")
Back to Journals » Journal of Pain Research » Volume 11
Presence of pain on three or more days of the week is associated with worse patient reported outcomes in adults with sickle cell disease
Authors Bakshi N, Ross D, Krishnamurti L
Received 26 August 2017
Accepted for publication 9 November 2017
Published 9 February 2018 Volume 2018:11 Pages 313—318
DOI https://doi.org/10.2147/JPR.S150065
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Katherine Hanlon
Nitya Bakshi,1,2 Diana Ross,1 Lakshmanan Krishnamurti1,2
1Division of Pediatric Hematology-Oncology-BMT, Department of Pediatrics, Emory University, Atlanta, GA, USA; 2Aflac Cancer and Blood Disorders Center, Children’s Healthcare of Atlanta, Atlanta, GA, USA
Abstract: While acute episodic pain is the hallmark of sickle cell disease (SCD), transition to chronic pain is a major cause of morbidity and impaired quality of life. One of the core diagnostic criteria used by Analgesic, Anesthetic, and Addiction Clinical Trial Translations Innovations Opportunities and Networks-American Pain Society Pain Taxonomy (AAPT) to define chronic SCD pain is the presence of pain on a “majority of days” in the past 6 months in one or more locations. The frequency characteristic of “majority of days” is adapted from the criteria of 15 days or more per month, used to define chronic migraine, but there are inadequate data to support this cutoff in SCD. Using an existing dataset of adults with SCD who completed patient-reported outcomes of pain interference, physical functioning, anxiety, depression, and fatigue using the National Institutes of Health (NIH) patient-reported outcomes measures information system (PROMIS) short-form instruments, we examined the association of the presence of pain on 3 or more days per week with patient-reported outcomes of functioning. In unadjusted analyses, presence of pain on 3 or more days a week was associated with higher median PROMIS scores of pain interference, anxiety, and depression. Median PROMIS scores of fatigue and physical function were worse in women compared with men in unadjusted analyses. We did not find any difference in median PROMIS pain scores between adults aged ≤35 years compared with those aged ≥35 years. In linear regression models, after adjustment for age and sex, the presence of pain on 3 or more days a week was found to be associated with worse pain interference and anxiety. These data support the clinical relevance of the frequency characteristic of pain on a “majority of days” in the definition of chronic SCD pain, and provide the rationale for prospective studies to validate the clinical definition of chronic pain in SCD.
Keywords: sickle cell disease, chronic pain, patient reported outcomes
Introduction
Pain is the hallmark of sickle cell disease (SCD), the most common inherited blood disorder in the USA. While acute episodic pain has been the hallmark of SCD, there is increasing awareness of the transition from acute episodic to of chronic persistent SCD pain. The Analgesic, Anesthetic, and Addiction Clinical Trial Translations Innovations Opportunities and Networks-American Pain Society Pain Taxonomy (AAPT) diagnostic criteria for chronic SCD pain1 addresses the long-standing gap in the literature regarding the lack of a well-accepted definition for the diagnosis of chronic SCD pain. Based on these guidelines, the core diagnostic criteria for chronic SCD pain include a diagnosis of SCD, presence of pain on a “majority of days” in the past 6 months in 1 or more locations, presence of at least one of the listed signs on physical exam, and the absence of an alternative diagnosis.2 The frequency characteristic of “majority of days” is adapted from the criteria of 15 days or more per month used to define chronic migraine. Data to support the reliability and validity of this criterion for the diagnosis of chronic SCD pain are lacking. There is, therefore, a need to gather additional evidence to support the definition of chronic pain in SCD. Using an existing dataset of adults with SCD who completed patient-reported outcomes (PROs) of pain interference, anxiety, depression, fatigue, and physical function, using National Institutes of Health-patient-reported outcomes measures information system (NIH-PROMIS) short-form instruments, as well answered questions about the frequency of vasocclusive pain, we sought to determine whether the presence of pain on 3 or more days per week is associated with worse pain-related PROs.
