")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Predictors of Length of Hospital Stay, Mortality, and Outcomes Among Hospitalised COVID-19 Patients in Saudi Arabia: A Cross-Sectional Study
Authors Alwafi H, Naser AY , Qanash S , Brinji AS, Ghazawi MA, Alotaibi B , Alghamdi A, Alrhmani A, Fatehaldin R, Alelyani A, Basfar A, AlBarakati A, Alsharif GF, Obaid EF, Shabrawishi M
Received 7 February 2021
Accepted for publication 25 March 2021
Published 15 April 2021 Volume 2021:14 Pages 839—852
DOI https://doi.org/10.2147/JMDH.S304788
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 7
Editor who approved publication: Dr Scott Fraser
Hassan Alwafi,1 Abdallah Y Naser,2 Sultan Qanash,3,4 Ahmad S Brinji,5 Maher A Ghazawi,5 Basil Alotaibi,6 Ahmad Alghamdi,7 Aisha Alrhmani,7 Reham Fatehaldin,7 Ali Alelyani,7 Abdulrhman Basfar,7 Abdulaziz AlBarakati,7 Ghaidaa F Alsharif,7 Elaf F Obaid,7 Mohammed Shabrawishi7,8
1Faculty of Medicine, Umm Al Qura University, Mecca, Saudi Arabia; 2Department of Applied Pharmaceutical Sciences and Clinical Pharmacy, Faculty of Pharmacy, Isra University, Amman, Jordan; 3King Saud bin Abdulaziz University for Health Sciences, King Abdulaziz Medical City, Jeddah, Saudi Arabia; 4Department of Internal Medicine, National Guard Hospital, King Abdulaziz Medical City, Jeddah, Saudi Arabia; 5Department of Radiology, Al Noor Specialist Hospital, Mecca, Saudi Arabia; 6College of Pharmacy, King Saud University, Riyadh, Saudi Arabia; 7Department of Internal Medicine, Al Noor Specialist Hospital, Mecca, Saudi Arabia; 8Department of Respiratory Medicine, Al Noor Specialist Hospital, Mecca, Saudi Arabia
Correspondence: Mohammed Shabrawishi
Department of Respiratory Medicine, Al Noor Specialist Hospital, Mecca, 24242, Saudi Arabia
Tel +966555500592
Email [email protected]
Background: COVID-19 pandemic is a major strain on health and economic systems, with rapidly increasing demand for in patients’ facilities. Disease diagnosis and estimating patients at higher risk is important for the optimal management during the pandemic. This study aimed to identify the predictors of mortality and length of hospital stay in COVID-19 patients.
Methods: A retrospective cross-sectional study was conducted between March 2020 and August 2020 at Al-Noor Specialist Hospital in Mecca, Saudi Arabia. All patients who were admitted and had a confirmed COVID-19 diagnosis by a real-time polymerase chain reaction (PCR) were included in the study. Descriptive statistics were used to describe patients’ demographic characteristics, laboratory findings, and clinical outcomes. Multiple logistic/linear regression analysis was used to identify predictors of death and length of stay at the hospital.
Results: A total of 706 patients were hospitalised for COVID-19. The mean age was 48.0 years (SD: 15.6 years). More than half of the patients (68.5%; n= 292) were males. The median duration of stay at the hospital was 6.0 days (IQR: 300– 10:00). The prevalence rate of venous thromboembolism (VTE) among the patients was 3.0% (n= 21). In the multivariate logistic regression analysis, age (AOR: 1.05; 1.02– 1.09), patients with end-stage renal disease (AOR: 6.44; 2.20– 18.87), low Oxygen saturation SPO2 (AOR: 9.92; 4.19– 23.50), D.dimer > 0.5 (AOR: 13.31; 5.45– 32.49), ESR> 10 mm/h (AOR: 4.08; 1.72– 9.68), Ferritin> 400mcg/L (AOR: 18.55; 6.89– 49.96), and Procalcitonin> 0.5ug/L (AOR: 8.23; 1.81– 37.40) were associated with a higher risk of death among patients with COVID-19. Patients with VTE (AOR: 12.86; 3.07– 53.92) were at higher risk of death due to COVID-19.
Conclusion: Hospitalised COVID-19 patients have multiple negative consequences in terms of their laboratory findings, signs and symptoms. Age and end-stage renal diseases have a significant impact on the mortality rate and the length of hospital stay among COVID-19 patients.
Keywords: COVID-19, hospitalisation, length of stay, survival, ICU, Saudi Arabia
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which was discovered in China in 2019, is an ongoing pandemic.1 In March 2021, it was reported that there are more than 117 million confirmed cases in the world, and the total number of deaths in the world is around 2,600,000 in 220 countries, with a mortality rate of around 2%.2 In Saudi Arabia, there were around 380,000 confirmed infected cases by January 2021, and a mortality rate of around 1.7%.3
Patients with COVID-19 usually complain of fever, cough, fatigue, anorexia, myalgia, and diarrhoea,4 but in severe illness, usually dyspnoea is the most common symptom often accompanied by hypoxemia.4 Mortality rates depend on patients who have severe respiratory failure related to interstitial pneumonia and acute respiratory distress syndrome,5 but higher mortality is found in association with older age, male sex, pre-existing cardiovascular diseases, uncontrolled diabetes, hypertension, asthma, chronic lung disease, and d-dimer greater than 1 μg/mL at admission.6 Length of hospital stay due to the COVID-19 depends on patients’ clinical situation, however, it also depends on local guidelines in the institution or local health authority and the capacity of hospitals.7,8
COVID-19 pandemic is a major strain on health and economic systems, and the demand for inpatients’ facilities is increasing with the increase in the number of infected cases.9 Predicting factors associated with the need for hospitalisation and length of stay can be important to help in aid prioritizing patients, decision-making and contingency planning.10 This study aimed to identify the predictors of mortality and length hospital of stay in COVID-19 patients.
