")
Back to Journals » Psychology Research and Behavior Management » Volume 12
Prevalence and associated factors of depression and anxiety among doctoral students: the mediating effect of mentoring relationships on the association between research self-efficacy and depression/anxiety
Authors Liu C , Wang L, Qi R, Wang W, Jia S, Shang D, Shao Y, Yu M, Zhu X, Yan S, Chang Q, Zhao Y
Received 19 November 2018
Accepted for publication 29 January 2019
Published 21 March 2019 Volume 2019:12 Pages 195—208
DOI https://doi.org/10.2147/PRBM.S195131
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Chunli Liu,1,2 Lie Wang,3 Ruiqun Qi,4,5 Weiqiu Wang,1 Shanshan Jia,6 Deshu Shang,7,8 Yangguang Shao,9,10 Min Yu,9,10 Xinwang Zhu,11 Shengnan Yan,12 Qing Chang,1 Yuhong Zhao1
1Department of Clinical Epidemiology, Shengjing Hospital of China Medical University, Shenyang, China; 2Department of Library and Medical Information, China Medical University, Shenyang, China; 3Department of Social Medicine, School of Public Health, China Medical University, Shenyang, China; 4Key Laboratory of Immunodermatology, Ministry of Health and Ministry of Education, China Medical University, Shenyang, China; 5Department of Dermatology, First Hospital of China Medical University, Shenyang, China; 6Key Laboratory of Health Ministry for Congenital Malformation, Shengjing Hospital of China Medical University, Shenyang, China; 7Department of Developmental Cell Biology, Key Laboratory of Medical Cell Biology, Ministry of Education, China Medical University, Shenyang, China; 8Department of Developmental Cell Biology, Cell Biology Division, Key Laboratory of Cell Biology, Ministry of Health, China Medical University, Shenyang, China; 9Department of Cell Biology, Key Laboratory of Cell Biology, National Health Commission of the PRC, China Medical University, Shenyang, China; 10Department of Cell Biology, Key Laboratory of Medical Cell Biology, Ministry of Education, China Medical University, Shenyang, China; 11Department of Nephrology, First Affiliated Hospital of China Medical University, Shenyang, China; 12Graduate Division, School of Public Health, China Medical University, Shenyang, China
Purpose: Although the mental health status of doctoral students deserves attention, few scholars have paid attention to factors related to their mental health problems. We aimed to investigate the prevalence of depression and anxiety in doctoral students and examine possible associated factors. We further aimed to assess whether mentoring relationships mediate the association between research self-efficacy and depression/anxiety.
Methods: A cross-sectional study was conducted among 325 doctoral students in a medical university. The Patient Health Questionnaire 9 and Generalized Anxiety Disorder 7 scale were used to assess depression and anxiety. The Research Self-Efficacy Scale was used to measure perceived ability to fulfill various research-related activities. The Advisory Working Alliance Inventory-student version was used to assess mentoring relationships. Linear hierarchical regression analyses were performed to determine if any factors were significantly associated with depression and anxiety. Asymptotic and resampling methods were used to examine whether mentoring played a mediating role.
Results: Approximately 23.7% of participants showed signs of depression, and 20.0% showed signs of anxiety. Grade in school was associated with the degree of depression. The frequency of meeting with a mentor, difficulty in doctoral article publication, and difficulty in balancing work–family–doctoral program was associated with both the level of depression and anxiety. Moreover, research self-efficacy and mentoring relationships had negative relationships with levels of depression and anxiety. We also found that mentoring relationships mediated the correlation between research self-efficacy and depression/anxiety.
Conclusion: The findings suggest that educational experts should pay close attention to the mental health of doctoral students. Active strategies and interventions that promote research self-efficacy and mentoring relationships might be beneficial in preventing or reducing depression and anxiety.
Keywords: mental health, major depressive disorder, generalized anxiety disorder, Advisory Working Alliance, research self-efficacy, doctoral students
Introduction
Recently, the mental health status of students has become a hot topic in public health, higher education, and research policy.1–3 Depression and anxiety are two of the most common psychological disorders. Researchers have reported depression and anxiety among students in several countries and in numerous disciplines, such as counseling, medicine, law, and psychology.4–14 Depression is defined as a mood that includes a feeling of hopelessness, helplessness, or worthlessness.2 Anxiety is an emotion characterized by unpleasant inner feelings, which is accompanied by caution, complaints, meditation, nervousness, and worry.5 Depression and anxiety can affect a person’s behavior, academic performance, and general health, as well as quality of sleep, eating habits, and well-being.8 In addition, it has been confirmed that depression and psychological distress influence suicidal ideation in undergraduate and graduate students.15–18 However, mental health among doctoral students has been relatively ignored by researchers and educational experts. It has only been in the last 2 years that this topic has begun to attract more and more attention.
A doctoral student’s school career is full of hardships and happiness. Doctoral students frequently feel a sense of urgency, worry, and stress as they work toward their doctoral degrees. In addition to financial support and future employment, doctoral students worry about writing a thesis, publishing papers, and handling relationships with advisors. In recent years, a few scholars have explored the prevalence of mental health problems among PhD students.3,12,19–21 In 2013, Levecquea et al investigated PhD students in Belgium. They concluded that approximately half the PhD students in Flanders had at least two symptoms, and 32% reported at least four symptoms on the 12-item General Health Questionnaire (GHQ12).3 According to a 2015 survey at the University of California, approximately half the PhD students in science and engineering were depressed.12 Springer Nature did a survey of PhD students in 2017, and confirmed that 12% reported seeking help for anxiety or depression caused by PhD studies.20 A 2018 survey of graduate students via social media revealed that 41% of graduate students scored in the moderate–severe range for anxiety and 39% scored in the moderate–severe range for depression.21 Doctoral students with mental health issues are more likely to drop out of PhD programs.22 The high attrition rate in PhD programs caused by the dropout of PhD students with psychological illness is damaging to research institutions and the whole research industry.23 However, there have been few reports on the mental health of doctoral students in medical universities.
Students in medical schools engage in rigorous medical training.24,25 Previous studies have demonstrated that medical students have more pressure, more burnout, and a greater prevalence of mental health disorders than the general population or students in other disciplines.26–31 Medical training varies considerably by discipline, institution, and country. US and Canadian medical students enter medical education systems after they receive a bachelor’s degree.32,33 In China, students can enter medical schools after graduating from high school (similarly to the UK and France). In general, there is an entrance examination required for students with a master’s degree who would like to study for doctoral degrees. Doctoral students need another 3 years to earn a doctoral degree, allowing for an extension of 3 years. Master’s degree candidates in grade two have the choice to apply for a master–doctor combined-training program (a total of 5 years for a doctoral degree, allowing an extension of 3 years). Doctoral students can be either full-time or part-time students. Part-time doctoral students are those who are studying doctoral courses while working in clinical settings or having another job. As such, for clinical doctoral students, some are still fully engaged in clinical work while earning their doctoral degree, whereas others are temporarily away from clinical work to concentrate on the doctoral program research. It is a bit too much to expect clinical doctoral students to do clinical work and research at the same time throughout their doctoral training.
Sociodemographic variables, such as age, sex, and marital status, have been reported to be associated with the mental health of postgraduate students.8,10 However, sex differences in depression among medical students have also yielded mixed results, showing either no difference or high prevalence among female or male medical students.27,29,33 Further exploration among doctoral students is still needed. The execution phase during doctoral study has been shown to be prone to mental health problems among doctoral students.3 Additionally, researchers have suggested that work–life balance is the key factor related to the mental health problems of postgraduate students.3,21 Employed doctoral students work full time or part time while they are studying for their doctoral degree. In this case, conflict concerns not only balancing family and work but also completing the doctoral program itself. Few scholars have focused on the conflicts among family, work, and a doctoral program. Getting married and raising children also puts a strain on doctoral students. Doing experiments, writing a doctoral thesis, and publishing doctoral qualification papers requires considerable time, energy, and financial resources.
