")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Predictors of Intention to Get a COVID-19 Vaccine of Health Science Students: A Cross-Sectional Study
Authors Nguyen VT , Nguyen MQ , Le NT, Nguyen TNH , Huynh G
Received 13 July 2021
Accepted for publication 4 September 2021
Published 24 September 2021 Volume 2021:14 Pages 4023—4030
DOI https://doi.org/10.2147/RMHP.S328665
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Van Tap Nguyen, 1 Minh Quan Nguyen, 2 Ngoc Thi Le, 3 Thi Ngoc Han Nguyen, 4 Giao Huynh 5
1Faculty of Medicine, Tra Vinh University, Tra Vinh City, Tra Vinh Province, Vietnam; 2Department of Scientific Research, Thu Duc District Hospital, Ho Chi Minh City, Vietnam; 3Health Management Training Institute, Hanoi University of Public Health, Hanoi City, Vietnam; 4Infection Control Department, University Medical Center at Ho Chi Minh City, Ho Chi Minh City, Vietnam; 5Faculty of Public Health, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam
Correspondence: Minh Quan Nguyen
Department of Scientific Research, Thu Duc District Hospital, 29 Phu Chau St, Thu Duc City, Ho Chi Minh City, Vietnam
Tel +84 799835555
Email [email protected]
Background: Vaccination is one of the interventions that can be employed to control coronavirus disease (COVID-19). The aim of this study is to identify factors that affect vaccination intention among health science students, by using the health belief model (HBM) as a theoretical framework.
Methods: This study was undertaken in April 2021 using a convenience sample strategy among health science students in Tra Vinh University, which is a university in South Vietnam. Participants were required to complete the self-report questionnaire. All data were calculated by using STATA 14 software, to determine the factors associated with COVID-19 vaccine acceptance, a multivariable logistic regression analysis was performed, along with odds ratio (OR) and 95% confidence interval (95% CI).
Results: A total of 412 eligible participants were taken part in the study, with a questionnaire response rate of 48.2%, reporting that 77.7% of participants intended to receive a COVID-19 vaccination when available. An overall score of knowledge was 7.8 ± 1.5 (range 0– 10), a positive attitude toward vaccination including perceived susceptibility and severity (3.1 ± 0.7), perceived benefits (3.1 ± 0.7) and cues to action (4.0 ± 0.6). Determinants of willingness to get a COVID-19 vaccination included their field of education, knowledge and factors in HBM model including perceived susceptibility and severity, perceived benefits and cues to action (all p < 0.05). In contrast, perceived barriers had a negative association with the probability of vaccine acceptance (p < 0.05). The study did indicate a number of participants not willing to receive a vaccination due to, mainly, safety (67.4%), development issues (58.7%) and side effects (79.3%).
Conclusion: The theoretical framework recognized factors that influence vaccine acceptance. These are considered evidence for the development of planning strategies to optimize the vaccination uptake and offer success in vaccination campaigns for both health science students and the general population.
Keywords: COVID-19 vaccine, health science, student, intention, Vietnam
A Letter to the Editor has been published for this article.
Introduction
Since the first case was confirmed in December 2019, the coronavirus disease 2019 (COVID-19) pandemic has caused an unprecedented public health crisis and the disruption of healthcare systems and economies, globally.1,2 Long COVID-19 positive cases have been frequently reported among COVID-19 survivors causing a potential long-term burden on health services across the country.3 The emergence of the new variants have been documented, especially the Delta Variant, which has demonstrated the highly infectious nature of the virus and prolonged the pandemic around the world.4 As of 18 June 2021, over 177 million confirmed cases have been reported, resulting in over 3.8 million deaths across the globe.5 South-East Asia has continuously reported high case numbers of COVID-19, with about 33 million cases and 466,989 deaths. In Vietnam, there were 12,231 confirmed cases with 61 deaths, with the South of Vietnam recording a low number of infections.6
Until now, there is no specific treatment for COVID-19, with some chemotherapeutic or biologic therapies have been used to support patients.7,8 Individuals infected by the virus may be experienced changeable symptoms ranging from no symptoms to mild or severe symptoms including fever, dry cough, fatigue, diarrhea, loss of taste or smell, difficulty breathing, chest pain and so on.9,10 Older people and those with chronic conditions were found to be at high risk of becoming severely ill from COVID-19.11
At the beginning of the pandemic, numerous prevention measures had been applied to control the spread, including restrictions like lockdowns, school or factory closures or adherence to several preventive behaviors such as washing hands, wearing masks, avoiding public places and social distancing.9 Previous studies showed that knowledge towards COVID-19, such as the cause of the disease, symptoms, treatments and preventive measures, are important when applying preventive practices.12,13 However, our earlier study indicated that the rate of knowledge among 551 students was relatively low (49.0%) and only 41% indicated good practices.13 Besides, a remarkable rate of infected individuals in the community have reported no symptoms whilst being COVID-19 positive, thus they are likely to be able to transmit the virus to another individuals. The emergence of vaccines has offered hope in controlling the rapid spread of COVID-19. Some vaccine brands have showed high efficacy and have been approved for emergency use in many countries. These brands include Pfizer-BioNTech, Moderna, and AstraZeneca.14 In Vietnam, a total of 2,034,781 vaccine doses have been administered thanks to the COVID-19 Vaccines Global Access Program (COVAX).6 This is in addition to the Government continuously trying to provide vaccines to ensure the vaccination of the entire population.
