")
Back to Journals » Cancer Management and Research » Volume 12
Predictors of Precancerous Cervical Lesions Among Women Screened for Cervical Cancer in Bahir Dar Town, Ethiopia: A Case–Control Study
Authors Alamiraw JA, Asres AW , Adella GA
Received 14 April 2020
Accepted for publication 26 June 2020
Published 27 July 2020 Volume 2020:12 Pages 6331—6339
DOI https://doi.org/10.2147/CMAR.S258167
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eileen O'Reilly
Jerusalem Azene Alamiraw,1 Abiyot Wolie Asres,2 Getachew Asmare Adella3
1Amhara Regional Health Bureau, Bahir Dar, Ethiopia; 2Department of Epidemiology and Biostatistics, School of Public Health, College of Health Science and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 3Department of Reproductive Health and Nutrition, School of Public Health, College of Health Science and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia
Correspondence: Getachew Asmare Adella
Department of Reproductive Health and Nutrition, School of Public Health, College of Health Science and Medicine, Wolaita Sodo University, Wolaita Sodo Ethiopia
Tel +251918315569
Email [email protected]
Purpose: Cancer of the cervix is the second most common cancer among women worldwide. Despite it is a serious public health problem in Sub-Saharan African countries including Ethiopia, formation on predictor of the precancerous cervical lesion is not well documented, particularly in the study area. This study aimed to identify the predictors of precancerous cervical lesions among women screened for cervical cancer in Bahir Dar town, North West Ethiopia, 2018/19.
Patient and Methods: Institution-based unmatched case–control study was conducted in selected health facilities in Bahir Dar town from November 15, 2018, to January 16, 2019. Data were collected from 102 cases and 305 controls using an interviewer-administered structured questionnaire and entered into Epi Data version 3.1, then export to SPSS version 23 for analysis. Variables with P-value ≤ 0.2 in the bivariate analysis were included in the multivariate logistic regression model. Odds ratio with 95% confidence interval was used to identify the predictors of precancerous cervical lesions.
Results: Women who initiated sexual intercourse before the age of 18 years (AOR = 1.68, 95% CI: 1.015– 2.804), history of sexually transmitted infection (AOR =1.74, 95% CI: 1.087– 2.790) and two or more lifetime sexual partners (AOR=1.733, 95% CI: 1.069– 2.810) were predictors for a precancerous cervical lesions.
Conclusion: This study confirms that the initiation of sexual intercourse before the age of 18 years, having history of sexually transmitted infection, and two or more lifetime sexual partners were determinants for precancerous cervical lesions. So that it should be focused on prevention through early detection and treatment of sexually transmitted infection with condom promotion. Women with a higher risk of precancerous lesions should also be encouraged to be screened more frequently for cervical cancer.
Keywords: precancerous cervical lesion, human papillomavirus, visual inspection with acetic acid
Introduction
Globally, approximately 570,000 cases of cervical cancer and 311,000 deaths from the disease occurred in 2018. Cervical cancer was the fourth most common cancer in women, ranking after breast cancer, colorectal cancer, and lung cancer. Approximately 90% of deaths from cervical cancer occurred in low- and middle-income countries. Ethiopia accounts for 7095 newly diagnosed cervical cancer cases and 4732 cervical cancer deaths in 2012.1,2
Cervical cancer is cancer arising from the cervix, in which the cells of the cervix become abnormal and start to grow uncontrollably, forming a tumor. Approximately 90% of intraepithelial neoplasm is attributed to human papillomavirus (HPV) infection.3
Visual Inspection with Acetic Acid (VIA) is one of the screening modality of the precancerous cervical lesion.4 Screening with VIA in low-income countries is a commonly preferred method than Human Papilloma Virus (HPV) test and cytologic or Pap smear. This is because it does not need more advanced trained crypto-technicians or pathologists and other programmatic requirements.5 In Ethiopia, screening uptake of women in the community is low6,7 because of the lack of awareness of the community about cervical cancer risk factors and prevention methods.8–11 In addition to these, screening uptake, as well as knowledge about cervical cancer risk factors and prevention, is also low among the health workers.12,13
Identifying predictors of the precancerous cervical lesion is important for planning more targeted screening programs to decrease the high morbidity and mortality of the disease in the country.14 However, the predictor of precancerous cervical lesions among the general population in Ethiopia is not well identified. Studies conducted so far in Ethiopia are limited to assessing the cost and its predictors of cervical cancer treatment, prevalence, and predictors of Pap smear cervical epithelial cell abnormality, risk factors associated with invasive cervical carcinoma, knowledge about cervical cancer, HPV prevalence, prevalence and risk factors among Human Immune Deficiency Virus (HIV) positive women. Even a study done about the predictor was centrally located in Addis Ababa where most facilities available to prevent as well as to detect early.14,16-19 The Ethiopian health sector development program IV (2010/11–2014/15) includes the prevention and control strategies of cancer.20 We undertook this research to identify predictors of the precancerous cervical lesion to inform and strengthen the existing cervical cancer prevention and control programs in peripheral regions in the country. Besides, the study will inform health education about cervical cancer prevention and stimulate etiologic research about cervical precancerous lesions.
