")
Back to Journals » International Journal of Women's Health » Volume 8
Prevalence and associated factors of female genital cutting among young adult females in Jigjiga district, eastern Ethiopia: a cross-sectional mixed study
Authors Gebremariam K, Assefa D, Weldegebreal F
Received 21 April 2016
Accepted for publication 10 June 2016
Published 9 August 2016 Volume 2016:8 Pages 357—365
DOI https://doi.org/10.2147/IJWH.S111091
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Kidanu Gebremariam,1 Demeke Assefa,2 Fitsum Weldegebreal3
1Department of Epidemiology, School of Public Health, Mekelle University, Mekelle, 2Reproductive Health and Health Service Management, School of Public Health, Addis Ababa University, Addis Ababa, 3Medical Laboratory Science, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Purpose: The aim of this study was to assess the prevalence and associated factors of female genital cutting (FGC) among young adult (10–24 years of age) females in Jigjiga district, eastern Ethiopia.
Methods: A school-based cross-sectional mixed method combining both quantitative and qualitative research methods was employed among 679 randomly selected young adult female students from Jigjiga district, Somali regional state, eastern Ethiopia, from February to March 2014 to assess the prevalence and associated factors with FGC. A pretested structured questionnaire was used to collect data. The qualitative data were collected using focus group discussion.
Results: This study depicted that the prevalence of FGC among the respondents was found to be 82.6%. The dominant form of FGC in this study was type I FGC, 265 (49.3%). The majority of the respondents, 575 (88.3%), had good knowledge toward the bad effects of FGC. Four hundred and seven (62.7%) study participants had positive attitude toward FGC discontinuation. Religion, residence, respondents’ educational level, maternal education, attitude, and belief in religious requirement were the most significant predictors of FGC. The possible reasons for FGC practice were to keep virginity, improve social acceptance, have better marriage prospects, religious approval, and have hygiene.
Conclusion: Despite girls’ knowledge and attitude toward the bad effects of FGC, the prevalence of FGC was still high. There should be a concerted effort among women, men, religious leaders, and other concerned bodies in understanding and clarifying the wrong attachment between the practice and religion through behavioral change communication and advocacy at all levels.
Keywords: female genital cutting, prevalence, Somali regional state, eastern Ethiopia, young adult, Jigjiga
Background
Female genital mutilation/cutting (FGM/C) is a traditional surgical modification of the female genitalia comprising all procedures involving partial or total removal of the external female genitalia or other injury to the female genital organs for cultural or nontherapeutic reasons. It is estimated that from 130 to 140 million women in the world have been circumcised. An average of about four girls a minute continue to be mutilated.1–5
Laws and policies on anti-FGM/C are codified almost in every country. The fight against FGM/C contributes to the achievement of Millennium Development Goal in 2015. Then, we can effectively address abatement of the consequences that female circumcision poses to the health of these women and possibly eliminate it from the future generations.6–8
FGM/C is associated with a series of health risks and many consequences mainly during the procedure. Girls are subject to violent pain, severe bleeding and, in many cases, shock and risk of HIV/AIDS infection. During puberty, many mutilated girls suffer from menstrual blood retention and predisposition to infection and further complications. Longer-term complications include fistula, repeated urinary tract infection, scars which could/might be opened during childbirth and which can lead to severe hemorrhage, obstructed menstrual flow, reproductive tract infection, and reduced fertility.9,10
According to Ethiopian Demographic and Health Survey (EDHS) 2005, FGM/C is common among Ethiopian women and >50% of young adult women are circumcised. This report shows that on a national level 74.3% of women are circumcised, 27.1% in the Gambella region, 97.3% in the Somali region, and >50% in Addis Ababa.11–13 FGM/C is a widespread practice both among Muslim and Christian populations in Somali region. Following the magnitude of the problem, Ethiopia has launched educational programs 20 years ago in consultation with traditional community associations (elders) and local healers. Similarly, different nongovernment organizations, embassies, and the regional government have been implementing different intervention programs in Somali region.13,14
Internationally, ~3 million girls are at risk of undergoing FGM/C and 130 to 140 million girls and women are currently living with its consequences. An average of about four girls are mutilated every minute. In Africa, it is estimated that 92 million girls aged 10 and above have undergone FGM/C. FGM/C is practiced almost in 28 African countries, the Middle East, and South East Asia. Most women who have experienced FGM/C live in one of the 28 countries in Africa; nearly half of them were just found in two countries: Egypt and Ethiopia. Women and girls who have undergone FGM/C are also found in Europe, Canada, US, and Australia because of the increasing movement of communities and individuals between countries. The estimated prevalence of FGM/C in 28 countries across Africa ranged from 98% in Somalia to <1% in Uganda.15,16
FGM/C is mostly carried out on girls aged between a few days old and 15 years. However, occasionally, adult and married women are also subjected to the procedure. The age at which FGM is performed varies with local traditions and circumstances, but is decreasing in some countries.7
The World Health Organization has classified FGM operation into four types. Type I (Sunna) FGC is a partial or total removal of the clitoris. Type II (intermediate FGM) refers to partial or total removal of the clitoris together with partial or total excision of the labia minora. Type III (infibulation) is partial or total removal of the external genitalia and stitching or narrowing of the vaginal opening. Type IV is relatively rare and refers to any genital surgeries, such as pricking or stretching the clitoris and/or surrounding tissues.17,18