Methods
Study Design and Participants
A retrospective cross-sectional study was conducted at Al-Noor Specialist Hospital in Mecca, Saudi Arabia. Al-Noor Specialist Hospital is a tertiary hospital in Mecca, Saudi Arabia, and it is part of the Ministry of Health. The description of the study settings and the hospital has been described previously.11 All patients had a confirmed COVID-19 diagnosis by a real-time polymerase chain reaction (PCR). The PCR samples were obtained through a nasopharyngeal swap. All patients were admitted between March 15, 2020, and June 15, 2020 and they were followed up for a time to assess the clinical outcome; and the final date of follow-up was August 15, 2020. Data collection were between March 2020, and August 2020. All patients who were admitted and had a confirmed diagnosis of COVID-19 during the study period were included in the study.
Data Collection and Study Variables
Data were collected from patients’ files and electronic records using a unique medical record number (MRN) for each patient. All data were collected, reviewed and checked by a medical team, including medical residents and a consultant pulmonologist. Data included the patient’s demographics, clinical symptoms, comorbidity, and laboratory findings. Data were collected at the time of admission to the hospital. Patients were classified according to their severity based on the following category: mild, moderate, severe and, critically severe disease. The definition of these categories has been described previously.11
Outcomes
The primary outcome was predictors of patients’ admission to an intensive care unit. Secondary outcomes were to identify predictors of length of hospital stay and mortality.
Ethical Approval and Consent-to-Participate
The study protocol and study methodology were approved by the Ministry of Health’s Institutional Review Board (IRB), as well as the hospital (No H-02-K-076-0920-386). Patients informed consent were obtained and patients were informed that their clinical data would be used for clinical or research purposes, while keeping all their personal information confidential. The ethical principles of the Declaration of Helsinki were adhered to during collection, handling, and storage of data, and all care was taken to protect patient confidentiality.
Statistical Analysis
Descriptive statistics were used to describe patients’ demographics, laboratory findings, and clinical outcomes. Independent sample t-test was used to compare the mean value for continuous variables. A Chi-squared test/Fisher test was used to compare proportions for categorical variables. Multiple logistic/linear regression analysis was used to identify predictors of death and length of stay at the hospital, and a confidence interval of 95% (p < 0.05) was applied to represent the statistical significance of the results. All statistical analyses were conducted using SPSS (Statistical Package for the Social Sciences) version 25.0 software (SPSS Inc.).
Results
Patients’ Clinical Characteristics
Table 1 below shows the characteristics of COVID-19 patients at presentation to the hospital. A total of 706 patients were hospitalised for COVID-19. The mean age was 48.0 years (SD: 15.6 years). More than half of the patients (68.5%; n= 292) were males. The majority of them were having mild to moderate cases. Twenty-five patients (3.5%) reported working in the healthcare sector. More than half of them (61.9%; n= 435) were non-Saudi. Around 17.4% (n= 122) reported a history of smoking. The most common comorbidities were diabetes mellitus (DM) (36.0%, n= 254), hypertension (30.2%, n= 213), and coronary heart diseases (10.9%; n= 77). Around 9.8% of the patients (n= 69) reported a recent travel history. Regarding the severity of the patients’ case, 33.7% were mild, 30.3% were moderate, and 24.2% were severe, and 11.8% were critical and required intensive care unit (ICU) care. Regarding patients’ vital signs upon arrival to hospital, 47.3% (n= 334) had fever (body temperature > 38 °C), 9.5% (n= 67) had respiratory rate (RR) more than 30, 22.1% (n= 156) had SPO2 < 93, and 4.2% (n= 30) had heart rate (HR) > 125.
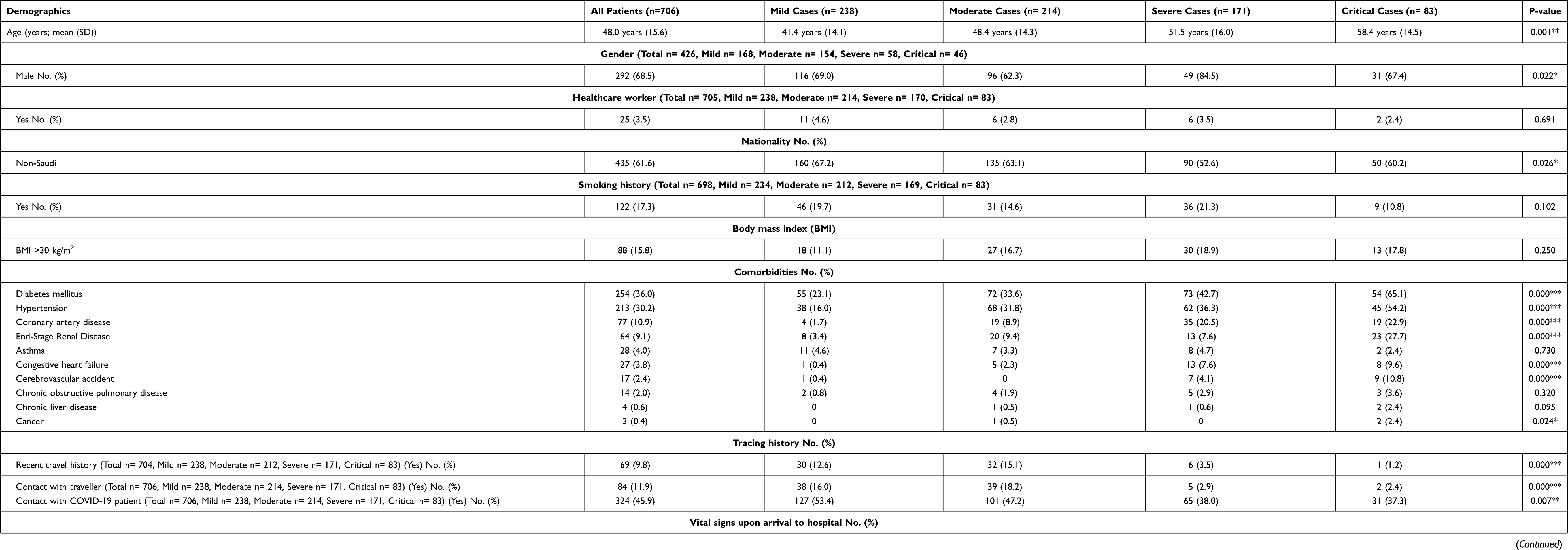 |
Table 1 Patients Demographic Characteristics at Presentation |
Fever was the most common symptom at presentation (72.4%, n= 511), followed by cough (63.0%, n= 445), and shortness of breath (56.4%, n= 398) (Table 2). Fever, cough, shortness of breath, nausea/vomiting, headache, loss of taste and smell, sputum were more common across severe and critical cases compared to others.
