")
Back to Journals » International Journal of General Medicine » Volume 14
Preliminary Exploration of Setting the Disease Severity Score in the Nutritional Risk Screening of Patients with Severe Novel Coronavirus Pneumonia by Applying NRS2002
Authors Sun Y, He J, Li W, Li S, Lin Y, Cen Y, Li Y
Received 27 November 2020
Accepted for publication 1 March 2021
Published 31 March 2021 Volume 2021:14 Pages 1167—1172
DOI https://doi.org/10.2147/IJGM.S289655
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Yanbo Sun,1,* Jing He,2,* Weiming Li,1,* Shumin Li,1 Yueying Lin,1 Yunyun Cen,1 Yanli Li3
1Department of Gastrointestinal Surgery, The Second Affiliated Hospital of Kunming Medical University, Kunming, 650000, People’s Republic of China; 2The First Department of Infectious Disease, The Third People’s Hospital of Kunming, Kuming, 650041, People’s Republic of China; 3First Department of Pulmonary and Critical Care Medicine, Yan’an Hospital of Kunming City/Yan’an Hospital Affiliated to Kunming Medical University, Yunnan, 650000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yunyun Cen
Department of Gastrointestinal Surgery, The Second Affiliated Hospital of Kunming Medical University, No. 374 of Yunnan-Burma Road, Kunming City, Yunnan Province, 650101, People’s Republic of China
Tel +86-871-63402778
Fax +86-871-65361017
Email [email protected]
Objective: This study was designed to explore the impact of different scoring settings of disease severity on the accuracy of screening by NRS2002.
Methods: Patients with severe COVID-19 who were admitted to our hospital from January 26, 2020, to March 16, 2020, were enrolled in this study. The basic data, the scores of the NRS2002 score sheet, and the serum prealbumin (PAB) level when these patients were admitted were collected, and the reflection of NRS2002 scores under different disease severity score settings to abnormal patients was analyzed.
Results: 1. When the severity of the disease was set to 0 points, four of the six hospitalized patients with PAB levels below the lower normal limit were not screened out; 2. When the severity was set to 1 point, two patients with COVID-19 who developed to a severe stage during the treatment process were screened out, but three of the six hospitalized patients with PAB levels below the lower normal limit at admission were not screened out; 3. When the severity of the disease of a patient with severe COVID-19 and fever scored 2 points, and that of a patient without fever scored 1 point, two patients with COVID-19 who developed to the severe stage during the treatment process were screened out, and six patients who were hospitalized with PAB levels below the lower normal limit at admission were also screened out.
Conclusion: When the severe degree of patients with COVID-19 and fever is rated as 2 points, and that of the patients without fever is rated as 1 point, it can more accurately reflect the severity degree of patients with undernourishment.
Keywords: novel coronavirus pneumonia, severe patients, nutritional risk, NRS2002, prealbumin
Introduction
The novel coronavirus pneumonia that started in Wuhan in December 2019 (COVID-19) spread rapidly worldwide, causing a world pandemic. The complication rate in severe cases is as high as 94.8%.1–4 According to the diagnostic criteria of the “Novel Coronavirus Infection Pneumonia Diagnosis and Treatment Plan (Trial Seventh Edition),” COVID-19 can be divided into four types: mild, common, severe, and critical.5 So far, no clear and effective drugs have been found for COVID-19, so the maintenance of the nutritional status of patients with severe and critical COVID-19 must become an important “line of defense” for patients to recover. The Nutrition Risk Screening 2002 (NRS2002) is a nutritional risk screening tool for inpatients proposed by Professor Kondrup of Denmark. In 2002, it was recommended by the European Nutrition Society as the preferred tool for nutritional risk screening of inpatients. Its score includes three parts: disease severity score, nutritional status score, and age score.6,7 Studies in China have also confirmed the obvious superiority of NRS2002 in the nutritional risk screening of hospitalized patients.8–10 Nutritional interventions based on NRS2002 implementation norms can effectively reduce the rate of nosocomial infections and improve the prognosis of patients.11 The “Novel Coronavirus (2019-nCoV) Pneumonia Diagnosis and Treatment Quick Recommendation Guide (Standard Edition)” also gives recommendations for the use of NRS2002 for nutritional risk screening.12 According to China’s guidelines and expert consensus, we have used the NRS2002 scale recommended by the guidelines and consensus to carry out nutritional risk screening and assessment since the beginning of the COVID-19 epidemic. However, due to the particularity of the COVID-19 epidemic, the disease severity score in the NRS2002 scale is not accurate and reliable at present. The rough use of the existing severe pneumonia score may cause data bias and lead to poor results. In this paper, we carried out a retrospective study to explore the impact of different scoring settings of disease severity on the accuracy of screening by NRS2002.
