")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Predictors of Outcome in Juvenile Myoclonic Epilepsy
Authors Chen Y , Chen J, Chen X, Wang R, Zeng J, Wang F, Miao J
Received 4 January 2020
Accepted for publication 12 May 2020
Published 19 June 2020 Volume 2020:13 Pages 609—613
DOI https://doi.org/10.2147/RMHP.S244725
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kent Rondeau
Yiqian Chen,1,* Jingzhen Chen,1,* Xingyu Chen,1,* Ru Wang,2 Jianqi Zeng,1 Feng Wang,3 Jiayin Miao1
1Department of Neurology, Zhongshan Hospital, Xiamen University, Xiamen 361004, People’s Republic of China; 2Department of Neurology, Weinan Central Hospital, Weinan 714000, People’s Republic of China; 3School of Computer Engineering, Jimei University, Xiamen 361021, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiayin Miao
Department of Neurology, Zhongshan Hospital, Xiamen University, Xiamen 361004, People’s Republic of China
Tel +86-15880281527
Fax +86 592-2212328
Email [email protected]
Background: Juvenile myoclonic epilepsy (JME) is the most common idiopathic generalized epilepsy syndrome, accounting for 10% of all epilepsy. However, there is limited information regarding the predictors of seizure outcome. The aim of this study was to determine the predictors of seizure outcome in JME patients.
Methods: A population-based retrospective study of JME patients who were treated at the Department of Neurology of affiliated Zhongshan Hospital, Xiamen University from 2008 to 2013.
Results: Sixty-three patients (30 women and 33 men) were enrolled in this study. The median age at seizure onset was 14 years old, and the average duration of epilepsy was 5 years. The onset of JME at age < 16 years was found in 63.5% of patients. The epileptiform runs ≥ 3 s were observed in 35.8% patients. Febrile seizure was noted in 28.9% of patients. Among 63 patients, 40 patients (63.5%) had remission. Multivariate analysis identified the following factors as significant predictors of seizure outcome: the onset of JME at age < 16 years, epileptiform runs ≥ 3 s runs, and febrile seizure.
Conclusion: The onset of JME at age < 16 years, febrile seizures and epileptiform runs ≥ 3 s might be associated with poor long-term seizure outcome in patients with JME.
Keywords: juvenile myoclonic epilepsy, seizure, predictor, outcome
Introduction
Juvenile myoclonic epilepsy (JME) is a type of idiopathic generalized epilepsy that usually occurs during adolescence. The leading symptom is early-morning myoclonic seizures (MS) alone or combined with generalized tonic-clonic seizures (GTCS) or absence seizures (AS).1,2 The interictal electroencephalography (EEG) shows generalized poly-spike waves at 4–6 Hz, and photosensitivity was noted in 30% of cases.3,4
Although the majority of JME patients can be controlled under appropriate treatment, JME has a high risk of relapse after the withdrawal of antiepileptic drugs (AEDS).5–7 A few studies focused on long-term seizure outcome of JME have shown that some patients are able to remain seizure free without AED medication.8–13 However, little is known about the predictors of seizure outcomes. It is difficult to predict who will develop refractory epilepsy in the early stages of the JME. Therefore, this study aimed to identify prognostic factors that can be predictive for seizure outcome in JME patients.
Materials and Methods
Subjects
This is a single-center retrospective study approved by the Ethics Committee of Zhongshan Hospital in accordance with the Declaration of Helsinki. All patients provided written informed consent. All data were collected from JME patients diagnosed at the department of neurology, out-patient department, affiliated Zhongshan hospital, Xiamen University China from 2008 to 2013. JME was diagnosed based on clinical history and EEG studies.
Inclusion criteria were: a diagnosis of JME on the basis of International League against Epilepsy (ILAE);14 patients who received medication in our outpatient department. Exclusion criteria were: the presence of focal neurological or intellectual impairment; abnormal brain imaging of CT or MRI; secondary to cerebral hypoxia, metabolic diseases or degenerative diseases.
Evaluation
We reviewed retrospectively the medical records of 63 patients and obtained data from the records included age, age at seizure onset, gender, family history of epilepsy, duration of epilepsy febrile seizure, EEG findings and seizure type. The international 10–20 system for electrode placement was used in all the EEG studies. Seizure outcomes were evaluated by clinic visits or telephone interview and divided into two categories: at the last follow-up, no seizures for more than 5 years defined as remission, while the remaining patients were defined as no remission.