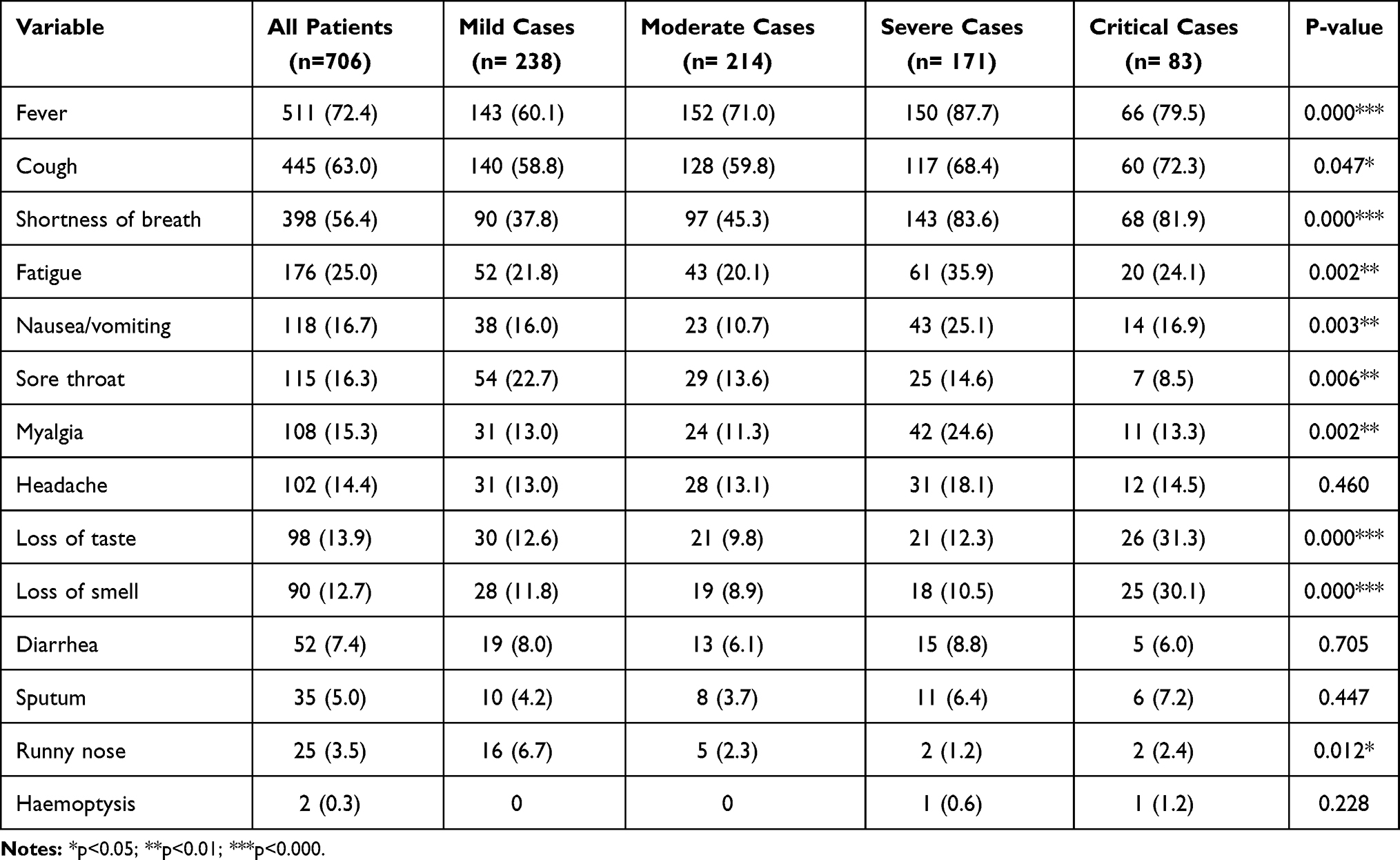 |
Table 2 Patient Signs and Symptoms Stratified by Severity |
Laboratory Findings
Around 16.5% (n= 116) of the patients had white blood cell (WBC)> 10,000, 13.9% (n= 98) had WBC< 4000, and 21.0% (n= 148) of them had lymphocyte count <1500. About 12.6% (89) had platelet count < 150 and 29.9% (n= 210) had D.dimer >0.5. The proportion of patients who had WBC >10,000, lymphocyte count <1500, platelet count < 150, and D.dimer >0.5 increase as the severity of the disease increase in a statistically significant pattern (p<0.001). The mean Neutrophil-lymphocyte ratio (NLR) value was 9.9 (SD:33.5). The most common blood groups of COVID-19 patients were A+, O+, and B+ accounting for 35.7%, 28.6%, and 20.5% respectively (Table 3).
