")
Back to Journals » Open Access Journal of Contraception » Volume 14
Predictors of Unintended Pregnancy Among Adolescent Girls During the Second Wave of COVID-19 Pandemic in Oyam District in Northern Uganda
Authors Okalo P, Arach AA, Apili B, Oyat J, Halima N, Kabunga A
Received 8 December 2022
Accepted for publication 2 February 2023
Published 5 February 2023 Volume 2023:14 Pages 15—21
DOI https://doi.org/10.2147/OAJC.S399973
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Ponsiano Okalo,1 Anna Agnes Arach,2 Brenda Apili,1 Jimmy Oyat,1 Namata Halima,3 Amir Kabunga1
1Department of Psychiatry, Lira University, Lira City, Uganda; 2Department of Nursing and Midwifery, Lira University, Lira City, Uganda; 3Department of Mental Health, Makerere University, Kampala City, Uganda
Correspondence: Amir Kabunga, Department of Psychiatry, Lira University, P.O BOX, 1035, Lira City, Uganda, Tel +256777929576, Email [email protected]
Background: In Uganda, unintended pregnancies are responsible for one in three births with detrimental consequences, a situation that worsened during COVID-19. Thus, the present examined unplanned pregnancy and its associated risks in Oyam district, northern Uganda during the COVID-19 epidemic.
Methods and Methods: This study employed a cross-sectional study among adolescent girls aged 15– 19 years who had a pregnancy during the second phase of COVID-19 in Oyam district, northern Uganda in November 2022. A consecutive method was employed to recruit the participants attending health facilities. A structured questionnaire was utilized to collect data. For data analysis, both bivariate and multivariable regression methods with adjusted odds ratio and 95% CI were used. A p-value of 0.05 was used to determine the significance level.
Results: Of the total respondents, 292 (69.5%) were aged between 18 and 19 years of age, 295 (70.2%) lived in rural areas, and 222 (52.9%) had no formal education. The results also show that 293 (69.8%) of the respondents had unintended pregnancies during COVID-19. The results indicate that participants who lacked knowledge of the ovulation period (AOR: 0.242; 95% CI: 0156– 0376; P< 0.001), sex education during COVID-19 (AOR: 0.563; 95% CI:: 0.365– 0.869; P=0.024) and lacked the freedom to discuss family planning-related issues with family members during COVID-19 (AOR: 0.228; 95% CI: 0.138– 0.376; P< 0.001) were more likely to have an unintended pregnancy compared to their counterparts.
Conclusion: Our study shows that unwanted pregnancies among adolescent girls remain a public health issue in Oyam district with more than two-thirds of adolescents having unwanted pregnancies during the crisis of COVID-19. The major correlates of unwanted pregnancies among adolescent girls during COVID-19 pandemic were inadequate knowledge of the ovulation period, sex education, and lack of freedom to discuss family planning-related issues with family members. There is a need to prioritize interventions, especially in rural settings. Sex education to improve contraceptive use and delay sexual debut. In light of the possibility that social and cultural norms in the Oyam district prohibit parents and children from discussing sexual subjects, it is crucial to promote sexual health education through the mass media, including newspapers, television, radio, and social media.