A cross-sectional study that was conducted among 492 respondents sampled from three refugee camps in Somali Regional State shows that the intention of the parents to circumcise their daughters was high (84%), and of 288 individuals reported having undergone FGC, 42.4% were ≤12 years of age. The prevalence increased with age, and ~52% and 95% were circumcised at the age of 7–8 and 11–12 years, respectively. Participation of the parents in anti-FGC interventions was statistically associated with lower practice and intention of the procedures.4
There are many reasons for the practice of FGM, and it is often described as a means to safeguard against premarital sexual activity, prevent female promiscuity and preserve virginity, for religious or health reasons, on hygienic grounds, for the sake of tradition or ethnic interests, and for socioeconomic or sex-related reasons.19,20
According to the Ye Ethiopia Goji Limadawi Dirgitoch Aswogaj Mahiber 2009 report for Ethiopian Somali region, the most pervasive reasons are avoidance of trouble to husband, respect for tradition, to control women’s reaction/emotion, to avoid difficulty at delivery, to get married, for religious requirement and hygienic reasons; and the worst type of FGM, infibulations, is performed in Somali region. There has been relatively a change in attitude and knowledge for the last 5 years; however, it had not brought changes in prevalence.21
According to some studies, the prevalence of FGM in Ethiopia and Somali region is very high. Considering the magnitude of the problem, government and nongovernment organizations have started anti-FGM campaign in Somali region. Due to lack of published research on the status of FGM in the region, this study was conducted to assess the current status of FGM/C prevalence and identify possible reasons and factors associated with the practice. The result of the study will help to assess the impact of intervention ever made and also the study will be used as area-specific baseline information to evaluate and monitor future interventions. At the same time, it is important for health planners and decision makers of the region to visualize the current status of the problem and modify any possible intervention activities in order to improve the quality of life and sexual reproductive life of girls and women.
Materials and methods
Study design, period, and area
A school-based cross-sectional mixed study combining both quantitative and qualitative research methods was employed from February to March 2014 to assess the prevalence and associated factors with FGM/C among young adult (15–24 years of age) females who attend high school and college in Jigjiga district from August 2013 to June 2014. The qualitative part was planned to supplement the quantitative findings. Somali region is one of the nine regional states that make the Federal Republic of Ethiopia. It is found in the eastern part of Ethiopia. Internationally it is bordered with Kenya in the south, Somalia in the east, and Djibouti in the north. Somali region is divided into nine zones, and the zones are further divided into 52 woredas. Among the six woredas in the Jigjiga Zone, Jigjiga district which is the capital city of Somali regional state, is located in the eastern part of the country at a distance of 635 km from Addis Ababa. The total population of Jigjiga district was estimated to be 345,407 in 28 Kebeles. Among this, 47% and 53% are females and males, respectively. Approximately 79,789 (23%) of the population are women aged 15–49.22
Sample size estimation and sampling procedures
The study was planned to recruit 679 individuals. The respondents were young-adult (10–24 years of age) female students. The sample size was determined using single population proportion formula. The assumption for calculation of sample size were 95% confidence level, 5% degree of precision, and 74% of the proportion of circumcised female (15–49 years).13 The 74% national FGC prevalence was taken to have maximum representative sample size when compared with the prevalence of FGC in Somali region (97.3%). Taking this assumption, “n” became 295 and with the design effect of 2% and 15% nonresponse rate, the final sample size became 679. Multistage sampling technique was employed to select study subjects. Among three high schools and four colleges found in the district, two colleges and two high schools were selected using lottery method. All sections from each selected high schools and colleges were taken as strata. In all, 679 female students were selected using stratified random sampling with proportionate allocation to size from each section. Four focus group discussions were undertaken among women/husbands, local leaders (religious, clan, and community), and female circumcisers separately.
Data collection
Data were collected using a standardized, structured, pretested, and self-administered questionnaire. The questionnaire was first prepared in English and then translated to the local language (Somaligna) and back translated to English to maintain its consistency. Three trained supervisors and six female data collectors participated in the data collection process. All of the data collectors were diploma holders and had data collection experience in reproductive health survey. Two days of intensive training was given to the data collectors and supervisors on how to conduct the data collection. A brief introduction to supervisors, data collectors, and students was given before and during the data collection time.
Data analysis
The data were entered into Epi Info3.5.3 statistical software (Centers for Disease Control and Prevention, Atlanta, GA, USA) and analyzed using SPSS version 17.0 packages (SPSS Inc., Chicago, IL, USA). Frequencies, proportions, and cross tabulations were used to summarize descriptive statistics of the data. All variables that were significant at bivariate analysis were entered into multiple logistic regressions. Finally, the variables that had a significant association were identified on the basis of adjusted odds ratio (AOR) with 95% confidence interval (CI) and a P-value <0.05 to fit the final regression model. The qualitative data were audio taped, transcribed, and coded with open-code version 3.6 and inductive content analysis was applied.
