")
Back to Journals » Cancer Management and Research » Volume 12
Preoperative Immune Prognostic Index Can Predict the Clinical Outcomes of Patients with Gallbladder Cancer: Single-Center Experience
Authors Sun L, Wang D, Zhang M , Jin Y , Jin B, Xu H, Du S, Xu Y, Zhao H, Lu X, Sang X , Zhong S, Yang H , Mao Y
Received 7 July 2020
Accepted for publication 10 November 2020
Published 25 November 2020 Volume 2020:12 Pages 12137—12150
DOI https://doi.org/10.2147/CMAR.S271044
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ahmet Emre Eşkazan
Lejia Sun,1,* Dongyue Wang,2,* Mengyuan Zhang,2,* Yukai Jin,1 Bao Jin,1 Haifeng Xu,1 Shunda Du,1 Yiyao Xu,1 Haitao Zhao,1 Xin Lu,1 Xinting Sang,1 Shouxian Zhong,1 Huayu Yang,1 Yilei Mao1
1Department of Liver Surgery, Peking Union Medical College (PUMC) Hospital, PUMC & Chinese Academy of Medical Sciences, Beijing 100730, People’s Republic of China; 2Peking Union Medical College (PUMC), PUMC & Chinese Academy of Medical Sciences, Beijing 100730, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yilei Mao; Huayu Yang
Department of Liver Surgery, Peking Union Medical College (PUMC) Hospital, PUMC & Chinese Academy of Medical Sciences, Beijing 100730, People’s Republic of China
Tel +86-10-69156042
Email [email protected]; [email protected]
Purpose: The immune prognostic index (IPI) has been used as a prognostic biomarker in various cancers. However, the prognostic value of the IPI in gallbladder cancer remains to be determined.
Patients and Methods: This study included 139 patients who were diagnosed with gallbladder cancer after surgical resection from 2003 to 2017. We used a Kaplan–Meier curve analysis to evaluate the overall survival (OS). Cox proportional hazards regression methodology was used to identify significant independent prognostic factors. Prognostic nomograms for predicting OS were established to achieve superior discriminatory abilities. The prognostic nomograms were verified according to the concordance index, calibration curves, and decision curve analyses in the training cohort and validation cohort.
Results: Of all 139 patients, 87 (62.6%) patients accepted R0 resection, 32% and 68% were stratified into the good and poor IPI group, respectively. The median OS was 55.9 (range, 5.93– 182.7) months in the good IPI group and 15.47 (range, 0.29– 190.37) months in the poor IPI group (P < 0.001). In the multivariate Cox model, the IPI was an independent predictor of OS along with the CA19-9, curative resection, and postoperative chemoradiotherapy. A nomogram based on these factors was efficient in predicting 1-, 3-, and 5-year survival probabilities. The nomogram showed higher sensitivity and specificity than the current cancer TNM staging system in the training cohort and validation cohort.
Conclusion: The IPI is an independent prognostic factor in gallbladder cancer. Our IPI-based nomogram can serve as a useful and convenient prognostic tool for gallbladder cancer.
Keywords: the immune prognostic index, gallbladder cancer, prognostic value, nomogram, overall survival
Introduction
Gallbladder cancer (GBC) is a rare type of cancer, but it is also the most common malignancy of the biliary tract, accounting for 1.2% of cancer incidence, which is more common in Chile, Eastern Europe, Northern India, and East Asia.1 Due to the lack of typical symptoms and specific examinations, most patients with GBC present with advanced stage.2–4 GBC has low sensitivity to both radiotherapy and chemotherapy,5 and effective drugs are lacking; thus, surgical resection is the main treatment.6,7 Physicians are now more concerned about the prognosis of GBC after surgical resection. The currently used systemic stratification is the 8th edition of the American Joint Committee on Cancer (AJCC) staging system. However, this system cannot offer accurate and individualized prognostic information.8 Therefore, identification of sensitive prognostic biomarkers for appropriate treatment is needed.
Growing evidence has recently shown that cancer-related inflammation responses have an important role in tumorigenesis, disease progression, and the patient’s prognosis.9,10 Chronic inflammation is a consistent feature of the tumor microenvironment and a major risk factor for GBC progression.2 Tumor-induced systemic inflammation leads to changes in the peripheral blood. Several studies have shown that lymphocytes, neutrophils, monocytes, and monocytes play critical roles in the tumor-induced systemic response.9,11 Therefore, inflammatory biomarkers have been studied as prognostic markers in various cancers. Various laboratory biomarkers, including the Glasgow prognosis score,12 platelet-to-lymphocyte ratio, C-reactive protein, and fibrinogen level,13 have been proposed as prognostic biomarkers. However, in real-world clinical trials, some prognostic parameters, such as nutrition-related factors, are difficult to measure. Among them, the relative value of a combined index of the neutrophil and lymphocyte counts (neutrophil-to-lymphocyte ratio [NLR]) can be easily accessed in the clinical setting and has been shown to have association with the prognosis of several tumors including lung cancer,14 pancreatic, liver, esophageal as well as testicular diffuse large B-cell lymphoma.15 Furthermore, a derived score composed of the white cell and neutrophil counts (absolute neutrophil count divided by absolute white cell count minus absolute neutrophil count [dNLR]) has been evaluated in patients with cancer, showing its prognostic value similar to that of the NLR. The dNLR has been proven to be an independent prognostic marker in patients with colon cancer16 and metastatic melanoma.17
The baseline serum lactate dehydrogenase (LDH) level is also an independent prognostic factor for poor survival outcomes in patients with metastatic melanoma,18 non-small cell lung cancer (NSCLC),19 pancreatic carcinoma,20 metastasized colorectal cancer,21 clear cell renal cell carcinoma (RCC),22 and gastric cancer.23 The LDH level has also been found to be associated with progression-free survival of patients with peripheral T-cell lymphoma24 and testicular diffuse large B-cell lymphoma.15
In 2019, Mezquita et al25 developed the immune prognostic index (IPI), which combines the pretreatment LDH level and the dNLR to stratify patients into poor, intermediate, and good prognostic groups. Other researchers have further examined the value of the IPI in NSCLC, RCC, and melanoma.24,26 However, whether the IPI has prognostic utility in GBC remains unknown.
In the study, we investigated the association of the IPI with the outcomes of GBC and attempted to establish a prognostic model based on the IPI.
Materials and Methods
Patients and Treatment
We conducted a retrospective study of a cohort of patients diagnosed with GBC by pathological examination after radical surgical resection at Peking Union Medical College (PUMC) Hospital in Beijing, China. From June 2003 to May 2017, 159 patients were reviewed. The inclusion criteria including undergoing surgery, pathologically confirmed GBC, no preoperative antitumor or anti-infection treatments, no other malignant tumors except GBC, and available clinical data at the time of the first diagnosis. The exclusion criteria were lack of a clear pathological diagnosis, history or presence of malignancy, perioperative mortality, and incomplete follow-up. Patients who underwent radical surgical protocols and had pathologically proven R0 resection are defined as curative resection.
