")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 11
Predictors of chronic kidney disease among HIV–infected patients on highly active antiretroviral therapy at the University of Calabar Teaching Hospital, Calabar, South-South Nigeria
Authors Okpa HO, Bisong EM, Enang OE, Effa EE , Monjok E , Essien EJ
Received 5 October 2018
Accepted for publication 18 February 2019
Published 5 April 2019 Volume 2019:11 Pages 61—67
DOI https://doi.org/10.2147/HIV.S189802
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Bassel Sawaya
Henry Ohem Okpa,1,2 Elvis Mbu Bisong,3 Ofem Egbe Enang,2,4 Emmanuel Edet Effa,1,2 Emmanuel Monjok,3,5 Ekere James Essien5
1Renal Unit, Department of Internal Medicine, University of Calabar Teaching Hospital, Calabar, Nigeria; 2Department of Internal Medicine, University of Calabar, Calabar, Nigeria; 3Department of Family Medicine, University of Calabar, Calabar and University of Calabar Teaching Hospital, Calabar, Nigeria; 4Endocrine and Metabolism Unit, University of Calabar Teaching Hospital, Calabar, Nigeria; 5Institute of Community Health, University of Houston, Texas Medical Center, Houston, TX, USA
Background: The burden of the people living with human immunodeficiency virus (HIV) infection and the acquired immunodeficiency syndrome (AIDS) is largely borne by communities in Sub-Saharan Africa. The rate of kidney disease is increasing amongst HIV patients and occurs more often in patients with advanced stage of the disease with lower CD4 counts and associated with a high rate of morbidity and mortality. The objective of this study is to determine the prevalence and predictors of chronic kidney disease (CKD) amongst HIV patients on highly active antiretroviral therapy (HAART) at the University of Calabar Teaching Hospital, Calabar.
Materials and methods: This was a cross-sectional study that was carried out over a 4-month period from May to August 2018. In all, a total of 118 patients with HIV on HAART were recruited into the study in a consecutive manner and their serum creatinine measured with the calculation of estimated glomerular filtration rate (eGFR). Other data collected were sex, age, weight, height, body mass index (BMI), waist hip ratio (WHR), packed cell volume, CD4 count etcetera. Data collected were inputted and analyzed with SPSS version 18, and statistical significance was taken to be p<0.05.
Results: There were more females (69.5%) amongst the HIV participants and the prevalence of CKD was 15.3%. The risk factors seen to be associated with CKD were lower levels of CD4 count below 200 cells/μl, lower PCV, weight, BMI, and eGFR. Also, higher levels of WHR and creatinine were associated with CKD. Factors directly correlated with CKD were weight, BMI and CD4 count levels, while creatinine level was inversely correlated with CKD. However, a logistic regression model showed only creatinine to be a predictor of CKD.
Conclusion: HIV patients on antiretroviral therapy, mainly the highly active antiretroviral therapy (HAART) have a relatively high prevalence of CKD of 15.3% and high level of serum creatinine was predictive of CKD in the logistic regression model in our study.
Keywords: predictors, chronic kidney disease, HIV, South – South, Nigeria
Introduction
The burden of the people living with human immunodeficiency virus (HIV) infection and the acquired immunodeficiency syndrome (AIDS) is largely borne by communities in Sub-Saharan Africa1 in which Nigeria is included.
Kidney disease is an important complication in HIV patients with an increasing rate in its prevalence. This kidney-related disease tends to occur more often in patients with advanced stage of the HIV infection with lower CD4 counts and is associated with a high rate of morbidity and mortality.2
Relevant comorbid conditions such as chronic kidney disease (CKD) and end-stage renal disease (ESRD) are found in HIV-infected individuals.3 Also, the risk of ESRD as shown by the United States renal data system is said to be 50-fold higher in African Americans living with HIV than in HIV-infected white patients.4
About 30% of HIV-infected patients have been shown to have abnormal kidney function, with HIV-related kidney disease becoming a main cause of ESRD requiring dialytic intervention, with subsequent progression of kidney disease to AIDS and ultimately death.5
In Nigeria, the overall prevalence of renal disorders among HIV-infected patients is not known. A study from Ile–Ife reported a prevalence of 38% for HIV-associated nephropathy (HIVAN),6 while another study in Jos showed a prevalence of 51.8% for renal disease in HIV-infected patients.7 Other studies done in South-East and South-West Nigeria showed prevalences of 22.9%8 and 23.5%9 respectively.
