")
Back to Journals » Clinical Interventions in Aging » Volume 18
Preferences and Attitudes Towards Life-Sustaining Treatments of Older Chinese Patients and Their Family Caregivers
Authors Zhu T , Liu D, van der Heide A, Korfage IJ, Rietjens JA
Received 9 November 2022
Accepted for publication 21 February 2023
Published 23 March 2023 Volume 2023:18 Pages 467—475
DOI https://doi.org/10.2147/CIA.S395128
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Tingting Zhu,1,2 Dongling Liu,1 Agnes van der Heide,2 Ida J Korfage,2 Judith AC Rietjens2
1Department of Nursing and Health, Zhengzhou University, Zhengzhou, People’s Republic of China; 2Department of Public Health, Erasmus MC, University Medical Center Rotterdam, Rotterdam, the Netherlands
Correspondence: Dongling Liu, Email [email protected]
Purpose: The family plays a major role in medical decision-making in China. Little is known about whether family caregivers understand patients’ preference for receiving life-sustaining treatments and are able to make decisions consistent with them when patients are incapable of making medical decisions. We aimed to compare preferences and attitudes concerning life-sustaining treatments of community-dwelling patients with chronic conditions and their family caregivers.
Patients and Methods: We conducted a cross-sectional study among 150 dyads of community-dwelling patients with chronic conditions and their family caregivers from four communities in Zhengzhou. We measured preferences for life-sustaining treatments (cardiopulmonary resuscitation, mechanical ventilation, tube feeding, hemodialysis, chemotherapy), who should decide, the timing of making decisions, and their most important consideration.
Results: The consistency of preferences for life-sustaining treatments between patients and family caregivers was poor to fair, with kappa values ranging from 0.071 for mechanical ventilation to 0.241 for chemotherapy. Family caregivers more frequently preferred each life-sustaining treatment for the patients than the patients themselves. More family caregivers than patients preferred the patient to make their own decisions about life-sustaining treatments (29% of patients and 44% of family caregivers). The most important considerations when deciding on life-sustaining treatments are family burden and the patient’s comfort and state of consciousness.
Conclusion: There is a poor to fair consistency between community-dwelling older patients and their family caregivers in their preferences and attitudes towards life-sustaining treatments. A minority of patients and family caregivers preferred that patients make their own medical decisions. We recommend healthcare professionals to encourage discussions between patients and their families on future care to improve the mutual understanding within the family about medical decision-making.
Keywords: older patients, life-sustaining treatment, serious illness conversation, Asia, culture
Introduction
In most Western countries, patient-centered care requires healthcare professionals and families to respect and prioritize patients’ values and preferences.1 Advance care planning conversations are used to enable patients to discuss their goals and preferences for future care with their family and healthcare professionals, which may contribute to goal-concordant care.2,3 Family members often make medical decisions with patients in a collaborative manner or as surrogate decision-makers when patients are incapable of making their own decisions.4,5 However, surrogate decision-making for ill loved ones is complex and challenging because patients rarely discuss their preference for future care with their families.6 According to previous studies, less than half of the families can correctly predict patients’ preferences for future care.7,8 In Taiwan, a family-oriented society, agreements between cancer patients and their family caregivers have been found to decline over a decade,9 with patients preferring less aggressive medical treatment while families shifting towards greater uncertainty.10,11
In traditional Chinese society, the perceived taboo of discussing death-related topics and the partial or non-disclosure of bad news reduces the opportunity to understand the end-of-life goals and preferences of patients.12,13 Patients, particularly older patients are barely involved in making decisions about their own treatment and care, for reasons such as the family’s wish to maintain patients’ hope and preserve familial harmony.14 Healthcare professionals are likely to discuss serious illnesses with the family and to inform the patient only with the family’s consent.14–16 Some attempts to address this dilemma are occurring in mainland China, the “living will” legislation in Shenzhen has been enacted and implemented from January 1st, 2023. It stipulates healthcare professionals and families should respect patients’ choices on end-of-life medical treatments.17 The perception of patients’ preferences of the family is important to consider when making critical medical decisions for patients, in particular in a family-oriented society such as China.18 Understanding patients’ and their families’ preferences for future care and its consistency is essential to support care that is aligned to the patient’s preferences19 and help inform more national legislation on respecting patients’ choices.20
However, life-sustaining treatment preferences and their consistency between patients and families have been mainly investigated in Western countries and developed Eastern countries.21–23 Only limited evidence is available to inform clinical practice in regions with a family-oriented culture, such as mainland China.24 Therefore, the aim of this study was to investigate the preferences and attitudes of older Chinese patients and their family caregivers on life-sustaining treatment and their consistency.
Material and Methods
Study Design
A cross-sectional survey was conducted among patients and their family caregivers in Zhengzhou, from January 2019 to November 2019. This study was approved by the Ethics Review Committee of Zhengzhou University in Zhengzhou, China. This study complies with the Declaration of Helsinki.
Setting and Participants
We purposefully selected four communities served by a community healthcare center equipped with an electronic healthcare record system. Community residents with hypertension, diabetes, coronary heart disease, and stroke are registered in this system and were recruited by a consecutive sampling method. Records in the system were sorted by the date the record was created. Patients were recruited when they were aged ≥60 years old, were diagnosed with a chronic condition (hypertension, type 2 diabetes, stroke, coronary heart disease), provided informed consent; and their family caregiver also agreed to participate in the study. Family caregivers were recruited when they were aged ≥18 years; were designated by the patient as the primary caregiver; and were an unpaid caregiver.