Keywords: adolescents, COVID-19, crisis, unintended pregnancy
Background
The United Nations Children's Fund (UNICEF) defined teenage pregnancy as “a teenage girl, usually with the ages of 13–19, becoming pregnant and refers to girls who have not achieved legal maturity, which varies across the world.”1 Although some pregnancies and births may be desired, reports indicate that the approximately 50% are not and which result in an estimated 12 million birth.2 Some complications associated with teenage pregnancy include preterm birth, intrauterine growth retardation, and low birth weight.3 Early pregnancy puts a mother’s health and that of her unborn child at serious risk.4 Adolescents in the age group of 15–19 are two times more likely to die due to pregnancy and childbirth-related causes as opposed to older women.5 Also, children born to adolescent girls have a 50% likelihood of dying before the age of one compared to those born to mothers in their twenties.6
Between 2015 and 2019, there were over 121 million unplanned pregnancies worldwide, with 64 unwanted conceptions per 1000 women between the ages of 15 and 49 on average.7 These unwanted pregnancies predominately happen in the sub-Saharan Africa region.8 The COVID-19 pandemic worsened teenage girls’ vulnerability to unwanted pregnancies.9 COVID-19 limited women’s access to contraceptives and other sexual and reproductive health services.10 One in three women including adolescent girls either delayed or cancelled had trouble accessing sexual and reproductive health services.11 This must have increased the risks of unintended pregnancies among adolescent girls.12 Survey reports from six countries including Colombia, the Democratic Republic of Congo, Bangladesh, Syria, and Nigeria show that overall, there was a decline in access to family planning counselling and contraceptives.13 For instance, contraceptive access in Bangladesh was reduced to 50% and 35%, respectively. Similar observations were reported in Colombia, DRC, Nigeria, and Burkina Faso.13 Thus, limited access to SRH care services due to crises like COVID-19 was a predisposing factor for unintended pregnancies. In Uganda, unintended pregnancies are responsible for one in three births with detrimental consequences, a situation that worsened during COVID-19.14 The pandemic affected reproductive health and family planning.10
November through December 2020 was designated as Wave 1 of COVID-19, and April through June 2021 as Wave 2. While the first wave in Uganda was predominantly triggered by a combination of non-Delta variations, the second wave was primarily caused by the Delta variant.15 Government officials and experts have shown concern at the rising number of cases of teenage pregnancies in the East African country of Uganda during COVID-19.16 Statistics show that 354,736 adolescent pregnancies occurred in Uganda during the pandemic, which was a 55% increase from 354,736 to 551,235 teenage pregnancies in the first 6 months of 2021.9 Studies have shown that predictors of teenage pregnancy during COVID-19 included age, primary decision-maker for family planning services, non-use of contraceptives, and getting involved in the sex trade.8,9
The northern part of Uganda had the highest pregnancy rate in the country before COVID-19.17 However, the number increased during COVID with Oyam district registering the highest number of cases of teenage pregnancies.18 For instance, by the time the lockdown was lifted, one in every five households had a teenager with either a child or pregnancy.19 Therefore, it is essential to pay attention to the sexual and reproductive health rights of adolescent girls. There is a lot of literature on teenage pregnancy, but its scope is limited to the prevalence of adolescent pregnancy. There are, however, very limited studies published that report on the predictors of unwanted pregnancies in Uganda during the COVID-19 pandemic. Thus, the current study examined the predictors of unwanted pregnancies among adolescent girls during the COVID-19 pandemic in Oyam district of Uganda.
Methods and Methods
Study Settings
This study was carried out in maternity wards in Oyam district health facilities, in the northern part of Uganda. The districts of Gulu, Pader, Kole, Apac, Kiryandongo, and Nwoya border the district of Oyam from the north, the northeast, the south, and the southwest, respectively. Oyam district was selected for the study because it registered the greatest cases of adolescent pregnancies in the region.18
Study Design
We employed an institutional-cross-sectional study design with a sample of adolescent girls who became pregnant during the second wave of COVID-19 in Oyam district.
Sample Size and Sample Size Estimation
The population of the study included adolescent girls aged 14–19 years of age who became pregnant during wave two of COVID-19 and accessing maternal health services in Oyam district health facilities, in northern Uganda. To estimate the sample size, we used a single proportion formula. Z=1.96, n=estimated proportion of adolescent girls assumed to be 50% with 95%, a margin of error of 5%, and a non-response rate of 10%. Using this formula, the final sample size generated is 424.
Sampling Criteria
We use a consecutive sampling technique to select the participants who gave written consent. In the technique, participants meeting the inclusion criteria were selected for the study. Pregnant and postpartum adolescent girls aged 14–19 years who became pregnant in wave two of COVID-19 consented to and obtained permission from their parents/guardians to participate were included in the study. Participants who at the time of data collection were emotionally or psychologically unstable or had difficulty communicating or had cognitive impairment were excluded.
