")
Back to Journals » International Journal of Women's Health » Volume 12
Predictors of Health-Promoting Lifestyle in Pregnant Women Based on Pender’s Health Promotion Model
Authors Jalili Bahabadi F, Estebsari F , Rohani C , Rahimi Khalifeh Kandi Z , Sefidkar R, Mostafaei D
Received 18 October 2019
Accepted for publication 3 January 2020
Published 24 February 2020 Volume 2020:12 Pages 71—77
DOI https://doi.org/10.2147/IJWH.S235169
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Farideh Jalili Bahabadi, 1 Fatemeh Estebsari, 2 Camelia Rohani, 3 Zahra Rahimi Khalifeh Kandi, 4 Reyhaneh Sefidkar, 5 Davoud Mostafaei 6
1Student Research Committee, Community Health Nursing Department, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 2Community Health Nursing Department, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 3Community Health Nursing Department, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 4Department of Public Health, Iran University of Medical Sciences, Tehran, Iran; 5Department of Biostatistics, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 6Health Services Management, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Correspondence: Fatemeh Estebsari
Department of Community Health Nursing, School of Nursing and Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Tel +98-2188655367 (330)
Fax +98-2188202518
Email [email protected]
Background and Objectives: Pregnancy causes changes in women’s lifestyle; therefore, their health-promoting behaviors should be improved in order to avoid problems during this critical period, which requires knowledge of the factors affecting these behaviors. This study was conducted to determine the predictors of health-promoting lifestyles in pregnant women based on Pender’s health promotion model constructs.
Methods: This descriptive study was carried out on 300 pregnant women in their second and third trimesters of pregnancy and sought to determine the correlation between lifestyle and the constructs of Pender’s health promotion model. Data were collected using a demographic questionnaire, the Health Promoting Lifestyle Profile II (HPLP-II) and a questionnaire based on Pender’s model constructs. Data were analyzed using descriptive and analytical statistics.
Findings: A health-promoting lifestyle had a significant positive correlation with the constructs of social support and perceived benefits and a significant negative correlation with the construct of perceived barriers (P< 0.05). A health-promoting lifestyle also had a significant relationship with the constructs of perceived barriers, social support and perceived benefits in pregnant women (P< 0.05) based on the results of the regression analysis. The regression coefficients showed that all the three variables can significantly explain the variance in health promoting lifestyles in pregnant women (P< 0.05).
Conclusion: According to the results of the present study and based on the constructs of Pender’s health promotion model, social support, perceived benefits and perceived barriers were the most important predictors of health-promoting lifestyles in pregnant women. These predictor constructs are recommended to be further considered in designing and implementing training packages and interventions for promoting pregnant women’s lifestyle.
Keywords: pregnant women, lifestyle, health promotion model, health-promoting behaviors
Introduction
The health and progress of any society largely depends on the health of its women. Women experience many biological changes throughout their life that have a significant impact on their health, including pregnancy and lactation.1 Pregnancy changes women’s lifestyle and they should at least begin to lead a healthy lifestyle and perform health-promoting behaviors during this critical period in order to avoid problems that could harm themselves or the embryo.2 Health-promoting behaviors during pregnancy reduce the likelihood of preterm delivery, the need for cesarean section and the risk of obesity and diabetes.3 Failure in observing such behaviors can lead to complications during pregnancy, such as bleeding and maternal infection, multiple admissions to intensive care units, low birth weight or early neonatal death.1 Since providing maternal and newborn health services is one of the priorities of health systems,4 various strategies have been considered by healthcare providers to ensure the health of pregnant women, which involves health-promoting behaviors and a healthy lifestyle.5 Given women’s role in maintaining their family’s health, these behaviors are important for all members of the society, especially women.6,7 According to statistics provided by the WHO, 60% of people’s quality of life and health status depends on their own behaviors and lifestyle.8,9 According to the literature,
a health-promoting lifestyle is a multi-dimensional pattern of self-initiated feelings and behaviors aiming at ensuring individual’s health, self-actualization, and self-accomplishment.10,11
These behaviors include any measures taken to maintain and enhance the health of an individual or a group.12,13 Health-promoting behaviors should be further emphasized because the promotion of health in society is a dynamic process of empowering individuals to control their health based on first-grade preventive interventions and is focused on positive lifestyle changes.14,15 Pregnant women’s lifestyle includes the way they work and rest, their type of nutrition, their manner of coping with stress or communicating with others and also prenatal care.8 The factors affecting health-promoting behaviors should be determined in pregnant women in order to promote their healthy behaviors.7 Multiple behavior change theories and models have been proposed by researchers due to the complexity of behaviors and the challenges of creating, maintaining and improving health-promoting behaviors.16 Some theories and models have identified the most important multi-faceted factors affecting a behavior and the relationship between these factors.17 Pender’s health promotion model is one of the comprehensive models used for accomplishing health-promoting behaviors15 and has been recognized as a framework for explaining healthy lifestyle and health-promoting behaviors. This model serves as a guide in discovering individuals’ complex biological-psychological processes in order to promote their health behaviors and explains how individuals make decisions about their health-promoting behaviors.11,18 The studies conducted by Pender et al19,20,21 have revealed the dimensions of health-promoting behaviors as spiritual growth, health responsibility, physical activity, nutrition, interpersonal relations, and stress management. Given the importance of women’s status in society and their role in the overall development of the country, appropriate planning and policy-making for improving women’s status and facilitating their progress should take account of their health status and identify its contributing factors.22 This study was conducted based on Pender’s health promotion model to investigate the predictors of pregnant women’s health-promoting lifestyles, since it is necessary to study and identify the factors affecting these behaviors separately for each group of the community.23 The results of this study might work as a basis for ensuring a higher quality of life in this vulnerable group of society.