Data Collection Process
The researcher used phone numbers from the system to contact patients. After the researcher introduced the purpose and procedures of the study, those patients interested in participating with their family caregivers were asked to make an appointment to complete questionnaire surveys. The sampling was stopped after 150 participants were included due to time constraints and limited resources. This survey was conducted in the participants’ homes. Patients and their family caregivers were asked to complete the questionnaire independently. The interviewer (T.Z.) used educational videos if patients or their family caregivers expressed difficulties in understanding specific life-sustaining treatments.
Survey Instrument
We developed a self-constructed questionnaire based on “the End-of-life Preferences Interview”.25 In addition, three community healthcare workers and three geriatric healthcare professionals critically reviewed the draft questionnaire, but no modification was made after their assessments. The questionnaire addressed the following topics:
- Demographic and clinical characteristics: age, gender, marital status, education level, religion, type of relation between patients and family caregivers (spouse/adult children). Patients were also asked about their main chronic condition (hypertension, type 2 diabetes, stroke, and coronary heart disease) and self-reported health status (scored on a 5-point scale from 1 - excellent to 5 - very poor).
- Preferences related to life-sustaining treatments were measured through four questions:
- “What treatment would you want to receive if you were incapable of making medical decisions?” (patients)/“When your family member was incapable of making medical decisions, what treatment do you wish he/she could receive?” (family caregivers). For each of the life-sustaining treatments (cardiopulmonary resuscitation, mechanical ventilation, tube feeding, hemodialysis, chemotherapy), answering options were “yes”, “no” and “never considered”.
- “If you are incapable of making medical decisions, who would you want to make decisions for you?”/“If the patient would be incapable of making medical decisions, who would you want to make decisions for him/her?”. The answering options were: “my previous decisions should be followed” (patients)/ “the patient’s previous decisions should be followed” (family caregivers), “family members”, and “healthcare providers”.
- “When do you think discussions about life-sustaining treatments should start?” The answering options were: “in a healthy state”, “when older than 60 years”, “when diagnosed with a life-limiting condition”, “when curative treatments are no longer effective”, “when life-sustaining treatments are inevitable due to deterioration”, “when initiated by healthcare providers”, and “when death is inevitable within a short period”.
- “What is your most important consideration when making decisions related to life-sustaining treatments?”. Answering options were “comfort”, “treatment affordability”, “state of consciousness”, “family burden”, and “others”.
The questionnaire is in Appendix 1.
Statistical Analysis
Means and standard deviations (SDs) were calculated for continuous variables, and frequencies and percentages were calculated for categorical variables. The agreement on preferences for life-sustaining treatments between patients and their family caregivers was analyzed using Cohen’s Kappa. Differences in patient and family caregiver’ preferences related to life-sustaining treatments were compared using chi squares. Fisher’s exact tests were applied for items where the expected count was <5. Data were analyzed using IBM SPSS for Windows version 20.0. A p-value<0.05 was considered statistically significant.
Results
Participants Demographic Information
Between January 2019 to November 2019, 150 pairs of patients and their family caregivers were enrolled. The demographic characteristics of participants are described in Table 1. The mean age of patients was 71 years (SD = 4.63) and family caregivers was 43 years (SD=5.48). More than half of all participants were female (75% of patients and 68% of family caregivers) and married (74% of patients and 81% of family caregivers); Less than ten percent of patients (8.7%) and the majority of family caregivers (90%) had received higher education (high school or university degree). Less than half of all participants were religious (20% of patients and 6% of family caregivers). Most of the patients (89%) reported a (very) good or excellent health status. Nearly half of the patients had hypertension (47%). The majority of family caregivers were the adult children of the patient (89%).
