0586-4
30. Jolly MC, Sebire NJ, Harris JP, Regan L, Robinson S. Risk factors for macrosomia and its clinical consequences: a study of 350,311 pregnancies. Eur J Obstetrics Gynecol Reproductive Biol. 2003;111(1):9–14. doi:10.1016/S0301-2115(03)00154-4
31. Rezaiee M, Aghaei M, Mohammadbeigi A, Farhadifar F, zadeh N. Fetal macrosomia: risk factors, maternal, and perinatal outcome. Ann Med Health Sci Res. 2013;3(4):546–550. doi:10.4103/2141-9248.122098
32. Nadir S, Jamil S, Hamid M. The prevalence of macrosomia in newborns and its association with maternal diabetes. J Med Sci. 2015;23(1):3–6.
33. Martorell R, Khan LK, Hughes ML, Grummer-Strawn LM. Obesity in women from developing countries. Eur J Clin Nutr. 2000;54(3):247–252. doi:10.1038/sj.ejcn.1600931
34. Young BC, Ecker JL. Fetal macrosomia and shoulder dystocia in women with gestational diabetes: risks amenable to treatment? Curr Diab Rep. 2013;13(1):12–18. doi:10.1007/s11892-012-0338-8
35. Fuchs F, Bouyer J, Rozenberg P, Senat M-V. Adverse maternal outcomes associated with fetal macrosomia: what are the risk factors beyond birthweight? BMC Pregnancy Childbirth. 2013;13(1):90. doi:10.1186/1471-2393-13-90
36. Hermann GM, Dallas LM, Haskell SE, Roghair RD. Neonatal macrosomia is an independent risk factor for adult metabolic syndrome. Neonatology. 2010;98(3):238–244. doi:10.1159/000285629
37. Tsai P-JS, Roberson E, Dye T. Gestational diabetes and macrosomia by race/ethnicity in Hawaii. BMC Res Notes. 2013;6(1):395. doi:10.1186/1756-0500-6-395
38. Duryea EL, Hawkins JS, McIntire DD, Casey BM, Leveno KJ. A revised birth weight reference for the United States. Obstet Gynecol. 2014;124(1):16–22. doi:10.1097/AOG.0000000000000345
39. Tabatabaee HR, Mohammad-Beigi A, Yazdani M, Zeighami B, Mohammad-Salehi N. Gestational diabetes risk factors modeling in pregnant women. Int J Diabetes Dev Countries. 2007;27(1):11. doi:10.4103/0973-3930.34751
40. Kc K, Shakya S, Zhang H. Gestational diabetes mellitus and macrosomia: a literature review. Ann Nutr Metab. 2015;66(Suppl. 2):14–20. doi:10.1159/000371628
41. Mahony R, Foley M, Mcauliffe F, O’HERLIHY C. Maternal weight characteristics influence recurrence of fetal macrosomia in women with normal glucose tolerance. Australian New Zealand J Obstetrics Gynaecology. 2007;47(5):399–401. doi:10.1111/j.1479-828X.2007.00764.x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.