")
Back to Journals » International Journal of Women's Health » Volume 12
Predictors of Intention to Use Maternity Waiting Home Among Pregnant Women in Bench Maji Zone, Southwest Ethiopia Using the Theory of Planned Behavior
Authors Nigussie T , Yaekob R, Geremew M, Asefa A
Received 15 June 2020
Accepted for publication 12 October 2020
Published 27 October 2020 Volume 2020:12 Pages 901—910
DOI https://doi.org/10.2147/IJWH.S267730
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Tadesse Nigussie,1 Rahel Yaekob,2 Mesfin Geremew,1 Adane Asefa1
1Department of Public Health, College of Health Science, Mizan-Tepi University, Mizan-Aman, Ethiopia; 2Department of Midwifery, College of Health Science, Mizan-Tepi University, Mizan-Aman, Ethiopia
Correspondence: Tadesse Nigussie
Department of Public Health, College of Health Sciences, Mizan-Tepi University, Mizan Aman, Ethiopia
Tel +251-911- 598- 639
Email [email protected]
Background: Ending preventable maternal mortality remains an unfinished agenda and one of the world’s most critical challenges. Skilled care at birth is one of the crucial strategies that help to prevent deaths that occur during delivery. Maternity waiting homes have been endorsed to facilitate access to skilled care during intra-partum and post-partum periods for women living in rural areas. However, the majority of pregnant mothers in Ethiopia do not use this service; hence, this study aimed to assess the predictors of intention to use maternity waiting home.
Methods: A community-based cross-sectional study was conducted from March 15 to June 20, 2018 in Bench Maji Zone, Southwest Ethiopia. A multistage sampling technique was used. The data were collected by trained data collectors using a structured pre-tested questionnaire. Data were entered into the epi data manager version 4.0.2.101 and exported to SPSS version 21 for analysis. The correlation among constructs of the theory of planned behavior was estimated. A hierarchical linear regression was used to identify predictors of intention to use maternity waiting home, and α value of less than 5% was used as a level of significance.
Results: A total of 829 women were interviewed. The mean age of respondents was 27.1 (± 5.2) years. Thirty-nine percent of the respondents used maternity waiting home previously. The attitude (β =0.12, p< 0.001), subjective norm (β =0.47, p< 0.001), perceived behavioral control (β =0.42, p< 0.001), and ANC use during current pregnancy (β =0.07, p=0.030) were predictors of intension to use maternity waiting homes. R square was calculated to be 81%.
Conclusion: The intention to use maternity waiting homes was significantly associated with antenatal care use, attitude, subjective norm, and perceived behavioral control. Thus, multidimensional interventions are important to increase the intension to use MWH.
Keywords: maternity waiting home, intention, behavior, theory of planned behavior
Background
An estimated 13.6 million women died due to pregnancy and related complications between 1990 and 2015 globally.1 Ninety-nine percent of these deaths occurred in low- and middle-income countries, with sub-Saharan Africa alone accounted for approximately 66% of these deaths. In 2015, the maternal mortality ratio (MMR) in Sub-Saharan Africa was 546 maternal deaths per 100,000 live births.2 Ethiopia is also among countries with the highest maternal morbidity and mortality in Sub-Saharan Africa.3 According to Ethiopia demographic and health survey 2016 report, the pregnancy-related mortality ratio was 412 maternal deaths per 100,000 live births.3
Promising progress has been made in the past 25 years in terms of reducing maternal mortality but the achievement varies across countries. Maternal mortality ratio (MMR) was reduced by 44% from an estimated 385 maternal deaths per 100,000 live births in 1990 to 216 maternal deaths per 100,000 live births in 2015 globally.4
Ending preventable maternal mortality remains an unfinished agenda and one of the world’s most critical challenges despite the remarkable achievements made in the past 25 years. To end this challenge, the global states devised the sustainable development goal (SDG) to reduce MMR by at least two-thirds from the 2010 baseline, and that no country should have an MMR higher than 140 deaths per 100 000 live births by 2030 and skilled care provision at every birth.5
Providing accessible and quality intra-partum and post-partum services, example through maternity waiting home, is a key strategy for SDG targets.6 Maternity waiting home (MWH) facilitates access to skilled care during intra-partum and postpartum, particularly for women living in rural and remote areas where distance and poor transportation severely restrict access to delivery services.7–10 It is a temporary residence for women to access health facilities easily and avoid delays during emergency.6 Maternity waiting home is an encouraging strategy to improve access to facilities for delivery and reduce maternal death. For instance, a study showed that utilization of this service increases the proportion of institutional delivery and improves access to essential and emergency obstetric care, which in turn results in improved maternal health, decreased risk of obstructed labour, decreased rates of stillbirths, and low risk of perinatal death.11 It is also indicated that there were differences in maternal mortality and morbidity between communities with maternity waiting homes and those without maternity waiting homes.12 Regardless of aforementioned benefits however, the utilization of MWH is low in Ethiopia.13 The rarely utilized maternity waiting home in the country is used by pregnant mothers with difficulty to promptly access health care for delivery services (those from rural areas). Mothers are expected to stay in MWH for approximately 15 days before delivery. All services including shelter, food, water, and other basic needs are provided for free by local government agency and contribution from community throughout their stay in health facility.
Regardless of these benefits, the utilization of MWH is low in Ethiopia.13 Due to different reasons, home delivery is high in Ethiopia especially for rural women.14–17 Maternity waiting home is the key intervention to decrease home delivery which has great on the health of both mothers and new-borns. Service utilization behaviour is affected by multiple factors; therefore, solutions do not come through a single detection, but rather from an array of innovations that address multiple factors.18–20 Therefore, we used the perspective of the theory of planned behaviours to identify the predictors of behavioural intention to use maternity waiting home.
The theory of planned behaviour (TPB) was developed by Fishbein and Ajzen in the 1970s. According to TPB, the best predictor of behaviour is behavioural intention, which, in turn determined by attitude toward the behaviour, social normative perceptions regarding it, and perceived behavioural control of performing the behaviour. TPB has been used successfully to predict and explain a wide range of health behaviours and intentions.21–23 For instance, it has explained well male involvement intention during childbirth in a rural setting. It was also used to predict the intention of cervical cancer screening service use,24 women’s participation in breast cancer screening,25 and the intention of exclusive breastfeeding.26 It was employed to explain the predictors of the intention of institutional delivery as well.27 In a similar manner, the current study aimed to investigate the predictors of behavioural intention toward MWH using the theory of planned behaviour so as to fill the dearth of evidence on this important issue.