Information and Methods
Subjects
According to the inclusion and exclusion criteria, 15 patients with severe COVID-19 who were admitted to our hospital from January 26, 2020, to March 16, 2020, were enrolled in this study.
Inclusion and Exclusion Criteria
Inclusion criteria: age >18 years old; no weight deficiency; severe New Coronavirus pneumonia. (diagnostic criteria reference Notification of the issuance of pneumonia diagnosis and treatment protocol for novel coronavirus infection)5
Exclusion criteria: tumor history, digestive system surgery history, antibiotic use history within 3 months, immunosuppression (AIDS, glucocorticoid, immunosuppressant), primary cardiac insufficiency, liver insufficiency, renal insufficiency, pulmonary dysfunction.
The 15 patients included in this study were all healthy people in the past.
Observation Indexes
Data collection process: after the outbreak in December 2019, we found that the patients were under too much pressure, which seriously affected their dietary intake. Due to the time difference between the onset and admission of most patients, there were problems in the routine admission nutritional risk screening score. Novel coronavirus pneumonia was evaluated by the “NRS2002 score”. We evaluated the severity of the disease in the NRS2002 score according to the “light and ordinary” score of 0. The “heavy and severe” group referred to the “severe pneumonia” score of 2 points. But during the course of the disease, we found that the definition of “severe and severe” in new crown pneumonia was significantly different from that of the previous severe pneumonia. There will be a major loophole in the clinical and scientific research of nutritional risk screening using NRS2002. Therefore, we excluded the underage patients and the patients with complications that may affect the conclusion from the case bank, and finally included the data of 15 patients. We wrote this article to remind the relevant professionals in the field to pay attention to the research and discussion in this direction and solve this problem.
The patients’ admission age, gender, pre-hospital illness time, NRS2002 score, PAB level at admission, and illness recovery were collected.
Statistics Analysis
Statistical software SPSS20.0 was used for statistical analysis and plotting. Measurement data were expressed as median and IQRs. Categorical variables are expressed and compared with rates. The effect was evaluated according to the screening rate.
Results
General Data
The medical data of 15 patients with severe COVID-19 who were diagnosed at admission were included. After treatment, two of these 15 patients developed to severe COVID-19, and no deaths occurred. General data are presented in Table 1, and respiratory indexes are presented in Table 2.
 |
Table 1 General Clinical Data of Patients |
 |
Table 2 Respiratory Related Indexes of Patients at Admission |
Correlation Between NRS2002 Score and PAB Level When Severe COVID-19 Severity Rated 0 Points
If the severity of severe COVID-19 was set to 0 points, two of these 15 patients had NRS2002 scores of ≥3 points, accounting for 13.33%. One of the two patients with COVID-19 who developed to the severe stage during the treatment process had an NRS2002 score of <3 points and four of the six patients hospitalized with PAB levels below the lower normal limit at admission were also not screened out (Figure 1A and B).