Data Collection Instruments
Data were collected with the help of interviewer-administered questionnaires. The items were adapted from the literature reviewed.20 The intended versus unintended pregnancy was assessed using a binary item with yes or no responses. The respondents were asked to tell whether the pregnancy was intended or not. Social-demographic information like the age of the respondents was collected. Based on previous studies,21 items on the risk (for example, did you use contraceptives when having sexual intercourse during COVID-19? Did you have any sexual education during COVID-19? Did you have counselling during COVID-19? Did you discuss matters related to pregnancy prevention with parents/guardians during COVID-19? Did you receive pregnancy-related information from health-care workers during COVID-19?) were adopted. The instrument was evaluated during the pre-test for clarity and reliability and based on pre-test results, the Cronbach’s alpha was 0.91.
Procedure
We conducted data collection for 3 weeks in November 2022. The nurses selected participants who attended the ante- and postnatal clinics and gave them a brief explanation of the study. We explained the inclusion and exclusion criteria to the nursing staff. The study’s goals and objectives, as well as research ethics, were covered in training for the six research assistants. The researcher welcomed the participants and provided them with a thorough explanation of the study’s objectives and ethical considerations. Within the antenatal and postnatal units, the interviews were done in discreet, secure settings. Before collecting data, the participants’ written informed consent was obtained.
Statistical Analysis
To conduct data analysis, SPSS statistics version 25.0 was used. Descriptive statistics including frequencies and percentages were used to summarise the participants’ characteristics. Bivariate analysis and crude odds ratio with 95% CI was used to determine the association between each independent and outcome variable. Variable with p≤0.05 in the bivariate analysis were included in the multivariate logistic model. The strength of the association between independent and outcome variables was assessed with the help of an adjusted odds ratio with 95% CI. A p-value was used to report the level of significance.