Methods and Materials
Study Area and Period
The study was conducted from November 15, 2018, to January 16, 2019, in Bahir Dar town (the capital city of the Amhara region) which is the second largest and populous region in Ethiopia, located approximately 565 km northwest of Addis Ababa capital city of Ethiopia. The total population of the town is 348, 778 of whom 179,849 (52%) are female. The town has one comprehensive specialized public hospital serving approximately five million people within and outside the city, ten public health centers, ten public health posts, two private hospitals, seventeen private medium clinics, twelve junior private clinics, and five Non-Governmental organization (NGO) comprehensive health facilities. The study was conducted in selected health facilities that provide cervical cancer screening services at Felege Hiwot Comprehensive Specialized Hospital (FHCSH), Family Guidance Association of Ethiopia (FGAE) and Maris topes international Ethiopia.21
Study Design
An institution-based unmatched case–control study design was conducted.
Source Population
All women who utilized services from FHCSH, FGAE, and Maris topes international Ethiopia.
Study Population
Cases – All women having positive cervical cancer screening result in FHCSH, FGAE and Maris topes international Ethiopia during the study period.
Controls – All women having negative cervical cancer screening result at FHCSH, FGAE, and Maris topes international Ethiopia during the study period.
Sample Size Determination and Sampling Procedure
Sample Size Determination
Two population proportion sample size calculation formula was used to estimate the required sample size using Epi Info version 7 with the assumption of 95% CI, power =80% with case and control ratio of 1:3 which was taken from the previous study done in Adama, Ethiopia, 2017.22 Based on the above assumptions the sample size became 378 (cases= 95 and controls=283). By adding a 10% non-response rate, the final sample size was 415 (104 cases and 311 controls) (Table 1).
 |
Table 1 Shows Sample Size Determination for Study Participants in 2018/19 |
Sampling Procedure
Out of the 56 health facilities in Bahir Dar town, three of them were given cervical cancer screening services with VIA, which were FHCSH, FGAE and Mari stop International Ethiopia. Those health facilities were selected purposively due to the provision of cervical cancer screening using VIA regularly for all women. The total sample size was proportionally allocated to each selected health facility based on average monthly client flow, as reviewed from the registration book. Finally, the case–control incidence density sampling method was used to select the study participants from each facility. Cases (positive visual inspection with acetic acid screens) enrolled consecutively as they were diagnosed to have precancerous cervical lesion until the required sample size was obtained. For each case, three controls (negative visual inspection with acetic acid screens) were selected consecutively from the same health facilities on the same day as soon as the cases were diagnosed (Figure 1).
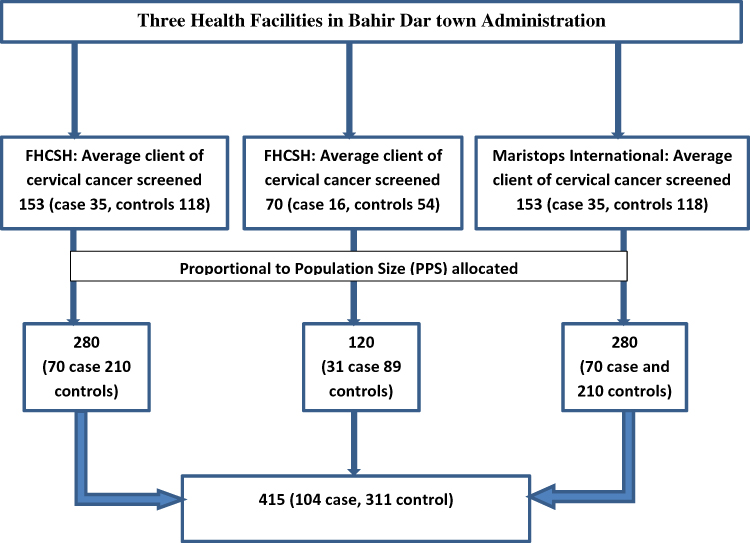 |
Figure 1 Sampling procedure of predictor of precancerous cervical lesions among women screened for cervical cancer in Bahir Dar Town, Ethiopia, 2018/19. |
For cases: women who are age 30–49 and positive VIA findings.
For controls: women who are age 30–49 and negative VIA findings.
For both cases and controls, women who were critically ill and unable to respond during the data collection period were excluded.
Precancerous cervical lesion
Socio-Demographic Descriptive Variables
- Age
- Residence
- Ethnicity
- Marital Status
- Educational status
- Occupation
- Religion
- Income
Reproductive Related Factor
- use of contraception
- History of STI
- Age at menarche
- Early initiation of sexual intercourse
- Lifetime sexual partner
- HIV/AIDS result H IV/AIDS tested
- ART follow up
- Male circumcision
- Abortion
- Number of pregnancy
- Age of first birth
- Number of children
- Family history of cervical cancer
Hygienic Related Factor
- Sharing of underwear
- Genital hygiene practice
Operational/Term Definitions
Case: A participant who had a precancerous lesion if a woman screened positive for VIA finding.6
Control: A participates who had a precancerous lesion if a woman screened negative for VIA finding.6
Multiple sexual partners: A woman who had two or more sexual partners in her lifetime.10
Early Age of sexual intercourse: Initiation of sexual intercourse below the age of 18 years.10
Sharing of underwear: women who sharing their pants from family, friends, and other relatives.10
Genital hygiene practice: vaginal washing practice per day.10
Data Collection Procedures
A structured interviewer-administered questionnaire was prepared by reviewing similar articles. The questionnaire was prepared in English language, then translated to Amharic language and translated back to English to maintain its consistency.