Mentorship effectiveness and mentoring functions are thought to be vital to graduate-student programs.34,35 Mentors have a great responsibility to guide their doctoral students through the doctoral program. Advisor mentoring affects student-research self-efficacy, productivity, and development as a scientist.36–38 Recently, a study explored the effect of a supervisor’s leadership style on the mental health of graduate students.3 Nearly half the doctoral students who withdrew from the doctoral program reported experiencing insufficient supervision, highlighting the fact that good supervision was important for completing the doctoral program.39,40 A survey in 2018 indicated that a weak relationship with a mentor is a common characteristic of most graduate students who experience anxiety and/or depression.21
Research self-efficacy refers to the individual’s confidence in the successful completion of various aspects of the scientific research process,41 such as data collection, performing experimental procedures, and writing papers.42 Studies have evaluated the important role of research self-efficacy in research training. Self-efficacy is a factor that affects how much effort students spend on research tasks and how long they persist when they experience difficulties.43 Some universities in the US have used research self-efficacy to evaluate the effects of degree programs on graduate research ability.44 A study has shown that research self-efficacy can predict the research interest and knowledge of doctoral students.45 Some researchers have reported that high research self-efficacy is correlated with future research involvement and research productivity.46,47 It was suggested that research self-efficacy could play a mediating role between the research-training environment and scientific research output. Furthermore, the relationship between stress and depression has been shown to be mediated by stress management self-efficacy.48 Interestingly, the length of student–advisor relationships has been reported to be significantly correlated with student research self-efficacy.36 Moreover, among agricultural students, research self-efficacy has been found to be negatively associated with research anxiety.49 Therefore, the higher the students’ research self-efficacy, the lower their research anxiety. However, it is not clear whether scientific research self-efficacy is correlated with levels of generalized anxiety.
In this study, we aimed to investigate the prevalence of depression and anxiety among doctoral students in a medical university in China, determine factors that are associated with depression and anxiety, determine whether mentoring relationships and research self-efficacy are associated with depression and anxiety, and test whether mentoring relationships mediate the association between research self-efficacy and depression/anxiety.
Methods
Participants
We recruited doctoral students from October to November 2017 using a combination of snowball sampling and stratified sampling from five medical schools and four affiliated clinical hospitals at a medical university in northeast China. This university has the authority to grant doctoral degrees in six major disciplines (basic medicine, clinical medicine, biology, stomatology, public health and preventive medicine, and nursing), including 49 different majors. Our inclusion criteria were still studying at the medical university, had not yet earned a PhD degree, enrollment in a successive postgraduate and doctoral program, and no history of depression or anxiety before entering medical school. A total of 437 doctoral students (218 male, 219 female) were enrolled. This study received approval from the Committee for Human Trials of China Medical University (CMU17/375/R). Written informed consent was obtained from all participants before they entered the experiment. All questionnaires were filled out anonymously and confidentially.
Sociodemographic and doctoral factors
Doctoral students’ sociodemographic status included age, sex, marital status, children, and income. In addition, we selected some doctoral characteristics that might affect the mental health of doctoral students. We asked participants whether they had been employed before doctoral enrollment. Clinical doctoral students refers to students who were doing clinical work while earning their doctoral degree. Grade was measured assigned to one of four categories (1, first year; 2, second year; 3, third year; 4, fourth year or above). Mentors meet with their doctoral students regularly or irregularly. They come together and analyze the latest literature, discuss the research direction or experimental methods, and revise the thesis. Therefore, the frequency of these meetings can reflect the strength of the relationship from a certain quantitative angle. The frequency with which doctoral students met with mentors was measured with one item: “On average, how often do you meet with your advisor? (1, at least once a week; 2, at least once a month; 3, seldom)”. In most medical universities, doctoral students are required to publish at least one academic paper indexed by the Science Citation Index or Social Science Citation Index. Only when this qualification has been reached are doctoral students able to apply for a doctoral degree. The perceived difficulty in publishing a doctoral qualification paper was assessed by one item: “How much effort do you think it takes to publish doctoral qualification papers? (1, a little bit of effort; 2, some effort; 3, a lot of effort). Considering that the total time and energy of doctoral students is limited, we asked the doctoral students, “Do you have difficulty in balancing work, family, and the PhD program? (1, almost no difficulty; 2, some difficulty; 3, great difficulty)”.
Depression questionnaire
We chose the nine-item Patient Health Questionnaire (PHQ-9)50 to evaluate depression among doctoral students. Each item is measured on a 4-point Likert-like scale (0, not at all; 3, almost every day) based on the frequency of depression symptoms over the last 2 weeks. Total scores range from 0 to 27. A higher PHQ-9 score represents more serious depression (0–4, none–minimal; 5–9, mild; 10–14, moderate; 15–19, moderately severe; 20–27, severe). In general, a diagnosis of depression can only be arrived at after clinical assessment by a mental health professional. With such questionnaires as the PHQ-9, it has been shown that at certain cutoffs there is good correlation with diagnostic interviews. PHQ-9 scores of 10 or above had a sensitivity of 88% and a specificity of 88% for major depressive disorder.50 The Chinese version of the PHQ-9 has been used in older people and hospital inpatients, with sound reliability. In the current study, Cronbach’s alpha for the PHQ-9 scale was 0.918.
Anxiety questionnaire
We used the seven item Generalized Anxiety Disorder (GAD-7) to indicate the degree of anxiety among doctoral students.51 The GAD-7 contains seven items that are rated on a 4-point Likert-like scale (0, not at all; 3, almost every day). The total score ranges from 0 to 21. A higher GAD-7 score indicates more serious anxiety (0–4, none–minimal; 5–9, mild; 10–14, moderate; 15–21, severe). Using a threshold score of 10, the GAD-7 has a sensitivity of 89% and a specificity of 82% for major generalized anxiety disorder.51 The Chinese version of the GAD-7 has been used in outpatients with satisfactory reliability. In the present study, Cronbach’s alpha for the GAD-7 scale was 0.946.
Mentoring-relationship questionnaire
The 30-item Advisory Working Alliance Inventory-student version (AWAI-S) was used to assess the mentoring relationship from the student’s perspective.36 This scale is a brief, self-reported measure designed on the basis of the Working Alliance model. Its developer, Schlosser, believed that a favorable supervisory alliance was vital to outcomes.52 The scale has had good reliability in previous studies.53 The AWAI-S consists of three domains: rapport (11 items), apprenticeship (14 items), and identification-individuation (5 items). Each item is rated on a 5-point Likert scale (1, strongly disagree; 5, strongly agree). The AWAI-S scale contains 16 reverse-scoring questions. High scores (after reverse scoring) suggest that the advisee has a strong mentoring relationship with the advisor. The internal consistency of AWAI-S scores from previous studies ranged from 0.84 to 0.9536,54 and was 0.95 in this study.
Research Self-Efficacy Scale
The Research Self-Efficacy Scale (RSES) was used to measure the doctoral students’ perceived ability to fulfill various research-related tasks.55 The RSES comprises 50 items with four subscales: conceptualization (18 items), implementation (19 items), early tasks (5 items), and presenting the results (8 items). Individuals were asked to mark the tasks they perceived they could perform. The strength of each item was rated on a 10-point scale ranging from 0 (no confidence) to 10 (complete confidence). A total RSES score was calculated, ranging from 75 to 500. A higher score indicates higher self-efficacy. The internal consistency of RSES scores was 0.98 in the present study.
Data analysis
We used SPSS 17.0 for all statistical analyses. We investigated demographic and doctoral characteristics using ANOVA for continuous variables and chi-squared for categorical data. Correlations among depression, anxiety, mentoring relationships, and research self-efficacy were examined by Pearson correlation. We performed hierarchical linear regression analysis to explore the association of mentoring relationship and research self-efficacy with depression/anxiety. In this study, depression and anxiety were modeled as dependent variables, RSES as an independent variable, AWAI-S as a mediator, and sociodemographic and doctoral variables as controlled variables. In step 1 of the regression, sociodemographic and doctoral variables were entered as controlled variables. Because linear hierarchical regression analysis requires continuous variables, the grade, frequency of meeting with a mentor, difficulty in publishing a doctoral qualification paper, and difficulty in balancing work–family–doctoral program was dummy coded. In step 2 of the regression, research self-efficacy was added. In step 3, the mentoring relationship was added. The asymptotic and resampling method was used to examine mentoring relationship as potential mediator in the association between research self-efficacy and depression/anxiety, based on 5,000 bootstrap samples.56 A bias-corrected and accelerated (BCa) 95% CI was used to estimate mediation. If the BCa 95% CI excludes 0, this indicates that the mediation is significant. All statistical tests were two-sided (α=0.05). P<0.05 was considered statistically significant.