Data Collection
Conventional clinicopathological parameters were examined within 3 days preoperatively, including complete physical examination findings, routine blood test results, biochemical test results, and levels of carbohydrate antigen 19–9 (CA19-9). A pathologist staged each patient’s cancer at the time of the postoperative histopathological examination according to the 8th edition of the AJCC staging system. The incisional margins, lymph node metastasis, lymphovascular invasion, perineural invasion, and tumor size were verified based on surgical observations and pathological evaluation. Postoperative chemotherapy was obtained by follow-up. All data were obtained from the hospital’s record system.
All patients were followed up via telephone, and the last follow-up was completed on 3 February 2020. The OS was calculated as the date of surgery to the date of death of any cause or censoring at the last follow-up visit. The dNLR was calculated as the absolute neutrophil count divided by the absolute white cell count minus the absolute neutrophil count.
The IPI was defined based on a dNLR of >1.4 and LDH level of >270 U/L, characterizing the patients into two groups (good, 0 factors; poor, 1–2 factors). According to the receiver operating characteristic (ROC) curve analysis, a dNLR cut-off value of 1.4 had the highest area under the curve, and the LDH cut-off value was defined according the limit at PUMC.
Statistical Analysis
Continuous variables with a Gaussian distribution are presented as mean and standard deviation, and those without a Gaussian distribution are shown as median and interquartile range. Categorical variables are reported as number (%). The optimal cut-off values for the dNLR and CA19-9 level were calculated according to the highest area under the ROC curve.
Baseline characteristics were compared between groups using the independent-sample t-test and chi-square test, as appropriate. The Log-rank test and Kaplan–Meier method were used to analyze and describe survival curves. Independent prognostic factors were identified by a Cox proportional hazards regression model. Variables with a p-value no more than 0.05 in univariate analysis and other potential important variables were selected to enter into the multivariate model.
The patients were randomly divided into the nomogram in the training cohort and validation cohort in a proportion of 1:1. Prognostic nomograms for OS were established based on the result of the multivariate analyses. The Harrell’s concordance index (C-index), calibration curves, and decision curve analysis (DCA) were further used to evaluate the predictive performance in the training cohort and validation cohort. The optimal cut-off value for our nomogram-based staging system was calculated through R package “survminer”.
SPSS version 25.0 for MacOS (IBM Corporation, Armonk, NY, USA) was used for the data analyses. Nomograms were established by R version 3.5.0 software (http://www.r-project.org/). The extension packages included “survival,” “rms,” “foreign,” “stdca,” and “survminer”. A P value of <0.05 indicated a significant difference.
Results
Clinicopathological Characteristics
We initially reviewed 159 patients who received surgical resection and finally 139 patients diagnosed with GBC were included in this analysis. Twenty patients were excluded, including 4 patients lost to follow-up, 2 patients with perioperative mortality, 4 patients with other malignant tumors, and 10 patients missing key data (LDH). The patients’ median age was 64 years (range, 29–85 years), and 59 (42.4%) were male. Among the study population, 67 (48.2%) patients’ CA19-9 was higher than 40U/mL, 80 (57.6%) patients underwent curative surgery and 24 (17.3%) patients received postoperative chemoradiotherapy. According to the TNM staging system, 5 (3.6%) patients had stage 0 GBC, 11 (7.9%) had stage 1, 13 (9.3%) had stage 2, 44 (31.7%) had stage 3A, 40 (28.8%) had stage 3B, 9 (6.5%) had stage 4A, and 17 (12.2%) had stage 4B. Among them, the patients in stage 4 received palliative resection in order to reduce tumors and improve their life qualities. The patients’ other clinicopathological and laboratory characteristics are summarized in Table 1.
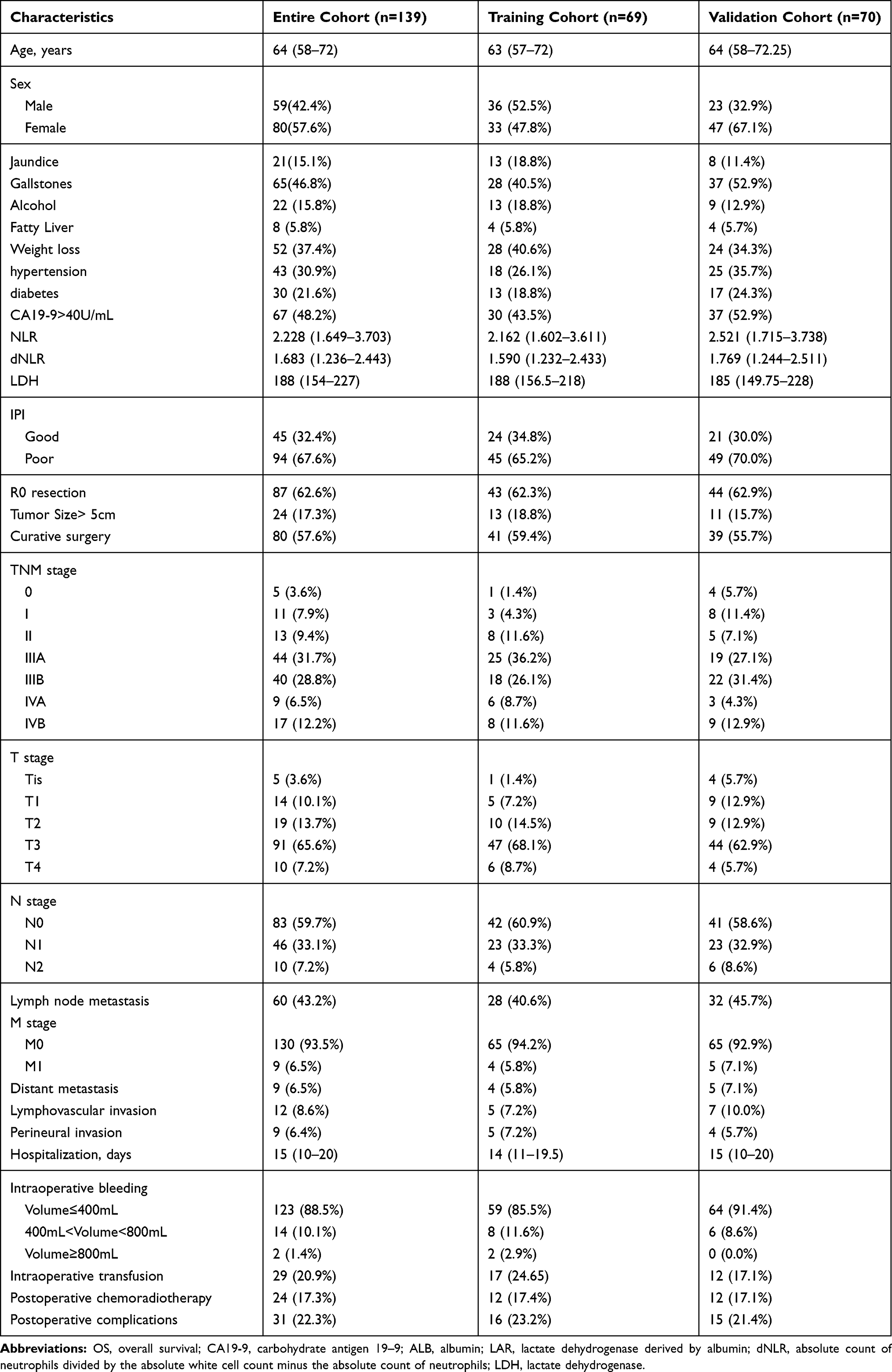 |
Table 1 Baseline Characteristics of Total Patients |
At the end of follow-up, 106 patients had died. The median follow-up duration was 20.5 months (95% confidence interval [CI], 1–153 months) and the median OS was 31.2 months (95% CI, 0.27–190 months).