Nevertheless, vaccination hesitancy is one of the major obstacles to achieving herd immunity, with several factors being identified, such as trust in the benefits of the vaccine and the ability of access to the vaccine.15 A study among US medical student reported that 23% of them were unwilling to get vaccinated although they were at high risk of exposure to the virus.16 Furthermore, our prior study showed that a there was a remarkable rate of unwillingness to get vaccinated among medical staff and high-risk populations.17,18 Previous studies have reported factors associated with COVID-19 vaccine acceptance. These reports included Wagner et al, who found that the pandemic has led to many individuals losing their jobs or having a reduced income, plus identified factors associated with vaccine acceptance or planning to vaccinated, such as experiences attained from personal, family/friend, and media.19 In Indonesia, Harapan et al found that being a healthcare worker and having a higher perceived risk of COVID-19 infection was associated with higher acceptance for a COVID-19 vaccine.20
Vietnam began its fourth wave of the pandemic, June 2021, and medical students are now an important source of support in health communication, and for front line health workers. At present, the Government has been implementing mass COVID-19 vaccination strategies with a priority vaccination available to the anti-epidemic force and high-risk populations including the elderly and chronically ill patients. At the time of survey, students were considered one of the priorities for receiving a COVID-19 vaccination, but they are still not being vaccinated against COVID-19 in Vietnam. Therefore, it is essential to investigate the acceptance of a COVID-19 vaccination amongst health science students, to determine the factors and barriers affected to the decision to receive a COVID-19 vaccine or not, thus encourage vaccine uptake to control the spread of the pandemic.
Methods
Study Population
A cross-sectional study was performed in April 2021 using a convenience sample strategy of all health science students in Tra Vinh University. A sample size was based on the estimated rate of intention to get a COVID-19 vaccine among healthcare worker from a previous study, being 76.1%, with a power of 0.8 and an alpha of 5%.17 The minimum sample size was 280.
Inclusion and Exclusion Criteria
All students were included in this study that submitted the questionnaire within the time limit of the survey. Students who did not complete the survey, or missed any questions in the areas of knowledge, attitude and acceptance of the vaccine, were excluded from the study.
Data Collection Procedures
Students, during their face-to-face lessons, were invited by the researchers to participate the survey. The data were collected through a self-administered questionnaire. The questionnaire took approximately 10 to 15 minutes to complete. All students had been informed about the aim of the study and signed the consent form before partaking in the study, and their answers were anonymous. Among a total of 850 health science students at the University, only 410 participants completed and returned the fully questionnaire. This was a response rate of 48.2%.
Measures
The questionnaire comprised 30 items, which was structured into four dimensions: (1) demographics of students such as age, gender, religion, education field, year of education, and source of information on COVID-19 vaccines; (2) Knowledge towards COVID-19 including ten items, which was developed and validated according to the study of Huynh G et al among healthcare workers and high-risk people which focused on Knowledge, Attitude, and Practices (KAP) related to COVID-19 in Vietnam;12,21 (3) Attitudes regarding vaccination that consisted of 12 items using a 5-point Likert scale with responses ranging from strongly disagree through strongly agree. The instrument has been assessed as reliable and valid in previous studies with cronbach’s alpha being 0.765;22 and (4) intention to receive a future COVID-19 vaccine was measured using item: “Will you intend to get a COVID-19 vaccination when it becomes available”, with responses yes or no being available. Participants who had answers of “no” to item of dimension 4 were asked an additional item explaining their reasoning for not accepting a vaccine (Appendix 1).
Statistical Analysis
Each correct answer, relating to knowledge, recorded one point, with an incorrect answer being given zero. An overall knowledge score was calculated by the sum of 10 items which ranged from 0 through 10. Relating to attitudes, the answers were marked by one point for strongly disagree to five points for strongly agree. The mean scores of each dimension were computed separately, for components of Susceptibility and Severity (4 items), Benefits of vaccination (3 items), and Cues to action (2 items), with the higher the mean scores suggesting the higher the possibility of positive attitudes, except for Barriers (3 items), that had a reverse association. The main outcome of the study was to identify the intention to get a COVID-19 vaccine recorded yes or no.
All data assessment was performed by using STATA 14 software. The characteristic demographics, knowledge, and attitudes were classified as the independent variables. Vaccination acceptance was considered the dependent variable. Categorical variables were computed as frequencies and percentages, while continuous variables were described as mean and standard deviation (SD). The univariate analysis was performed using Chi-square or Fisher’s exact test for categorical variables and t-test for continuous variables. The multivariable logistic regression analysis was followed to describe the determinants of COVID-19 vaccine acceptance. The odds ratio (OR) values and their 95% confidence intervals (95% CI) were reported, with a p-value of less than 0.05, which was considered statistically significant.
Ethical Approval
Our research complied with the Declaration of Helsinki. All participants agreed and gave informed consent before participating. The protocols of the study were approved by the Ethics Council of the University of Medicine and Pharmacy at Ho Chi Minh City (Protocol number 27/UMP-BOARD).
Results
Demographic Characteristics of Students
Overall 412 students, from first to sixth-year, completed the questionnaire, whose mean age was 22.5±2.8 years, with more than a half of them being female (54.1%). Their field of education included, mainly, general medicine (53.2%). The majority of information on the COVID-19 vaccines were received through social media and television (83.0% and 80.6%, respectively). The rate of vaccination acceptance was fairly high (77.7%) (Table 1).
