")
Back to Journals » Psychology Research and Behavior Management » Volume 9
Predictors of disability-related attitudes: considering self-esteem, communication apprehension, contact, and geographic location
Authors Magsamen-Conrad K, Tetteh D, Lee YI
Received 20 May 2016
Accepted for publication 28 July 2016
Published 2 December 2016 Volume 2016:9 Pages 329—338
DOI https://doi.org/10.2147/PRBM.S113218
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Kate Magsamen-Conrad,1 Dinah Tetteh,2 Yen-I Lee3
1Department of Communication, Bowling Green State University, Bowling Green, OH, 2Department of Communication, Arkansas State University, Jonesboro, AR, 3Grady College of Journalism and Mass Communication, University of Georgia, Athens, GA, USA
Abstract: Individuals’ attitudes about persons with disability (PwD) strongly affect differently-abled persons’ quality of life and position in society. Some research offers support for the ability of systematic, supported, longitudinal contact between different groups of individuals to improve attitudes. College campuses, in particular, offer a potentially useful arena in which to facilitate this type of contact. This study explored contextual factors (eg, geographic region, biological sex) and predictors of disability-related attitudes among a college student population to determine strategies for course-based intervention design (eg, as community-engaged or service-learning initiatives). Surveying participants from universities in two regions of the United States, we found that self-esteem, audience-based communication apprehension, and contact with PwD explain more than 50% of the variance in disability-related attitudes. Further, we found that geographic location affects both self-esteem and audience-based communication apprehension (communicating/interacting with PwD). We discuss the implications for community engagement and/or service learning and highlight the importance of partnerships among relevant community stakeholders, including university faculty, students, and staff.
Keywords: community engagement, service learning, intervention, regional culture, PwD, intergroup, quality of life, college students, community partnerships
Introduction
In the United States, individuals and groups have employed multiple mechanisms to improve the quality of life for persons with disability (PwD) and facilitate their full inclusion in society. One of the major mechanisms was the Americans with Disability Act (ADA) of 1990, which criminalizes discrimination against PwD in employment, transportation, and public accommodation.1 The ADA boasts success. For example, a 2010 survey of 870 disability community leaders found that more than 90% of the respondents believed the quality of life of PwD had improved with the passage of the ADA.2 According to Frieden,2 “the ADA is helping to improve both the self-esteem of PwD, and how they are perceived by others.” However, despite the actions undertaken to ensure equal opportunity and full participation and inclusion of PwD in society,2 there are indications that some people in society still have negative attitudes toward PwD. These negative attitudes affect PwD on multiple levels.
More work is needed to understand the attitudes and beliefs that underlie behaviors toward PwD in order to affect a positive shift in disability-related attitudes. The ability of attitudes to influence behavior is well supported by previous studies3,4 as well as in interventions founded in classic behavior change theories.5,6 The foundational ideas from these theories may relate to attitudes about the self (eg, self-esteem), cultural attitudes (eg, regional culture), and/or fear about interaction with PwD (eg, communication apprehension [CA]). Existing research has established a relationship between self-esteem and CA,7 and contact with PwD and related attitudes.8–10 Other research supports the success of interaction-based interventions grounded in intergroup contact theory11–13 that facilitate a series of systematic and supportive interactions between ingroups and outgroups to positively affect health, broadly interpreted (eg, community health, relational health, self-esteem, prejudice and bias reduction).14,15 The purposes of this study are to determine: 1) the combined effects of self-esteem, CA, contact, and regional culture on attitudes toward PwD and 2) the insights these offer in designing interventions to improve engaged learning, attitudes toward PwD, and partnerships between instructors, students, PwD, and related programs. We aim to answer the following research questions: 1) How do self-esteem, CA, and frequent contact with PwD influence attitudes toward PwD? 2) How does geographic location affect self-esteem and contact, especially in the context of attitudes toward PwD?
Self-esteem, CA, contact, and attitudes
College students’ disability-related attitudes and intervention design
College students are an especially important population in the conversation about a positive shift in disability-related attitudes. This population comprises future leaders who will make decisions that directly or indirectly affect PwD. Audience-based apprehension reduction interventions can be designed and integrated into collegiate coursework. Some of the numerous studies conducted to measure students’ attitudes toward PwD have indicated a positive shift in attitudes throughout the degree program tenure, even without the implementation of a formal intervention. Researchers discovered that although there are differences in attitudes toward PwD among students pursuing various health care-related degrees at the initial stages of their degree programs, there is no difference in attitude by the end of their programs.16 Some also determined that a combined cognitive and behavioral intervention that brought students into contact with colleagues with physical disability led to a positive attitude change toward PwD.9 Other research illustrated how interactional diversity experiences in general have positive outcomes, especially for White students.17 These findings suggest that education and interventions that expose students to PwD serve an important role in improving attitudes.
Individuals’ experiences are influenced by the multiple contexts within which their lives are situated, including the social context.18,19 Therefore, it is important to study some of the major factors that can impact individuals’ attitudes toward PwD. This understanding will help improve the lives of both people with and those without disability. Understanding how college students’ attitudes toward PwD are shaped, as well as the role of regional culture, contact, and CA, will help in designing interventions especially for college student populations that can be implemented during coursework (eg, community-engaged or service-learning initiatives). This study is important because an understanding of these factors on attitudes toward PwD will enable communication scholars, educators, psychologists, and others to design interventions for improving how people perceive and relate to PwD. In the following sections, we investigate the overarching research question of how foundational concepts from behavior change theories (self-esteem, regional culture, fear about interaction with PwD, and actual contact) may explain attitudes about PwD. These concepts were selected based on their relevance to attitudes about PwD demonstrated in previous literature that could inform intervention design.
Self-esteem
Self-esteem is an internal evaluation of individuals’ worth in relation to themselves and others. Scholars have defined self-esteem as an attitude, that is, “a positive or negative attitude toward a particular object, namely, the self,”20 or as an evaluation, that is, “an evaluation, either positive or negative, of one’s own self-worth or value.”21 Many scholars discuss the relationship between self-esteem and related concepts, such as self-worth, self-image, and self-concept. The major difference indicated is that self-esteem is a value judgment based on individuals’ experiences and societal norms that people use to establish the value of “their own unique attributes and limitations.”22 Further, self-esteem is dynamic and based on various external factors, such as ingroup and outgroup culture.
