")
Back to Journals » Patient Preference and Adherence » Volume 16
Preference to Family Doctor Contracted Service of Patients with Chronic Disease in Urban China: A Discrete Choice Experiment
Authors Wang H, Sun H, Jin C, Wang M, Luo Y, Song W, Wang H
Received 19 April 2022
Accepted for publication 2 August 2022
Published 13 August 2022 Volume 2022:16 Pages 2103—2114
DOI https://doi.org/10.2147/PPA.S371188
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Naifeng Liu
Haode Wang,1 Hui Sun,1,2 Chunlin Jin,1 Meifeng Wang,1 Yashuang Luo,1 Wenqian Song,3 Haiyin Wang1
1Shanghai Health Development Research Center, Shanghai Medical Information Center, Shanghai, People’s Republic of China; 2Key Laboratory of Health Technology Assessment, National Health Commission; School of Public Health, Fudan University, Shanghai, People’s Republic of China; 3Shanghai Overseas Rescue and Aid Service Center, Shanghai, People’s Republic of China
Correspondence: Haiyin Wang, Shanghai Health Development Research Center, Minhang District, No. 181 Xinbei Road, Shanghai, 201199, People’s Republic of China, Tel +86- 18917769216, Email [email protected]
Objective: Shanghai is one of the pioneers proposing family doctor contract service (FDCS). However, there is no quantitative research focusing on the Shanghai experience from a demand-side perspective. This study investigated Shanghai chronic patients’ relative preferences for FDCS using a discrete choice experiment method.
Methods: A face-to-face discrete choice experiment (DCE) was performed to elicit the preference with 300 samples. Attributes and levels were extracted from the literature review and focus group consultation with patients. Seven attributes, follow-up frequency, medicine accessibility, family doctor competency, health management, referral convenience, appointment flexibility, and shared decision-making, were decided. Three levels were attached to each attribute. A mixed logit model was used to evaluate the multiple-choice data.
Results: A total of 248 patients completed the survey. Patient valued FDCS medicine accessibility (β=0.57, P < 0.05), and high family doctor competency (β= 0.43, P < 0.05), regular health management activities (β=0.36, P < 0.05), high follow-up frequency (β=0.31, P < 0.05) the most. The good doctor-patient shared decision-making atmosphere (β=0.12, P < 0.05), high referral convenience (β=0.06, P < 0.05) and high appointment flexibility (β=0.04, P < 0.05) are valued as less important. No significant preference heterogeneity was identified for patients with different sociodemographic characteristics. Respondents reported other FDCS needs, including online health consultation, specialist services in local institutes, higher reimbursement rates, free rehabilitation guidance for the disabled and personal health management.
Conclusion: This research is the first discrete choice experiment FDCS preference research targeting on Chinese urban population. The results suggested that to increase the quality of FDCS, policy-makers should prioritize follow-up frequency, medicine accessibility, family doctor competency and health management. The service package should consider a higher reimbursement rate and rehabilitation guidance for the disabled if extra health-care resources available. Future FDCS policy should consider stated societal preference and be congruent with it.
Keywords: primary care, family doctor contract services, urban resident preferences, discrete choice experiment
Introduction
Family doctor is the health “gatekeeper” of residents in the healthcare system and successfully manages most health problems.1,2 Community residents seek primary care services from their family doctor and the affiliated primary health-care institute, which is fundamental to the hierarchical medical system in China.3,4 While the definition of health-care professionals providing forefront primary care service varies among countries and provinces——for instance, the general practitioner (GP) in the UK National Health Service (NHS) system,5 we defined the family doctor as the physician and public physician providing national public health service and contracted or uncontracted service under primary care-tertiary hospitals two-way referral mechanism.6–8 The contract service is a voluntary bi-direction free health management supplementary service supported by the central government in China.5,9,10 The service has been regarded as a critical strategy to provide continuous primary care and improve health awareness of the vulnerable populations, such as senior citizens, pregnant women and patients with non-communicate chronic diseases.11
Many empirical studies have reported the positive feedback on contract service with cross-sectional data, especially for chronic disease patients.4,10,12–14 Compared with other types of regular primary care and regular primary care doctors, family doctor contract service (FDCS) improved the health outcome of community residents, and households reported to receive follow-up on treatments more efficiently.14 It was also proved to be a cost-effective intervention for chronic disease patients. A prospective survey indicated that all contracted patients (80.79%) implemented family doctors were important for non-communicable disease management.15 As China’s healthcare security system is facing heavy financial barriers caused by the rapidly surging chronic disease morbidity rate,16,17 FDCS can provide a less costly alternative.
Shanghai launched the FDCS program in 2011, and over eight million citizens have been covered for now.18 The Shanghai Health Commission issued notice on further implementation of contract services for family doctors in 2017 to increase the coverage of this service.19 Between 2011 and 2021, the percentage of chronic disease patients (hypertension and diabetic patients) coverage increased from around 50% to 84%.20 However, the ratio of using FDCS service out of the total number of signed residents remained low.3,20 A cross-sectional survey in Changning district, Shanghai, indicated that the contracted service outperformed typical family doctors in the perspective of visiting behavior, but the rate was still lower than 30%.21 Yao et al reviewed the remaining barriers to the FDCS service that may result in a lower utilization rate,22 and from a supply-side perspective, one-third of all studies mentioned low participation willingness.23 The knowledge of the patients’ preferences could assist the policy-makers, and local health service providers, in optimizing the FDCS service to be more responsive to patient demand. The DCE method was increasingly used to elicit preference to address health policy-making and healthcare resource allocation concerns.24 For instance, it was used to determine the value of aspects of rheumatoid arthritis intervention25 and measure the relative preference for family doctor service in rural China.5 Unfortunately, no preference research focuses on the urban chronic patient cohort published.
This study intends to remedy this research gap by evaluating the stated preference of non-communicable chronic disease patients in Shanghai. Unlike retrospective studies eliciting revealed preference from behaviors, this prospective study would elicit stated preference from statements indicating a quantitative relationship between aspects of FDCS service.26 While the survey-based technique describes what patients expect to happen in the future, hypothetical states are presented as alternative options.
The discrete choice experiment (DCE) is a frequently used technique to elicit preference by comparing two or more alternative scenarios. The method is based on Lancaster’s theory, in which the consumer utility is determined by the characteristics (attributes) and specifications (attributes levels) of each consumed objective.27 The individual’s choice of paired or triplet scenarios indicated their preference on each attribute and level, assuming that the respondent considers all the information simultaneously. Another DCE theoretical foundation is the random utility theory (RUT), in which the individual behaves in a probabilistic way: the utility function consists of the explicit (systematic part) and the implicit (random part).28 This study seeks to explore the patient preference for each identified factor by using the DCE method. The study results would provide evidence for optimizing the contracted services and adjusting service packages specially designed for non-communicable chronic disease patients in Shanghai.