Ethical Approval and Consent to Participants
The current study followed the procedures recommended by the declaration of Helsinki. The study was cleared by the Gulu University Ethical committee (GUREC-2022-315). Further permission was obtained from the Oyam District Health officer. We also obtained written informed consent from the participants. The girls who needed psycho-social support were given counselling services as two of the investigators were counselling psychologists.
Results
Social-Demographic and Pregnancy-Related Information of the Respondents
A total of 420 adolescent girls were involved in the present study giving a response rate of 99.5% and data was analyzed, as shown in Table 1. The majority of respondents 292 (69.5%) were aged between 18 and 19 years of age, 237 (56.4%) were not married, 295 (70.2%) lived in rural areas, and 222 (52.9%) had no formal education. The results also indicate that 293 (69.8%) of the participants had unintended pregnancies during COVID-19. The univariate logistic analysis in Table 1 indicates that the factors associated with unintended pregnancy among the participants were age, knowledge of the ovulation period, having multiple partners during COVID-19, sex education, exposure to mass media family planning messages, discussing pregnancy-related issues with parents during COVID-19, knowledge about contraceptives and freedom to discuss family planning-related issues with family members during COVID-19.
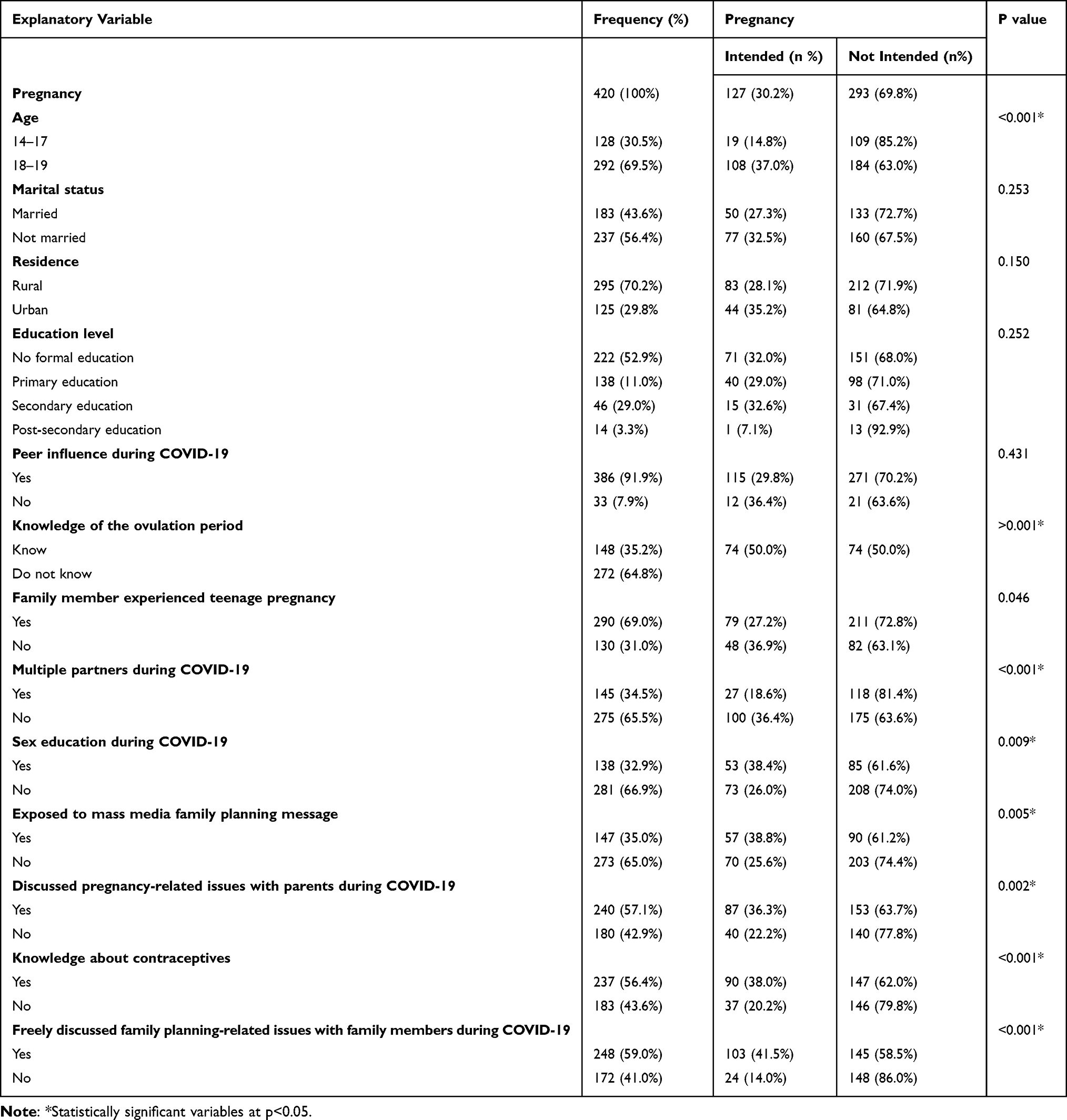 |
Table 1 Social-Demographic and Pregnancy-Related Information of Respondents |
A Multivariable Logistic Regression Analysis of Factors Associated with Unintended Pregnancy
Binary logistic regression results showed that participants who lacked knowledge of the ovulation period (AOR: 0.242; 95% CI: 0.156–0.376; P<0.001), sex education during COVID-19 (AOR: 0.563; 95% CI: 0.365–0.869; P=0.024) and lacked the freedom to discuss family planning-related issues with family members during COVID-19 (AOR: 0.228; 95% CI: 0.138–0.376; P<0.001) had greater odds of having unintended pregnancy (Table 2).