Individuals’ feelings of self-esteem may vary situationally. Consider the concept of collective self-esteem, in which people vary their private and public images in terms of different relationships. Researchers23 explained how private collective self-esteem addressed individuals’ assessments of the valence of their social groups, whereas public collective self-esteem is comprised of individuals’ judgments of others’ evaluations of their social groups, similar to the concepts of descriptive and injunctive norms24 – social norms concepts that are important to behavior change and intervention design. These aspects of self-esteem are especially important to consider in the context of disability because when people with different communication and culture orientations communicate with each other, communication behaviors are malleable because interactants have different conceptions of self-esteem. Humans constantly compare themselves and their groups to others to evaluate themselves (social comparison theory).25
Self-esteem is related to stereotyping as well as to value judgments. Corrigan et al26 examined a population of people with psychiatric disabilities and found self-esteem to be one of the significant factors of stereotype awareness. Stereotyped judgments or opinions influence individuals’ self-esteem and impact their communication behaviors and attitudes toward other subjects. Self-esteem also can influence the willingness and frequency with which people have contact with other individuals.
Self-esteem and attitude toward disability
Studies that have investigated self-esteem in the context of disability have primarily focused on the self-esteem of PwD. PwD’s self-esteem can be affected by personal factors (eg, health status) and external factors (eg, sociocultural beliefs and attitudes).27 The latter includes value judgments from others in the society, which can affect not only PwDs’ self-esteems but also their interactions and communication with others and the effectiveness of health problem management strategies. Self-esteem is also an important factor in the coping strategies PwD use to manage illnesses.28 These past studies utilized the concept of self-esteem to analyze health issues, but like most of the studies concerning self-esteem and disability, the emphasis was on the PwD population. Little is known about how self-esteem of nondisabled individuals, such as college students, affects attitudes toward PwD. It is this gap in research that this study aims to fill.
Self-esteem is an internal and psychological aspect about self-value judgments. Therefore, self-esteem may influence attitudes about disability as well as degree of comfort or anxiety about communicating with PwD. As noted in the preceding paragraphs, past research has indicated a relationship between self-esteem and CA.29 The following section explores the concept of CA, especially in the context of disability.
Communication apprehension
CA is an individual’s fear or anxiety about communicating with other people.29 Scholars once theorized that CA can be both “state” (ie, based on situation) and “trait” (ie, resulting from inborn traits, genetics). Later, McCroskey et al30 expanded this conceptualization identifying four types of CA—trait-like, context-based, audience-based, and situational. They argued that the anxiety that individuals experience at one point in time is not due merely to a trait or the state of the person, but that these elements interact and the results are much more complex. CA, then, is a continuum and an individual’s position on it at a point in time (ie, degree of CA experienced) is subject to change.
CA and self-esteem
In this paper, we focus specifically on audience-based CA. Previous research has demonstrated an association between self-esteem and some types of CA. For example, scholars7 found a “substantial” correlation between CA related to oral communication and self-esteem, such that high apprehensives have lower self-esteem than moderate or low apprehensives. However, little known research has been conducted concerning audience-based CA (specifically about PwD). Past research has shown that CA can cause people to withdraw from general communication interactions with other people. Withdraw-oriented communication patterns would influence individuals’ contact experience(s) with others, especially those with disabilities. The following sections explore how CA may be related to contact with and attitudes toward PwD.
Contact with PwD
Little is known about the associations between self-esteem and contact with PwD or audience-based CA and contact with PwD. We hypothesize that self-value judgments and anxious communication behavior can affect the frequency of contact people have with PwD. Some research suggests that frequency of contact with PwD can be an implied indicator for people’s attitudes toward PwD. Numerous past studies have discovered a relationship between contact with PwD and attitudes toward such persons.8–10,16 Individuals who have frequent contact with PwD have a more positive attitude toward such people than those who have less frequent contact with PwD.8,9,16 Other researchers31 attributed the difference in attitudes toward PwD between occupational therapy and medical technology students to the knowledge about disability and contact with such persons provided by the occupational therapy curriculum. Hence, collegiate education can help improve attitudes toward PwD.
Attitude toward PwD
Attitudes toward PwD have been studied on various levels. For example, the concept has been studied as the degree of social distance between general populations and persons with intellectual disability;32 in terms of societal and individual attitudes toward PwD;8 or the factors (eg, social situation and disability) that influence attitudes toward PwD.33 Further research has supported the conclusion that attitudes toward PwD vary depending on the disability, social context, and the interaction between the two.34,35 Also, attitude toward PwD is influenced by amount/level of contact and training about PwD,8,9,36,37 age, level of education, occupational grouping,36–38 and biological sex.39
In addition, contact with PwD is a predictor of disability-related attitudes, and CA may be a predictor of contact. CA is associated with attitudes in general because apprehension influences behavior. Specifically, research has established that CA is related to students’ attitudes toward school, specific types of instruction, and performance.29,40,41 We seek to understand the association between CA and disability-related attitudes. It stands to reason that highly apprehensive individuals (ie, audience-based CA) would prefer to have less social contact with PwD and would therefore have less positive attitudes toward PwD than low apprehensives.
Scholars have argued that measuring attitudes toward PwD does not directly affect the lives of PwD or influence behavior especially if the attitude is general and not contextualized.16 However, negative attitudes toward PwD have implications for these individuals and society at large. For instance, preexisting stereotypes, negative perceptions, and lack of knowledge about PwD can reinforce negative attitudes.35 Therefore, the ability to articulate and understand predictors of attitudes toward PwD is important. This question is especially important in the college student population, the future leaders, and policymakers of our country.