Methods
Generate Attributes and Levels
Systematic literature reviews informed the attribute and level selection of the published literature and qualitative works. A recently published literature review in the English language and a meta-analysis identified attributes highly related to this study.23,29 However, there was no published systematic review that considered preference articles published in the Chinese language. The literature review conducted by the research team synthesized the attribute and levels of information regarding the family doctor preference research in Chinese languages and updated the English review. The attribute information from the literature review shared the equal weight and merged if attributes overlapped.
Phase I and II were focus group consultations with general public samples (n = 20) and eight interviews with other stakeholders, including city or district Health Commission members, health-care professionals and independent think tank researchers. Each focus group consultation was organized in the Songjiang district with four chronic patients who signed the FDCS contract and two primary care patients. They were encouraged to share their opinions on:
- how did they use the FDCS or family doctor service,
- the factors that may influence them in selecting a family doctor or signing the FDCS,
- satisfaction with the local family doctor service, and
- other recommendations for this policy.
Following the semi-structured questions, they would be presented with 10 attributes elicited from the literature reviews,23 with a detailed explanation on each attribute. The respondents ranked the attributes from the most important to the least relevant. All the data were analyzed with thematic method.
Eight interviews with stakeholders reviewed the focus group outcome and decreased the attribute from 10 to 7: follow-up frequency, medicine accessibility, family doctor competency, health management, referral convenience, appointment flexibility, and shared decision-making. Levels were assigned to each of the seven attributes according to stakeholder suggestions and review evidence. Each attribute had three levels to reflect the key characteristics. Each attribute’s descriptions are as follows, and Figure 1 provides the details.
- Follow-up frequency: the follow-up frequency indicated the average number of visits of family doctors for their contracted chronic disease patients. The local health-care professionals specified the levels: 4 times per month as high frequency, 2 times per month as medium frequency and one time per month as merely meeting the requirement.
- Medicine accessibility: Pharmaceutical service was a critical part of FDCS service, which referred to the availability of necessary chronic disease medicine or the difficulty with getting the required prescription. The attribute reflected the extent of fundamental pharmaceutical needs was satisfied. A three-level specification, fully satisfied, satisfied and not satisfied at all, was assigned.
- Family doctor competency: the family doctor competency indicated physicians’ skills and professional title, which was closely related to patient confidence with FDCS.15 A family doctor with high credentials and a well-renowned professional title will boost the willingness for service use. The attribute levels are: low, medium and high.4) Referral convenience: this attribute measured the satisfaction of the need for utilizing referrals to specialists. The attribute levels are: low, medium and high.
- Health management: the health management service was intended to deal with multiple challenges: polypharmacy, multiple chronic disease conditions, mental health problems, harmful lifestyle and compulsory informal care. Models for the FDCS health management were not well established in Shanghai. However, the normal activities included frequent checkups, health recording and health promotion. There are three frequency levels for this attribute: 6 times per month (regular), four times per month (medium), and one time per month (seldom).
