")
Back to Journals » Infection and Drug Resistance » Volume 13
Predictors of Time to Sputum Culture Conversion Among Drug-Resistant Tuberculosis Patients in Oromia Region Hospitals, Ethiopia
Authors Tekalegn Y , Woldeyohannes D , Assefa T , Aman R , Sahiledengle B
Received 22 February 2020
Accepted for publication 17 June 2020
Published 27 July 2020 Volume 2020:13 Pages 2547—2556
DOI https://doi.org/10.2147/IDR.S250878
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Yohannes Tekalegn,1 Demelash Woldeyohannes,1 Tesfaye Assefa,2 Rameto Aman,1 Biniyam Sahiledengle1
1Department of Public Health, School of Health Sciences, Goba Referral Hospital, Madda Walabu University, Bale Goba, Ethiopia; 2Department of Nursing, School of Health Sciences, Goba Referral Hospital, Madda Walabu University, Bale Goba, Ethiopia
Correspondence: Yohannes Tekalegn Addis Ababa 22847 code 1000, Ethiopia
Tel +251 913578901
Email [email protected]
Purpose: Multi-drug-resistant tuberculosis occurs when the tuberculosis bacteria develop resistance to at least the two most effective first-line anti-tuberculosis drugs, isoniazid and rifampicin. Sputum culture conversion is one of the indicators to monitor patients’ prognosis throughout the treatment. Hence, this study aimed to assess time to culture conversion and its determinants among drug-resistant tuberculosis patients.
Patients and Methods: A total of 228 drug-resistant tuberculosis patients in selected hospitals in Oromia region, Ethiopia, were included in this study. Descriptive statistics like median time to sputum smear and culture conversion were computed. Bivariate and multivariate Cox proportional hazard models were used to identify the independent predictors of time to culture conversion. The adjusted hazard ratio (AHR) with 95% confidence interval (CI) was used to report the strength of association. Statistical significance was declared at p < 0.05.
Results: The median age of the study participants was 28 years with inter-quartile range of (IQR) of 22– 32 years, and 60% of the patients were male. The median time to culture conversion was 61 days (IQR: 34– 92 days). The proportion of sputum culture conversion at 2nd, 4th, and 6th months of treatment initiation was 47%, 82.5%, and 89%, respectively. The final adjusted multivariate Cox proportional hazard model revealed that patients with massive effusion on chest radiographic finding had a 60%-decreased culture conversion time (AHR: 0.4, 95% CI: 0.1– 0.9). Patients with abnormalities without cavitations (AHR: 0.5, 95% CI: 0.2– 0.9) and those with uninterpreted findings (AHR: 0.3 95% CI: 0.1– 0.5) had delayed culture conversion time.
Conclusion: Chest radiographic findings such as massive effusion, abnormalities without cavitations, and uninterpreted findings were found to be predictors of time to sputum culture conversion. Patients with such characteristics have prolonged culture conversion time. Hence, they may need special attention during the treatment.
Keywords: multi-drug-resistant tuberculosis, tuberculosis, time to sputum culture conversion, predictors, survival analysis, treatment outcome, Oromia, Ethiopia
Introduction
Tuberculosis (TB) is an infectious disease caused by mycobacterium tuberculosis which can spread from person to person through the air.1 Normally, TB is treatable and curable. However, people with TB can suffer from complications and death if they do not get appropriate treatment.1 Globally, more than 1.7 billion people are infected by TB and about 10 million people became ill with TB in 2018.2 The burden of TB varies from region to region but almost 90% of TB case occurs in 30 high TB burden countries.2–5 Ethiopia is among the 30 high TB burden countries listed by the World Health Organization (WHO). In 2018, the incidence rate of TB was estimated to be 151 per 100,000 populations, and the incidence of multidrug-resistant TB (MDR-TB) or rifampicin-resistant (RR) was 1.4 per 100,000 people.2
MDR-TB occurs when the TB bacteria develop resistance to the two most effective first-line anti TB drugs, isoniazid and rifampicin.6–8 Even though ending the TB epidemic by 2030 is among the health targets of the Sustainable Development Goal.9 Drug-resistant TB remains to be a serious public health problem throughout the world. In 2018, there were about 500,000 new cases of rifampicin-resistant TB of which 78% had MDR-TB. The three countries with the largest share of the global burden were India (27%), China (14%) and the Russian Federation (9%).10–12 MDR-TB commonly develop in the course of TB treatment, and is most commonly due to incorrect or inadequate treatment, use of the wrong medications, not taking medication consistently or not completing full treatment course, and person to person transmission is also uncommon.13–16
Evidence shows that MDR-TB is associated with high treatment costs, increased risk of adverse drug events, and poor treatment outcomes.17–22 Culture conversion is one of the indicators of MDR-TB treatment success.23 However, MDR-TB treatment success is affected by multiple factors such as HIV co-infection, presence of lung fibrosis and consolidations, presence of multiple drug resistance, type of treatment regimen.24–28 Limited studies assessed the predictors of time to culture conversion among MDR-TB patients in Ethiopia, particularly in our study area. This study aimed to generate evidence on predictors of time to culture conversion among drug-resistant TB patients in Oromia regional state of Ethiopia.
Patients and Methods
Study Area, Period, Design, and Source Population
This study was conducted in Oromia regional state, Ethiopia. Oromia is the largest regional state in Ethiopia which covers 353, 690 square kilometers. According to the central statistical agency (CSA) report on the 2007 census, the region’s population size was 28,067,000 people.29 There are 74 hospitals, 1360 health centers, and 6778 health posts in the region. Out of all hospitals in the region, only seventeen hospitals have started multi-drug-resistant tuberculosis (MDR-TB) treatment during this study period. All MDR-TB patients in the region referred to those hospitals to get the treatment. From those hospitals, we selected eight hospitals that have a five-year registry of MDR-TB patients, namely, Metu Karl hospital, Shanan Gibe hospital, Nekemte Hospital, Bishoftu hospital, Shashamane hospital, Adama hospital, Chiro hospital, and Dadar hospital. These hospitals have a separate unit for MDR-TB treatment, and all patients included in this study were drug-resistant TB patients.