The questionnaire included important issues like; socio-demographic information of the respondents, reproductive health-related variables, and other hygienic related factors.
Three diploma clinical nurse data collectors and one BSc supervisor in the health field were assigned. The data collectors had relatively similar working experience in cancer clinics. They were also had experience in data collection on the same issue in other areas of the country. Training was given for two days on the way of interviewing and filling the questionnaire.
According to the World Health Organization (WHO) guidelines for screening and treatment of precancerous lesions of cervical cancer prevention, the result can be interpreted as positive when an acetowhitish lesion with well-defined margins observed within the vicinity of the transformation zone, on the other hand, if the whole cervix turned white (visual inspection with acetic acid—positive).
The result would be negative when there is no acetowhitish lesion (visual inspection with acetic acid—negative); or suspicious for cancer when there is a visible ulcerative cauliflower-like ulcer, oozing and bleeding on touch. Women with findings of “suspicious” were not included in the study (N=8).
Data Quality Assurance
The questionnaire was pre-tested on 5% of the sample in Debre Markos referral hospital before the actual data collection period. During the data collection, the principal investigator had made close supervision to support data collectors. All the collected data were reviewed by the principal investigator each day. The questionnaire was checked for completeness on a daily basis by the immediate supervisors.
Data Analysis Procedures
Data were entered, cleaned, checked, edited, and coded into Epi Data version 3.1 and analyzed using SPSS version 23 statistical software. Categorical variables were summarized as frequencies and percentages. Bivariate and multivariable logistic regressions were used to determine the association of dependent and independent variables. The statistical significance was declared at p-value <0.05.