Methods
Study Design and Setting
A community-based cross-sectional study was conducted in Bench Maji Zone, Southern Nations, Nationalities and Peoples Region from March 15 to June 20, 2018. The zone’s capital city, Mizan-Aman is located 561 km away from Addis Ababa in the Southwest direction. Bench-Maji zone is divided into one urban district (Mizan-Aman), five pastoral/semi-pastoral districts (Surma, Maji, Meint Goldia, Meint Shesha, and Bero districts) and five agrarian districts (Sheko, Semen-Bench, Debub-Bench, Shey-Bench, and Guraferda districts). The zone had 1 hospital, 40 health centers, 300 health posts, and 31 functional maternity waiting homes during the study period. The service given in MWH includes shelter in the health facility, food, water and other supports. The fund for MWH covered by government and also contributed by local residents. There are recruited staffs who facilitate the services in MWH. The zonal health department’s annual report of 2016/17 indicated that only 42.07% of the eligible mothers used maternity waiting home.28
Population
Source population: source populations were all pregnant mothers residing in rural area of Bench Maji Zone, southwest Ethiopia.
Study population: study populations were randomly selected pregnant women who were living in rural area of Bench Maji Zone, southwest Ethiopia during the data collection period. The sampling unit and study unit were individual pregnant woman.
Eligibility criteria: pregnant women those lived at least 6 months prior to the study in the study area were included while pregnant women who were severely sick and unable to respond to an interview during the data collection period were excluded from the study.
Sample Size and Sampling Procedure
The sample size was calculated using sample size determination formula for single population proportion ( ) with assumptions of: 50% proportion of intended women to use maternity waiting home (p), 95% confidence level (Zα/2=1.96), 5% margin of error (d), and a design effect of 2. After adding 10% for non-response, the final sample size became 846.
) with assumptions of: 50% proportion of intended women to use maternity waiting home (p), 95% confidence level (Zα/2=1.96), 5% margin of error (d), and a design effect of 2. After adding 10% for non-response, the final sample size became 846.
Multistage sampling technique used to recruit study participants. The study area (Bench-Maji zone) is stratified into five pastoral or semi-pastoral districts and five agrarian districts. This is due to health service coverage and its utilization differs across pastoral and agrarian communities. Then, three districts from each stratum were randomly selected to include at least 30% of the districts in the study. The selected districts were further stratified into kebeles (administrative units below district in Ethiopia). In the same way, 30% of kebeles were selected from each district using simple random sampling technique. The sample was proportionally allocated to each kebele based on the total number of pregnant mothers (Figure 1). Finally, the required sample randomly selected from kebeles that were included in the study by using family folders registry as sampling frame. Family folder is a registry book containing family profiles in the kebele.
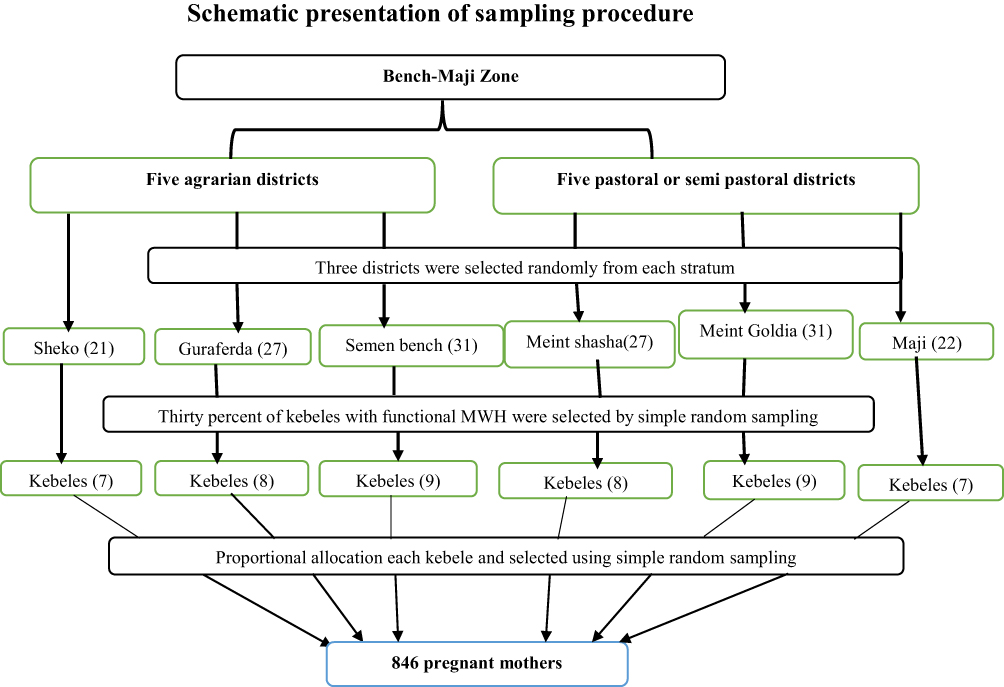 |
Figure 1 Schematic presentation of sampling procedure in assessment of predictors’ intention to use maternity waiting home in Bench Maji Zone, South West Ethiopia, 2018. |
Data Collection Instrument and Procedures
A structured questionnaire was adapted from previously conducted studies and has the following parts, including socio-demographic, obstetric history, attitude, subjective norm, perceived behavioral control, and intention and past experiences of using maternity waiting home.22,29–31 The questionnaire was translated into the local language (Amharic) by persons who are proficient in both languages and have a good knowledge of the subject matter. Then, the questionnaire was pre-tested on a 5% total sample size in a district that was not selected for the actual study. Modifications were made based on pretest finding like sequence, grammatical issues and the time it takes to conduct the study was estimated. In addition, it had used in previously conducted studies the internal consistency was checked for components of theory of planned behavior after the pretest. The cronbach alpha for each item was greater than 0.7 (Table 1). Fifteen experienced BSc public health professionals and three MPH supervisors were recruited and trained for data collection and supervision, respectively. The training was given for 3 days and included how to ensure confidentiality, tool understanding, and interview techniques as training elements. The data were collected through a face-to-face interview and the supervisors and principal investigators supervised the process on a daily basis.