Methods
This descriptive research was designed to determine the predictors of a health-promoting lifestyle in pregnant women based on the constructs of Pender’s health promotion model and examine the correlation between the model constructs and lifestyle. The sample included pregnant women in Yazd Province who were selected from 2018 to 2019. The sample size was obtained as 259 using the sample size equation, type-I error probability of α=0.05, test power of 1-β=0.90 and Pearson’s correlation coefficient of r=0.20; ultimately, 300 individuals were included in the study to take account of a 15% probability of sample loss.
After making the necessary arrangements, the samples were selected through simple random sampling from pregnant women in the second and third trimesters of their pregnancy, covered by one of the community health centers of Yazd Province. The pregnant women with problems such as high-risk pregnancy (bleeding, membrane rupture, preeclampsia or eclampsia and gestational diabetes with insulin injections) or pre-pregnancy physical problems were excluded from the study. Before completing the questionnaires, the participants were briefed on the research objectives and gave their written consent. The research was carried out in accordance with the Declaration of Helsinki.
The participants were carefully monitored during their completion of the questionnaires. Data were collected using a demographic questionnaire, the Health-Promoting Lifestyle Profile II (HPLP-II) and a questionnaire based on Pender’s model constructs.
Demographic Questionnaire
The demographic questionnaire inquired about variables such as age, the woman’s education and employment status, the husband’s education and employment status, gestational age and the woman’s BMI.
Health-Promoting Lifestyle Profile II (HPLP-II)
Health-promoting behaviors were measured using the HPLP-II, designed by Pender et al (as described in ref.1). This questionnaire consists of 52 items and measures health-promoting lifestyle behaviors within six dimensions: Physical activity (eight items), nutrition (nine), spiritual growth (nine), interpersonal relations (nine), stress management (eight) and health responsibility (nine items). The questionnaire items are scored based on a 4-point Likert scale: Never (1 point), sometimes (2 points), often (3 points) and always (4 points). The mean score of each dimension is calculated, and the total lifestyle score is then calculated by adding these scores. Higher scores indicate more favorable behaviors. The validity and reliability of this instrument have been confirmed in numerous studies.9,20,24,25 This questionnaire has also been translated in Iran, and the validity and reliability of the Persian version have been confirmed in several studies.26,27
Questionnaire Based on Pender’s Model Constructs
