")
Back to Journals » OncoTargets and Therapy » Volume 11
Pretreatment hematologic markers as prognostic predictors of gastroenteropancreatic neuroendocrine tumors: a systematic review and meta-analysis
Authors Zhou Y, Li D, Lin Y, Yu M, Lu X, Jian Z, Na N, Hou B
Received 27 September 2017
Accepted for publication 18 February 2018
Published 1 May 2018 Volume 2018:11 Pages 2489—2496
DOI https://doi.org/10.2147/OTT.S152657
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Geoffrey Pietersz
Yu Zhou,1,* Dezhi Li,1,* Ye Lin,1,* Min Yu,1 Xin Lu,1 Zhixiang Jian,1 Ning Na,2 Baohua Hou1
1Department of General Surgery, Guangdong General Hospital, Guangdong Academy of Medical Sciences, Guangzhou, Guangdong, People’s Republic of China; 2Department of Kidney Transplantation, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, Guangdong, People’s Republic of China
*These authors contributed equally to this paper
Background: Systemic inflammation can be reflected by peripheral hematologic parameters and combined index like the lymphocyte count, neutrophil count, platelet count, neutrophil-to-lymphocyte (NLR), and platelet-to-lymphocyte ratio (PLR). This systematic review and meta-analysis aimed to summarize the association between the hematologic markers and prognosis of gastroenteropancreatic neuroendocrine tumors (GEP–NETs).
Methods: A computerized systematic search of PubMed, Embase, and Web of Science was conducted up to August 2016. Studies evaluating prognosis value of hematologic parameters in patients with GEP–NETs were retrieved. For meta-analysis, hazard ratios (HRs) with 95% confidence intervals (95% CIs) were extracted and synthesized using Review Manager software.
Results: We identified eight retrospective cohort studies comprising a total of 724 cases. The majority of included studies focused on pancreatic neuroendocrine tumors (PNETs). The prognostic values of NLR, PLR, and platelet count were reported in six studies, two studies, and one study, respectively. All the parameters were associated with prognostic outcomes in patients with GEP–NETs. A high NLR was significantly associated with poor prognosis in GEP–NETs (pooled HR 3.05, 95% CI 1.96–4.76, I2 = 0%, P < 0.00001 for overall survival (OS); pooled HR 3.30, 95% CI 2.04–5.32, I2 = 0%, P < 0.00001 for recurrence-free survival [RFS]). In PNETs, pooled-analyses also showed significant superiority of a low NLR on OS (pooled HR 4.21, 95% CI 1.95–9.13, I2 = 0%, P = 0.0003) and RFS (pooled HR 5.37, 95% CI 2.14–13.47, I2 = 0%, P = 0.003).
Conclusions: These findings suggest that the elevated NLR could be an adverse prognosis factor for GEP–NETs. The conclusion should be mainly limited to PNETs as the majority of included cases were PNET patients. The prognostic value of other hematologic parameters deserves further investigation. We recommend that further studies should use a continuous NLR variable and adopt a prospective and matched study design.
Keywords: neuroendocrine tumor, blood cell, lymphocyte, neutrophil, platelet, prognosis
Introduction
Gastroenteropancreatic neuroendocrine tumors (GEP–NETs) are biologically diverse neoplasms that arise from the diffuse endocrine system in the gastrointestinal tract and/or pancreas.1 In recent decades, GEP–NETs have exhibited a significantly increased incidence,2 and today comprise approximately 2% of all malignant gastrointestinal tumors.3 Due to the highly heterogeneous features and unpredictable biological behaviors of GEP–NETs, discovery of markers with efficient diagnosis and/or prognosis effect could help determine optimal clinical managements and follow-up strategies.4–7
The link between chronic inflammation and cancer has been established for a long time.8,9 Numerous epidemiologic studies support a clear connection between chronic inflammation and the development of many cancers. In turn, the tumor itself can initiate and maintain inflammatory processes that foster tumor growth and development. Many inflammation-related cytokines and chemokines have been extensively documented in cancers of the stomach, liver, lung, esophagus, breast, and prostate. In addition, an important hallmark of cancer is that cancer cells evade immunological attack, and recent studies have identified that chronic inflammation is associated with immunosuppression, mediated primarily by immature myeloid-derived suppressor cells.10–12
Studies in the past decades have identified a close connection between GEP–NETs and chronic inflammation. It was shown that chronic inflammation can lead to hyperplasia and neoplastic transformation of enteroendocrine cells.13–15 Additionally, single nucleotide polymorphisms of some inflammatory cytokines, such as TNF-α –1031T/C, IL-6 –174 C/G, and IL-2 –330T/G allele, have been identified to be associated with the overall susceptibility to develop GEP–NETs.16–18 Nowadays, many typical factors of systematic inflammation, such as C-reactive protein, interleukin, some growth factors and chemokines have been validated as predictive in various types of cancer.19–21 Recently, emerging studies have focused upon the prognosis value of hematologic parameters of systemic inflammation, including leukocyte counts, neutrophil counts, platelet counts, and the ratios between them such as neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) because they are cheap and easily acquired markers during clinical practice.22–26 Hence, we aimed to conduct a systematic review and meta-analysis to evaluate the prognostic value of hematologic parameters in patients with GEP–NETs.