Regional differences
Existing research supports the contention that people from different regions of the US have different attitudes. Past studies have revealed that geographic regions differ in diversity (eg, the Midwest is a more homogenous region with less diversity than the East Coast);41 thus, people from those regions have different attitudes, thoughts, feelings, and behaviors toward social and civic engagement.42,43 Additionally, scholars determined that the geographic region also influences the behavior of voting registration; for example, people are 20% more likely to register to vote in the Mid-West than in the South.44 Moreover, researchers found that the ADA significantly influenced job accommodation in the Mid-West.45 According to these studies, the regions play a significant role to influence people’s attitude toward social and health issues as well as lead to different outcomes of ADA implementation.
One goal of this study is to understand potential predictors of disability-related attitudes among college students with a future goal of designing interventions that positively affect disability-related attitudes. In order to appropriately tailor intervention design, we seek to understand the potential effect of culture, viewing culture from a geographic regional lens. Little is known about potential regional differences in self-esteem. Some research indicates cultural differences in self-esteem42 and cultural differences in sources of self-esteem (eg, benevolence, merit, and bias).43 Regional areas of the US may collectively illustrate “cultural” differences. For example, past research indicates regional differences in attitudes about corporal punishment,44 violence,45 gender roles,46 and the “culture of honor” in the southern US.47 Thus, we ask: how does the geographic region affect self-esteem, contact, and attitudes?
Methods
Participants and procedure
The participants (N=243) in this study were students in undergraduate programs in universities in the Mid-West (n=117) and on the East Coast (n=126) in the US. Seventy-five (n=75) males, 150 (n=150) females, and 18 people who did not specify their biological sex participated. The average age of the participants was 22 (standard deviation [SD] =3, range =19–51). Participants were predominately Caucasian (69.5%); others were Black (20.4%), Hispanic/Latino/Mexican (6.1%), Asian (2%), and Biracial (2%).
Procedure
We collected the data using convenience and network sampling methods. Researchers briefly explained the study before participants completed a survey (30 minutes) either on paper or through an online link disseminated by university instructors. After participants read and signed consent forms, participants decided to complete the survey or declined to participate in this study. Some participants received an extra credit for participation; this was determined by the instructor. This research was approved by the Human Subjects Review Board, Bowling Green State University (Bowling Green, OH, USA).
Measures
The main variables measured were self-esteem, audience-based CA, contact with PwD, and attitudes toward PwD, as well as biological sex and geographic location (see Table 1).
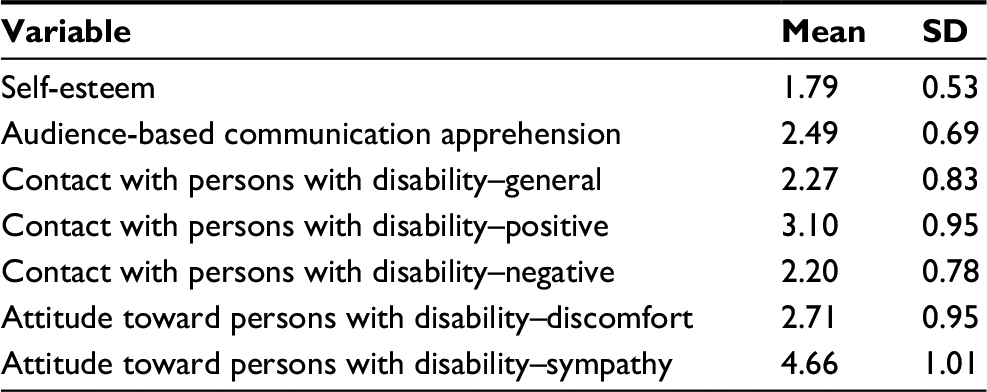 | Table 1 Descriptions of study variables Abbreviation: SD, standard deviation. |
Self-esteem
We used Rosenberg’s20 self-esteem scale to measure participants’ self-esteem. The scale consists of ten items, with a 4-point scale ranging from I strongly agree (1) to I strongly disagree (4). Half of the items were keyed negatively and half positively to control for any acquiescence response bias (eg, “I feel that I have a number of good qualities” and “I feel I do not have much to be proud of”). The items have good reliability (α=0.87, M=1.79, SD =0.53; eigenvalue =4.84; 48.35% variance [var]). In the original scale, higher values indicate lower self-esteem. However, to keep coding consistent with other study variables, we recoded the items in the scale such that a higher score indicates higher self-esteem.
Audience-based CA
We adapted McCroskey’s48 Personal Report of Communication Apprehension scale to measure participants’ CA toward PwD (audience-based CA). The Personal Report of Communication Apprehension scale has 12 items with responses ranging from strongly disagree (1) to strongly agree (5). One sample item includes “I am calm and relaxed while communicating with people with disabilities (R).” A factor analysis indicated a single factor (eigenvalue =7.25; 60.42% var). The items had good reliability (α=0.94, M=2.49, SD =0.69) and were averaged such that a higher score means more CA with PwD.
Contact with PwD
We used Yuker and Hurley’s10 Contact with Disabled Persons scale to measure how frequently participants were in contact with PwD. It is a 20-item Likert-type scale with responses ranging from never (1) to very often (5). A factor analysis indicated three factors after items 4, 9, and 16 were eliminated for loading below 0.40; this is consistent with past research.49 The first factor (general contact) included items 1, 2, 5, 6, 7, 8, 10, 11, and 12; the second factor (positive contact experience) included items 13, 15, 18, and 19; and the third factor (negative contact experience) included items 14, 17, and 20. The coefficient alpha for factor one (general contact) was 0.90 (eigenvalue =7.41; 43.85% var, M=2.27, SD =0.83). The coefficient alpha for factor two (positive contact experience) was 0.88 (eigenvalue =2.29; 13.50% var, M=3.10, SD =0.95). The coefficient alpha for the third factor (negative contact experience) was 0.81 (eigenvalue =1.42; 8.35% var, M=2.02, SD =0.78). Items on all the subscales were averaged such that a higher score means contact that is more frequent with PwD. Note that although some items are negatively valenced, for example, “How often have you had unpleasant experiences interacting with disabled persons?,” all items are scored the same way because the scoring is based on the assumption that the frequency of contact is more important than the valence of the contact.10
Attitudes toward PwD
To measure participants’ attitudes toward PwD, we used Gething’s37 20-item Likert-type scale called Interaction with Disabled Persons scale. This scale was developed as an alternative to other instruments used to measure people’s attitudes toward PwD, such as the Attitude Toward Disabled Persons scale and the Scale of Attitudes toward Disabled Persons.4 Responses to the items on the scale range from strongly disagree (1) to agree very much (6). Items 10, 14, and 15 were reverse coded consistent with previous research37,50 and a factor analysis indicated two factors. Factor one (discomfort) included items 9, 11, 12, 16, 17, 18, and 20 (eigenvalue =3.84; 42.69% var). Factor two (sympathy) included items 2 and 3 (eigenvalue =1.50; 16.71% var). The coefficient alpha for each factor was 0.85 (M=2.71, SD =0.95) and 0.69 (M=4.66, SD =1.01), respectively. A higher score for the discomfort factor means a negative attitude and a higher score for the sympathy factor means a positive attitude, consistent with the coding in previous research.