Methods
The participants in this study were enrolled in a randomized clinical trial of the use of a web-based decision aid for examining therapeutic options in SCD. Of the 120 participants enrolled in this trial, 79 were adults with SCD and the remaining were caregivers/parents of adults with SCD. The sample was geographically diverse, and recruited through advertisements and booths at regional and national SCD conferences as well as from local SCD clinics. Adults with SCD aged ≥18 years were eligible if they spoke English and were considering a disease-modifying treatment (hydroxyurea, bone marrow transplantation, or chronic blood transfusion), and had not obtained the treatment option of interest in the past 12 months. Data collection at baseline/study entry for the randomized trial included self-report of demographic, clinical and disease-related variables, PROs of functioning, surveys and qualitative interviews about decision making regarding various treatment options in SCD. In particular, patients were asked if they experienced pain on 3 or more days a week. This question was framed as “Do you experience pain on 3 or more days a week?” If this was the case, patients were asked to report their average daily pain score on a scale of 1–10. PROMIS measures developed by the NIH-PROMIS initiative were used in measurement of PROs. These included measures of pain interference, anxiety, depression, physical function, and fatigue.2–6 Short-form PROMIS measures were used in this study and were as follows: PROMIS Pain Interference (6-item), PROMIS Anxiety (6-item), PROMIS Depression (6-item), PROMIS Physical Function (8-item), and PROMIS Fatigue (6-item). As PROMIS scores are referenced to the general US population, a T-score of 50 represents the mean for the general US population, and the SD is 10.3 A higher number indicates greater presence of the trait. For PROMIS Pain Interference, Anxiety, Depression, and Fatigue, a score of 60 is 1 SD worse than the population mean, whereas for PROMIS Physical Function, a score of 40 is 1 SD worse than the population mean. Since PROMIS measures have population-based norms, the goals of this analysis were as follows: 1) describe the association of patient-reported pain interference, anxiety, depression, fatigue, and physical function in adults with SCD in patient with pain on 3 or more days a week, and compare with population-based norms, and 2) determine whether factors such as age, sex, and presence of pain on 3 or more days a week were predictive of worse patient-reported pain interference, anxiety, depression, fatigue, and physical function.
All procedures were approved by the Institutional Review Board at Emory University and informed consent was obtained prior to all procedures.
Results
Of the 79 adults with SCD who participated in the randomized trial, 47 completed PROMIS questionnaires at baseline. Demographic data for these participants is described in Table 1. Of the 32 adults who did not complete PROMIS questionnaires, 15 could either not be contacted, or if contacted, did not complete any study interviews or PROMIS questionnaires; and 17 of the 32 completed the interview portion at study entry but did not complete baseline PROMIS questionnaires. Participants who did not complete PROMIS questionnaires were found to be younger compared with those who completed PROMIS questionnaires (median age 25 vs 35 years, respectively, p=0.08). No significant differences in the proportion of women or adults with pain on 3 or more days a week were found between those who completed PROMIS questionnaires compared with those who did not.
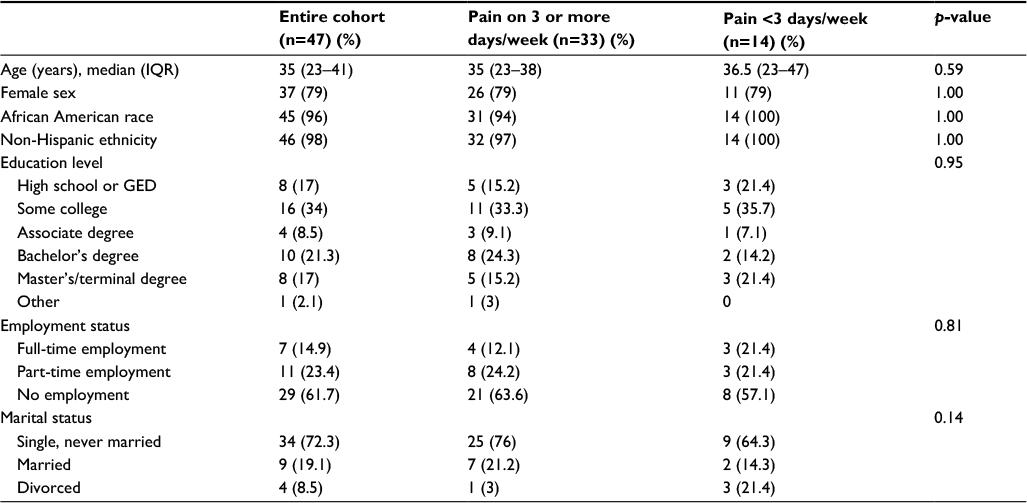 | Table 1 Demographic and clinical data Notes: Tests for significance Wilcoxon rank-sum test (continuous variables), Fisher exact (categorical variables). Abbreviations: GED, general equivalency diploma; IQR, interquartile range. |
Participants who completed PROMIS questionnaires were divided into 2 groups, those who reported pain on 3 or more days a week (n=33), and those who did not report pain on 3 or more days a week (n=14). No statistically significant differences in the demographic variables were found between these 2 groups. Clinical SCD-related history and treatment were obtained from participant self-report (no medical records were reviewed), and is presented in Table 2.