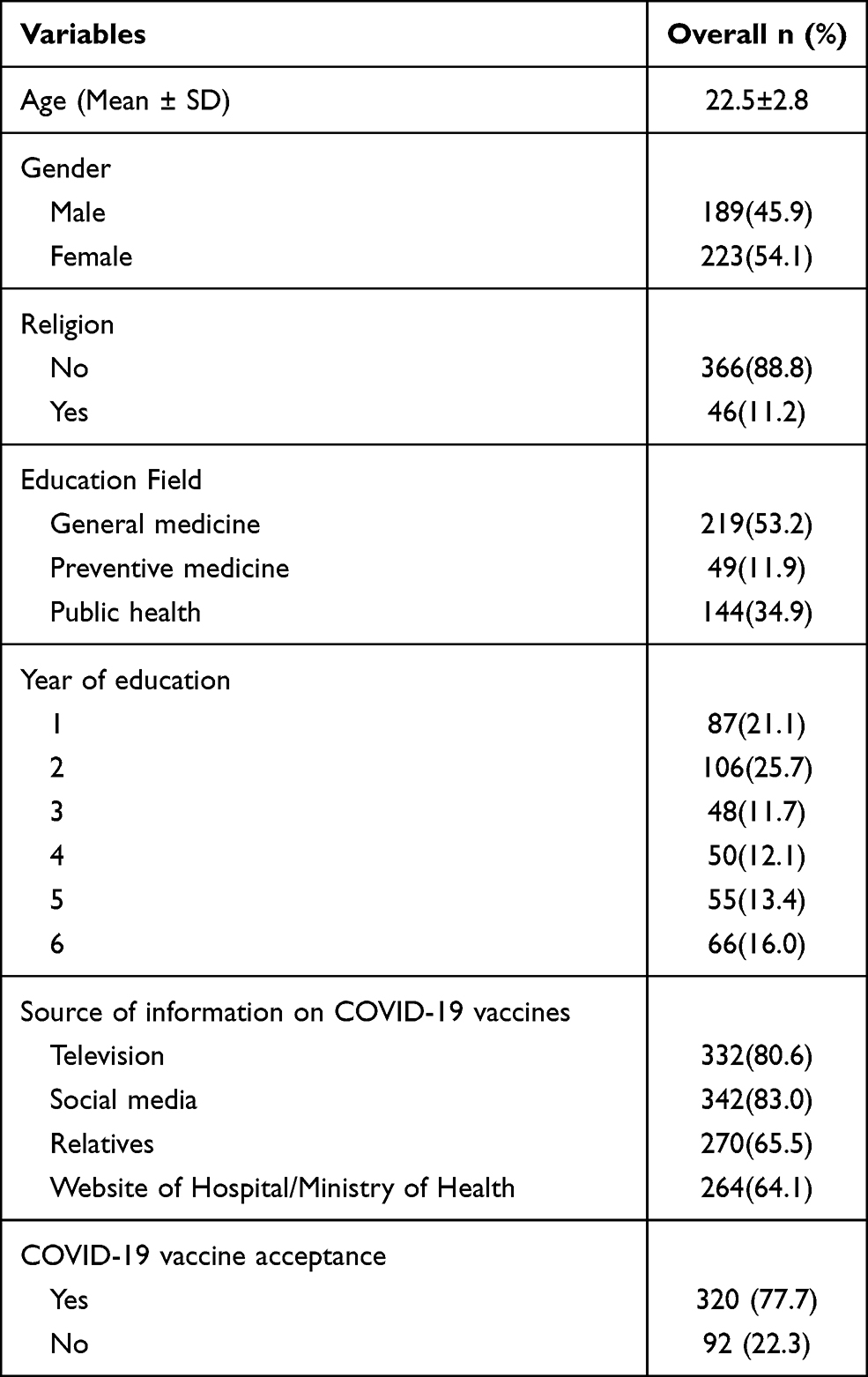 |
Table 1 Demographics and COVID-19 Vaccine Acceptance (N= 412) |
Knowledge and Attitudes Toward the COVID-19
Table 2 shows most students had good knowledge about COVID-19, ranging from 71.1% to 98.1% in all areas including cause, common symptoms, the isolation period, treatment approaches, preventive measures, high-risk subjects and the dangers of COVID-19. At the negative end, the participants did not report a good level of knowledge in relation to ways of COVID-19 transmission and availability of a vaccine, showing a low percentage of correct knowledge (51.1% and 40.8%, respectively). The overall knowledge score was 7.8 ± 1.5 (ranging from 0 to 10). Most participants believed that they were at risk and COVID-19 was a serious illness (3.1 ± 0.7), also they believed the Benefits of vaccination outweighed the Barriers of vaccination, with mean scores of 3.1 ± 0.7 and 2.4± 0.5, respectively, and the majority of them had a high level of Cues to action (4.0 ± 0.6) (ranging 1 to 5).