Methods
Study identification and selection
A systematic literature search of PubMed, Embase, and the Institute for Scientific Information (ISI) Web of Knowledge was conducted in August, 2017, by two independent reviewers (Yu Zhou & Dezhi Li) to retrieve potential relevant studies with restriction to English language. We used Mesh terms and text words to retrieve potential eligible studies with the following retrieval logic: (“neutrophil” or “lymphocyte” or “leukomonocyte” or “monocyte” or “platelet” or “thrombocyte” or “blood cell” or “blood routine” or “hematologic” or “hematological”) and (“neuroendocrine tumor” or “neuroendocrine tumour” or “neuroendocrine neoplasm” or “neoplasm cancer” or “neoplasm malignancy” or “carcinoid” or “insulinoma” or “vipoma” or “gastrinoma” or “paraganglioma”). We did not limit the search based on tumor site of gasteoenteropancreatic organs in case of missing articles. Reference lists of the retrieved articles were also searched for relevant studies. The initial selection was performed to eliminate obviously irrelevant articles, reviews, meeting abstracts, comments, letters, and basic research. We retained potentially relevant articles about hematologic parameters or GEP–NET prognostic risk factors by reviewing the titles and abstracts. Thereafter, the full-text was reviewed. Studies of patients with GEP–NETs that evaluated the effect of at least one of the hematologic parameters on prognosis were included.
Data extraction and quality assessment
The investigators (Yu Zhou & Dezhi Li) extracted information independently using a standardized data extraction table. The information about the basic characteristics of included studies and population, details of methodological characteristics, and relevant outcomes were recorded, including first author, year of publication, study period, study design, sample size, clinicopathologic characters of the study cohort, cut-off value of hematologic parameters, method of statistical analysis, and clinical outcomes. The hazard ratio (HR) was preferred for evaluating the survival outcome since it is time-to-event data. The values of HRs, 95% CIs, and P-values were extracted. For studies that did not provide sufficient data, the HR values were obtained by contacting the corresponding authors or were estimated by the methods described by Tierney et al.44 The primary outcomes were cancer-specific survival (CSS) and overall survival (OS). The secondary outcomes included recurrence-free survival (RFS), distal metastasis-free survival (DMFS), local relapse-free survival (LRFS), and progression-free survival (PFS). There are no standard quality-assessment tools for prognostic studies in systematic reviews. The Newcastle-Ottawa Quality Assessment Scale (NOS) was adopted to assess the quality of each included study independently by our two investigators. NOS scores more than 6 were considered as high-quality studies. The two investigators had discussions to reach a consensus when there was any disagreement.
Statistical analysis
All the synthesis analyses were carried out using the Review Manager software (Version 5.3, The Cochrane Collaboration, Copenhagen, Denmark). A two-tailed P-value < 0.05 was considered statistically significant. HRs with 95% CIs were used to evaluate the prognosis value of hematological parameters (high level vs low level). When the study reported both univariate and multivariate results, we chose multivariate analysis for final calculation. Cochran’s Q test and Higgins I2 statistic were performed for evaluating heterogeneity among studies. Studies with a P ≥ 0.1 or I2 < 50% were considered to have low heterogeneity and the fixed-effects model was used. Otherwise, the random-effects model was applied. A funnel plot was performed to assess publication bias.
Ethics approval
Since this was a protocol for a systematic review based upon available evidence, ethics approval was not required.
Results
Data retrieval
Figure 1 shows the flow chart for study search and selection. After searching the database of PubMed, Embase, and ISI Web of Knowledge, we finally identified 716 relevant references, of which 226 were duplicated. After removing duplicate articles, and further screening titles and abstracts, 389 articles were excluded, including laboratory investigations, case reports, meeting abstracts, comments, letters, reviews, and other articles irrelevant to our topic. After the full-text review, a total of eight studies were ultimately included.