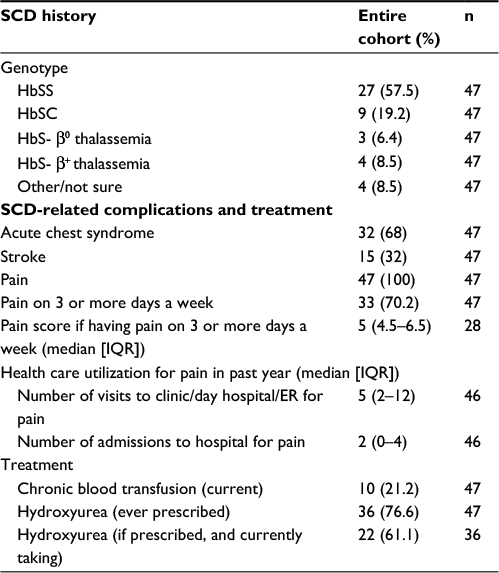 | Table 2 Self-reported clinical and treatment-related characteristics Note: Three participants endorsed being both on hydroxyurea and receiving chronic blood transfusion. Abbreviations: ER, emergency room; Hb, hemoglobin; IQR, interquartile range; SCD, sickle cell disease. |
PROMIS measures of functioning in adult patients with SCD
In adult patients with SCD, median PROMIS scores appeared to be worse in all aspects of functioning when compared with population-based norms; however, the difference was less pronounced in measures of depressive symptoms, fatigue, and anxiety. Also, statistically significant differences were found between median scores of PROMIS pain interference, anxiety, and depression among those who reported pain on 3 or more days a week vs those who did not, and those with pain on 3 or more days a week reported poorer scores than those who did not report pain on 3 or more days a week. These data are presented in Table 3.
 | Table 3 PROMIS measures of functioning in adults with SCD Note: *Wilcoxon rank-sum test. Abbreviations: PROMIS, patient-reported outcomes measures information system; SCD, sickle cell disease. |
We also examined the effect of age and sex on these PROs. We divided the study cohort into 2 groups, <35 years and >35 years of age, as the median age of this cohort was 35 years. No statistically significant differences (p<0.05) in median PRO scores were found between those <35 years and >35 years of age in this cohort. On comparing the median PRO scores between males and females, it was found that females had worse scores on physical functioning and fatigue, as shown in Table 4.
 | Table 4 PROMIS measures of functioning by sex Note: *Wilcoxon rank-sum test. Abbreviation: PROMIS, patient-reported outcomes measures information system. |
Finally, using linear regression methods, we incorporated age, sex, and presence of pain on more than 3 or more days a week as independent (or predictor) variables and PROMIS measures of pain interference, anxiety, depression, fatigue, and physical function as dependent (or outcome) variables. The presence of pain on 3 or more days a week (0=no 1=yes, reference group-no), sex (0=male 1=female, reference group-male) and age were all incorporated into the same model. These regression models are shown in Table 5. Adjusted for age and sex, the presence of pain on 3 or more days a week is independently associated with worse patient-reported pain interference and anxiety , and the association trended towards significance for physical function. The interaction between presence of pain on 3 or more days a week and sex was not significant.
 | Table 5 Linear regression models with PROs as dependent (or outcome) variables and presence of pain on 3 or more days a week, age and sex as independent (or predictor) variables Notes: Pain3d coded as 0= absent; 1= present; reference group =0; sex 0= male, 1= female, reference group = male. *p<0.05. **p<0.01. ***p<0.001. ap=0.075. Abbreviations: PRO, patient-reported outcomes; PROMIS, patient-reported outcomes measures information system. |
Discussion
This study indicates that the presence of pain on 3 or more days a week is independently associated with worse patient-reported pain interference and anxiety. While previous studies have reported worse scores on PROMIS measures in SCD when compared with the general population,7 this is the first study to report that the presence of pain on 3 or more days a week is associated with poorer PROs of functioning. In the recently released AAPT guidelines for the diagnosis of chronic pain, pain on a “majority of days” over the past 6 months has been proposed to be one of the diagnostic criteria for chronic SCD pain. While this study was not designed to validate the definition of SCD chronic pain, results of this study provide evidence that pain on 3 or more, or approximately “most” days of the week, adjusted for age and sex, is associated with worse patient-reported pain interference, anxiety, and physical function, and as such, supports the clinical relevance of frequency characteristic of “majority of days” for the diagnosis of chronic SCD pain.