Inclusion Criteria
All complete and initially culture-positive drug-resistant tuberculosis patients’ chart registered between November 2012 and December 2017 were included in the study.
Exclusion Criteria
Patient records that have incomplete data regarding the drug regimen followed, date of treatment initiation, date of treatment outcomes, and smear or culture results, and other clinical characteristics required by the data collection tool.
Diagnostic Techniques
GeneXpert MTB/RIF assay, line probe assay, or culture methods were used to diagnose drug resistance in all patients treated at the study hospitals..
Treatment of MDR-TB
All hospitals follow the national ministry of health standardized treatment protocol for the treatment of RR/MDR-TB. The Ethiopian Federal Ministry of Health adopted a standardized treatment regimen which consists of an 8-month intensive phase with a combination of pyrazinamide, capreomycin, levofloxacin, and prothionamide or ethionamide and cycloserine followed by a 12-month continuation phase with a combination of pyrazinamide, levofloxacin, prothionamide or ethionamide and cycloserine.30 Most of the patients were admitted to the hospitals to follow the intensive phase of their treatment. They were discharged from the hospital once their smear and/or culture result converted to negative. Upon discharge, the patients continued their treatment at MDR-TB follow up clinics where daily direct observation treatments (DOTs) were given. The patients returned to their respective hospital outpatient MDR-TB follow up clinics monthly for evaluation. Sputum smears and cultures were collected and processed monthly for all inpatients and outpatients.
Dependent and Independent Variables
Time to sputum culture conversion was the dependent variable for this study. Censored was defined as: when culture result has not been converted for an individual. This includes when the patient stops the treatment even though the culture was positive, deceased before culture conversion, transferred out to another treatment site before culture conversion, and study time completion before culture conversion.
Data Collection Tools and Procedures
Semi-structured data collection tool was developed after reviewing different literature and client record/logbook.31 The tool contains variables on the outcome of interest that is time to smear and culture conversion, variables regarding socio-demographic characteristics, and clinical characteristics.
Data Quality Assurance
Data extraction tool was pretested on 15% of patients’ charts at Goba referral hospital hospital. Based on the finding of pre-test necessary amendments were made on the tool before the actual data collection. Data collectors and supervisors were recruited from the health professionals with clinical experience. Two days of training was given for data collectors and supervisors on the objectives of the study and how to use the data extraction tool. The completeness of the data was checked daily before leaving the facility.
Data Analysis
The collected data were first entered into EpiData V.3.1 and exported to SPSS V.20 for analysis. Descriptive statistics like median time to sputum smear and culture conversion were computed. Kaplan–Meier survival curve was used to illustrate the median time to culture conversion. The bivariate and multivariate Cox proportional hazard model was used to detect independent predictors of time to culture conversion. The adjusted hazard ratio with 95% confidence level was used to report the strength and presence of an association. Statistical significance was declared at p <0.05.
Ethical Statement
Ethical clearance was obtained from Madda Walabu University Ethical Review Committee. Upon the ethical approval, permission letter to conduct the study was submitted to the respective Clinical Director/Managers of the Hospitals. Tuberculosis clinic heads gave the consent for accessing and extracting data from records at each Hospital. Patient names and identification numbers were not extracted to ensure the confidentiality of patient information.
Operational Definitions
Sputum conversion: Is defined as two sets of consecutive negative smears and cultures, from samples collected at least 30 days apart. The date of collection for the first sample is considered as the date of conversion.
Multi-drug resistance: Resistance to at least both isoniazid and rifampicin
Rifampicin resistance (RR-TB): Resistance to rifampicin detected using phenotypic or genotypic methods, with or without resistance to other anti-TB drugs. It includes any resistance to rifampicin, whether mono-drug resistance, multi-drug resistance, poly-drug resistance, or extensive drug resistance.
New case: A patient who has received no or less than one month of anti-tuberculosis treatment.
Previously treated with First-line drugs: A patient who has received first-line anti-tuberculosis treatment for four weeks or more.
Relapse: A patient who was previously treated for TB and whose most recent treatment outcome was “cured” or “treatment completed”, and who is subsequently diagnosed with bacteriologically positive TB by sputum smear microscopy, GeneXpert MTB/RIF, or culture.
Treatment after being lost to follow-up: A patient after taking treatment for more than one month who returns to treatment, bacteriologically positive by sputum smear microscopy, GeneXpert MTB/RIF TB/RIF, or culture, following interruption of treatment for two or more consecutive months.
Treatment after failure of New TB regimen: A patient who has received a new regimen for TB and in whom treatment has failed. Failure is defined as sputum smear-positive at five months or later during treatment.
Treatment after failure of Retreatment regimen: A patient who has received a retreatment regimen for TB and in whom treatment has failed. Failure is defined as sputum smear-positive at five months or later during treatment.
Transfer in: A patient who has been transferred from another treatment initiation center to continue MDR-TB treatment.
Cured: Treatment completed according to national recommendation without evidence of failure and three or more consecutive cultures taken at least 30 days apart are negative after the intensive phase.
Treatment completed: Treatment completed according to national recommendation without evidence of failure but no record that three or more consecutive cultures taken at least 30 days apart are negative after the intensive phase.
Treatment failure: Treatment was considered to be failed if two or more of five cultures in the final 12 months of therapy are positive or if any one of the final three cultures is positive.
Died: A patient who dies during TB treatment.