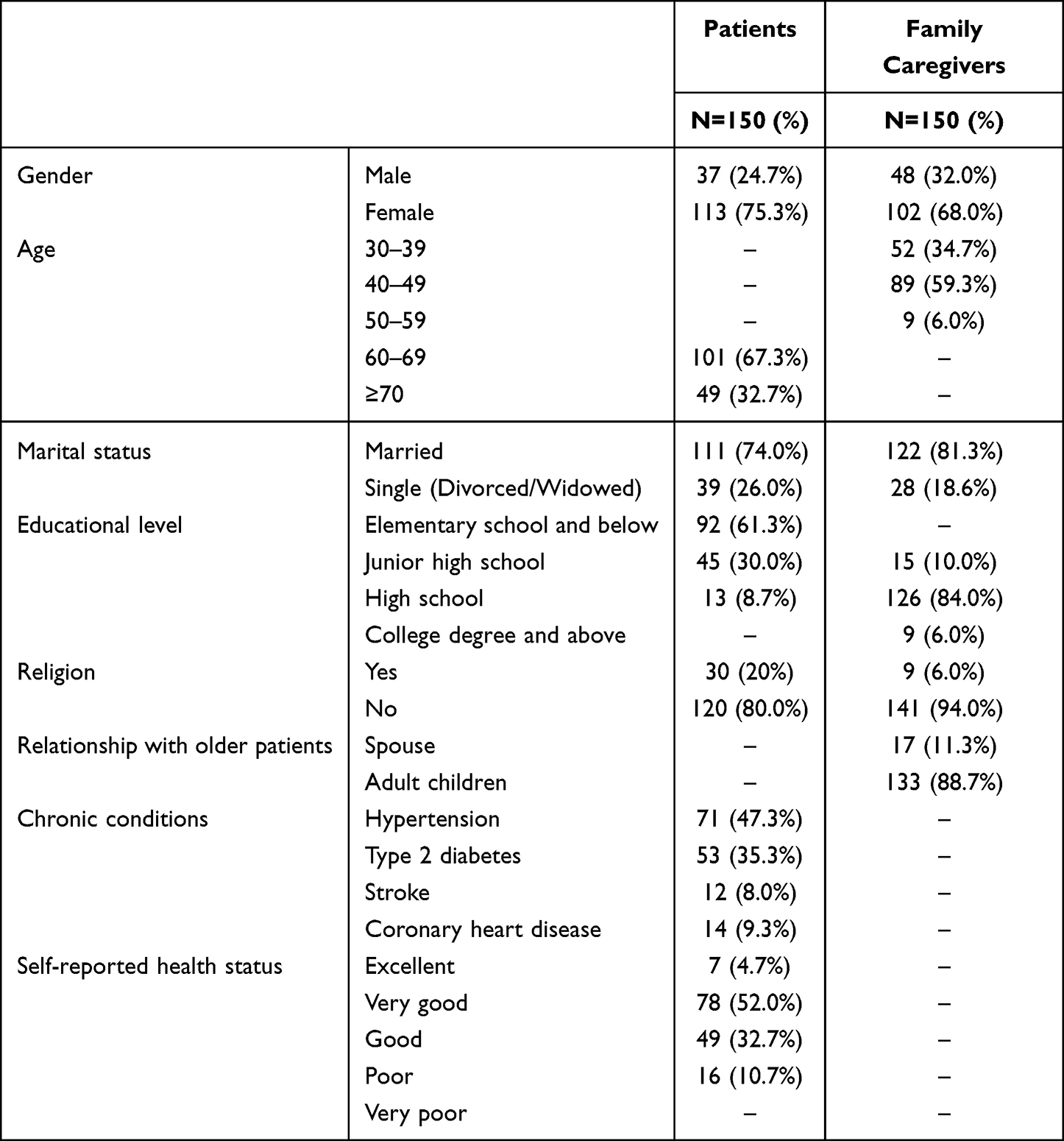 |
Table 1 Characteristics of Patients and Family Caregivers |
The Preferences of Patients and Their Family Caregivers on Life-Sustaining Treatment
According to the date in Table 2, for each of the life-sustaining treatments (cardiopulmonary resuscitation, mechanical ventilation, tube feeding, hemodialysis, chemotherapy), family caregivers more frequently than patients indicated that they would prefer that treatment for the patient in case the patient would be incapable of making medical decisions (0–67% for patients and 8–76% for family caregivers). Among the five treatment options, patients and family caregivers had the highest agreement in their preference for chemotherapy, with a Kappa value of 0.241 indicating fair agreement. None of the patients preferred chemotherapy, compared to 8% of family caregivers. The majority of both patients and family caregivers preferred tube feeding (67% and 70%, respectively), but their agreement was poor (kappa value =0.179). Most family caregivers (76%) preferred the patients to receive mechanical ventilation, but only 10% of patients preferred to receive mechanical ventilation, with low consistency (kappa value=0.071). Sixty-one percent of patients and 44% of family caregivers had never considered their preferences for hemodialysis, these percentage were lower for other types of life-sustaining treatment, ranging from CPR with 10% for patients and 14% for family caregivers, to chemotherapy with 22% for patients and 28% for family caregivers.
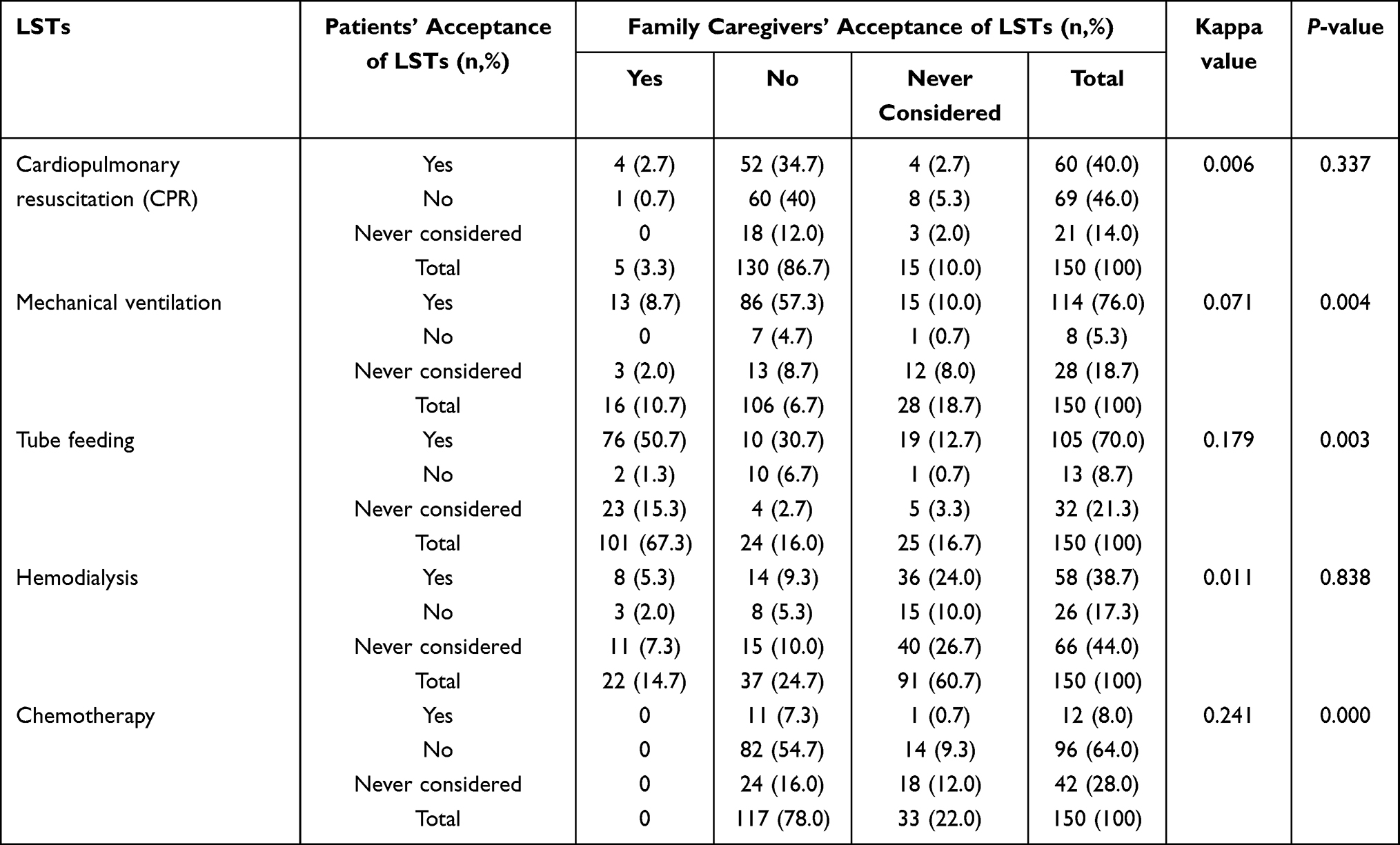 |
Table 2 The Agreement on Preferences of Life-Sustaining Treatments Between Patients and Family Caregivers When Patients Were Incapable of Making Medical Decisions |
The Attitudes of Patients and Their Family Caregivers Towards Life-Sustaining Treatment