Pender’s health promotion model was examined in this study according to Mohammadian’s research,18 which was conducted on the constructs of perceived self-efficacy, affect, social support and benefits, and barriers. This study used the perceived self-efficacy construct of the Health Locus of Control Scale adapted by Smith et al. The Health Locus of Control Scale consists of eight items scored based on a 5-point Likert scale, ranging from strongly disagree (1 point) to strongly agree (5 points). The score ranges from 8 to 40 in this scale. Higher scores indicate the individual’s greater ability to control the outcomes and consequences of health-related programs. The Cronbach’s alpha coefficient calculated for this instrument by Smith et al was 0.84 (as described in ref. 18). The affect construct was evaluated using an assessment tool adapted by Watson et al. This assessment tool contains 20 items, including ten on positive affect and ten on negative affect, and is scored based on a 5-point Likert scale, ranging from never (1 point) to always (5 points). The score obtained for each of the positive and negative affects ranges from 10 to 50. Higher scores indicate better reported emotional states over the past 24 hours. The Cronbach’s alpha coefficient reported by Watson et al was 0.94 for positive affect and 0.91 for negative affect.18 The social support construct was evaluated using an assessment tool adapted by Canty et al, including 12 items scored based on a 7-point Likert scale (strongly disagree =1 point, to strongly agree =7 points). The score obtained ranges from 12 to 84. Higher scores indicate greater support from friends, family and other key people. The Cronbach’s alpha coefficient reported by Canty et al for this assessment tool was 0.91.18 The perceived barriers construct was evaluated using an assessment tool adapted by Becker et al, which has 18 items scored based on a 4-point Likert scale (never =1 point, to always =4 points). The score obtained for this scale ranges from 18 to 72. Higher scores indicate more barriers in health-promoting behaviors. The Cronbach’s alpha coefficient reported by Becker et al for this assessment tool was 0.80.18 In this study, the perceived benefits construct was evaluated using an assessment tool adapted by Mohammadian et al, which consisted of 20 items scored based on a 7-point Likert scale (strongly disagree =1 point, to strongly agree =7 points). The score obtained ranges from 20 to 140 and higher scores indicate more benefits perceived for health-promoting behaviors.28
The content and face validity were evaluated quantitatively to determine the questionnaire’s validity. For this purpose, the questionnaires were distributed among ten individuals, including four community health nursing professors, three maternal and child health specialists and three family health professionals. All the experts approved the items of the questionnaire. Cronbach’s alpha was used as a measure of content reliability to evaluate the reliability of the questionnaires and was reported as 0.92 for the social support dimension, 0.74 for the self-efficacy dimension, 0.90 for the perceived barriers dimension, 0.84 for the affect dimension, 0.77 for the perceived benefits dimension and 0.85 for health-related lifestyle.