This study also highlights the impact SCD has on functioning. The entire cohort experienced worse patient-reported pain interference, anxiety, depression, fatigue, and physical function, with a magnitude of 0.5–1 SDs different from the population norms. A difference of 0.5 SD is considered the threshold for changes in health-related quality of life in chronic illness,8 and the minimally important difference in PROMIS T-scores ranges between 2.5 and 6 in cancer patients.9 While chronic illness is associated with worse PROMIS scores,4 these scores in adults with SCD are worse than reference norms of PROMIS scores for individuals with cancer in the Surveillance, Epidemiology, and End Results (SEER) registry,10 highlighting the often under-recognized and under-appreciated morbidity, and the significant personal toll of this disease. The morbidity associated with SCD manifests not only in poorer QOL, but also in other aspects such as employment.11 More than half of this study sample reported not being currently employed.
Similar to previous studies in adults with SCD, this study also confirms that PROs are worse in several domains in patients with SCD when compared with the general population.7 PROMIS measures have been validated in both adults6 and children with SCD12,13 and in adults with SCD, and they correlate well with disease severity.7 The relationship of female sex with PROMIS scores, however, has not described in adults with SCD. In our unadjusted analyses, median PROMIS scores of fatigue and physical function were worse in women than men. Notably, female sex remained significantly associated with fatigue and physical functioning, as well as with pain interference, in the presence of pain on 3 or more days a week, in linear regression models. Ameringer et al14 have reported that patients with SCD have high fatigue scores, that fatigue scores are higher in women compared with men, and that fatigue scores also correlate with higher pain scores. This finding may not be unique to SCD since higher levels of fatigue have been reported in women in the general US population.15 McClish et al have reported worse body pain scores in women compared with men on the 36-item short-form survey (SF-36) subscale,16 but also report that in diary data from the PISCES study, the largest epidemiological study of pain in SCD, women did not experience more pain, more severe pain, more days with pain, more interference on pain days, or more distress from pain compared with men.16 The largest study in adults with SCD describing the validity of PROMIS7 did not interrogate gender-related differences in PROs. In this study, female sex was independently associated with pain interference, along with the presence of pain on 3 or more days a week. Results from this cohort also suggest that gender influences patient-reported fatigue and physical function. These results provide the rationale and population estimates for the design of larger, prospective studies of the impact of chronic pain on patient-reported measures of functioning, and underscore the relevance of studying gender-related differences in PROs in SCD. This study also highlights the need for consistent measurement of outcomes, since results of gender differences in outcomes may vary across instruments.
The strength of this study is the comprehensive assessment of several domains of PROs in adults with SCD, as well as an exploration of PROs across age, gender, and most importantly, presence of pain on 3 or more days of the week. Limitations of this study include a small sample size, and that this was a post hoc analysis of data gathered as part of a larger study of decision making, and not primarily gathered to determine PROs in SCD. The diagnostic criteria for SCD chronic pain require the presence of both patient-reported pain on majority of days for at least 6 months and presence of signs on physical examination. We neither collected data on pain intensity for 6 months nor examined the patients for associated physical signs. As such, this study was not designed to validate the definition of chronic SCD pain. Patients answered a single question about whether they had pain on 3 or more days a week. The answer to the question may be subject to their interpretation or recall bias. We, therefore, cannot be certain which participants met all the proposed diagnostic criteria of chronic pain. This study is also subject to the response bias observed commonly in survey studies, as well as by the fact that clinical data were based on self-report rather than chart review. Additionally, we did not obtain pain intensity data of those who did not experience pain on 3 or more days a week. The results of this study may not be generalizable to the larger SCD population as the sample constituted more women than men. In addition, the sample was drawn from patients who attended national conferences, these patients are activated and engaged in seeking information related to their care, and have access to resources that allow for attendance at national conferences. Despite the limitations, we believe this study offers initial perspective on PROs in the presence of pain on 3 or more days of the week in SCD, and more importantly, provides the rationale to conduct future prospective studies to gather evidence for the validity of the definition of chronic SCD pain.