Ethical considerations
The study protocol was reviewed and approved by the Institutional Ethical Review board of School of Public Health, University of Addis Ababa. Official permission was secured after communication with the district and respective school administrators through a formal letter. Respondents were informed about the purpose of the study and verbal consent was obtained from the study participants so as to maintain confidentiality by omitting their names on the questionnaire. For those students who were under the age of consent, assent was taken from their school members and/or parents, and/or themselves when they were independent minor.
Results
In all, 662 respondents participated in the quantitative study making a response rate of 97.5% among young adult females. Four focus group discussions were conducted for the qualitative part of the study. Of these, the majority 374 (56.5%) were in the age range of 15–19. The mean age of the respondents was 20 (±2.4) years ranging from 15 to 24 years. The majority of the respondents, 511 (77.2%), were Muslim followers. More than half, 430 (65%), of the respondents were members of the Somali ethnic group. Nearly half of the respondents, 355 (53.6%), reported that they were residing in rural areas. Almost all, 626 (94.6%), of the respondents were not married. In all, 243 (36.7%) and 214 (32.3%) of the respondents’ mothers and fathers did not attend any formal education (illiterate), respectively. Out of the total, 347 (52.4%) respondents’ mothers were housewives (Table 1).
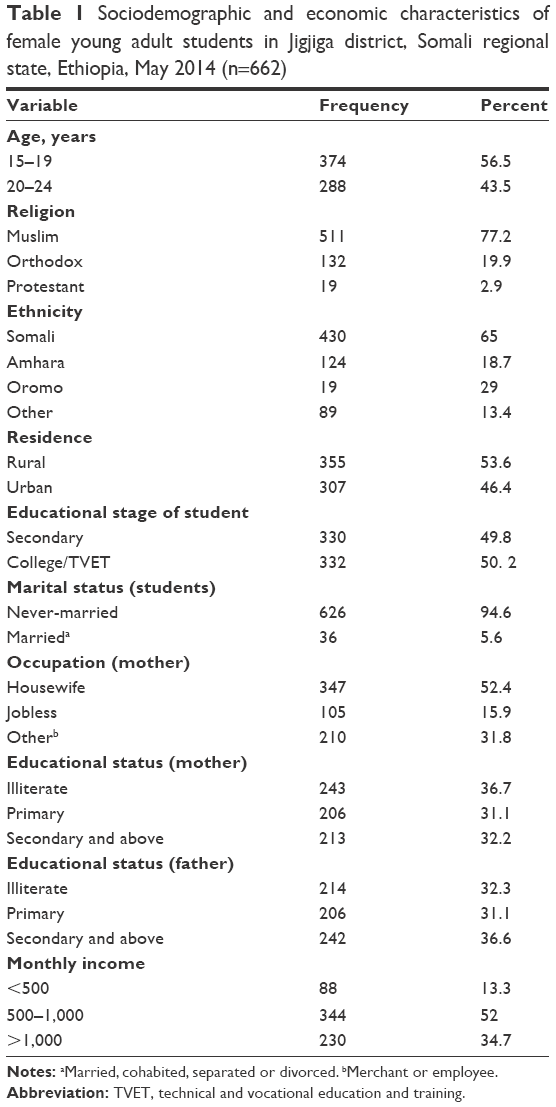 | Table 1 Sociodemographic and economic characteristics of female young adult students in Jigjiga district, Somali regional state, Ethiopia, May 2014 (n=662) |
A total of 538 (82.6%) study participants underwent one or more of the different forms of FGM/C. Of these, 268 (49.9%) were circumcised during the age of 7–10 years with a mean age of 8.3 years. In all, 414 (63.6%) respondents reported that FGM/C was performed at their own home. The majority, 473 (72.7%), of the participants stated that FGC was performed by a traditional circumciser followed by a traditional birth attendant, 166 (25.5%) (Figure 1). The decision to have FGM/C was made by respondents’ mothers (555 [83.5%]), followed by grandmothers (247 [37.9%]), and religious leaders (157 [24.1%]). A total of 265 (49.3%) respondents had type I FGC followed by 244 (45.4%) with type III (Table 2).