- Appointment flexibility: Hole (2008) defined appointment flexibility as the choice of appointment times offered.30 The increase in appointment flexibility would lower the opportunity cost for patients with an increasing health budget. The levels are high (lots of alternative appointment times), medium (some alternative appointment times), and low (assigned appointment time).
- Shared decision-making: this attribute was frequently used, and it could be defined as the doctor involved patients in decisions about chronic disease treatments and pharmacist prescriptions. The assigned levels were well involved, appeared to be involved and were not involved (Table 1).
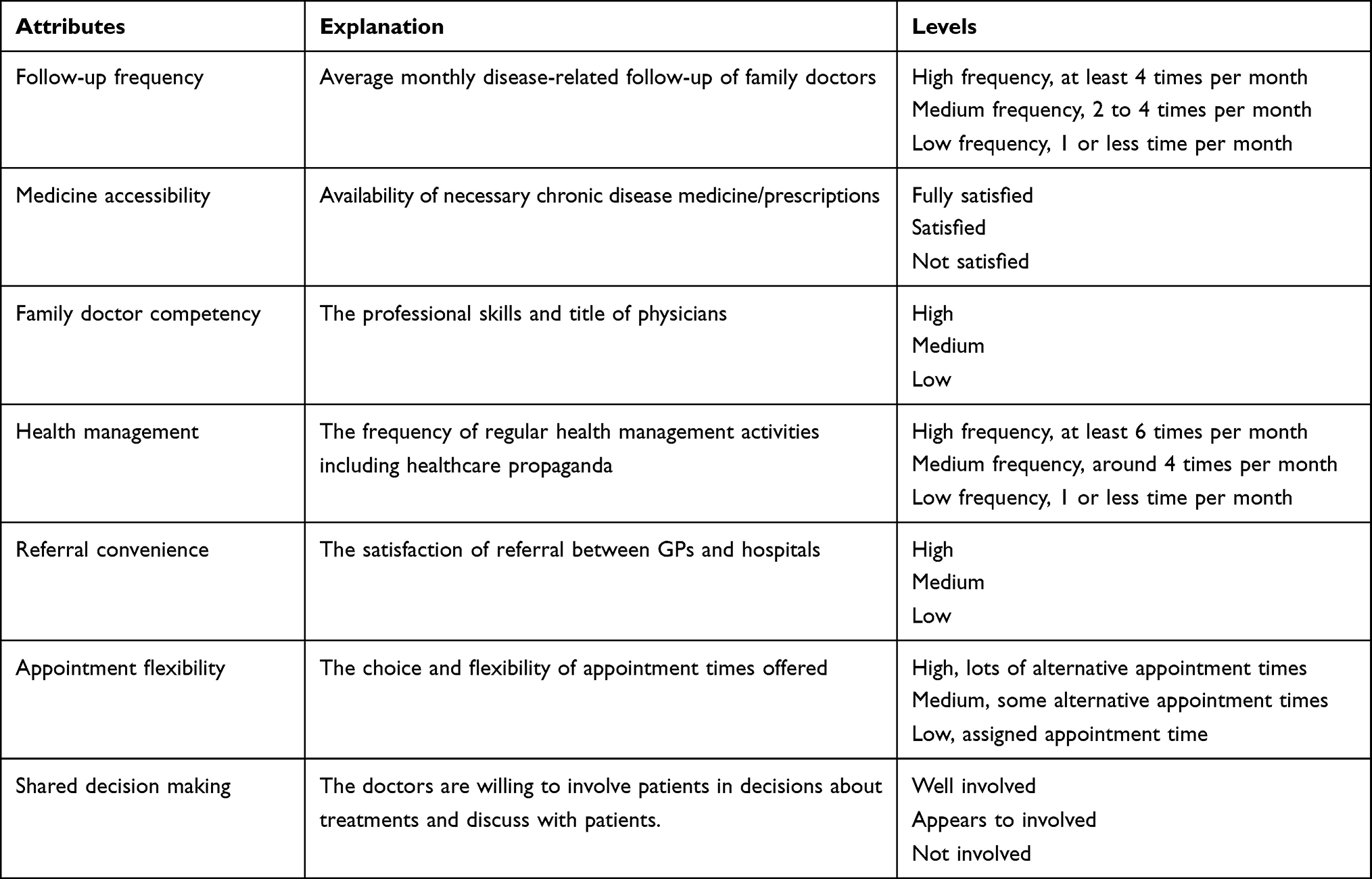 |
Table 1 Discrete Choice Attribute, Explanation and Levels |
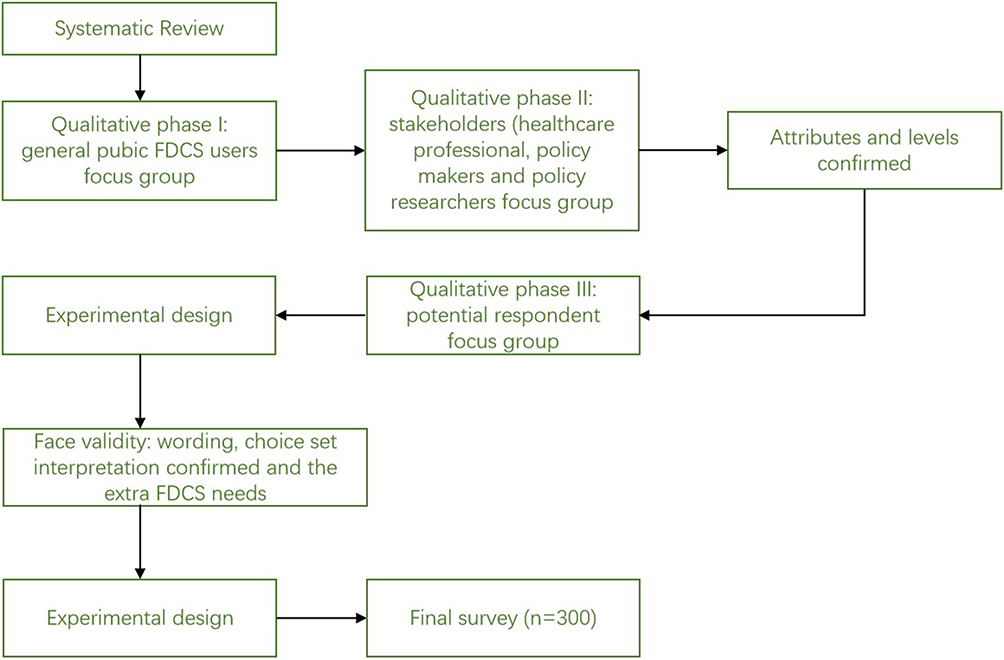 |
Figure 1 Development of the DCE survey. Note: The literature review is conducted with Chinese and English key words separately. |
Phase III validated each item’s wording and tested the public understanding of the multiple-choice tasks using face-to-face interviews. The consultation with five patients provided supplementary information for further refinement of the description of each attribute. Although the level for some attributes was abstract and published articles expressed the same meaning with controversial expressions, respondents interpreted the levels correctly.
Study Design
The experimental design and choice data analysis were simultaneously considered, with a consideration to identify functional forms of interest while minimizing the number of choice sets and avoiding any implausible scenarios. A fractional factor analysis method decreases the 2187 (37) hypothetical scenarios to a reasonable number. An efficient main effect design was applied, and the design was conducted with the software Ngene. The efficient design followed recommended health economics DCE best practice guidelines considering the two-way interactions between attributes.31,32 Although the utility-neutral optimal design was not competitive with Bayesian optimal designs,33 it was proved that fixed prior value performed as well as probabilistic priors and may generate a more efficient design if the attribute value distribution remained unknown. All comparisons containing a dominant scenario, ie, a hypothetical scenario with all attributes better than the comparator, were excluded. All of the attributes were effects coded.34 Eighteen choice sets were generated, and a pre-test (with ten respondents) was conducted to confirm the understandability and validity (Table 2).
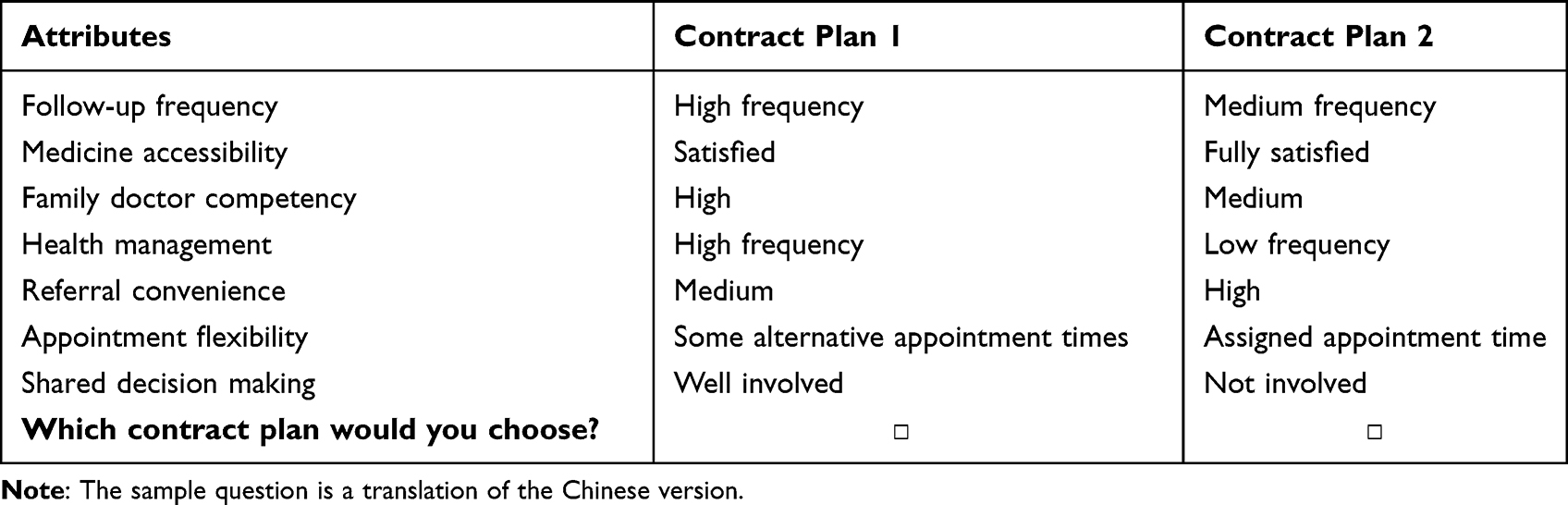 |
Table 2 An Example of a DCE Question. Imagine There are Two Alternative Contract Plans for You to Select, Please Choose the One You Prefer |
Data Collection
The DCE survey was conducted through a face-to-face interview in Shanghai with chronic disease patient samples from Songjiang district, Huangpu district and Pudong district. Random sampling was employed to choose samples from the local FDCS patient list. This research employed empirical evidence and theoretical formula to calculate the sample size.5,35 Enumerators surveyed 300 samples in 2019. One reminder, together with the consent, was presented before the formal data collection to ensure each respondent clearly understood the research target and data protection policy. Then, two warm-up paired comparison questions were introduced first to check if the respondents had the cognitive ability to complete the DCE task. The formal questionnaire contained 18 choice tasks plus a set of socio-demographic questions. The enumerator and the researcher double-checked all questionnaires. Any questionnaire with a respondent time less than 30 minutes, over one-third of all the questions skipped, selected the same answer (eg, select A for all the paired comparisons), and selected randomly without judgement would be dropped. Enumerators would pay members in vouchers (50 Yuan) for their contribution.
