")
Back to Journals » Clinical Interventions in Aging » Volume 15
Predictors of Fall Protective Behaviors Among Iranian Community-Dwelling Older Adults: An Application of the Protection Motivation Theory
Authors Taheri-Kharameh Z, Bashirian S, Heidarimoghadam R, Poorolajal J , Barati M , Rásky É
Received 22 July 2019
Accepted for publication 20 December 2019
Published 5 February 2020 Volume 2020:15 Pages 123—129
DOI https://doi.org/10.2147/CIA.S224224
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Richard Walker
Zahra Taheri-Kharameh,1 Saeed Bashirian,2 Rashid Heidarimoghadam,3 Jalal Poorolajal,4 Majid Barati,2 Éva Rásky5
1Student Research Committee, Department of Public Health, Hamadan University of Medical Sciences, Hamadan, Iran; 2Department of Public Health, School of Health, Social Determinants of Health Research Center, Hamadan University of Medical Sciences, Hamadan, Iran; 3Department of Ergonomics, School of Health, Research Center for Health Sciences, Hamadan University of Medical Sciences, Hamadan, Iran; 4Research Center for Health Sciences, Department of Epidemiology, School of Public Health, Hamadan University of Medical Sciences, Hamadan, Iran; 5Institute of Social Medicine and Epidemiology, Medical University of Graz, Graz, Austria
Correspondence: Majid Barati
Department of Public Health, Hamadan University of Medical Sciences, Hamadan, Iran
Tel +988138380090
Email [email protected]
Purpose: The protection motivation theory (PMT) is a common framework understanding the use of protective behaviors. The aim of this study was to assess the predictors of fall protective behaviors among community-dwelling older adults, Iran.
Methods: The cross-sectional study was conducted in Qom, Iran, from May to October 2018. Three hundred older people were selected from retirement centers via stratified sampling method. Data were collected by a questionnaire containing items on socio-demographic information, Falls Behavioral (FaB) Scale, and PMT constructs scale. Data analysis was performed using descriptive statistics and structural equation modeling.
Results: The mean (SD) age of the participants was 64.6 (5.5) and the majority were male (77.7%). Level of perceived fall threat was lower than perceived efficacy of fall protective behaviors. There was a significant relationship between protection motivation and fall protective behaviors (β= 0.515, t-value= 13.650). Coping appraisals (β= 0.409, t-value= 7.352) and fear (β= 0.194, t-value= 2.462) were associated with motivation. The model explained approximately 27% of the variance in fall protective behaviors. The goodness of fit index of 0.48 indicating the model good fit.
Conclusion: The results indicated that protection motivation, coping appraisals and reasonable fear are considered as the strongest predictors of fall protective behaviors among older people. The results can help health care providers to develop appropriate interventions to fall prevention among older people.
Keywords: fall prevention, protection motivation theory, coping appraisals, threat appraisals, aging
Introduction
A fall refers to an event that results in a person coming to rest inadvertently on the ground or on a lower level, which is a major public health problem worldwide.1,2 According to the World Health Organization (WHO), 28–35 percent of older people fall every year, and the incidence increases with age.2 Falls are known to be the main cause of injury, physical inability, and death in older adults.3 Educational interventions are an important element in health promotion and prevention programs. The effectiveness of which is linked to health behavior theories. The guiding framework derived from health behavior theories can help to understand factors affecting protective behavior to develop effective health promotion programs.4 The Protection Motivation Theory (PMT), introduced by Rogers (1975) has widely been used as a framework for predicting protective behaviors.5 Based on PMT, it is assumed that accepting a recommended protective behavior against a health risk is a direct action of one’s motivation to protect him/herself. PMT also assesses fear in order to predict and encourage people to do protective behaviors,6 and explains the mediating cognitive processes in terms of threat and coping appraisal. The PMT threat appraisal depends on 1) one’s belief on the seriousness of the perceived problem (perceived severity), 2) one’s estimate of the chance to experience the disease (perceived vulnerability), and 3) one’s belief on positive aspects of her/his unhealthy behavior (perceived rewards). Greater motivation to engage in health-promoting behavior is, therefore, expected if the perceived severity and vulnerability are high and perceived rewards are low. The PMT coping appraisal consists of 1) an individual’s assessment of whether the protective behavior is effective in overcoming the threat (response efficacy), 2) an individual’s belief in his/her abilities to perform protective behavior successfully (self-efficacy), and 3) one’s estimate of any cost such as money, person, time, and effort related to doing protective behavior (perceived response costs).7 “Response-efficacy” and “self-efficacy” are expected to promote “coping appraisal”, whereas ‘response costs’ are expected to reduce it (Figure 1).