Results
Sociodemographic and doctoral characteristics of respondents
After exclusion of 45 doctoral students who refused to fill out questionnaires, the 392 who completed the questionnaires were included. A total of 67 questionnaires with missing values >10% were deemed invalid. As such, we collected 325 valid responses. The effective response rate was 74.37%. The mean age of the participants was 31.1±5.3 (23–47) years. Of the 325 respondents, 60.3% were female, 50.8% married or lived with a partner, and 40% had one or more child. The monthly income for 56.6% of respondents was <CN¥3,000 per month (equivalent of local per capita income), 50.8% had been employed before doctoral enrollment, and 40.6% were clinical doctoral students. Furthermore, 13.8% seldom met with their mentors, 37.2% thought they should try their best to publish a PhD qualification paper, and 31.1% reported that they had difficulty in balancing work–family–PhD (Table 1).
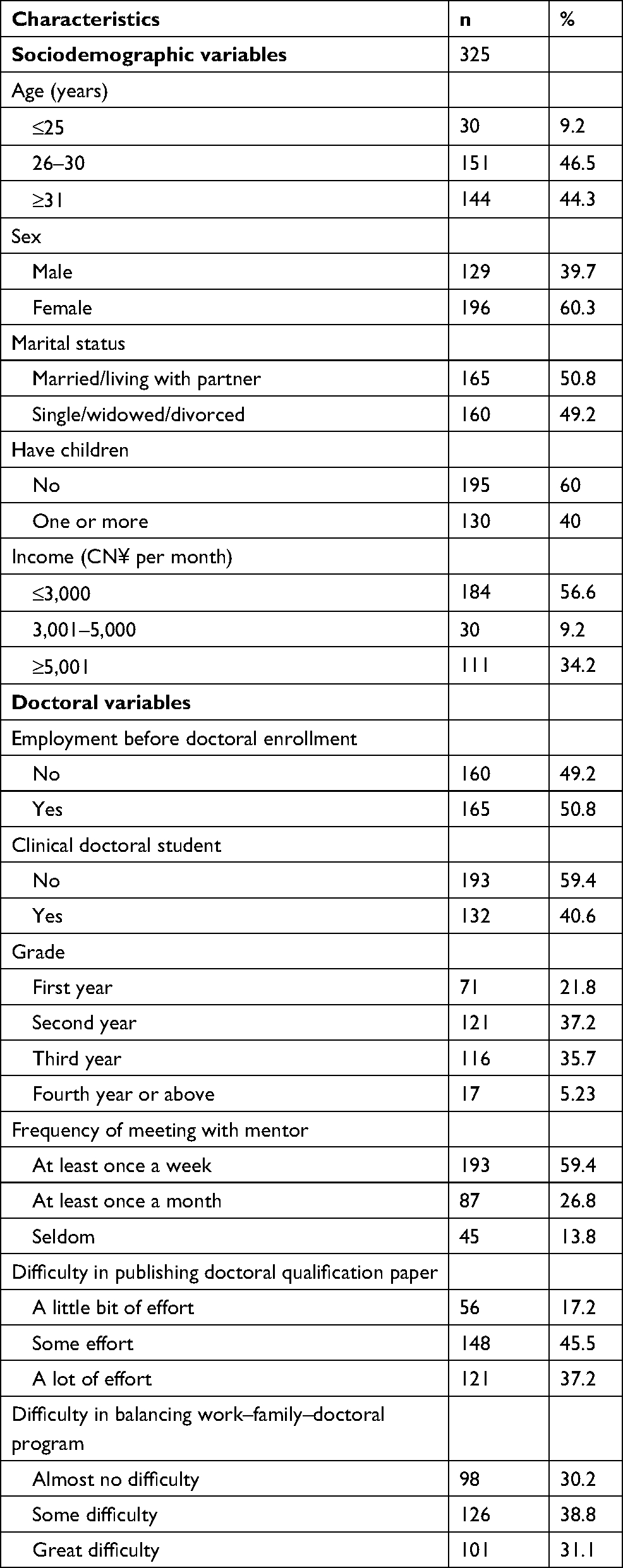 | Table 1 Sociodemographic and doctoral characteristics of respondents (n=325) |
Sociodemographic and doctoral characteristics by depression and anxiety
The prevalence of clinical depression was 23.7% (moderate, moderately severe, and severe) and the prevalence of clinical anxiety was 20.0% (moderate and severe; Tables 2 and 3). Factors that were significantly different among respondents at varying levels of depression included age, marital status, having children, employment, grade, frequency of meeting with mentors, difficulty in publishing, and difficulty in balancing work–family–doctoral program. Factors that were significantly different among respondents at varying levels of anxiety included being a clinical doctoral student, frequency of meeting with mentors, difficulty in publishing, and difficulty in balancing work–family–doctoral program.
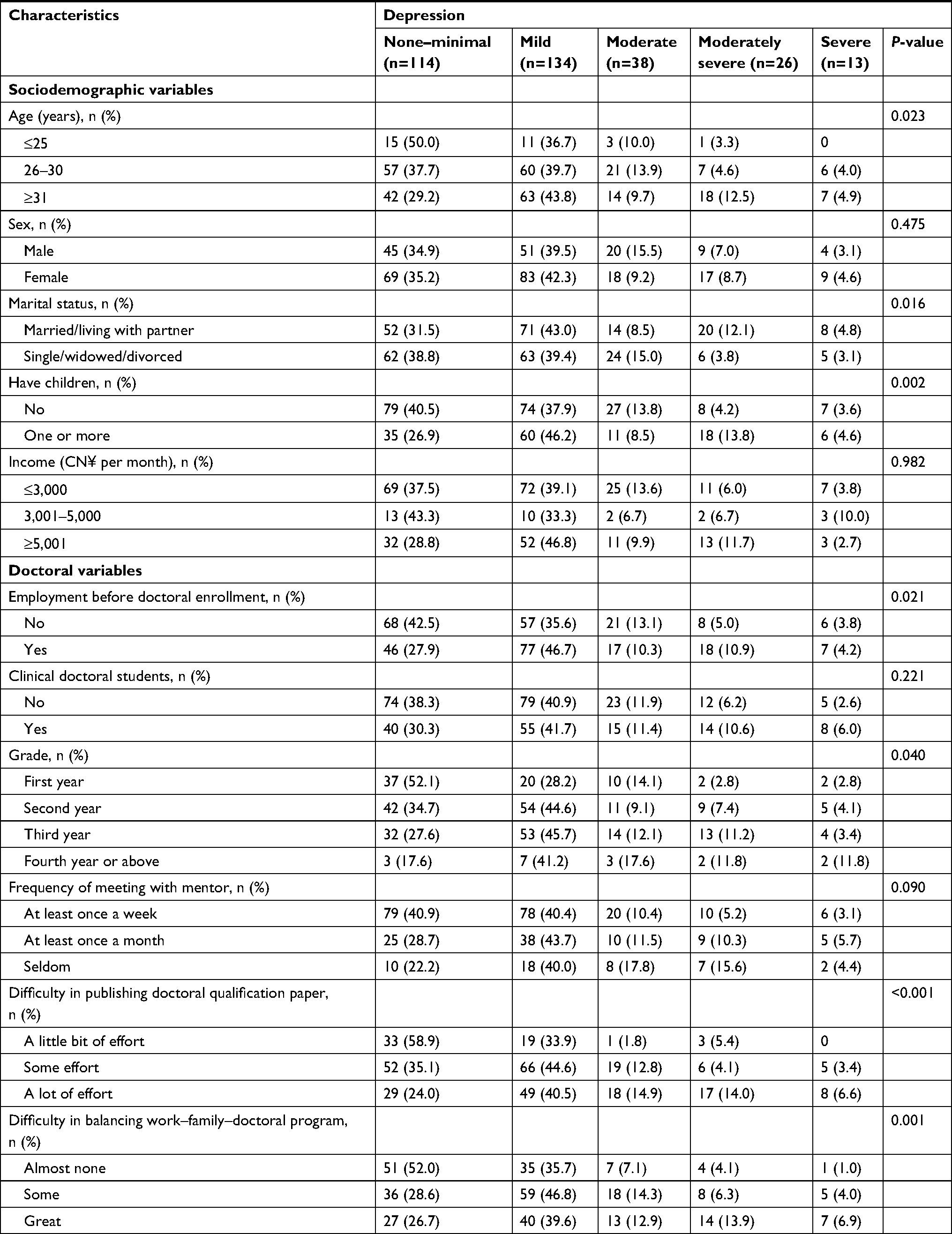 | Table 2 Sociodemographic and doctoral characteristics by depression (n=325) |
