")
Back to Journals » Open Access Journal of Contraception » Volume 7
Predictors of non-use of intrauterine contraception among women aged 18–49 years in a general practice setting in the UK
Authors Walker SH , Newton VL, Hoggart L, Parker MJ
Received 11 July 2016
Accepted for publication 11 September 2016
Published 21 October 2016 Volume 2016:7 Pages 155—160
DOI https://doi.org/10.2147/OAJC.S116994
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Igal Wolman
Video abstract presented by Susan H Walker.
Views: 131
Susan H Walker,1 Victoria L Newton,2 Lesley Hoggart,3 Mike J Parker4
1Faculty of Health, Social Care & Education, Anglia Ruskin University, Chelmsford, 2Faculty of Health & Social Care, The Open University, Milton Keynes, 3School of Health, Wellbeing and Social Care, The Open University, Milton Keynes, 4Postgraduate Medical Institute, Anglia Ruskin University, Chelmsford, UK
Objectives: Our research examined the barriers to the uptake of intrauterine contraception (IUC) by women in a general practice (GP) setting in the UK. This study reports predictors of non-use of IUC in this context.
Design: We used a mixed method Qual/Quant approach in which the initial qualitative research provides a framework for subsequent larger quantitative surveys. Utilizing findings derived from 30 qualitative interviews, a quantitative survey was developed and distributed to a pragmatic sample of 1,195 women, aged 18–49 years, who were recruited through 32 participating GP practices in an area of England, UK. Outcome measures were percentage of attributes or responses in the sample and use or non-use of IUC. Results were analyzed using descriptive statistical analysis and binary logistic regression, using use/non-use as a binary response variable.
Results: Attitudinal variables, which were the strongest predictors of non-use of IUC, were an adverse opinion on long-acting aspect of IUC (odds ratio [OR]=8.34), disliking the thought of IUC inside the body (OR=3.138), concerns about IUC causing difficulties becoming pregnant in the future (OR=2.587), concerns about womb damage (OR=2.224), having heard adverse opinions about levonorgestrel-releasing intrauterine system (Mirena®) (OR=2.551), having an adverse opinion of having light, irregular periods (OR=2.382) and, having an adverse opinion of having no periods (OR=2.018).
Conclusion: Concerns about the long-acting nature of IUC and persisting concerns about the safety of IUC may act as barriers to its use. Information for women, tailored to specifically address these concerns, is needed.
Implications: Clinicians should provide more reassurance and information to potential users of IUC to increase their confidence about the possibility of removing IUC early or on request. They should also specifically seek to alleviate concerns about internal damage, damage to the womb, or damage to future fertility from using the methods.
Keywords: intrauterine device, intrauterine contraception, intrauterine system, general practice, UK
Introduction
Intrauterine contraception (IUC) is safe, highly effective and, as with all methods of contraception, available free to women in the UK. Long-acting reversible contraceptive (LARC) methods are recommended by the UK National Institute of Clinical Excellence (NICE) because of their cost-effectiveness and potential to reduce the numbers of unplanned and unwanted pregnancies.1 Despite its effectiveness, of those women attending UK community contraceptive clinics in 2014–2015, only 9% were using IUC (4% were using an intrauterine device [IUD] and 5% using an intrauterine system [IUS]).2 Accurate data on IUC provided by general practice (GP) in the UK are hard to obtain and no national survey of contraceptive use has been carried out since 2008–2009, when 8% of 15- to 49-year-old reported using an IUC.3 LARC prescription rate to women aged 15–44 years in GP (excluding the contraceptive injection but including contraceptive implants and IUC) was 50/1,000 women/year in 2014.4
To explore possible reasons for the low use of IUC in a GP setting, we examined the views on IUC of women aged 18–49 years, attending GP practices in a region of England.
Methods
Ethical approval for this project was obtained from NRES Committee London South East (14/LO/0004).