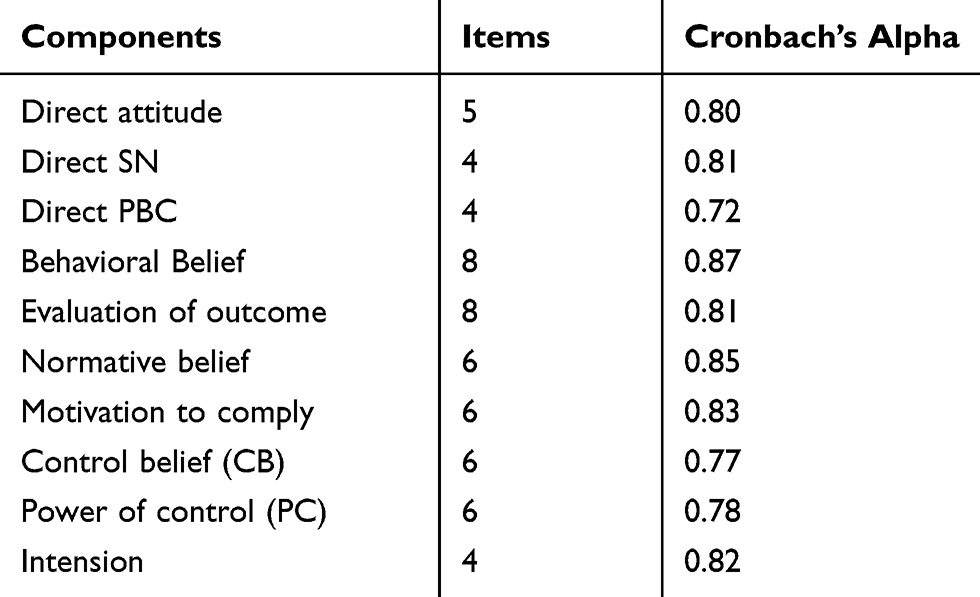 |
Table 1 Internal Consistency of Constructs Theory of Planned Behaviors |
Study Variables
Dependent variable was the intention to use the maternity waiting home. Independent variables were socio-demographic characteristics (age, religion, educational status, occupational status, monthly income, ethnicity, and marital status), ANC visit during the current pregnancy, birth experiences, previous place of delivery, past MWH use, parity, constructs of theory of planned behavior (direct attitude, indirect attitude, direct subjective norm, indirect subjective norm, direct perceived behavioral control, and indirect perceived behavioral control).
Measurements
The intention to use MWH: was measured using four items on 5-point Likert scale responses (strongly agree (5), agree (4), not neutral (3), disagree (2), and strongly disagree (1)). The item scores were summed to give a composite score, and the score approaching the maximum sum score of the total items was considered as a high report of intention to use MWH. The mean of the sum score was also used to categorize the intention as intended and not intended if they were scored at or above mean and below mean, respectively.
The direct attitude toward the use of MWH was measured using five semantic differential scales. Respondents rate their feelings toward staying in WHM for institutional delivery for approximately 15 days before giving birth on bipolar adjectives (bad (1) to good (5), useless (1) to useful (5), unpleasant (1) to pleasant (5), boring (1) to interesting (5)). The score of approaching the maximum sum score was considered a positive attitude toward MWH use.
Behavioral belief: was measured by eight items which answered on 5-point Likert scales (strongly disagree (1) to strongly agree (5)). The respondents asked to rate their beliefs about the outcomes of using MWH. For instances “staying in MWH for institutional delivery helps me to be attended by health professionals, and prevent myself from death related to delivery”
Evaluation of the outcome of MWH uses was measured by eight items that addressed the evaluation consequences using MWH. For instance, a statement “for me getting delivery assisted by health professionals prevent myself from death related to delivery” was rated on five scale ranging from very bad (1) to very good (5). Each behavioral belief item was multiplied by the score of evaluation of the outcome to create a new variable (indirect attitude) that represents the weighted score for each behavioral belief.
Direct subjective norm: was measured by four items Likert scales. The respondents were asked to rate the four statements that address how important persons (husband, father, mother, and health extension worker) in their lives would perceive their stay at MWH for institutional for 15 days before birth on five scales ranging from strongly disagree (1) to strongly agree (5). The four items were summed to form a direct subjective norm score, and the highest score highest influences of the important reference.
Normative belief: was measured by six items, and the response for each item ranged from 1 (strongly disagree) to 5 (strongly agree). The items measure mothers’ beliefs of how important referents think the use of MWH.
Motivation to comply with belief: was assessed using six items, on a 5-point Likert scale. Finally, each item score of normative belief was weighted against the score of motivation to comply with belief, and by summing up all the product scores, the new composite scores of the indirect subjective norm were created.
Direct perceived behavioral control (PBC): was measured using semantic differential scales that address the amount of the control participants perceived regarding MWH. For instance, the statement “staying in MWH for institutional delivery for fifteen days before delivery” was rated on bi-polar differential scales ranging from difficult (1) too easy (5), not under my controls (1) to under my control (5), sudden (1) to planned (5), and conditional (1) to conditional (5). The four items were summed to form the PBC score, and the high score, the less difficult to use MWH.
Control belief: was measured by items that responded on 5-point Likert scale. The control beliefs included the belief that one had sufficient money for transportation or walked a long distance to MWH, getting enough food at MWH, able to stay even alone at MWH, getting a person caring for a family left at home and celebrating traditional ceremony (coffee ceremony) at MWH.
Perceived power: was also measured with six items on 5-point Likert scale. Perceived power was the weighted impact of those control factors in facilitating or inhibiting the behavior (transportation, distance, food, staying alone, the person caring family left in a home, and celebrating valued ceremony). Finally, each item score of control belief was weighted against the score of perceived power, and by summing up all the product scores, the new composite scores of the indirect perceived behavioral control (PBC).
Data Processing and Analysis
Data were entered into the epi data version manager version 4.0.2.101 and exported to SPSS version 21 for analysis. Descriptive statistics such as frequency, percent, mean, and standard deviation were calculated for different variables. The correlations between different TPB constructs were assessed using Pearson’s correlation coefficient. Simple linear regression and multiple hierarchical linear regression analysis was done to identify the predictors of intention to use MWH, and α value of less than 0.05 considered statistically significant. Standardized β coefficients with its confidence interval and R2 values were used to interpret the effects and variability of the dependent variable, respectively.
Results
Socio-Demographic Characteristics
A total of 829 women were interviewed making a response rate of 98%. The mean age of the respondents was 27.1 (±5.2) years. Two hundred fifty (30.2%) of the respondents were from the Bench ethnicity group. Five hundred twenty (64.2%) were protestant in religion. Of the total respondents, 740 (89.3%) were married, 449 (46.7%) did not attend formal education, and 740 (89.3%) were housewife (Table 2).