Statistical Analysis
Data analysis was performed by using SPSS version 24. T-test was used for continuous variables. Pearson chi-square and Fisher exact test were used for classified variables. Multivariate logistic regression was carried out to identify the predictors of seizure outcome. Odds ratios and 95% confidence intervals were calculated. P-value < 0.05 was considered statistically significant.
Results
General Information of the Subjects
In this retrospective study, we analyzed 63 patients. The mean age was 20.4±6.9 years. The mean age of onset of epilepsy was 14.63±3.8 years. Five (7.9%) patients had a positive family history of epilepsy, and febrile seizures were noted in 9 patients (14.2%). There was a significant difference in the onset of JME at age <16 years of JME between the remission and no remission group (P = 0.017< 0.05) (Table 1).
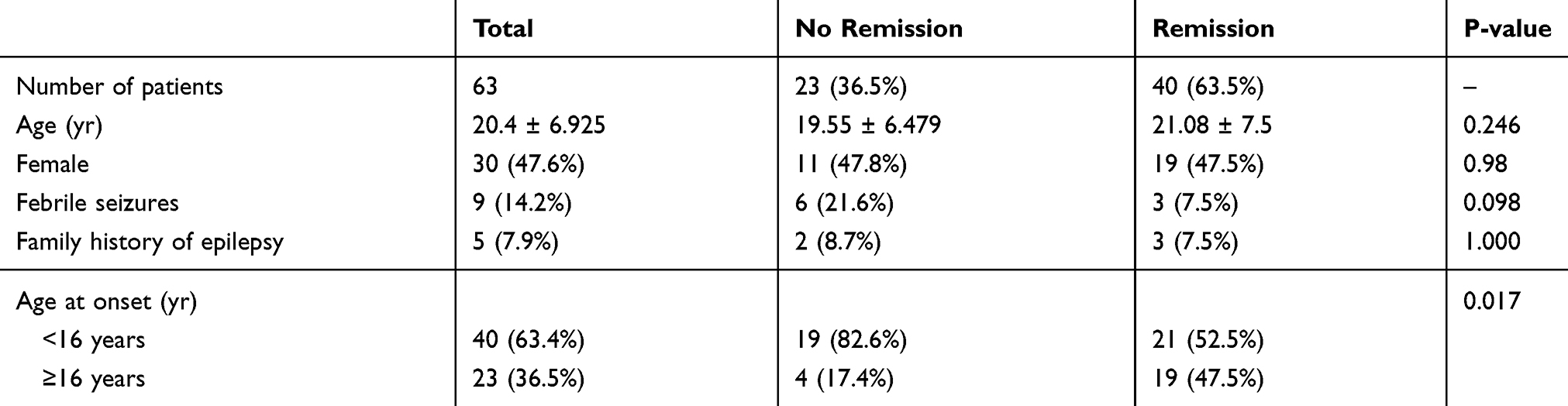 |
Table 1 Basic Information of the Patients in Two Groups |
MS was noted in all the patients; 57 (90.4%) had GTCS, 10 (15.8%) had AS. Sixteen patients (25.5%) had seizure predisposing factors, which included visual stimulation and fatigue. 22 (34.9%) had seizures on awakening, and 5 (7.9%) had seizures (GTCS) only in sleep, while 36 (57.1%) had seizures both while asleep and awake (Table 2).