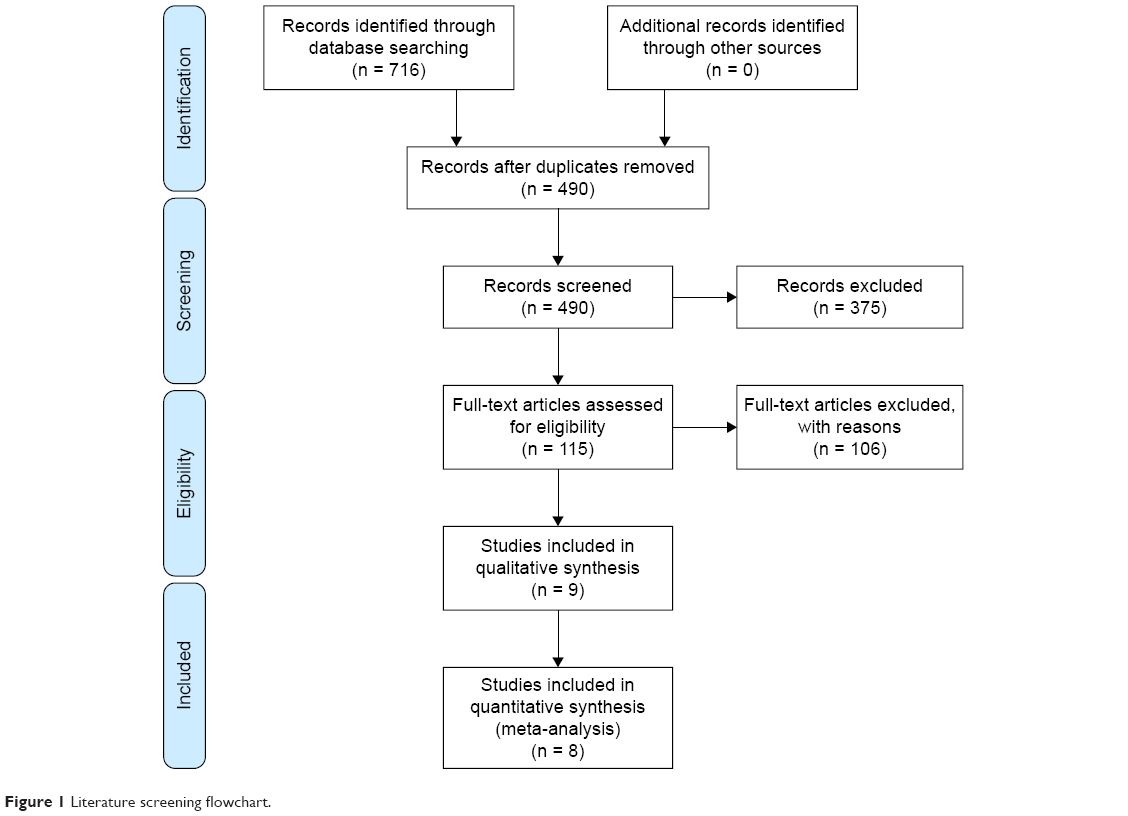 | Figure 1 Literature screening flowchart. |
Characteristics of studies and data quality
Tables 1 and 2 show the characteristics of included studies. The eight eligible studies were published between 2009 and 2017, and all were retrospective analysis.27–34 A total of 724 cases were involved, and the sample sizes of included studies ranged from 34 to 165. Five studies only enrolled PNETs patients,27–30,34 one study only enrolled patients with gastric neuroendocrine tumors (G–NETs),31 one study enrolled patients with gastro-entero-pancreatic neuroendocrine tumors (GEP–NETs),32 and another study enrolled patients with neuroendocrine tumors regardless of the primary site.33 The prognosis values of NLR were reported in six articles,27–29,31–33 the prognosis values of PLR were reported in two articles,34 and only one study reported the prognosis value of platelet count.30 Most studies determined the cut-off values of the hematologic markers by using receiver operating characteristic (ROC) curves to select the most significant points. The HRs for survival outcomes were provided in seven studies.27–31,33,34 and all of them were adjusted for potential confounders using the Cox proportion hazard model. The NOS scores of the included studies ranged from 6 to 7. The major inadequacies among the included studies were incomparability between groups.