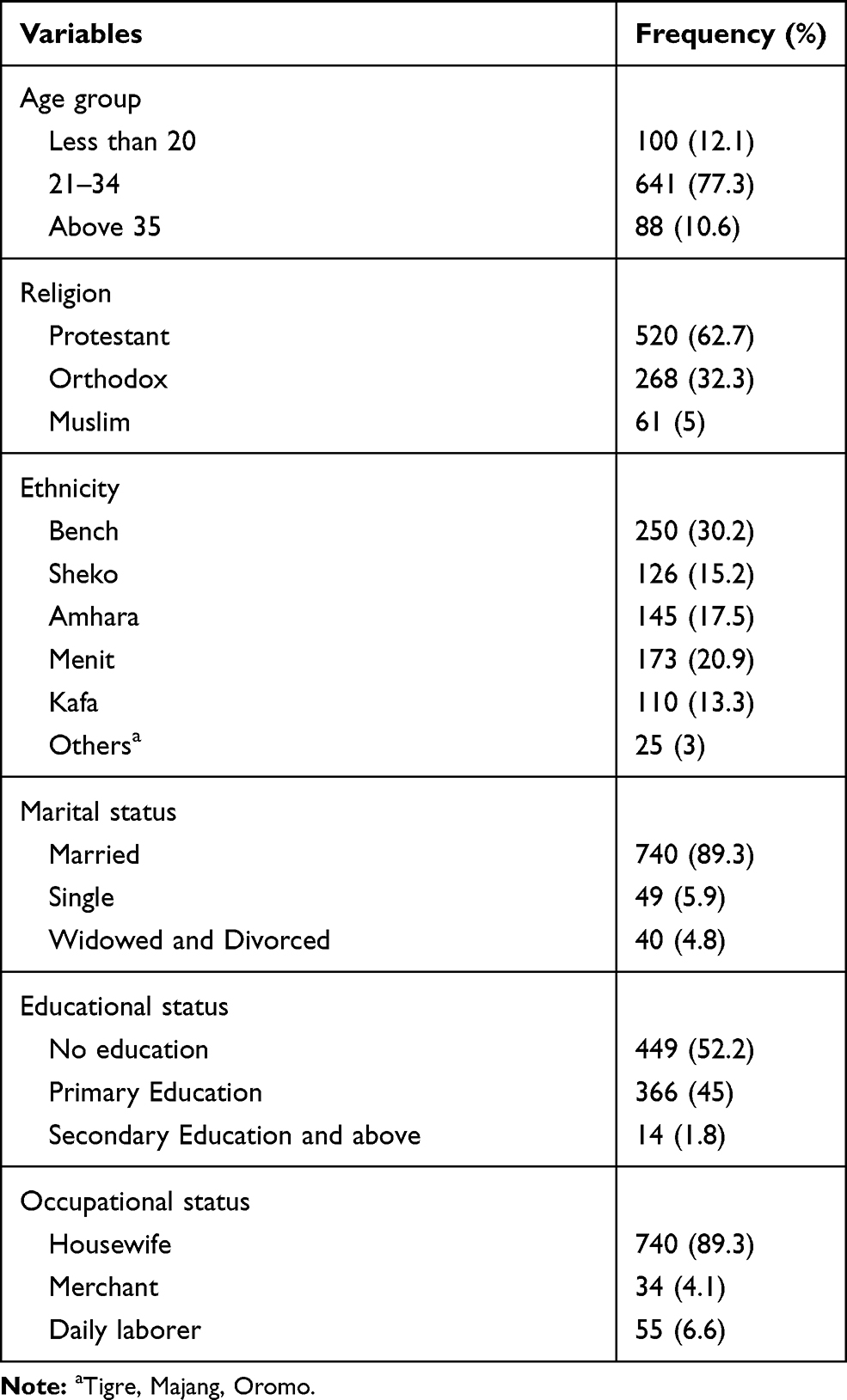 |
Table 2 Socio-Demographic Characteristics of Pregnant Mothers in Bench Maji Zone South West Ethiopia (N=829) October 2018 |
Reproductive Characteristics of the Respondents
The mean age at first marriage was 17.1 (± 4.75) years. Among the total 829 respondents, 641 (77.3%) had a history of childbirth, and 219 (37.6%) of previous pregnancies were delivered at home. Furthermore, 708 (86.7%) of the respondents reported that the current pregnancy was intentional, and 761 (91.8%) had at least one ANC visit during the current pregnancy. Three hundred twenty-three (39%) mothers had a history of previous maternity waiting for home use (Table 3).
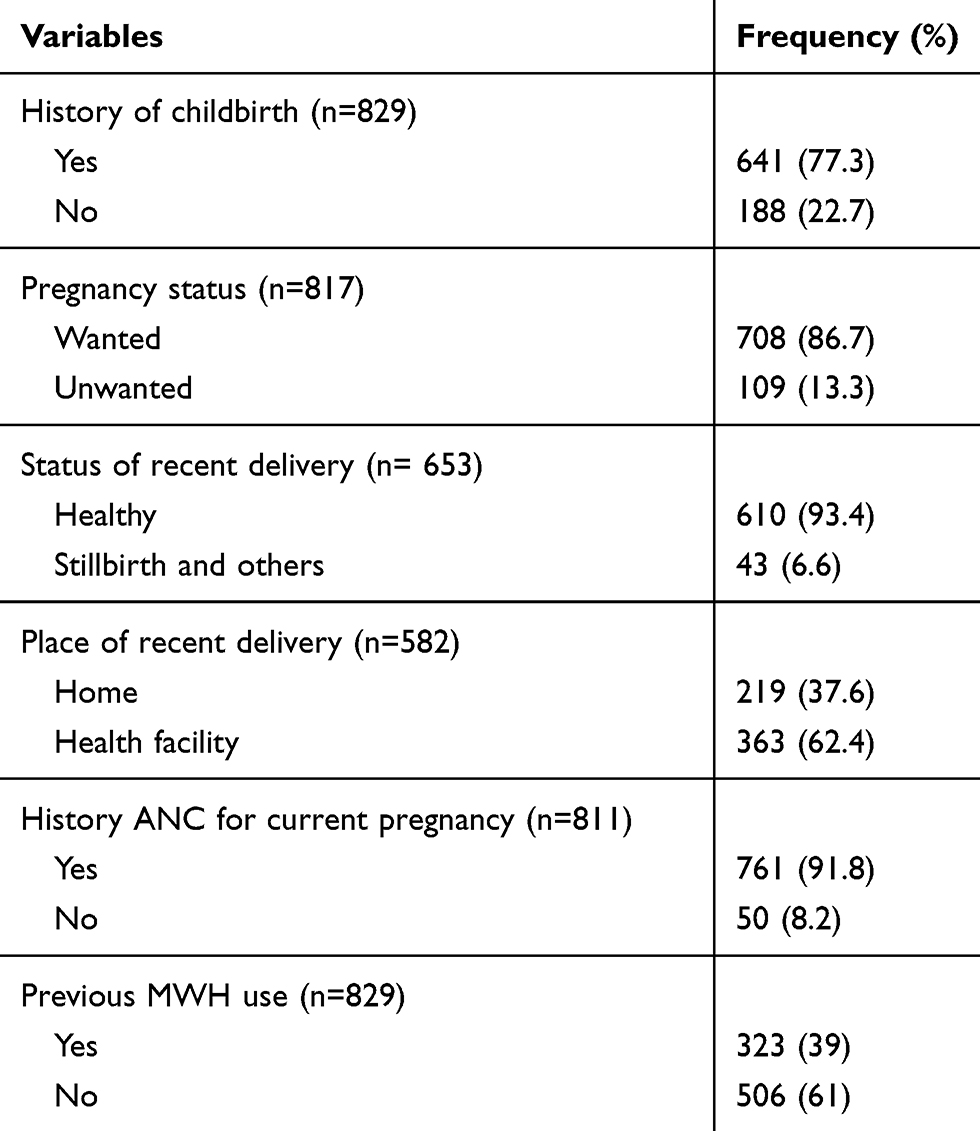 |
Table 3 Reproductive Characteristics of Pregnant Mothers in Bench Maji Zone South West Ethiopia (N=829) October 2018 |
Constructs of the Theory of Planned Behaviors (TPB)
Three hundred fifty-three (42.6%) of the respondents had a behavioral intention to use MWH. Direct attitude, subjective norm, and PBC had mean scores of 15.97 (SD= 3.14), 19.71 (SD= 3.69) and 13.92 (SD= 3.55) respectively. The indirect attitude had a mean score of 135.47 (± 35.94), while the indirect subjective norm had a mean score of 97.78 (± 29.49). The mean score of the indirect perceived behavioral control measure indicated a lower value of 79.21 (± 30.9). There was a higher intention to use maternity waiting