Most patients and family caregivers preferred family members to make decisions for the patient when the patient would be incapable of making decisions (70% of patients and 48% of family caregivers, P=0.003), as shown in Table 3. Patients more often preferred to begin discussions about life-sustaining treatments when they were over 60 years old (32%) or in a healthy state (29%), and family caregivers more often preferred to begin discussions when curative treatment was no longer effective for the patient (44%) with P =0.051. Patients most frequently reported family burden (38%) or comfort (28%) as their most important consideration when making decisions about life-sustaining treatments, and family caregivers most frequently reported the patient’s state of consciousness (47%) or the patient’s comfort (38%) as the most important consideration with P =0.823.
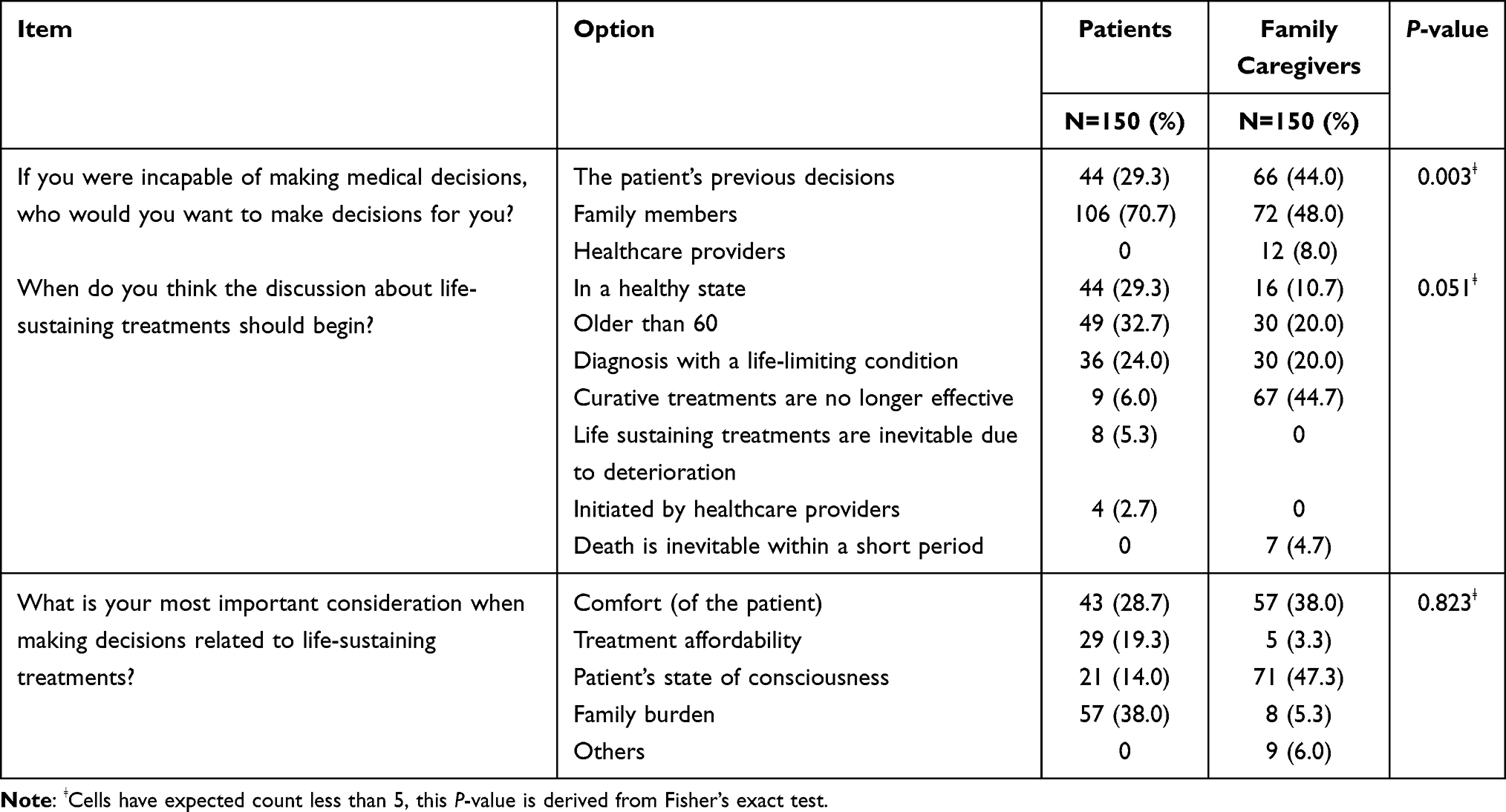 |
Table 3 The Difference in Preferences Related with Life-Sustaining Treatments Between Patients and Family Caregivers |
Discussion
In our study, patients and their family caregivers showed a slight to fair agreement in their preferences for life-sustaining treatments. For each of the life-sustaining treatments (cardiopulmonary resuscitation, mechanical ventilation, tube feeding, hemodialysis, chemotherapy), family caregivers more frequently than patients indicated that they would prefer that treatment for the patient in case the patient would be incapable of making medical decisions. More family caregivers than patients preferred that the patient makes their own decision about life-sustaining treatments. Patients more often preferred to begin discussions about life-sustaining treatments when they were over 60 years old or in a healthy state, and family caregivers more often preferred to begin discussions when curative treatment was no longer effective for the patient. The most important considerations when making decisions on life-sustaining treatments for most patients and family caregivers were family burden and patients’ comfort and state of consciousness.