We used a mixed method Qual/Quant approach in which the initial qualitative research provides a structure for subsequent larger quantitative surveys. Sequential mixed methods are increasingly used in health care settings, where qualitative findings are drawn on to devise quantitative surveys, whose data can help to indicate how prevalent the qualitative findings are in a wider population (Qual/Quant).5
Study design and development of survey instrument
Patients were invited to take part in the study through their GP practices. First, 30 women from 7 practices gave written, or audio-recorded, informed consent to take part in the qualitative interviews. Interviews explored knowledge about, and attitudes toward, IUC, including whether it had been considered as a method. Only never users of IUC were recruited in this arm. The qualitative data were analyzed thematically.6 First, the transcripts were read and reread by two independent researchers to ensure familiarity with the data. A coding frame was then devised and refined through discussion. The transcripts were broad coded into themes. Each emerging theme was then fine coded. To ensure rigor, the researchers compared their interpretation of the data at a number of stages throughout the process to ensure that findings were firmly grounded in what the research participants themselves had to say.
To help facilitate analysis, the researchers utilized the data management software package NVivo (QSR International Pty Ltd, Doncaster, Australia). The broad themes arising from the qualitative analysis, which informed the quantitative survey, were lack of knowledge about IUC, accounts of friends and family, concerns about fitting and removal, concerns about the hormonal component of levonorgestrel-releasing IUS (LNG-IUS), concerns about effects of IUC on the menstrual cycle, concerns about the devices moving, falling out or being felt during sex, the need to arrange for a clinician to stop or start the methods, having a device inside the body, concerns about the long-term nature of IUC, and concerns about the effects of IUC on the body and fertility.
A quantitative survey, incorporating these themes, was subsequently distributed to women (users and non-users) within participating GPs (Supplementary material). The survey asked for demographic data, opinions, experiences and knowledge of IUC, current contraceptive method and level of agreement, using a discrete visual analog scale (VAS), with statements of concern about IUC, which were derived from the qualitative interviews. There was also a free-text box in which respondents were asked to state their main reason (if any) for not using IUC. The survey was piloted before use with two separate groups of students (undergraduate and postgraduate) in a higher educational establishment, and wording of the items was altered according to their feedback on acceptability and clarity. The survey was administered in English and took about 10–15 minutes to complete.
Survey sample
All women between the ages of 18 and 49 years, attending 32 selected GP premises between February and August 2015, were eligible to take part in the subsequent quantitative survey, regardless of their reason for attending or contraceptive history. A sample size calculation showed that a minimum of 1,068 respondents was required to be able to estimate, with a 95% confidence interval (CI) half-length of 3%, the percentages of attributes or responses in the target population, when the true percentage was 50%, the case with the largest variance.
Of 4,300 questionnaires distributed, 1,244 questionnaires were returned, indicating a response rate of 28.9%. Removing blank questionnaires and respondents who were outside the intended age range (18–49 years) resulted in 1,195 responses for analysis, which exceeded our intended target.
Statistical analysis
Quantitative analysis was carried out using both SPSS and “R” software.7 We used descriptive statistics to summarize the knowledge of IUC and demographic characteristics and Student’s t-tests or Fisher’s exact test to compare these characteristics between users and non-users of IUC. Binary logistic regression models were fitted to relate current non-use of IUC to each variable in a set of 26 variables in single-predictor models and binary logistic regression performed using Firth’s penalized maximum likelihood estimation provided by function logistf from R package logistf.8
Taking use/non-use of IUC (both copper IUD and IUS) as a binary response variable in single-predictor binary logistic models, we looked at which attitudinal or demographic variables appeared to predict non-use. The responses to the attitudinal statements were recoded so that a response suggesting a greater likelihood of non-use scored more highly. For example, “It puts me off a lot” was coded to score highest, whereas “It attracts me a lot” was coded to score lowest. The results are presented as odds ratios (ORs), which represent a greater or lesser likelihood of non-use with every increment along the discrete VAS.
Missing responses and “do not know” responses have been omitted from the analysis that is presented in Table 1.