The collected data were entered into SPSS-20. Initially, the normality of the data was tested using the Kolmogorov–Smirnov (K-S) test, and a normal distribution was obtained. Data were analyzed using descriptive and analytical statistics, including frequency distribution tables, mean, standard deviation, Pearson’s correlation coefficient and the multiple linear regression model. The confidence interval was 0.95%. Before completing the questionnaires, the participants were fully briefed on the study objectives and were ensured that their information would remain confidential and that the results would only be used for research purposes and be published in general. Also, written consent was obtained from all the participants for taking part in the study.
Findings
The mean age of the pregnant women was 32.85±6.85 years. A total of 27% of the women were illiterate or less educated, while the rest were educated; 66% were housewives and the rest were employed. Table 1 presents their other demographic details.
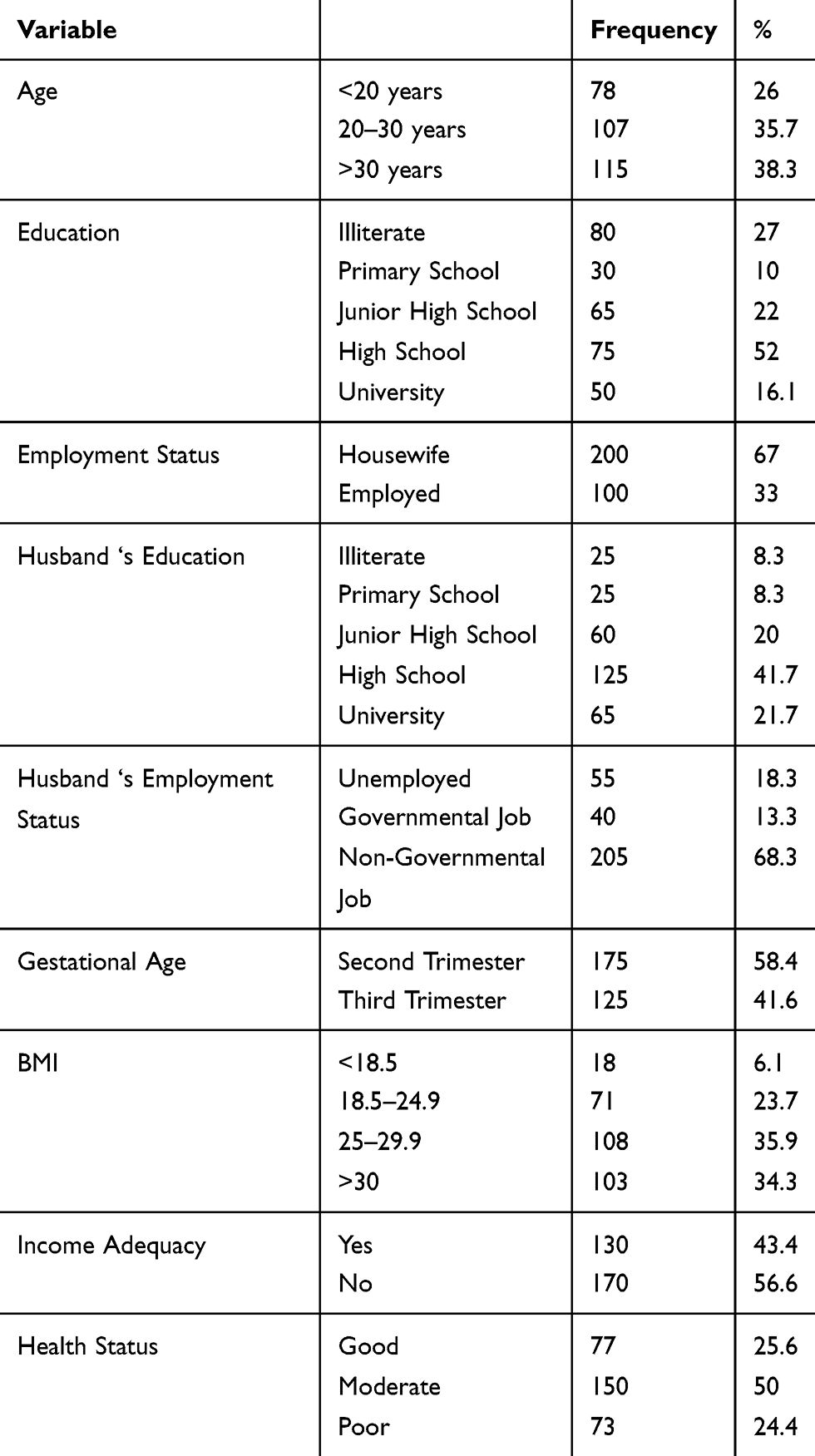 |
Table 1 The Frequency Distribution and Mean of Demographic Variables in the Participating Pregnant Women |
Table 2 shows the mean and standard deviation of the pregnant women’s scores in the health-promoting lifestyle dimensions and Pender’s model constructs. As shown in the table, the mean score of health-promoting behaviors was 154.9±2.2. Also, among all the health-promoting lifestyle dimensions, the spiritual growth dimension had the highest score with a mean of 30±3.6 and the physical activity dimension the lowest score with the mean of 17±10.2. Table 2 presents information on the other dimensions of health-promoting lifestyle. Furthermore, among Pender’s model constructs, perceived benefits had the highest score with a mean of 123.4±10.1 and self-efficacy the lowest score with a mean of 24±4.2. Table 2 presents information on the other constructs. According to the results of the regression analysis of the health-promoting lifestyle dimensions and Pender’s model constructs (Table 3), health-promoting lifestyle had a significant relationship with the perceived barriers construct, social support and perceived benefits (P<0.05) and the regression coefficients of each of the three predictor variables (social support, perceived barriers and perceived benefits) indicated that all the three variables can significantly explain the variance in health-promoting lifestyles (P<0.05). According to Table 3, the correlation matrix of health-promoting lifestyle and Pender’s model constructs using Pearson’s correlation coefficient showed that health-promoting lifestyles were significantly and positively correlated with social support and perceived benefits and significantly and negatively with perceived barriers. Also, based on the results of the correlation coefficient test, there was a significant correlation between the dimensions of self-efficacy and support (r=0.28), self-efficacy and affect (r=−0.3), barriers and affect (r=0.28), perceived barriers and perceived benefits (r=0.14), perceived barriers and health-promoting lifestyle (r=0.45), social support and affect (r=0.15), social support and health-promoting lifestyle (r=0.24) and perceived benefits and health-promoting lifestyle (r=0.194); (P<0.01; Table 3).