among pregnant women (mean score of 14.17 (± 2.38)) (Table 4). Pearson’s correlation coefficients showed that there was a significant correlation among all constructs of the theory of planned behavior. There was a strong correlation between the direct and indirect subjective norm (r= 0.908), intention and indirect subject norm (r=0.935), and intention and indirect perceived behavioral control (r=0.916) (Table 5).
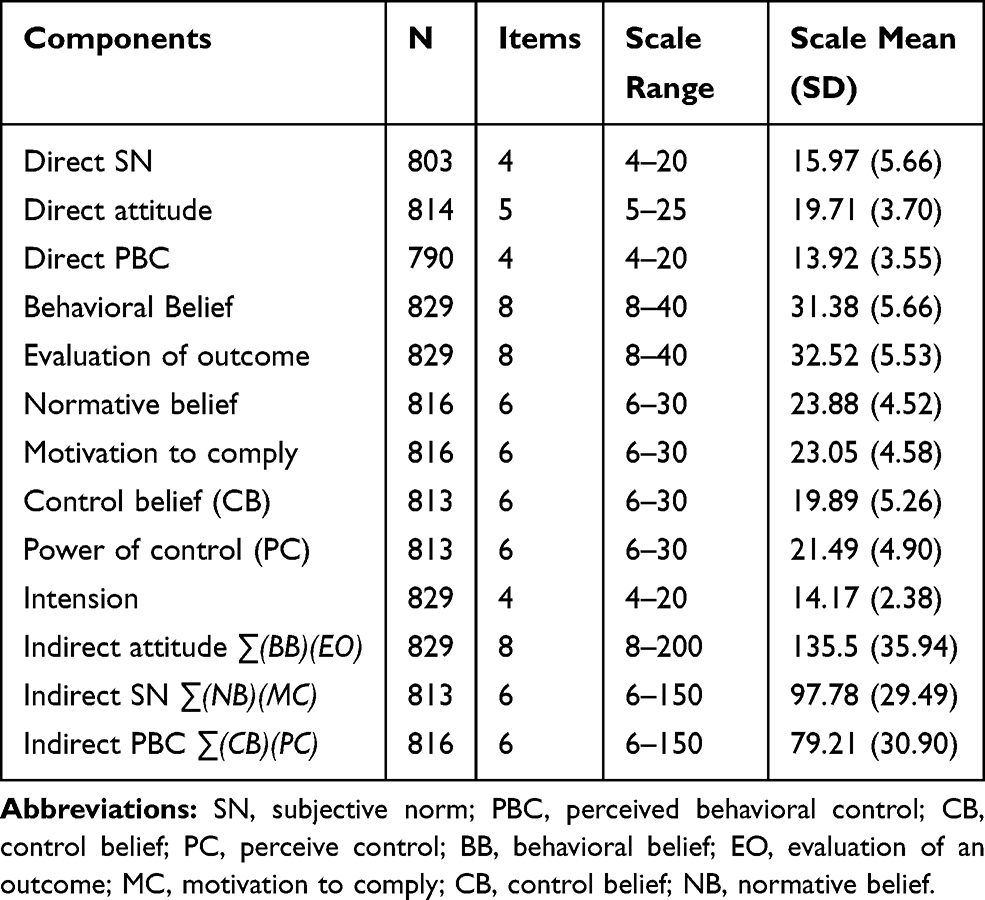 |
Table 4 Descriptive Statistics for the Components of the Theory of Planned Behavior Pregnant Mothers in Bench Maji Zone South West Ethiopia (N=829) October 2018 |
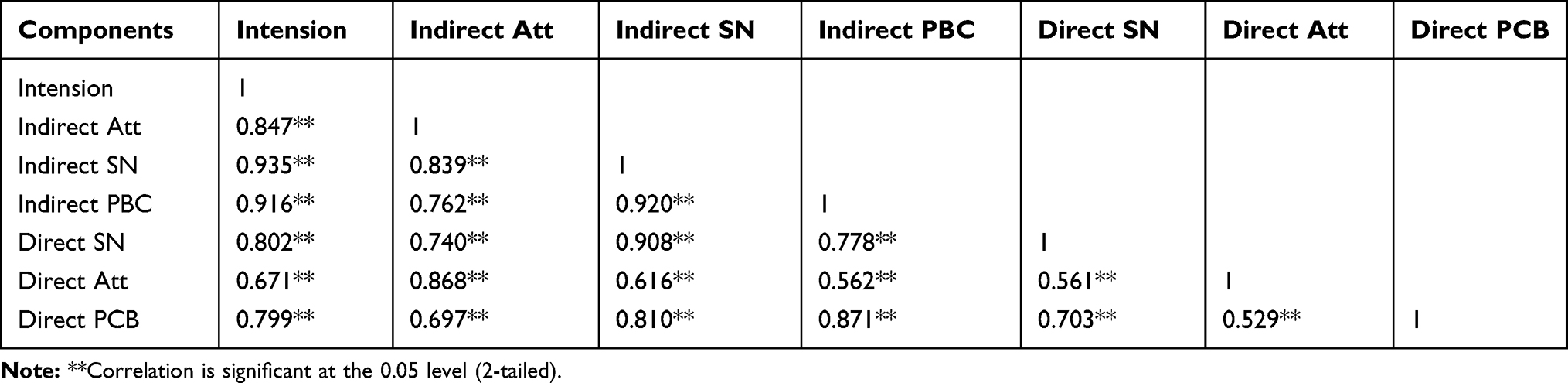 |
Table 5 Partial Correlations Among the Indirect and Direct Measures of TPB, Bench Maji Zone South West Ethiopia (N=829) October 2018 |
Predictors of Intention to Use Maternity Waiting Home
Hierarchical multiple linear regression was done to identify independent predictors of intention to use maternity waiting home. Accordingly, socio-demographic variables (age, educational status, marital status), current pregnancy intention, place of delivery of previous pregnancy, ANC use for current pregnancy, and MWH for previous birth were entered into the first block. The constructs of health theory of planned behavior (direct subjective norm, direct attitude, and direct PCB) were entered into the second block. R square (R2) was calculated to be 81%.