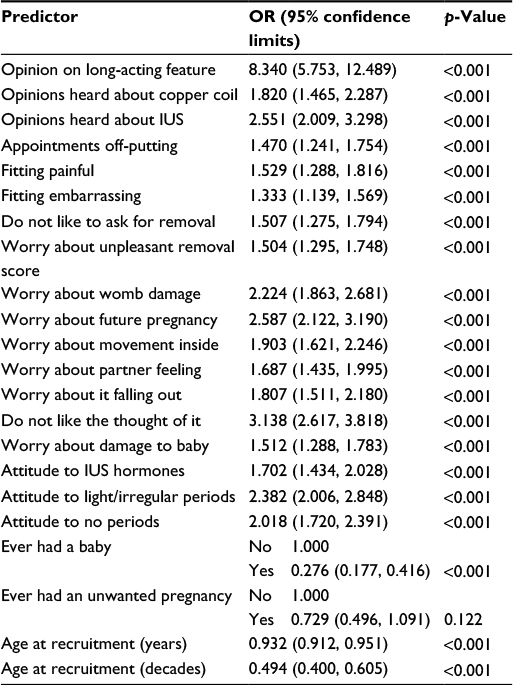 | Table 1 Predictors of non-use of IUC in single-predictor binary logistic models Abbreviations: IUC, intrauterine contraception; OR, odds ratio; IUS, intrauterine system. |
Results
Sample characteristics
The mean age of the 1,195 respondents was 33.9 years; 79.8% self-identified as White British. The majority of respondents were parous (58.5%) and had never experienced an unwanted pregnancy (75.6%).
Use of IUC in a UK GP setting
Of our sample, 26.1% reported ever having used IUC: 17.1% had used LNG-IUS, 5.7% had used a copper IUD, and 1.6% had used both.
When asked about current use, 10.5% reported using a LNG-IUS and 2.6% a copper IUD. The most common current contraceptive method was the combined oral contraceptive pill (Figure 1).
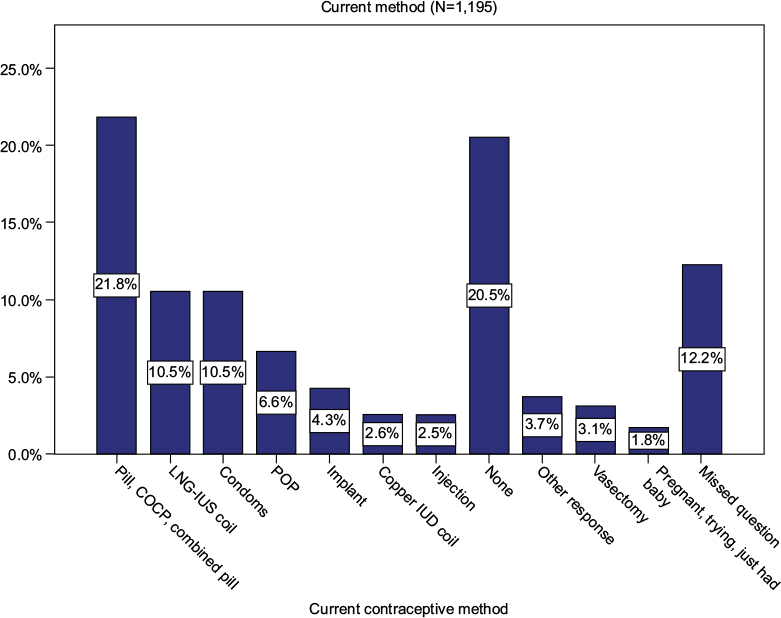 | Figure 1 Current contraceptive use. Abbreviations: COCP, combined oral contraceptive pill; LNG-IUS, levonorgestrel-releasing intrauterine system; POP, progestogen-only pill; IUD, intrauterine device. |
Knowledge of IUC
A total of 45.3% reported knowing “a lot” (10.3%) or “some” (35%) about IUC, whereas 25.3% knew “a little” and 26.6% “almost nothing”.
Demographic variables vs user/non-user
Nulliparity was statistically significantly associated with being a non-user, and parous women reported being current IUC users in greater numbers than nulliparous women (p<0.001). Of the current users, 82.7% reported having had a baby compared to 56.3% of non-users. In a largely White British sample, neither ethnicity (p=0.897) nor a history of unplanned pregnancy (p=0.134) was statistically significantly associated with being a current non-user. The mean age of users (38.3 years) was statistically significantly higher than the mean age of non-users (33.1 years) (t=7.487, p<0.001). For age at recruitment to the survey (years), the odds in favor of non-use is reduced by 6.8% as age increases by 1 year (OR=0.932 [CI=0.912, 0.951], p<0.001).