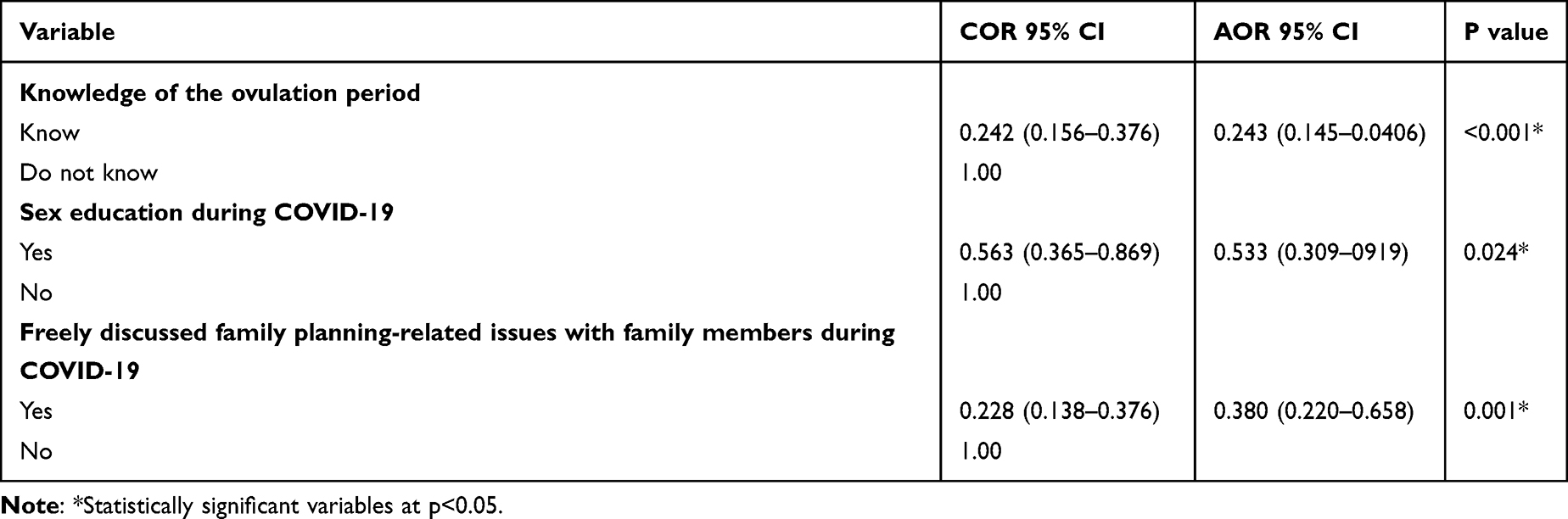 |
Table 2 A Multivariable Logistic Regression Analysis of Factors Associated with Unintended Pregnancy |
Discussion
The study assessed unintended pregnancy and its predictors among adolescent girls during the COVID-19 crisis in Oyam district, northern Uganda. Our findings showed that 293 (69.8%) of the respondents had unintended pregnancies. The factors independently associated with unintended pregnancy were inadequate knowledge of the ovulation period, sex education during COVID-19, and lack of freedom to discuss family planning-related issues with family members during COVID-19. Before COVID-19, the proportion of unwanted in Africa was 10–54%.22 Our findings tend to suggest that COVID-19 has a strong influence on unintended pregnancies among adolescent girls. This observation has been reported in other surveys.10 The pandemic has affected reproductive health and family planning.10 COVID-19 limited women’s access to contraceptives and other sexual and reproductive health services.10 Sexual and reproductive services were much harder to come by during COVID-19, leaving women and adolescent girls in particular less able to control their fertility.12 Our results are remarkably similar to other studies conducted in Ethiopia,8 and Uganda.9 This result gives insight to policymakers and stakeholders to establish management strategies for adolescent girls to prevent unintended pregnancy in any similar crisis.
Our results revealed that adequate knowledge of the ovulation period is related to a lower probability of unwanted pregnancy among adolescent girls. Adolescent girls may experience unsafe abortions and inadvertent or unplanned pregnancies as a result of inadequate awareness of the reproductive cycle.23 This was a surprising result because a 2016 demographic and health survey in Uganda shows that periodic abstinence is rarely reported as a method of contraception. Nonetheless, given that COVID-19 restricted access to contraceptives and other sexual and reproductive health services,10 some teenagers may have used the option of abstinence. The significance of knowing the fertility window for unwanted pregnancy is often overlooked in studies on reproductive health in teenagers and young adults in favour of the use of contraception.24 Similar to our findings, inadequate knowledge of the ovulation period was a predictor of unintended pregnancy among adolescent girls.25 Therefore, proper fertility awareness is likely to help lower the likelihood of unplanned pregnancy, particularly in rural areas where access to contraception is limited.
Our results showed that sex education during COVID-19 was correlated with lower unplanned pregnancies among adolescent girls. Sex education is likely to have an impact on pregnancy in adolescents or via a variety of processes. Adolescents’ expected utility from getting involved in sexual activity depends on their knowledge and beliefs about the consequences of sex including pregnancy as well as their perception of the likelihood that such consequences will occur.26 Sex education may affect behaviour and, consequently, consequences like teenage pregnancy if it helps adolescents learn more about sexual activity, contraceptive use, and pregnancy. Observational studies consistently demonstrate that sex education is linked to decreased pregnancy risks, later age at first sex, and a higher likelihood of using contraceptives.27 Our results suggest that unintended pregnancy among adolescents should decline if the information provided on sex education programs is successful in changing young people’s preferences away from early births.