Clinical Features According to IPI
The IPI was calculated according to a baseline dNLR of >1.4 and LDH level of >270 U/L. Among the 139 patients, 45 (32.4%) had a good IPI and 94 (67.6%) had a poor IPI. As shown in Table 2, the NLR was higher in the poor than good IPI group (3.053 vs 1.466, respectively; P < 0.001). The proportions of patients with CA19-9 higher than 40U/mL (31.1% vs 56.4%, P=0.005), curative surgery (75.6% vs 48.9%, P = 0.003). As shown in Figure 1, a good IPI was associated with longer OS in the overall population and the subgroups divided according to the TNM stage. The other characteristics of the patients in each group are summarized in Table 2.
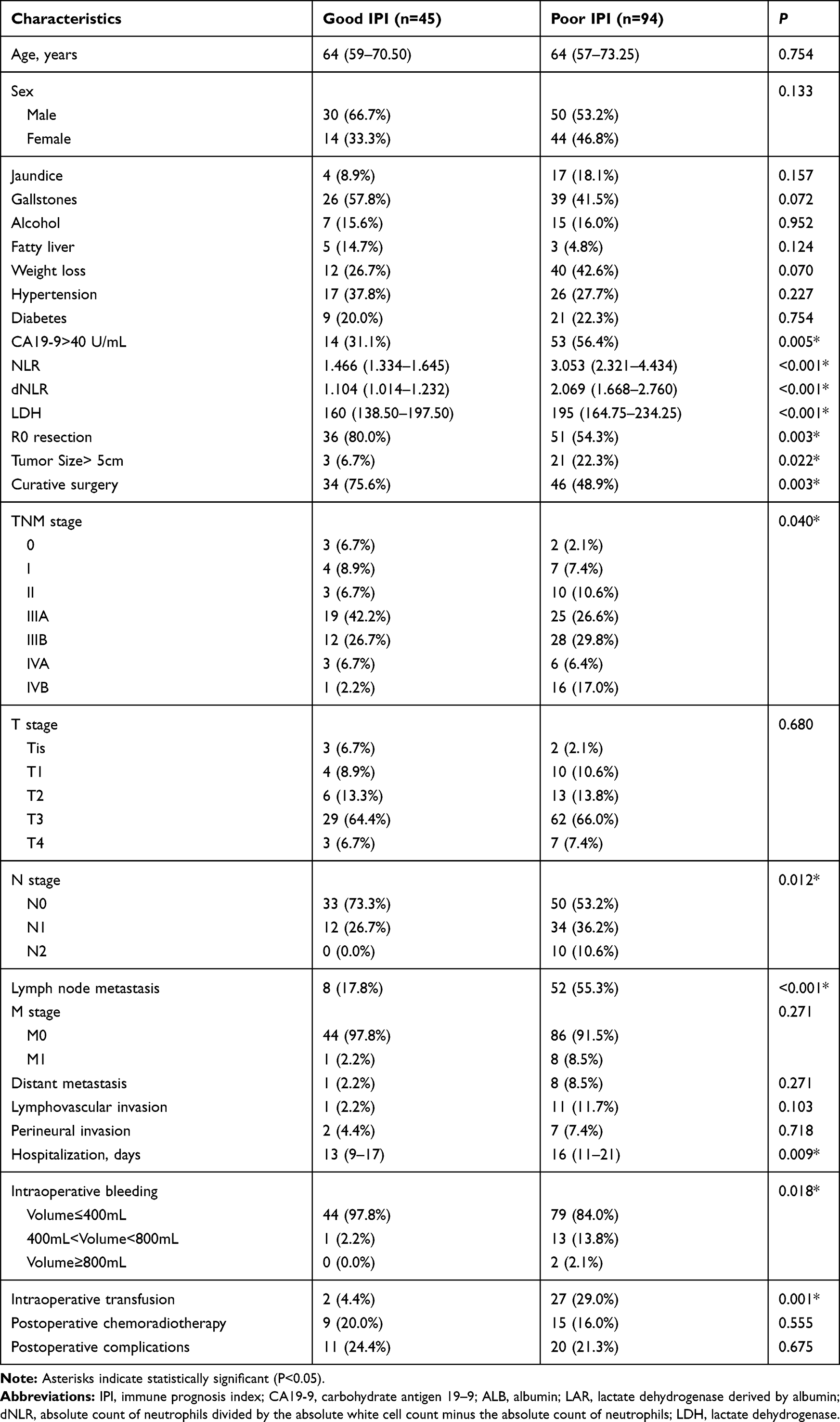 |
Table 2 Correlation Between IPI and Clinicopathological Characteristics |
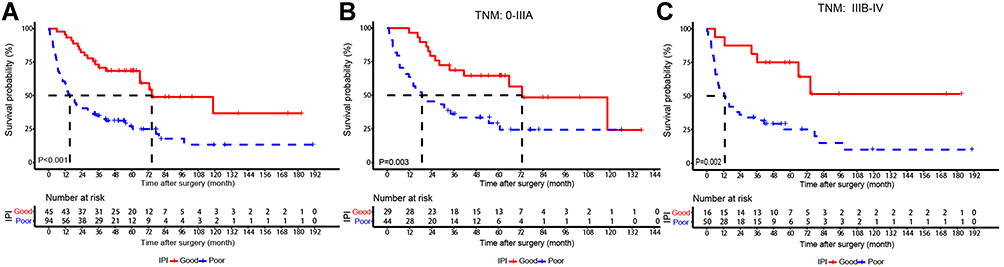 |
Figure 1 Kaplan–Meier (K–M) survival curves for overall survival rate stratified according to IPI. (A) Kaplan–Meier survival curves shows the overall survival rate in total gallbladder cancer patients; (B) K–M curves shows the overall survival rate in the gallbladder cancer patient graded ≤3A; (C) K–M curves shows the overall survival rate in the gallbladder cancer patient graded≥3B. |
Prognostic Factors for Surgical Outcome and OS
A poor IPI is associated with poor surgical outcomes. As shown in Table 2, patients with a poor IPI tended to have a longer hospitalization (13 vs 16 days, P =0.009). We also found that patients with a poor IPI endured more intraoperative transfusion (2 vs 27, P = 0.001), as well as more intraoperative bleeding (44 vs.79, P = 0.018).