Results
We used version 19 of the SPSS software (IBM Corporation, Armonk, NY, USA) to analyze the data. Table 2 presents the zero-order correlation matrix for all variables.
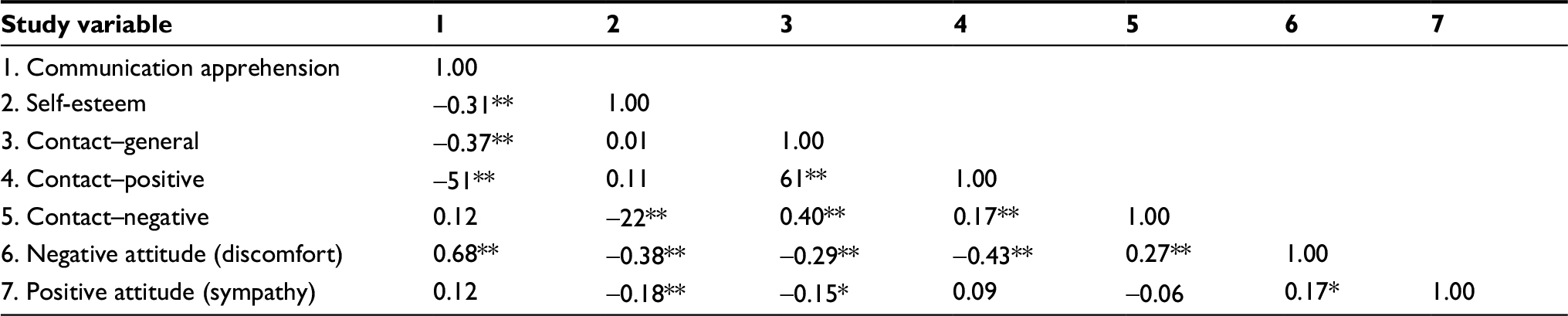 | Table 2 Correlation matrix for study variables Note: **P≤0.01, *P≤0.05, two-tailed. |
We utilized t-tests, regressions, and analysis of variance analyses to test the research questions with the alpha level was set at P<0.05 for all analyses. Results are presented next by research question.
The overarching research question asked how self-esteem, CA, and frequent contact with PwD influence attitudes toward PwD. To explore this relationship, we conducted a stepwise regression with attitude as the criterion and self-esteem, CA, and contact with PwD as the predictors. The first step was significant (adjusted R2=0.45, F(1,213)=178.33, P<0.001); CA positively (β=0.68, t=13.35, P<0.001) predicted negative attitude (discomfort) toward PwD. The second step produced a significant change, ∆R2=0.49, F(2,212)=103.96, P<0.001, with self-esteem negatively predicting attitude (discomfort) (β=−0.21, t=−4.07, P<0.001). The third step produced a significant change, ∆R2=0.51, F(3,211)=74.86, P<0.001, with negative contact with PwD positively predicting attitude (discomfort) (β=0.15, t=2.98, P<0.01). In the final model, more CA, lower self-esteem, and more contact that is negative predicted 52% of the variance in attitude (discomfort) toward PwD. The results are shown in Table 3. We also explored the effects of sex and regional differences for all study variables and the only significant difference was for self-esteem. This is illustrated in Table 4.