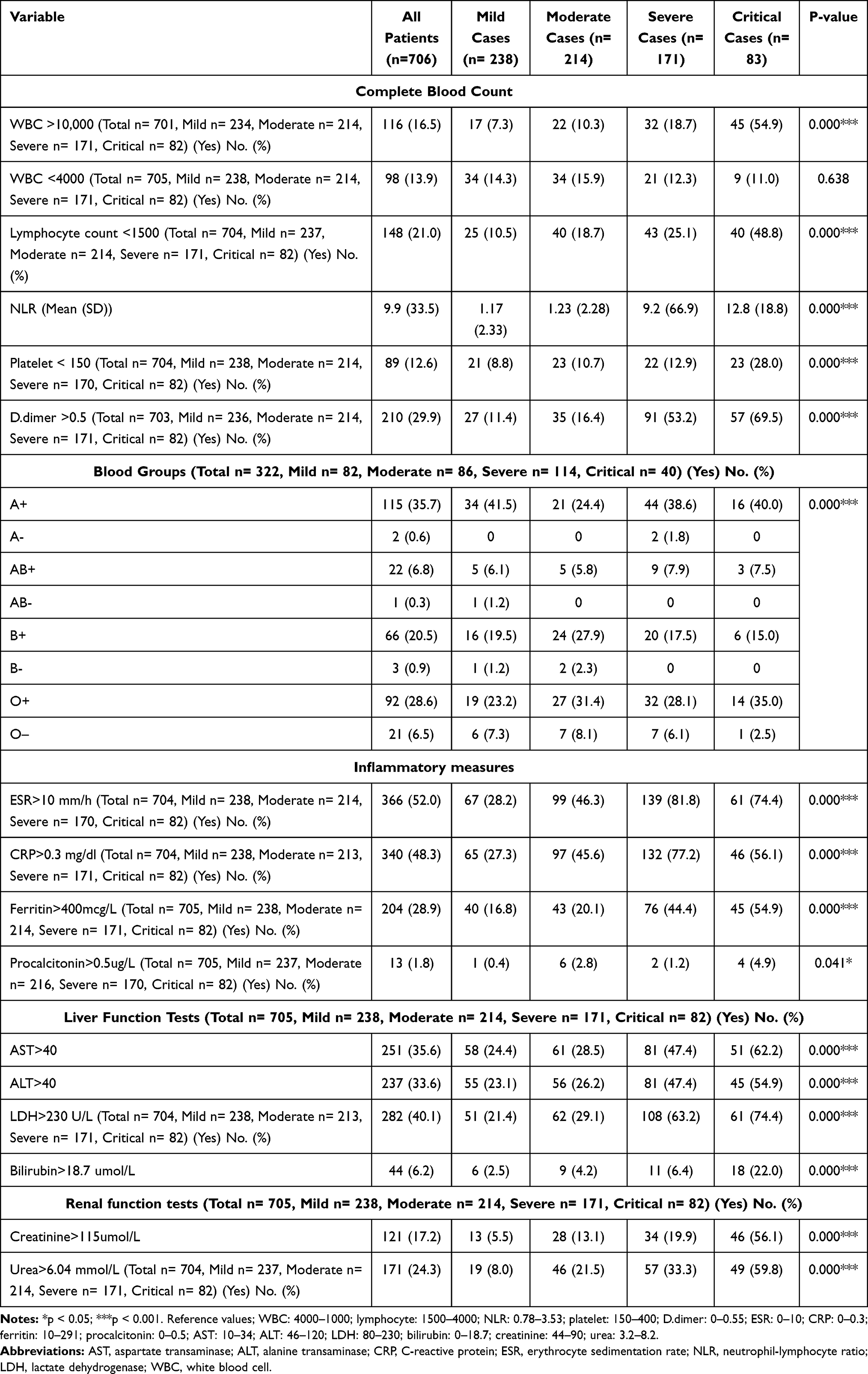 |
Table 3 Laboratory Findings of the Study Participants Stratified by Severity |
Regarding patients’ inflammatory measures, around half of the patients had erythrocyte sedimentation rate (ESR)>10 mm/h and C-reactive protein (CRP)>0.3 mg/dl. One-third of the patients had Ferritin>400mcg/L, and 1.8% of them had Procalcitonin>0.5ug/L. Concerning patients’ liver function tests, around one-third of the patients had AST>40 and ALT>40. Additionally, 40.1% of them had lactate dehydrogenase (LDH)>230 U/L, and 6.2% had Bilirubin>18.7 umol/L. Regarding patients’ kidney function tests, 17.2% of them had Creatinine>115 umol/L, and 24.3% had Urea>6.04 mmol/L (Table 3).
Factors Associated with Death
The median duration of stay at the hospital was 6.0 days (IQR: 300– 10:00). The duration of stay in the hospital ranged from one day to 55 days. The prevalence rate of venous thromboembolism (VTE) among the patients was 3.0% (n= 21). More than half of the patients (63.6%; n= 450) pneumonia radiologically. At the end of the follow-up period, a total of 623 patients (91.6%) recovered. Three patients (0.4%) did not recover at the end of the follow-up, and 7.6% of the patients (n= 54) deceased while the remaining either transferred to other facility or still in the hospital, at last, follow up. The severity of the cases affected the recovery rate and mortality rate in a statistically significant way (p>0.001) (Table 1).
In the multivariate logistic regression analysis, the following risk factors were associated with a higher risk of death among patients with COVID-19. Age (AOR: 1.05; 1.02–1.09), high respiratory rate (RR) (AOR: 153.90; 9.80–2416.60), low Oxygen saturation SPO2 (AOR: 9.92; 4.19–23.50), D.dimer >0.5 (AOR: 13.31; 5.45–32.49), ESR>10 mm/h (AOR: 4.08; 1.72–9.68), Ferritin>400mcg/L (AOR: 18.55; 6.89–49.96), and Procalcitonin>0.5ug/L (AOR: 8.23; 1.81–37.40). Patients with VTE (AOR: 12.86; 3.07–53.92) were at higher risk of death due to COVID-19. End-stage renal diseases were identified to increase the risk of COVID-19. For further details, please refer to Table 4.