In the univariate analysis, as shown in Table 3, a dNLR of >1.4 (hazard ratio [HR], 2.897; 95% CI, 1.754–4.783; P < 0.001), LDH level of >270 U/L (HR, 2.185; 95% CI, 1.211–3.945; P = 0.009), and the IPI (HR, 3.036; 95% CI, 1.821–5.062; P < 0.001) were associated with shorter OS. The univariate analysis also showed that CA19-9>40 U/mL (HR,3.326; 95% CI, 2.073–5.051; P <0.001), NLR>2 (HR, 2.433; 95% CI, 1.518–3.898; P<0.001), jaundice (HR, 2.183; 95% CI, 1.322–3.607; P = 0.002), R0 resection (HR, 0.436; 95% CI, 0.287–0.664; P < 0.001), lymph node metastasis (HR, 3.096; 95% CI, 2.003–4.784; P < 0.001), and curative surgery (HR, 0.369; 95% CI, 0.287–0.664; P < 0.001) had significant differences in the Cox proportional hazards regression model. Considering that the clinical significance of postoperative chemoradiotherapy was related to prognosis, it is included in the multivariable model although the p value was close to 0.05.
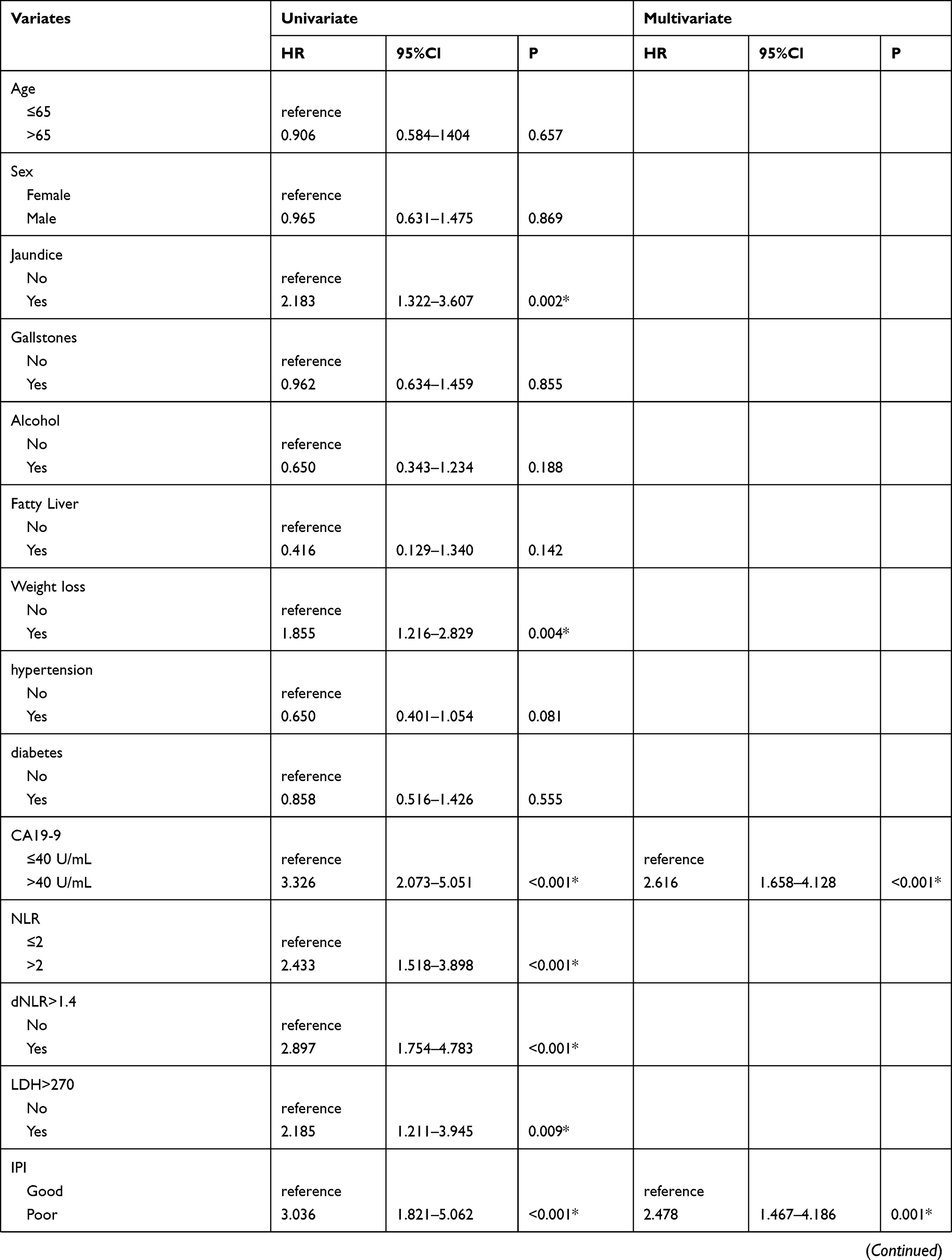 | 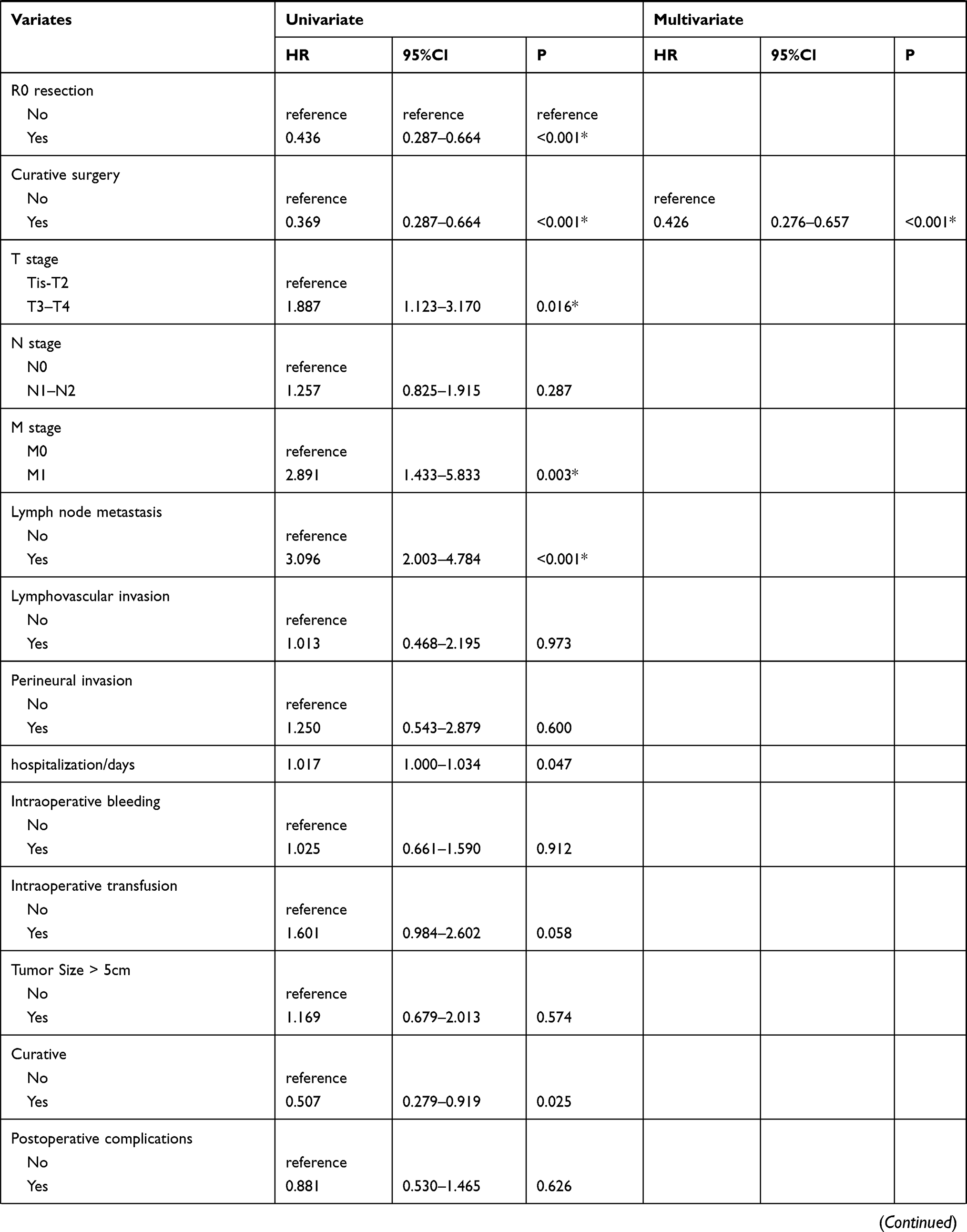 | 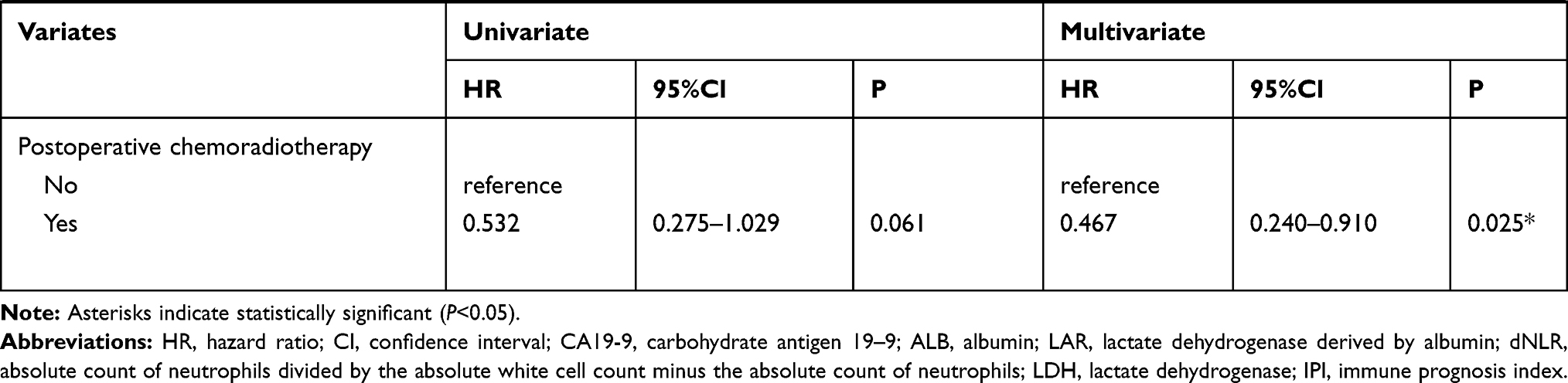 |
Table 3 Univariate and Multivariate Cox Proportional Hazard Analysis of Factors Associated with Overall Survival |
The multivariable model revealed that the IPI (HR, 2.478; 95% CI, 1.467–4.186; P = 0.001), CA19-9>40U/mL (HR, 2.616; 95% CI, 1.658–4.128; P<0.001), curative surgery (HR, 0.426; 95% CI, 0.267–0.657; P<0.001) and postoperative chemoradiotherapy (HR, 0.467; 95% CI, 0.240–0.910; P = 0.025) were independently associated with OS.