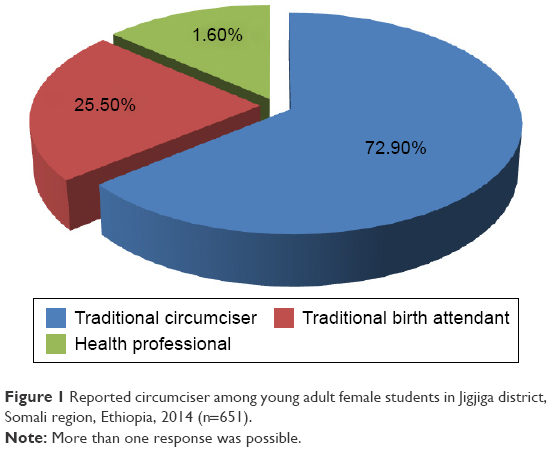 | Figure 1 Reported circumciser among young adult female students in Jigjiga district, Somali region, Ethiopia, 2014 (n=651). |
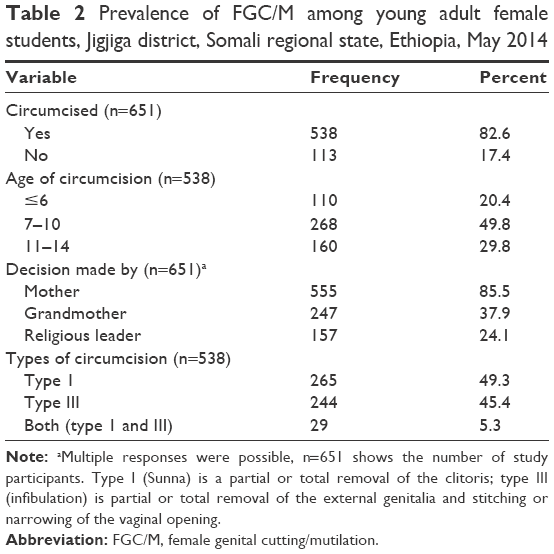 | Table 2 Prevalence of FGC/M among young adult female students, Jigjiga district, Somali regional state, Ethiopia, May 2014 |
In all, 573 (88.3%) of the young adult females had a good knowledge of FGC practice and its complication. Knowledge about the specific complications of FGM/C was asked, and it was consistently above 50% in major complication areas. Among 651 study participants, 557 (85.6%) participants responded that it transmits HIV, 537 (82%) that is causes severe pain during the procedure, 528 (81.1) that it causes excessive bleeding, 521 (80%) that is causes sexual dissatisfaction, and 367 (56.4%) that it creates difficulty during delivery. The source of information regarding FGM/C and its bad effects were health professions, 456 (70%), followed by anti-FGM training, 397 (61%).
Most of the study participants were also aware of the types of circumcision, particularly 479 (89.5%) type I (clitoridectomy) and 333 (62.2%) type III (infibulation). The study subjects were asked about reasons of FGC; above three-quarters, 518 (79.6%), of female respondents believed that there is at least one benefit or reason of FGC to be carried out. Of these, 395 (60.7%) said it can prevent having premarital sex, 359 (55.1%) to have social acceptance from the community, 192 (29.5%) to have better marriage prospects, and 116 (17.8%) and 113 (17.4%) responded that it is beneficial in providing hygiene/cleanliness and it is important for religious approval, respectively (Table 3). The group discussants and respondents were also discussed about female circumcision following community enforcing factors. The participants stated that an uncircumcised woman is considered a marginal woman, hypersexual, infidel, non-Muslim, and nonpure. According to some participants also, they consider FGC as a license for marriage. The majority of focused group informants said that most families are forced to practice FGC due to fear of discrimination for deviating from community norms in their area. Some respondents also discussed that the Somali community as a whole has a fear of God’s punishment if it is not performed in their daughters. This is why the Somali community still struggles to change the attitude of the community.
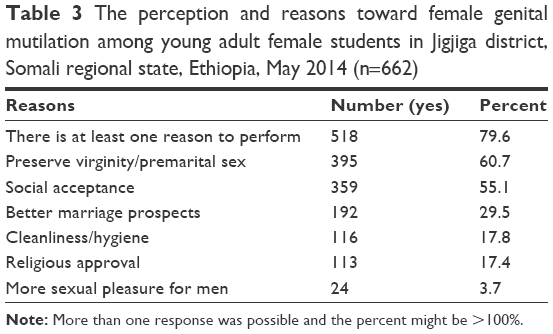 | Table 3 The perception and reasons toward female genital mutilation among young adult female students in Jigjiga district, Somali regional state, Ethiopia, May 2014 (n=662) |
The study participants were also asked about attitude toward the continuation of the practice: 244 (37.5%) respondents favor the continuation of the practice. Of these, 190 (79.5%) said due to religious demand, 219 (91.6%) preserves virginity, 175 (73.2%) increases better marriage prospects, 141 (59%) good tradition, 104 (43.5%) for clean/hygienic reasons, and 60 (25.4%) as a good custom.
When logistic regression analysis were done among dependent and independent variables of the study mainly to see the association among factors associated with the FGC/M, Muslim were subjected positively and significantly to FGM practice compared to Christian respondents (AOR =3.7; 95% CI =1.1, 12). The prevalence of FGC was four times more likely among rural residence compared to their counterpart in urban (AOR =4; 95% CI =2.4, 6.8). The odds of circumcised female students more likely to be circumcised whose mothers are illiterate were 2.4 times when compared with those whose mothers had completed high school and above (AOR =2.4; 95% CI =1.3, 4.3). The prevalence of FGC is less by 50% in those who had a positive attitude toward discontinuation of the practice when compared with those who had a negative attitude (AOR =0.5; 95% CI =0.3, 0.8). Female students at high school level were less likely to be circumcised compared to female students at college level (AOR =0.5; 95% CI =0.3, 0.8). The odds of the practice was 2.3 times higher and statistically significant among those who believe FGM/C is required by their religion when compared with those who do not believe (AOR =2.3; 95% CI =1.5, 3.5) (Table 4).