Results
Socio-Demographic Characteristics
A total of 228 drug-resistant tuberculosis patients with initial positive sputum culture were included in this analysis. The median age of the patients was 28 years (IQR: 22–32 years). Male accounts for 60% of the study participants. More than half (62%) of the patients were urban dwellers (Table 1).
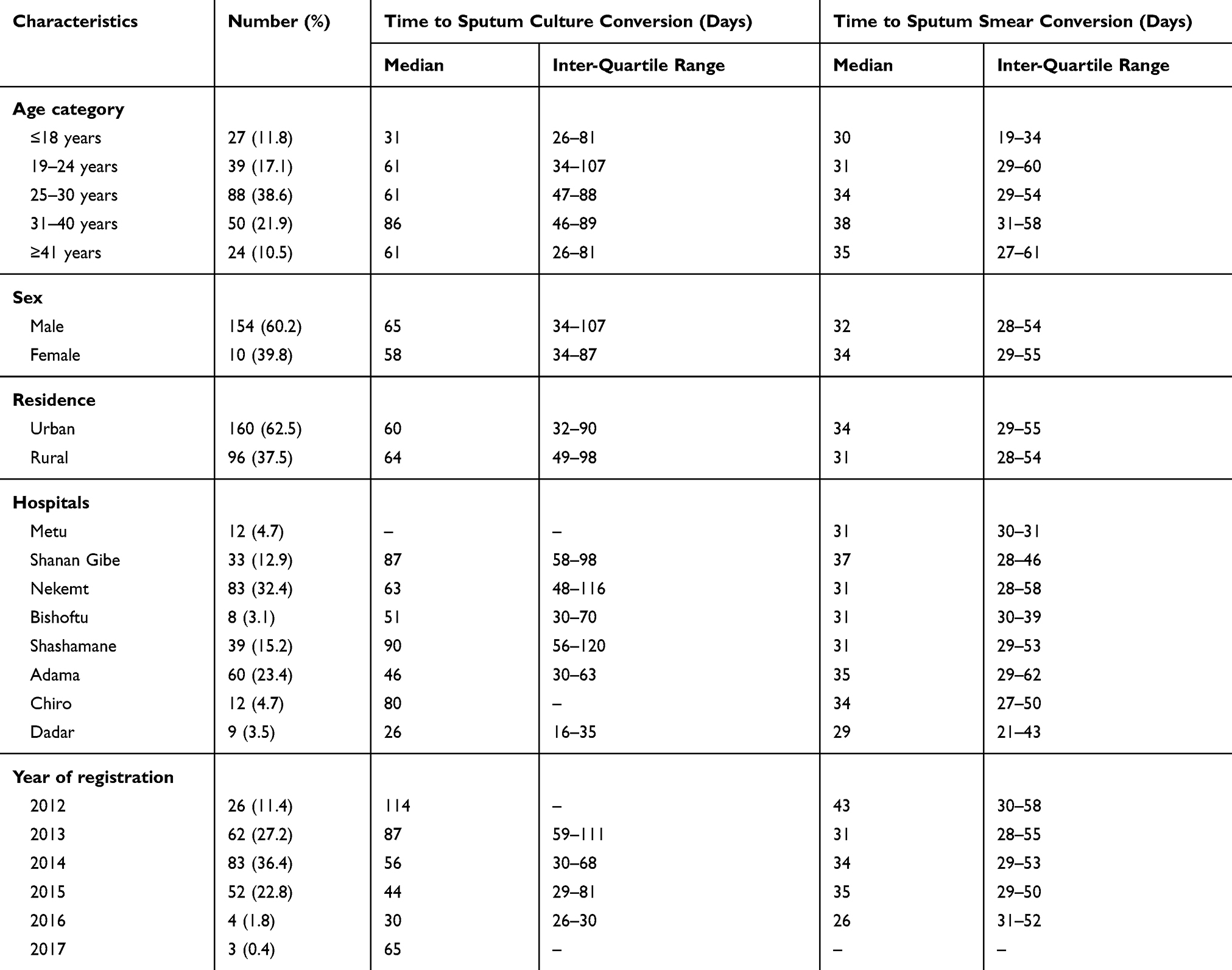 |
Table 1 Socio-Demographic Characteristics of Drug-Resistant Tuberculosis Patients Following Treatment in Oromia Regional State Hospitals from 2012 to 2017, Oromia, Ethiopia |
Clinical Characteristics of Study Participants
Out of 228 patients with initial culture positive result, 10% were new cases, about 16% relapse, about 48% were after the failure of retreatment with the first-line anti-TB regimen and 20% were failures after a new fist line anti-TB regimen. The diagnosis of drug resistance was made by GeneXpert MTB/RIF assay (79.4%), line probe assays (14.9%), or culture (5.7%). Regarding the drug-resistance, about 32% of the patients had drug susceptibility tests (DST) showing both isoniazid (INH) and rifampicin (RIF) resistance while 97.8% had rifampicin resistance. About 10% of study participants encountered adverse drug effects during treatment. Out of all study participants, about 5% had a history of smoking. Regarding the body mass index (BMI) of study participants, most (69%) of them had a BMI <18.5 kg/m2 (Table 2).