Our results indicated that participants who did not have the freedom to discuss family planning-related issues with family members during COVID-19 were likely to have unwanted pregnancies compared to their counterparts. Parents, especially in rural settings, tend not to discuss matters related to sex and contraceptives yet they are crucial in early pregnancy prevention. Early sexual debut is greatly influenced by the taboo around sex issues between parents and children, which is reflected in societal and cultural conventions.28 Interventions in parent-adolescent communication should raise awareness of contraception, educate parents about the negative effects of gender biases in the dissemination of information, and train parents in communication techniques that will help them play a more active role in their children’s sexual development.
Conclusion
Our study shows that unwanted pregnancies among adolescent girls remain a public health issue in Oyam district with more than two-thirds of adolescents having unwanted pregnancies during the crisis of COVID-19. The major correlates of unwanted pregnancies among adolescent girls during COVID-19 pandemic were inadequate knowledge of the ovulation period, sex education, and lack of freedom to discuss family planning-related issues with family members. There is a need to prioritize interventions, especially in rural settings. Sex education to improve contraceptive use and delay sexual debut. In light of the possibility that social and cultural norms in the Oyam district prohibit parents and children from discussing sexual subjects, it is crucial to promote sexual health education through the mass media, including newspapers, television, radio, and social media.
Strengths and Limitations of the Study
Our study is limited in scope and focused on adolescent girls attending Oyam district health centres in northern Uganda. Therefore, the experiences of women who had unwanted pregnancies were not captured. This study has some limitations: The association reported cannot be construed as a cause-and-effect relationship because the study is cross-sectional. Additionally, we could not rule out under-reporting of sexual activity given that it is a sensitive subject that is subject to social desirability bias. Despite its limitations, this study produced data that will help researchers better understand why teenage girls were prone to unwanted pregnancies during the COVID-19 pandemic.
Data Sharing Statement
The data used or analyzed in the present study are available from the corresponding author upon reasonable request.
Acknowledgment
We wish to acknowledge every participant who took part in the present study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research work was supported by seed funding from the Center for International Reproductive Health Training (CIRHT-UM), at the University of Michigan, it mainly supported the process of proposal development, data collection, and processing. The funder does not have any influence on the study findings or its processes.
Disclosure
The authors report no conflicts of interest in this work.
References
1. UNICEF. State of the World’s Children: Celebrating 20 Years of the Convention on the Rights of the Child. Unicef; 2009.
2. Sully EA, Biddlecom A, Darroch JE, et al. Adding it up: investing in sexual and reproductive health 2019. Sex Reprod Health. 2020;2020:10.
3. Anena MR, Orishaba J, Mwesigwa D. Literature review of teenage pregnancy in Uganda. Adv Soc Sci Res J. 2020;7(8):586–593. doi:10.14738/assrj.78.8848
4. Black AY, Fleming NA, Rome ES. Pregnancy in adolescents. Adolesc Med State Art Rev. 2012;23:123–xi.
5. Loaiza E, Liang M. Adolescent Pregnancy: A Review of the Evidence. Unfpa; 2013.
6. Mayor S. Pregnancy and childbirth are leading causes of death in teenage girls in developing countries; 2004.
7. Bearak J, Popinchalk A, Ganatra B, et al. Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990–2019. Lancet Glob Heal. 2020;8:e1152–e1161. doi:10.1016/S2214-109X(20)30315-6
8. Molla W, Hailemariam S, Mengistu N, et al. Unintended pregnancy and associated factors during COVID-19 pandemic in Ethiopia: community-based cross-sectional study. Women’s Heal. 2022;18. doi:10.1177/17455057221118170
9. Musinguzi M, Kumar G, Keswani T, et al. Prevalence and correlates of teenage pregnancy among in-school teenagers during the COVID-19 pandemic in Hoima district western Uganda–A cross sectional community-based study. PLoS One. 2022;17:e0278772. doi:10.1371/journal.pone.0278772
10. Kumar N, Singh AK. Impact of COVID-19 on gender equality, sexual and reproductive health rights of adolescent girls and young women: a narrative review. Curr Womens Health Rev. 2022;18:6–12. doi:10.2174/1573404817666210707094622
11. Lindberg LD, VandeVusse A, Mueller J, Kirstein M. Early impacts of the COVID-19 pandemic: findings from the 2020 Guttmacher survey of reproductive health experiences; 2020.