Among the variables included in the model, direct attitude (β =0.12, p<0.001), direct subjective norm (β =0.47, p<0.001), direct perceived behavioral control (β =0.42, p<0.001), and ANC use for the current pregnancy (β =0.07, p=0.030) was significant predictors of behavioral intention. For a positive unit change in the attitude towards the advantage of using maternity waiting home, intention to use MWH will increase by 0.12 units if other variables are kept constant. For a positive unit change in perception that other referents approve the use of MWH, intention to use MWH will increase by 0.47 units, provided that other variables are kept constant. For a positive unit change in perceived control of beliefs on environmental or situational facilitators to use MWH, the intention increases by 0.42 units, provided that other variables are kept constant. Those pregnant women who were using ANC for the current pregnancy had 0.07 units more intention to use MWH than those who had no history of ANC for the current pregnancy (Table 6).
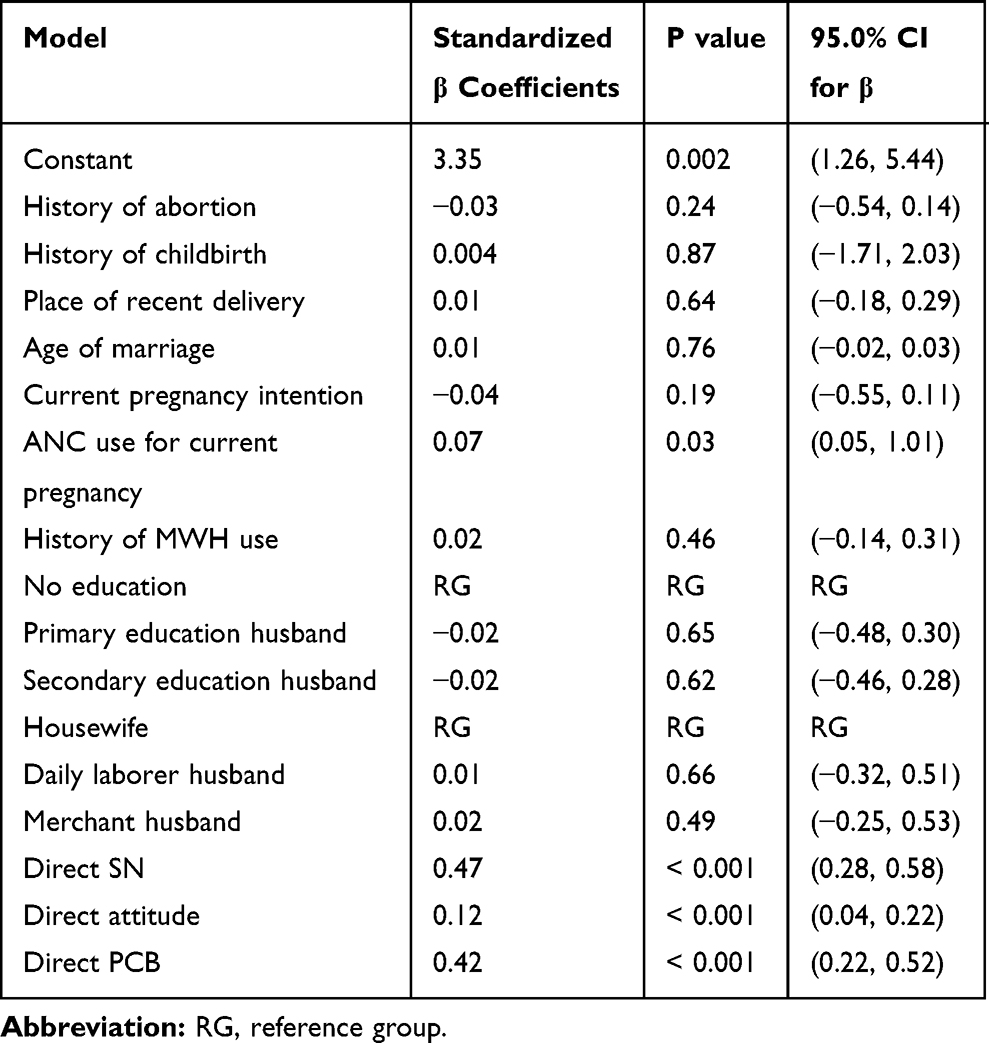 |
Table 6 Predictors of Intention to Use MWH Among Pregnant Mothers on Multivariable Linear Regression Analysis Bench Maji Zone South West Ethiopia (N=829) October 2018 |
Discussion
This study aimed to assess the predictors of intention to use maternity waiting home among pregnant women. Accordingly, the study revealed that ANC utilization, attitude toward MWH, subjective norm, and perceived behavioral control were significant predictors of intention to use MWH. However, none of the socio-demographic variables were associated with intention to use of MWH. Moreover, only 42.6% of the study participants had an intention to use MWH.