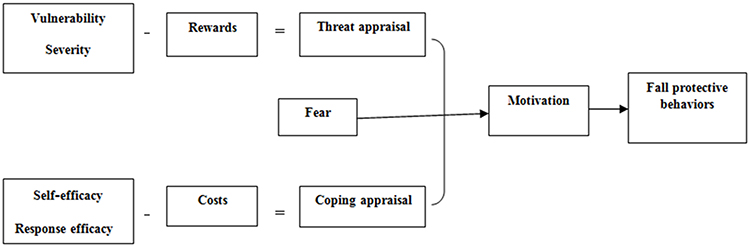 |
Figure 1 Framework of the Protection Motivation Theory (PMT). |
PMT has been widely adopted as a framework for the prediction of and intervention in a range of health-related behaviors such as skin cancer preventive behaviors,8,9 physical activity,10 cancer screening,11,12 tobacco use13,14 and sexual protective behaviors.15,16 However, theory-based studies are very limited in terms of fall preventative behaviors. In fact, to the best of our knowledge, there is no study to measure the determinants of fall preventive behaviors using PMT. Determinants of fall preventive behaviors can be considered as a priority for designing appropriate intervention programs. Therefore, this study aimed to assess the predictors of PMT-based preventive fall behaviors among community-dwelling older adults in Iran.
Method
Design and Participants
This cross-sectional study conducted from May to October 2018 in Qom, Iran. Three hundred were recruited from the older peoples who referred to active elderly centers via stratified sampling method. Participants were selected based on the following inclusion criteria: age 60 years or older; living independently in the community; Persian speaking; ability to complete the survey and willing to participate in this study
Data Collection
The purpose of the study, data collection procedure, and confidentiality of information to the researcher were explained to the participants, followed by obtaining their satisfaction. Data were then collected from the questionnaires conducted in the form of face-to-face interviews over a period of 6 months. Completion lasted for about 20–30 mins for each participant.
Measurements
We used a questionnaire in three sections follows:
- Socio-demographic information including age, gender, marital status, educational status, economic status, body mass index (BMI), comorbidity, falls history was asked in the first section of the questionnaire.
- The fall protective behaviors were measured using the Falls Behavioral (FaB) Scale, originally developed by Clemson (2008) to identify the older person’s awareness of and practice of behaviors that could potentially protect against falls. FaB includes 30 items related to fall prevention behaviors, including cognitive adaptation, protective mobility, avoidance and awareness among others. Respondents are asked to indicate how much each item describes the actions they are in fact doing in their everyday life. Each item of the FaB is rated on a four-level response scale ranging from 1 (never) to 4 (always). An average item score can be computed for the respondent after completion of the FaB. Previous evaluation of the original of the FaB indicated good reliability and validity.17
- PMT constructs were assessed using the PMT scale for behaviors of falls. It was compiled of 35 items, and 8 subscales as follows: perceived vulnerability (3 items, e.g., “I’ll likely fall in the future”), perceived severity (6 items, e.g., “If I fall, I will break and injure my extremities”). fear (3 items, e.g., “When I think of falling, I become anxious”), costs (5 items, e.g., “I do not know how to prevent falls”), rewards (2 items, e.g., “Making things fast is a pleasure for me”), perceived self-efficacy (5 items, e.g., “I can use a cane or auxiliary equipment when needed, even if I seem unable”), response efficacy (6 items, e.g., “Considering the possible dangers of doing things, falls can be prevented”), and protection motivation (5 items, e.g., “I intend to look for new information to protect myself from the falls”). These items were assessed using a 5-point Likert scale from 1 strongly disagree to 5 strongly agree. The score of each subscale was obtained by the average computed as the sum of items of it. Content validity ratio (CVR) and content validity index (CVI) were used to determine content validity. The Result showed high overall CVI and CVR of the PMT scale. CFA confirmed an acceptable eight-factor model fit of the PMT sub-constructs with factor loadings from 0.59 to 0.93. The discriminant validity was verified using Fornel and Larcker method. The Cronbach’s alpha ranged from 0.68 to 0.90 and the test-retest reliability ranged from 0.78 to 0.90, indicating an acceptable result.