Establishment and Validation of the Nomogram
According to the results of the Cox proportional hazards model, the nomogram for OS survival (P-risk Plus model) included IPI, CA19-9, curative surgery, and postoperative chemoradiotherapy; it was generated as shown in Figure 2A. In this nomogram, each variable is imputed a weighted point, and the sum of the points can predict 1-, 3-, and 5-year survival probabilities. A higher patient grade is associated with a lower survival probability.
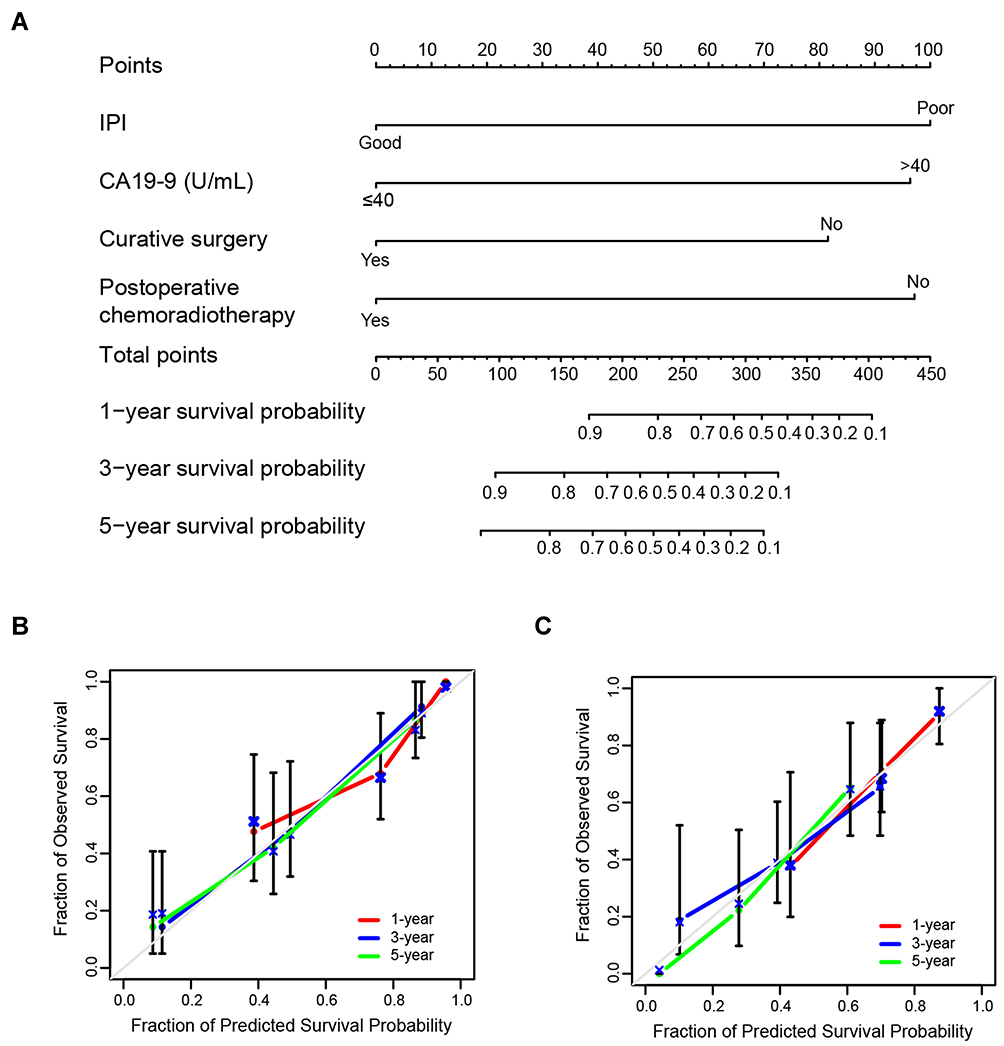 |
Figure 2 Nomogram and calibration curves. (A) Nomogram based on IPI, CA19-9, curative surgery, and postoperative chemoradiotherapy for predicting overall survival. Calibration curves of the nomogram for 1-year, 3-year, and 5-year OS in training set (B) and validation set (C). The x-axis represents nomogram predicted probability of OS, and the y-axis is the actually observed survival probability. |
The results showed that the model had superior discrimination (C-index, 0.791 in the training cohort, 0.700 in the validation cohort). Besides, the performance of the nomogram was evaluated using a calibration curve (Figure 2B). The predicted line matched the reference line well for 1-, 3-, and 5-year survival, showing good performance of the nomogram. The result showed excellent consistency between nomogram-prediction and actual observation. Similar result was obtained in the validation group (Figure 2C).