Predictors of non-use of IUC
Attitudinal variables increasing the odds of being a non-user by >2 for each increment along a discrete VAS were
- An adverse opinion on long-acting aspect of IUC (OR=8.34);
- Disliking the thought of IUC inside the body (OR=3.138);
- Concerns about IUC causing difficulties becoming pregnant in the future (OR=2.587);
- Concerns about womb damage (OR=2.224);
- Having heard adverse opinions about LNG-IUS (OR=2.551);
- Adverse opinion on having light, irregular periods (OR=2.382);
- Adverse opinion on having no periods (OR=2.018).
Concerns about unpleasant fitting and removal, although common, were not the strongest predictors of use or non-use in this sample.
The long-acting nature of IUC
The extent to which a respondent was attracted or “put off” by the long-acting nature of IUC was a strong predictor of non-use. The opinion that the long-acting nature of IUC was a “good” or “very good” feature of the method was statistically significantly associated with current use. For every increment along a discrete VAS indicating that the long-acting nature of IUC was a negative feature, a respondent was 8 times the odds of being a non-user (OR=8.340 [CI=5.753, 12.489], p<0.001).
Disliking the thought of IUC inside the body
Disliking the thought of IUC inside the body was also a strong predictor of non-use.
For every increment along a 5-point discrete VAS toward agreement with this statement “I do not like the thought of having something like that inside me”, the odds of a respondent being a non-user increase by 3.1 times (OR=3.138 [CI=2.617, 3.818], p<0.001).
Concerns about the effect of IUC on future pregnancy and the womb
Worries about the effect of using IUC upon future fertility or upon the womb of the user also predicted non-use. For every increment along a 5-point discrete VAS toward agreeing with the statement “I worry that it will damage my womb”, a respondent had 2.2 times the odds of being a non-user (OR=2.224 [CI=1.863, 2.681], p<0.001). Similarly for every increment along a 5-point discrete VAS agreeing with the statement “I worry that it will make it harder to get pregnant in the future”, a respondent had 2.6 times the odds of being a non-user (OR=2.587 [CI=2.122, 3.190], p<0.001).
Reported experiences of other people who had used IUC
The effect of other people’s experiences of IUC was statistically significant both for IUD (OR=1.820 [CI=1.465, 2.287], p<0.001) and for LNG-IUS (OR=2.551 [CI=2.009, 3.298], p<0.001), although it was stronger for LNG-IUS. For every shift along a discrete VAS toward knowledge of other people’s increasingly bad experience of LNG-IUS, a respondent was 2.55 times more likely to be a non-user of IUC.
With regard specifically to LNG-IUS, the effect on the menstrual cycle was a predictor of non-use. For every increment along a 5-point discrete VAS toward being “put off a lot” by the fact that LNG-IUS can cause light, irregular periods, the odds of a respondent being a non-user increased by 2.4 times (OR=2.382 [CI=2.006, 2.848], p<0.001).
For every increment along a 5-point discrete VAS toward being “put off a lot” by the fact that LNG-IUS can cause periods to stop completely, the odds of a respondent being a non-user increased by 2 times (OR=2.018 [CI=1.720, 2.391], p<0.001).
Discussion
The percentages for current use of IUC (13.1%) in this sample are somewhat higher than those reported from contraceptive clinics in the same time period in the UK. This may reflect recruitment bias or may show a different pattern of IUC use, and in particular, greater use of LNG-IUS, in GP than is recorded in data from contraceptive clinics.