Data Analysis
The analysis of ordinal data is based on choice-based statistical models to generate relative coefficients of attribute levels, and the relative significance can be interpreted as a relative preference for each attribute level.32  represents the latent utility value, which is a linear additive function of the attribute levels (
represents the latent utility value, which is a linear additive function of the attribute levels ( and the error term
and the error term .
.

In the health sector, reviews found that ordinal data (especially discrete choice data) were commonly analyzed by Multinomial Logit (MNL) models and mixed logit models.36,37 MNL model is a homogeneous model assuming independence of irrelevant alternatives (IIA), and error terms are independent and identically distributed.38 The mixed logit model relaxed the homogeneity assumption by allowing the parameter to be random with imposed distributions.38 This research employed the heterogeneity model as the respondents had various chronic disease types and sociodemographic characteristics. All attributes were coded as dummy variables. The coefficients of each attribute level indicated the utility level of each variable. Because FDCS was a free service, there was no willingness to pay information, and the relative importance implies no monetary preference. All analyses were performed in Stata statistical software (version 14 SE, Stata Corp).
Results
Study Participants
A total of 248 participants completed the survey questionnaire after excluding 52 participants who failed to satisfy the criteria. The sample characteristics are reported in Table 3. Among the quantified respondents, approximately 42% (n = 105) were male, with a mean age of 58.3. The majority of them received high school or above education (77%, n = 166), and the self-reported monthly household income ranged from less than 3000 (n = 27) to over 10,000 (n = 10) RMB. The reported chronic diseases numbers were: hypertension (n = 213), coronary disease (n = 82), apoplexy (n = 50), diabetes (n = 139) and hyperlipemia (n = 149). Over half of all FDCS served patients had two or more chronic diseases.
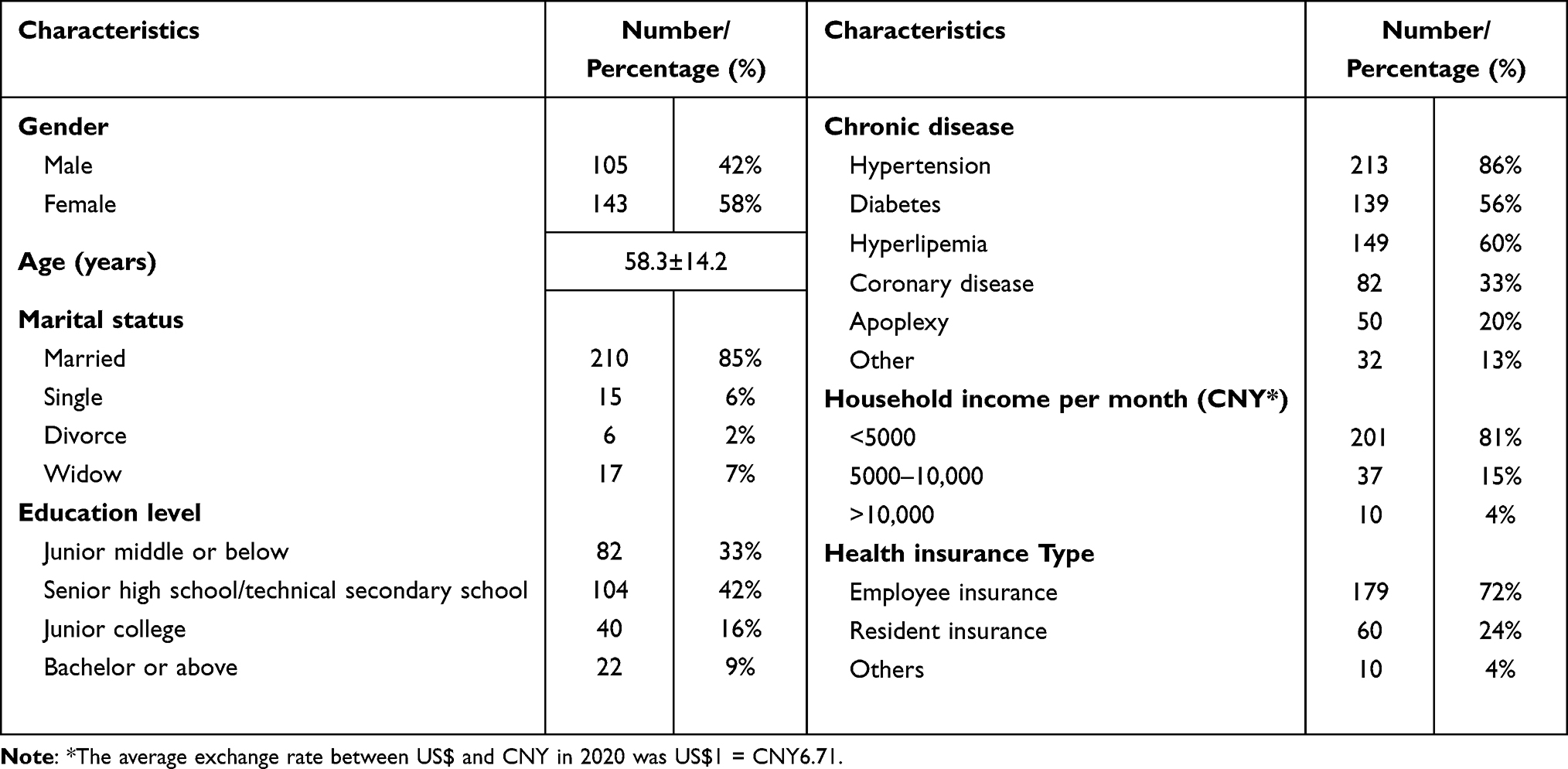 |
Table 3 Demographic Characteristics of Samples |
Model Estimation
The concept of relative preference intensity was used for comparing the degree of attribute preference. Fraquehar (1989) introduced the concept and noted that it simplified the utility analysis in decision problems.39,40 Results are illustrated in Figure 2, with 10 representing the most preferred attributes and 0 representing the least preferred. The vertical bars around each level mean estimate denoted the 95% confidence interval about the point estimation. The DCE with chronic patients revealed that the preferences intensity for follow-up frequency (5.3± 1.3), medicine accessibility (10.0 ± 2.0), family doctor competency (6.0 ± 1.1), health management (5.1± 0.9) were above 5, which indicated a relatively high preference. The preferences intensity for referral convenience, appointment flexibility, and shared decision-making was lower than 2.5.