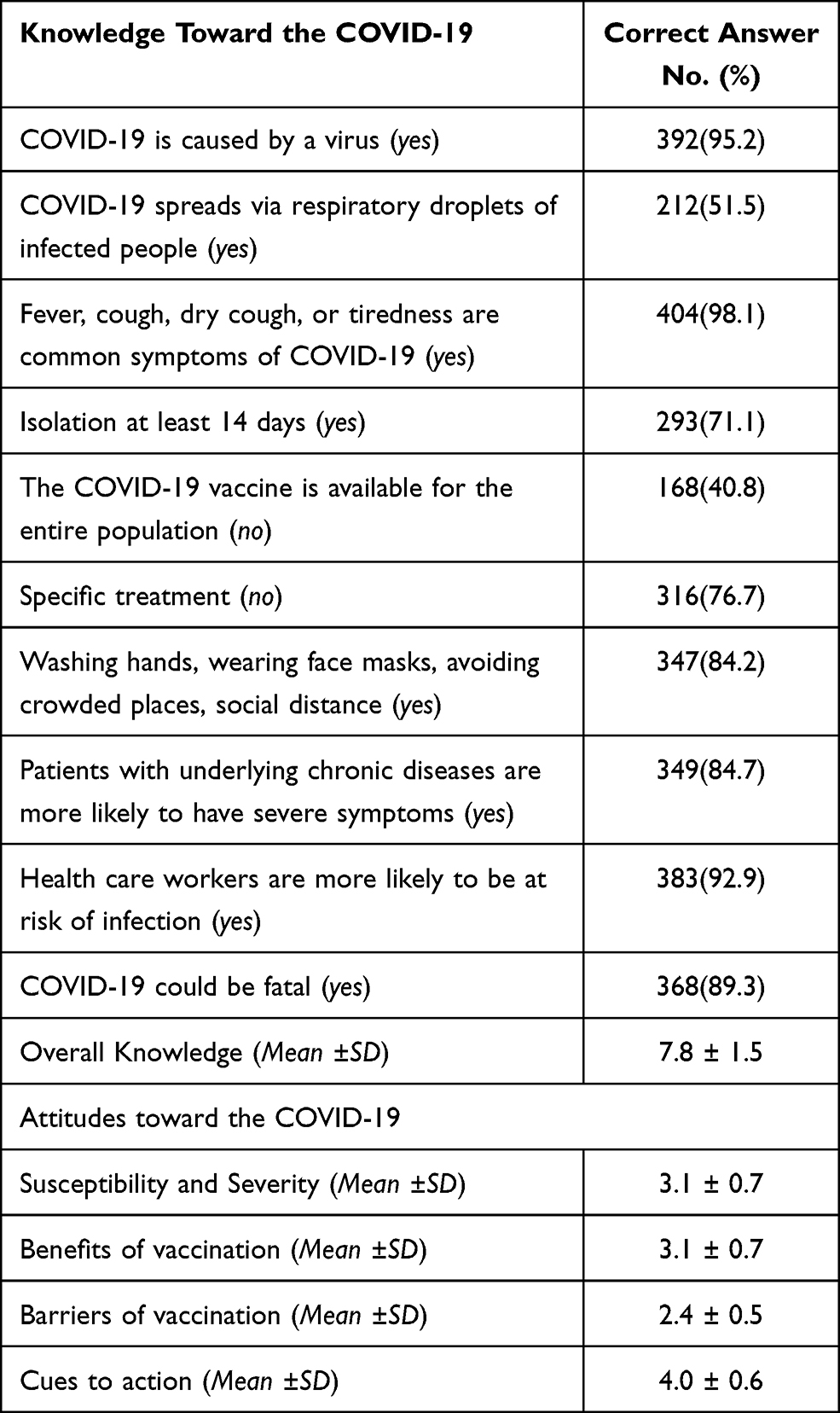 |
Table 2 Knowledge and Attitudes Toward the COVID-19 (N=412) |
Factors Associated with Vaccination Acceptance in the Univariate Analysis
There was a relationship between the demographics including field of education, year of education, and source of information of the COVID-19 vaccines and vaccination acceptance (p < 0.05). In terms of knowledge and attitude, there was an association between vaccination intention and knowledge (p < 0.05), as well as all four domains of attitudes toward vaccination (all p < 0.001) (Table 3).
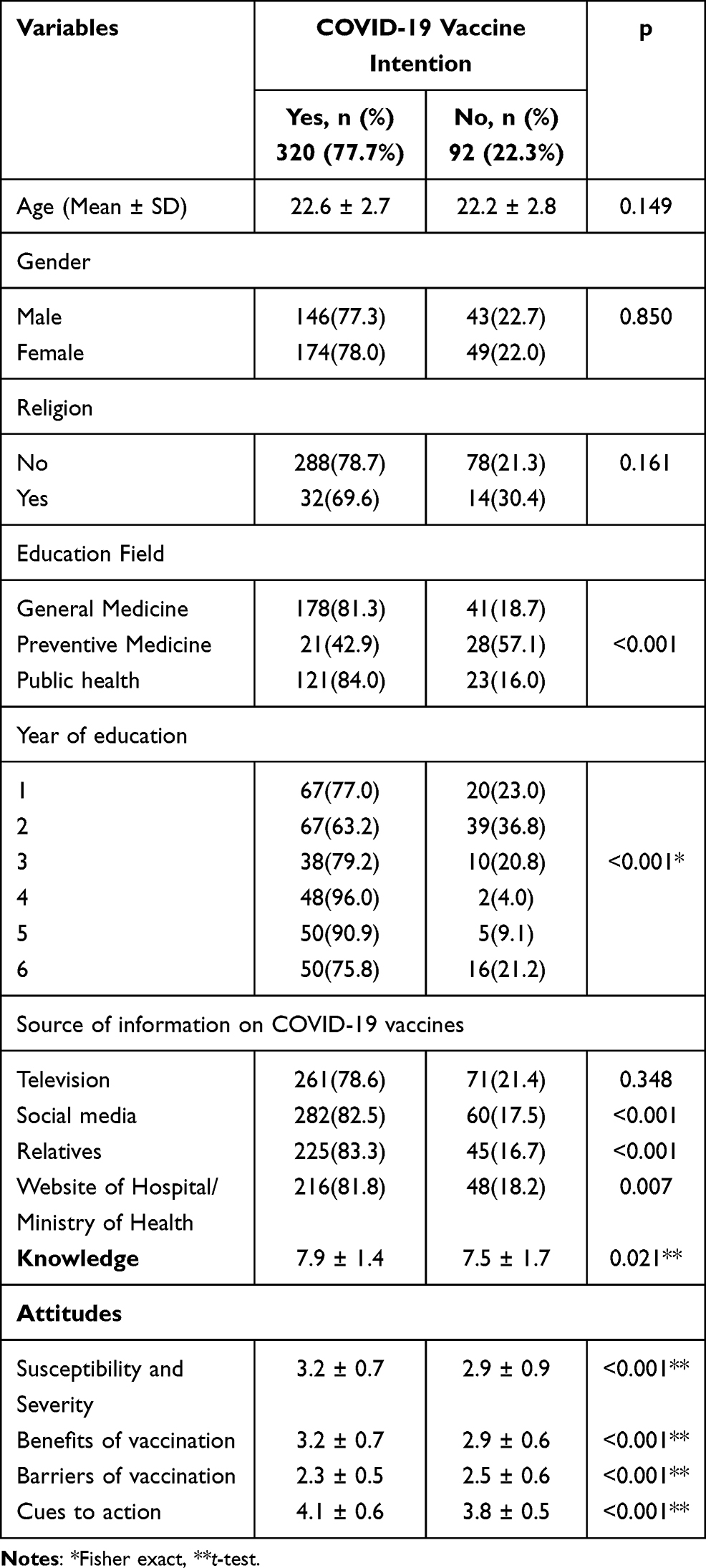 |
Table 3 Factors Associated with Vaccination Acceptance in Univariate Analysis (N= 412) |
Determinants of a COVID-19 Vaccination Acceptance in Multivariable Logistic Analysis
Factors associated with COVID-19 vaccine acceptance in the multivariable logistic analysis were presented in Table 4, with the findings showing the field of education was associated with vaccine acceptance (p < 0.001), and high intention was statistically associated with good knowledge (OR = 1.3, 95% CI [1.04, 1.57], p < 0.05). Besides, participants were more likely to plan to get the vaccination if they had a positive attitude towards the Susceptibility and Severity (OR = 1.5, 95% CI [1.03, 2.16], p < 0.05), Benefits of vaccination (OR = 1.9, 95% CI [1.31, 2.98], p < 0.05), and Cues to Action (OR = 2.1, 95% CI [1.29, 3.49], p < 0.05), except for Barriers that had a negative association with the probability of vaccine acceptance (OR = 0.4, 95% CI [0.26, 0.76], p < 0.05).