Conclusion
The presence of pain on 3 or more days a week is associated with worse patient-reported pain interference and anxiety. In the presence of pain on 3 or more days a week, pain interference, fatigue, and physical function are also influenced by gender, with women faring worse than men. These data support the clinical relevance of the frequency characteristic of pain on a “majority of days” in the definition of chronic SCD pain, and provide the rationale for prospective studies to validate the clinical definition of chronic pain in SCD.
Acknowledgments
The authors thank study participants for participation in this study. This study was supported by Patient-Centered Outcomes Research Institute.
Disclosure
The authors report no conflicts of interest in this work.
References
Dampier C, Palermo TM, Darbari DS, Hassell K, Smith W, Zempsky W. AAPT diagnostic criteria for chronic sickle cell disease pain. J Pain. 2017;18(5):490–498. | ||
Amtmann D, Cook KF, Jensen MP, et al. Development of a PROMIS item bank to measure pain interference. Pain. 2010;150(1):173–182. | ||
Cella D, Riley W, Stone A, et al. The patient-reported outcomes measurement information system (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005–2008. J Clin Epidemiol. 2010;63(11):1179–1194. | ||
Rothrock NE, Hays RD, Spritzer K, Yount SE, Riley W, Cella D. Relative to the general US population, chronic diseases are associated with poorer health-related quality of life as measured by the patient-reported outcomes measurement information system (PROMIS). J Clin Epidemiol. 2010;63(11):1195–1204. | ||
Pilkonis PA, Choi SW, Reise SP, et al. Item banks for measuring emotional distress from the patient-reported outcomes measurement information system (PROMIS(R)): depression, anxiety, and anger. Assessment. 2011;18(3):263–283. | ||
Rose M, Bjorner JB, Becker J, Fries JF, Ware JE. Evaluation of a preliminary physical function item bank supported the expected advantages of the patient-reported outcomes measurement information system (PROMIS). J Clin Epidemiol. 2008;61(1):17–33. | ||
Keller S, Yang M, Treadwell MJ, Hassell KL. Sensitivity of alternative measures of functioning and wellbeing for adults with sickle cell disease: comparison of PROMIS(R) to ASCQ-Me. Health Qual Life Outcomes. 2017;15(1):117. | ||
Norman GR, Sloan JA, Wyrwich KW. Interpretation of changes in health-related quality of life: the remarkable universality of half a standard deviation. Med Care. 2003;41(5):582–592. | ||
Yost KJ, Eton DT, Garcia SF, Cella D. Minimally important differences were estimated for six patient-reported outcomes measurement information system-cancer scales in advanced-stage cancer patients. J Clin Epidemiol. 2011;64(5):507–516. | ||
Jensen RE, Moinpour CM, Potosky AL, et al. Responsiveness of 8 patient-reported outcomes measurement information system (PROMIS) measures in a large, community-based cancer study cohort. Cancer. 2017;123(2):327–335. | ||
Sanger M, Jordan L, Pruthi S, et al. Cognitive deficits are associated with unemployment in adults with sickle cell anemia. J Clin Exp Neuropsychol. 2016;38(6):661–671. | ||
Dampier C, Barry V, Gross HE, et al. Initial evaluation of the pediatric PROMIS(R) health domains in children and adolescents with sickle cell disease. Pediatr Blood Cancer. 2016;63(6):1031–1037. | ||
Dampier C, Jaeger B, Gross HE, et al. Responsiveness of PROMIS(R) pediatric measures to hospitalizations for sickle pain and subsequent recovery. Pediatr Blood Cancer. 2016;63(6):1038–1045. | ||
Ameringer S, Elswick RK, Jr., Smith W. Fatigue in adolescents and young adults with sickle cell disease: biological and behavioral correlates and health-related quality of life. J Pediatr Oncol Nurs. 2014; 31(1):6–17. | ||
Junghaenel DU, Christodoulou C, Lai JS, Stone AA. Demographic correlates of fatigue in the US general population: results from the patient-reported outcomes measurement information system (PROMIS) initiative. J Psychosom Res. 2011;71(3):117–123. | ||
McClish DK, Levenson JL, Penberthy LT, et al. Gender differences in pain and healthcare utilization for adult sickle cell patients: the PiSCES Project. J Womens Health (Larchmt). 2006;15(2):146–154. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.