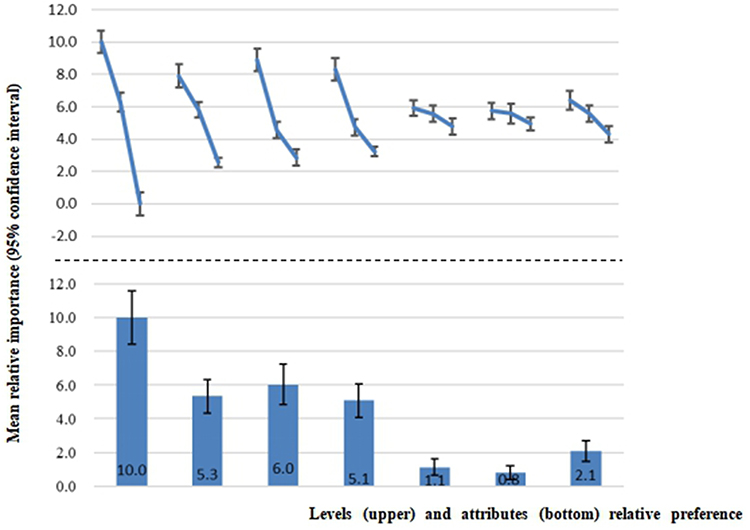 |
Figure 2 Relative preference intensity of each attribute. Notes: From left to right: medicine accessibility, follow-up frequency, family doctor competency, health management, referral convenience, appointment flexibility, shared decision-making. Upper figure showed the relative preference of each level and the bottom figure showed the relative preference of the attribute in general. |
The main effects of mixed logit model results are displayed in Table 4. All attribute levels had significant coefficients (indicating the attribute levels significantly influenced the decision-making process). The result had an expected sign (a worse level had a relatively minor coefficient), indicating the results were logically consistent.
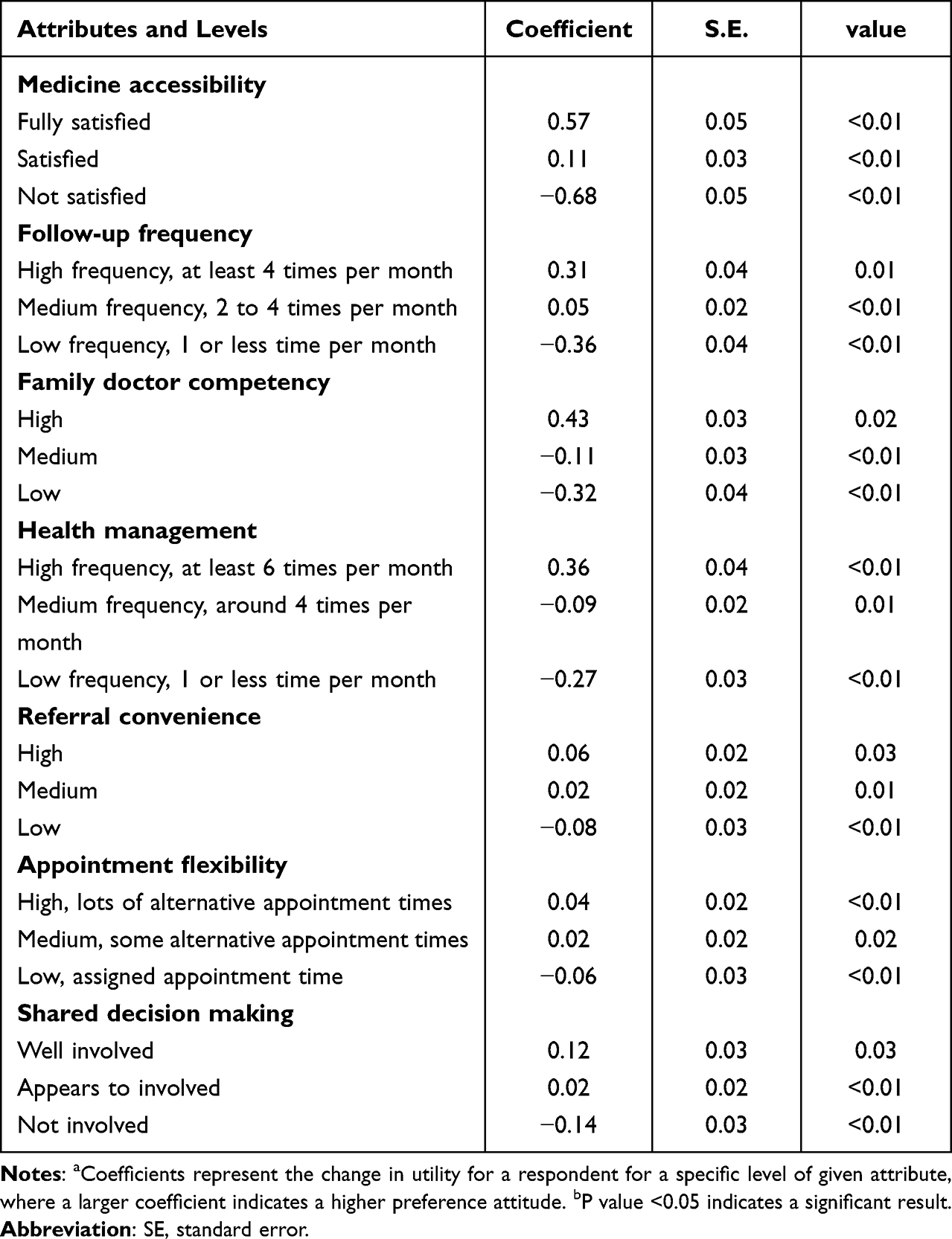 |
Table 4 Main Effects Model Estimation Logit Model Results |
Within the scenarios, the highest level of medicine accessibility (coefficient, 0.57 [Standard error (SE), 0.05]), followed by family doctor competency (coefficient, 0.43 [Standard error (SE), 0.03]) and health management (coefficient, 0.36 [Standard error (SE), 0.04]), were the main drivers of respondent choice. Replicating the scenarios but varying follow-up frequency, health management and appointment flexibility weights increased greater than level change: although the times are doubled for each upper level (eg, the follow-up frequency changed from 1 time to 2 times, and from 2 times to 4 times respectively), the increment in weights from the lowest level to medium level was much larger than the increments from medium level to the highest level. The most significant marginal increase was from fully satisfied medicine accessibility to satisfied medicine accessibility—all of the results consistent with the economic diminishing marginal utility theory.