More than half (51.9%) of survey respondents reported little or no knowledge of IUC. Previous studies have also found that women reported having little reliable information on IUC.9–17 Greater IUC knowledge has been associated with greater LARC use and positive attitudes toward IUC.17,18
The strongest predictor of non-use was not liking the fact that IUC is long acting. Our qualitative interviews, and free-text responses in the survey, suggest that concern about the health implications of a long-term device in the body and plans to conceive within the 5- to 10-year lifetime of the methods lie behind the dislike of the long-acting nature of the method. The qualitative interview data do not suggest that fear of being denied removal of the method (i.e. coercion to continue) lies behind this finding, although lack of control over stopping the method was cited in some of the free-text survey responses. We tentatively suggest that this concern may help explain some of the responses in the wider survey sample and that this would be an area for further research. Better information on the ease of removal and the fact that the device can be removed on request may mitigate against this concern. Recent work on the acceptability of self-removal of IUC is relevant, and this possibility may remove a potential barrier to the use of IUC.19,20
Our data indicate that fears about internal damage or dislike of the idea of an internal device are strong predictors of non-use of IUC. These concerns echo those reported in other studies in the UK, Canada, and USA.9–13,16,17,21 These are attitudes that could be addressed by clearer information about the risks associated with IUC. Negative experiences of other people who used the method also predict non-use. The “folk memory” of risks with earlier versions of IUC and the influence of lay knowledge upon contraceptive decision making are consistent with other studies and may not be given sufficient weight by clinicians.16,22
The disruptive effect on menstruation of hormonal IUC appears to present a barrier to non-use in this sample. We do not know how many of this sample of women experienced heavy or troublesome periods, and it is possible that this feature of the method may be welcomed by women who do experience heavier periods.
The belief that irregular or absent periods are unhealthy has been previously reported and may be addressed by better counseling and information about IUC.13
Our UK-based survey of women’s attitudes to IUC reflects many of the findings of surveys carried out in the US and Canada. The strong negative effect of the long-acting nature of IUC is unexpected and is a new finding.
Limitations and strengths
The recruitment of only non-users to the qualitative interview stage of the project means that the concerns enumerated in the quantitative survey are not based on first-hand experience of using IUC, which is a limitation of our findings.
The sample used in the quantitative arm of this study was not randomly generated, limiting the level of scientific evidence of the findings. However, the large sample of women attending GP for a variety of reasons can be considered a “typical” sample and likely to be representative of the range of views of women in this context. Those with poor literacy skills and those who did not speak English are less likely to have completed this survey.
The relatively poor response rate (28.9%) to the survey presents a possible source of bias because we have no information about the characteristics of non-respondents.
The majority of our sample (79.8%) self-identified as White British. Since ethnic differences have been correlated with contraceptive preference in the US, it would have been useful to have been able to examine whether this effect was present in our UK sample.23 However, the small, and ethnically diverse, numbers of non-White British respondents in our sample prevented this.
Cross-sectional data such as ours can highlight associations but cannot prove causality.
Response bias is possible due to the location of recruitment, although this is likely to be reduced because the surveys were completed and returned independently of health professionals.
Conclusion
The long-acting nature of IUC is the strongest predictor of non-use in this sample. Dislike of the “idea” of the device inside the body was also a strong predictor of non-use. The negative effect of fears for future pregnancy or about damage to the womb suggests that lack of knowledge about IUC, and in particular, about the safety profile, acts as a barrier to its uptake. With regard to hormonal IUS, dislike of the effects on bleeding patterns predicted non-use. Vernacular knowledge of IUC including “folk memories” and other peoples’ accounts of bad experiences are strong predictors of non-use.
Implications
There is a requirement for better information for women about IUC, which specifically addresses their concerns about risks, bleeding patterns, and effects on future fertility, which may have been acquired from vernacular accounts. For those women who dislike the long-acting nature of IUC, reassurance about removal on request at any time after insertion may make IUC more acceptable.