12. Shrivastava SR, Shrivastava PS. Unintended pregnancy and gender-based violence in settings experiencing humanitarian crisis. Indian J Heal Sci Biomed Res. 2022;15:180.
13. Mohammad S, Acharya N, Borkar K, Mohammad S. Effects of COVID-19 on Sexual and Reproductive health. Int J Res Pharm Sci. 2020;11:1841–1845. doi:10.26452/ijrps.v11iSPL1.4432
14. Wasswa R, Kabagenyi A, Atuhaire L. Determinants of unintended pregnancies among currently married women in Uganda. J Heal Popul Nutr. 2020;39:1–17.
15. Elayeete S, Nampeera R, Nsubuga EJ, et al. Comparative epidemiologic analysis of COVID-19 patients during the first and second waves of COVID-19 in Uganda. IJID Reg. 2022;3:160–167. doi:10.1016/j.ijregi.2022.03.017
16. Nuwematsiko R, Nabiryo M, Bomboka JB, et al. Unintended socio-economic and health consequences of COVID-19 among slum dwellers in Kampala, Uganda. BMC Public Health. 2022;22:1–13. doi:10.1186/s12889-021-12453-6
17. Ochen AM, Chi PC, Lawoko S. Predictors of teenage pregnancy among girls aged 13–19 years in Uganda: a community based case-control study. BMC Pregnancy Childbirth. 2019;19:1–14. doi:10.1186/s12884-019-2347-y
18. Bill O, Ojok G. O. 23,000 girls impregnated in Lango in one year - NGO. Monitor News Paper; 2021.
19. Sarah Biryomumaisho ST. How Covid-19 lockdown spiked teenage pregnancy. Observer. 2022;2022:105.
20. Mehare T, Mekuriaw B, Belayneh Z, Sharew Y. Postpartum contraceptive use and its determinants in Ethiopia: a systematic review and meta-analysis. Int J Reprod Med. 2020;2020:1–14. doi:10.1155/2020/5174656
21. Norton M, Chandra-Mouli V, Lane C. Interventions for preventing unintended, rapid repeat pregnancy among adolescents: a review of the evidence and lessons from high-quality evaluations. Glob Heal Sci Pract. 2017;5:547–570. doi:10.9745/GHSP-D-17-00131
22. Ameyaw EK, Budu E, Sambah F, et al. Prevalence and determinants of unintended pregnancy in sub-Saharan Africa: a multi-country analysis of demographic and health surveys. PLoS One. 2019;14(8):e0220970. doi:10.1371/journal.pone.0220970
23. Hampton K, Mazza D. Fertility-awareness knowledge, attitudes and practices of women attending general practice. Aust Fam Physician. 2015;44:840–845.
24. Kost K, Maddow-Zimet I, Arpaia A. Pregnancies, Births and Abortions Among Adolescents and Young Women in the United States, 2013. New York: National and state trends by age, race and ethnicity; 2017.
25. Iyanda AE, Dinkins BJ, Osayomi T, et al. Fertility knowledge, contraceptive use and unintentional pregnancy in 29 African countries: a cross-sectional study. Int J Public Health. 2020;65:445–455. doi:10.1007/s00038-020-01356-9
26. Oettinger GS. The effects of sex education on teen sexual activity and teen pregnancy. J Polit Econ. 1999;107:606–644. doi:10.1086/250073
27. Cheedalla A, Moreau C, Burke AE. Sex education and contraceptive use of adolescent and young adult females in the United States: an analysis of the National Survey of Family Growth 2011–2017. Contracept X. 2020;2. doi:10.1016/j.conx.2020.100048
28. Mark NDE, Wu LL. More comprehensive sex education reduced teen births: quasi-experimental evidence. Proc Natl Acad Sci. 2022;119. doi:10.1073/pnas.2113144119
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.