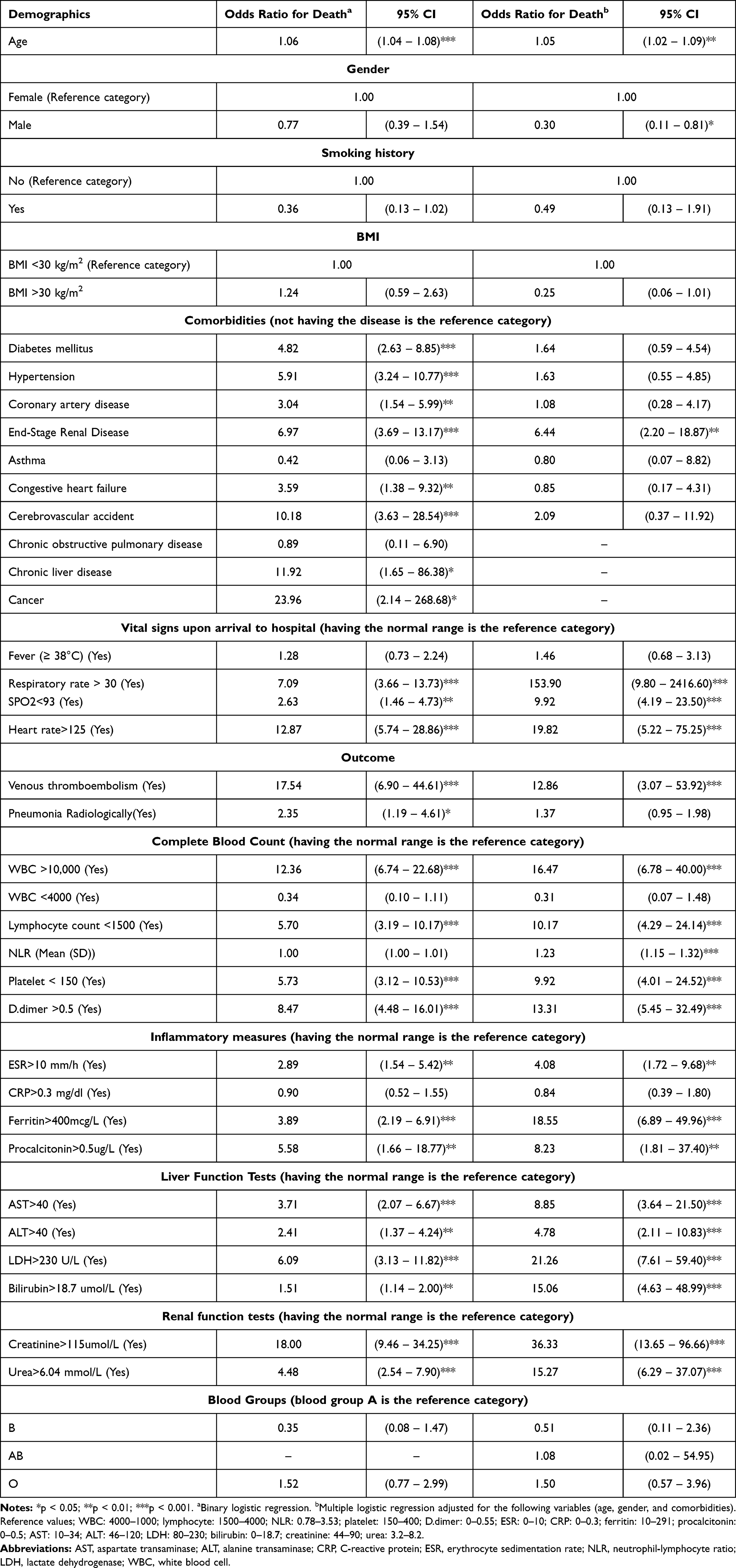 |
Table 4 Logistic Regression to Identify Risk Factors of Death |
Factors Associated with Increased Length of Stay
Several factors were associated with increased risk of the length of stay, including comorbidities such as congestive heart failure, cerebrovascular accident, and COPD, fever, D.dimer value of more than >0.5, WBC>10,000, ESR>10 mm/h, CRP>0.3 mg/dl, ferritin > 400 mcg/L, procalcitonin >0.5 ug/L, LDH>230 U/L, creatinine >115 umol/L, and blood group O (p<0.05), for further details, please refer to Table 5.