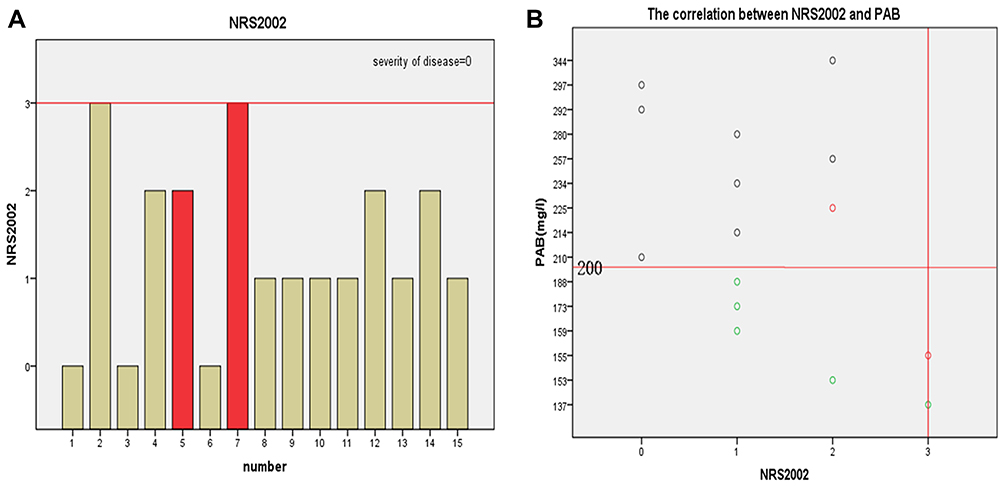 |
Figure 1 (A and B) Correlation between NRS2002 score and PAB level when severe COVID-19 severity is scored 0 points. Notes: The red column bar indicates patients with COVID-19 who developed to the severe stage during the treatment process. The green scatter points are hospitalized patients with PAB levels below the lower normal limit at admission, and the red column scatter points are patients with COVID-19 who developed to the severe stage during the treatment process. |
If the severity of severe COVID-19 was set to 1 point, then six of these 15 patients had NRS2002 scores of ≥3 points, accounting for 40%. Two patients with COVID-19 who developed to the severe stage during the treatment process were screened out, and three of the six patients hospitalized with PAB levels below the lower normal limit at admission were screened out, accounting for 50% (Figure 2A and B).
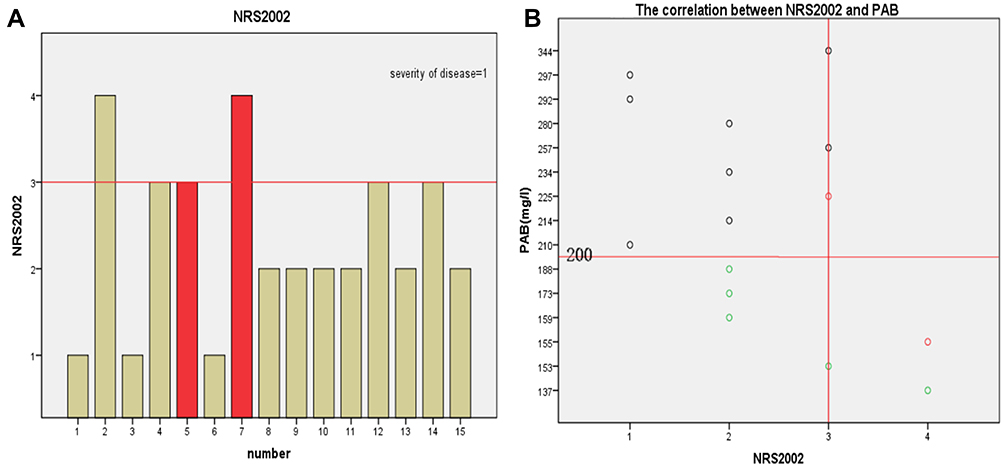 |
Figure 2 (A and B) Correlation between NRS2002 score and PAB level when severe COVID-19 severity is scored 1 point. Notes: The red column bar indicates patients with COVID-19 who developed to the severe stage during the treatment process. The green scatter points are hospitalized patients with PAB levels below the lower normal limit at admission, and the red column scatter points are patients with COVID-19 who developed to the severe stage during the treatment process. |
Correlation Between NRS2002 Score and PAB Level When the Severity of the Disease of a Patient with Severe COVID-19 and Fever Was Scored 2 Points, and That of a Patient Without Fever Was Scored 1 Point
When the severity of the disease of a patient with severe COVID-19 and fever was scored 2 points, and that of a patient without fever was scored 1 point, then 11 of these 15 patients had NRS2002 scores of ≥3 points, accounting for 73.33%. Two patients with COVID-19 who developed to the severe stage during the treatment process were screened out, and three of the six patients hospitalized with PAB levels below the lower normal limit at admission were screened out (Figure 3A and B).