The standard deviation (SD) results suggested no significant preference heterogeneity existed among the Shanghai chronic disease patients. Preference heterogeneity existed if the confidence intervals (CI) crossed 0. However, the result did show that the CI of attributes referral convenience (medium level) and appointment flexibility (medium level) contained 0. Preference heterogeneity risk still exists, and methodology research proved mixed logit model provided more convincing under this circumstance.38
Discussion
The Chinese government has fundamentally changed the family doctor and regarded family doctor as a solution to provide rudimentary and accessible primary care in low-resourcing settings in recent years.2,41 Compared with family doctors in other western countries, a family doctor in China was not an independent general practitioner. On the contrary, the national healthcare commission (NHC) introduced the primary target of the family doctor was providing public health services and health management consultations for vulnerable groups, including senior citizens, young children, pregnant women, disabled people and chronic disease patients.18 To strengthen the link between family doctors and patients, NHC proposed a new five-year plan on establishing a contracted family doctor service system around the country in 2016 and targeted full coverage in 2020.42 The reformation emphasized that FDCS referred patients had higher reimbursement rates in hospitals. However, with the ageing population and prevalence of chronic disease, the FDCS system should be as strong as the patients and government expected. Shanghai was the first city to raise and implement the FDCS primary care reformation to promote the efficiency of scarce health resource allocation and enhance the family doctor’s “health gatekeeper” role. To further optimise the policy and achieve the full-coverage goal, studying incentives that appeal to residents to sign with the family doctors would be significant.9,21
This DCE research, targeting urban chronic disease patients, provided quantitative insight into family doctor preference. This study relied on data from a discrete choice experiment survey with chronic patients from Shanghai to investigate the patient preference for the FDCS. A comprehensive literature review on Chinese and English family doctor preference research was conducted to identify the potential attributes, and the result was presented to help focus group consultees and interviewed stakeholders on deciding DCE attributes and levels. A fractional factorial design method was applied, and a DCE survey was conducted in Songjiang, Shanghai. Building on the multiple-choice data of which the respondents lived in an urban area, the analysis reflected the general preference of urban chronic patients.
Some findings stemmed from the analysis: firstly, patients highly valued medicine accessibility, family doctor competency, health management and follow-up frequency. This finding was consistent with the role of family doctors and primary care in Shanghai, where pharmaceutical service was the most important need for patients with a chronic condition, requiring long-term medication. However, the family doctor prescription should in-line with the national essential drugs list.43 This regulation prevented a large proportion of mobility-impaired patients and financially less well-off patients from accessing high-quality medicine conveniently and inexpensively.44 From the perspective of doctor competency, a published preference study targeting rural FDCS users, where experienced health-care provider was limited, indicated a high preference for the quality of family doctor.5,15 This study finding suggested that even for the urban area, lacking qualified family doctors was still one of the top concerns of FDCS users. The conclusion was supported by a multi-center survey where the respondents regarded the levels of skills as the main reason that they refused to visit primary care institutions.6 The comprehensive and considerable health management service was one of the well-renowned characteristics of Shanghai family doctor service since 1994,45 when Shanghai tertiary hospitals launched the “serve patients in their community” campaign.18 Shanghai Healthcare Commission required all the family doctors to plan health management and face-to-face follow-up with the vulnerable contracted residents every month. After 10 years of effort, the high preference for health management and follow-up frequency indicated that participants gradually realized the advantages of community health management. Besides, real-world evidence also proved the achievements.4,14 A retrospective effect analysis proved that management of the hypertension cohort increased the blood pressure control rate by 15.6%.46
Second, we found that the patients valued less on referral convenience, appointment flexibility and shared decision-making. Referral convenience and appointment flexibility were results of the density of primary care institutes and hospitals. Zhang et al analyzed the China Health and Retirement Longitudinal Survey (CHARLS) data-set to investigate the preference factors of the aged population and discovered density of hospitals was significantly associated with lower primary care use.3 We found heterogeneous preference with chronic disease patients that density of hospitals was an insignificant factor. The first reason could be that for chronic disease patients, although secondary and tertiary hospitals commanded well-trained doctor resources, the need for high drug availability was superior to institution density. Another reason was that Shanghai had the richest medical resources in China and the resources47 constraints might be less considered. The patient-centered care preference attribute, shared decision-making, achieved a similar result as UK primary care discrete choice research,48 where patients were less preferred this factor. However, we suspected that respondents might not fully understand the importance of shared decision-making and heuristically interpreted it as a family doctor’s attitude, where the “share” factor had been neglected.
Thirdly, apart from the attributes, participants reported other FDCS requirements, including online health consultation, specialist services in local institutes, higher reimbursement rates, free rehabilitation guidance for the disabled and personal health management. We suggested that policy-makers consider the extended health service with the DCE modelling results. For instance, the online health consultation and specialist services in local institutes reflected concerns with referral mechanism and could be achieved in a low-resource setting if a medical alliance among primary care institutes and the local secondary hospital could be established. Higher reimbursement rates and rehabilitation guidance requirements for the disabled indicated that poor residents still had a financial burden for using the FDCS service. Higher reimbursement rates for necessary chronic disease medicine and free fundamental rehabilitation therapy would break the pro-rich inequity.