Ethics Approval and Consent to Participants
Bahir Dar University, College of Medicine and Health Science, Institutional Review Board with a protocol number of CMHS 0143/18-19 approved the study and ethical clearance was obtained from this office. The study was conducted in accordance with the Declaration of Helsinki. A written letter was given to each health institution from Bahir Dar city administration health office. The respondents were informed about the purpose of the study, and written consent was obtained from the study subjects.
Result
Socio-Demographic Characteristics of Study Participants
A total of 407 women were participated in the current study with a response rate of 98%. The median age of the participants was 38 years ± 11 IQR years. Majority of the ethnicity and religions were Amhara 404 (99.3%) and Orthodox 390 (95.8%) respectively. A higher proportion of study participants 296 (72.7%) were married and 192 (63%) of participants were housewives. Majority of 261 (64.1%) participants had no formal education (Table 2).
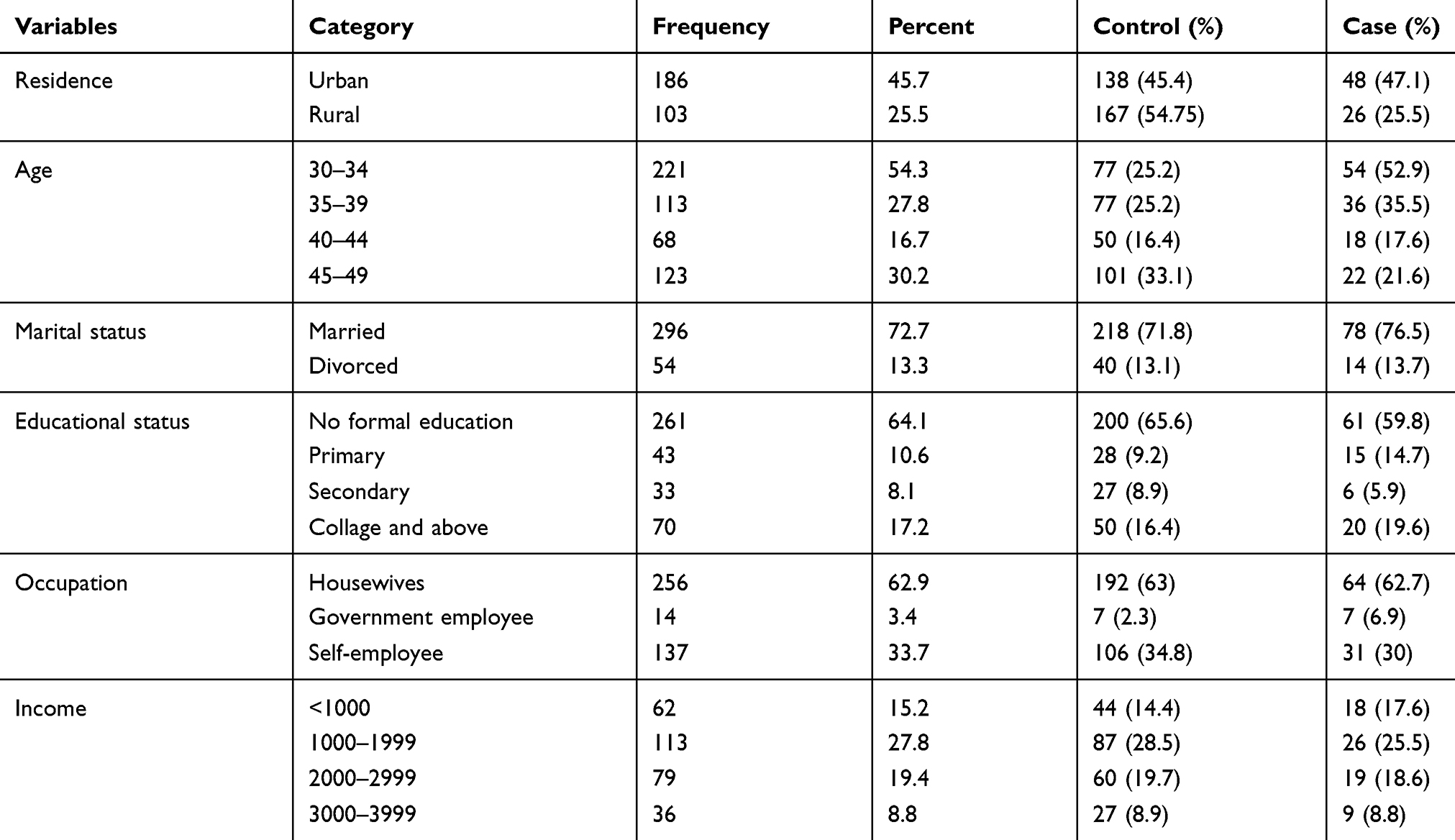 |
Table 2 Socio-Demographic Characteristics of Women Screened for Cervical Cancer in Bahir Dar, Ethiopia, 2018/19 |
Sexual and Reproductive Health-Related Characteristics of Study Participant
The mean age of first sexual intercourse of the women was 16.4 ± 4.1 SD years. Out of the participants more than half of the women 258 (63.4%) had first sexual intercourse below the age of 18 years. Concerning women’s’ sexual history, 235 (57.7%) had two or more sexual partners in their lifetime. About one hundred forty-one (34.6%) of women had a history of sexually transmitted diseases. Out of the participants, only 14 (3.4%) had history of oral contraceptive use for more than five years. Among the total participants 228 (56%) women had 4 and above history of pregnancy and (86%) women had a history of at least one childbirth, and 40.3% of women had a history of abortion. About 119 (29.2%) of participants have had menstruation before 15 years. Concerning participants’ HIV/AIDS status, 61 (14.7%) were positive for HIV and only 3.2% participants had family history of cervical cancer (Table 3).