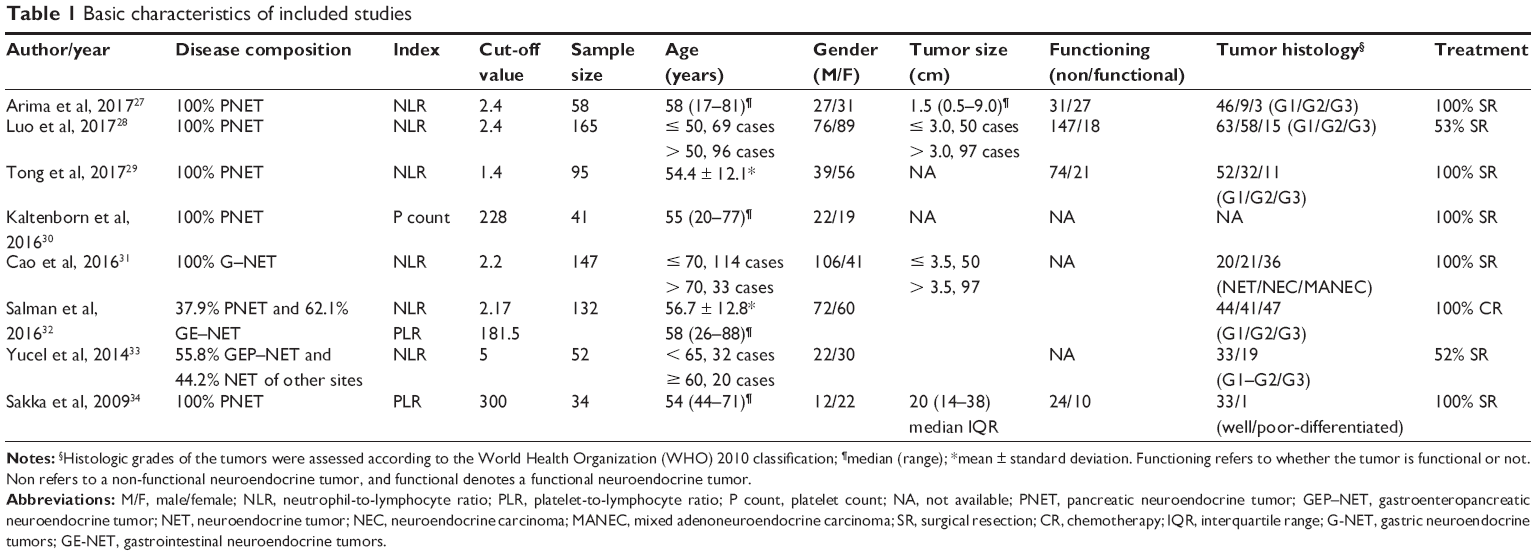 | Table 1 Basic characteristics of included studies |
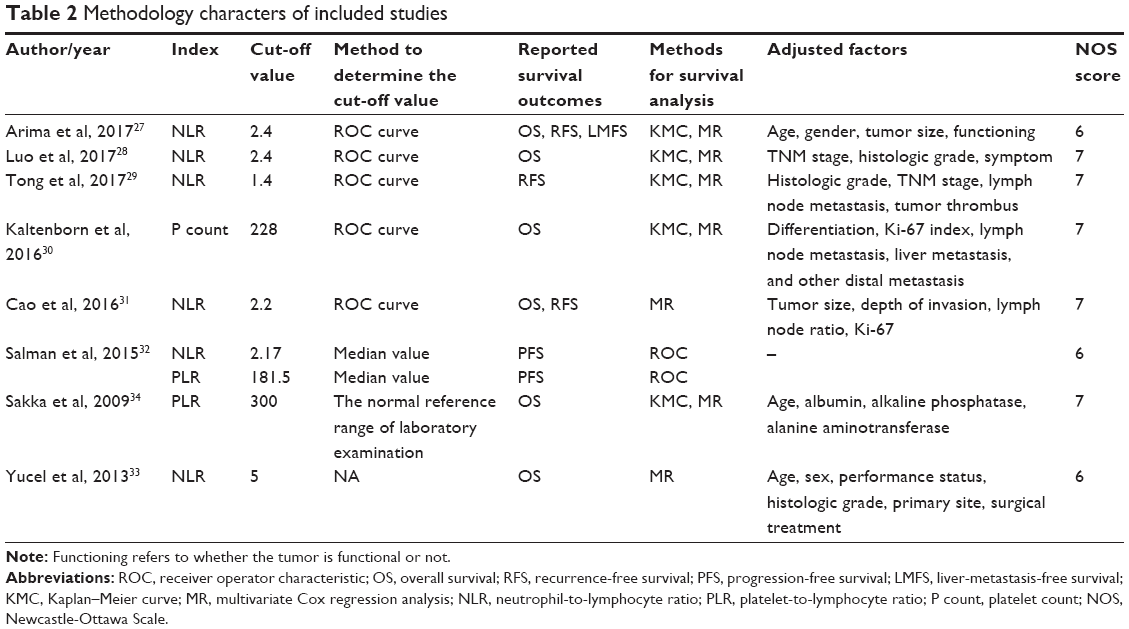 | Table 2 Methodology characters of included studies |
Correlation between hematologic parameters and survival outcomes
NLR
Table 3 summarizes the results of the prognostic value of each hematologic parameter. Most studies focused on the prognosis value of NLR. The effect of NLR on OS, RFS, and LMFS was available in four studies,27,28,31,33 four studies,27,29,31,32 and one study,27 respectively. All of these studies suggested that NLR was a marker for poor prognosis. Using the Cox proportional-hazard model, four studies showed patients with high NLR had poor OS,27,28,31,33 and three studies reported that high NLR correlated with poor RFS.27,29,31 Arima et al also specifically reported NLR was an independent predictor of postoperative liver metastasis.27 In addition, Salman et al found that a median NLR of 2.17 accurately predicted a PFS of 11.5 months (area under the curve [AUC] 0.94, P < 0.001) with 98.5% sensitivity and 53.7% specificity on the ROC curve.32 Pooled-analyses of the HRs revealed that patients with elevated NLR had both higher mortality risk and recurrence risk than those with a low NLR (pooled HR 3.05, 95% CI 1.96–4.76, I2 = 0%, P < 0.00001 for OS; pooled HR 3.30, 95% CI 2.04–5.32, I2 = 0%, P < 0.00001 for RFS).