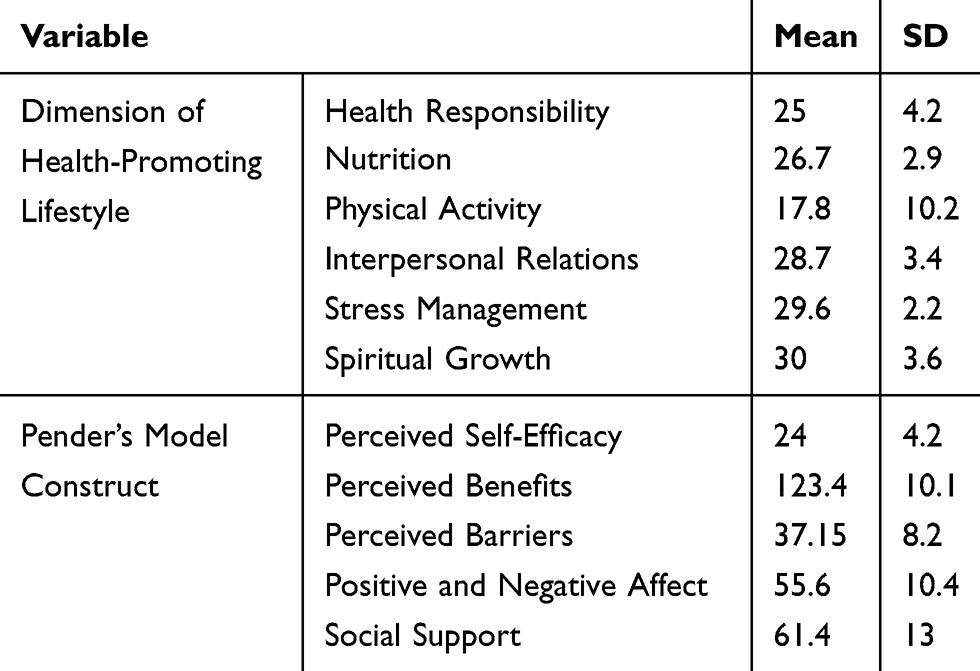 |
Table 2 The Mean and Standard Deviation of the Scores on the Dimensions of Health-Promoting Lifestyle and the Constructs of Pender’s Health Promotion Model |
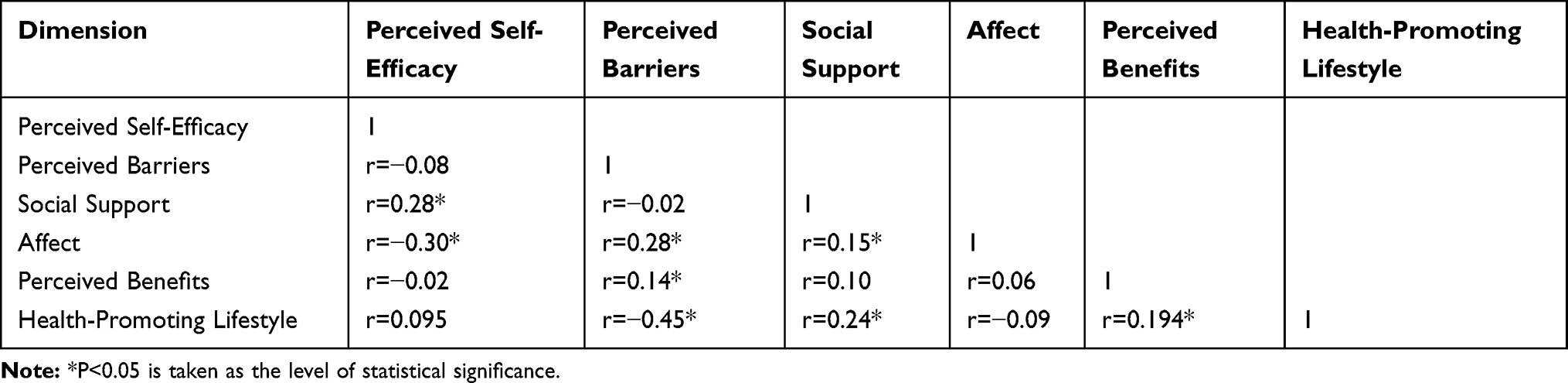 |
Table 3 The Correlation Matrix of the Health-Promoting Lifestyle Dimensions and Pender’s Model Constructs |
The predictors of health-promoting lifestyle were determined using a multiple regression model, as shown in Table 4. Among the constructs of Pender’s model, social support (P=0.001), perceived barriers (P=0.001) and perceived benefits (P=0.001) had a significant effect on health-promoting lifestyle, such that the mean score of health-promoting lifestyle decreased by 1.28 units per one unit increase in the score of perceived barriers (assuming the other variables were constant; P=0.001). Also, the mean score of health-promoting lifestyle increased by 0.46 units (P=0.001) per one unit increase in social support (assuming the other variables remained constant), and the mean score of health-promoting lifestyle increased by 0.63 units (P=0.001) per one unit increase in perceived benefits (assuming the other variables remained constant).