Our study showed a slight to a fair agreement between patient and family caregiver preference for patients’ proposed life-sustaining treatments when the patient is incapable of making decisions. Family caregivers were more likely to prefer life-sustaining treatments for the patient than the patients themselves, which makes providing goal-concordant care for patients more difficult on the basis of a family-driven end-of-life care discussion process. A study on Taiwanese cancer patients suggests that patient-caregiver discrepancies were most likely when patients rejected all types of life-sustaining treatment but family caregivers preferred requesting more treatment for the patient.9 Studies showed that more than one-third of surrogates were unable to make decisions consistent with patients’ preferences for end-of-life care, the consistency was higher in situations involving the patient’s current health situations rather than responses to hypothetical scenarios.7,26,27 The uncertainty and complexity of the last months of a patient’s life complicate the surrogate’s prediction of the patient’s preferences.28,29 Fagerlin and Marks found that family surrogate decision-makers failed to represent patients’ wishes because they are likely to project their views onto what they think are the patients’ preferences.30,31 Family members might wish to maintain control and hope, and they may feel a sense of guilt and disappointment when treatment is withheld from the patient.32,33 In addition to this, familism and filial piety are widely discussed in Chinese end-of-life practices. Family members view partly or non-disclosure of bad news and making decisions on behalf of patients as their duties. Adult children are expected to pursue measures to prolong their parents’ life.34,35 This complicates advance care planning in terms of balancing the role of the family with meeting the patient’s wishes.