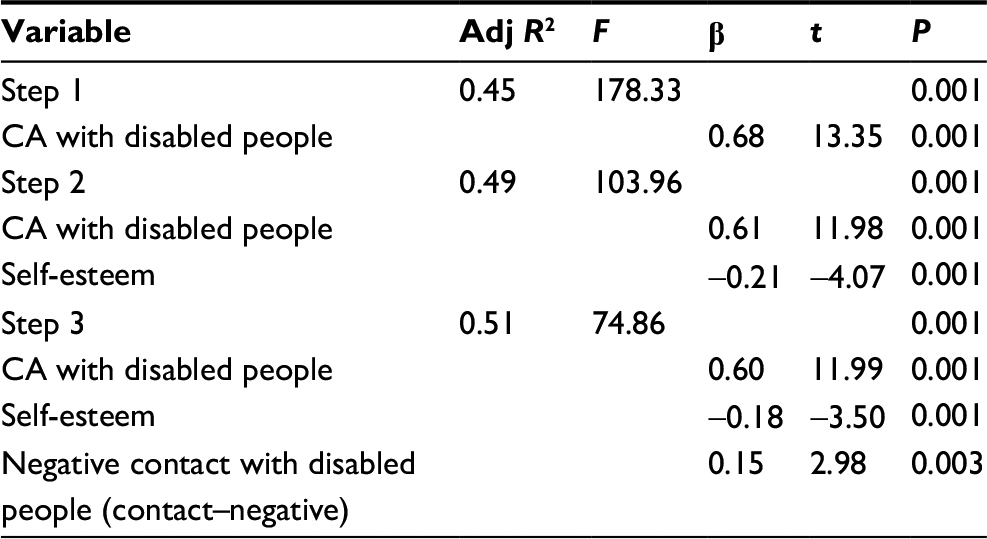 | Table 3 Summary of stepwise regression for attitude toward PwD Abbreviations: Adj, adjusted; CA, communication apprehension; PwD, persons with disability. |
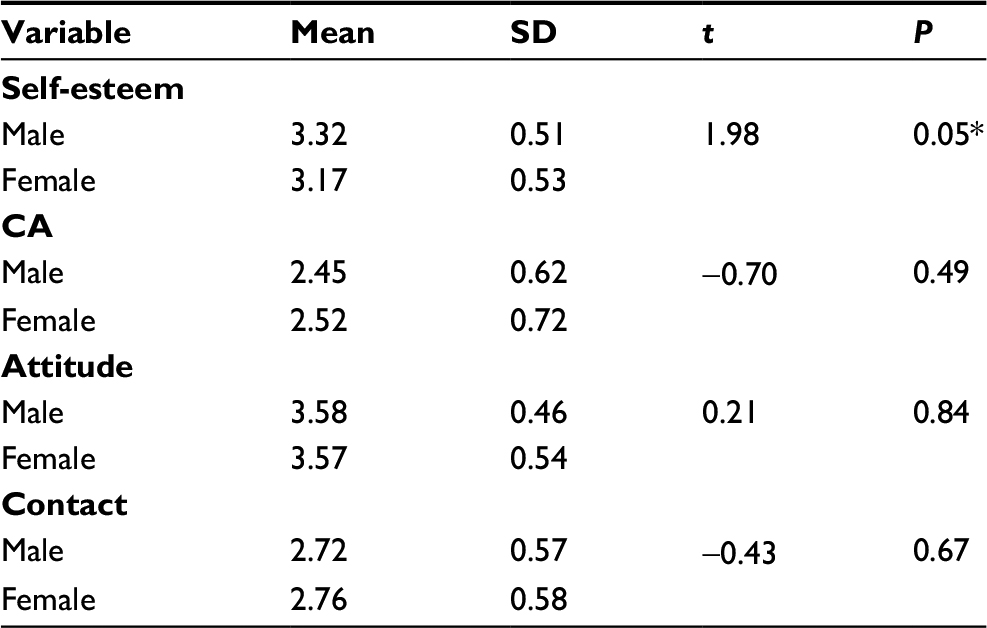 | Table 4 Independent samples t-test for sex differences among all study variables Note: *P≤0.05, two-tailed. Abbreviations: CA, communication apprehension; SD, standard deviation. |
Finally, we asked how geographic location affects self-esteem, contact, and attitudes toward PwD. The results of an analysis of variance illustrated a significant main effect for geographic location and self-esteem (F(1,227)=8.01, P<0.01), suggesting that Mid-West students had higher self-esteem (M=1.71, SD =0.51) than East Coast students (M=1.88, SD =0.54), confirming a geographic difference for self-esteem. Again, there was a significant main effect for geographic location and discomfort-related attitude (F(1,226)=6.17, P<0.01), indicating that East Coast students (M=2.86, SD =0.93) had more discomfort when interacting with PwD than Mid-West students (M=2.55, SD =0.94), confirming a geographic difference for discomfort. There was a significant effect for geographic location and sympathetic attitude (F(1,228)=4.01, P<0.05), indicating that East Coast students (M=4.79, SD =0.98) had more sympathetic attitude toward PwD than Mid-West students (M=4.53, SD =1.40). However, there was no significant effect between geographic location and contact with PwD (F(1,227)=0.33, P>0.05). Results are shown in Table 5.
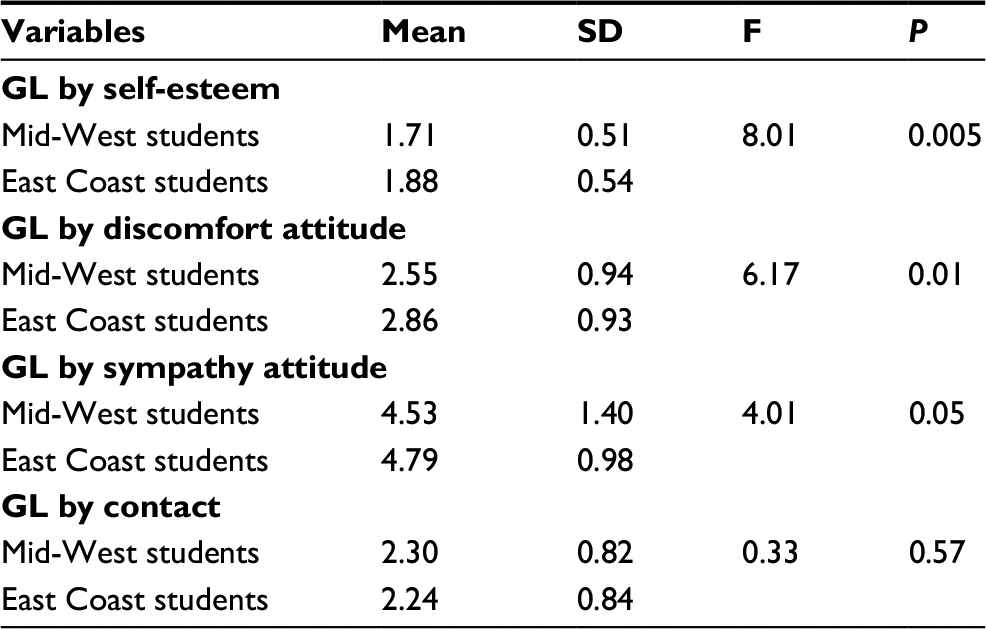 | Table 5 Factorial ANOVA for geographic location (GL) moderate variable Abbreviations: ANOVA; analysis of variance; SD, standard deviation. |
Discussion
The aim of this study was to find out how self-esteem, CA, and contact with PwD influence college students’ attitudes toward individuals with disability. We also wanted to examine how geographic location and biological sex affect the relationship between potential intervention variables and attitudes toward PwD. Our overall goal was to broaden understanding on best practices to improve community engagement experiences for students and members of the community they engage with, including PwDs. The results from this study are consistent with past research that suggested an association among self-esteem, CA, contact, and attitudes toward PwD. This research has implications for course-based intervention design, especially for service learning and community engagement.