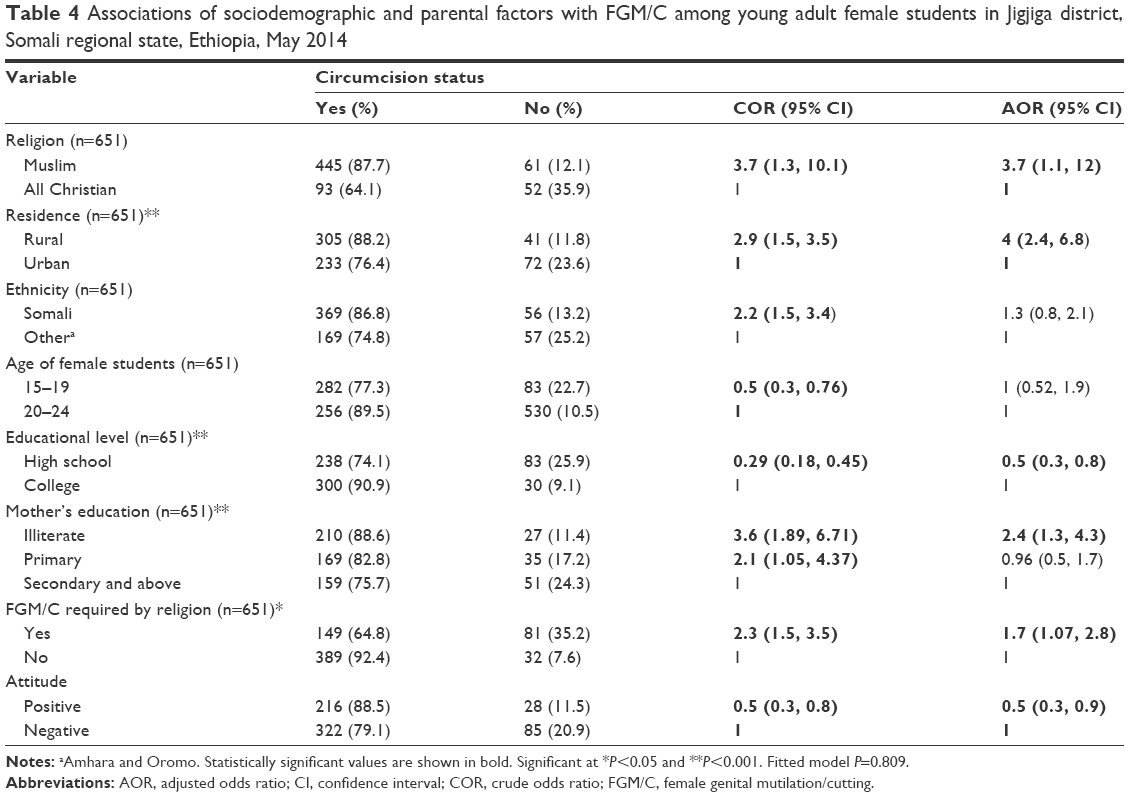 | Table 4 Associations of sociodemographic and parental factors with FGM/C among young adult female students in Jigjiga district, Somali regional state, Ethiopia, May 2014 |
The study participants mentioned ways to best struggle against the practice; 283 (69%) through educational campaigning and 219 (53.2%) women empowerment in socioeconomic and other related factors. A total of 190 (46.1%) served as an educational promoter and enforcer in a community practicing FGC, 79 (19.2%) believed that the father should take more responsibility, and 67 (16.3%), that implementing enforced laws/legislation was the main method to fight against this practice and other harmful traditional practices (Figure 2).