A study in Baltimore, USA showed that, in a kidney biopsy report amongst some CKD patients of African American descent, there was a 3-fold higher rate in the risk of progression to ESRD with HIVAN than in those with other forms of renal histopathologic lesions.10
The pathologic characteristics of HIV-associated CKD is varied in nature, with biopsy and autopsy series showing a wide range of pathologic lesions during analysis of the tissues.11–14 However, among the African descendants, mostly found is the collapsing variant of focal segmental glomerulosclerosis, termed “HIVAN,”11,14,15 which has been reported to have a more aggressive downward course and rapid progression to ESRD.16,17
The increased availability and usage of HAART by HIV-infected patients has influenced the rise of kidney diseases, as most HIV patients now live longer to develop such complications associated with the kidneys.18 However, there is an appreciable reduction in the risk of developing ESRD by 40–60%, mainly due to the slower clinical course of kidney disease among HIV patients, with an attendant increase from 25% to 75% in the 1-year survival rate while undergoing dialysis and renal transplantation is a successful treatment option.19,20
Kidney disease and its associated risk factors are frequently found among HIV-infected patients, irrespective of the improvements with the use of HAART, and it remains a cause of morbidity and mortality.21 The associated risk factors for kidney in this population include black race, older age, hypertension, diabetes, low CD4 cell count, and high viral load.21
Also, acute or chronic kidney disease has been shown to be associated with the use of antiretroviral regimens.21 Drugs such as tenofovir and some protease inhibitors have been implicated as a cause of severe renal impairment.22
There are still very few studies in Nigeria, particularly in the South-South region of the country where our institution is located that conducted a study on the prevalence and predictors of CKD among HIV patients on HAART.
These findings prompted us to undertake this study in order to determine the prevalence and risk factors associated with CKD in HIV patients on HAART at the University of Calabar Teaching Hospital, Calabar.
Materials and methods
Study design, settings, and population
This was a cross-sectional study that was conducted in the special treatment clinic for HIV patients at the University of Calabar Teaching Hospital (UCTH), Calabar over a 4 month period from May to August, 2018.
A total of 118 HIV patients on HAART attending the special treatment clinic were consecutively recruited after meeting the study criteria and all participants provided written informed consent.This study was conducted in accordance with the Declaration of Helsinki.
All subjects underwent interview by using a structured questionnaire.
Information regarding patients’ age, sex, occupation, religion, and educational status were obtained. Moreso, information on the family history of hypertension and history suggestive of renal disease were obtained. All subjects were fully examined and anthropometric measurements such as weight and height were taken by the investigators. Body mass index (BMI) was calculated from these. Subjects in the study had their blood pressures measured using a mercury sphygmomanometer and a standard sized cuff using the usual methods with the patient sitting quietly. The mean of two readings taken at least 2 minutes apart after the patient had rested in a relaxed sitting position for 5 minutes in a quiet room was recorded as the blood pressure.
Hypertension was defined as systolic blood pressure (SBP) 140 mmHg at least and/or diastolic blood pressure (DBP) 90 mmHg at least, using the Joint National Committee 7 (JNC 7) guideline or history of hypertension with the use of antihypertensive medications.
Samples for urine and blood were obtained from the participants at first contact with the investigators during the clinic visits of the HIV patients.