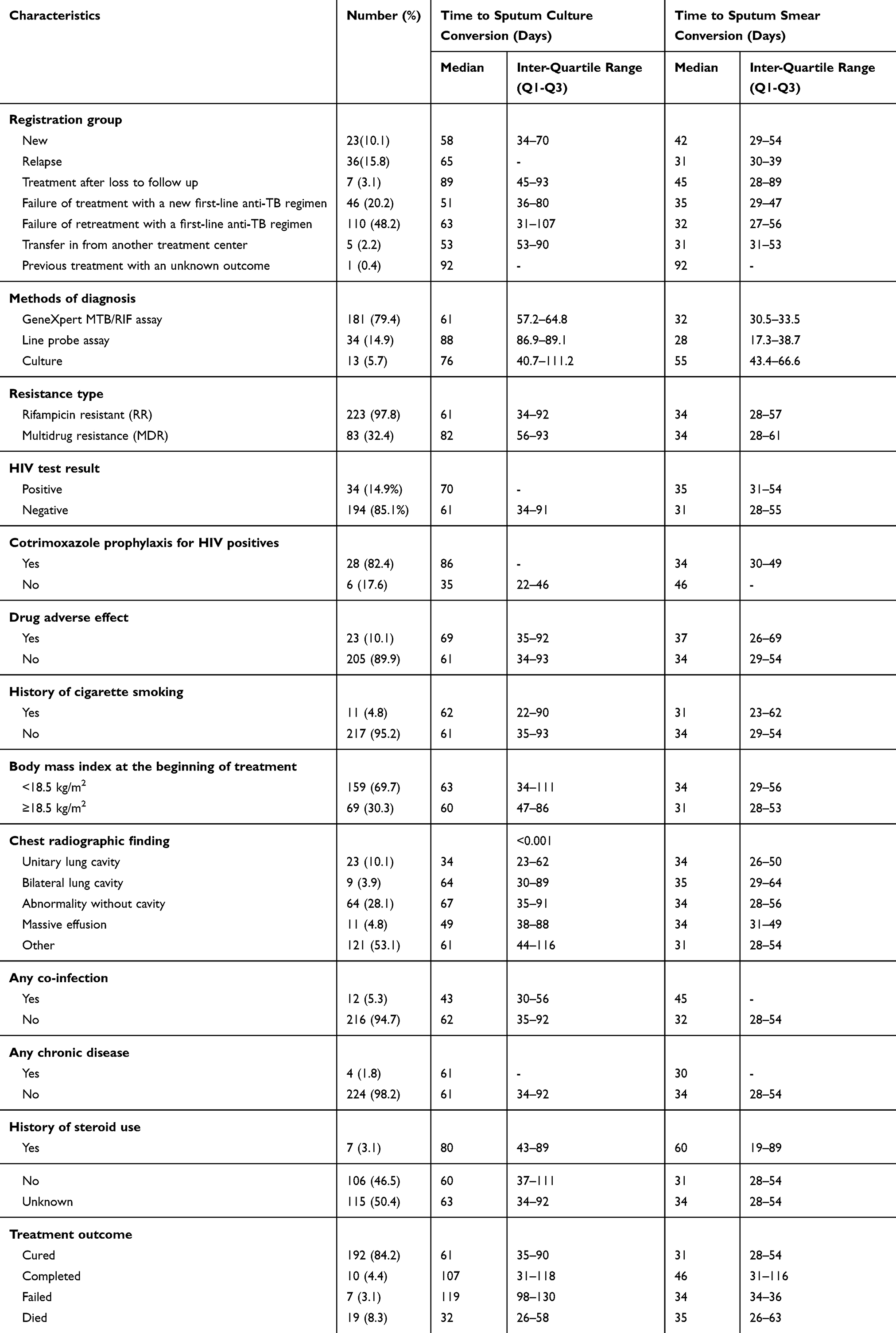 |
Table 2 Clinical Characteristics of Drug-Resistant Tuberculosis Patients Following Treatment in Oromia Regional State Hospitals from 2012 to 2017, Oromia, Ethiopia |
Time to Sputum Smear and Culture Conversion
The median time to sputum culture conversion to negative was 61 days with an inter-quartile range of 34–92 days. At the same time, the median time to sputum smear conversion was 34 days with an inter-quartile range of 28–54 days. The proportion of culture conversion at 2nd, 4th, and 6th months was 46.9%, 82.5%, and 89%, respectively. The proportion of smear conversion at 2nd, 4th, and 6th months was 81.6%, 94.5%, and 94.9%, respectively (Table 3).
 |
Table 3 Time to Sputum Smear and Culture Conversion of Drug-Resistant Tuberculosis Patients Following Treatment in Oromia Regional State Hospitals from 2012 to 2017, Oromia, Ethiopia |
Predictors of Time to Sputum Culture Conversion
Socio-demographic and clinical characteristics of patients were assessed for a possible difference in survival distribution using the Kaplan-Meier curve and Log rank tests. Patient characteristics like age, use of cotrimoxazole prophylaxis for HIV patients, body mass index, and chest-radiographic findings were found to have a significant difference in time to culture conversion (Table 4).