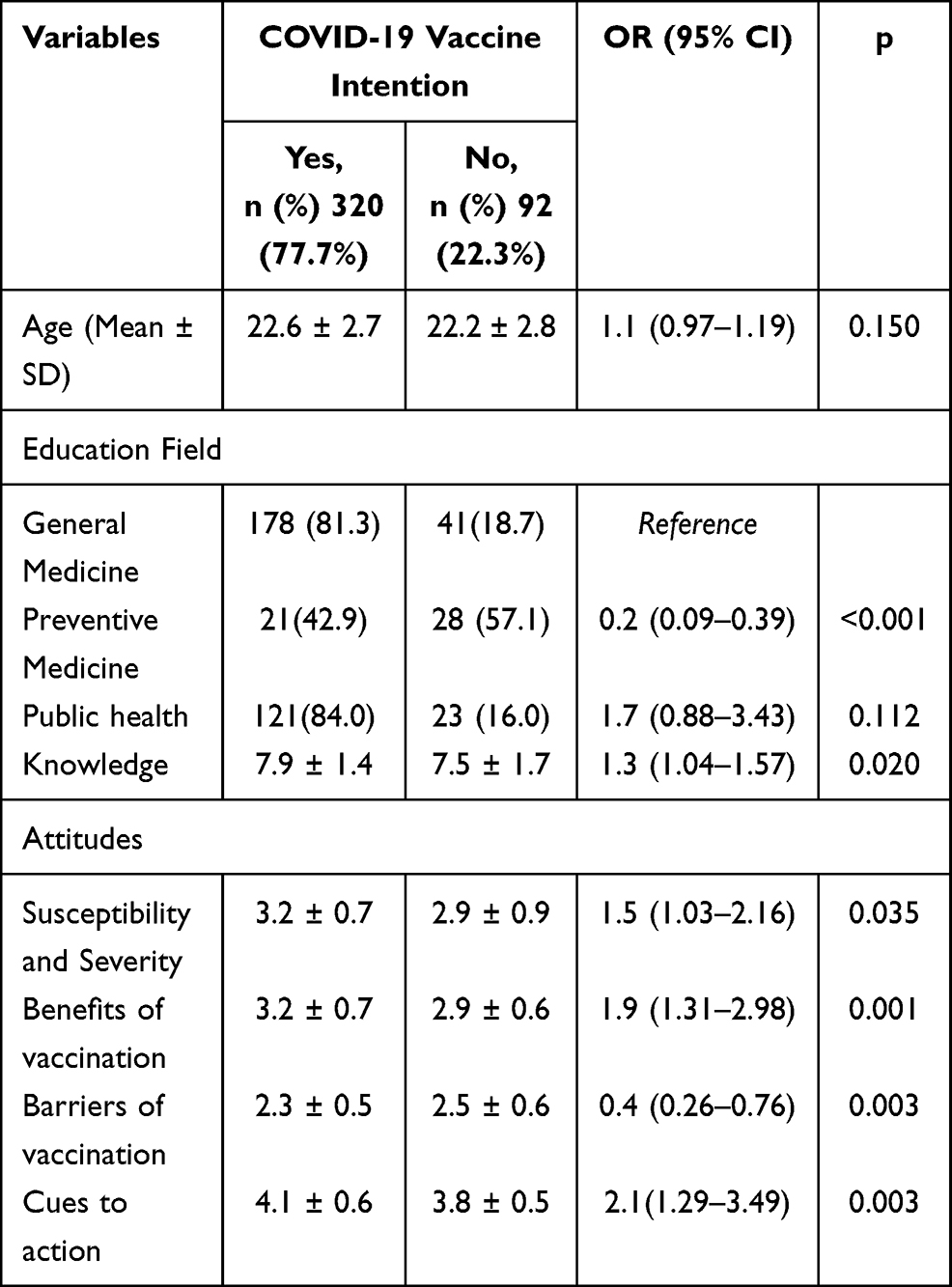 |
Table 4 Multivariable Logistic Analysis of Factors Associated with COVID-19 Vaccine Acceptance (N= 412) |
Reasons for COVID-19 Vaccine Hesitancy
Among participants who did not accept a COVID-19 vaccine, the main reasons included being afraid of the side effects (79.3%), a desire to delay and follow up on the safety of the vaccine (67.4%), and afraid of the process of new vaccine development (58.7%). A lesser number of students (<50%) reported reasons for hesitancy that the vaccine could lead to illness (46.7%), concerned about the expensive vaccination costs (46.7%), having a plan to use other preventive measures (39.1%), not considered themselves in the high-risk group (39.1%), afraid of needles (11.9%), do not trust the government (11.9%), and vaccines are not effective (8.7%) (Table 5).
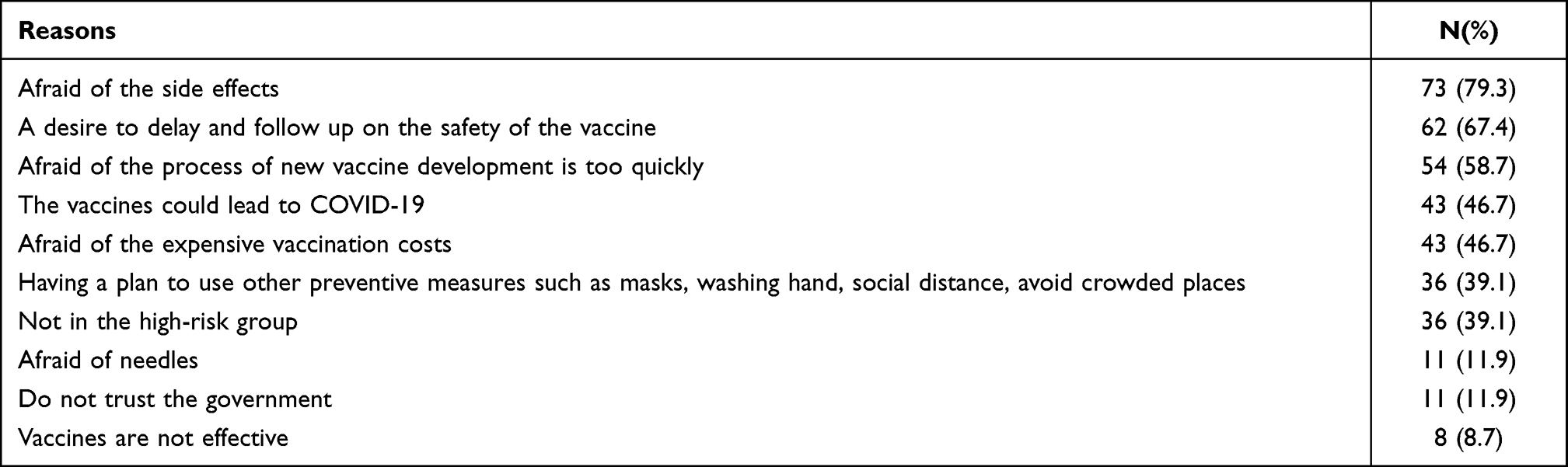 |
Table 5 Reasons for COVID-19 Vaccine Hesitancy (n=92) |
Discussion
This study highlights Vietnamese health science students’ acceptance of COVID-19 vaccines, and associated factors in the background, whilst being faced with the fourth wave of COVID-19 and the number of confirmed cases increasing daily. The emergence of the efficacy and availability of the vaccine plays an essential role in arresting the pandemic. However, vaccine hesitancy has been recorded as a concerning issue around the world, which may affect the success of herd immunity.23
In this study, we found that there was a high level of knowledge, attitude and the acceptance of COVID-19 vaccines. This study reported 77.7% of the participants were willing to receive the vaccine. These results are in line with those of previous studies that showed 76.1% of healthcare workers and 84% of the high-risk population had a willingness to obtain the vaccine.17,18 In contrast, this finding is higher than prior studies conducted in medical students in other countries such as Uganda (37.3%),24 Egypt (35%),25 and US dental students (56%).26 We found that over one-fifth of participants were hesitant about the vaccine. The main reasons reported included being afraid of the side effects (79.3%), a desire to delay and follow up the safety of the vaccine (67.4%), and afraid of the process of new vaccine development occurring too quickly (58.7%). These findings are in agreement with those of earlier surveys that showed people were concerned about the side effects and safety of the vaccine (29.8%), intent to receive the vaccine later if it is safe (14.5%) and afraid the development of the vaccine being too quick (10.4%).27 Moreover, the aspect of safety and side effects of the vaccine are also considered in various previous studies.16,25 At present, vaccination plays an important role in protecting the health of the population and reduce the devastating consequences of the virus. Interventions should be applied to ensure the trust of the vaccine and enhance the acceptance among health science students due to them being an important force in assisting the health care response teams in communities.