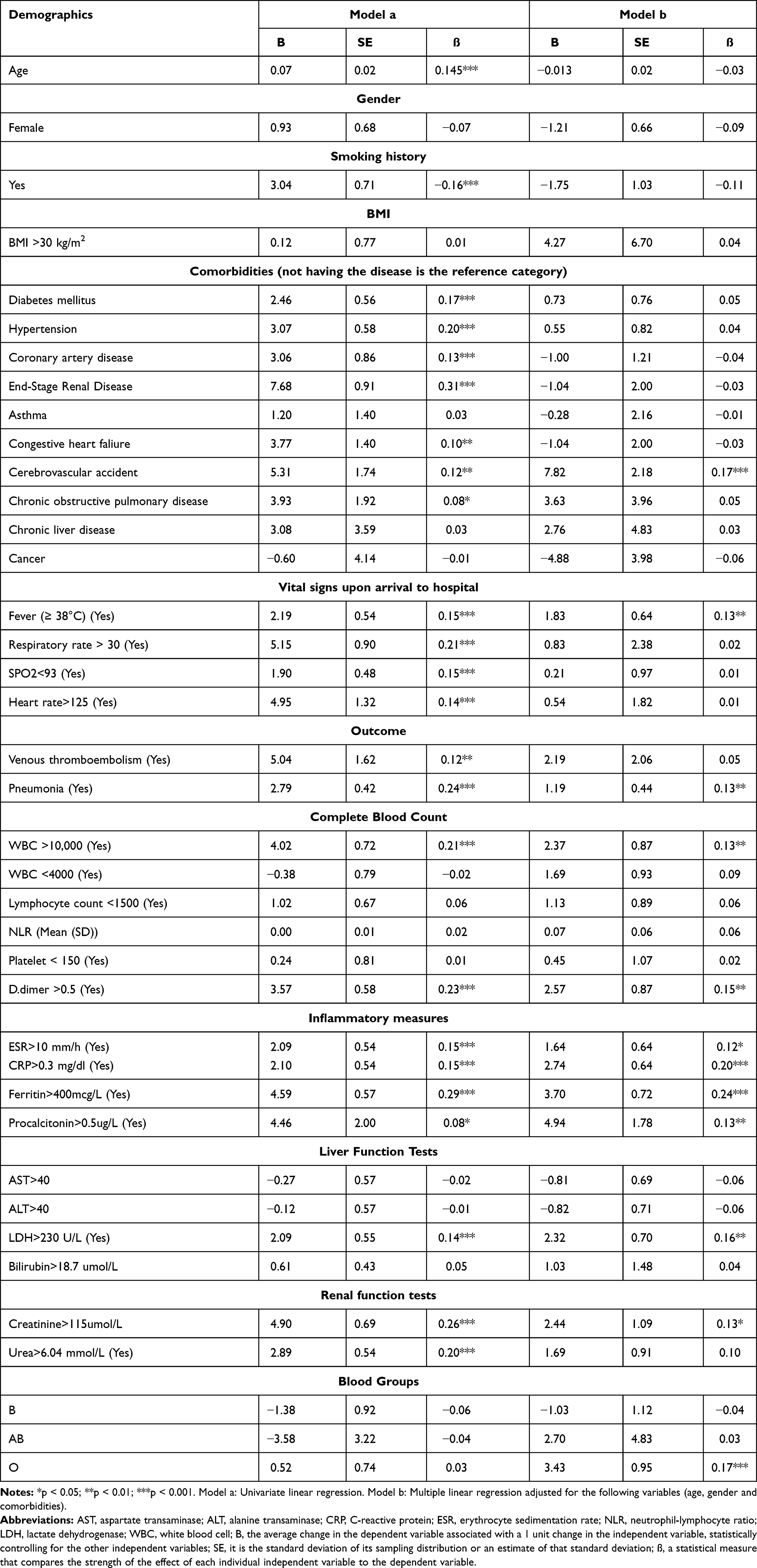 |
Table 5 Linear Regression to Identify Predictors of Length of Stay |
Discussion
In this cross-sectional study, we investigated the predictors of mortality and length of stay in hospital among hospitalised patients with COVID-19. The key findings of this study are that age, patients with chronic comorbidities, patients with VTE and radiological evidence of pneumonia, and higher D-dimer values were important risk factors that were associated with a higher risk of death and increased length of stay in hospital.
Our findings revealed the significant impact of age and chronic conditions on the mortality rate and the length of hospital stay. It comes as no surprise that the escalated rate of mortality and prolonged hospital stay was associated with older patients. Thus this study substantiates the previous findings of the literature.12 This may also be due to their weak immune system and some behavioural responses in the measures taken.13,14 Chronic diseases demonstrate a significant influence on the outcomes; diabetes patients were more vulnerable to fatal consequences and longer hospitalisation compared to non-DM patients, which is consistent with results reported from the previous study.15 Hypertensive patients have a propensity to express high mortality rate and stay hospitalised longer. Likewise, pre-existent cardiovascular and cerebrovascular events carry a high risk of death and a longer duration of hospitalisation. The effect of SARS-COV-2 on the vascular endothelium could be explained by the current understanding that angiotensin-converting enzyme 2 (ACE2) cellular receptors as the entry sites of SARS-COV2 as shown in different studies.16,17
There are several explanations for these results, Renin-Angiotensin system (RAAS) and inflammatory cytokines have been mentioned as mediators in severe outcomes among hypertensive patients.18 Furthermore, the frequent utilisation of angiotensin-converting enzyme inhibitors (ACEIs) can lead to a decrease in angiotensin-converting enzyme (ACE) and an increase in the expression of ACE2 in the lungs which eventually facilitates the invasion of Covid-19 virus,19,20 nonetheless this still controversial as illustrated by other studies.21 Further, the severe viral virulence may lead to high oxygen demand, physiological and reflex tachycardia and aggravates the manifestation of coronary artery diseases accompanied by respiratory distress, finally, unfavourable outcomes will present.22 Patients with chronic liver diseases (CLD) were also more susceptible to fatal consequences either death or a longer hospitalisation period. The confirmed laboratory findings emphasise the negative impact of Covid-19 on liver functions. The previous study elucidated the high mortality rate among CLD patient who they are Covid-19 infected.23,24 Our findings also highlighted the high mortality rate and the long period of hospitalisation among cancer patients. The nature of cancer and the antineoplastic agents compromise the immune system. Consequently, it spikes the probability of lethal and severe infection of the Covid-19 virus among these patients. Moreover, the redundant clinical visits for follow up and chemotherapy dose also expose the patients to the infection.25
The hypercoagulability of Covid-19 patients was observed and confirmed by laboratory findings. Venous thrombus embolism was one of the poor outcomes among covid-19 patients with a significant correlation and high odd ratios. The severe infection and long bed-ridden interval in ICU dysregulate the homeostasis of the cascade system by activating the inflammatory cytokines.26 Not withstanding, the pathogeneses of VTE-induced by Covid-19 are complex and multifactorial. Our study provides further evidence of Covid-19 pneumonia as a predictor for the high mortality rate and prolonged hospitalisation. These findings support the aggressive preventive measures that be taken to halt the mortality rate among these patients.