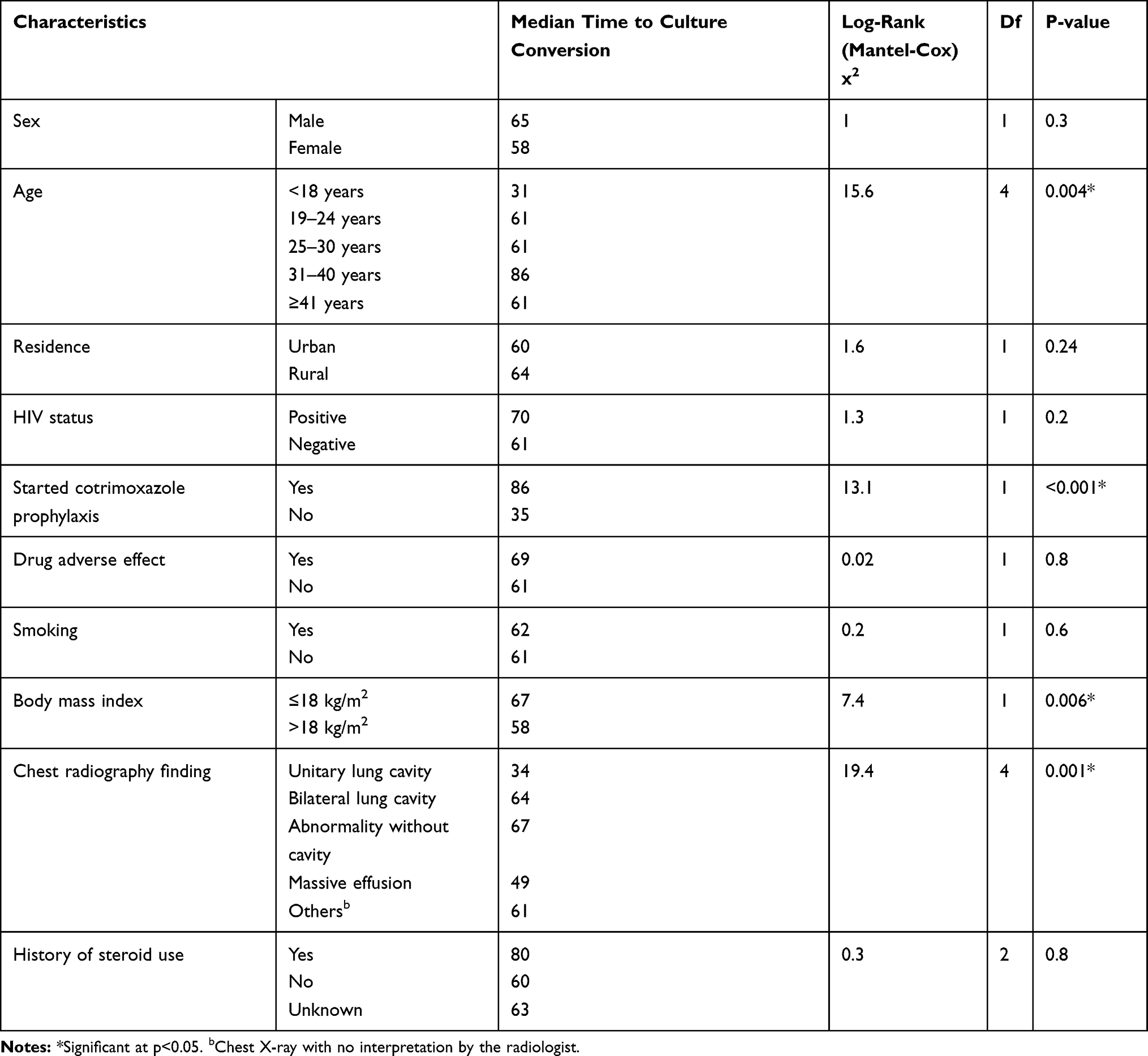 |
Table 4 Test of Equality of Survival Distribution Among Drug-Resistant Tuberculosis Patients Following Treatment in Oromia Regional State Hospitals from 2012 to 2017, Oromia, Ethiopia |
In the final multivariate Cox-regression analysis, we found that the patient’s chest radiographic finding was a predictor of time to culture conversion. The culture conversion rate among patients with massive effusion was decreased by 60% (AHR: 0.4, 95% CI: 0.1–0.9) as compared to those with unitary lung cavitations. At the same time, the culture conversion rate among patients with abnormalities without cavitations decreased by 50% (AHR: 0.5, 95% CI: 0.2–0.9) when compared to those with unitary lung cavitations (Table 5).
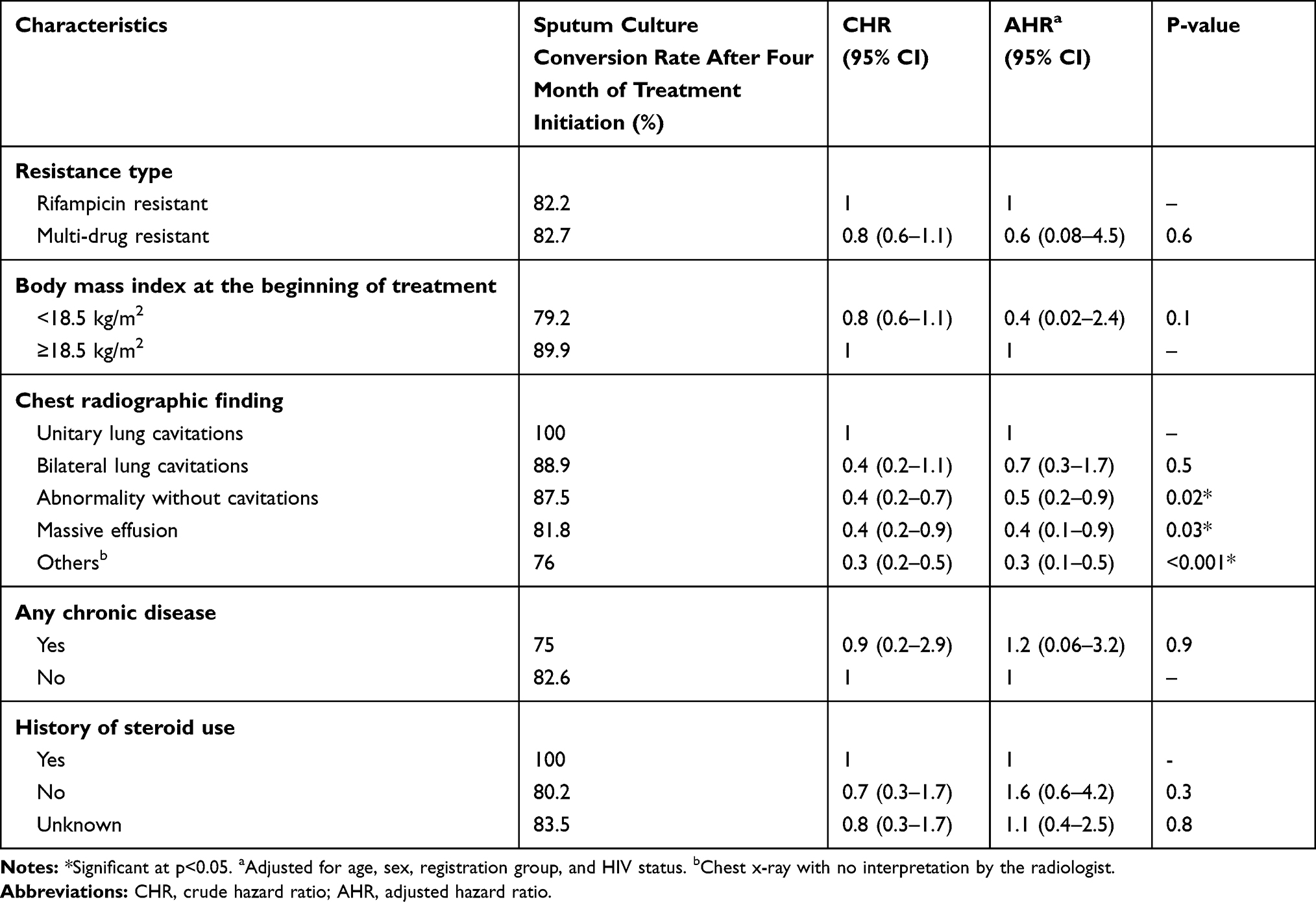 |
Table 5 Predictors of Time to Culture Conversion Among Drug-Resistant Tuberculosis Patients Following Treatment in Oromia Regional State Hospitals from 2012 to 2017, Oromia, Ethiopia |
Discussion
In the treatment of multidrug-resistant tuberculosis (MDR-TB) Sputum culture conversion is used as an indicator for the success of the treatment and used to guide the patient treatment regimen.32,33 This study assessed predictors of time to culture conversion among Drug-resistant tuberculosis (DR-TB) patients attending their treatment in Oromia regional state hospitals, Ethiopia.
A total of 228 initially culture-positive DR-TB patients were included in this study. The median time to culture conversion was 61 days. This finding is comparable with studies conducted in the Amhara region (65 days)34 and Gondar (72 days),35 Latvia (60 days),28 Peru (59 days),36 and Indonesia (60 days).37 The present study reported a shorter median time to culture conversion compared to studies conducted in China (159 days),38 USA (93 days),39 Delhi (91 days),40 London (91 days).41 The median time to culture conversion in the present study is longer than the study conducted in Seoul (19 days),42 Germany (39 days),43 and India (35 days).44 The discrepancy in the median time to sputum culture conversion could be due to the reporting system of the time to conversion. Some studies used two consecutive negative culture results to report culture conversion, and others reported initial culture conversion to negative as well as re-conversion to a negative culture. This study used the first month in which the culture result turns negative to report the time to sputum conversion. The other possible source of the discrepancy could be factors such as the frequency with which sputum samples are tested (weekly vs monthly), resistance to additional drugs (which can vary by geographical region), and the availability of effective drugs. Some of the hospitals included in this study have no facility for culture testing so that they collect and send sputum to the other hospital this, in turn, might result in delayed reporting or sometimes missing of the result might have occurred.