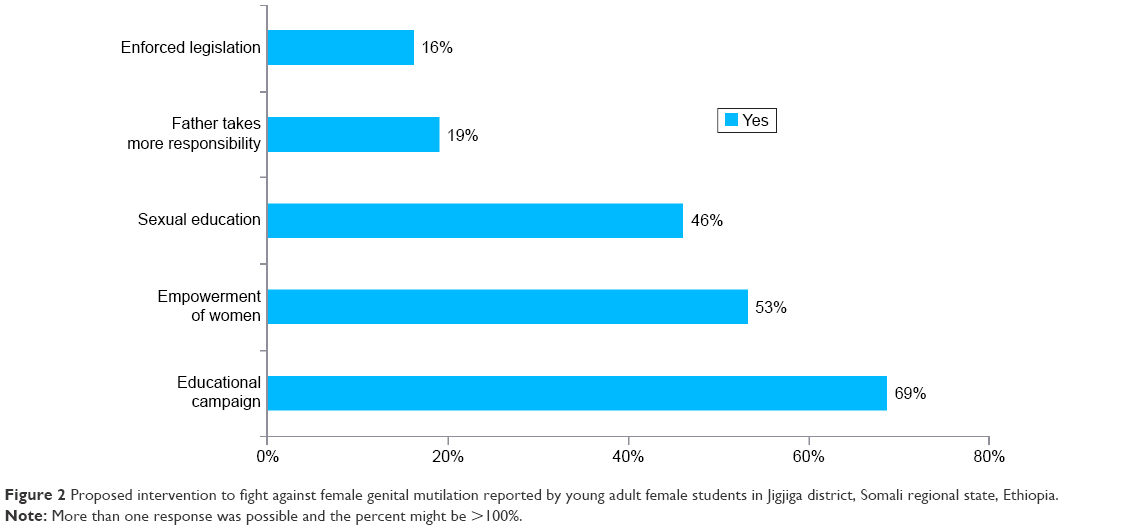 | Figure 2 Proposed intervention to fight against female genital mutilation reported by young adult female students in Jigjiga district, Somali regional state, Ethiopia. |
Discussion
The overall prevalence of female circumcision was as high as 82.6% among the respondents in this study. This was also supported by qualitative data where an uncircumcised woman was considered as hypersexual, infidel, non-Muslim, refused to marry, and nonpure. It is higher than that reported from the recent national figure (74%) and closely related with the Somali region (97.3%).13 The prevalence of FGC among 15–19 and 20–24 years old in this study was 77.3% and 89.5%, respectively. This finding is also higher than the national prevalence for 15–19 (62.1%) and 20–24 (73%) years of age and other sub-Saharan countries according to EDHS 2005.7,10,13,17,23 This might be because of the deep-seated negative values given by the society to the uncircumcised girl considered as unfaithful and hyperactive sexually. And the practice could be supported by the local religion and direct legal measure might not be taken seriously. Moreover, the overall prevalence in the study area on the younger group was somehow decreased, which might be attributed due to the time gap and the increasing understanding of parents about the harmful effects of FGC, which could be the result of different awareness-raising anti-FGC interventions implemented in the area and the advancement of educational provision as compared to the previous times. The reason could be due to sample size variation and skewing to one ethnicity when compared with that of the national study.
The most common age for FGC was as early as few days old for Christians; nevertheless, for the majority of respondents, 49.8% were circumcised during the age of 7–10. This study is closely related to the study conducted in Northern Amhara, Tigray, and Somali region refugee camps; for example, FGC is performed at infancy usually on the eighth day after birth and the age of 7 to 10.4,13,24 This study is also closely related to a study conducted in Egypt where 80% of girls were circumcised between the ages of 5 and 9 years and in Sudan where 20% of girls are between the age of 4 and 9 and 50% of girls are above 10.1 This shows that in Ethiopia, the age at which FGC is performed varies among the different ethnic groups. This finding is contrary to the study conducted in Sudan and report from EGLDMA 2009 where the probability of subjecting a girl to FGC increases beyond the age of 10.22,24 This inconsistency might be due to early initiation of menarche, that is, once the girls see menses, FGC is prohibited.
Regarding the forms of female circumcision, type I (Sunna or clitoral cutting) was becoming a dominant practice in this study and accounted for ~49.3% followed by infibulation, 45.3%. There is an increasing shift from infibulation to the less severe form of FGC among the respondents. The result is contrary with EDHS 2005; >80% of women in the Somali region have been victims of the most severe form of FGM, along with 60% in the Afar region.13 This is in line with a study done in Sudan; students who favor the practice believe that it is a religious dictate, especially type I FGC.18,22 The reason for the decrease might be due to fear of the legal repercussions from the government and the implementation of anti-FGC campaign activities. In addition, they believe that infibulation is not supported by religion. The higher rate and persistency might also be explained by religious demand and other social reasoning, such as an uncircumcised female is socially discriminated.
The finding of the study indicated that almost three-quarters of the FGC procedure was carried out by the local traditional circumciser (73%) and health professional (1.6%). This is in line with a study conducted in Somali refugee camps and other studies.2,4,13 This result signifies that society or the community believe that traditional practitioners are well experienced, and are therefore accepted and respected, allowing for FGC to continue. Health professional involvement in the procedure and lack of coordination in the fight against the practice may contribute for the continuation of FGC that needs attention for the anti-FGC intervention. Furthermore, health professionals involvement might help to reduce the spread of infectious disease by avoiding the use of unsterilized utensils and undertaking unnecessary procedures due to the FGC procedure done by someone who has no knowledge on the female anatomy.
In this study, most of the respondents, 88%, had good information and knowledge about the grave effect of FGC on women’s health. Their main sources of information were from mass media, anti-FGC intervention, school, and health professions. This is related with studies conducted in eastern Ethiopia, Oromia region, and other sub-Saharan countries.1,2,4,13,16,24,25 Though there is a good knowledge toward the practice, there is a gap between the prevalence and knowledge. Prevailing social pressure, religious demand, and having a positive attitude toward the practice is causing this gap.