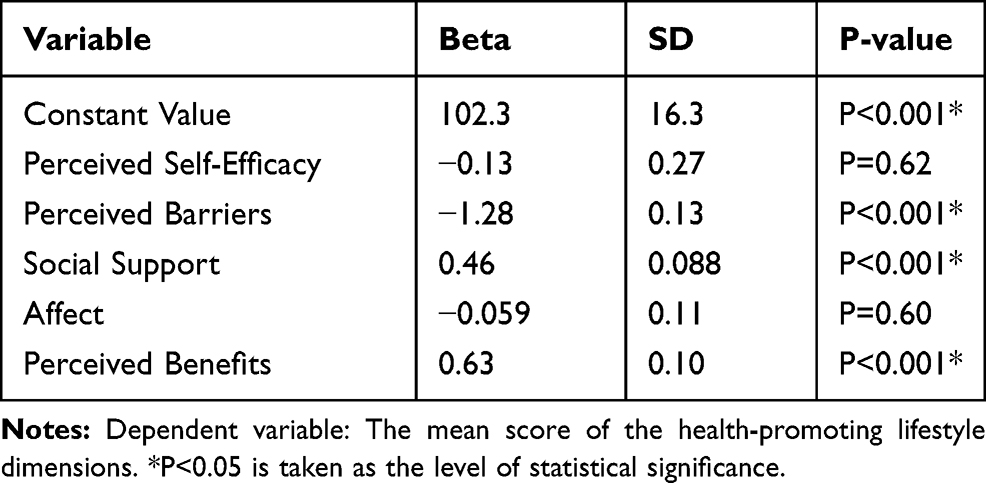 |
Table 4 The Concurrent Effects of Pender’s Model Constructs on the Dimensions of Health-Promoting Lifestyle in the Participating Pregnant Women |
Discussion
This study was conducted to investigate the predictors of health-promoting lifestyles in pregnant women based on Pender’s health promotion model.
Based on the predictive constructs of Pender’s model and their effect on health-promoting behaviors, the constructs of perceived benefits and social support, at higher levels, and the construct of perceived barriers, at lower levels, were most correlated with health-promoting behaviors, whereas perceived self-efficacy and affect had the least correlation with health-promoting behaviors. The results of other studies have also confirmed this finding.22,29,30,31 Pregnant women’s greater awareness about the positive outcomes of health-promoting behaviors increases their intention to adopt these behaviors. Higher social support also leads to the greater adoption of health-promoting behaviors in pregnant women.1 In a study conducted by Thaewpia32 on older pregnant women, there was a significant correlation between health-promoting behaviors and education, perceived benefits, self-efficacy and social support. Research has shown that women with higher self-efficacy and perceived benefits scores are more likely to receive favorable social support and are therefore more likely to engage in health-promoting behaviors.9,20 A study by Lin et al,21 which had only considered the self-efficacy and perceived health constructs of Pender’s model as predictors of health-promoting behaviors in pregnant women, revealed a significant and positive correlation between health-promoting behaviors and perceived self-efficacy. This finding is not in agreement with the results of the present study. In this study, perceived self-efficacy, perceived benefits and social support had a direct impact on health-promoting behaviors and perceived benefits. This finding is in agreement with the results of the present study. The positive effects of perceived benefits and social support on health-promoting behaviors have been confirmed by many other studies.14,33 In some studies, social support, perceived barriers and perceived benefits had the highest correlation with health-promoting behaviors,1,14 while in other studies, self-efficacy played a significant role in health-promoting behaviors.32,34 Research suggests that social support improves physical and mental health, and the lack of social support has a negative and adverse effect on health. Social support facilitates the support provided by others to adopt a behavior. In addition, social support can decrease negative psychosocial complications and consequences such as injuries and illness as well as restrictions and thus improve people’s health and quality of life. Perceived benefits and perceived barriers are two constructs explaining behavior in some behavior change models; that is, they explain people’s action based on whether there is a balance or imbalance between their perceived positive and negative forces on health behavior. People perform a behavior or avoid it based on their analysis of its benefits minus its barriers. Given the importance of this issue, the possibility of adopting a behavior is expected to increase when its perceived barriers are reduced and its perceived benefits are increased.17 Overall, it can be argued that if pregnant women have the desired social support, their self-efficacy in adopting a healthy lifestyle and their control over health behaviors will increase and they will become more likely to adopt a healthy lifestyle. Consequently, they will have fewer problems with pregnancy, experience a successful, risk-free or at least less-risky pregnancy, give birth to a healthy baby and suffer less complications, such as less preterm labor and preterm infants.1
One of the limitations of this study was that the participants were restricted to second- and third-trimester pregnant women due to the unavailability of accurate information on women in their first trimester of pregnancy. Therefore, if possible, lifestyle behaviors are recommended to be investigated from the onset of pregnancy, when hormonal changes begin, especially pregnancy symptoms. One of the strengths of the present study was the use of linear regression models to determine the degree and type of correlation between the constructs and lifestyle.