Limitations
Although the research processes were well-designed, there were still several limitations: given the nature of the survey participants, the research result might have low external validity for patients living in other cities in China. Although Shanghai has over 30 million residents and the sample size was representative enough, it was notable that the GDP per capita in Shanghai was significantly higher than in other provinces.49 Another limitation was the participant’s understanding of attribute and DCE tasks. Although the qualitative consultations confirmed the validity of our study design, the majority of our respondents were senior residents and they may have lower cognitive ability to consider all the information together. Future research with analysis of patients living in other cities could give further insight into patient preferences.
Conclusion
This innovative study examined the relative preference of non-communicative chronic disease patients for FDCS. The modelling result indicated that medicine accessibility, family doctor competency, health management and follow-up frequency were the top factors determining patient preference, while referral convenience, appointment flexibility and shared decision-making were less important. Recently, a more evidence-based approach to allocating public health resources has been recommended.50 Policy-makers should provide the right incentives for chronic patients and allocate extra health resources as the patients expect. This research provided quantitative evidence to assist FDCS policy making. This research recommends conducting further DCE preference research with samples from other provinces to get a more comprehensive perspective on FDCS preference, t.
Ethics Approval and Consent to Participate
The Ethical Committee of the Shanghai Health Development and Research Center approved the study protocol. The writer and research team confirm that this research caused no harm (physical or mental) to any participants. The research process complies with the Declaration of Helsinki. The investigation was conducted after written informed consent was obtained from all participants.
Acknowledgments
Haode Wang and Hui Sun are first co-authors. Haiyin Wang and Hui Sun are the correspondent co-authors. The study was funded by Shanghai Health Development and Research Center and Shanghai Health Commission. We would like to thank all the staff involved in the field survey for their excellent research assistance.
Disclosure
The authors declare no conflict of interest.
References
1. Starfield B. Is primary care essential? Lancet. 1994;344(8930):1129–1133. doi:10.1016/S0140-6736(94)90634-3
2. Li X, Lu J, Hu S, et al. The primary health-care system in China. Lancet. 2017;390(10112):2584–2594. doi:10.1016/S0140-6736(17)33109-4
3. Zhang A, Nikoloski Z, Albala SA, et al. Patient choice of health care providers in China: primary care facilities versus hospitals. Health Syst Reform. 2020;6(1):e1846844. doi:10.1080/23288604.2020.1846844
4. Zhou Z, Zhao Y, Shen C, et al. Evaluating the effect of hierarchical medical system on health seeking behavior: a difference-in-differences analysis in China. Soc Sci Med. 2021;268:113372. doi:10.1016/j.socscimed.2020.113372
5. Fu P, Wang Y, Liu S, et al. Analysing the preferences for family doctor contract services in rural China: a study using a discrete choice experiment. BMC Fam Pract. 2020;21(1):148. doi:10.1186/s12875-020-01223-9
6. Shang X, Huang Y, Li B, et al. Residents’ awareness of family doctor contract services, status of contract with a family doctor, and contract service needs in Zhejiang Province, China: a cross-sectional study. Int J Environ Res Public Health. 2019;16(18):3312. doi:10.3390/ijerph16183312
7. Yin—ying Y, Wang F, Li X, Jia M, Tian M. A systematic review of the current status of contracting services for family doctors in China. Chin Healthcare Manag. 2019;36(03):
8. Xia-Sun C, Liu T, Jiang F, Si S, Chu S, Wang P. The development process and implementation of policies related to family doctor in China. Chin Gen Pract. 2021;24(07):765–774.
9. Liu S, Liu Y, Zhang T, et al. The developing family doctor system: evidence from the progress of the family doctor signing service from a longitudinal survey (2013–2016) in Pudong new area. Shanghai BMC Fam Pract. 2021;22(1):11. doi:10.1186/s12875-020-01353-0
10. Li Z, Li J, Fu P, et al. Family doctor contract services and health-related quality of life among patients with chronic diseases in rural China: what is the role of socioeconomic status? Int J Equity Health. 2021;20(1):191. doi:10.1186/s12939-021-01530-2
11. Office, N.M.R. Notice on promoting guidance for family doctor contract services; 2016. Available from: http://www.mohrss.gov.cn/SYrlzyhshbzb/shehuibaozhang/zcwj/yiliao/201606/t20160615241854.html.
12. Lam CL, Yu EYT, Lo YYC, et al. Having a family doctor is associated with some better patient-reported outcomes of primary care consultations. Front Med. 2014;1:29. doi:10.3389/fmed.2014.00029
13. Zheng Q, Shi L, Pang T, et al. Utilization of community health care centers and family doctor contracts services among community residents: a community-based analysis in Shenzhen, China. BMC Fam Pract. 2021;22(1):100. doi:10.1186/s12875-021-01444-6
14. Feng S, Cheng A, Luo Z, et al. Effect of family doctor contract services on patient perceived quality of primary care in southern China. BMC Fam Pract. 2020;21(1):218. doi:10.1186/s12875-020-01287-7
15. Li J, Li J, Fu P, et al. Willingness of patients with chronic disease in rural China to contract with family doctors: implication for targeting characteristics. BMC Fam Pract. 2021;22(1). doi:10.1186/s12875-021-01553-2
16. Xu T, Wang B, Liu H, et al. Prevalence and causes of vision loss in China from 1990 to 2019: findings from the global burden of disease study 2019. Lancet Public Health. 2020;5(12):e682–e691. doi:10.1016/S2468-2667(20)30254-1
17. Wang LM, Chen ZH, Zhang M, et al. 中国老年人群慢性病患病状况和疾病负担研究. [Study of the prevalence and disease burden of chronic disease in the elderly in China]. Zhonghua Liu Xing Bing Xue Za Zhi. 2019;40(3):277–283. Chinese. doi:10.3760/cma.j.issn.0254-6450.2019.03.005
18. Zhiying ZCC. analysis of the concept of family doctor from the history of family doctor-Take Shanghai as an example. Chin Commun Dr. 2019;35(10):
19. Shanghai, H.C.o. Notice on Further implementation and details of the primary healthcare service; 2017. (In Chinese); Available from: http://wsjkw.sh.gov.cn/zxghjh/20180815/0012-57264.html.
20. Hao L. Analysis of the intervention effect of family doctor contract service model in community high-risk groups of chronic diseases. Chin Commun Dr. 2019;35(15):173–174.