Ethical Considerations
Approval to conduct the study was obtained from the Medical Ethics Committee at Hamadan University of Medical Sciences (registration number: IR.UMSHA.REC.1396.911). The study procedure was explained to the participants who met the eligibility criteria. Written informed consent to participate in the study was obtained from all participants. They were free to withdraw from the study. The study was conducted in accordance with the Declaration of Helsinki.
Data Analysis
Statistical analyses were completed using SPSS software version 20 and the Partial Least Square (PLS) software version 3. Descriptive statistics were used to summarize the sample characteristics. Pearson correlation coefficients were computed to assess the relationship between the fall protective behaviors and PMT constructs. Moreover, structural modeling was applied to analyze the strength of influence between the fall protective behaviors and PMT constructs. Regarding the theoretical framework of this study, PMT constructs, as independent variable fall protective behaviors as a dependent variable were included in the model. In the structural model, two important criteria, path coefficient, and R square were used to measure relationships among constructs. The results demonstrate path coefficients for each hypothesized path, while the corresponding t-values that denote the direction and significance of the coefficients along with R square values for the dependent variables.18 Accordingly, coping appraisals appear to play a greater role than the threat components in predicting fit (GoF) index was calculated to display the model fit to the data.19
Results
Sample Characteristics
The sample comprised 300 older people of 60–88 years, with a mean age of 64.6 years. Most participants were males (77.7%), married (88.7%), and had low literacy (58.6%). 55% of participants had a history of falls; 24% of those had fallen more than once and 6.3% of participants reported one or more injurious falls. The demographic characteristics of participants are presented in Table 1.
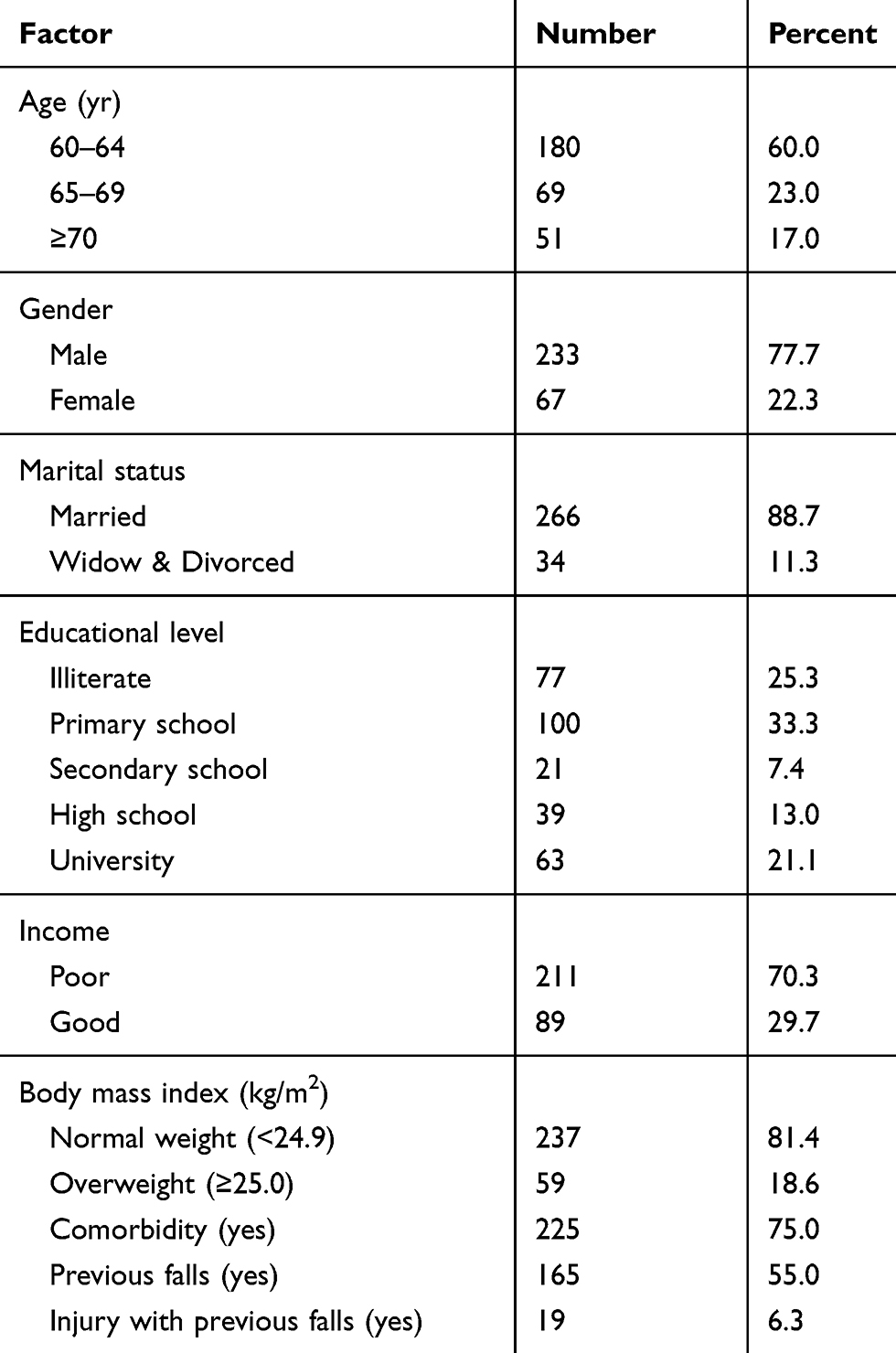 |
Table 1 Demographic Characteristics of the Study Sample (n = 300) |
PMT Constructs About Fall Protective Behaviors
Table 2 shows the means and standard deviations of PMT constructs. Participants rated fear (39%) and susceptibility (47%) as the lowest percentage indicating they did not perceive fall as a serious risk. Rewards (81%), response efficacy (80%), and self-efficacy (73%) were the highest percentage of the mean from the maximum obtainable score.
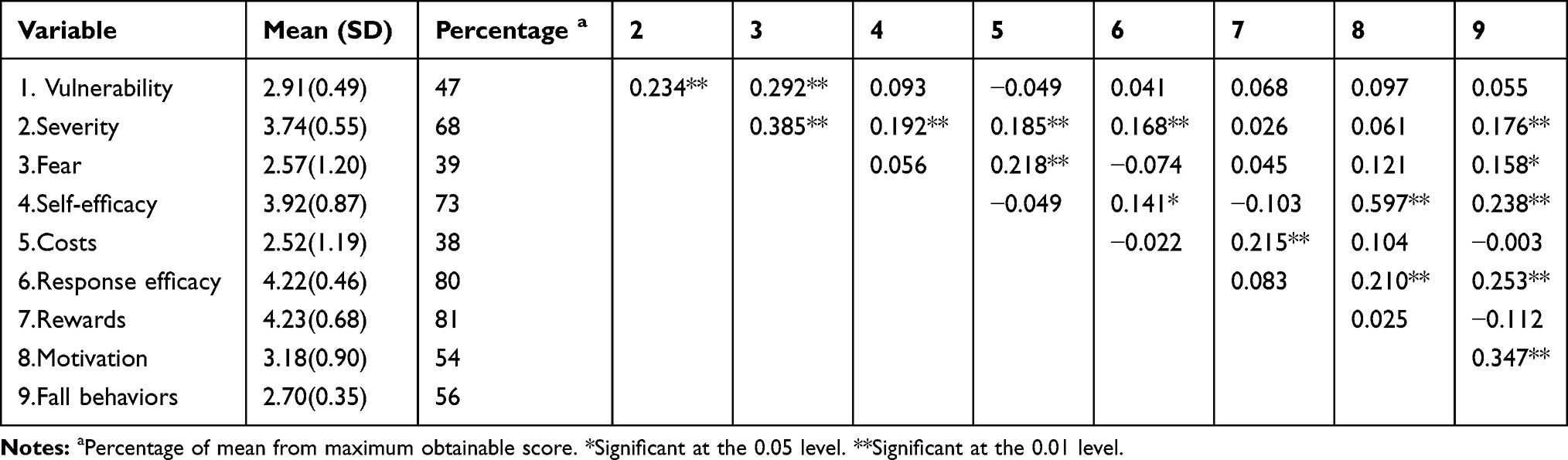 |
Table 2 Bivariate Correlations of PMT Variables and Fall Behaviors |
Relationships of the PMT Constructs and Behavior Measure
Relationships among PMT constructs and FaB are shown in Table 2. Fall protective behaviors were significantly associated with severity (r = 0.176, p= 0.009), fear (r = 0.158, p= 0.019), self-efficacy (r = 0.238, p< 0.001), and response efficacy (r = 0.253, p< 0.001), and motivation (r=0.347, p<0.001). No significant associations were observed between other PMT constructs with FaB.