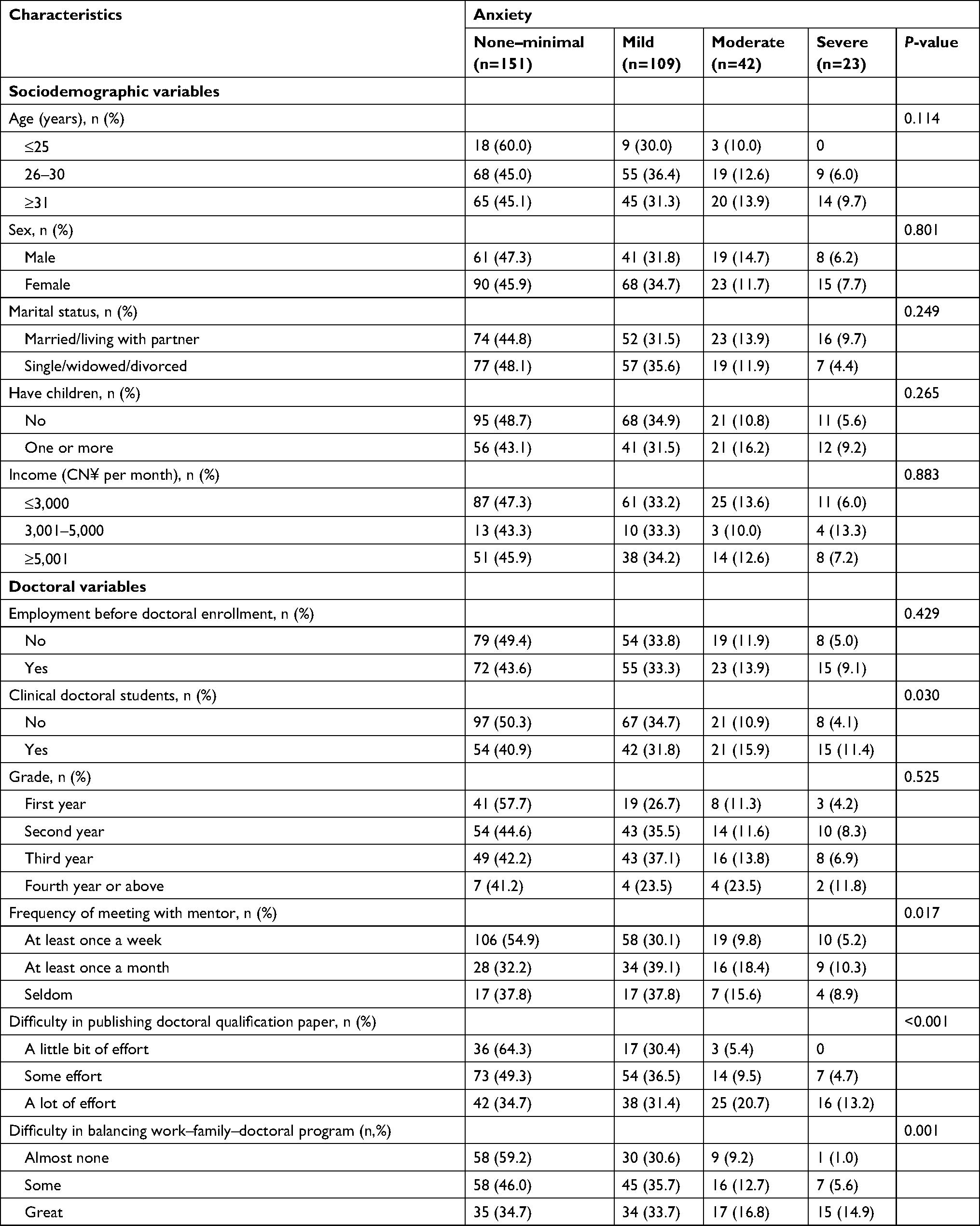 | Table 3 Sociodemographic and doctoral characteristics by anxiety (n=325) |
Means and correlations among age and PHQ-9, GAD-7, AWAI-S, and RSES scores
Mean scores for the PHQ-9, GAD-7, and AWAI-S and their correlations with each other and age are presented in Table 4. Age was positively associated with the PHQ-9. However, there was no significant effect of age on the GAD-7. Both PHQ-9 and GAD-7 scores were negatively associated with AWAI-S and RSES scores.
 | Table 4 Correlations among age, AWAI-S, RSES, PHQ-9, and GAD-7 scores Note: *P<0.05; **P<0.01. Abbreviations: AWAI-S, Advisory Working Alliance Inventory-student version; GAD, Generalized Anxiety Disorder; PHQ, Patient Health Questionnaire; RSES, Research Self-Efficacy Scale. |
Associations of mentoring relationship and research self-efficacy with depression/anxiety
As shown in Tables 5 and 6, sociodemographic and doctoral variables contributed to 17.7% of the variance in PHQ-9 scores and to 18.3% of the variance in GAD-7 scores. Doctoral students in their fourth year had greater PHQ-9 and GAD-7 scores than first-year doctoral students. Compared with those who met with their mentors at least once a week, doctoral students who met with their mentors only once a month had higher PHQ-9 and GAD-7 scores. Moreover, respondents who reported that they had to try their best to publish doctoral qualification papers had higher PHQ-9 and GAD-7 scores than those who felt they only had to put forth a little effort. Finally, doctoral students who had great difficulty in balancing work–family–doctoral program exhibited a higher level of depression and anxiety than those who had almost no difficulty.
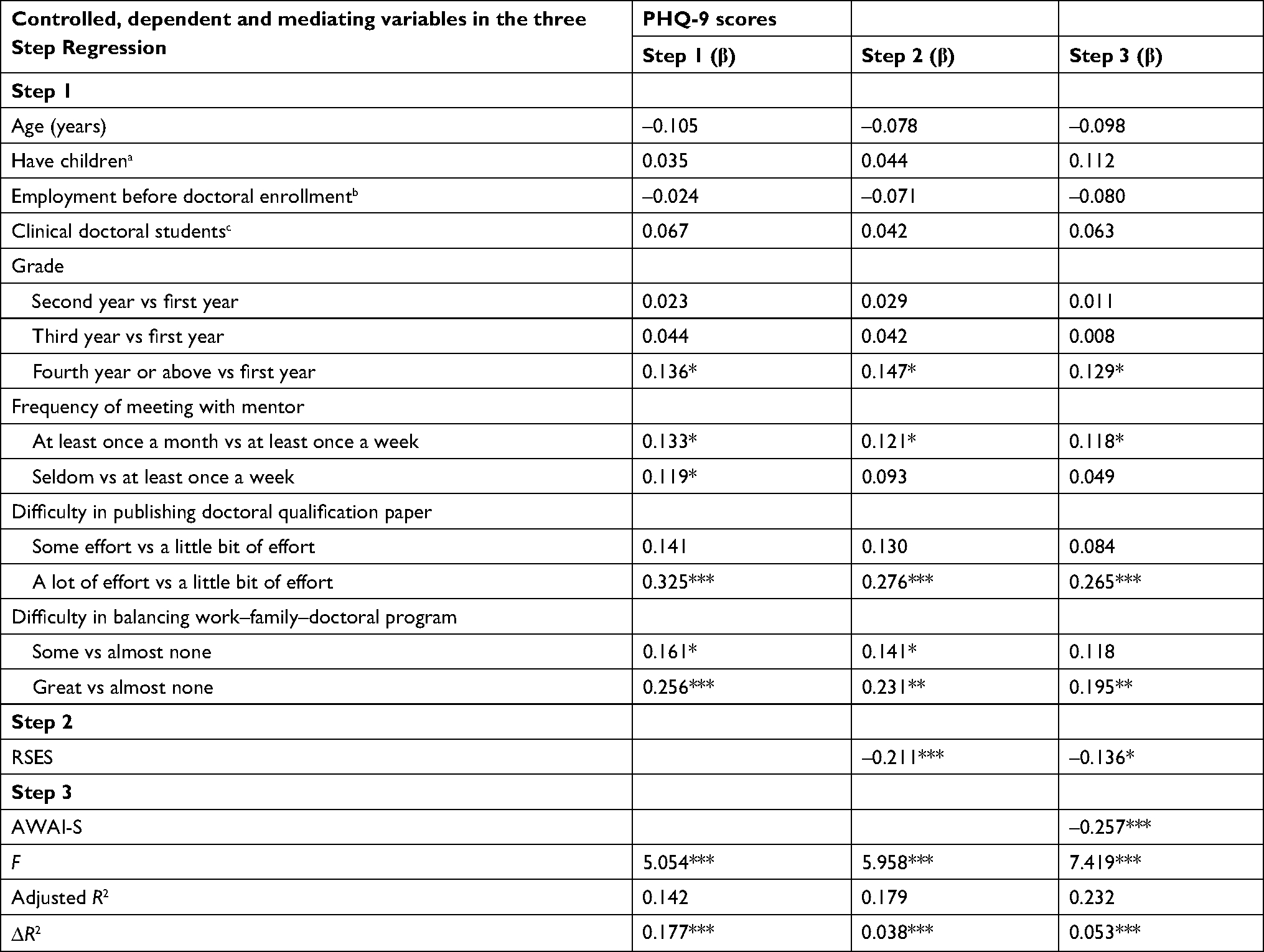 | Table 5 Factors related to depression using hierarchical regression analysis Notes: a1, Have no children; 2, have one or more children. b1, Not employed before doctoral enrollment; 2, employed before doctoral enrollment. c1, Not clinical doctoral students; 2, clinical doctoral students. Grade, doctoral grade. *P<0.05 (two-tailed); **P<0.01 (two-tailed); ***P<0.001 (two-tailed). Abbreviation: PHQ, Patient Health Questionnaire. |