In our study, we found no significant difference between blood group type and the risk of death. However, we found a significant difference in the duration of hospital stay for patients with blood group O. Previous reports showed a reduced prevalence of Covid-19 infection in blood group O.27 However, this was later contradicted, as some other published report suggested that there is no link between Covid-19 infection and type of blood group.28,29 Future studies on a larger scale and different populations are needed to investigate this association.
In our study and similar to published reports, patients with chronic obstructive pulmonary disease (COPD) were found to be at higher risk for a severe outcome,30 likely due to the fact that these patients usually have reduced lung function along with various comorbidities.31 Interestingly, on the other hand, patients with pre-existent asthma did not have a risk of worse outcome,32 and this could be partly explained by the lower expression of ACE2 in asthmatic bronchial epithelium.33
Obesity is one of the major comorbidities to be considered. Above increasing the risk of different complications such as DM, liver diseases and cardiovascular diseases, we observed obesity also increases the mortality rate and the demand on intensive care facilities among SARS-COV-2 patients, which augments the findings in a previous systematic review.34 Henceforth, obesity is one of the potential predictors for the study outcomes. However, the underlying mechanism behind the bad prognosis of obese patients still unknown.
We believe that our results are similar to the literature, it may help in earlier risk stratification, and triage of COVID-19 patients admitted to the hospital and in reducing the overload on emergency departments visits and intensive care units in order to facilitate COVID-19 cases and other emergency care cases. Some factors identified in this study, such as older age and comorbidities, may help policymakers and guidelines in their recommendations about prioritising patients based on their symptoms and may help to improve the patient’s care. Furthermore, the founded risk factors might be helpful in establishing a scoring system that can be applied to predict mortality and appropriate management plan.
This study has some limitations. First, the study population only included patients from a single-centre hospital in Saudi Arabia. Second, the cross-sectional study design restricted our ability to identify causality between study variables.
Conclusion
Hospitalised COVID-19 patients have multiple negative consequences in term of their laboratory findings, signs and symptoms. Age and chronic conditions have a significant impact on the mortality rate and the length of hospital stay among COVID-19 patients. Earlier risk stratification of the COVID-19 patients admitted to the hospital is recommended.
Author Contributions
Conceptualization, Hassan Alwafi, Mohammed Shabrawishi, Sultan Qanash, Abdallah Y Naser; Data curation, Mohammed Shabrawishi, Ahmad S Brinji, Maher A Ghazawi, Ahmad Alghamdi, Aisha Alrhmani, Reham Fatehaldin, Ali Alelyani, Abdulrhman Basfar, Abdulaziz Al Barakati, Ghaidaa F Alsharif, Elaf F Obaid; Formal analysis, Abdallah Y Naser, Hassan Alwafi; Investigation, Mohammed Shabrawishi, Sultan Qanash, Abdallah Y Naser, Ahmad S Brinji and Hassan Alwafi; Methodology, Mohammed Shabrawishi, Abdallah Y Naser, Sultan Qanash and Hassan Alwafi; Project administration, Mohammed Shabrawishi and Hassan Alwafi; Resources, Ahmad Alghamdi, Aisha Alrhmani, Reham Fatehaldin, Ali Alelyani, Abdulrhman Basfar, Abdulaziz Al Barakati, Ghaidaa F Alsharif, Elaf F Obaid; Supervision, Mohammed Shabrawishi and Hassan Alwafi; Validation, Mohammed Shabrawishi, Abdallah Y Naser, Maher A Ghazawi, Ahmad S Brinji and Hassan Alwafi; Writing – original draft, Mohammed Shabrawishi, Abdallah Y Naser, Sultan Qanash, Basil Alotaibi and Hassan Alwafi; Writing– review & editing, Mohammed Shabrawishi, Sultan Qanash, Abdallah Y Naser, Ahmad S Brinji, Maher A Ghazawi, Ahmad Alghamdi, Aisha Alrhmani, Reham Fatehaldin, Ali Alelyani, Abdulrhman Basfar, Abdulaziz Al Barakati, Ghaidaa F Alsharif, Elaf F Obaid, Basil Alotaibi and Hassan Alwafi. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors have stated explicitly that there are no conflicts of interest in connection with this article.
References
1. Zhu N, Zhang D, Wang W, et al. A Novel Coronavirus from patients with Pneumonia in China, 2019. N Engl J Med. 2020;382(8):727–733. doi:10.1056/NEJMoa2001017
2. World Health Organization. Coronavirus disease 2019 (COVID-19)Situation Report–209; 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports.
3. (SCDC) Scfdpac. COVID-19 disease daily report November 18 2020; 2020. Available from: https://covid19.cdc.gov.sa/daily-updates.