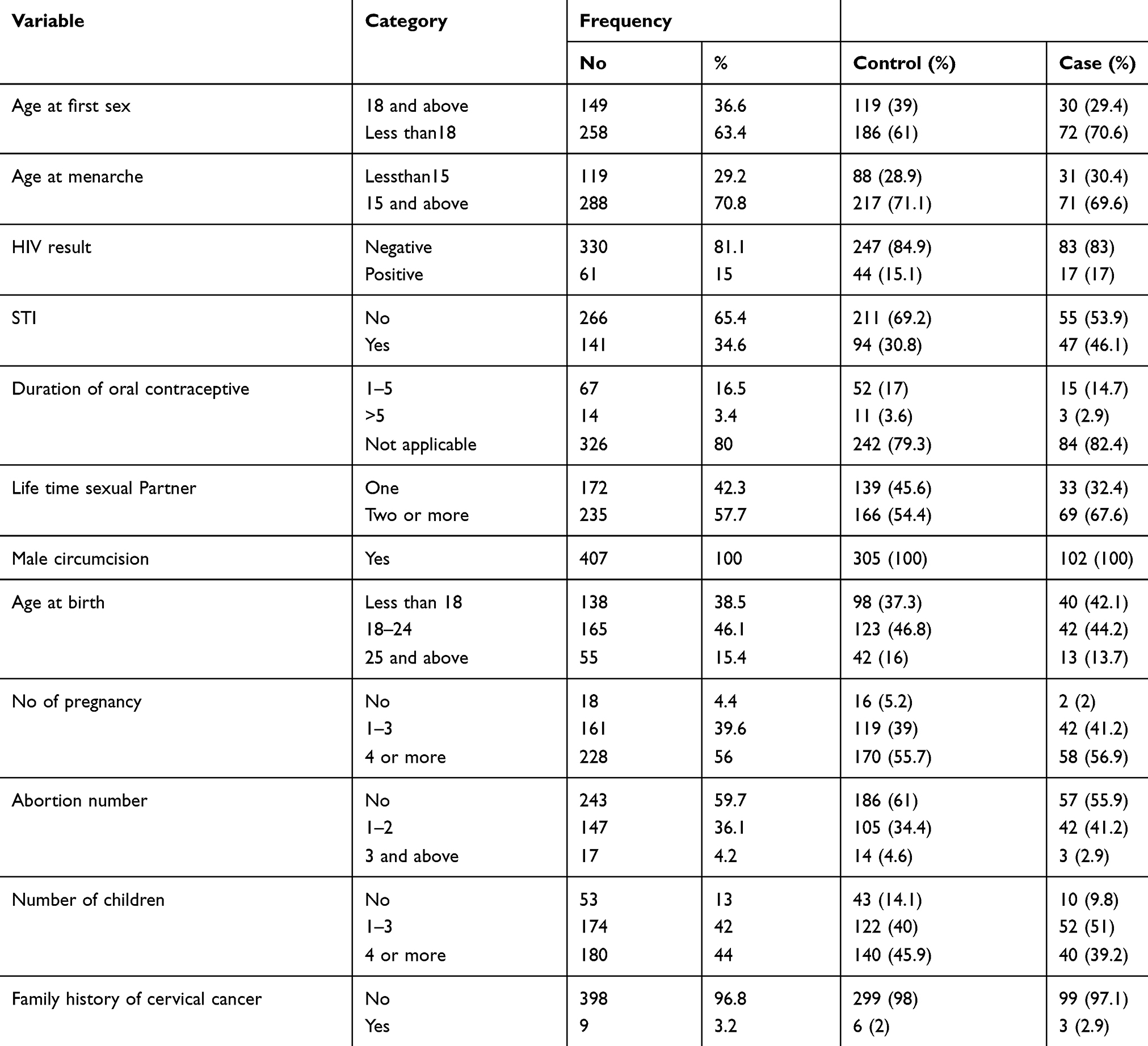 |
Table 3 Sexual and Reproductive Health-Related Character of Women Screened for Cervical Cancer in Bahir Dar, Ethiopia, 2018/19 |
Hygienic Related Characteristics of Study Participants
Among women participated in the study, only 13 (3.2%) women had history of sharing underwear from family, colleges, and relative. Concerning vaginal cleaning, out of the women participated, 375 (92.1%) of women washed or cleaned their vagina two or more times a day (Table 4).
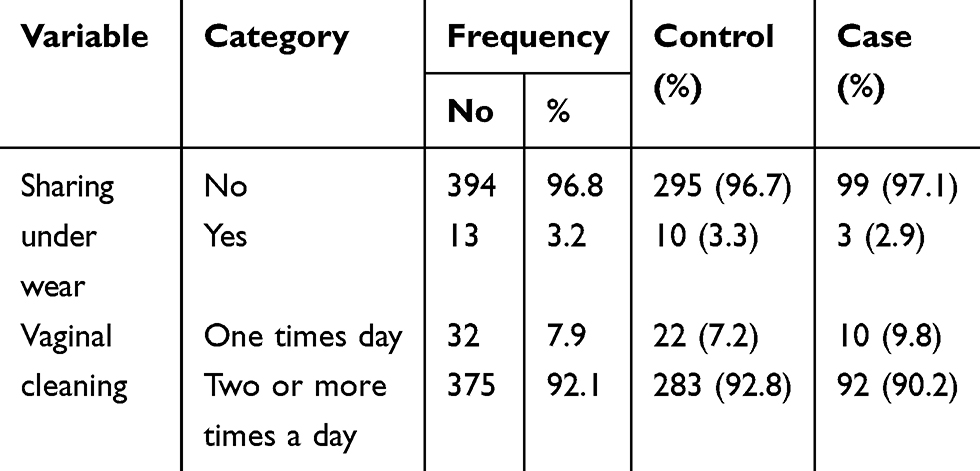 |
Table 4 Hygienic Related Characteristics of Screened Women in Bahir Dar Town, Ethiopia, 2018/19 |
Factors Associated with Precancerous Cervical Lesion
In Bivariable analysis, occupation, age at first sex, history of STIs, lifetime sexual partner, number of children and age of the respondents were found to have a p-value of ≤0.2. To control the effect of other confounding factors they were entered into multivariable logistic analysis. In the multivariable analysis, initiation of sexual intercourse, having a history of STIs and multiple sexual partners were found to be a significant predictor of precancerous cervical lesion in women with precancerous cervical cancer.
Women who had early initiated sexual intercourse before the age of 18 were 1.7 times more likely to have the lesion compared with those who initiated sexual intercourse at the age of 18 years and late (AOR = 1.68: 95% CI [1.02, 2.80]). Women who had history of STIs were 1.74 times more likely to have cervical precancerous lesions than those who had no history of STI (AOR =1.74:95% CI (1.09, 2.8)). Similarly, those having two or more lifetime sexual partners were 1.75 times higher to develop precancerous cervical cancer (AOR=1.75: 95% CI (1.09, 2.81)) (Table 5).