In terms of knowledge, we found that most students had good knowledge with an overall score of 7.8 ± 1.5 (ranging from 0 to 10). These results showed the effectiveness of health education programs, which helped to improve knowledge among health sciences students in Vietnam, compared to our prior study in the early period of the pandemic.13 Moreover, students who had good knowledge also were more likely to have an acceptance of the vaccine. We hope that the adequate levels of knowledge towards COVID-19, which lead to efficient implementation of immunization strategies, bring greater benefits over the course of this pandemic. However, the health education programs should be continuously promoted to enhance the practice of preventive behaviors, even if the majority of people have been vaccinated, because previous data reported the increase of COVID-19 cases after personal preventives behaviors were loosened.28
Regarding attitude, participants were more likely to plan to receive a vaccination if they had a positive attitude towards Susceptibility and Severity. This is consistent with Evridiki et al who showed that participants who had high risk perceptions regarding COVID-19, were likely to accept the vaccine.29 Moreover, students who perceive the benefits of vaccination are more likely to be vaccinated. This result matches those observed in our earlier study among healthcare workers, implying that willingness to receive vaccines relies on personal risk and benefit perception.17 It is possible, therefore, that it is necessary to enhance the perceived risk and severity of COVID-19, as well as emphasize the benefits of the vaccine. On the subject of Cues to Action, significant elements increased the acceptance of vaccines. These observations are in line with our previous studies,17,18 which suggest that recommendation from the Ministry of Health, Healthcare Providers and the Government, being an element to promote the willingness of vaccination. In contrast, Barriers to receive vaccination were negatively associated with the probability of vaccine acceptance. These results are consistent with data obtained in prior studies.17,18,30 Therefore, interventions should be focused on declining barriers such as costs, inconvenience and side effects to improve vaccine acceptance.
Strengths and Limitation
Some limitations need to be considered when interpreting the results. Firstly, this study used convenience sampling to collect data in one of the universities located in the South of Vietnam, which may be lead to limits of generalizability of the results. Secondly, a cross-sectional observation can limit to derive causal conclusions between the willingness to receive the vaccine and associated factors. Thirdly, this study was conducted before the vaccine was available, so information about the effectiveness and safety of vaccine was not yet clear, thus the rate of intention to vaccinate could differ when the vaccine became available. However, our findings could serve as a foundation for the planning and development of vaccine strategies among students who are an important group to support a country’s health system.
Conclusion
These findings highlighted the intention to receive a COVID-19 vaccine among health science students, which was relatively high. The study did indicate a number of participants not willing to receive a vaccination due to, mainly, safety, development issues and side effects. The use of the theoretical framework recognizes factors that influence vaccine acceptance, which included high Susceptibility and Severity, Benefits, Barriers and Cues to Action. These are evidence that indicates the need for planning of campaigns to promote the vaccine as a priority solution for health science students.
Data Sharing Statement
Available upon request to the corresponding author.
Acknowledgments
We thank the administrators and all the students at Tra Vinh University for the time and effort they devoted to this study. We also thank Raymond A Kuschert for assisting in editing the manuscript.
Author Contributions
All authors made substantial contributions to study conception and design, acquisition and analysis of data; took part in drafting the article or revising it critically for important intellectual content; agreed on the journal to which the article was submitted; provided approval of the final version to be published; and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. World Health Organization. Impact of COVID-19 on people’s livelihoods, their health and our food systems. Available from: https://www.who.int/news/item/13-10-2020-impact-of-covid-19-on-people's-livelihoods-their-health-and-our-food-systems.
2. Haldane V, De Foo C, Abdalla SM, et al. Health systems resilience in managing the COVID-19 pandemic: lessons from 28 countries. Nat Med. 2021;27(6):964–980. doi:10.1038/s41591-021-01381-y
3. Yusuf F, Fahriani M, Mamada SS, et al. Global prevalence of prolonged gastrointestinal symptoms in COVID-19 survivors and potential pathogenesis: a systematic review and meta-analysis. F1000Res. 2021;10:301. doi:10.12688/f1000research.52216.1
4. CDC. About variants of the virus that causes COVID-19. Available from: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant.html.
5. World Health Organization. WHO Coronavirus (COVID-19) dashboard. Available from: https://covid19.who.int/.
6. World Health Organization. Viet Nam situation. Available from: https://covid19.who.int/region/wpro/country/vn.
7. FDA. Know your treatment options for COVID-19. Available from: https://www.fda.gov/consumers/consumer-updates/know-your-treatment-options-covid-19.