Conclusion
According to the results of the present study on pregnant women, among all the constructs of Pender’s health promotion model, social support and perceived benefits, and, to a less extent, perceived barriers, had the greatest effects on health-promoting behaviors. Given the effect of lifestyle on quality of life and health status, the results of this study can help health service policymakers and providers plan appropriate interventions for promoting the lifestyle of pregnant women.
The researchers recommend further educational intervention studies based on Pender’s health promotion model to promote healthy behaviors in pregnant women.
Acknowledgments
This study was approved by the Research Council of Shahid Beheshti University of Medical Sciences with the ethics code IR.SBMU.RETECH.1397.27. Hereby, we wish to express our gratitude to the Vice Chancellor of Research and Technology of Shahid Beheshti University of Medical Sciences for funding this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hamzehgardeshi Z, Gelehkolaee Keshvar S, Kardan Soraky M. Health-promoting lifestyles and related factors in pregnant women. Int Med Med Investigation J. 2018;3(4):12–17. doi:10.24200/imminv.v2i4.165
2. Malakouti J, Sehhati F, Mirghafourvand M, Nahangi R. Relationship between health promoting lifestyle and perceived stress in pregnant women with preeclampsia. J Caring Sci. 2015;4(2):155–163. doi:10.15171/jcs.2015.016
3. Mourtakos SP, Tambalis KD, Panadiotakos DB, et al. Maternal lifestyle characteristics during pregnancy, and the risk of obesity in the offspring: a study of 5125 children. BMC Pregnancy Childbirth. 2015;15:66. doi:10.1186/s12884-015-0498-z
4. Abedi P, Jorfi M, Afshari P. Evaluation of the health promotion lifestyle and its related factors in reproductive aged women in Ahvaz, Iran. Community Health J. 2015;9(1):68–74.
5. Silva A, Pereira B, Souza S, et al. Impact of a healthy lifestyle intervention program during pregnancy on women and newborn: STUDY PROTOCOL for a quasi-experimental study. Porto Biomed J. 2019;4(2):e29. doi:10.1016/j.pbj.0000000000000029
6. Gharaibeh M, Al-Ma’aitah R, Al Jada N. Lifestyle practices of Jordanian pregnant women. Int Nurs Rev. 2005;52(2):92–100. doi:10.1111/inr.2005.52.issue-2
7. Asci O, Rathfisch G. Effect of lifestyle interventions of pregnant women on their dietary habits, lifestyle behaviors, and weight gain: a randomized controlled trial. J Health Popul Nutr. 2016;35:7. doi:10.1186/s41043-016-0044-2
8. Mirghafourvand M, Baheiraei A, Nedjat S, Mohammadi E, Mohammad-alizadeh Charandabi S, Majdzadeh R. A population-based study of health-promoting behaviors and their predictors in Iranian women of reproductive age. Health Promot Int. 2014;30(3):586–594. doi:10.1093/heapro/dat086
9. Rahimi Foroushani A, Estebsari F, Mostafaei D, et al. The effect of health promoting intervention on healthy lifestyle and social support in elders: a clinical trial study. Iran Red Crescent Med J. 2014;16(8):e18399. doi:10.5812/ircmj
10. Tol A, Tavassoli E, Shariferad GR, Shojaeezadeh D. Health-promoting lifestyle and quality of life among undergraduate students at school of health, Isfahan University of Medical Sciences. J Educ Health Promot. 2013;2:11. doi:10.4103/2277-9531.108006
11. Darkhor S, Estebsari F, Hosseini M, Charati JY, Vasli P. Effect of health promotion intervention on nurses’ healthy lifestyle and health-promoting behaviors: RCT study. J Adv Pharm Educ Res. 2018;8(1):108–114.
12. Abbaszadeh A, Hosseini M, Borhani F, Estabsari F, Shakeri N. The effects of self-care training on health-promoting behaviors of asthmatic patients. Ann Trop Med Publ Health. 2017;10(6):1785–1791. doi:10.4103/ATMPH.ATMPH_656_17
13. Estebsari F, Taghdisi MH, Rahimi Foroushani A, Eftekhar Ardebili H, Shojaeizadeh D. An educational program based on the successful aging approach on health-promoting behaviors in the elderly: a clinical trial study. Iran Red Crescent Med J. 2014;16(4):e16314. doi:10.5812/ircmj
14. Rahimian M, Mohammadi M, Mehry A, Rakhshani MH. The predictors of physical activity among health volunteers based on Pender’s health promotion model. J Res Health. 2018;8(4):308–312.
15. Heydari A, Khorashadizadeh F. Pender’s health promotion model in medical research. J Pak Med Assoc. 2014;64(9):1067–1074.