Antenatal care use for the current pregnancy was associated with higher behavioral intention. Mothers who had ANC visits might be counseled by health professionals about the use of the maternity waiting home, and plan for the place of delivery; this might be a reason for the association between antenatal care use and behavioral intention. Studies have also shown that ANC use is important for the utilization of other maternal health services32–35 and helps mothers to have access to health information regarding the importance of institutional delivery. This can help women to decide to use MWH to reduce the health and economic consequences of home delivery or delayed arrival at health facility.
Having a favorable attitude toward maternity waiting home is also associated with high behavioral intention. This finding is similar to a study conducted in Gomma woreda, Jimma zone, Southwest Ethiopia.22 Other studies have also shown that the more favorable is the attitude toward certain behavior, the stronger the person’s intention to practice those behaviors.36–38 This finding implies that the interventions that can bring a favorable attitude toward MWH can have a potential to enhance the utilization of the services.
A subjective norm was another important predictor of the intention to use maternity waiting home. This implies that behavioral intention to use MWH is more likely to be influenced by important referent individuals. Thus, interventions that address the involvement of other referents such as husbands, neighbors, fathers, and mothers in law and health extension workers could be helpful to enhance the utilization of MWH and institutional delivery. The use of MWH forces mothers to leave their home and family members for days; as a result, mothers need someone who cares for families left at home. Therefore, assurances of referent others to manage a family issue helps to resolve/minimize the concern of pregnant mothers. Findings from the current study are consistent with reports from other studies.22,39 Likewise, a study conducted in Indonesia showed that subjective norm was a significant predictor of exclusive breastfeeding.40 A study done in Southern Ethiopia also revealed that subjective norm was a predictor of the intention to use cervical cancer screening services.41
The current study also showed that pregnant women who had perceived control over environmental or situational facilitators or inhibitors to use MWH had increased intention to utilize MWH similar to a study conducted in Mettu district, Southwest Ethiopia.39 A study conducted on predictors of intention to use cervical cancer screening services also has shown that perceived behavioral control was a strong predictor of intention to utilize the services.41 This indicates that empowering women against challenges like transportation, food in WHM, and water supply may improve the utilization of MWH.
Conclusion
The intention to use MWH was significantly associated with ANC use, attitude, subjective norm, and perceived behavioral control. Thus, multidimensional interventions that can improve access to, and utilization of ANC, improve the awareness and attitude toward MWH, involve important other, and empowering women are necessary to increase the utilization of MWH.
Abbreviations
ANC, Antenatal Care; MWH, Maternity Waiting Home; TPB, Theory of Planned Behavior.
Data Sharing Statement
All data generated during and/or analyzed during the study are available from the corresponding author on reasonable request.
Ethical Approval
Ethical approval was obtained from the ethical review committee of Mizan Tepi University College of Health Science. Permission letters were obtained from the respective district and kebele administration before data collection. Verbal informed consent was obtained from each participant before beginning the study which was approved by the Ethical Review Committee of Mizan Tepi University College of Health Science. Verbal informed consent was preferred because our study participants were rural mothers where literacy level is low. The study was conducted as per Helsinki declaration.
Acknowledgment
We would like to thank Mizan Tepi University for providing financial support. We would also, like to thank the data collectors, supervisors and study participants.
Funding
The financial fund was covered by Mizan Tepi University. The funding body (Mizan Tepi University) has no role in the design of the study, data collection, analysis of data, interpretation of result, and writing manuscript.
Disclosure
The authors report no conflicts of interest for this work.
References
1. World Health Organization. Trends in maternal mortality: 1990 to 2015. Estimates by WHO, UNICEF. UNFPA, the World Bank and the United Nations Population Division. Geneva: World Health Organization; 2014. Available from: Http://Apps.Who.Int/Iris/Bitstream.
2. WHO. Trends in Maternal Mortality: 1990 to 2015: Estimatesby WHO, UNICEF, UNFPA, World Bank, and the United Nations Population Division. Geneva; 2016.
3. CSA [Ethiopia]and ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2017.
4. WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Trends in Maternal Mortality: 1990 to 2015: Geneva: World Health Organization; 2015.
5. WHO. Strategies Toward Ending Preventable Maternal Mortality (EPMM); 2015.
6. Van Lonkhuijzen L, Stekelenburg J, van Roosmalen J. Maternity waiting facilities for improving maternal and neonatal outcome in low-resource countries (Review); 2009.
7. Dadi TL, Bekele BB, Kasaye HK, Nigussie T. Role of maternity waiting homes in the reduction of maternal death and stillbirth in developing countries and its contribution for maternal death reduction in Ethiopia: a systematic review and meta-analysis 11 medical and health sciences 1117 Public Health. BMC Health Serv Res. 2018;18(1):1–10. doi:10.1186/s12913-018-3559-y
8. Sialubanje C, Massar K, Van Der Pijl MSG, Kirch EM, Hamer DH, Ruiter RAC. Improving access to skilled facility-based delivery services: women’s beliefs on facilitators and barriers to the utilisation of maternity waiting homes in rural Zambia. Reprod Health. 2015;12(1). doi:10.1186/s12978-015-0051-6
9. Meshesha B, Dejene G, Hailemariam T. The role of maternity waiting area in improving obstetric outcomes: a comparative cross-sectional study, Jinka Zonal Hospital, Southern Regional State. J Womens Health Care. 2017;6(6). doi:10.4172/2167-0420.1000406
10. Bekele BB, Dadi TL, Tesfaye T. The significant association between maternity waiting homes utilization and perinatal mortality in Africa: systematic review and meta-analysis. BMC Res Notes. 2019;12(1):1–6. doi:10.1186/s13104-019-4056-z
11. Fogliati P, Straneo M, Mangi S, Azzimonti G, Kisika F, Putoto G. A new use for an old tool: maternity waiting homes to improve equity in rural childbirth care. Results from a cross-sectional hospital and community survey in Tanzania. Health Policy Plan. 2017;32:1354–1360. doi:10.1093/heapol/czx100
12. Lori JR, Williams G, Munro ML, Diallo N, Boyd CJ. It takes a village: a comparative study of maternity waiting homes in rural Liberia. Lancet Glob Health. 2014;2:S11. doi:10.1016/S2214-109X(15)70033-1
13. Kurji J, Gebretsadik LA, Wordofa MA, et al. Factors associated with maternity waiting home use among women in Jimma Zone, Ethiopia: a multilevel cross-sectional analysis. BMJ Open. 2019;9(8):e028210. doi:10.1136/bmjopen-2018-028210
14. Ibrahim S, Handiso T, Jifar M, Yoseph E. Analyzing prevalence of home delivery and associated factors in Anlemo District, Southern Ethiopia. Int Ann Med. 2017;1(6). doi:10.24087/iam.2017.1.6.169
15. Abdella M, Abraha A, Gebre A, Surender Reddy P. Magnitude and associated factors for home delivery among women who gave birth in last 12 months in Ayssaita, Afar, Ethiopia-2016. A community based cross sectional study. Glob J Fertil Res. 2017;2(1):030–039. doi:10.17352/gjfr.000009
16. Tilahun W, Bekana F, Biru A. Magnitude of home delivery and associated factors among antenatal care booked mothers in Delanta District, South Wollo Zone, North East Ethiopia: a cross-sectional study, March 2018. Int J Women’s Health Wellness. 2018;4(2). doi:10.23937/2474-1353/1510086
17. Chernet AG, Dumga KT, Cherie KT. Home delivery practices and associated factors in Ethiopia. J Reprod Infertil. 2019;20(2):102–108.