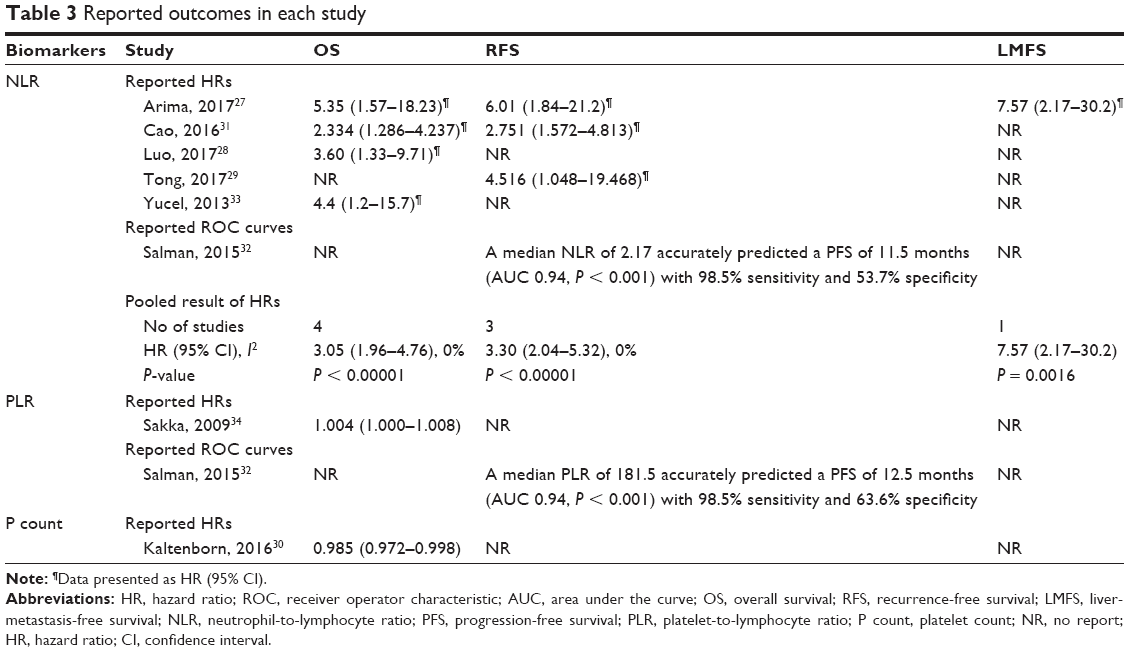 | Table 3 Reported outcomes in each study |
PLR
Two studies reported the effect of PLR on prognosis.32,34 The study conducted by Sakka et al found that decreased PLR values predicted better OS thorough the Kaplan–Meier method and survival curves.34 Salman et al showed patients with lower PLR values had decreased median PFS time in comparison with patients with higher PLR values, and additionally they also revealed that a median PLR of 181.5 accurately predicted a PFS of 12.5 months by using the ROC analysis.32 Because the study by Sakka et al only reported HR value, pooled-analysis was not performed.34 The results of these two studies suggested lower PLR predicted better prognosis, but more evidence is needed.
P count
Only one study reported the prognosis value of platelet count. The study by Kaltenborn et al found the OS was significantly different between patients with low platelet counts and those with high platelet counts and showed that patients with higher platelet counts had better OS.30
NLR in PNET
Five studies enrolled only PNET patients. Among them, two studies27,28 provided sufficient data on OS,27–30,34 and two studies provided sufficient data on RFS outcome for the pooled estimate.27,29 As shown in Figure 2, the result of meta-analysis showed significant superiority of a low NLR on OS (pooled HR 4.21, 95% CI 1.95–9.13, I2 = 0%, P = 0.0003). Meanwhile, the pooled HR for RFS also favored patients with a low NLR (pooled HR 5.37, 95% CI 2.14–13.47, I2 = 0%, P = 0.003) (Figure 3).
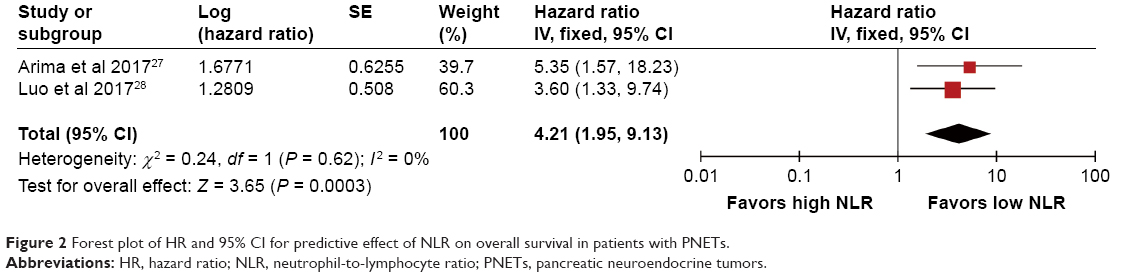 | Figure 2 Forest plot of HR and 95% CI for predictive effect of NLR on overall survival in patients with PNETs. |
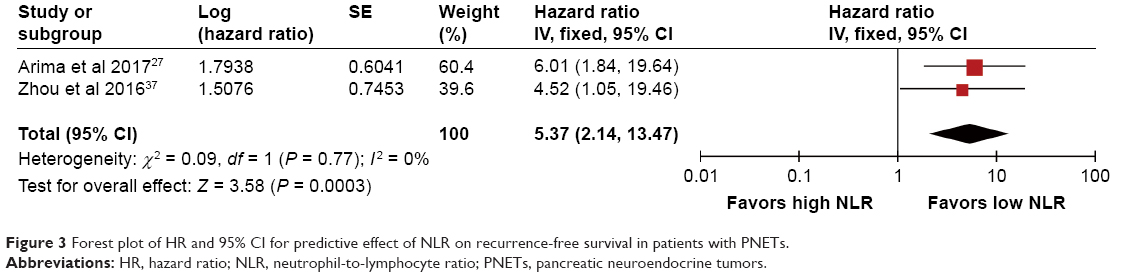 | Figure 3 Forest plot of HR and 95% CI for predictive effect of NLR on recurrence-free survival in patients with PNETs. |
Publication bias
The funnel plot showed an unsymmetrical distribution around the vertical axis (Figure 4). However, because the number of included studies was small, the funnel plots may make little sense.