We found that 67% of patients and 70% of family caregivers preferred to receive tube feeding when patients are incapable of making medical decisions. Available evidence suggests that patients’ preferences for tube feeding vary according to their current and expected health status.36,37 Recent studies have provided evidence that Chinese nursing home residents who report better health status are more willing to receive tube feeding than those with greater health impairments.24 Similar results have been found for Chinese patients with advanced cancer.38 Studies of Taiwanese patients with cancer have shown that those who were not informed of their prognosis more often preferred to receive tube feeding.39,40 A survey of Japanese physicians showed that they were reluctant to withdraw patients’ tube feeding, because they considered it to be less invasive than other types of life-sustaining treatments.41 Chang et al42 found that seriously ill Taiwanese patients still retained tube feeding even after withdrawal of mechanical ventilation, they interpret providing food to patients as maintaining closeness and delivering family care, while forgoing tube feeding might be viewed as allowing patients to starve to death, which is incompatible with Chinese cultural norms.24,43
Nearly a third of the patients and more family caregivers in our study preferred patients to make their own decisions about life-sustaining treatments. Three systematic reviews showed that patients with cancer from western countries preferred a more active role in making medical decisions, whereas Asian patients preferred a more passive role.44–46 This can be explained by healthcare professionals’ tendency to exclude the patients from the conversation and the patient’s priority of family-based decision making, which are common aspects of serious illness conversations in Asia.6,47,48 Chinese patients prefer to be informed and engage in shared discussions with important ones and only a small number wanted to be in control of important medical decisions.49–51 Chinese patients’ preferences regarding the level of involvement in medical decision-making practices may vary at different stages. Our findings suggest that most family caregivers prefer to start discussing life-sustaining treatments only when the patient is seriously ill, because they do not want the patient to lose hope too early, in which case patients’ opportunities to participate in the decision-making process may be reduced by the late initiation. Even though most patients in this study preferred to begin the discussions of life-sustaining treatment at an earlier stage, they might rarely initiate such discussions for reasons such as preserving familial harmony.52
Implications
Our study highlights the importance of discussing preferences for future care in advance between patients and their family caregivers. Healthcare professionals should understand variations in patients’ preferences for the level of participating in serious illness decision-making. The participatory approach should also be adapted considering the individual’s preferences for information, discussion, and decision control in the medical decision-making process. More efforts should be made to develop culturally sensitive medical decision-making approaches for patients with a serious illness. In order to identify the right timing to initiate such conversations, it is necessary to assess the patient-family dynamics and their communication patterns. Emphasizing shared considerations and expectations for future care may be helpful in reaching an agreement between patients and family caregivers.
Strengths and Limitations
This study has several strengths. First, to capture the dynamics between patients and family caregivers regarding life-sustaining treatment, we purposefully enrolled them in dyads. Second, the consistency of data collection was sustained by one interviewer (TZ). Several limitations must be considered when interpreting the findings. Firstly, this study was conducted in a community setting, and most participants in our study reported good or excellent health, which limits its generalizability to other populations and settings. Secondly, unfortunately, we could not collect data about the number of people who refused to participate in the study nor their reasons.
Conclusion
Our findings indicate that patients and their family caregivers differ greatly in their preferences regarding the use of life-sustaining treatments for the patients on the basis of different motivations. Although the family was expected an important role in patients’ decision-making process, there were some patients and family caregivers who prefer that patients make their own medical decisions. This highlights the need to share an understanding of each other’s perspectives and considerations for future care, and to discuss the role of the family in serious illness conversation and decision-making. Healthcare professionals, especially geriatric doctors and nurses, should assess family dynamics and facilitate advance discussions between patients and families when possible to help them be prepared when decisions need to be made.
Funding
This study was funded by the China Scholarship Council (grand number 202007040013).
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Kuipers SJ, Cramm JM, Nieboer AP. The importance of patient-centered care and co-creation of care for satisfaction with care and physical and social well-being of patients with multi-morbidity in the primary care setting. BMC Health Serv Res. 2019;19(1):13. doi:10.1186/s12913-018-3818-y
2. Rietjens JAC, Sudore RL, Connolly M, et al. Definition and recommendations for advance care planning: an international consensus supported by the European Association for Palliative Care. Lancet Oncol. 2017;18(9):e543–e551. doi:10.1016/S1470-2045(17)30582-X
3. McMahan RD, Tellez I, Sudore RL. Deconstructing the complexities of advance care planning outcomes: what do we know and where do we go? A scoping review. J Am Geriatr Soc. 2021;69(1):234–244. doi:10.1111/jgs.16801
4. Hopp FP. Preferences for surrogate decision makers, informal communication, and advance directives among community-dwelling elders: results from a national study. Gerontologist. 2000;40(4):449–457. doi:10.1093/geront/40.4.449
5. Elwyn G, Durand MA, Song J, et al. A three-talk model for shared decision making: multistage consultation process. BMJ. 2017;359:j4891. doi:10.1136/bmj.j4891
6. Cheng SY, Lin CP, Chan HY, et al. Advance care planning in Asian culture. Jpn J Clin Oncol. 2020;50(9):976–989. doi:10.1093/jjco/hyaa131
7. Abdul-Razzak A, Heyland DK, Simon J, et al. Patient-family agreement on values and preferences for life-sustaining treatment: results of a multicentre observational study. BMJ Support Palliat Care. 2019;9(1):e20. doi:10.1136/bmjspcare-2016-001284
8. Chuang IF, Shyu YL, Weng LC, Huang HL. Consistency in end-of-life care preferences between hospitalized elderly patients and their primary family caregivers. Patient Prefer Adherence. 2020;14:2377–2387. doi:10.2147/PPA.S283923
9. Liu TW, Wen FH, Wang CH, et al. Terminally ill Taiwanese cancer patients’ and family caregivers’ agreement on patterns of life-sustaining treatment preferences is poor to fair and declines over a decade: results from two independent cross-sectional studies. J Pain Symptom Manage. 2017;54(1):35–45.e4. doi:10.1016/j.jpainsymman.2017.02.013
10. Tang ST, Liu TW, Wen FH, et al. A decade of changes in preferences for life-sustaining treatments among terminally ill patients with cancer. J Natl Compr Canc Netw. 2015;13(12):1510–1518. doi:10.6004/jnccn.2015.0179
11. Tang ST, Wen FH, Liu LN, et al. A decade of changes in family caregivers’ preferences for life-sustaining treatments for terminally ill cancer patients at end of life in the context of a Family-Oriented Society. J Pain Symptom Manage. 2016;51(5):907–915.e2. doi:10.1016/j.jpainsymman.2015.12.326
12. Hong M, Noh H, Kim K, Qualitative A. Exploration of end-of-life care planning with Korean Americans: awareness, attitudes, barriers, and preferences. J Hosp Palliat Nurs. 2022;24(5):E212–E218. doi:10.1097/NJH.0000000000000883
13. Liu Y, Yang J, Huo D, Fan H, Gao Y. Disclosure of cancer diagnosis in China: the incidence, patients’ situation, and different preferences between patients and their family members and related influence factors. Cancer Manag Res. 2018;10:2173–2181. doi:10.2147/CMAR.S166437
14. Liu L, Ma L, Chen Z, et al. Dignity at the end of life in traditional Chinese culture: perspectives of advanced cancer patients and family members. Eur J Oncol Nurs. 2021;54:102017. doi:10.1016/j.ejon.2021.102017
15. Fan R. The Confucian bioethics of surrogate decision making: its communitarian roots. Theor Med Bioeth. 2011;32(5):301–313. doi:10.1007/s11017-011-9191-z
16. Raposo VL. Lost in ‘Culturation’: medical informed consent in China (from a Western perspective). Med Health Care Philos. 2019;22(1):17–30. doi:10.1007/s11019-018-9835-0
17. Hamer LJ. Shenzhen becomes China’s First City to allow death with dignity. [Internet]. Available from: https://www.thatsmags.com/china/post/34697/shenzhen-becomes-china-s-first-city-to-allow-death-with-dignity.