Acknowledgments
This project was funded by Bayer who manufactures several types of IUDs and IUSs. The funder played no part in the design or implementation of the research, other than requesting that we explored, in the qualitative interviews, the participants’ opinion of a new product Jaydess®. The funder has had no influence over the article written up and submitted for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
NICE [webpage on the internet]. NICE Guidelines [CG30] Long-Acting Reversible Contraception. 2016. Available from: https://www.nice.org.uk/guidance/cg30. Accessed August 23, 2016. | ||
Health and Social Care Information Centre. Sexual and Reproductive Health Services, England Statistics for 2014-15. 2015. Available from: http://digital.nhs.uk/catalogue/PUB18597/srh-serv-eng-14-15-rep.pdf. Accessed August 23, 2016. | ||
Lader D. Omnibus Survey Report No 41, Contraception and Sexual Health 2008/9. 2010. Available from: http://www.ons.gov.uk/ons/rel/lifestyles/contraception-and-sexual-health/2008-09/2008-09.pdf. | ||
Public Health England [webpage on the Internet]. Sexual and Reproductive Health Profiles. 2016. Available from; http://fingertips.phe.org.uk/profile/sexualhealth. Accessed September 15, 2016. | ||
Andrew S, Halcomb EJ. From ‘should we be?’ to ‘how are we’: moving forward with mixed methods health research. Int J Mult Res Approaches. 2011;5(1). | ||
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi: 10.1191/1478088706qp063oa. | ||
R Development Core Team [Website on the internet]. R: A language and environment for statistical computing. 2011. Vienna, Austria: the R Foundation for Statistical Computing. ISBN: 3-900051-07-0. Available from: http://www.R-project.org/. Accessed September 28, 2016. | ||
Heinze G, Ploner M, Dunkler D, Southworth H. “logistf: Firth’s bias reduced logistic regression”. R Package Version. 2013;1:21. | ||
Hall KS, Ela E, Zochowski MK, et al. “I don’t know enough to feel comfortable using them:” women’s knowledge of and perceived barriers to long-acting reversible contraceptives on a college campus. Contraception. 2016;93(6):556–564. | ||
Fleming K, Sokoloff A, Raine T. Attitudes and beliefs about the intrauterine device among teenagers and young women. Contraception. 2010;82(2):178–182. | ||
Asker C, Stokes-Lampard H, Beavan J, Wilson S. What is it about intrauterine devices that women find unacceptable? Factors that make women non-users: a qualitative study. J Fam Plann Reprod Health Care. 2006;32(2):89–94. | ||
Whitaker AK, Johnson LM, Harwood B, Chiappetta L, Creinin MD, Gold MA. Adolescent and young adult women’s knowledge of and attitudes toward the intrauterine device. Contraception. 2008;78(3):211–217. | ||
Hauck B, Costescu D. Barriers and misperceptions limiting widespread use of intrauterine contraception among Canadian Women. J Obstet Gynaecol Can. 2015;37(7):606. | ||
Callegari LS, Parisi SM, Schwarz EB. Perceptions of intrauterine contraception among women seeking primary care. Contraception. 2013;88(2):269–274. | ||
Michie L, Cameron ST, Glasier A, Wellings K, Loudon J. Myths and misconceptions about intrauterine contraception among women seeking termination of pregnancy. J Fam Plann Reprod Health Care. 2014;40(1):36–40. | ||
Glasier A, Scorer J, Bigrigg A. Attitudes of women in Scotland to contraception: a qualitative study to explore the acceptability of long-acting methods. J Fam Plann Reprod Health Care. 2008;34(4):213–217. | ||
Secura GM, Allsworth JE, Madden T, Mullersman JL, Peipert JF. The contraceptive CHOICE project: reducing barriers to long-acting reversible contraception. Obstet Gynecol. 2010;203(2):.e1–.e115. | ||
Whitaker AK, Terplan M, Gold MA, Johnson LM, Creinin MD, Harwood B. Effect of a brief educational intervention on the attitudes of young women toward the intrauterine device. J Pediatr Adolesc Gynecol. 2010;23(2):116–120. | ||
Foster DG, Grossman D, Turok DK, et al. Interest in and experience with IUD self-removal. Contraception. 2014;90(1):54–59. | ||
Foster DG, Karasek D, Grossman D, Darney P, Schwarz EB. Interest in using intrauterine contraception when the option of self-removal is provided. Contraception. 2012;85(3):257–262. | ||
Rubin S, Winrob L. Urban female family medicine patients’ perceptions about intrauterine contraception. J Womens Health. 2010;19:735–740. | ||
Kohler H. Learning in social networks and contraceptive choice. Demography. 1997;34(3):369–383. | ||
Jackson AV, Karasek D, Dehlendorf C, Foster DG. Racial and ethnic differences in women’s preferences for features of contraceptive methods. Contraception. 2016;93(5):406–411. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.