21. Huang J, Lu W, Wang L, et al. A preliminary effect analysis of family doctor and medical insurance payment coordination reform in Changning District of Shanghai, China. BMC Fam Pract. 2019;20(1):60. doi:10.1186/s12875-019-0949-0
22. Yao Z, Gao B, Xu W, Qi G, Lu X. Current status and need of collaborative health management of diabetes in community health service centers. Chin Gen Pract. 2019;22(11):1258.
23. Kleij K-S, Tangermann U, Amelung VE, et al. Patients’ preferences for primary health care – a systematic literature review of discrete choice experiments. BMC Health Serv Res. 2017;17(1). doi:10.1186/s12913-017-2433-7
24. Lancsar E, Louviere J. Conducting discrete choice experiments to inform healthcare decision making. PharmacoEconomics. 2008;26(8):661–677. doi:10.2165/00019053-200826080-00004
25. Harrison M, Marra C, Shojania K, et al. Societal preferences for rheumatoid arthritis treatments: evidence from a discrete choice experiment. Rheumatology. 2015;54(10):1816–1825. doi:10.1093/rheumatology/kev113
26. Ghijben P, Gu Y, Lancsar E, et al. Revealed and stated preferences of decision makers for priority setting in health technology assessment: a systematic review. Pharmacoeconomics. 2018;36(3):323–340. doi:10.1007/s40273-017-0586-1
27. Carson RT, Louviere JJ, Anderson DA, et al. Experimental analysis of choice. Mark Lett. 1994;5(4):351–367. doi:10.1007/BF00999210
28. Train KE. Discrete choice methods with simulation. Comput Math Appl. 2004;47(6–7):1148. doi:10.1016/S0898-1221(04)90100-9
29. Linlin JIA, CAO Xuefei ZY, Yanhong HOU. Residents’ willingness to renew family doctors contract services in China: a metaanalysis. Chin J Evid-Based Med. 2022;22(03):324–331.
30. Hole AR. Modelling heterogeneity in patients’ preferences for the attributes of a general practitioner appointment. J Health Econ. 2008;27(4):1078–1094. doi:10.1016/j.jhealeco.2007.11.006
31. Johnson FR, Lancsar E, Marshall D, et al. Constructing experimental designs for discrete-choice experiments: report of the ISPOR conjoint analysis experimental design good research practices task force. Value Health. 2013;16(1):3–13. doi:10.1016/j.jval.2012.08.2223
32. Lancsar E, Fiebig DG, Hole AR. Discrete choice experiments: a guide to model specification, estimation and software. Pharmacoeconomics. 2017;35(7):697–716. doi:10.1007/s40273-017-0506-4
33. Seeger M, Steinke F, Tsuda K. Bayesian inference and optimal design in the sparse linear model. In: Artificial Intelligence and Statistics. PMLR; 2007.
34. Bech M, Gyrd‐Hansen D. Effects coding in discrete choice experiments. Health Econ. 2005;14(10):1079–1083. doi:10.1002/hec.984
35. de Bekker-Grob EW, Donkers B, Jonker MF, et al. Sample size requirements for discrete-choice experiments in healthcare: a practical guide. Patient. 2015;8(5):373–384. doi:10.1007/s40271-015-0118-z
36. Clark M, Determann D, Petrou S, et al. Discrete choice experiments in health economics: a review of the literature. Pharmacoeconomics. 2014;32(9):883–902. doi:10.1007/s40273-014-0170-x
37. de Bekker-Grob EW, Ryan M, Gerard K. Discrete choice experiments in health economics: a review of the literature. Health Econ. 2012;21(2):145–172. doi:10.1002/hec.1697
38. Kjaer T, Gyrd-Hansen D. Preference heterogeneity and choice of cardiac rehabilitation program: results from a discrete choice experiment. Health Policy. 2007;85(1):124–132. doi:10.1016/j.healthpol.2007.07.002
39. Mirelman AMPH, Mentzakis E, Kinter E, et al. Decision-making criteria among national policymakers in five countries: a discrete choice experiment eliciting relative preferences for equity and efficiency. Value Health. 2012;15(3):534–539. doi:10.1016/j.jval.2012.04.001
40. Sun H, Wang H, Shi L, et al. Physician preferences for chemotherapy in the treatment of non-small cell lung cancer in China: evidence from multicentre discrete choice experiments. BMJ Open. 2020;10(2):e032336. doi:10.1136/bmjopen-2019-032336
41. China, T.C.P.s.G.o.t.P.s.R.o. Opinions on Deepening the Reform of the Medical and Health System; 2009. Available from: http://www.gov.cn/jrzg/2009-04/06/content_1278721.htm.
42. Office, N.M.R. Notice on promoting guidance for family doctor contract services, S.C.a.N.H. commission, editor; 2016: Available from: http://www.mohrss.gov.cn/SYrlzyhshbzb/shehuibaozhang/zcwj/yiliao/201606/t20160615_241854.html.
43. Tian X, Song Y, Zhang X. National Essential Medicines List and policy practice: a case study of China’s health care reform. BMC Health Serv Res. 2012;12:401. doi:10.1186/1472-6963-12-401
44. Wang Z, Chang R, Luo YB, et al. Evaluation of need and distribution of national essential medicines list in village clinics: a cross-sectional study based on the perspective of village doctors in China. Curr Med Sci. 2019;39(4):663–669. doi:10.1007/s11596-019-2089-0
45. Lei D, Kapur K, Joyce GF, Van Vorst KA. Preliminary analysis of health and expense“gatekeeper”of family doctor. Chin Prim Health Care. 2022;36(01):40–42.
46. Yang H, Huang X, Zhou Z, et al. Determinants of initial utilization of community healthcare services among patients with major non-communicable chronic diseases in South China. PLoS One. 2014;9(12):e116051. doi:10.1371/journal.pone.0116051
47. Li D, Zhou Z, Si Y, et al. Unequal distribution of health human resource in mainland China: what are the determinants from a comprehensive perspective? Int J Equity Health. 2018;17(1):29. doi:10.1186/s12939-018-0742-z
48. Cheraghi-Sohi S, Hole AR, Mead N, et al. What patients want from primary care consultations: a discrete choice experiment to identify patients’ priorities. Ann Fam Med. 2008;6(2):107–115. doi:10.1370/afm.816
49. Chen J, Lin Z, Li L-A, et al. Ten years of China’s new healthcare reform: a longitudinal study on changes in health resources. BMC Public Health. 2021;21(1):2272. doi:10.1186/s12889-021-12248-9
50. Brownson RC, Fielding JE, Maylahn CM. Evidence-based decision making to improve public health practice. Front Public Health. 2013;2(2):2.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.