Urinalysis with multistix (combi – 9) were carried out on all participants for the presence of overt proteinuria. Serum creatinine value was measured using alkaline picrate method while the creatinine clearance was calculated using the cockcroft and Gault formula for predicting glomerular filtration rate (GFR) as follows:
This formula is readily preferred due to its simplicity and good predictive ability of GFR in HIV – positive patients.23
The subjects were classified using the GFR according to the National Kidney Foundation using the Kidney Disease Outcomes Quality Initiative (K/DOQI) guidelines as follows:24
Stage 1 (Normal or increased eGFR) ≥90 mL/min/1.73 m2
Stage 2 (Mildly decreased eGFR) =60–89 mL/min/1.73 m2
Stage 3 (Moderately decreased eGFR) =30–59 mL/min/1.73 m2
Stage 4 (Severely decreased eGFR) =15–29 mL/min/1.73 m2
Stage 5 (Kidney failure) <15 mL/min/1.73 m2
Chronic kidney disease was therefore defined based on either of the two criteria. First, on the eGFR of <60 mL/min24 and secondly on elevated plasma creatinine levels using values for the classification of chronic progressive renal disease:25
Reduced renal reserve (88.4–221 mmol/L)
Renal insufficiency (221–530.4 mmol/L)
Renal failure (486.2–972.4 mmol/L)
ESRD (>707.2 mmol/L)
Inclusion criteria
- Patients confirmed to have been diagnosed with HIV and on HAART at UCTH.
- HIV patients aged 18 years and above.
- HIV patients that consent to the study.
Exclusion criteria
- HIV patients with comorbid conditions such as diabetes and liver cirrhosis.
- HIV patients below 18 years of age.
- HIV patients that do not give consent.
Data analysis
The data obtained were inputted and analyzed using Statistical Package for Social Sciences (SPSS) version 18. Continuous variables and categorical variables were expressed as means ± SD and percentages respectively. Comparison of means was done using Independent sample Student t-test and ANOVA; and Bivariate Correlation and Binary Logistic regression were used to determine the predictors of CKD. Other statistical tests were used as appropriate. p<0.05 was accepted to be significant.
Ethical consideration
Ethical approval was duly applied for and subsequently obtained from the Health Research Ethical Committee (HREC) of the University of Calabar Teaching Hospital, Calabar.
Results
Table 1 shows more female participants (69.5%) with about 58.3% of the patients below the age of 41 years and 15.3% of the participants having eGFR below 60 mls/min. The majority of the participants were married (54.2%), had secondary education (40.7%), were mainly business persons (62.7%) and resided in the urban region (73.7%). About half of the participants were on tenofovir-based combination ARV.
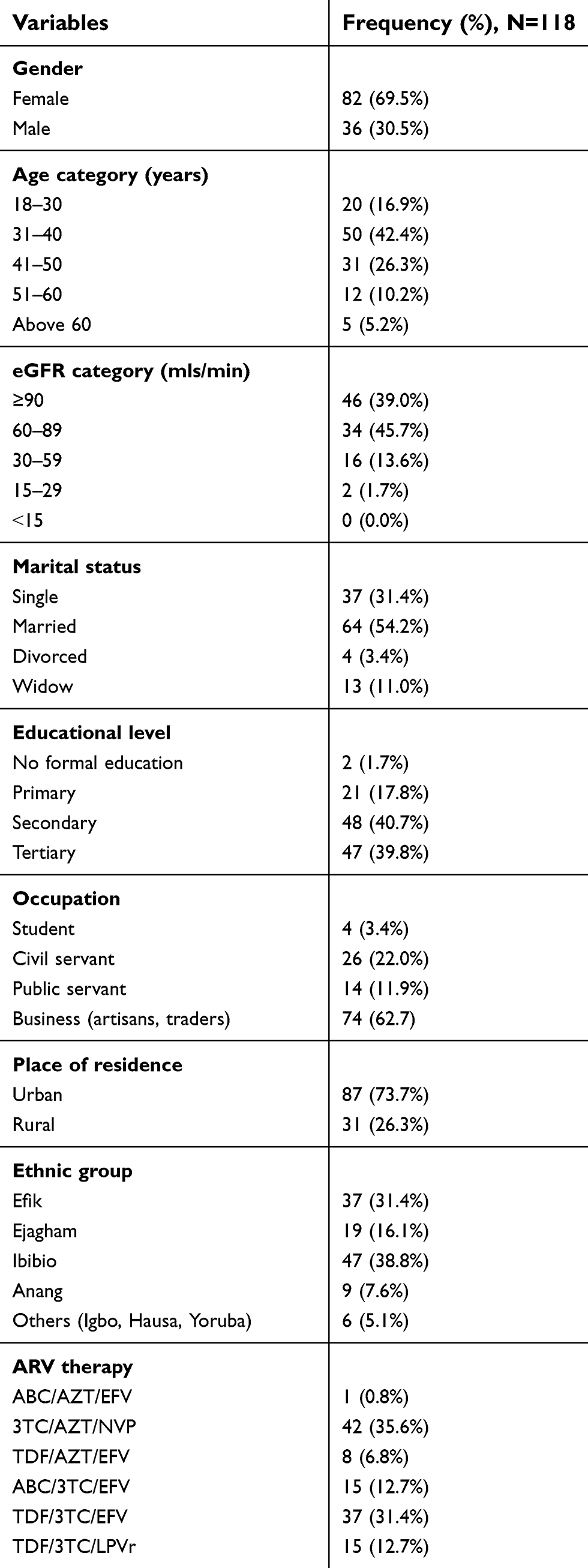 | Table 1 Clinical and demographic characteristics of participants |
Table 2 showed that participants with a CD4 count ≤200 and those on TDF/3TC/EFV ARV therapy are more likely to develop CKD with significant values of 0.006 and 0.038 respectively.