Results from the Structural Modeling Analysis
Table 3 and Figure 2 provide the results of the structural model. The model explained 27% of the variance of fall protective behaviors as the dependent variable (R square = 0.265). The R square for protection motivation is 0.278 that suggesting 28% of the variance of protection motivation can be explained by coping appraisals.
 |
Table 3 Path Analysis of PMT Fall Prevention Model (n = 300) |
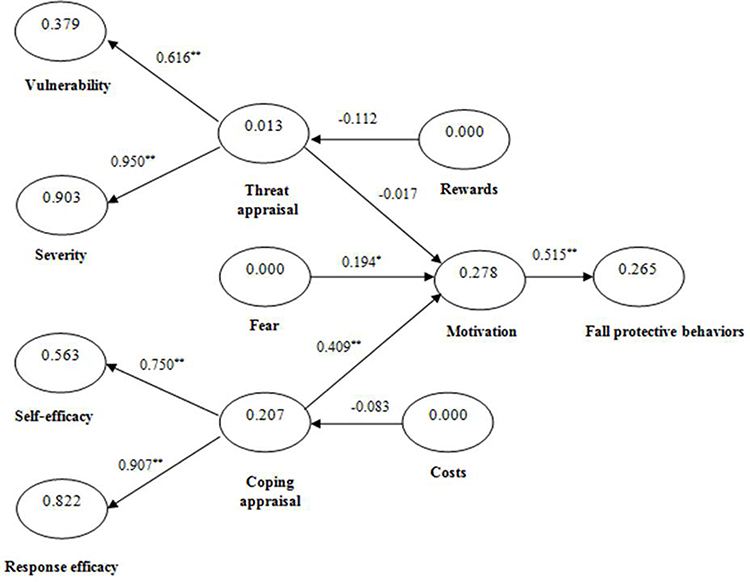 |
Figure 2 Structural equation modeling of fall protective behaviors. *Significant at the 0.05 level. **Significant at the 0.01 level. |
Coping appraisals (β= 0.409, t-value= 7.352) and fear (β= 0.194, t-value= 2.462) associated with motivation. Also, motivation (β= 0.515, t-value= 13.650) was associated to fall protective behaviors. No significant associations were observed between threat appraisal with motivation and fall protective behaviors (Table 3).
The model’s predictive power was tested by calculating Q2 indexes of motivation (Q2 = 0.22) and fall protective behaviors (Q2 = 0.13), exceeding the recommended threshold value (Q2 > 0), demonstrating an adequate predictive value of the model. Finally, GoF = 0.48, indicating the model good fit.