18. Turchik JA, Gidycz CA. Prediction of sexual risk behaviors in college students using the theory of planned behavior: a prospective analysis. J Soc Clin Psychol. 2012;31(1):1–27. doi:10.1521/jscp.2012.31.1.1
19. Moshi FV, Kibusi SM, Fabian F. Using the theory of planned behaviour to describe male involvement intention during childbirth among expecting. East African Health Res J. 2019;3(1):31–41. doi:10.24248/eahrj.v3i1.596
20. Vermeiden T, Schiffer R, Langhorst J, Klappe N, Asera W, Getnet G. Facilitators for maternity waiting home utilisation at Attat Hospital: a mixed-methods study based on 45 years of experience. Trop Med Int Health. 2018;23(12):1332–1341. doi:10.1111/tmi.13158
21. Lera T, Admasu B, Dirar A. Intention to use institutional delivery and associated factors among ANC attendants in Wollaita Soddo Town, Southern Ethiopia: a cross-sectional community based study, application of theory of planned behavioral model. Am J Public Health Res. 2017;5(4):89–97. doi:10.12691/ajphr-5-4-1
22. Endalew GB, Gebretsadik LA, Gizaw AT. Intention to use maternity waiting home among pregnant women in Jimma District, Southwest Ethiopia. Glob J Med Res. 2016;16(6). doi:10.4172/2155-6113.1222658
23. Imm CM, Holst A, Iversen JM An application of a revised theory of planned behavior: predicting the intention to use personal care products without endocrine disrupting chemicals; 2011.
24. Roncancio AM, Ward KK, Sanchez IA, et al. Using the theory of planned behavior to understand cervical cancer screening among latinas. Health Educ Behav. 2015;42(5):621–626. doi:10.1177/1090198115571364
25. Lawal O, Murphy F, Hogg P, Nightingale J. Health behavioural theories and their application to women ’ s participation in mammography screening. J Med Imaging Radiat Sci. 2017;48(2):122–127. doi:10.1016/j.jmir.2016.12.002
26. Alina T, Ismail T, Abdul W, Wan M, Bakar MI. The extended theory of planned behavior in explaining exclusive breastfeeding intention and behavior among women in Kelantan, Malaysia. Exclus Breastfeed Intent Behav. 2015;1–7. doi:10.4162/nrp.2016.10.1.49
27. Moshi FV, Kibusi SM, Fabian F. Using the theory of planned behavior to explain birth in health facility intention among expecting couples in a rural setting Rukwa Tanzania: a cross-sectional survey. BMC Reprod Health. 2020;17:1–12.
28. Bench Maji zone Health Department. Health Related Report; 2017.
29. Fitzpatrick R. Factors and perceptions that influence women to use a maternal waiting home (MWH) in Ifakara, Tanzania Maaike Josephina van Rijn the Netherlands Master in International Health; September 2013.
30. Waiting M, Officer CH, Province ME. Reducing the number of deaths in pregnancy and childbirth in Zimbabwe; 2010.
31. Elizabeth G, Semrau K, Hamer DH, et al. The influence of quality maternity waiting homes on utilization of facilities for delivery in rural Zambia The influence of quality maternity waiting homes on utilization of facilities for delivery in rural Zambia. Reprod Health. 2017;14(1):68. doi:10.1186/s12978-017-0328-z
32. Ryan BL, Krishnan RJ, Terry A, Thind A. Do four or more antenatal care visits increase skilled birth attendant use and institutional delivery in Bangladesh? A propensity-score matched analysis. BMC Public Health. 2019;19(1):1–6. doi:10.1186/s12889-019-6945-4
33. Fekadu A, Yitayal M, Alemayehu GA, et al. Frequent antenatal care visits increase institutional delivery at Dabat health and demographic surveillance system site, Northwest Ethiopia. J Pregnancy. 2019;2019:1–6. doi:10.1155/2019/1690986
34. Melaku YA, Weldearegawi B, Tesfay FH, et al. Poor linkages in maternal health care services’ evidence on antenatal care and institutional delivery from a community-based longitudinal study in Tigray region, Ethiopia. BMC Pregnancy Childbirth. 2014;14(1):1–13. doi:10.1186/s12884-014-0418-7
35. Bayu H, Adefris M, Amano A, Abuhay M. Pregnant women’s preference and factors associated with institutional delivery service utilization in Debra Markos Town, North West Ethiopia: a community based follow up study. BMC Pregnancy Childbirth. 2015;15(1):1–9. doi:10.1186/s12884-015-0437-z
36. Karen G, Barbara K, Rimer K. Health Education and Health Promotion: Theory, Research and Practice.
37. Moshi FV, Kibusi SM, Fabian F. Using the theory of planned behavior to explain expecting couples birth preparedness intentions in a rural setting: a cross-sectional study from Rukwa, Southern Tanzania. Adv Public Health. 2018;2018.
38. Alina T, Ismail T, Abdul W, Wan M, Bakar MI. The extended theory of planned behavior in explaining exclusive breastfeeding intention and behavior among women in Kelantan, Malaysia. Nutr Res Pract. 2016;10(1):49–55. doi:10.4162/nrp.2016.10.1.49
39. Yismaw W Intention to use maternity waiting home among pregnant women in Mettu district, southwest Ethiopia; 2018.
40. Sulaeman ES, Murti B, Setyawan H, Rinawati S. Exclusive breastfeeding behavior model in rural Central Java, Indonesia: the application of theory of planned behavior. Glob J Health Sci. 2018;10(10):35–49. doi:10.5539/gjhs.v10n10p35
41. Abamecha F, Tena A, Kiros G. Psychographic predictors of intention to use cervical cancer screening services among women attending maternal and child health services in Southern Ethiopia: the theory of planned behavior (TPB) perspective. BMC Public Health. 2019;19(1):434.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.