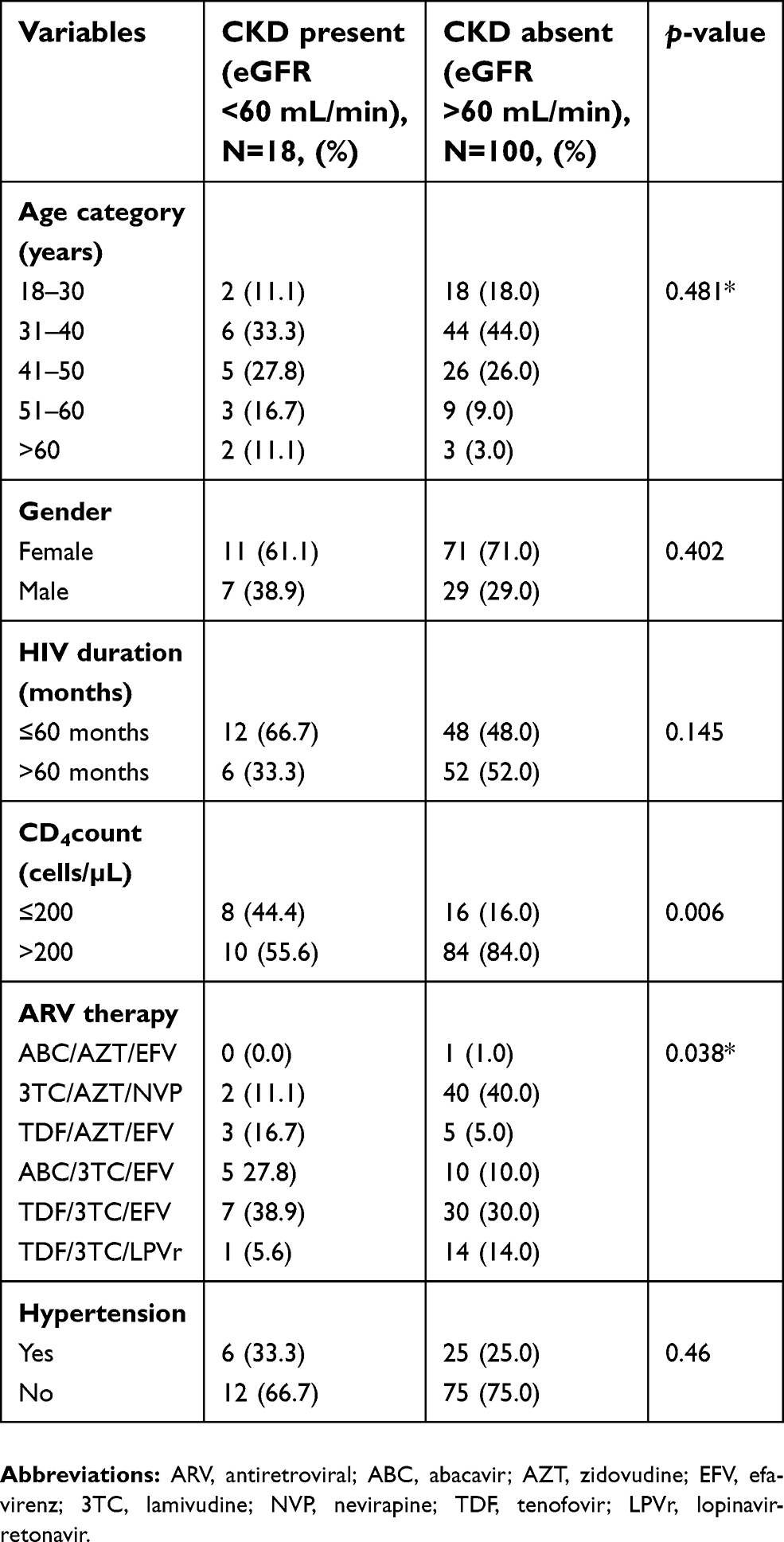 | Table 2 Cross tabulation of clinical and biochemical parameters |
In Table 3, the mean WHR and creatinine levels are significantly higher in subjects with CKD (p<0.05) while the mean weight, BMI, eGFR and CD4 count levels are significantly lower in subjects with CKD (p<0.05).