Discussion
The current study utilized a PMT framework to identify the relationship between perceived risk of falls and fall protective behaviors among a community-based sample of older adults. To the best of our knowledge, this is the first study to investigate the applicability of PMT in understanding the fall protective behaviors among older adults. Promising targets for interventions designed to decrease PMT constructs are considered to be key determinants of fall protective behaviors among older people. Based on the protection motivation theory, preventative actions will be of greater attention in a high threat situation when both the self-efficacy and the efficacy of the recommended action are known to be high.6
A strong significant association was found between protection motivation and fall protective behaviors supporting previous findings that the intention of human being was generally regarded as the most vital determinant of such behaviors.20 In the absence of protection motivation, the recommended protective action is judged to be ineffective in averting the threat or impossible to undertake, resulting in no intention to act.21
Coping appraisals were identified to have significant positive associations with protection motivation. The strong relationships of the coping appraisal components with fall protective behaviors are similar to those of previous studies showing that coping appraisals to be important in predicting fall protective behaviors.22 Accordingly, coping appraisals appear to play a greater role than the threat components in predicting intent; however, it would be premature to focus exclusively on coping appraisals without a better understanding of threat appraisal contributions to overall PMT model.23,24
Contrary to the current expectations based on the PMT constructs, it is generally seen that none of the threat appraisal components (severity, vulnerability, and maladaptive response rewards) predicted protection motivation and behavior accurately. A possible explanation for this ineffective predictive relationship is that fall protective behavior is less likely to be affected by emotional factors.25 Additionally, as levels of perceived vulnerability and severity were low based on PMT, people know what to do but are not really motivated to do much, so they should be trained about the risk. Rippletoe and Rogers (1987) reported that high perceived threat could have different consequences, with increasing motivation leading to preventive behaviors in some cases, but resulting in avoidance and denial in other cases.25
There are several limitations in this study, which should be noted cautiously. First, data used for this study were collected through a cross-sectional survey, which limits the potential for recall and interviewer biases. Longitudinal data design could clarify the direction of influence between variables. Second, given that all our participants were members of elderly centers and only 6.3% had ever been injured due to a fall, the findings of this study might not be generalized to all populations of older people. It is also important to note that the current study focuses on PMT only in terms of fall protective behaviors. Future research can investigate predictors of fall protective behaviors from a more ecological approach by examining PMT constructs accompanied by broader levels of individual and social factors.
Conclusion
In conclusion, the present study demonstrates that some of the PMT constructs such as protection motivation, coping appraisals and, reasonable fear are useful in understanding fall protective behaviors, and can help health care providers to develop appropriate interventions to fall prevention among older people.
Acknowledgments
This research is extracted from a part of a dissertation project with the code number of 9612228374 at the Social Determinants of Health Research Center of Hamadan University of Medical Sciences. The researchers express participants in this study as well as the research Deputy of Hamadan University of Medical Sciences to support and funding this project.
Disclosure
The authors report no conflict of interests in this work.
References
1. Ku Y-C, Liu M-E, Tsai Y-F, Liu W-C, Lin S-L, Tsai S-J. Associated factors for falls, recurrent falls, and injurious falls in aged men living in Taiwan veterans homes. Int J Gerontol. 2013;7(2):80–84. doi:10.1016/j.ijge.2012.07.004
2. WHO. WHO Global Report on Falls Prevention in Older Age. Geneva: WHO; 2014.
3. Shankar KN, Liu SW, Ganz DA. Trends and characteristics of emergency department visits for fall-related injuries in older adults, 2003–2010. West J Emerg Med. 2017;18(5):785–793. doi:10.5811/westjem.2017.5.33615
4. Michie S. Designing and implementing behaviour change interventions to improve population health. J Health Serv Res Policy. 2008;13(3_suppl):64–69. doi:10.1258/jhsrp.2008.008014
5. Sommestad T, Karlz H, Hallberg J. A meta-analysis of studies on protection motivation theory and information security behaviour. Int J Inf Sec Priv. 2015;9(1):26–46. doi:10.4018/IJISP.2015010102
6. Rogers RW. A protection motivation theory of fear appeals and attitude change1. J Psychol. 1975;91(1):93–114. doi:10.1080/00223980.1975.9915803
7. Rogers RW. Cognitive and psychological processes in fear appeals and attitude change: a revised theory of protection motivation. Social Psychophysiol. 1983;153–176.
8. Moeini B, Ezati E, Barati M, Rezapur-Shahkolai F, Mohammad Gholi Mezerji N, Afshari M. Skin cancer preventive behaviors in Iranian farmers: applying protection motivation theory. Workplace Health Saf. 2018;2165079918796850.