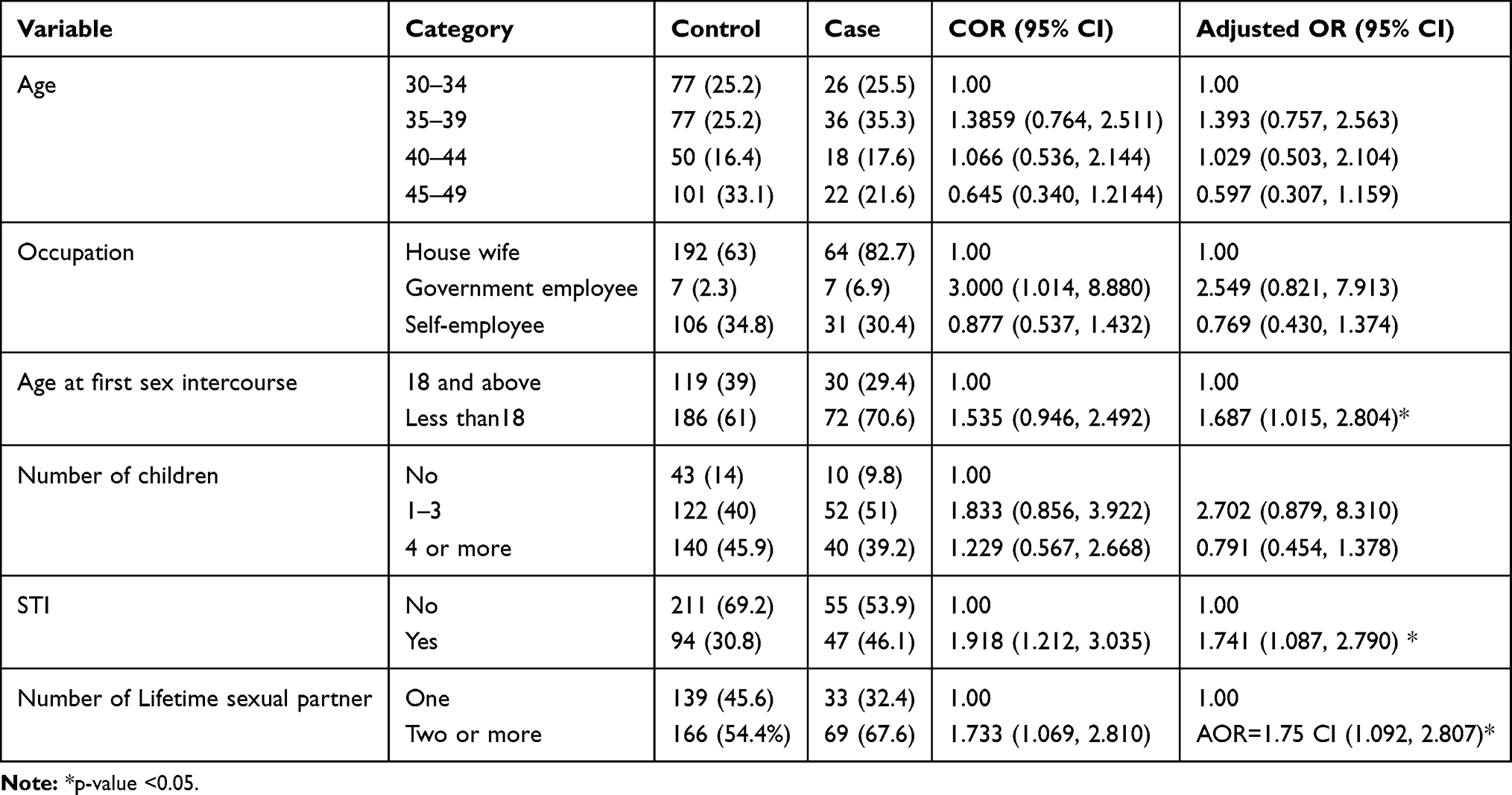 |
Table 5 Multivariate Analysis of Selected Variables Among Study Participants of Bahir Dar, Ethiopia, 2018/19 |
Discussion
This study was intended to identify the predictor of precancerous cervical lesion.
In the current study, women who initiated first sexual intercourse before the age of 18 were at a higher risk for the development of precancerous cervical lesions compared with those who initiated 18 and late.
The finding of this study was consistent with studies done in Yirgalem zonal hospital, Debre Markos hospital and Adama in which women who had a history of early initiation of first sexual intercourse before18 years and less were at higher risk to develop precancerous cervical lesion than those whose age is ≥18 years’ age.16,22,23
The reason behind this may be during puberty, cervical tissue undergoes physiologic changes, transformation zone on the ectocervix becomes enlarged, and becoming exposed to HPV facilitate infection facilitating the development of dysplasia, a cervical squamous precancerous. This was supported by Rodriguez that culmination of transmission of HPV infection usually occurs early in the first year after the start of sexual intercourse. This is due to HPV infection is highly contagious and endemic in women who had sex the first time aged < 17 years 2–3 times the risk for cancer compared with those having sex aged ≥20 years.24
However, the result of this study was different from the study done in Swaziland and Jimma where there was no difference among women who initiated first sexual intercourse early and late age. The possible explanation for the observed difference might be differences in sample size and the type of study design ie this study was case control while a study conducted in Swaziland and Jimma were cross-sectional studies.10,25
This study also showed that women who had a history of sexually transmitted infections were at a higher risk of developing precancerous cervical lesions. This result is comparable with a study done in Jimma, Swaziland and North Ethiopia which revealed that women who had a history of sexually transmitted infection were at a higher risk to develop precancerous cervical lesions than women who had no history of sexually transmitted infection.10,25,26 This might be due to Long-term inflammation caused by sexually transmitted diseases increases the risk of precancerous cervical lesions.