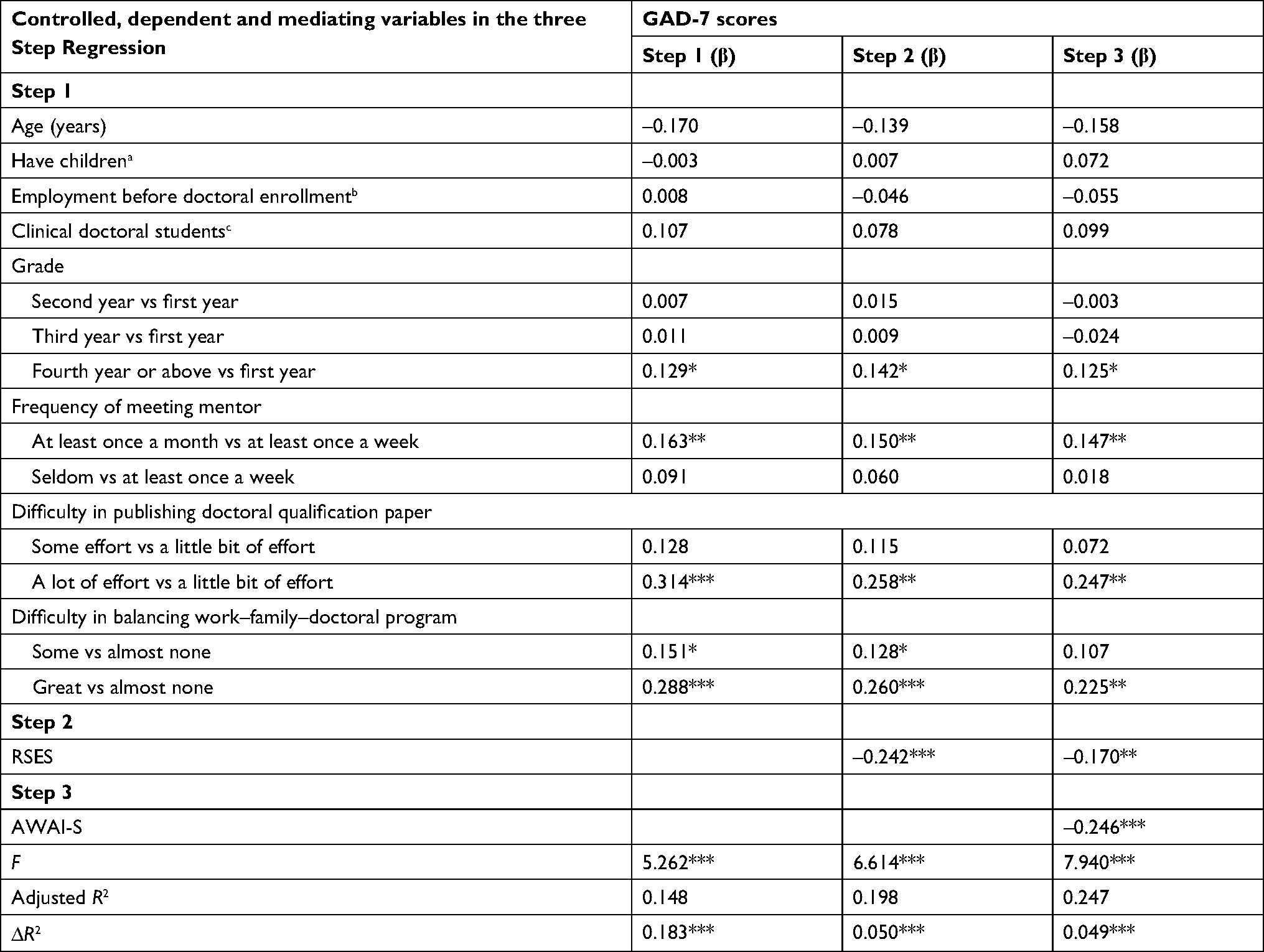 | Table 6 Factors related to anxiety using hierarchical regression analysis Notes: a1, Have no children; 2, have one or more children. b1, Not employed before doctoral enrollment; 2, employed before doctoral enrollment. c1, Not clinical doctoral students; 2, clinical doctoral students. Grade, doctoral grade. *P<0.05 (two-tailed); **P<0.01 (two-tailed); ***P<0.001 (two-tailed). Abbreviation: GAD, Generalized Anxiety Disorder. |
After adjustment for controlled variables, the RSES was negatively associated with depression (b=–0.211, P<0.001) and anxiety (b=–0.242, P<0.001), and accounted for 3.8% of the variance for depression and 5.0% of the variance for anxiety. In step 3, the AWAI-S was negatively associated with depression (b=–0.257, P<0.001) and anxiety (b=–0.246, P<0.001), and accounted for 5.3% of the variance for depression and 4.9% of the variance for anxiety. In step 3, when the AWAI-S was added, the absolute value of RSES b was diminished. Therefore, the AWAI-S might be a mediator in the association between research self-efficacy and depression/anxiety.
Mediating role of mentoring relationship
As shown in Table 7 and Figure 1, research self-efficacy had a significantly negative correlation with depression/anxiety (c). Research self-efficacy correlated with the mentoring relationship (a). Mentoring relationship correlated with depression/anxiety negatively (b). BCa 95% CI for a×b of the mentoring relationship did not include 0, indicating that mentoring relationship partially mediated the relationship between research self-efficacy and depression/anxiety (c’). Mentoring relationship explained 37.68% of the variance for depression and 29.73% of the variance for anxiety.