This study found that 89% of DR-TB patient’s sputum culture converted to negative at 6 months of treatment initiation. This finding is in line with the study conducted in Gondar (88.6%),35 India (87%),45 South Africa (89%),46 Peru (92.9%),36 and China (90.5%).38 On the other hand, the four-month sputum conversion rate in the current study found to be 82.5%. The four-month conversion rate is higher than the study conducted in Latvia (60%).28 The two-month culture conversion rate in this study was 46.9% which is much lower than the study conducted in Seoul (90.1%)42 China (65.2%)47 and Germany (61%),43 but higher than reported finding from Chinese study (33.3%).38 The difference in the culture conversion rate among different study sites might be related to a difference in treatment protocol followed in different sites, the difference in the study population, type of drug resistance, and the difference in the quality of reported data.
In this study patients in the age group, less than 18 years have shorter culture conversion time (p=0.004) compared to older ages. The previous study reported that as age increases the risk of TB drugs adverse outcome increases.48 Furthermore, patients with baseline body mass index lower than 18 kg/m2 had a long time to culture conversion than their counterparts. Similar previous studies reported that malnourished MDR-TB patients had longer conversion time.35,40,49
In this study patient’s chest radiologic findings like lung cavitations, and massive effusion was found to affect the time to sputum culture conversion. In Cox regression analysis patients with massive effusion found to have less sputum culture conversion rate than those with unitary lung cavitations. When we compare the Kaplan Meier survival curve using a Log rank test, patients with unitary lung cavity had a shorter median time to culture conversion than those with bilateral lung cavitations, and massive effusion. Previous studies reported that patients with lung cavitations had delayed time to culture conversion.34,50 This might be related to the fact that lung cavitations might hinder drug penetration and thus decrease the therapeutic efficacy of the drugs.
This study tried to assess the predictors of time to sputum culture conversion. Some of the strengths of this study were using data from eight hospitals and using five-year data. However, this study had limitations so that results from the study should be used with caution. Among the limitations, and the study used initial culture conversion to assess time to culture conversion, it does not assess the re-conversion of culture. The study used secondary data from hospital records so that limitations associated with secondary data might apply.
Conclusion
Chest radiographic findings such as massive effusion, abnormalities without cavitations, and uninterpreted findings were found to be predictors of time to sputum culture conversion. Patients with such characteristics have prolonged culture conversion time. Hence, they may need special attention during the treatment.
Acknowledgments
We thank Madda Walabu University for its financial support for this research. We thank all study participants, data collectors, and supervisors involved in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global tuberculosis report 2015 (WHO/HTM/TB/2015.22). Geneva. Available from: https://apps.who.int/iris/bitstream/handle/10665/191102/9789241565059_eng.pdf;jsessionid=257E179B7641F5CE7FD14BEF18488436?sequence=1.