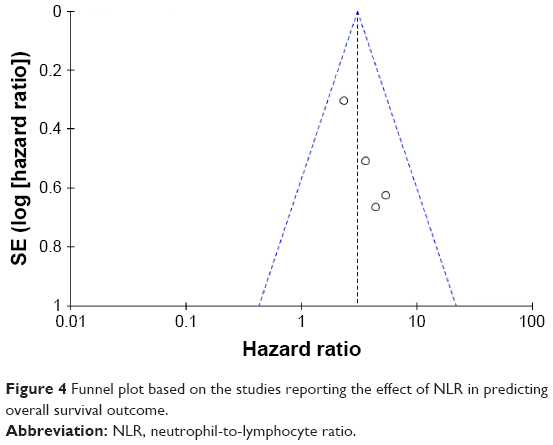 | Figure 4 Funnel plot based on the studies reporting the effect of NLR in predicting overall survival outcome. |
Discussion
Several hematologic parameters of systemic inflammation, such as lymphocyte counts, neutrophil counts, platelet counts, NLR, LMR, and PLR, have emerged as prognostic factors for a variety of cancer types.35–38 Because these markers can be easily acquired from blood routine test, they are cheap and easily acquired prognostic markers with a potential for widespread clinical use, many studies have focused on the association between these markers and prognosis in kinds of cancers. GEP–NETs are a type of relatively rare tumor, and the prognostic factors and surveillance strategy for GEP–NETs patients have not been well established due to the complexity and rarity of this disease. Therefore, a clear demonstration of the prognosis values of these easily applicable markers in GEP–NETs patients may help predict individual outcome and guide clinical decisions. In this study, we have summarized the published evidence on the association between the hematologic parameters and GEP–NETs outcomes. We found, in the field of this rare tumor, NLR, PLR, and platelet counts were all correlated with prognosis. Our pooled-analysis identified that NLR is an effective prognosis factor in GEP–NETs patients. The prognosis value of other hematologic parameters warrants interest and further study.
Most patients involved in the present study were PNET patients. The management of PNETs remains a big challenge because of their heterogeneous pathologic features and unpredictable clinical behaviors. Several markers have been identified as diagnosis markers or prognosis factors in PNETs. Chromogranin A (CgA) is the most commonly used biomarker and has been reported to be elevated in 50%–80% of PNET patients.39 However, its prognosis value has been questioned due to some studies which showed there was no association between CgA and survival in PNETs.40 Other potential markers include neurokinin A, pancreatic polypeptide, serotonin, neuron-specific enolase, etc., but their role is still unclear. Future research is needed to discover new markers and to determine which markers provide better prognostic information.6,41–43 Although the number of studies investigating the predictive value of NLR in PNETs is much less than studies for other tumors, they all revealed that NLR was a remarkable prognosis marker for predicting both survival and recurrence in PNETs. Therefore, NLR has the potential to serve as a supplemental prognostic marker. Besides, NLR is an easily available marker obtained from routine blood tests, which enhances the practicality.
There are some limitations in the present study. Most of the included studies used ROC curve to determine a cut-off value for hematologic parameters.27–31 Therefore, the NLR and PLR were used as dichotomous variables. Additionally, since the cut-off values were artificially chosen, the clinicopathological characters between groups in each study were incomparable. Moreover, the hematologic parameters could be affected by different conditions and diseases, and the survival time of NETs is usually longer than other cancers because most NETs are biologically less aggressive, but all studies only used one result before treatment and did not monitor hematologic parameters during follow-up. Besides, because G3 tumors are invariably lethal, and the malignant potentials of G1 and G2 tumors were relative indolent, it is better for further studies to give additional information regarding the association between hematologic markers and prognosis in G1/G2 patients and G3 patients separately. We also noted that no study reported cancer-specific survival, which is a better outcome indicator than OS because of the relatively long survival time of patients with GEP–NETs. Last but importantly, due to the retrospective nature of the current study, patients may be prone to potential selection bias. Prospective and larger studies with a longer follow-up are required to confirm these findings.
In conclusion, this present systematic review and meta-analysis summarized the current evidence on the prognosis values of hematologic parameters in GEP–NETs. Our results showed that NLR was an effective prognostic predictor. The prognostic value of other hematologic parameters deserves further investigation. The conclusion should be limited mainly to PNETs due to the majority of included cases being PNETs. We recommend that future studies should use a continuous NLR variable and adopt a prospective and matched study design.