18. Liao J, Wu B, Ni P, Mao J. Advance directive preferences among terminally ill older patients and its facilitators and barriers in China: a scoping review. J Am Med Dir Assoc. 2019;20(11):1356–1361.e2. doi:10.1016/j.jamda.2019.05.013
19. Kang L, Liu XH, Zhang J, et al. Attitudes toward advance directives among patients and their family members in China. J Am Med Dir Assoc. 2017;18(9):808.e7–808.e11. doi:10.1016/j.jamda.2017.05.014
20. Hwang H, Yang SJ, Jeong SY. Preferences of older inpatients and their family caregivers for life-sustaining treatments in South Korea. Geriatr Nurs. 2018;39(4):428–435. doi:10.1016/j.gerinurse.2017.12.015
21. Xu C, Yan S, Chee J, et al. Increasing the completion rate of the advance directives in primary care setting - a randomized controlled trial. BMC Fam Pract. 2021;22(1):115. doi:10.1186/s12875-021-01473-1
22. Inagaki A, Noguchi-Watanabe M, Sakka M, Yamamoto-Mitani N. Home-care nurses’ community involvement activities and preference regarding the place for end-of-life period among single older adults: a cross-sectional study in Japan. Health Soc Care Community. 2021;29(5):1584–1593. doi:10.1111/hsc.13224
23. Bennett FB, Hadidi NN, O’Conner-Von SK. End-of-life care communication in long-term care among nurses, residents, and families: a critical review of qualitative research. J Gerontol Nurs. 2021;47(7):43–49. doi:10.3928/00989134-20210604-03
24. Ni P, Ko E, Mao J. Preferences for feeding tube use and their determinants among cognitively intact nursing home residents in Wuhan, China: a cross-sectional study. J Transcult Nurs. 2020;31(1):13–21. doi:10.1177/1043659619832078
25. Borreani C, Brunelli C, Miccinesi G, et al. Eliciting individual preferences about death: development of the End-of-Life Preferences Interview. J Pain Symptom Manage. 2008;36(4):335–350. doi:10.1016/j.jpainsymman.2007.10.013
26. Shalowitz DI, Garrett-Mayer E, Wendler D. The accuracy of surrogate decision makers: a systematic review. Arch Intern Med. 2006;166(5):493–497. doi:10.1001/archinte.166.5.493
27. Hammami MM, Abuhdeeb K, Hammami MB, De padua SJS, Al-Balkhi A. Prediction of life-story narrative for end-of-life surrogate’s decision-making is inadequate: a Q-methodology study. BMC Med Ethics. 2019;20(1):28. doi:10.1186/s12910-019-0368-8
28. Khandelwal N, Curtis JR, Freedman VA, et al. How often is end-of-life care in the United States inconsistent with patients’ goals of care? J Palliat Med. 2017;20(12):1400–1404. doi:10.1089/jpm.2017.0065
29. Modes ME, Heckbert SR, Engelberg RA, Nielsen EL, Curtis JR, Kross EK. Patient-reported receipt of goal-concordant care among seriously ill outpatients-prevalence and associated factors. J Pain Symptom Manage. 2020;60(4):765–773. doi:10.1016/j.jpainsymman.2020.04.026
30. Marks MA, Arkes HR. Patient and surrogate disagreement in end-of-life decisions: can surrogates accurately predict patients’ preferences? Med Decis Making. 2008;28(4):524–531. doi:10.1177/0272989X08315244
31. Fagerlin A, Ditto PH, Danks JH, Houts RM, Smucker WD. Projection in surrogate decisions about life-sustaining medical treatments. Health Psychol. 2001;20(3):166–175. doi:10.1037/0278-6133.20.3.166
32. Wen FH, Chou WC, Chen JS, Chang WC, Hsieh CH, Tang ST. Evolution and predictors of patient-caregiver concordance on states of life-sustaining treatment preferences over terminally ill cancer patients’ last six months of life. J Palliat Med. 2019;22(1):25–33. doi:10.1089/jpm.2018.0307
33. Echarte LE, Bernacer J, Larrivee D, Oron JV, Grijalba-Uche M. Self-deception in terminal patients: belief system at stake. Front Psychol. 2016;7:117. doi:10.3389/fpsyg.2016.00117
34. Zivkovic T. About face: relationalities of ageing and dying in Chinese migrant families. Soc Sci Med. 2021;291:112827. doi:10.1016/j.socscimed.2020.112827
35. Lou C, Lou K, Ridley J. Exploring the meaning of dignity at end of life for Chinese Canadians caregivers: a qualitative cross-cultural study. Palliat Med. 2021;35(1):142–150. doi:10.1177/0269216320956809
36. Nakajima N. Difficulties in addressing artificial hydration and nutrition therapy for terminal cancer patients: what to do if patients/families’ wishes differ from the medically appropriate treatment plans? Am J Hosp Palliat Care. 2022;39(8):926–933. doi:10.1177/10499091211058029
37. Shinada K, Kohno T, Fukuda K, et al. Caregiver experience with decision-making difficulties in end-of-life care for patients with cardiovascular diseases. J Cardiol. 2022;79(4):537–544. doi:10.1016/j.jjcc.2021.11.001
38. Zhou W, Mao J, Wen Q, et al. Consistency in attitudes toward advance directive and life sustaining treatments between end-of-life cancer patients and their family members. Chin J Nurs. 2018;53(1):27–32.