In contrary to this study, the result was different from the study done in Debre Markos and Mekelle hospitals. Sexually transmitted infection was not associated with the risk of precancerous cervical lesion development.16,19 The possible explanation may be the population of Mekelle and Debre Markos were women who had known HIV-positive status. This might protect them from STIs (because of the perceived risk of STIs) due to awareness about opportunistic infection for HIV during follow up.
The current study also showed that women who had more than one-lifetime sexual partners were at a higher risk of developing precancerous cervical lesions than women who had only one-lifetime partner. The finding was comparable with a study conducted in Mekelle, Swaziland, and Yogyakarta that multiple sexual partners were a determinant factor for the development of precancerous cervical lesions.8,25,27 This is because having multiple sexual partners exposes for HPV which increases the risk of developing precancerous cervical lesions. However, another studies done in Zimbabwe and Harare showed that having more than five sexual partners was found to be protective compared to having one sexual partner.28 The difference may be as a result of sample size difference (180) in Zimbabwe compared (407) to the current study.
Conclusion
This study confirmed that initiation of early sexual intercourse before the age of 18 years, having history of sexually transmitted diseases and history of two or more lifetime sexual partners were factors associated with precancerous cervical lesions. So that it should be focused on prevention through early detection and treatment of sexually transmitted infections with condom promotion. Women with a higher risk of precancerous lesions should also be encouraged to be screened more frequently for cervical cancer.
Abbreviations
AOR, Adjusted Odds ratio; CI, Confidence Interval; CMHS, Collage of Medicine and Health Science; FGAE, Family Guidance Association of Ethiopia; FHCSH, Felege Hiwot Compressive Specialized Hospital; HIV, Human Immune Virus; HPV, Human Papilloma Virus; NGO, Non-Governmental Organization; SD, Standard Deviation; SPSS, Statistical Package for Social Science; STI, Sexually Transmitted Infection.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgment
We are very grateful to Bahir Dar University for giving us the ethical clearance to conduct this study. We are also indebted to thank Bahir Dar City Administration Health Office, kebeles administrations, and study participants for their cooperation during data collection.
Author Contributions
JA: conceived the research idea and developed the proposal, participated in data collection and analysis, and drafted the paper. GA and AW: Enriched the concept and proposal write up, participated in data analysis and drafting of the manuscript, and critically reviewed the manuscript. GA: Prepared and critically reviewed the manuscript. Generally, all authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Torre LA, Siegel RL, Ward EM, Jemal A. Global cancer incidence and mortality rates and trends—an update. Cancer Epidemiol Prev Biomarkers. 2016;25(1):16–27. doi:10.1158/1055-9965.EPI-15-0578
2. Arbyn M, Weiderpass E, Bruni L, et al. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. Lancet Glob Health. 2020;8(2):191–203. doi:10.1016/S2214-109X(19)30482-6
3. Getachew E. Knowledge Attitude and Practice on Cervical Cancer and Screening among Reproductive Health Service Clients, Addis Ababa, Ethiopia (Doctoral dissertation), Addis Abeba Universty; 2015.
4. Pathfinder international. Single-Visit Approach to Cervical Cancer Prevention. Clinical Standards of Practice and Counseling Guidelines; May 2012.
5. Shiferaw N, Salvador-Davila G, Kassahun K, et al. The single-visit approach as a cervical cancer prevention strategy among women with HIV in Ethiopia: successes and lessons learned. Glob Health Sci Pract. 2016;4(1):87–98.
6. World Health Organization. WHO guidelines for screening and treatment of precancerous lesions for cervical cancer prevention. Geneva: World Health Organization; 2013. https://www.ncbi.nlm.nih.gov/books/NBK195239/.
7. Tefera F, Mitiku I. Uptake of cervical cancer screening and associated factors among 15–49-year old women in dessie town, northeast Ethiopia. Journal of Cancer Education. 2016. PMID: 27075197. Epub 2016/ 04/15. eng. doi:10.1007/s13187-016-1021-6.