Contributions and implications for service learning
This study provides insight into disability-related attitude shifting course-based intervention design, most especially those that promote engaged and reciprocal learning accomplished through effective partnership among students, PwD, faculty, and agencies. Further, research indicates that effective partnerships are the key to enabling students, faculty, organizations, universities, and communities to build beneficial situations that advantage reciprocal learning.51 In this study, we were able to explain more than 50% of the variance in college students’ attitudes toward PwD with concepts of self-esteem, audience-based CA, and contact. Further, audience-based CA emerged as the strongest predictor of disability-related attitudes. Thus, it is important to provide activities and training that encourage and promote students’ self-esteem prior to engaging with community members in service learning and community engagement projects. This training, which can be provided by community agencies or faculty in relevant disciplines, will help prepare students psychologically before they embark on community engagement projects, facilitating project success and the forging of lasting partnerships with relevant community stakeholders.
The results of our study also highlight the benefit of frequent contact with PwD to improving attitudes toward such individuals. However, as explained earlier, CA can inhibit efforts at promoting frequent contact with PwD. The insight that project designers, faculty, community agencies, administrators, disciplines, and other stakeholders can draw from our research is how to increase students’ self-esteem, decrease CA, and improve contact with PwD when designing community-engaged learning projects to influence people’s attitudes toward PwD. We suggest turning to interventions designed to help people cope with CA52–54 as models to adapt. Future partners can utilize this knowledge to develop interventions especially for college students that involve systematic, supported contact with PwD through college coursework that would systematically desensitize audience-based CA (with PwD) and ultimately positively affect disability-related attitudes.
The wealth of existing CA reduction research is an asset to the application of CA in this context and offers recommendations for how to prepare to enter a service-learning partnership with PwD. CA interventions are categorized as cognitive, affective, and behavioral and include systematic desensitization, cognitive modification, skills training, and visualization.52 For example, systematic desensitization has been shown to be an effective intervention measure to improve CA53,54 because it helps overcome withdrawal from communication interactions that people experience as a result of CA, thereby helping them make their full contributions to society. Existing interventions for CA involve strategies that encourage people to think about or imagine themselves doing something that they could previously not do, such as speaking in front on an audience; these intervention strategies prove successful over a period of time and can be generalized to situations outside the controlled experimental settings.54 These CA intervention strategies have been found to be effective depending on the mode of delivery and the individual characteristics of people for whom the interventions are designed.52 In addition, Bowland et al55 found that the values of mutual positive regard, such as treating each other with warmth, respect, sympathy, and civility in a give-and-take exchange, positively impact results of community activities on community residents. Thus, community partners interested in disability-attitude change should integrate aspects of the cognitive, affective, and behavioral in order to be effective, because attitudes are formed based on cognitive process, behavioral, and affective practices. This means that community-engaged learning projects aimed to improve attitudes toward PwD should be process-based to help people to take time to adjust to the idea of dealing/interacting with others with disability. The process can include series of activities and trainings offered by community agencies and interdisciplinary faculty members. In addition, to ensure effective community-engaged projects aimed at improving attitude toward PwD, audience (PwD)-based intervention design should include aspects that help condition the minds of participants and provide positive visual and mental images of the benefits of having a positive attitude toward PwD.52 Participants (especially students) should be reminded of the benefits of having positive attitudes toward PwD as they progress through the intervention process. This will help bring the broader societal/community goals of the project into perspective for participants; painting a clear and straightforward picture of the impact of positive attitudes toward PwD can help all those involved.
Other components of intervention design
This study also explored the effects of self-esteem, contact, biological sex, and regional culture in order to recommend intervention design strategies. Our results elucidate potential areas of focus for community partners to consider when planning interventions to positively affect disability-related attitudes.
Self-esteem, sex, and geographic location
Studies considering self-esteem and attitudes focus on the relationship between self-esteem and value expression or value-relevant involvement, indicating that self-esteem is an important determinant of individual attitudes.55–58 Overall, we discovered minimal difference in self-esteem between males and females, consistent with some previous studies.27 One possible explanation for this is that education helps reduce the differences between the self-esteem of males and females; this result was not surprising considering our population was college students. However, we did find some interaction effects between geographic location and self-esteem. These findings indicate that intervention designs should consider the potential impact of geographic location and regional culture on self-esteem. Thus, community engagement project planning must carefully consider the prevailing culture of the location and how this might influence the attitudes of community partners involved in the project. Designers should conduct a thorough research and assessment of the geographic location utilizing partnerships with relevant community stakeholders.
Many past studies on self-esteem simply compared the level of self-esteem among people from Eastern and Western cultures, but little work has been done to examine how the different social and geographic contexts within the same country might influence self-esteem. The results of the present study showed a difference in self-esteem among students from the Mid-West and East Coast regions of the US, reflecting the notion of collective self-esteem instead of personal self-esteem.23 An explanation for this difference could be found in the cultural and environmental differences between the two regions, which might influence the differential experiences of people residing in these parts of the US. Thus, both personal and collective experiences can impact students’ attitudes toward PwD in these two regions. Further, biological sex and geographic location affected students’ sympathetic attitudes toward PwD: students from the East Coast displayed less social distance toward PwD than those from the Mid-West. Thus, geographic location has some influence on people’s positive attitude toward PwD, and this knowledge should be utilized in designing interventions.
Limitations and future research
One noted limitation to this study is that participants were a convenience sample of college students, which could have affected the results of our study because college students are noted to have different characteristics and orientations toward issues than the general population. However, we specifically targeted college students due to their importance in future leadership and the ability to implement interventions with this population. The sampling strategy also limits our regional comparison in analysis. Another limitation is the notion of social desirability in that participants tend to give favorable responses to questions in order to appear good before people. Thus, answers participants provided might not reflect their true self-esteem, CA, contact with or attitudes toward PwD. In addition, it is important to mention that there are many variables related to attitudes toward PwD that could have been examined. However, in this study, we chose to focus on self-esteem, contact with PwD, and CA.