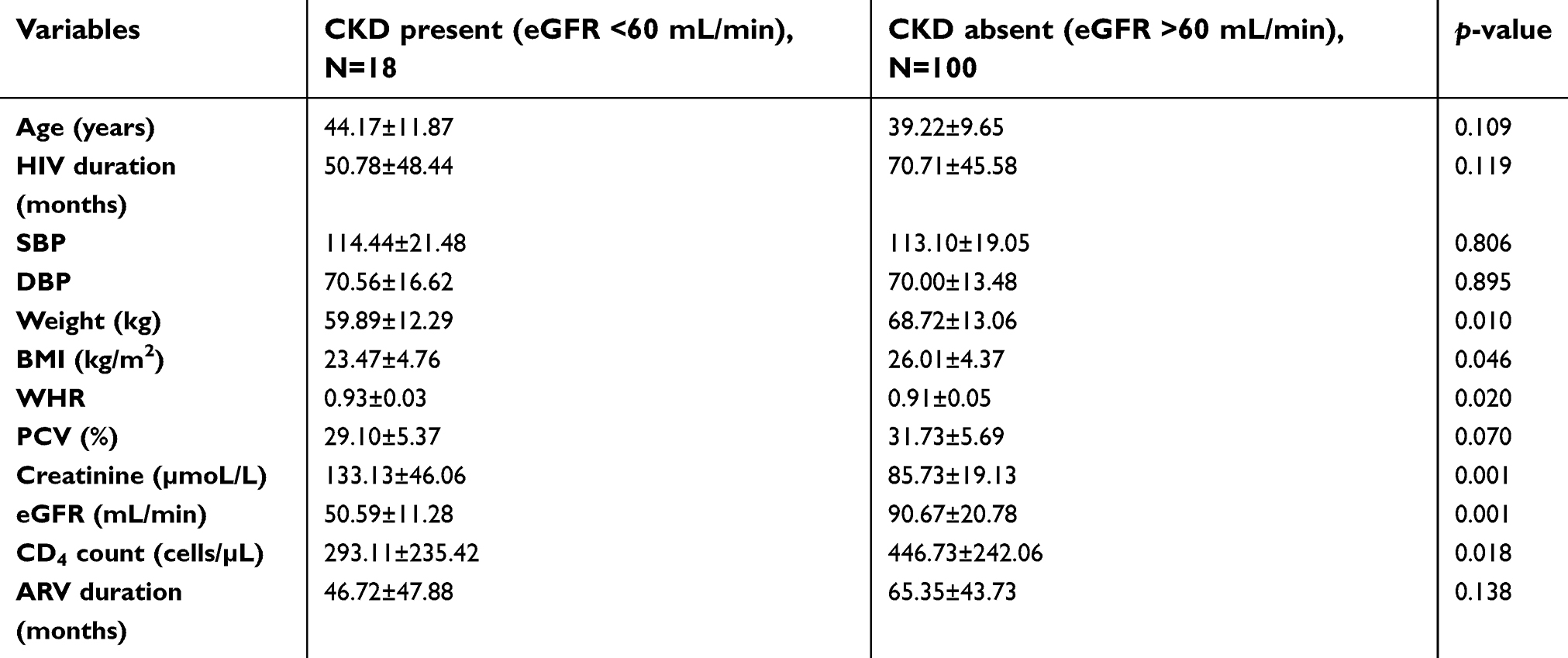 | Table 3 Relationship between CKD and some selected variables |
Table 4 shows that the weight, BMI, PCV and CD4 count levels are directly correlated with eGFR, while creatinine levels are inversely correlated.