4. World Health Organization. Coronavirus disease (COVID-19) outbreak 2020; 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
5. Ranieri VM, Rubenfeld GD, Thompson BT, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526–2533. doi:10.1001/jama.2012.5669
6. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet (London, England). 2020;395(10229):1054–1062. doi:10.1016/S0140-6736(20)30566-3
7. Wu Z, McGoogan JM. Characteristics of and important lessons from the Coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323(13):1239–1242. doi:10.1001/jama.2020.2648
8. Chen S, Zhang Z, Yang J, et al. Fangcang shelter hospitals: a novel concept for responding to public health emergencies. Lancet (London, England). 2020;395(10232):1305–1314. doi:10.1016/S0140-6736(20)30744-3
9. Xing C, Zhang R. COVID-19 in China: responses, challenges and implications for the health system. Healthcare. 2021;9(1):82. doi:10.3390/healthcare9010082
10. Rees EM, Nightingale ES, Jafari Y, et al. COVID-19 length of hospital stay: a systematic review and data synthesis. BMC Med. 2020;18(1):270. doi:10.1186/s12916-020-01726-3
11. Shabrawishi M, Al-Gethamy MM, Naser AY, et al. Clinical, radiological and therapeutic characteristics of patients with COVID-19 in Saudi Arabia. PLoS One. 2020;15(8):e0237130. doi:10.1371/journal.pone.0237130
12. Wei C, Liu Y, Liu Y, et al. Clinical characteristics and manifestations in older patients with COVID-19. BMC Geriatr. 2020;20(1):395. doi:10.1186/s12877-020-01811-5
13. Sun Z, Yang B, Zhang R, Cheng X. Influencing factors of understanding COVID-19 risks and coping behaviors among the elderly population. Int J Environ Res Public Health. 2020;17(16):5889. doi:10.3390/ijerph17165889
14. Sun Z, Cheng X, Zhang R, Yang B. Factors influencing rumour re-spreading in a public health crisis by the middle-aged and elderly populations. Int J Environ Res Public Health. 2020;17(18):6542. doi:10.3390/ijerph17186542
15. Alguwaihes AM, Al-Sofiani ME, Megdad M, et al. Diabetes and Covid-19 among hospitalized patients in Saudi Arabia: a single-centre retrospective study. Cardiovasc Diabetol. 2020;19(1):205. doi:10.1186/s12933-020-01184-4
16. Kreutz R, Algharably EAE, Azizi M, et al. Hypertension, the renin-angiotensin system, and the risk of lower respiratory tract infections and lung injury: implications for COVID-19. Cardiovasc Res. 2020;116(10):1688–1699. doi:10.1093/cvr/cvaa097
17. Imai Y, Kuba K, Penninger JM. The discovery of angiotensin-converting enzyme 2 and its role in acute lung injury in mice. Exp Physiol. 2008;93(5):543–548. doi:10.1113/expphysiol.2007.040048
18. Wang Y, Chen B, Li Y, et al. The use of renin–angiotensin–aldosterone system (RAAS) inhibitors is associated with a lower risk of mortality in hypertensive COVID-19 patients: a systematic review and meta-analysis. J Med Virol. 2021;93(3):1370–1377. doi:10.1002/jmv.26625
19. Miesbach W. Pathological Role of Angiotensin II in Severe COVID-19. TH Open. 2020;4(2):e138–e44. doi:10.1055/s-0040-1713678
20. Gheblawi M, Wang K, Viveiros A, et al. Angiotensin-converting enzyme 2: SARS-CoV-2 receptor and regulator of the renin-angiotensin system: celebrating the 20th anniversary of the discovery of ACE2. Circ Res. 2020;126(10):1456–1474. doi:10.1161/CIRCRESAHA.120.317015
21. Zhang P, Zhu L, Cai J, et al. Association of inpatient use of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers with mortality among patients with hypertension hospitalized with COVID-19. Circ Res. 2020;126(12):1671–1681. doi:10.1161/CIRCRESAHA.120.317134
22. Nishiga M, Wang DW, Han Y, Lewis DB, Wu JC. COVID-19 and cardiovascular disease: from basic mechanisms to clinical perspectives. Nat Rev Cardiol. 2020;17(9):543–558. doi:10.1038/s41569-020-0413-9
23. Li C, Chen Q, Wang J, et al. Clinical characteristics of chronic liver disease with coronavirus disease 2019 (COVID-19): a cohort study in Wuhan, China. Aging (Albany NY). 2020;12(16):15938–15945. doi:10.18632/aging.103632
24. Moon AM, Webb GJ, Aloman C, et al. High mortality rates for SARS-CoV-2 infection in patients with pre-existing chronic liver disease and cirrhosis: preliminary results from an international registry. J Hepatol. 2020;73(3):705–708. doi:10.1016/j.jhep.2020.05.013
25. Saini KS, Tagliamento M, Lambertini M, et al. Mortality in patients with cancer and coronavirus disease 2019: a systematic review and pooled analysis of 52 studies. Eur J Cancer. 2020;139:43–50. doi:10.1016/j.ejca.2020.08.011
26. Porfidia A, Valeriani E, Pola R, Porreca E, Rutjes AWS, Di Nisio M. Venous thromboembolism in patients with COVID-19: systematic review and meta-analysis. Thromb Res. 2020;196:67–74. doi:10.1016/j.thromres.2020.08.020
27. Barnkob MB, Pottegård A, Støvring H, et al. Reduced prevalence of SARS-CoV-2 infection in ABO blood group O. Blood Adv. 2020;4(20):4990–4993. doi:10.1182/bloodadvances.2020002657
28. Zietz M, Zucker J, Tatonetti NP. Associations between blood type and COVID-19 infection, intubation, and death. Nat Commun. 2020;11(1):5761. doi:10.1038/s41467-020-19623-x
29. Bhattacharjee S, Banerjee M, Pal R. ABO blood groups and severe outcomes in COVID-19: a meta-analysis. Postgrad Med J. 2020;
30. Alqahtani JS, Oyelade T, Aldhahir AM, et al. Prevalence, severity and mortality associated with COPD and smoking in patients with COVID-19: a rapid systematic review and meta-analysis. PLoS One. 2020;15(5):e0233147–e. doi:10.1371/journal.pone.0233147
31. Sin DD, Anthonisen NR, Soriano JB, Agusti AG. Mortality in COPD: role of comorbidities. Eur Respir J. 2006;28(6):1245–1257. doi:10.1183/09031936.00133805
32. Matsumoto K, Saito H. Does asthma affect morbidity or severity of COVID-19? J Allergy Clin Immunol. 2020;146(1):55–57. doi:10.1016/j.jaci.2020.05.017
33. Jackson DJ, Busse WW, Bacharier LB, et al. Association of respiratory allergy, asthma, and expression of the SARS-CoV–2 receptor ACE2. J Allergy Clin Immunol. 2020;146(1):203–206.e3. doi:10.1016/j.jaci.2020.04.009
34. Chu Y, Yang J, Shi J, Zhang P, Wang X. Obesity is associated with increased severity of disease in COVID-19 pneumonia: a systematic review and meta-analysis. Eur J Med Res. 2020;25(1):64. doi:10.1186/s40001-020-00464-9
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.