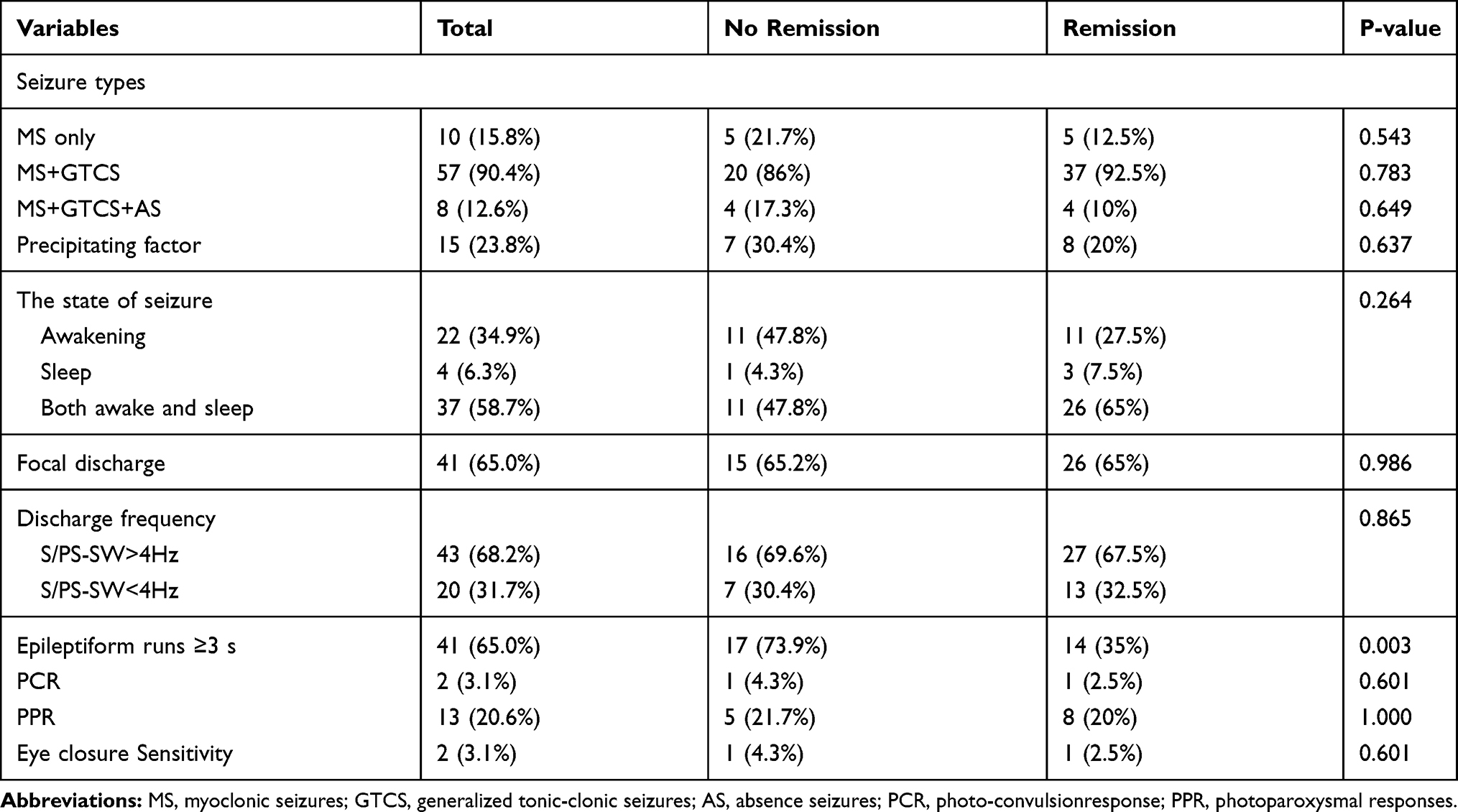 |
Table 2 Clinical and EEG Data of the Patients in Two Groups |
The focal discharge was shown in 41 patients (65%). The frequency was fast (>4 HZ) in 46 patients (68.2.5%) and slow (<4 Hz) in 39 patients (14.7%). Photoparoxysmal response (PPR) was positive in 13 patients (20.6%). Photo convulsion response (PCR) was shown in 2 patients (3.1%) and eye closure sensitivity was seen in 2 patients (3%) (Table 2).
The epileptiform runs ≥3 s was seen in 17 patients (73.9%) in the no remission group, compared to 14 patients (35.0%) in the remission group (P=0.002<0.05, Table 2).
Predictors of Patent Outcome
To identify potential predictors of patient outcome, we performed multivariate logistic regression analysis. The results showed that significant predictors of adverse seizure outcome included epileptiform runs ≥3 s, febrile seizure and the age of onset <16 years (Table 3).
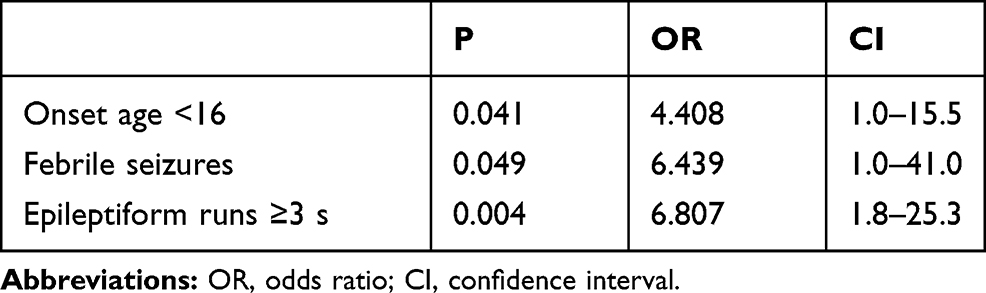 |
Table 3 Independent Risk Factors for No Remission |
Discussion
In this study, we identified several predictor factors of outcome in JME patients based on a retrospective analysis of 63 patients admitted in a single center. First, the onset age of JME <16 years was associated with adverse epilepsy outcomes. We selected the age of onset at 16 years as the predictive variable because epilepsy over 16 years of age is defined as adult epilepsy.15 The mean age of onset of JME was 14.6, which was similar to the previously reported mean age of 14.3.11 A previous study showed that the younger onset age of seizure, the higher the correlation with more severe intellectual impairment and biological behavior conditions.16 The age of onset of seizure may point to a particular disease or cause. Two studies found that younger age of onset of JME was more likely to associate with persistent seizures in JME, which may be related to the insensitivity of younger age to AED treatment.17,18 However, two long-term studies suggested that the onset age of JME was unrelated to the seizure outcome of JEM epilepsy.11,12 The different results may be explained by different research methods, follow-up time and sample size.