Future research should explore these findings among members of the general population as participants using a random sampling strategy. In addition, future research can integrate other methodologies to explore this issue further with the hope of providing a better understanding of the factors that can influence individuals’ attitudes toward PwD. To provide a comprehensive view of the factors that predict attitudes toward PwD, future research can investigate different predictors of attitudes toward PwD beside those examined in this study.
Conclusion
This study broadens understanding on best practices to improve community engagement experiences for students and members of the community they engage with and contributes to knowledge about designing interventions that positively affect attitudes about PwD. The results of this study suggest factors community agencies, faculty members, administrators, and intervention designers should consider (ie, self-esteem, CA, and contact) when designing community engagement projects aimed at improving attitudes toward PwD. We highlight the need for partnerships among relevant community stakeholders and university faculty, staff, and students in forging lasting and meaningful community engagement and service-learning initiatives. Our suggestions may be particularly impactful for college students, who may still be in the learning stages of molding attitudes toward differently-abled individuals. Community partnerships are pertinent to exposing college students to “different” others and giving all participants the opportunity to build their self-esteem and decrease audience-based CA. This study suggests ways to augment and develop mechanisms that improve the quality of life for PwD and facilitate their full inclusion in society, ultimately contributing to a healthy society. Finally, our findings extend the potential impact of the CA literature, expanding applicability into new contexts, including service learning and community engagement.
Acknowledgments
The research was funded, in part, by the Bowling Green State University (BGSU) Office of the Vice President for Research and Economic Development 2013 Building Strength Program and the BGSU Service Learning Community (2013). Additionally, this research was supported in part by the Center for Family and Demographic Research, BGSU, which has core funding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development [R24HD050959].
Disclosure
The authors report no conflicts of interest in this work.
References
U.S. Department of Justice. A Guide to Disability Rights Law; 2009. Available from: http://www.ada.gov/cguide.htm. Accessed July 11, 2013. | ||
Frieden L. Impact of the ADA in American Communities; 2010. Available from: http://www.dvrgetsjobs.com/Documents/Pubs/ImpactOfTheADA.pdf. Accessed July 11, 2013. | ||
Antonak RF, Livneh H. Measurement of attitudes towards persons with disabilities. Dis Rehab. 2000;22(5):211–224. | ||
Tait K, Purdie N. Attitudes towards disability: teacher education for inclusive environments in an Australian university. Intl J Dis Dev Ed. 2000;47(1):25–38. | ||
Fishbein M, Ajzen I. Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research. Reading, MA: Addison-Wesley; 1975. | ||
Ajzen I. From intentions to actions: A theory of planned behavior. In: Kuhl J, Beckman J, editors. Action-Control: From Cognition to Behavior. Heidelberg: Springer;1985:11–39. | ||
McCroskey JC, Richmond VP, Daly JA, Falcione RR. Studies of the relationship between communication apprehension and self-esteem. Hum Com R. 1977;3(3):269–277. | ||
Daruwalla P, Darcy S. Personal and societal attitudes towards disability. Ann Tourism Res. 2005;32(3):549–570. | ||
Krahé B, Altwasser C. Changing negative attitudes towards physical disability: An experimental intervention. J Commun Appl Soc Psychol. 2006;16:59–69. | ||
Yuker HE, Hurley MK. Contact with and attitudes towards persons with disability: The measurement of intergroup contact. Rehabil Psychol. 1987;32(3):145–154. | ||
Allport GW. The Nature of Prejudice. Reading, MA: Addison Wesley; 1954. | ||
Pettigrew TF. Intergroup contact theory. Annu Rev Psychol. 1998;49:65–85. | ||
Pettigrew TF, Tropp LR. A meta-analytic test of intergroup contact theory. J Per Soc Psychol. 2006;90(5);751–783. | ||
Magsamen-Conrad K, Hanasono LK, Billotte Verhoff C. Health communication in the context of aging: The development of an Intergenerational Communication Intervention to reduce biases and discrimination. In: Eaves M, editor. Applications in Health Communication: Emerging Trends. Dubuque, IA: Kendall Hunt; 2013:101-125. | ||
Magsamen-Conrad K. Digital native, meet digital immigrant: Building intergenerational relationships through a technology literacy project [2014]. Community Works Journal. Available at: http://communityworksinstitute.org/cwjonline/articles/aarticles-text/digitalnatives.html. Accessed October 12, 2016. | ||
Stachura K, Garven F. Comparison of occupational therapy and physiotherapy students’ attitude towards PwD. Phychol. 2003;89(11):653–644. | ||
Hu S, Kuh GD. Diversity experiences and college student learning and personal development. J Coll Student Dev. 2003;44:320–334. | ||
Bronfenbrenner U. Ecological systems theory. In: Vasla R, editor. Annals of Child Development. Greenwich, CT: JAI Press; 1989:187–249. | ||
Umaña-Taylor AJ, Shin N. An examination of ethnic identity and self-esteem with diverse populations: exploring variation by ethnicity and geography. Cultur Divers Ethnic Minor Psychol. 2007;13(2):178–186. | ||
Rosenberg M. Society and the Adolescent Self-Image. Princeton, NJ: Princeton University Press. 1965. | ||
Johnson P. The prevalence of low self-esteem in an intellectually disabled forensic population. J Intellect Disabil Res. 2012;56(3):317–325. | ||
Miyahara M, Piek J. Self-esteem of children and adolescents with physical disabilities: Quantitative evidence from meta-analysis. J Dev Phychol Dis. 2006;18(3):219–324. | ||