8. Bayu H, Berhe Y, Mulat A, Alemu A. Cervical cancer screening service uptake and associated factors among age eligible women in Mekelle Zone, Northern Ethiopia, 2015: a community based study using health belief model. PLoS One. 2016;11(3):e0149908. PMID: 26963098. Pubmed Central PMCID: PMC4786115. Epub 2016/ 03/11. eng. doi:10.1371/journal.pone.0149908
9. Mitiku I, Tefera F. Knowledge about cervical cancer and associated factors among 15–49-year-old women in Dessie Town, Northeast Ethiopia. PLoS One. 2016;11(9):e0163136. PMID: 27690311. Pubmed Central PMCID: PMC5045174. Epub 2016/ 10/01. eng. doi:10.1371/journal.pone.0163136
10. Bezabih M, Tessema F, Sengi H, Deribew A. Risk factors associated with invasive cervical carcinoma among women attending Jimma University specialized hospital, Southwest Ethiopia: a case-control study. Ethiop J Health Sci. 2015;25(4):345–352. PMID: 26949299. Pubmed Central PMCID: PMC4762973. Epub 2016/ 03/08. Eng. doi:10.4314/ejhs.v25i4.8
11. Belete N, Tsige Y, Mellie H. Willingness and acceptability of cervical cancer screening among women living with HIV/AIDS in Addis Ababa, Ethiopia: a cross-sectional study. Gynecol Oncol Res Pract. 2015;2:6. PMID: 27231566. Pubmed Central PMCID: PMC4881166. Epub 2015/ 01/01. eng. doi:10.1186/s40661-015-0012-3
12. Getahun F, Mazengia F, Abuhay M, Birhanu Z. Comprehensive knowledge about cervical cancer is low among women in Northwest Ethiopia. BMC Cancer. 2013;13:2. PMID: 23282173. Pubmed Central PMCID: PMC3559275. Epub 2013/ 01/04. eng. doi:10.1186/1471-2407-13-2
13. Dulla D, Daka D, Wakgari N. Knowledge about cervical cancer screening and its practice among female health care workers in southern Ethiopia: a cross-sectional study. Int J Women’s Health. 2017;9:365–372. PMID: 28579837. Pubmed Central PMCID: PMC5446960. Epub 2017/ 06/06. eng. doi:10.2147/IJWH.S132202
14. Teame H, Addissie A, Ayele W, et al. Factors associated with cervical precancerous lesions among women screened for cervical cancer in Addis Ababa, Ethiopia: a case-control study. PLoS One. 2018;13(1):e0191506. doi:10.1371/journal.pone.0191506
15. Wondimu YT. Cervical cancer: assessment of diagnosis and treatment facilities in public health institutions in Addis Ababa, Ethiopia. Ethiop Med J. 2015;53(2):65–74. PMID: 26591294. Epub 2015/ 11/26. Eng.
16. Getinet M, Gelaw B, Sisay A, Mahmoud EA, Assefa A. Prevalence and predictors of Pap smear cervical epithelial cell abnormality among HIV-positive and negative women attending gynecological examination in cervical cancer screening center at Debre Markos referral hospital, East Gojjam, Northwest Ethiopia. BMC Clin Pathol. 2015;15(1):16. doi:10.1186/s12907-015-0016-2
17. Gedefaw A, Astatkie A, Tessema GA. The prevalence of precancerous cervical cancer lesion among HIV-infected women in southern Ethiopia: a cross-sectional study. PLoS One. 2013;8(12):e84519. doi:10.1371/journal.pone.0084519
18. Leyh-Bannurah SR, Prugger C, de Koning MN, Goette H, Lellé RJ. Cervical human papillomavirus prevalence and genotype distribution among hybrid capture 2 positive women 15 to 64 years of age in the Gurage zone, rural Ethiopia. Infect Agent Cancer. 2014;9(1):33. doi:10.1186/1750-9378-9-33
19. Gessesse Z, Tadesse Z, Alemayehu M, et al. Determinant factors of Visual Inspection with Acetic Acid (VIA) positive lesions among HIV positive women in Mekelle Hospital, Northern Ethiopia: a case control study. EMJ. 2015;1:17–24.
20. Federal Democratic Republic of Ethiopia Ministry of Health. Health Sector Development Programme IV 2010/11–2014/15, final draft; 2010.
21. Bahir dar city administration bureau of finance and economic development annual report in Amhara region, Ethiopia; 2017.
22. Kassa RT. Risk factors associated with precancerous cervical lesion among women screened at Marie Stops Ethiopia, Adama town, Ethiopia: a case-control study. BMC Res Notes. 2018;11(1):145. doi:10.1186/s13104-018-3244-6
23. T YB H, Aschenaki H, Mamaye E, et al. Prevalence of cervical cancer and associated risk factors among women attending cervical cancer screening and diagnosis center at Yirgalem General Hospital, Southern Ethiopia. J Cancer Sci Ther. 2017;9:730–735.
24. Rodriguez RP, Morelos PR, Ruiz VV, et al. Prevalence of human papillomavirus in the cervical epithelium of Mexican women: meta-analysis. Infect Agent Cancer. 2012;7(34):1–8. doi:10.1186/1750-9378-7-1
25. Jolly PE, Mthethwa-Hleta S, Padilla LA, et al. Screening, prevalence, and risk factors for cervical lesions among HIV positive and HIV negative women in Swaziland. BMC Public Health. 2017;17(1):218. doi:10.1186/s12889-017-4120-3
26. Misgina KH, Belay HS, Abraha TH. Prevalence of precancerous cervical lesion and associated factors among women in North Ethiopia. J Public Health Epidemiol. 2017;9(3):46–50. doi:10.5897/JPHE2016.0891
27. Sari HE, Mudigdo A, Demartoto A. Multilevel analysis on the social determinants of cervical cancer in Yogyakarta. J Epidemiol Public Health. 2016;1(2):100–120. doi:10.26911/jepublichealth.2016.01.02.03
28. Vere M. Risk factors for cervical precancerous lesions among women attending cervical cancer screening clinics in Harare. 2013.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.