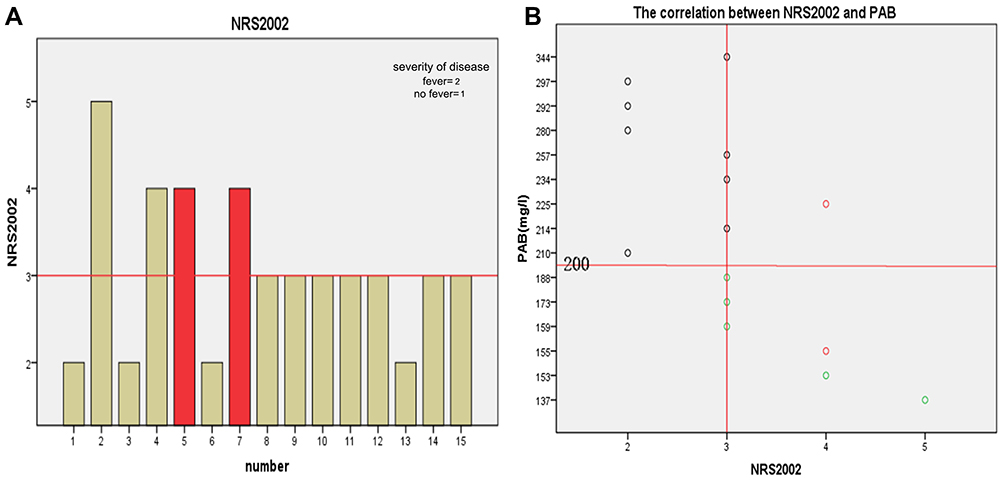 |
Figure 3 (A and B) Correlation between NRS2002 score and PAB level when severe COVID-19 severity is scored 2 points. Notes: The red column bar indicates patients with COVID-19 who developed to the severe stage during the treatment process. The green scatter points are hospitalized patients with PAB levels below the lower normal limit at admission. |
Discussion
COVID-19 is an acute respiratory infectious disease caused by a novel coronavirus infection. Since it was discovered in Wuhan in December 2019, it has spread rapidly in China. After the epidemic situation outbreak, all aspects of COVID-19 were studied by scholars of respiratory illnesses, infections, and viruses. The “Quick Recommendation and Guidelines for the Diagnosis and Treatment of Pneumonia Caused by Novel Coronavirus (2019-nCoV) Infection (Standard Version)” recommends that nutritional risk screening and nutritional intervention should be carried out using NRS2002 at admission. However, there is no public report of such data so far.
When patients with COVID-19 were first received, the investigators found that most patients had obvious anorexia. NRS2002 was used to carry out nutritional risk screening. The score of disease severity of severe COVID-19 was initially set as 2 points, and patients with NRS2002 scores of ≥3 points were treated with diet and nutritional support education or diet and oral nutrition supplement. All 15 patients recovered and were discharged, and no deaths occurred. In the process of diagnosis and treatment, the novel coronavirus pneumonia severity score in the course of NRS2002 application was reviewed. Combined with the “COVID-19 classification standard,” the disease severity score with 2 points in NRS2002 seemed to be inappropriate, so the literature was reviewed, and a retrospective review was carried out preliminarily.
NRS2002 was proposed by Kondrup et al in Denmark after analyzing 128 randomized controlled trial (RCT) studies. It is based on the following concepts: nutritional support is suitable for patients with severe illness or severe malnutrition who have increased nutritional needs, or patients with a certain degree of disease severity and a certain degree of malnutrition.13 However, NRS2002 has only specified “chronic obstructive pulmonary disease (COPD), severe pneumonia” in the disease severity score standard; there is no evidence to support the scores of all types of COVID-19. In this study, only the NRS2002 disease severity score of severe COVID-19 was discussed initially.