16. Khodaveisi MP, Omidi AM, Farokhi SM, Soltanian ARP. The effect of Pender’s health promotion model in improving the nutritional behavior of overweight and obese women. Int j Community-Based Nurs Midwifery. 2017;5(2):165–174.
17. Mohebi S, Sharifirad G, Feizi A, Botlani S, Hozori M, Azadbakht L. Can health promotion model constructs predict nutritional behavior among diabetic patients? J Res Med Sci. 2013;18(4):346–359.
18. Mohammadian H, Eftekhar Ardebili H, Rahimi Foroushani A, Taghdisi MH, Shojaei Zadeh D. Evaluation of Pender health promotion model in predicting living quality of adolescent girls. J Faculty Health Health Res Inst. 2011;8(4):1–13.
19. Yang SC, Luo YF, Chiang CH. The associations among individual factors, eHealth literacy, and health-promoting lifestyles among college students. J Med Internet Res. 2017;19:1. doi:10.2196/jmir.5964
20. Estebsari F, Dastoorpoor M, Mostafaei D, et al. Design and implementation of an empowerment model to prevent elder abuse: a randomized controlled trial. Clin Interv Aging. 2018;13:669–679. doi:10.2147/CIA.S158097
21. Lin Y-H, Tsai E-M, Chan T-F, Chou F-H, Lin Y-L. Health promoting lifestyles and related factors in pregnant women. Chang Gung Med J. 2009;32(6):650–661.
22. Rostami Gooran N, Sayarifard A, Nazari M, Rahbari M, Javadinasab H, Ahmadi B. Scientific publications on women’s health in Islamic Republic of Iran during three decades (1981 to 2012): a review. Payesh. 2018;17(1):7–19.
23. Chenary R, Noroozi A, Tahmasebi R. Health promoting behaviors in veterans in Ilam province. J Military Med. 2013;15(1):95–102.
24. Baheiraei A, Bakouei F, Mohammadi E, Montazeri A, Hosseni M. The social determinants of health in association with women’s health status of reproductive age: a population-based study. Iran J Public Health. 2015;44(1):119–129.
25. Baheiraei A, Mirghafourvand M, Mohammadi E, et al. Health-promoting behaviors and social support of women of reproductive age, and strategies for advancing their health: protocol for a mixed methods study. BMC Public Health. 2011;11:191. doi:10.1186/1471-2458-11-191
26. Hulsman BL The relationship between self-directedness and health promotion in the elderly [Doctoral Dissertation]. Tennessee: University of Tennessee, Knoxville; 2011.
27. Taghdisi MH, Estebsari F, Rahimi Foroushani A, et al. The educational program based on the successful aging approach on elders health-promoting behaviors: a clinical trial study. Razi J Med Sci. 2014;21(125):25–36.
28. Mohamadian H, Eftekhar H, Rahimi A, Mohamad HT, Shojaiezade D, Montazeri A. Predicting health‐related quality of life by using a health promotion model among Iranian adolescent girls: a structural equation modeling approach. Nurs Health Sci. 2011;13(2):141–148. doi:10.1111/nhs.2011.13.issue-2
29. Bahar Z, Beser A, Ozbıcakcı S, Ozturk Haney M. Health promotion behaviors of Turkish women. Dokuz Eylul Univ Hemsirelik Yuksekokulu E Dergisi. 2013;6(1):9–16.
30. Protheroe J, Whittle R, Bartlam B, Estacio EV, Clark L, Kurth J. Health literacy, associated lifestyle and demographic factors in adult population of an English city: a cross‐sectional survey. Health Expectations. 2017;20(1):112–119. doi:10.1111/hex.2017.20.issue-1
31. Kiajamali M, Hosseini M, Estebsari F, et al. Correlation between social support, self-efficacy and health-promoting behavior in hemodialysis patients hospitalized in Karaj in 2015. Electron Phys. 2017;9(7):4820–4827. doi:10.19082/4820
32. Thaewpia S, Clark MJ, Howland LC, James KS. Factors predicting health promoting behaviors among older pregnant Thais. Pacif Rim Int J Nurs Res. 2012;16(2):113–123.
33. Jackson ES, Tucker CM, Herman KC. Health value, perceived social support, and health self-efficacy as factors in a health-promoting lifestyle. J Am Coll Health. 2007;56(1):69–74. doi:10.3200/JACH.56.1.69-74
34. Wu TY, Pender N. Determinants of physical activity among Taiwanese adolescents: an application of the health promotion model. Res Nurs Health. 2002;25:25–36. doi:10.1002/nur.10021
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.