Luhtanen R, Crocker J. A collective self-esteem scale: self-evaluation of one’s social identity. Pers Soc Psychol Bul. 1992;18:302–318. | ||
Park HS, Smith SW. Distinctiveness and influence of subjective norms, personal descriptive and injunctive norms, and societal descriptive and injunctive norms on behavioral intent: A case of two behaviors critical to organ donation. Hum Commun Res. 2007;93:194–218. | ||
Festinger L. A theory of social comparison processes. Hum Relat. 1954;7(2):117–140. | ||
Corrigan PW, Watson, AC, Barr L. The self-stigma of mental illness: Implications for self esteem and self-efficacy. J Soc Clin Psychol. 2006;25(9):875–884. | ||
Omolayo B. Self-esteem and self-motivational needs of disabled and non-disabled: A comparative analysis. J Alter Pers Soc Sci. 2009;1(2):449–458. | ||
Dahlbeck DT, Lightsey OR Jr. Generalized self-efficacy, coping, and self-esteem as predictors of psychological adjustment among children with disabilities or chronic illnesses. Child Health Care. 2008;37:293–315. | ||
McCroskey JC. Classroom consequences of communication apprehension. Commun Educ. 1977;26:27–33. | ||
McCroskey JC, Richmond VP, Davis LM. Apprehension about communicating with supervisors: A test of a theoretical relationship between types of communication apprehension. West J Speech Commun. 1986;50(2):171–182. | ||
Estes JP, Deyer CA, Hansen RA, Russell JC. Influence of occupational therapy curricula on students’ attitudes toward persons with disabilities. Am J Occup Ther. 1991;45(2):156–159. | ||
Morin D, Rivard M, Crocker AG, Boursier CP, Caron J. Public attitudes towards intellectual disability: A multidimensional perspective. J Intellect Disabil Res. 2013;57(3):279–292. | ||
Grand SA, Bernier JE, Strohmer D. Attitudes toward disabled persons as functions of social context and specific disability. Rehab Psychol. 1982;27(3):165–174. | ||
Gordon ED, Minnes PM, Holden, RR. The structure of attitudes towards persons with a disability: When specific disability and context are considered. Rehabil Psychol. 1990;35(2):79–90. | ||
Shannon CD, Schoen B, Tansey TN. The effect of contact, context, and social power on undergraduate attitudes toward persons with disabilities. J Rehabil. 2009;75(4):11–18. | ||
Forlin C, Fogarty G, Carroll AM. Validation of the factor structure of the Interactions with Disabled Persons Scale. Aust J Psychol. 1999;51(1):50–55. | ||
Gething L. Interaction with Disabled Persons Scale: Manual and Kit. Sydney, Australia: University of Sydney; 1991. | ||
Ouellette-Kuntz H, Burge P, Brown, HK, Arsenault E. Public attitudes towards individuals with intellectual disabilities as measured by the concept of social distance. JARID. 2010;23:132–142. | ||
MacLean D, Gannon PM. Measuring attitudes toward disability: The Interaction with Disabled Persons Scale revisited. J Soc Behav Pers. 1995;10(4):791–806. | ||
Scott MD, Wheeless LR. Communication apprehension, student attitudes, and levels of satisfaction. West J Speech Commun. 1977;41(3):188–198. | ||
Hurt TH, Preiss R. Silence isn’t necessarily golden: Communication apprehension, desired social choice, and academic success among middle-school students. Hum Commun Res. 1978;4(4):316–328. | ||
Song H, Cai H, Brown JD, Grimm KJ. Differential item functioning of the Rosenberg Self-Esteem Scale in the US and China: measurement bias matters. Asian J Soc Psychol. 2011;14(3):176–188. | ||
Kwan VY, Lu K, Hui NH. Identifying the sources of self-esteem: the mixed medley of benevolence, merit, and bias. Self Identity. 2009;8(2/3):176–195. | ||
Flynn CP. Regional differences in attitudes toward corporal punishment. J Marriage Fam. 1994;56(2):314–324. | ||
Nisbett RE. Violence and U.S. regional culture. Am Psychol. 1993;48(4):441–449. | ||
Rice TW, Coates DL. Gender role attitudes in the Southern United States. Gend Soc. 1995;9(6):744–756. | ||
Cohen D, Nisbett RE. Self-protection and the culture of honor: explaining Southern violence. Pers Soc Psychol Bul. 1994;20(5):551–567. | ||
McCroskey JC. Validity of the PRCA as an index of oral communication apprehension. Commun Monogr. 1978;45:192–203. | ||
Pruett S, Lee E, Chan F, Wang M, Lane F. Dimensionality of the contact with disabled persons scale: Results from exploratory and confirmatory factor analyses. Rehab Couns Bul. 2008;51(4):210–220. | ||
Thomas A, Palmer JK, Coker-Juneau CJ, Williams DJ. Factor structure and construct validity of the interaction with disabled persons scale. Educ Psychol Meas. 2003;63(3):465–483. | ||
Hosman L. International service-learning partnerships: lessons of successes and challenges that defy simple categorization. Part: J Ser Lear Civ Engeg. 2014;5(1):24–50. | ||
Ayres J, Heuett B, Sonandre DA. Testing refinement in an intervention for communication apprehension. Commun Rep. 1998;11(1):73–83. | ||
Kondas O. Reduction of examination anxiety and ‘stage-fright’ by group desensitization and relaxation. Behav Res Ther 1967;5(4):275–281. | ||
McCroskey JC. The implementation of a large scale program of systematic desensitization for communication apprehension. Speech Ther. 1972;21:255–264. | ||
Bowland S, Hines-Martin VP, Edward J, Haleem AS. Reflection on interdisciplinary teamwork in service-learning. Part: J Ser Lear Civ Engag. 2015;6(2):19–35. | ||
Cha NH, Seo EJ, Sok S. Factors influencing the successful aging of older Korean adults. Contemp Nurse. 2012;41(1):78–87. | ||
Levin KD, Nichols DR, Johnson BT. Involvement and persuasion: Attitude functions for the motivated processor. In: Olson JM, Maio GR, editors, Why We Evaluate: Functions of Attitudes. Mahwah, NJ: Lawrence Erlbaum Associates. 2000:163–194. | ||
Wiersema DV, Harreveld F, Pligt J. Shut your eyes and think of something else: Self-esteem and avoidance when dealing with counter-attitudinal information. Soc Cognition. 2012;30(3):323–334. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.