8. Frediansyah A, Tiwari R, Sharun K, Dhama K, Harapan H. Antivirals for COVID-19: a critical review. Clin Epidemiol Glob Health. 2021;9:90–98. doi:10.1016/j.cegh.2020.07.006
9. World Health Organization. Coronavirus. Available from: https://www.who.int/health-topics/coronavirus#tab=tab_3.
10. Harapan H, Itoh N, Yufika A, et al. Coronavirus disease 2019 (COVID-19): a literature review. J Infect Public Health. 2020;13(5):667–673. doi:10.1016/j.jiph.2020.03.019
11. CDC. People with certain medical conditions. Available from: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html.
12. Huynh G, Nguyen TN, Tran VK, Vo KN, Vo VT, Pham LA. Knowledge and attitude toward COVID-19 among healthcare workers at District 2 Hospital, Ho Chi Minh City. Asian Pac J Trop Med. 2020;13(6):260–265. doi:10.4103/1995-7645.280396
13. Huynh G, An LP, Nguyen VT, et al. Factors relating to preventive practices of health science students during the early stage of the COVID-19 pandemic. Medpharmres. 2020;2020(4):27–31. doi:10.32895/UMP.MPR.4.4.5
14. Olliaro P, Torreele E, Vaillant M. COVID-19 vaccine efficacy and effectiveness-the elephant (not) in the room. Lancet Microbe. 2021;Advance online publication. doi:10.1016/S2666-5247(21)00069-0
15. MacDonald NE; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33(34):4161–4164. doi:10.1016/j.vaccine.2015.04.036
16. Lucia VC, Kelekar A, Afonso NM. COVID-19 vaccine hesitancy among medical students. J Public Health (Oxf). 2020;Advance online publication:fdaa230. doi:10.1093/pubmed/fdaa230
17. Huynh G, Tran TT, Nguyen HT, Pham LA. COVID-19 vaccination intention among healthcare workers in Vietnam. Asian Pac J Trop Med. 2021;14(4):159–164. doi:10.4103/1995-7645.312513
18. Huynh G, Nguyen TV, Nguyen DD, Lam QM, Pham TN, Nguyen H. Knowledge about COVID-19, beliefs and vaccination acceptance against COVID-19 among high-risk people in Ho Chi Minh City, Vietnam. Infect Drug Resist. 2021;14:1773–1780. doi:10.2147/IDR.S308446
19. Wagner AL, Rajamoorthy Y, Taib NM. Impact of economic disruptions and disease experiences on COVID-19 vaccination uptake in Asia: a study in Malaysia. Narra J. 2021;1(2):e42. doi:10.52225/narraj.v1i2.42
20. Harapan H, Wagner AL, Yufika A, et al. Acceptance of a COVID-19 vaccine in southeast asia: a Cross-Sectional Study in Indonesia. Front Public Health. 2020;8:381. doi:10.3389/fpubh.2020.00381
21. Huynh G, Nguyen MQ, Tran TT, et al. Knowledge, attitude, and practices regarding COVID-19 among chronic illness patients at outpatient departments in Ho Chi Minh City, Vietnam. Risk Manag Healthc Policy. 2021;13:1571–1578. doi:10.2147/RMHP.S268876
22. Huynh G, Nguyen HTN, Nguyen VT, Pham AL. Development and psychometric properties of the health belief scales toward COVID-19 vaccine in Ho Chi Minh City, Vietnam. Risk Manag Healthc Policy. 2021;14:2517–2526. doi:10.2147/RMHP.S301645
23. Dror AA, Eisenbach N, Taiber S, et al. Vaccine hesitancy: the next challenge in the fight against COVID-19. Eur J Epidemiol. 2020;35(8):775–779. doi:10.1007/s10654-020-00671-y
24. Kanyike AM, Olum R, Kajjimu J, et al. Acceptance of the coronavirus disease-2019 vaccine among medical students in Uganda. Trop Med Health. 2021;49(1):37. doi:10.1186/s41182-021-00331-1
25. Saied SM, Saied EM, Kabbash IA, Abdo SAE. Vaccine hesitancy: beliefs and barriers associated with COVID-19 vaccination among Egyptian medical students. J Med Virol. 2021;93(7):4280–4291. doi:10.1002/jmv.26910
26. Mascarenhas AK, Lucia VC, Kelekar A, Afonso NM. Dental students’ attitudes and hesitancy toward COVID-19 vaccine. J Dent Educ. 2021;published online ahead of print. doi:10.1002/jdd.12632
27. Nguyen KH, Srivastav A, Razzaghi H, et al. COVID-19 vaccination intent, perceptions, and reasons for not vaccinating among groups prioritized for early vaccination — United States, September and December 2020. MMWR Morb Mortal Wkly Rep. 2021;70(6):217–222. doi:10.15585/mmwr.mm7006e3
28. USA Today. Map of COVID-19 case trends, restrictions and mobility. Available from: https://www.usatoday.com/storytelling/coronavirus-reopening-america-map/.
29. Evridiki P, Galanis P, Mechili EA, et al. Factors influencing nursing students’ intention to accept COVID-19 vaccination: a pooled analysis of seven European countries. Nurse Educ Today. 2021;104:105010. doi:10.1016/j.nedt.2021.105010
30. Goruntla N, Chintamani SH, Bhanu P, et al. Predictors of acceptance and willingness to pay for the COVID-19 vaccine in the general public of India: a health belief model approach. Asian Pac J Trop Med. 2021;14(4):2517–2526. doi:10.2147/RMHP.S301645
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.