The finding showed that the main reasons for the continuation of FGC were to keep virginity, to improve social acceptance, to have better chance of marriage, and have religious approval. This finding is in agreement with the studies conducted in Oromia region, Somali refugee camps, and in sub-Saharan African.4,10,13,21,24 This is also underpinned by the qualitative result that the practice is still to date commonly practiced in Somali region as a result of religious demand, social pressure, cultural identity, and psychosexual reasoning. This might be due to lack of knowledge and the prevailing negative attitude. The wrong attachment between the religion and practice may be attributed to the FGC, which has no scientific justification.
The prevalence of female circumcision was a significant predictor among rural respondents when compared to their counterparts in urban respondents. It was four times higher among rural respondents than those who lived in urban areas (AOR =4; 95% CI =2, 6.8). This is in line with the report of EDHS 2005.13 This may be because of the tight tradition and religious association and loose legal concern for the practice in the rural areas and may become a convenient place for the practice; additionally, rural women are mostly influenced by traditional practices. This may be as most anti-FGC interventions, health promotion through media, and legally punishable action might not addressed in rural areas as in urban areas.
Women’s education appears to be a positive and independent predictor for the occurrence of FGC in this study. Mothers who did not attend formal education are more likely to perform the procedure in their daughters when compared with those mothers who had completed secondary education and above. This finding is in agreement with a study conducted in Amhara and Oromia region which shows that maternal education was an independent and significantly associated predictor of FGC practice.4,26–28 This may be because educated women are able to make wise decisions about their own health and seek proper modern health care than their counterparts. This shows that improving education status of women is the most important factor that needs attention while aiming to reduce and abolish FGC. Education is likely to enhance female autonomy so that women develop great confidence and capability to make decision regarding their own health. Moreover, educated women are more likely to be aware of the risky effect of FGC and, as a result, they are more likely to fight against the practice.
Educational levels of the respondent were also an important independent predictor of FGC. The practice of FGC in this study was less likely to occur in those who were high school female students when compared with those who attend college level. This indicates that the current prevalence of FGC in the study area is decreased positively in high school students by 69% compared to college students (AOR =0.29; 95% CI =0.2, 0.45). This is consistent with studies done elsewhere.2,4,22,26 This may be due to increased awareness, knowledge, and attitude toward the bad effect of FGC on women health from time to time and the high school respondents were relatively younger.
Religious requirement for the practice was a significant predictor of FGC in the study area. The odds of female circumcision were 2.3 times more likely performed in those who believe FGC is required by their religion than those who did not believe (AOR =4.5; 95% CI =2.64, 7.55). This is in agreement with a study done in another part of Somali region4 and elsewhere.22 This may be due to deep-rooted values given for FGC by religion and sociocultural factors. Some religious leaders believe and recommend especially the Sunna (type I) form of circumcision. This practice may be wrongly attached with religion without having any logical reason and solid justification why they are associated. FGC is not referred to any reliable hadith while sharia law is clear on other points; Islam teaches respect, equality, and sexual pleasure for women. The verse (Quran: 4: 125) is only applicable to male circumcision but nothing is written about the Sunna form of FGC. Islam condemns harmful cultural practices, including female infanticide (Quran: 81: 8–9).
The attitude of the respondents significantly increases the intention toward the discontinuation of FGC in the young age group (62.3%), but there is a gap between the prevalence and attitude. This is higher than that reported from the recent figure in Somali region (25.7%) according to EDHS 2005.13 This may be clearly visible due to partaking in anti-FGC campaign, time variation, educational advancement, and a wide spread discouragement of the practice. This might be because FGC is a deeply-rooted norm, which is accepted by the society as a whole and by the women themselves. For example, men generally prefer to marry women who have undergone FGC as they might not want a woman who is sexually hyperactive and unfaithful.
Conclusion
Despite the girls’ knowledge and attitude toward the bad effects of FGC, the prevalence of FGC was high in this study. The direct and indirect effect of FGC on violation of human rights of girls/women may seriously affect the effort made toward realization of empowering women and sex equity. There should be a concerted effort among women, men, religious leaders, and other concerned bodies in understanding and clarifying the wrong attachment between the practice and religion through behavioral change communication and advocacy at all levels.
Acknowledgments
The authors are grateful to the study participants. The study was financially supported by the Addis Ababa University, School of Public Health.