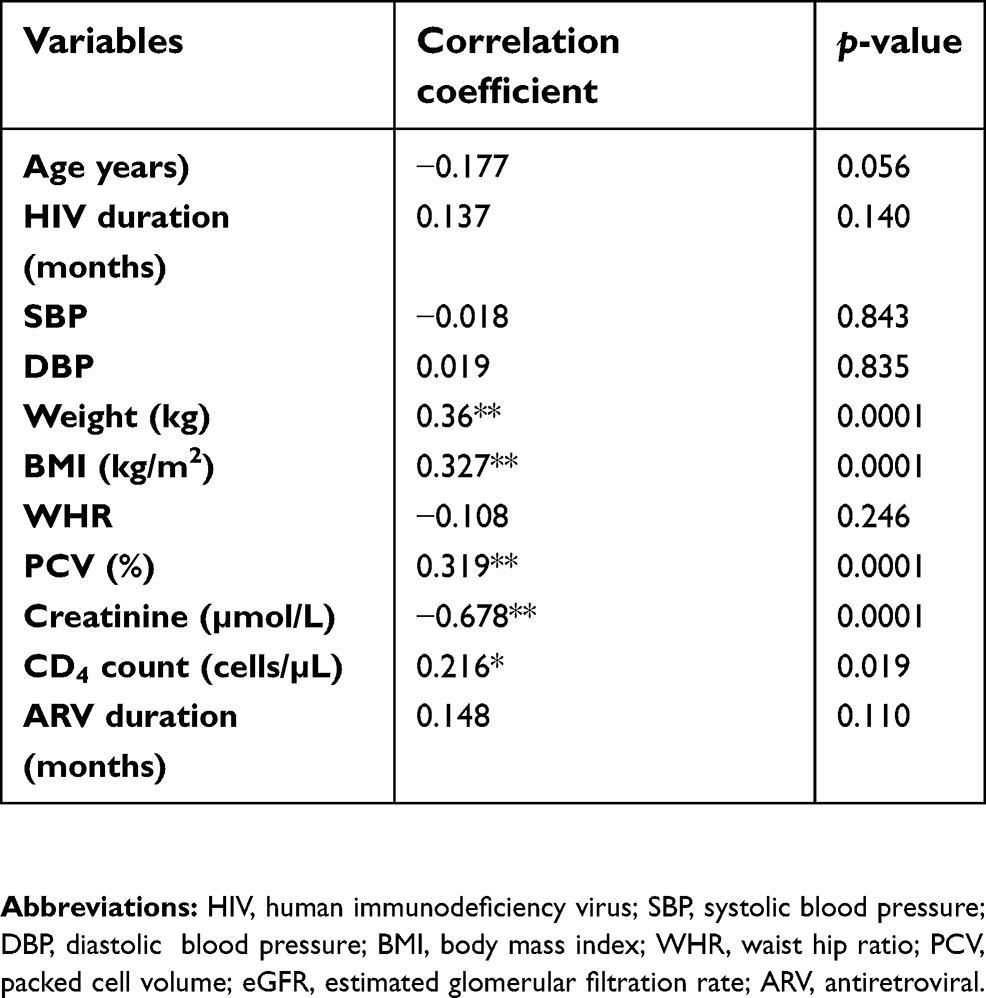 | Table 4 Correlation of eGFR and some selected variables |
In the logistic regression model in Table 5, when the risk factors that were significantly correlated in Table 4 were put into the model, creatinine levels were the main predictor of CKD.