 | Table 7 Bootstrapping test of indirect effect of mentoring relationship acting as mediator on association between research self-efficacy and depression/anxiety Notes: a×b, indirect effect of research self-efficacy on depression/anxiety via mediator mentoring relationship; c, association between research self-efficacy and depression/anxiety; a, association between research self-efficacy and mentoring relationship; b, association between mentoring relationship and depression/anxiety; c’, association between research self-efficacy and depression/anxiety after adding mentoring relationship as mediator. *P<0.05; **P<0.01; ***P<0.001. Abbreviations: BCa, bias-corrected and accelerated; GAD, Generalized Anxiety Disorder; PHQ, Patient Health Questionnaire. |
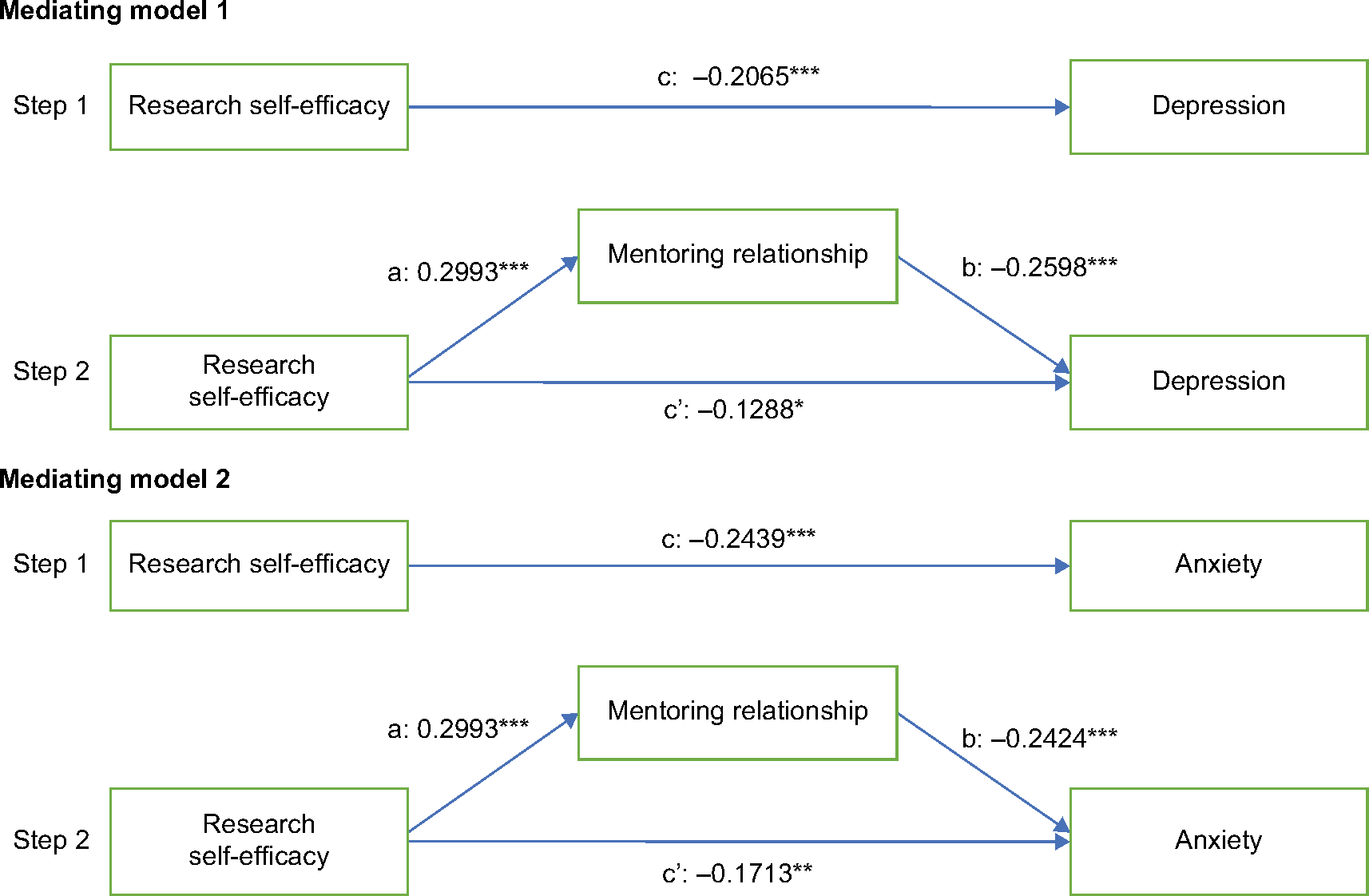 | Figure 1 Theoretical model through which mentoring relationship mediates association between research self-efficacy and depression/anxiety. Notes: c, Association between research self-efficacy and depression/anxiety; a, association between research self-efficacy and mentoring relationship; b, association between mentoring relationship and depression/anxiety; c’, association between research self-efficacy and depression/anxiety after adding mentoring relationship as a mediator. *P<0.05; **P<0.01; ***P<0.001. |
Discussion
We found that depression and anxiety symptoms are common among doctoral students in medical universities. Approximately 41.2% of doctoral students showed symptoms of mild depression and 23.7% showed signs of moderate–severe depression. Moreover, 33.5% of the students had mild anxiety symptoms and 20.0% had moderate–severe anxiety symptoms. Researchers worldwide have used the same scales to carry out epidemiological surveys on depression and/or anxiety. An investigation indicated that 53.8% of undergraduate college students at Emory University had moderate–severe depression.57 In 2017, it was reported that 29.2% of medical students in Nepal had moderate–severe depression.58 Evans et al conducted a survey that included 90% PhD students and 10% master’s students. Results suggested that 39% of postgraduates had moderate–severe depression and 41% moderate–severe anxiety.21 Differences in terms of score and positive rate might be related to differing methodologies. Levesque et al found that 33.33% of doctoral students experienced a common psychiatric disorder (GHQ12), such as depression. A PhD candidate was 2.4 times more likely to develop psychiatric health problems than someone in the general population with a bachelor’s degree.3 Bernstein reported that 42% of PhD students in science and 48% of PhD students in engineering at the University of California were depressed on the Center for Epidemiologic Studies Depression Scale.12 The psychological stress of medical doctoral students is much higher than that of students with other majors, and students in medical schools have more symptoms of depression than the general population.26,29 However, few reports have focused on the mental health of doctoral students in Chinese medical universities.
Research self-efficacy negatively correlated with depression and anxiety. However, few researchers have reported such an association. Mee found that self-efficacy mediated the relationship between smoking behavior and depression.59 Pu et al verified that dispositional optimism partially mediated the relationship between self-efficacy and depression.60 Razavi et al reported a negative relationship between self-efficacy (General Self-Efficacy Questionnaire) and research anxiety among master’s and PhD students at Islamic Azad University.61 In addition, we found that research self-efficacy (RSES) and mentoring relationship (AWAI-S) correlated significantly. This result was consistent with a previous study.64 Research self-efficacy has often been studied in relation to research-training environments and research productivity.47,62 Lambie et al found that among PhD students, research self-efficacy was associated with research interest and knowledge.45
Our study indicated that the association between research self-efficacy and depression/anxiety was partly mediated by the mentoring relationship. As for strategies for promoting research self-efficacy of doctoral students, Overall et al found that high levels of autonomy and strong levels of academic support were associated with higher levels of research self-efficacy. Likewise, students with lower research self-efficacy experienced lower levels of autonomy and lower levels of personal support.44 Love et al reported that supportive peers or supervisors contributed to positive research experience. Positive team-research experiences were able to predict research self-efficacy.63 As such, the correlation between mentoring relationship and research self-efficacy might be bidirectional.
Our results also indicated that mentoring relationship correlated with depression and anxiety. Studies suggest that the mentoring relationship is positively correlated with research self-efficacy and negatively correlated with student stress.53,54,64,65 Peluso et al found that the academic advisor relationship played a role in protecting the mental health of experimental psychology students in Canada.10 Gottschall also showed a significant association between a harmonious mentoring relationship (RHI-M subscale) and decreased depressive symptoms among Canadian graduate students.66 In addition, Lunsford suggested that mentoring by doctoral advisors correlated with student outcomes, including satisfaction and academic production.37
Most importantly, we found that mentoring relationship mediated the correlation between research self-efficacy and depression/anxiety. As far as we know, this issue has not been studied before. The empirical findings in this study have very important applications for general doctoral training strategies and specific interventions for depression and anxiety. The mediating effect suggests that active strategies and interventions that promote research self-efficacy and mentoring relationships might benefit the mental health of doctoral students. Developing courses related to choosing research topics, performing experiments, analyzing data, and writing papers are good strategies for improving research self-efficacy. We should encourage doctoral students to participate in research practices and academic exchange. In addition, we should monitor mentoring relationships, depression, and anxiety by mixed methods at regular intervals, with students’ permission. If we find poor relationships between mentors and their mentees, we must recognize this issue’s importance and adopt flexible methods to deal with it. For example, we should allow the student to change mentors or give them more research support from another faculty.
The percentage of scores that could be categorized as depression and anxiety in the fourth year or above was higher than that in any other grade. Senior students might face more pressure from the institution, the need to graduate, financial burdens, and finding a job than is faced by more junior students. Our findings are in line with a survey in Vietnam, which indicated that major depression and general anxiety rates of medical students were higher in the fifth grade than in the first grade.67 In contrast, a study of undergraduates in Brazil discovered that 30.8% of first-year students and 9.4% of sixth-year students presented anxiety.68 Levecque et al observed that mental health problems were more prevalent at the beginning of the PhD program than in the execution phase. This difference with our results could be due to cross-cultural differences in training systems and graduation requirements.
The frequency with which mentees met with their mentors showed a significant relationship with depression and anxiety. This measure is a function of the mentors in terms of quantity. Under great academic pressure, doctoral students who often met with their mentors were less stressed than those who seldom met with their mentors. An ideal situation is that the advisor is accessible at almost all times. Besides weekly group meetings, students should schedule a weekly one-on-one session with an advisor. Students who meet less frequently with their mentor are more likely to be depressed when they encounter difficulties. Moreover, the duration of each meeting and the content of the meeting might also play a vital role in completion of the doctoral program.