Acknowledgment
We gratefully acknowledge the National Natural Science Foundation of China (No. 81602172).
Disclosure
The authors report no conflicts of interest in this work.
References
Modlin IM, Oberg K, Chung DC, et al. Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol. 2008;9(1):61–72. | ||
Fraenkel M, Kim M, Faggiano A, de Herder WW, Valk GD, Knowledge NETwork. Incidence of gastroenteropancreatic neuroendocrine tumours: a systematic review of the literature. Endocr Relat Cancer. 2014;21(3):R153–R163. | ||
Turaga KK, Kvols LK. Recent progress in the understanding, diagnosis, and treatment of gastroenteropancreatic neuroendocrine tumors. CA Cancer J Clin. 2011;61(2):113–132. | ||
Orgera G, Krokidis M, Cappucci M, et al. Current status of interventional radiology in the management of gastro-entero-pancreatic neuroendocrine tumours (GEP–NETs). Cardiovasc Intervent Radiol. 2015;38(1):13–24. | ||
Cives M, Soares HP, Strosberg J. Will clinical heterogeneity of neuroendocrine tumors impact their management in the future? Lessons from recent trials. Curr Opin Oncol. 2016;28(4):359–366. | ||
Landry CS, Cavaness K, Celinski S, Preskitt J. Biochemical prognostic indicators for pancreatic neuroendocrine tumors and small bowel neuroendocrine tumors. Gland Surg. 2014;3(4):215–218. | ||
Kanakis G, Kaltsas G. Biochemical markers for gastroenteropancreatic neuroendocrine tumours (GEP–NETs). Best Pract Res Clin Gastroenterol. 2012;26(6):791–802. | ||
Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and cancer. Cell. 2010;140(6):883–899. | ||
Sethi G, Shanmugam MK, Ramachandran L, Kumar AP, Tergaonkar V. Multifaceted link between cancer and inflammation. Biosci Rep. 2012;32(1):1–15. | ||
Baniyash M, Sade-Feldman M, Kanterman J. Chronic inflammation and cancer: suppressing the suppressors. Cancer Immunol Immunother. 2014;63(1):11–20. | ||
Bunt SK, Clements VK, Hanson EM, Sinha P, Ostrand-Rosenberg S. Inflammation enhances myeloid-derived suppressor cell cross-talk by signaling through Toll-like receptor 4. J Leukocyte Biol. 2009;85(6):996–1004. | ||
Gabrilovich DI, Nagaraj S. Myeloid-derived suppressor cells as regulators of the immune system. Nature Rev Immunol. 2009;9(3):162–174. | ||
Cadden I, Johnston BT, Turner G, McCance D, Ardill J, McGinty A. An evaluation of cyclooxygenase-2 as a prognostic biomarker in mid-gut carcinoid tumours. Neuroendocrinology. 2007;86(2):104–111. | ||
Klöppel G, Clemens A. The biological relevance of gastric neuroendocrine tumors. Yale J Biol Med. 1996;69(1):69–74. | ||
Le Marc’hadour F, Bost F, Peoc’h M, Roux JJ, Pasquier D, Pasquier B. Carcinoid tumour complicating inflammatory bowel disease. A study of two cases with review of the literature. Pathol Res Pract. 1994;190(12):1185–1192; discussion 1193–1200. | ||
Haukim N, Bidwell JL, Smith AJ, et al. Cytokine gene polymorphism in human disease: on-line databases, supplement 2. Genes Immun. 2002;3(6):313–330. | ||
Berkovic MC, Jokic M, Marout J, Radosevic S, Zjacic-Rotkvic V, Kapitanovic S. IL-6-174 C/G polymorphism in the gastroenteropancreatic neuroendocrine tumors (GEP–NETs). Experim Molec Pathol. 2007;83(3):474–479. | ||
Berkovic MC, Jokic M, Marout J, Radosevic S, Zjacic-Rotkvic V, Kapitanovic S. IL-2 −330 T/G SNP and serum values-potential new tumor markers in neuroendocrine tumors of the gastrointestinal tract and pancreas (GEP–NETs). J Molec Med (Berlin). 2010;88(4):423–429. | ||
Clarke SJ, Chua W, Moore M, et al. Use of inflammatory markers to guide cancer treatment. Clin Pharmacol Therapeut. 2011;90(3):475–478. | ||
Schubert C, Hong S, Natarajan L, Mills PJ, Dimsdale JE. The association between fatigue and inflammatory marker levels in cancer patients: a quantitative review. Brain Behav Immun. 2007;21(4):413–427. | ||
Vermeire S, Van Assche G, Rutgeerts P. The role of C-reactive protein as an inflammatory marker in gastrointestinal diseases. Nat Clin Pract Gastroenterol Hepatol. 2005;2(12):580–586. | ||
Porrata LF, Ristow K, Colgan JP, et al. Peripheral blood lymphocyte/monocyte ratio at diagnosis and survival in classical Hodgkin’s lymphoma. Haematologica. 2012;97(2):262–269. | ||