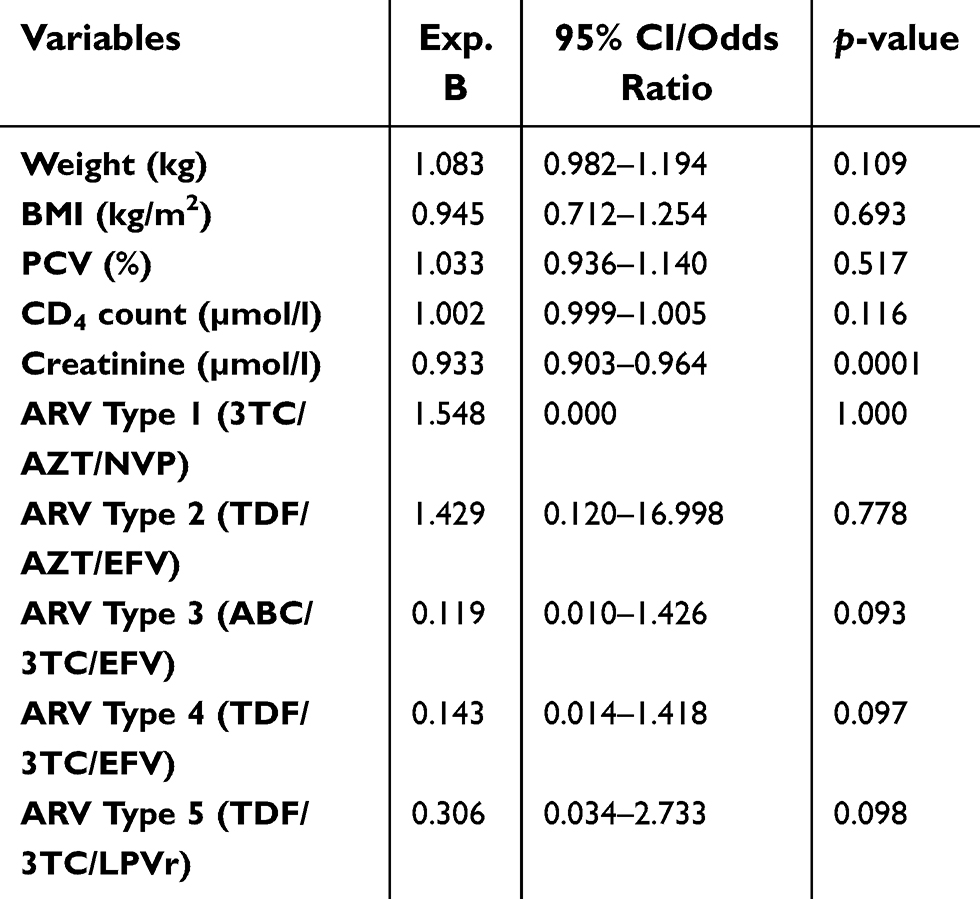 | Table 5 Logistic regression analysis of risk factors for CKD |
Discussion
Our study showed that 15.3% of the HIV subjects had CKD, and the risk factors associated with the development of CKD were lower levels of CD4 count below 200 cells/µL, lower PCV, weight, BMI and eGFR. Also, higher levels of WHR and creatinine were associated with CKD. Factors directly correlated with CKD were weight; BMI and CD4 count levels, while the creatinine levels were inversely correlated. However, a logistic regression model showed only creatinine to be a predictor of CKD.
The prevalence of 15.3% in our study is lower than that obtained from some Nigerian studies with a range of 22–51%,6–9 but has similarity with the studies in USA with a range of 2–15.5%.26–28 The difference noted in the prevalence of CKD in our study and the former reports may be adduced to the differences in sample size and HAART combination, as our study had protease inhibitor-based combination while the former reports were mainly nucleoside and nucleotide reverse transcriptase inhibitors combination.
This study showed that lower CD4 count is a risk factor for CKD, and lower CD4 count has also been shown to be associated with advanced HIV disease.2 This finding in our study is in contrast with another study8 but in keeping with other studies where lower CD4 count was a predictor of CKD.6,29
Also, studies have shown low BMI and hemoglobin to be predictors of CKD,8,30 but our study showed these parameters to be associated with CKD as risk factors as they were not significant in the logistic regression model.