2. World Health Organization. Global tuberculosis report 2019. Geneva. 2019. Licence: CC BY-NC-SA 3.0 IGO.
3. World Health Organization. WHO and Global Fund sign cooperation agreement. Strategic Initiative to reach missed TB cases a critical component of grant; 2019. Geneva. Available from: https://www.who.int/tb/features_archive/WHO_Global_Fund_agreement/en/.
4. World Health Organization. Public–private mix (PPM) for TB prevention and care [website]; 2018. Geneva. Available from: https://www.who.int/tb/areas-of-work/public-private-mix/en/.
5. Wang H, Naghavi M, Allen C, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1459–1544. doi:10.1016/S0140-6736(16)31012-1
6. LoBue P, Sizemore C, Castro KG. Plan to combat extensively drug-resistant tuberculosis: recommendations of the Federal Tuberculosis Task Force. MMWR Recomm Rep. 2009;58(RR–3):1–43.
7. WHO. Multidrug-resistant tuberculosis (MDR-TB). In: 2015 UPDATE. Programme Wgt. Geneva: World Health Organization; 2015.
8. WHO. Definitions and Reporting Framework for Tuberculosis– 2013 Revision. Vol. 2013. Geneva: World Health Organization; 2013.
9. Callithen N, Matthew N, 2007. United Nations Development Programme (UNDP).
10. WHO (2019). Tuberculosis key facts. Available from: https://www.who.int/en/news-room/fact-sheets/detail/tuberculosis.
11. United Nations General Assembly. Resolution 73/3: political declaration of the high-level meeting of the General Assembly on the fight against tuberculosis. United Nations; 2018 Available from: https://www.un.org/en/ga/search/view_doc.asp?symbol=A/RES/73/3.
12. World Health Organization. Thirteenth general programme of work, 2019–2023. Geneva. 2018. Available from. https://apps.who.int/iris/bitstream/handle/10665/324775/WHO-PRP-18.1-eng.pdf.
13. Iseman MD. Treatment of multidrug-resistant tuberculosis. N Engl J Med. 1993;329(11):784–791. doi:10.1056/NEJM199309093291108
14. Millard J, Ugarte-Gil C, Moore DA. Multidrug resistant tuberculosis. BMJ. 2015;350(feb26 10):h882. doi:10.1136/bmj.h882
15. Keshavjee S, Farmer PE. Tuberculosis, drug resistance, and the history of modern medicine. N Engl J Med. 2012;367(10):931–936. doi:10.1056/NEJMra1205429
16. Iang L, Wu Q, Gao L, et al. Factors contributing to the high prevalence of multidrug-resistant tuberculosis: a study from China. Thorax. 2012;67(7):632. doi:10.1136/thoraxjnl-2011-200018
17. World Health Organization. Global tuberculosis report 2016. Geneva, Switzerland 2016.
18. European Centre for Disease Prevention and Control (ECDC). Tuberculosis Surveillance and Monitoring in Europe 2016. Stockholm, Sweden: European Centre for Disease Prevention and Control; 2017.
19. Ahuja SD, Ashkin D, Avendano M, et al. Multidrug resistant pulmonary tuberculosis treatment regimens and patient outcomes: an individual patient data meta-analysis of 9153 patients. PLoS Med. 2012;9(8):e1001300. doi:10.1371/journal.pmed.1001300
20. Falzon D, Gandhi N, Migliori GB, et al. Resistance to fluoroquinolones and second-line injectable drugs: impact on multidrug-resistant TB outcomes. Eur Respir J. 2013;42(1):156–168. doi:10.1183/09031936.00134712
21. Sotgiu G, Centis R, D’Ambrosio L, et al. Efficacy, safety and tolerability of linezolid containing regimens in treating MDR-TB and XDR-TB: systematic review and meta-analysis. Eur Respir J. 2012;40(6):1430–1442. doi:10.1183/09031936.00022912
22. Günther G, Gomez GB, Lange C, Rupert S, van Leth F; Tbnet. Availability, price and affordability of anti-tuberculosis drugs in Europe: a TBNET survey. Eur Respir J. 2015;45(4):1081–1088. doi:10.1183/09031936.00124614
23. World Health Organization. Multidrug-resistant tuberculosis (MDR-TB) indicators. A minimum set of indicators for the programmatic management of MDR-TB in national tuberculosis control programmes. Geneva. 2010. WHO/HTM/TB/2010.11; http://whqlibdoc.who.int/hq/2010/WHO_HTM_TB_2010.11_eng.pdf.
24. Mulu WMD, Admassu A, Admassu A, Abera B. Risk factors for multi drug resistant tuberculosis patients in Amhara National Regional State. Afr Health Sci. 2015;15(2):368. doi:10.4314/ahs.v15i2.9
25. Kanda R, Nagao T, Tho NV, et al. Factors affecting time to sputum culture conversion in adults with pulmonary tuberculosis: historical cohort study without censored cases. PloSone. 2015;10(11):e0142607. doi:10.1371/journal.pone.0142607
26. Lee J, Lee BJ, Yoon HI, Lee CT, Lee JH. Influence of previous tuberculosis treatment history on acid fast bacilli smear and culture conversion. Int J Tuberc Lung Dis. 2012;16(10):1344–1348. doi:10.5588/ijtld.12.0113
27. Kurbatova E, Gammino V, Bayona J, et al. Predictors of sputum culture conversion among patients treated for multidrug-resistant tuberculosis. Int J Tuberc Lung Dis. 2012;16(10):1335–1343. doi:10.5588/ijtld.11.0811
28. Holtz TH, Sternberg M, Kammerer S, et al. Time to sputum culture conversion in multidrug-resistant tuberculosis: predictors and relationship to treatment outcome. Ann Intern Med. 2006;144(9):650–659. doi:10.7326/0003-4819-144-9-200605020-00008
29. Office of the Population and Housing Census Commission, 2008. Summary and statistical report of the 2007 population and housing census: population size by age and sex. Federal Democratic Republic of Ethiopia, Population Census Commission. Ethiopia.