Author contributions
KG designed the study, participated in the data collection, analysis, interpretation, and write-up, drafted the manuscript, and critically revised the manuscript. DA participated in the study design and critically revised the manuscript. FW participated in drafting the manuscript and critically revising the manuscript. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Rushwanu H. Female genital mutilation management during, pregnancy, childbirth & the postpartum period. Int J Gynaecol Obstet. 2012;70(1):99–104. | ||
Sayed GH, Abedl-Aty MA, Fadel KA. The practice of female genital mutilation in Upper Egypt. Int J Gynecol Obstet. 1996;55(3): 285–291. | ||
World Health Organization. Eliminating female genital mutilation: an interagency statement: UNAIDS, UNDP, UNECA, UNESCO, UNFPA, UNHCHR, UNHCR, UNICEF, and UNIFEM. Geneva, Switzerland: World Health Organization; Available from: www.who.int/reproductive-health | ||
Getnet M, Deressa W. Prevalence and associated factors of female genital mutilation among Somali refugees in eastern Ethiopia, 2009. Available from: http://www.biomedcentral.com/1471-2458/9/264/ | ||
Shell-Duncan B, Hernlund Y. Female “Circumcision” in Africa: Culture, Controversy, and Change. Boulder, CO: Lynne Rienner Publishers, Inc; 2000. | ||
Dara C. Female Genital Cutting: Findings from the Demographic and Health Survey. Calverton, MD: Macro International; 1997. | ||
World Health Organization &UNCEF2005a. Research on the elimination of female genital mutilation. Available from: who.int/mediacentre/factsheets/fs241/en/index.html. Accessed February 2012. | ||
Gender, Human Rights and Culture Branch, Technical Division, UNFPA. Global Consultation on Female Genital Mutilation/Cutting. Accessed August 2012. | ||
Sarkis M. The female genital cutting education and networking project female genital cutting (FGC). Available from: http://www.fgmnetwork.org/intro/fgmintro.html. Accessed July 19, 2016. | ||
Berg RC, Denison E. Interventions to reduce the prevalence of female genital mutilation/cutting in African countries. Campbell Syst Rev. 2012:9. | ||
Getachew I. Fighting female genital mutilation/cutting in Ethiopia’s Somali region. Addis Ababa: UNICEF; 2006. Available from: www.mbali.info/doc214.htm. Accessed July 27, 2016. | ||
Made Michael H. Ethiopia Young Adult Survey, Study in Seven Regions. UNFPA; 2010. | ||
Central Statistical Authority (CSA, Ethiopia). Ethiopian Demographic and Healthy Survey, Addis Ababa: Ethiopia; 2005. | ||
Tonje B, Aud T. The Norwegian International Effort against Female Genital Mutilation, Oslo: Norwegian Agency for Development Cooperation; July 2007. | ||
Bedri NM. Ending FGM/C through Evidence Based Advocacy in Sudan. AUW; March 2012. | ||
UNICEF. Female genital mutilation/cutting in Ethiopia. Available from: http://www.unicef.org/ethiopia/et_fgm.pdfonaugust2012 www.unicef.org/ethiopia/et_fgm.pdf%20on%20august%202012 | ||
World Health Organization, Female Genital Mutilation, Programmes to Date: What Works and What Doesn’t. Geneva: World Health Organization; 2011. | ||
Diop NJ, Askew I. The effectiveness of a community-based education program on abandoning female genital mutilation/cutting in Senegal. Int Perspect Sexual Reproduct Health. 2010;36(1):307–318. | ||
Sami A, ABU-Sahlie H. To Mutilate in the Name of Jehovah or Allah: Legitimization of Male and Female Circumcision. Available from: http://www.hollyfeld.org/fgm/refer/mutilate.html. Accessed February 2012. | ||
De Bruyn M. Discussion paper: socio-cultural aspects of female genital cutting. In Leye E, De Bruyn M, Meuwese S, editors. Proceedings of the Expert Meeting on Female Genital Mutilation; November 5–7, 1998; Ghent. ICRH Publications N°2. Lokeren: De Consulterij; 2003:68–82. | ||
MOH/GTZ FGM Project. Baseline survey on female genital mutilation practices in Koibatek district, Kenya, Rift Valley Province; 2001. | ||
Herieka E. Female genital mutilation in the Sudan: survey of the attitude of Khartoum university students towards this practice. Sex Transm Infect. 2003;79(3):220–223. | ||
WHO. Female Genital Mutilation, an Overview. Geneva: WHO; 1998. | ||
Ye Ethiopia Goji Limadawi Dirgitoch Aswogaj Mahiber (EGLDAM.) report, 2009, Addis Ababa, Ethiopia. | ||
Yirga WS, Kassa NA, Gebremichael MW, Aro AR. Female genital mutilation: prevalence, perceptions and effect on women’s health in Kersa district of Ethiopia. Int J Womens Health. 2012;4:45–54. | ||
Allam MF, de Irala-Estevez J, Fernandez-Crehuet Navajas R, et al. Factors associated with the condoning of female genital mutilation among university students. Public Health. 2001;115(5):350–355. | ||
Masho SW, Matthews L. Factors determining whether Ethiopian women support continuation of female genital mutilation. Int J Gynaecol Obstet. 2009;107(3):232–235. | ||
Abu-Bakr I, Iliyasu Z, Kabir M, Uzoho CC, Abdulkadir MB. Knowledge, attitude and practice of female genital cutting among antenatal patients in Aminu Kano Teaching Hospital. Niger J Med. 2004;13(3):254–258. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.