Serum PAB is synthesized by hepatocytes, which is a carrier protein. Its molecular weight is smaller than that of albumin. The half-life is about two days. This protein is recognized as one of the indexes that can better reflect the changes in short-term nutritional status.14,15 Limited by conventional detection conditions in this study, patients with serum prealbumin levels lower than normal were defined as patients with abnormal nutritional status, according to the different scoring standards of NRS2002, and a preliminary analysis was carried out.
The first step of this study is that the NRS2002 disease severity score of severe COVID-19 was set to 0 points. Retrospective analysis revealed that only two of these 15 patients had NRS2002 scores of ≥3 points, accounting for 13.33%, and the NRS2002 score of one patient with COVID-19 who developed to the severe stage during the treatment process was less than 3 points (Figure 1A and B). Four of the six patients hospitalized with PAB levels below the lower normal limit at admission were not screened out (Figure 1A and B). This suggests that setting the NRS2002 disease severity score of severe COVID-19 as 0 points cannot reflect the malnutrition of patients and also does not reflect the patients with a poor prognosis. In the second step, the NRS2002 disease severity score of severe COVID-19 was set to 1 point to observe the effect. Retrospective analysis revealed that when the NRS2002 disease severity score of severe COVID-19 was set to 1 point, six of these 15 patients had NRS2002 scores of ≥3 points, accounting for 40%. Two patients with COVID-19 who developed to the severe stage during the treatment process were screened out (Figure 2A and B), and three of the six patients hospitalized with PAB levels below the lower normal limit at admission were screened out, accounting for 50% (Figure 2A and B). Although two patients with COVID-19 who developed to the severe stage during the treatment process were screened out under this condition, three (50%) of six patients hospitalized with PAB levels below the lower normal limit at admission were not screened out. Patients with short-term malnutrition were not fully monitored.
COVID-19 is a type of viral pneumonia. If the score of disease severity of all patients with severe COVID-19 is set as 2 points, the same as the score for patients with severe pneumonia, this is contrary to the results of RCT studies involved in NRS2002. Therefore, Professor Kondrup’s NRS2002 contribution was reviewed.13 We found that it is stated after the disease severity (≈ stress metabolism), in addition to patients’ serious panic about COVID-19, the disease severity score of some patients with fever was raised to 2 points, and the disease severity score of the other patients was still set to 1 point, 11 of these 15 patients had NRS2002 scores of ≥3 points, accounting for 73.33%. Two patients with COVID-19 who developed to the severe stage during the treatment process were screened out (Figure 3A and B), and all of the six patients hospitalized with PAB levels below the lower normal limit at admission were screened out (Figure 3A and B). Under this condition, NRS2002 has monitored all patients with malnutrition and poor prognosis.
In summary, According to the existing authoritative guidelines and consensus recommendations, nutritional risk screening is the first step for COVID-19 patients to receive clinical nutritional support.12,16,17 In the absence of high-quality RCT research support, different disease severity scores will screen out different populations. In mild cases, it wastes human resources and material resources. In serious cases, it will delay “opportunity for combat.” Therefore, we should be careful when using NRS2002 for nutritional risk screening. On the basis of the results of this study, the investigators consider that patients with severe COVID-19 and fever should be rated as 2 points, and patients with severe COVID-19 without fever should be rated as 1 point, which seems to be a better choice for patients who are undernourished. When the disease severity score of severe pneumonia in the NRS2002 score sheet is set to 2 points, the accuracy of the later treatment plan and RCT evidence supports that a uniform score of 1 for disease severity of patients with severe COVID-19 seems very likely. It is expected that the multi-center large sample data will illustrate the problem.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of The second Affiliated Hospital of Kunming Medical University. This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Funding
Yunnan Province Medical Discipline Reserve Talent Training Program (H-2018067) and the Special Fund for Famous Doctors of the Second Affiliated Hospital of Kunming Medical University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Guan WJ, Ni ZY, Hu Y, et al; China Medical Treatment Expert Group for Covid-19. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720. PMID: 32109013; PMCID: PMC7092819. doi:10.1056/NEJMoa2002032.
2. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. PMID: 31986264; PMCID: PMC7159299. doi:10.1016/S0140-6736(20)30183-5
3. Lu R, Zhao X, Li J, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020;395(10224):565–574. PMID: 32007145; PMCID: PMC7159086. doi:10.1016/S0140-6736(20)30251-8.
4. Zhu N, Zhang D, Wang W, et al; China Novel Coronavirus Investigating and Research Team. A novel coronavirus from patients with Pneumonia in China, 2019. N Engl J Med. 2020;382(8):727–733. PMID: 31978945; PMCID: PMC7092803. doi:10.1056/NEJMoa2001017.
5. General Office of the National Health Commission. Office of the State Administration of Chinese Medicine. Notification of the issuance of pneumonia diagnosis and treatment protocol for novel coronavirus infection (pilot version 7) [EB/OL]; 2020. Available from: http://www.nhc.gov.cn/xcs/zhengcwj/202003/46c9294a7dfe4cef80dc7f5912eb1989.shtml.
6. Kondrup J, Allison SP, Elia M, Vellas B, Plauth M; Educational and Clinical Practice Committee, European Society of Parenteral and Enteral Nutrition (ESPEN). ESPEN guidelines for nutrition screening 2002. Clin Nutr. 2003;22(4):415–421. PMID: 12880610. doi:10.1016/s0261-5614(03)00098-0.
7. Rabito EI, Marcadenti A, da Silva Fink J, Figueira L, Silva FM. Nutritional risk screening 2002, short nutritional assessment questionnaire, malnutrition screening tool, and malnutrition universal screening tool are good predictors of nutrition risk in an emergency service. Nutr Clin Pract. 2017;32(4):526–532. PMID: 28199797. doi:10.1177/0884533617692527
8. Miao JP, Quan XQ, Zhang CT, et al. Comparison of two malnutrition risk screening tools with nutritional biochemical parameters, BMI and length of stay in Chinese geriatric inpatients: a multicenter, cross-sectional study. BMJ Open. 2019;9(2):e022993. PMID: 30782871; PMCID: PMC6411257. doi:10.1136/bmjopen-2018-022993.
9. Dong W, Liu X, Zhu S, et al. Selection and optimization of nutritional risk screening tools for esophageal cancer patients in China. Nutr Res Pract. 2020;14(1):20–24. PMID: 32042370; PMCID: PMC6997145. doi:10.4162/nrp.2020.14.1.20
10. Wang J, Yu B, Ye Y, et al. Predictive value of nutritional risk screening 2002 and prognostic nutritional index for esophageal cancer patients undergoing definitive radiochemotherapy. Nutr Cancer. 2018;70(6):879–885. PMID: 30273001. doi:10.1080/01635581.2018.1470656
11. Sun DL, Li WM, Li SM, et al. Impact of nutritional support that does and does not meet guideline standards on clinical outcome in surgical patients at nutritional risk: a prospective cohort study. Nutr J. 2016;15(1):78. doi:10.1186/s12937-016-0193-6.
12. Hui JY, Lin C, Shun CZ, et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). J PLA Med. 2020;1.
13. Kondrup J, Rasmussen HH, Hamberg O, Stanga Z; Ad Hoc ESPEN Working Group. Nutritional risk screening (NRS 2002): a new method based on an analysis of controlled clinical trials. Clin Nutr. 2003;22(3):321–336. PMID: 12765673. doi:10.1016/s0261-5614(02)00214-5.
14. Xuehong W, Xuefeng L. Diagnostics.
15. Xiaoping C, Jianping W, Jizong Z. Surgery.
16. CSPEN. Expert advice for enteral parenteral nutrition in critically ill patients with New Coronavirus pneumonia. Chin Med J. 2020;100(12):889–892. doi:10.3760/cma.j.cn112137-20200212-00261.
17. Barazzoni R, Sc B, Krznaric Z, et al. ESPEN expert statements and practical guidance for nutritional management of individuals with SARS-CoV-2 infection[J]. Clin Nutr. 2020;39(6):1631–1638. doi:10.1016/j.clnu.2020.03.022
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.