Stotz M, Gerger A, Eisner F, et al. Increased neutrophil-lymphocyte ratio is a poor prognostic factor in patients with primary operable and inoperable pancreatic cancer. Br J Cancer. 2013;109(2):416–421. | ||
Cho H, Hur HW, Kim SW, et al. Pre-treatment neutrophil to lymphocyte ratio is elevated in epithelial ovarian cancer and predicts survival after treatment. Cancer Immunol Immunother. 2009;58(1):15–23. | ||
Tao S, Haug U, Kuhn K, Brenner H. Comparison and combination of blood-based inflammatory markers with faecal occult blood tests for non-invasive colorectal cancer screening. Br J Cancer. 2012;106(8):1424–1430. | ||
Tomita M, Shimizu T, Ayabe T, Nakamura K, Onitsuka T. Elevated preoperative inflammatory markers based on neutrophil-to-lymphocyte ratio and C-reactive protein predict poor survival in resected non-small cell lung cancer. Anticancer Res. 2012;32(8):3535–3538. | ||
Arima K, Okabe H, Hashimoto D, et al. Neutrophil-to-lymphocyte ratio predicts metachronous liver metastasis of pancreatic neuroendocrine tumors. Int J Clin Oncol. 2017;22(4):734–739. | ||
Luo G, Liu C, Cheng H, et al. Neutrophil-lymphocyte ratio predicts survival in pancreatic neuroendocrine tumors. Oncol Lett. 2017;13(4):2454–2458. | ||
Tong Z, Liu L, Zheng Y, et al. Predictive value of preoperative peripheral blood neutrophil/lymphocyte ratio for lymph node metastasis in patients of resectable pancreatic neuroendocrine tumors: a nomogram-based study. World J Surg Oncol. 2017;15(1):108. | ||
Kaltenborn A, Matzke S, Kleine M, et al. Prediction of survival and tumor recurrence in patients undergoing surgery for pancreatic neuroendocrine neoplasms. J Surg Oncol. 2016;113(2):194–202. | ||
Cao LL, Lu J, Lin JX, et al. A novel predictive model based on preoperative blood neutrophil-to-lymphocyte ratio for survival prognosis in patients with gastric neuroendocrine neoplasms. Oncotarget. 2016;7(27):42045–42058. | ||
Salman T, Kazaz SN, Varol U, et al. Prognostic value of the pretreatment neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio for patients with neuroendocrine tumors: an Izmir Oncology Group Study. Chemotherapy. 2016;61(6):281–286. | ||
Yucel B, Babacan NA, Kacan T, et al. Survival analysis and prognostic factors for neuroendocrine tumors in Turkey. Asian Pacific J Cancer Prevent. 2014;14(11):6687–6692. | ||
Sakka N, Smith RA, Whelan P, et al. A preoperative prognostic score for resected pancreatic and periampullary neuroendocrine tumours. Pancreatology. 2009;9(5):670–676. | ||
Su L, Zhang M, Zhang W, Cai C, Hong J. Pretreatment hematologic markers as prognostic factors in patients with nasopharyngeal carcinoma. A systematic review and meta-analysis. Medicine. 2017;96(11):e6364. | ||
Gnjatic S, Bronte V, Brunet LR, et al. Identifying baseline immune-related biomarkers to predict clinical outcome of immunotherapy. J Immunother Cancer. 2017;5:44. | ||
Zhou X, Xu L, Huang Z, et al. The hematologic markers as prognostic factors in patients with resectable gastric cancer. Cancer Biomark. 2016;17(3):359–367. | ||
Ashrafganjoei T, Mohamadianamiri M, Farzaneh F, Hosseini MS, Arab M. Investigating preoperative hematologic markers for prediction of ovarian cancer surgical outcome. Asian Pacific J Cancer Prevent. 2016;17(3):1445–1448. | ||
Kidd M, Bodei L, Modlin IM. Chromogranin A: any relevance in neuroendocrine tumors? Curr Opin Endocrinol Diabetes Obesity. 2016;23(1):28–37. | ||
Sherman SK, Maxwell JE, O’Dorisio MS, O’Dorisio TM, Howe JR. Pancreastatin predicts survival in neuroendocrine tumors. Ann Surg Oncol. 2014;21(9):2971–2980. | ||
Yao JC, Pavel M, Phan AT, et al. Chromogranin A and neuron-specific enolase as prognostic markers in patients with advanced pNET treated with everolimus. J Clin Endocrinol Metabolism. 2011;96(12):3741–3749. | ||
McCall CM, Shi C, Klein AP, et al. Serotonin expression in pancreatic neuroendocrine tumors correlates with a trabecular histologic pattern and large duct involvement. Human Pathol. 2012;43(8):1169–1176. | ||
Zandee WT, van Adrichem RC, Kamp K, Feelders RA, van Velthuysen MF, de Herder WW. Incidence and prognostic value of serotonin secretion in pancreatic neuroendocrine tumours. Clin Endocrinol. 2017;87(2):165–170. | ||
Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials. 2007;8:16. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.