9. Babazadeh T, Nadrian H, Banayejeddi M, Rezapour B. Determinants of skin cancer preventive behaviors among rural farmers in Iran: an application of protection motivation theory. J Cancer Educ. 2017;32(3):604–612. doi:10.1007/s13187-016-1004-7
10. Ali Morowatisharifabad M, Abdolkarimi M, Asadpour M, Fathollahi MS, Balaee P. The predictive effects of protection motivation theory on intention and behaviour of physical activity in patients with Type 2 diabetes. Open Access Macedonian J Med Sci. 2018;6(4):709–714. doi:10.3889/oamjms.2018.119
11. Malmir S, Barati M, Khani Jeihooni A, Bashirian S, Hazavehei SMM. Effect of an educational intervention based on protection motivation theory on preventing cervical cancer among marginalized women in West Iran. Asian Pac J Cancer Prev. 2018;19(3):755–761. doi:10.22034/APJCP.2018.19.3.755
12. Bai Y, Liu Q, Chen X, et al. Protection motivation theory in predicting intention to receive cervical cancer screening in rural Chinese women. Psychooncology. 2018;27(2):442–449. doi:10.1002/pon.v27.2
13. Sabzmakan L, Ghasemi M, Asghari Jafarabadi M, Kamalikhah T, Chaleshgar Kordasiabi M. Factors Associated with Tobacco Use among Iranian Adolescents: an Application of Protection Motivation Theory. Subst Use Misuse. 2018;53(9):1511–1518. doi:10.1080/10826084.2017.1415356
14. Macdonell K, Chen X, Yan Y, et al. A protection motivation theory-based scale for tobacco research among Chinese youth. J Addict Res Ther. 2013;4:154. doi:10.4172/2155-6105.1000154
15. Lwin MO, Stanaland AJ, Chan D. Using protection motivation theory to predict condom usage and assess HIV health communication efficacy in Singapore. Health Commun. 2010;25(1):69–79. doi:10.1080/10410230903473540
16. Zhang L, Li X, Zhou Y, et al. Predictors of consistent condom use among Chinese female sex workers: an application of the protection motivation theory. Health Care Women Int. 2015;36(7):816–833. doi:10.1080/07399332.2014.942902
17. Clemson L, Bundy AC, Cumming RG, Kay L, Luckett T. Validating the falls behavioural (FaB) scale for older people: a Rasch analysis. Disabil Rehabil. 2008;30(7):498–506. doi:10.1080/09638280701355546
18. Henseler J, Ringle CM, Sinkovics RR. The use of partial least squares path modeling in international marketing. In Advances in International Marketing|Adv. Int. Mark.. Vol. 20. Bingley: Emerald Publishing Limited. 2009. p. 277-319. (Advances in International Marketing). doi:10.1108/S1474-7979(2009)0000020014
19. Henseler J, Sarstedt M. Goodness-of-fit indices for partial least squares path modeling. Comput Stat. 2013;28(2):565–580. doi:10.1007/s00180-012-0317-1
20. Starfelt Sutton LC, White KM. Predicting sun-protective intentions and behaviours using the theory of planned behaviour: a systematic review and meta-analysis. Psychol Health. 2016;31(11):1272–1292. doi:10.1080/08870446.2016.1204449
21. Popova L. The extended parallel process model: illuminating the gaps in research. Health Educ Behav. 2012;39(4):455–473. doi:10.1177/1090198111418108
22. Ch’ng JW, Glendon AI. Predicting sun protection behaviors using protection motivation variables. J Behav Med. 2014;37(2):245–256. doi:10.1007/s10865-012-9482-5
23. Bui L, Mullan B, McCaffery K. Protection motivation theory and physical activity in the general population: a systematic literature review. Psychol Health Med. 2013;18(5):522–542. doi:10.1080/13548506.2012.749354
24. Ruthig JC. Health risk perceptions and exercise in older adulthood: an application of protection motivation theory. J Appl Gerontol. 2016;35(9):939–959. doi:10.1177/0733464814544214
25. Rippetoe PA, Rogers RW. Effects of components of protection-motivation theory on adaptive and maladaptive coping with a health threat. J Pers Soc Psychol. 1987;52(3):596. doi:10.1037/0022-3514.52.3.596
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.