In addition, we found that patients with epileptiform runs ≥3 s were more likely to remission. Our results indicated that epileptiform runs ≥3 s epileptiform runs were negative predictors of seizure outcome, consistent with previous studies.19,20 In this study, epileptiform runs ≥3 s was observed in 50% of JME patients, different from epileptiform runs ≥3 s noted in 30% of JME patients in another study.20 The difference may be that we performed all 24 hrs EEG, making it easier to detect abnormalities.
Furthermore, our results showed that febrile seizure was related to adverse outcomes in JME patients. A small number of patients with febrile convulsions may subsequently develop epilepsy.21,22 Factors affecting the incidence of epilepsy following febrile seizure include neurological and developmental abnormalities, and the severity of initial febrile seizure. One study reported that prolonged febrile seizure was associated with intractable epilepsy.23 Another study showed that prolonged febrile seizure may damage hippocampal, which led to temporal lobe epilepsy.24 We speculated two possible reasons for the association between febrile epilepsy and prognosis of epilepsy. First, the risk factors of epilepsy after febrile seizures may also be the risk factors of adverse epilepsy outcomes. Second, prolonged febrile seizures may damage the brain with the consequent potential for adverse seizure outcome.
We found that the seizure outcome had no association with the seizure type. These results are different with some studies which suggest that MS+GTCS, MS+GTCS+AS, AS are related to seizure outcome,11,12,17 but are consistent with the results of other studies.9,10 Possible explanation for the controversy may be related to the small sample size and different study approaches. In addition, we found no significant association between PPR and long-term seizure outcome, consistent with previous studies.11,12
This study has several limitations. The major limitation is single-center retrospective study. Second, the sample size is relatively small. In addition, the family history of epilepsy is very low, which may be due to small sample size of this study. Furthermore, we did not evaluate the role of AED or perform formal psychiatric assessment. Therefore, large multicenter cohort studies are needed to support our findings.
In summary, we found that predictors of JME outcome included onset age <16 years, epileptiform runs ≥3 s, and febrile seizure. These findings help clinicians manage patients with JME and improve long-term outcome.
Acknowledgments
This study was funded by grants from the National Natural Science Foundation (No. 81400984) and the Natural Science Foundation of Fujian Province (No. 2014D009).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Janz D. Epilepsy with impulsive petit mal (juvenile myoclonic epilepsy). Acta Neurol Scand. 1985;72(5):449–459. doi:10.1111/j.1600-0404.1985.tb00900.x
2. Ke M, Cao L, Liu G. Model for cascading failures in functional networks: application to epileptic patients with generalized tonic-clonic seizures. J Integr Neurosci. 2019;18(2):133–139.