30. Kebede B, Ayele A, Kassa A, et al. Guidelines on Programmatic Management of Drug Resistant Tuberculosis in Ethiopia. Addis Ababa, Ethiopia: Health FDROEMO;2013.
31. Federal Ministry of Health of Ethiopia (FMOH). Guideline for Program and Clinical Management of Drug Resistant Tuberculosis. Addis Ababa: FMOH; 2009.
32. World Health Organization. Guidelines for Establishing DOTS-Plus Pilot Projects for the Management of Multidrug-Resistant Tuberculosis (MDR-TB). Geneva: World Health Organization;2000.
33. Laserson KF, Thorpe LE, Leimane V, et al. Speaking the same language: treatment outcome definitions for multidrugresistant tuberculosis. Int J Tuberc Lung Dis. 2005;9(6):640–645.
34. Yihunie Akalu T, Muchie KF, Alemu Gelaye K, Munderloh UG. Time to sputum culture conversion and its determinants among multi-drug resistant Tuberculosis patients at public hospitals of the Amhara Regional State: a multicenter retrospective follow up study. PLoS One. 2018;13(6):e0199320–e. doi:10.1371/journal.pone.0199320
35. Shibabaw A, Gelaw B, Wang S-H, Tessema B, Cardona P-J. Time to sputum smear and culture conversions in multidrug resistant tuberculosis at University of Gondar Hospital, Northwest Ethiopia. PLoS One. 2018;13(6):e0198080–e. doi:10.1371/journal.pone.0198080
36. Tierney DB, Franke MF, Becerra MC, et al. Time to culture conversion and regimen composition in multidrug-resistant tuberculosis treatment. PLoSONE. 2014;9(9):e 108035. doi:10.1371/journal.pone.0108035
37. Putri FA, Burhan E, Nawas A, et al. Body mass index predictive of sputum culture conversion among MDR-TB patients in Indonesia. Int J Tuberc Lung Dis. 2014;18(5):564–570. doi:10.5588/ijtld.13.0602
38. Lu P, Liu Q, Martinez L, et al. Time to sputum culture conversion and treatment outcome of patients with multidrug-resistant tuberculosis: a prospective cohort study from urban China. Eur Respir J. 2017;49(3):1601558. doi:10.1183/13993003.01558-2016
39. Shah NS, Pratt R, Armstrong L, Robison V, Castro KG, Cegielski JP. Extensively Drug-Resistant Tuberculosis in the United States, 1993–2007. JAMA. 2008;300(18):2153–2160. doi:10.1001/jama.300.18.2153.
40. Velayutham B, Nair D, Kannan T, et al. Factors associated with sputum culture conversion in multi-drug resistant pulmonary tuberculosis. Int J Tuberc Lung Dis. 2016;20(12):1671–1676. doi:10.5588/ijtld.16.0096
41. Rieu R, Chang C, Collin SM, et al. Time to detection in liquid culture of sputum in pulmonary MDR-TB does not predict culture conversion fore arly discharge. J Antimicrob Chemother. 2016;71(3):803–806. doi:10.1093/jac/dkv407
42. Lee HY, Chae KO, Lee CH, et al. Culture conversion rate at 2 months of treatment according to diagnostic methods among patients with culture-positive pulmonary tuberculosis. PLoS One. 2014;9(8):e103768. doi:10.1371/journal.pone.0103768
43. Heyckendorf J, van Leth F, Avsar K, et al. Treatment responses in multidrug-resistant tuberculosis in Germany. Int J Tuberc Lung Dis. 2018;22(4):399–406. doi:10.5588/ijtld.17.0741
44. Parikh R, Nataraj G, Kanade S, Khatri V, Mehta P. Time to sputum conversion in smear positive pulmonary TB patients on category I DOTS and factors delaying it. J Assoc Physicians India. 2012;60:22–26.
45. Joseph P, Rao Desai VB, Mohan NS, et al. Outcome of standardized treatment for patients with MDR-TB from Tamil Nadu, India. Indian J Med Res. 2011;133:529–534.
46. Brust JCM, Lygizos M, Chaiyachati K, et al. CultureConversion among HIVCo-infected multidrug-resistant tuberculosis patients in Tugela Ferry, South Africa. PLoS One. 2011;6(1):e15841. doi:10.1371/journal.pone.0015841
47. Lv L, Li T, Xu K, et al. Sputum bacteriology conversion and treatment outcome of patients with multidrug-resistant tuberculosis. Infect Drug Resist. 2018;11:147. doi:10.2147/IDR.S153499
48. Akinsola OJ, Yusuf OB, Ige OM, Okonji PE. Models for predicting time to sputum conversion among multi-drug resistant tuberculosis patients in Lagos, South–West Nigeria. Front Public Health. 2018;6:347. doi:10.3389/fpubh.2018.00347
49. Magee MJ, Kempker RR, Kipiani M, et al. Diabetes mellitus, smoking status, and rate of sputum culture conversion in patients with multidrug-resistant tuberculosis: a cohort study from the country of Georgia. PLoS One. 2014;9(4):e94890. doi:10.1371/journal.pone.0094890
50. Yew WW, Chan CK, Chau CH, et al. Outcomes of patients with multidrug-resistant pulmonary tuberculosis treated with ofloxacin/levofloxacin-containing regimens. Chest. 2000;117(3):744–751. doi:10.1378/chest.117.3.744
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.