Comparison of Predictive Accuracy for OS Between Nomogram and TNM Staging System
We used DCA to compare the clinical utility between the prognostic model, TNM, and a nomogram without IPI, which is named as reference model in Supplement Figure 1. Higher threshold probability represented better estimation for decision outcomes. Compared with other models, the model yielded the best net benefit across in the range of threshold probability for 1-, 3- and 5-year OS in both training set and validation set, indicating its ability for clinical decision-making is better than TNM staging. The result also showed that the model with IPI showed better net benefit than the model without IPI, which indicated that IPI was occupied a major position in the prediction of the nomogram.
Furthermore, we compared the time-dependent receiver operating characteristic (ROC) curves of the nomogram, the nomogram without IPI (Reference) as well as TNM (Supplement Figure 2). The result of time-dependent ROC curves indicated that the nomogram has better accuracy than the 8th TNM staging and the nomogram without IPI. The nomogram also showed significant relationship with longer OS in the overall population and in the subgroups divided according to the TNM stage and curative surgery (Supplement figure 3).
We also investigated whether our nomogram could distinguish different outcomes of patients with the same TNM stage of GBC. Thus, a histogram of the nomogram-predicted 1-, 3- and 5-year survival probabilities of patients with different TNM stages were developed (Figure 3). Even patients with the same TNM stage clearly had various survival probabilities. The heterogeneity of the nomogram-predicted survival probabilities in the same TNM stage group suggests that our nomogram is able to provide a more detailed classification of the prognosis in patients with GBC than is the 8th version of the AJCC TNM staging system.
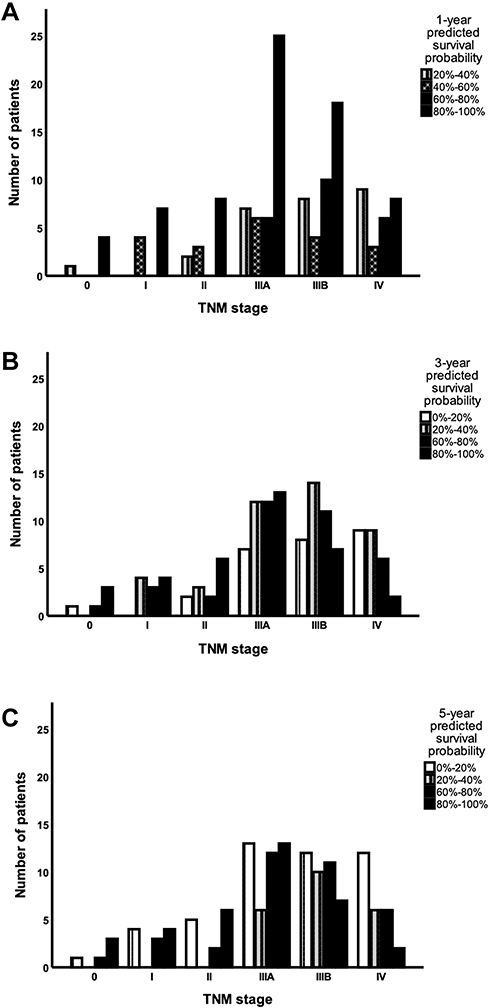 |
Figure 3 1-year (A), 3-year (B), and 5-year (C) survival probability predicted by nomogram in patients divided in TNM stage. The x-axis represents patients in different TNM stages, and the y-axis is the number of patients within the corresponding interval of nomogram-predicted survival probability. |
Discussion
GBC is an uncommon cancer with a poor prognosis.27,28 Surgery is the only effective curative treatment.2 Therefore, obtaining accurate prognostic information is necessary.6 For patients with advanced GBC, the current TNM staging system is not useful for clinicians to determine a precise treatment before the operation. Thus, a way to more precisely and specifically predict survival is required. Inflammation plays an important role in tumorigenesis.29 Additionally, chronic inflammation is a major risk factor for GBC progression.2 From this perspective, inflammatory biomarkers have been proven to be associated with the prognosis of cancer. Mezquita et al demonstrated that the IPI combined with the LDH level and dNLR was significantly associated with treatment outcomes in patients with NSCLC.25 Furthermore, use of the IPI has been proven effective for predicting the prognosis in patients with RCC and melanoma.24,26
In this cohort of 139 patients, the level of dNLR and LDH had significant associations with OS. Using a combination of these two parameters, an IPI-based scoring system for GBC had developed. This analysis revealed that a poor IPI was significantly associated with shorter OS both in the overall population of the cohort and the subgroups divided by TNM stages. Compared with patients in the good IPI group, patients in the poor IPI group were more likely to have worse survival outcomes and poorer surgical outcomes, including longer hospitalization and more postoperative complications.
The NLR may reflect the host’s systemic response to tumor-induced inflammation. Neutrophils can secrete several cytokines to help suppress the tumor-induced T-cell response which elicits tumorigenesis and metastasis.30 A lower lymphocyte count, which leads to a higher NLR, indicates a decreased antitumor response.31,32 LDH takes part in the last step of glycolysis by reversibly catalyzing the conversion of pyruvate to lactate.33 Because cancer cells use glycolysis for energy production, most cancer cells rely on lactate production for their survival. Therefore, the LDH level is a classic marker revealing the metabolic activity of tumor in patients with cancer. Many analyses have revealed that the NLR and LDH level are significantly associated with OS in patients with melanoma,34 biliary cancer,35 and testicular diffuse large B-cell lymphoma.15 Because the absolute lymphocyte count is not routinely documented in clinical trials despite measurement of the differential white blood cell count, the dNLR is calculated using the white blood cell count and absolute neutrophil count and has become an alternative to the NLR. A study conducted by Proctor et al36 showed that the prognostic value of the dNLR was similar to that of the NLR in different solid cancers.