Our results also suggest that difficulty in publishing a doctoral qualification paper has a significant effect on depression and anxiety. This has also become one of the main factors preventing students from completing the doctoral degree. Certainly, doctoral students who have greater academic self-efficacy might have less academic pressure and a low risk of mental health problems. In recent years, many policies have been implemented to increase the number of doctoral students enrolled, develop master–doctor combined programs, and expand the requirements for a doctoral degree. However, the cultivation of mentoring ability, availability of funding for doctor training, and assistance for doctoral students in mastering experiments and writing papers are still lacking. Such problems might not only be related to increasing the risk of mental health disorders but might also correlate with deferred graduation, increased dropout rates, and academic misconduct.
Finally, it has been shown that doctoral students who have difficulty in balancing work–family–doctoral program will have a greater risk of depression and anxiety than those who have almost no difficulty. An imbalance among family, work, and doctoral program places great pressure on doctoral students and seriously hampers their progress in doctoral programs, which leads to poorer mental health and even poorer physical health. Although the effect of work–life balance on mental health has been identified in the past,69,70 only in recent years has work–life–doctoral program balance been taken seriously. Sapey, a scientist in the UK, has pointed out that work–life balance in academia is a challenge for her.71–73 She said that she has balanced two vocations (clinical and academic work) and a family (mother of a child), sometimes very badly, sometimes reasonably, and only very, very occasionally has she handled it very well. Is there any successful family–work–doctoral program balance experience from which to learn? Bellucci and Nancy performed a qualitative investigation of PhD nursing students in the US, and suggested that multiple time management and stress management strategies would play a crucial role in balancing the responsibilities of work, family, and a PhD program.74 Martinez et al interviewed full-time doctoral education students and categorized balancing school–work–life into four themes: purposeful management, well-being, support, and tradeoffs.75
Limitations
Several limitations of this study should be mentioned. First, we performed only an exploratory survey of doctoral students in a medical university. We will perform a multicenter investigation in multiple cities in the future. Second, it was a cross-sectional study. The results of this study did not reveal causality. We expect to conduct a longitudinal study on associated themes. Further studies should include qualitative measures as well.
Conclusion
Our study has provided insight into the prevalence and factors associated with depression and anxiety among doctoral students in China. Our study revealed that 23.7% of doctoral students showed signs of depression and 20.0% signs of anxiety. Our findings indicated that research self-efficacy and mentoring relationships were protective factors for depression and anxiety. Mentoring relationship mediated the association between research self-efficacy and depression/anxiety. In addition, we revealed that the frequency of meeting with mentors, difficulty in publishing a doctoral qualification paper, and difficulty in balancing work–family–doctoral program were significantly associated with both depression and anxiety. Our findings also indicated that year in school was also associated with depression and anxiety. These findings suggest that policymakers and managers in medical universities should pay close attention to the mental health of doctoral students. Potential interventions might include (but are not limited to) promoting research self-efficacy of doctoral students, monitoring the mentoring relationship, and developing courses that teach how to perform various tasks necessary for obtaining a doctoral degree.
Acknowledgments
This study was funded by the Liaoning Province Education Science 13th Five-Year Plan 2017 of China (No. JG17DB564) and the National Natural Science Foundation of China (No. 71473268). We would like to thank the experts who have offered us constructive suggestions. We would like to acknowledge all the faculty and students for their great help in distributing questionnaires and collecting data.
Disclosure
The authors report no conflicts of interest in this work.
References
Kernan W, Bogart J, Wheat ME. Health-related barriers to learning among graduate students. Health Educ. 2011;111(5):425–445. | ||
Eisenberg D, Gollust SE, Golberstein E, Hefner JL. Prevalence and correlates of depression, anxiety, and suicidality among university students. Am J Orthopsychiatry. 2007;77(4):534–542. | ||
Levecque K, Anseel F, de Beuckelaer A, van der Heyden J, Gisle L. Work organization and mental health problems in PhD students. Res Policy. 2017;46(4):868–879. | ||
Jungbluth C, Macfarlane IM, Veach PM, Leroy BS. Why is everyone so anxious? An exploration of stress and anxiety in genetic counseling graduate students. J Genet Couns. 2011;20(3):270–286. | ||
Shete A, Garkal KD. A study of stress, anxiety, and depression among postgraduate medical students. CHRISMED J Health Res. 2015;2(2):119. | ||
Helmers KF, Danoff D, Steinert Y, Leyton M, Young SN. Stress and depressed mood in medical students, law students, and graduate students at McGill university. Acad Med. 1997;72(8):708–714. | ||
Taniya A, Kumar A. Level of anxiety and depression among postgraduate psychology students. Int J Indian Psychol. 2015;2(2):121–127. | ||
Farrer LM, Gulliver A, Bennett K, Fassnacht DB, Griffiths KM, et al. Demographic and psychosocial predictors of major depression and generalised anxiety disorder in Australian university students. BMC Psychiatry. 2016;16(1):1–9. | ||
Madhan B, Rajpurohit AS, Gayathri H. Mental health of postgraduate orthodontic students in India: a multi-institution survey. J Dent Educ. 2012;76(2):200–209. | ||
Peluso DL, Carleton RN, Asmundson GJG. Depression symptoms in Canadian psychology graduate students: do research productivity, funding, and the academic advisory relationship play a role? Can J Behav Sci/Revue canadienne des sciences du comportement. 2011;43(2):119–127. | ||
Sturman ED, Mongrain M. Entrapment and perceived status in graduate students experiencing a recurrence of major depression. Can J Behav Sci/Revue canadienne des sciences du comportement. 2008;40(3):185–188. | ||
Bernstein R. Depression afflicts almost half of STEM graduate students at UC Berkeley. Available from: http://www.sciencemag.org/careers/2015/05/depression-afflicts-almost-half-stem-graduate-students-uc-berkeley. Accessed May 20, 2018. | ||
University staff scared to disclose mental health problems; 2015. Available from: http://www.theguardian.com/education/2015/feb/13/university-staff-scared-to-disclose-mental-health-problems. Accessed May 20, 2018. | ||
Feng Q, Zhang QL, Du Y, Ye YL, He QQ. Associations of physical activity, screen time with depression, anxiety and sleep quality among Chinese College freshmen. PLoS One. 2014;9(6):e100914. | ||
Meng H, Li J, Loerbroks A, Wu J, Chen H. Rural/urban background, depression and suicidal ideation in Chinese college students: a cross-sectional study. PLoS One. 2013;8(8):e71313. | ||
Garcia-Williams AG, Moffitt L, Kaslow NJ. Mental health and suicidal behavior among graduate students. Acad Psychiatry. 2014;38(5):554–560. | ||
Tang F, Byrne M, Qin P. Psychological distress and risk for suicidal behavior among university students in contemporary China. J Affect Disord. 2018;228:101–108. | ||
Smith SS, Smith Carter J, Karczewski S, Pivarunas B, Suffoletto S, Munin A. Mediating effects of stress, weight-related issues, and depression on suicidality in college students. J Am Coll Health. 2015;63(1):1–12. | ||
Elisabeth Pain. Ph.D. students face significant mental health challenges. 2017. Available from: http://www.sciencemag.org/careers/2017/04/phd-students-face-significant-mental-health-challenges. Accessed April 4, 2017. | ||
Woolston C. Graduate survey: a love-hurt relationship. Nature. 2017;550:549–552. | ||
Evans TM, Bira L, Gastelum JB, Weiss LT, Vanderford NL. Evidence for a mental health crisis in graduate education. Nat Biotechnol. 2018;36(3):282–284. | ||
Stubb J, Pyhältö K, Lonka K. The experienced meaning of working with a PHD thesis. Scand J Educ Res. 2012;56(4):439–456. | ||
Gardner SK. Student and faculty attributions of attrition in high and low-completing doctoral programs in the United States. Higher Education. 2009;58(1):97–112. | ||