3. Proposal for revised classification of epilepsies and epileptic syndromes. Commission on classification and terminology of the international league against epilepsy. Epilepsia. 1989;30(4):389–399. doi:10.1111/j.1528-1157.1989.tb05316.x
4. Genton P, Thomas P, Kasteleijn-NolstTrenite DG, Medina MT, Salas-Puig J. Clinical aspects of juvenile myoclonic epilepsy. Epilepsy Behav. 2013;28(Suppl 1):S8–S14. doi:10.1016/j.yebeh.2012.10.034
5. Shinnar S, Berg AT, Moshe SL, et al. Discontinuing antiepileptic drugs in children with epilepsy: a prospective study. Ann Neurol. 1994;35(5):534–545. doi:10.1002/ana.410350506
6. Calleja S, Salas-Puig J, Ribacoba R, Lahoz CH. Evolution of juvenile myoclonic epilepsy treated from the outset with sodium valproate. Seizure. 2001;10(6):424–427. doi:10.1016/S1059-1311(00)90530-2
7. Martinez-Juarez IE, Alonso ME, Medina MT, et al. Juvenile myoclonic epilepsy subsyndromes: family studies and long-term follow-up. Brain. 2006;129(Pt 5):1269–1280. doi:10.1093/brain/awl048
8. Baykan B, Altindag EA, Bebek N, et al. Myoclonic seizures subside in the fourth decade in juvenile myoclonic epilepsy. Neurology. 2008;70(22 Pt 2):2123–2129. doi:10.1212/01.wnl.0000313148.34629.1d
9. Camfield CS, Camfield PR. Juvenile myoclonic epilepsy 25 years after seizure onset: a population-based study. Neurology. 2009;73(13):1041–1045. doi:10.1212/WNL.0b013e3181b9c86f
10. Geithner J, Schneider F, Wang Z, et al. Predictors for long-term seizure outcome in juvenile myoclonic epilepsy: 25–63 years of follow-up. Epilepsia. 2012;53(8):1379–1386. doi:10.1111/j.1528-1167.2012.03526.x
11. Senf P, Schmitz B, Holtkamp M, Janz D. Prognosis of juvenile myoclonic epilepsy 45 years after onset: seizure outcome and predictors. Neurology. 2013;81(24):2128–2133. doi:10.1212/01.wnl.0000437303.36064.f8
12. Hofler J, Unterberger I, Dobesberger J, Kuchukhidze G, Walser G, Trinka E. Seizure outcome in 175 patients with juvenile myoclonic epilepsy-a long-term observational study. Epilepsy Res. 2014;108(10):1817–1824. doi:10.1016/j.eplepsyres.2014.09.008
13. Baykan B, Martinez-Juarez IE, Altindag EA, Camfield CS, Camfield PR. Lifetime prognosis of juvenile myoclonic epilepsy. Epilepsy Behav. 2013;28(Suppl 1):S18–S24. doi:10.1016/j.yebeh.2012.06.036
14. Engel J
15. Wagner AL. A clinical and epidemiological study of adult patients with epilepsy. Acta Neurol Scand Suppl. 1983;94:63–72.
16. Manor L, Streiner DL, Yam WK, et al. Age-related variables in childhood epilepsy: how do they relate to each other and to quality of life? Epilepsy Behav. 2013;26(1):71–74. doi:10.1016/j.yebeh.2012.10.024
17. Guaranha MS, Filho GM, Lin K, Guilhoto LM, Caboclo LO, Yacubian EM. Prognosis of juvenile myoclonic epilepsy is related to endophenotypes. Seizure. 2011;20(1):42–48. doi:10.1016/j.seizure.2010.10.004
18. Ollivier ML, Dubois MF, Krajinovic M, Cossette P, Carmant L. Risk factors for valproic acid resistance in childhood absence epilepsy. Seizure. 2009;18(10):690–694. doi:10.1016/j.seizure.2009.09.007
19. Seneviratne U, Boston RC, Cook M, D’Souza W. EEG correlates of seizure freedom in genetic generalized epilepsies. Neurol Clin Pract. 2017;7(1):35–44. doi:10.1212/CPJ.0000000000000323
20. Arntsen V, Sand T, Syvertsen MR, Brodtkorb E. Prolonged epileptiform EEG runs are associated with persistent seizures in juvenile myoclonic epilepsy. Epilepsy Res. 2017;134:26–32. doi:10.1016/j.eplepsyres.2017.05.003
21. Dube CM, Brewster AL, Baram TZ. Febrile seizures: mechanisms and relationship to epilepsy. Brain Dev. 2009;31(5):366–371. doi:10.1016/j.braindev.2008.11.010
22. Sapir D, Leitner Y, Harel S, Kramer U. Unprovoked seizures after complex febrile convulsions. Brain Dev. 2000;22(8):484–486. doi:10.1016/S0387-7604(00)00187-X
23. Camfield P, Camfield C, Gordon K, Dooley J. What types of epilepsy are preceded by febrile seizures? A population-based study of children. Dev Med Child Neurol. 1994;36(10):887–892. doi:10.1111/j.1469-8749.1994.tb11779.x
24. Scott RC, King MD, Gadian DG, Neville BG, Connelly A. Hippocampal abnormalities after prolonged febrile convulsion: a longitudinal MRI study. Brain. 2003;126(Pt 11):2551–2557. doi:10.1093/brain/awg262
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.