The similar combination of metabolic and inflammation including GLR (glucose to lymphocyte ratio). It is proved to be one of the independent factors affecting the OS of GBS patients after surgical resection,37 which represent the aggressive biologic behavior of gallbladder cancer. However, the research of IPI mainly focused on all the GBS patients with radical resection, the investigation of GLR was mainly focused on the GBS patients with diabetes. It is currently difficult to determine which indicators’ combination is better because of the different population. Further research is needed to explore the contrast between GLR and IPI.
The previously published dNLR cut-off value by Proctor36 is 2.0, which provides less prognostic value than the cut-off value of 1.4 in our cohort. The same situation occurred in the research conducted by Gyeong-Won.38 The discrepancy between these cut-off values might be due to the differences in tumor types and our limited population. The cut-off values of IPI require further validation in larger and independent cohorts.
In terms of grouping, Mezquita et al divided the IPI into three groups: good, intermediate, and poor. This analysis found that the main difference of IPI in OS was limited in the poor IPI group, and there was no significant difference in OS between the good and intermediate IPI groups. This was also found in patients with RCC in a study by Daniel et al.39 Considering the smaller population size of our cohort, we merged the good and intermediate IPI groups into one group.
For more accurate prediction of survival of patients with GBC, a prognostic nomogram using was constructed, using the factors selected according to the results of the Cox proportional hazards model: IPI, CA19-9, curative surgery, and postoperative chemoradiotherapy. The nomogram predicts the 1-, 3-, and 5-year survival probabilities. More assessments were performed using DCA, concordance index and ROC curves, which showed that our predictive model had satisfactory predictive ability, clinical utility, and improvement over the current staging system. The comparison of DCA, C-index, and ROC between the nomogram with and without IPI showed that IPI is an important factor in predicting the prognosis of GBS patients. We found that according to the nomogram, the survival of patients in the same TNM staging group can still be differed. The result indicates that the nomogram provides more precise prognostic information.
Besides, just as like other tumors, GBC results from the accumulation of multiple genetic alterations. Extensive research showed that a number of genetic alterations, such as TP53, KRAS, NRAS, and IDH1, played an important role in progression of GBC. The molecular characteristics of GBC have obvious heterogeneity and there were significant differences in survival between different molecular subgroups based on molecular characteristics. Therefore, the molecular characteristics should be considered as factors added to the prognostic model of GBC in the future. Besides, Whether IPI is associated with some of these genetic changes is unknown.
Our study has several limitations. First, retrospective data were used from a rather small population at a single institution; thus, bias cannot be avoided. Second, the validation of this study is an internal validation, further external validation is needed. Third, the TNM staging of the patients may have heterogeneity, which needs to be excluded through more precise and strict research. Finally, other factors that may influence survival, such as jaundice and lymph node metastasis, were not considered in this prognosis model.
Conclusions
In conclusion, this study is the first to demonstrate that the IPI is a prognostic indicator for patients with GBC. Our data showed that the IPI was an independent predictor of OS in patients with GBC, and a suitable prognostic nomogram was established. If these results are validated, this IPI-based nomogram can be reliably used for prognostic prediction in patients with GBC. Further validation through a large-population, multicenter, prospective study is needed.
Ethics and Consent
Ethical approval was obtained from the ethics committees of the PUMC Hospital of the Chinese Academy of Medical Sciences. The study was accompanied with the ethical criteria of the Declaration of Helsinki. Informed consent was not required because of the retrospective nature of the study. All patient data accessed complied with relevant data protection and privacy regulations. The study was registered in Research Registry and the unique Identifying number is 5561. The Hyperlink to this specific registration is: https://www.researchregistry.com/browse-the-registry#home/registrationdetails/5eac1b9fd0b7cd0015832876/.
Acknowledgment
This work was supported by grants from CAMS Innovation Fund for Medical Sciences (CIFMS) (No.2016-I2M-1-001) and Tsinghua University-Peking Union Medical College Hospital Cooperation Project (PTQH201904552). The funding source had no involvement in the works.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yang P, Javle M, Pang F, et al. Somatic genetic aberrations in gallbladder cancer: comparison between Chinese and US patients. Hepatobiliary Surg Nutr. 2019;8:604–614. doi:10.21037/hbsn.2019.04.11
2. Shaffer E, Hundal R. Gallbladder cancer: epidemiology and outcome. Clin Epidemiol. 2014;99. doi:10.2147/CLEP.S37357
3. Choi YH, Lee JW, Lee SH, et al. A high monocyte-to-lymphocyte ratio predicts poor prognosis in patients with advanced gallbladder cancer receiving chemotherapy. Cancer Epidemiol Biomarkers Prev. 2019:
4. Chen M, Lin J, Cao J, et al. Development and validation of a nomogram for survival benefit of lymphadenectomy in resected gallbladder cancer. Hepatobiliary Surg Nutr. 2019;8:480–489. doi:10.21037/hbsn.2019.03.02
5. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
6. Bai Y, Liu Z-S, Xiong J-P, et al. Nomogram to predict overall survival after gallbladder cancer resection in China. World J Gastroenterol. 2018;24(45):5167–5178. doi:10.3748/wjg.v24.i45.5167