Grendar J, Beran T, Oddone-Paolucci E. Experiences of pressure to conform in postgraduate medical education. BMC Med Educ. 2018;18(1):4. | ||
Shi M, Liu L, Wang ZY, Wang L. Prevalence of depressive symptoms and its correlations with positive psychological variables among Chinese medical students: an exploratory cross-sectional study. BMC Psychiatry. 2016;16(1):3. | ||
Rotenstein LS, Ramos MA, Torre M, et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students. JAMA. 2016;316(21):2214–2236. | ||
Puthran R, Zhang MW, Tam WW, Ho RC. Prevalence of depression amongst medical students: a meta-analysis. Med Educ. 2016;50(4):456–468. | ||
Bacchi S, Licinio J. Qualitative literature review of the prevalence of depression in medical students compared to students in non-medical degrees. Acad Psychiatry. 2015;39(3):293–299. | ||
Hope V, Henderson M. Medical student depression, anxiety and distress outside North America: a systematic review. Med Educ. 2014;48(10):963–979. | ||
Divaris K, Polychronopoulou A, Taoufik K, Katsaros C, Eliades T. Stress and burnout in postgraduate dental education. Eur J Dent Educ. 2012;16(1):35–42. | ||
McLuckie A, Matheson KM, Landers AL, Landine J, Novick J, Barrett T, Dimitropoulos G. The relationship between psychological distress and perception of emotional support in medical students and residents and implications for educational institutions. Acad Psychiatry. 2017;1:1–7. | ||
Cyranoski D, Gilbert N, Ledford H, Nayar A, Yahia M. Education: the PHD factory. Nature. 2011;472(7343):276–279. | ||
Dyrbye LN, Thomas MR, Shanafelt TD. Systematic review of depression, anxiety, and other indicators of psychological distress among U.S. and Canadian medical students. Acad Med. 2006; 81(4):354-373. | ||
Lechuga VM. Faculty-graduate student mentoring relationships: mentors’ perceived roles and responsibilities. Higher Education. 2011;62(6):757–771. | ||
Busch JW. Mentoring in graduate schools of education: mentors’ perceptions. Am Educ Res J. 1985;22(2):257–265. | ||
Schlosser LZ, Gelso CJ. Measuring the working alliance in advisor-advisee relationships in graduate school. J Counsel Psychol. 2001;48(2):157–167. | ||
Lunsford L. Doctoral advising or mentoring? Effects on student outcomes. Mentoring Tutoring: Partnership Learning. 2012;20(2):251–270. | ||
Gelso CJ. Research in counseling: methodological and professional issues. Counsel Psychol. 1979;8(3):7–35. | ||
Lee A. How are doctoral students supervised? concepts of doctoral research supervision. Stud High Educ. 2008;33(3):267–281. | ||
Raffing R, Jensen TB, Tønnesen H. Self-reported needs for improving the supervision competence of PHD supervisors from the medical sciences in Denmark. BMC Med Educ. 2017;17(1):188. | ||
Kahn JH, Scott NA. Predictors of research productivity and science-related career goals among counseling psychology doctoral students. Counsel Psychol. 1997;25(1):38–67. | ||
Forester M, Kahn JH, Hesson-Mcinnis MS. Factor structures of three measures of research self-efficacy. J Career Assess. 2004;12(1):3–16. | ||
van Dinther M, Dochy F, Segers M. Factors affecting students’ self-efficacy in higher education. Educ Res Rev. 2011;6(2):95–108. | ||
Overall NC, Deane KL, Peterson ER. Promoting doctoral students’ research self-efficacy: combining academic guidance with autonomy support. Higher Edu Res Dev. 2011;30(6):791–805. | ||
Lambie GW, Hayes BG, Griffith C, Limberg D, Mullen PR. An exploratory investigation of the research self-efficacy, interest in research, and research knowledge of Ph.D. in education students. Innovat High Educ. 2014;39(2):139–153. | ||
Lei SA. Factors changing attitudes of graduate school students toward an introductory research methodology course. Education. 2008;128(4):667–685. | ||
Bieschke KJ. Research self-efficacy beliefs and research outcome expectations: implications for developing Scientifically Minded PSYCHOLOGISTS. J Career Assess. 2006;14(1):77–91. | ||
Sawatzky RG, Ratner PA, Richardson CG, et al. Stress and depression in students: the mediating role of stress management self-efficacy. Nurs Res. 2012;61(1):13. | ||
Rezaei M, Zamani-Miandashti N. The relationship between research self-efficacy, research anxiety and attitude toward research: a study of agricultural graduate students. J Educ Instruct Stud World. 2013;3(4):69–78. | ||
Kroenke K, Spitzer Rl, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–613. | ||
Swinson RP. The GAD-7 scale was accurate for diagnosing generalised anxiety disorder. Evid Based Med. 2006;11(6):184. | ||
Bordin ES. A working alliance based model of supervision. Counsel Psychol. 1983;11(1):35–42. | ||
Rice KG, Suh H, Yang X, Choe E, Davis DE. The advising Alliance for international and domestic graduate students: measurement invariance and implications for academic stress. J Couns Psychol. 2016;63(3):331–342. | ||
Morrison MA, Lent RW. The Advisory working alliance and research training: test of a relational efficacy model. J Couns Psychol. 2014;61(4):549–559. | ||
Bieschke KJ, Bishop RM, Garcia VL. The utility of the research self-efficacy scale. J Career Assess. 1996;4(1):59–75. | ||
Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008;40(3):879–891. | ||
Garlow SJ, Rosenberg J, Moore JD, et al. Depression, desperation, and suicidal ideation in college students: results from the American foundation for suicide prevention college screening project at Emory University. Depress Anxiety. 2008;25(6):482–488. | ||
Adhikari A, Dutta A, Sapkota S, Chapagain A, Aryal A, Pradhan A. Prevalence of poor mental health among medical students in Nepal: a cross-sectional study. BMC Med Educ. 2017;17(1):232. | ||
Mee S. Self-efficacy: a mediator of smoking behavior and depression among college students. Pediatr Nurs. 2014;40(1):9–15. | ||
Pu J, Hou H, Ma R. Direct and indirect effects of self-efficacy on depression: the mediating role of dispositional optimism. Curr Psychol. 2016;36(3):1–7. | ||
Razavi SA, Shahrabi A, Siamian H. The relationship between research anxiety and self-efficacy. Mater Sociomed. 2017;29(4):247–250. | ||
Gelso CJ, Mallinckrodt B, Judge AB. Research training environment, attitudes toward research, and research self-efficacy: the revised research training environment scale. Counseling Psychologist. 1996;24(2):304–322. | ||
Love KM, Bahner AD, Jones LN, Nilsson JE, et al. An investigation of early research experience and research self-efficacy. Prof Psychol Res Pract. 2007;38(3):314–320. | ||
Schlosser LZ, Lyons HZ, Talleyrand RM, Kim BSK, Johnson WB. Advisor-advisee relationships in graduate training programs. J Career Dev. 2011;38(1):3–18. | ||
Wei M, Tsai PC, Chao RC, Du Y, Lin SP. Advisory working alliance, perceived English proficiency, and acculturative stress. J Couns Psychol. 2012;59(3):437–448. | ||
Gottschall S. The influences of sex, gender identity and power on faculty-graduate student relational mentoring and its association with student psychological health. 2014. Available from: https://curve.carleton.ca/a165bace-60c2-437b-b57b-1a5ffaac1627. Accessed June 3, 2018. | ||
Tan N, Ro K, Dong T, et al. Symptoms of depression and anxiety: a study of first and fifth year medical students in Vietnam. Med Edu. 2016;20(2):73–81. | ||
Bassols AM, Okabayashi LS, Silva AB, et al. First- and last-year medical students: is there a difference in the prevalence and intensity of anxiety and depressive symptoms? Braz J Psychiatry. 2014;36(3):233–240. | ||
Jang SJ, Park R, Zippay A. The interaction effects of scheduling control and work-life balance programs on job satisfaction and mental health. Int J Soc Welfare. 2011;20(2):135–143. | ||
Hämmig O, Bauer G. Work-life imbalance and mental health among male and female employees in Switzerland. Int J Pub Health. 2009;54(2):88–95. | ||
Sapey E. Work–life balance in academic medicine. Lancet. 2015;385(Suppl 1):S6–S7. | ||
Rafnsdóttir GL, Heijstra TM. Balancing work-family life in academia: the power of time. Gender Work Organization. 2013;20(3):283–296. | ||
Currie J, Eveline J. E-technology and work/life balance for academics with young children. Higher Education. 2011;62(4):533–550. | ||
Bellucci NA. A qualitative investigation of strategies used by PHD nursing students for balancing work, family, and the attainment of a PHD; 2016. Available from: https://search.proquest.com/openview/f0b9aee5e5120ae3fdd5702455748d1b/1?pq-origsite=gscholar&cbl=18750&diss=y. Accessed July 3, 2017. | ||
Martinez E, Ordu C, Della Sala MR, et al. Striving to obtain a school-work-life balance: The full-time doctoral student. Int J Doc Stud. 2013;8:39–59. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.