39. Tang ST, Liu TW, Chow JM, et al. Associations between accurate prognostic understanding and end-of-life care preferences and its correlates among Taiwanese terminally ill cancer patients surveyed in 2011–2012. Psychooncology. 2014;23(7):780–787. doi:10.1002/pon.3482
40. Liu LN, Chen CH, Liu TW, et al. Preferences for Aggressive End-of-life Care and Their Determinants Among Taiwanese Terminally Ill Cancer Patients. Cancer Nurs. 2015;38(3):E9–E18. doi:10.1097/NCC.0000000000000155
41. Bito S, Asai A. Attitudes and behaviors of Japanese physicians concerning withholding and withdrawal of life-sustaining treatment for end-of-life patients: results from an Internet survey. BMC Med Ethics. 2007;8:7. doi:10.1186/1472-6939-8-7
42. Chang HT, Lin MH, Chen CK, et al. Aggressive end-of-life care and symptom relief treatments in terminally ill patients who had discussed withdrawal of mechanical ventilation: a hospital-based observational study. Am J Hosp Palliat Care. 2020;37(11):897–903. doi:10.1177/1049909120906612
43. Ngan OMY, Bergstresser SM, Sanip S, et al. Cultural considerations in forgoing enteral feeding: a comparison between the Hong Kong Chinese, North American, and Malaysian Islamic patients with advanced dementia at the end-of-life. Dev World Bioeth. 2020;20(2):105–114. doi:10.1111/dewb.12239
44. Noteboom EA, May AM, van der Wall E, de Wit NJ, Helsper CW. Patients’ preferred and perceived level of involvement in decision making for cancer treatment: a systematic review. Psychooncology. 2021;30(10):1663–1679. doi:10.1002/pon.5750
45. Tariman JD, Berry DL, Cochrane B, et al. Preferred and actual participation roles during health care decision making in persons with cancer: a systematic review. Ann Oncol. 2010;21(6):1145–1151. doi:10.1093/annonc/mdp534
46. Yılmaz NG, Schouten BC, Schinkel S, van Weert JCM. Information and participation preferences and needs of non-Western ethnic minority cancer patients and survivors: a systematic review of the literature. Patient Educ Couns. 2019;102(4):631–650. doi:10.1016/j.pec.2018.11.018
47. Martina D, Kustanti CY, Dewantari R, et al. Opportunities and challenges for advance care planning in strongly religious family-centric societies: a Focus group study of Indonesian cancer-care professionals. BMC Palliat Care. 2022;21(1):110. doi:10.1186/s12904-022-01002-6
48. Martina D, Geerse OP, Lin CP, et al. Asian patients’ perspectives on advance care planning: a mixed-method systematic review and conceptual framework. Palliat Med. 2021;35(10):1776–1792. doi:10.1177/02692163211042530
49. Wang Y, Zhang Y, Hong Y, et al. Advance directives and end-of-life care: knowledge and preferences of patients with brain Tumours from Anhui, China. BMC Cancer. 2021;21(1):25. doi:10.1186/s12885-020-07775-4
50. Yang Z, Hou B, Chen P, Zhang H. Preference and influencing factors of advance care planning for Chinese elderly patients with chronic diseases: a mixed-methods approach. J Hosp Palliat Nurs. 2021;23(2):178–186. doi:10.1097/NJH.0000000000000734
51. Xiao L, Peng M, Liu Y, Zhang L. Information, deliberation, and decisional control preferences for participation in medical decision-making and its influencing factors among Chinese cancer patients. Health Expect. 2021;24(5):1725–1736. doi:10.1111/hex.13312
52. Bowman KW, Singer PA. Chinese seniors’ perspectives on end-of-life decisions. Soc Sci Med. 2001;53(4):455–464. doi:10.1016/s0277-9536(00)00348-8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.