7. Mislav Raki Ć, Patrlj L, Kopljar M, et al. Gallbladder cancer. Hepatobiliary Surg Nutr. 2014;3(5).
8. Amin MB, Greene FL, Edge SB, et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging: the eighth edition AJCC cancer staging manual. CA Cancer J Clin. 2017;67(2):93–99. doi:10.3322/caac.21388
9. Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):e493–e503. doi:10.1016/S1470-2045(14)70263-3
10. Gabrilovich DI, Ostrand-Rosenberg S, Bronte V. Coordinated regulation of myeloid cells by tumours. Nat Rev Immunol. 2012;12(4):253–268. doi:10.1038/nri3175
11. McMillan DC. Systemic inflammation, nutritional status and survival in patients with cancer. Curr Opin Clin Nutr Metab Care. 2009;12(3):223–226. doi:10.1097/MCO.0b013e32832a7902
12. Proctor MJ, Morrison DS, Talwar D, et al. An inflammation-based prognostic score (mGPS) predicts cancer survival independent of tumour site: a glasgow inflammation outcome study. Br J Cancer. 2011;104(4):726–734. doi:10.1038/sj.bjc.6606087
13. Pichler M, Hutterer GC, Stojakovic T, Mannweiler S, Pummer K, Zigeuner R. High plasma fibrinogen level represents an independent negative prognostic factor regarding cancer-specific, metastasis-free, as well as overall survival in a European cohort of non-metastatic renal cell carcinoma patients. Br J Cancer. 2013;109(5):1123–1129. doi:10.1038/bjc.2013.443
14. Chen Y-M, Lai C-H, Chang H-C, et al. Baseline and trend of lymphocyte-to-monocyte ratio as prognostic factors in epidermal growth factor receptor mutant non-small cell lung cancer patients treated with first-line epidermal growth factor receptor tyrosine kinase inhibitors. PLoS One. 2015;10(8):e0136252. doi:10.1371/journal.pone.0136252
15. Yang J, Guo X, Hao J, Dong Y, Zhang T, Ma X. The prognostic value of blood-based biomarkers in patients with testicular diffuse large b-cell lymphoma. Front Oncol. 2019;9:1392. doi:10.3389/fonc.2019.01392
16. Absenger G, Szkandera J, Pichler M, et al. A derived neutrophil to lymphocyte ratio predicts clinical outcome in stage II and III colon cancer patients. Br J Cancer. 2013;109(2):395–400. doi:10.1038/bjc.2013.346
17. Ferrucci PF, Ascierto PA, Pigozzo J, et al. Baseline neutrophils and derived neutrophil-to-lymphocyte ratio: prognostic relevance in metastatic melanoma patients receiving ipilimumab. Ann Oncol. 2018;29(2):524. doi:10.1093/annonc/mdx059
18. Hopkins AM, Rowland A, Kichenadasse G, et al. Predicting response and toxicity to immune checkpoint inhibitors using routinely available blood and clinical markers. Br J Cancer. 2017;117(7):913–920. doi:10.1038/bjc.2017.274
19. Russo A, Franchina T, Ricciardi GRR, et al. Baseline neutrophilia, derived neutrophil-to-lymphocyte ratio (dNLR), platelet-to-lymphocyte ratio (PLR), and outcome in non small cell lung cancer (NSCLC) treated with Nivolumab or Docetaxel. J Cell Physiol. 2018;233(10):6337–6343. doi:10.1002/jcp.26609
20. Tas F, Aykan F, Alici S, Kaytan E, Aydiner A, Topuz E. Prognostic factors in pancreatic carcinoma. Am J Clin Oncol. 2001;24(6):4. doi:10.1097/00000421-200112000-00003
21. Fahmueller YN, Nagel D, Hoffmann R-T, et al. Predictive and prognostic value of circulating nucleosomes and serum biomarkers in patients with metastasized colorectal cancer undergoing selective internal radiation therapy. BMC Cancer. 2012;12(1):5. doi:10.1186/1471-2407-12-5
22. Girgis H, Masui O, White NM, et al. Lactate Dehydrogenase A is a potential prognostic marker in clear cell renal cell carcinoma. Mol Cancer. 2014;13(1):101. doi:10.1186/1476-4598-13-101
23. Zhao Z, Han F, Yang S, Hua L, Wu J, Zhan W. The clinicopathologic importance of serum lactic dehydrogenase in patients with gastric cancer. Dis Markers. 2014;2014:1–7. doi:10.1155/2014/140913
24. Yi JH, Kim JH, Baek KK, et al. Elevated LDH and paranasal sinus involvement are risk factors for central nervous system involvement in patients with peripheral T-cell lymphoma. Ann Oncol. 2011;22(7):1636–1643. doi:10.1093/annonc/mdq645
25. Mezquita L, Auclin E, Ferrara R, et al. Association of the lung immune prognostic index with immune checkpoint inhibitor outcomes in patients with advanced non–small cell lung cancer. JAMA Oncol. 2018;4(3):351. doi:10.1001/jamaoncol.2017.4771
26. Sorich MJ, Rowland A, Karapetis CS, Hopkins AM. Evaluation of the lung immune prognostic index for prediction of survival and response in patients treated with atezolizumab for nsclc: pooled analysis of clinical trials. J Thorac Oncol. 2019;14(8):1440–1446. doi:10.1016/j.jtho.2019.04.006
27. Randi G, Franceschi S, La Vecchia C. Gallbladder cancer worldwide: geographical distribution and risk factors. Int J Cancer. 2006;118(7):1591–1602. doi:10.1002/ijc.21683
28. Aloia TA, Járufe N, Javle M, et al. Gallbladder cancer: expert consensus statement. HPB. 2015;17(8):681–690. doi:10.1111/hpb.12444
29. Wu Y, Zhou BP. Inflammation: A driving force speeds cancer metastasis. Cell Cycle. 2009;8(20):3267–3273. doi:10.4161/cc.8.20.9699
30. Ardi VC, Kupriyanova TA, Deryugina EI, Quigley JP. Human neutrophils uniquely release TIMP-free MMP-9 to provide a potent catalytic stimulator of angiogenesis. Proc Natl Acad Sci. 2007;104(51):20262–20267. doi:10.1073/pnas.0706438104
31. Kobayashi N, Usui S, Kikuchi S, et al. Preoperative lymphocyte count is an independent prognostic factor in node-negative non-small cell lung cancer. Lung Cancer. 2012;75(2):223–227. doi:10.1016/j.lungcan.2011.06.009
32. Milne K, Alexander C, Webb JR, et al. Absolute lymphocyte count is associated with survival in ovarian cancer independent of tumor-infiltrating lymphocytes. J Transl Med. 2012;10(1):33. doi:10.1186/1479-5876-10-33
33. Bui T, Thompson CB. Cancer’s sweet tooth. Cancer Cell. 2006;9(6):419–420. doi:10.1016/j.ccr.2006.05.012
34. Capone M, Giannarelli D, Mallardo D, et al. Baseline neutrophil-to-lymphocyte ratio (NLR) and derived NLR could predict overall survival in patients with advanced melanoma treated with nivolumab. J Immunother Cancer. 2018;6(1):74. doi:10.1186/s40425-018-0383-1
35. Salati M, Filippi R, Vivaldi C, et al. The prognostic nutritional index predicts survival and response to first‐line chemotherapy in advanced biliary cancer. Liver Int. 2020;40(3):704–711. doi:10.1111/liv.14314
36. Proctor MJ, McMillan DC, Morrison DS, Fletcher CD, Horgan PG, Clarke SJ. A derived neutrophil to lymphocyte ratio predicts survival in patients with cancer. Br J Cancer. 2012;107(4):695–699. doi:10.1038/bjc.2012.292
37. Navarro J, Kang I, Hwang HK, et al. Glucose to lymphocyte ratio as a prognostic marker in patients with resected pt2 gallbladder cancer. J Surgical Res. 2019;8(240):17–29. doi:10.1016/j.jss.2019.02.043
38. Lee G-W, Park SW, Go S-I, et al. The derived neutrophil-to-lymphocyte ratio is an independent prognostic factor in transplantation ineligible patients with multiple myeloma. Acta Haematol. 2018;140(3):146–156. doi:10.1159/000490488
39. Meyers DE, Stukalin I, Vallerand IA, et al. The Lung Immune Prognostic Index Discriminates Survival Outcomes in Patients with Solid Tumors Treated with Immune Checkpoint Inhibitors. Cancers (Basel). 2019;11(11):1713. doi:10.3390/cancers11111713
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.