In this study, tenofovir-based combination ARV therapy was associated with CKD in HIV patients; TDF/3TC/EFV combination was also a major implication.
Research has shown that tenofovir has been demonstrated to contribute to severe renal impairment in HIV-infected patients.22 There appears to be a consistent slight drop (up to 10%) in eGFR with the use of TDF, across some studies,31–33 and appears to be more marked during the first years of exposure. However a study suggested that this decrease was largely irreversible,30 but the difference was of doubtful clinical significance. Studies have been conducted on patients who have initiated TDF in the presence of renal dysfunction and have shown that while the majority of patients did not deteriorate during study follow-up, those with pre-existing stage 2 (eGFR between 60 mL/min/1.73 m2 and 89 mL/min/1.73 m2) and stage 3 (30–59 mL/min/1.73 m2) renal disease were associated with progression to renal failure on TDF,34,35 although one study actually demonstrated improvement on TDF in patients with severe (<30 mL/min/1.73 m2) renal failure
High levels of serum creatinine were found to be predictive of CKD in HIV patients in our study which is in keeping with earlier studies.6,8 Surprisingly, creatinine-based estimated GFR which is a more reliable tool in assessing renal function was associated with CKD but not predictive.36
Our study did not demonstrate any association between gender and CKD in HIV patients, in contrast with a study that found female sex to be associated with CKD and another study which is in keeping with our findings.8,37
According to a report by Agbaji et al,37 older age was associated with and a predictor of CKD in HIV patients. However, our study did not show such relationship, despite almost the same mean age of the subjects in their study and ours.
This study did not report any association between SBP, DBP, and CKD. This is in agreement with an earlier mentioned study.8 In contrast, some other studies reported SBP and DBP to be predictors of CKD.6,38 The difference with the later reports may be due to difference in study design.
Conclusion
In conclusion therefore, the prevalence of CKD reported among HIV subjects in this study was 15.3% and the risk factors associated with CKD in HIV subjects on HAART were lower levels of CD4 count below 200 cells/µL, lower PCV, weight, BMI, and eGFR. Also, higher creatinine was associated and predictive of CKD in HIV subjects.
Limitations of the study
It was a cross-sectional study carried out in one center which may not give a true prevalence of CKD in HIV patients in the South-South region of Nigeria, a multicenter study wwould be very helpful.
Also, other investigations that would have contributed to the risk factors and predictors of CKD were not measured; these include renal biopsy, HIV viral load, Hepatitis B and C, and lipid profile.
Acknowledgment
The authors acknowledge the University of Calabar Teaching Hospital HIV special clinic staff for their unreserved support during the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. UNAIDS Report on the Global AIDS Epidemic 2013. UNAIDS; 2013. Available from:
2. Szczech LA, Hoover DR, Feldman JG, et al. Association between renal disease and outcomes among HIV-infected women receiving or not receiving antiretroviral therapy. Clin Infect Dis. 2004;39(8):1199–1206. doi:10.1086/424013
3. Schwartz EJ, Szczech LA, Ross MJ, Klotman ME, Winston JA, Klotman PE. Highly active antiretroviral therapy and the epidemic of HIV+ end-stage renal disease. J Am Soc Nephrol. 2005;16:2412–2420. doi:10.1681/ASN.2005040340
4. Eggers PW, Kimmel PL. Is there an epidemic of HIV infection in the US ESRD program? J Am Soc Nephrol. 2004;15:2477–2485. doi:10.1097/01.ASN.0000138546.53152.A7
5. Gupta SK, Eustace JA, Winston JA, et al. Guidelines for the management of chronic kidney disease in HIV infected patients: recommendations of the HIV Medicine Association of the Infectious Disease Society of America. Clin Infect Dis. 2005;40:1559–1585. doi:10.1086/430257
6. Emem-Chioma P, Arogundade FA, Sanusi AA, Wokoma FS, Akinsola A. Renal disease in HIV-seropositive patients in Nigeria: an assessment of prevalence, clinical features and risk factors. Nephrol Dial Transplant. 2008;23:741–746. doi:10.1093/ndt/gfm836
7. Agaba EI, Agaba PA, Sirisena ND, Anteyi EA, Idoko JA. Renal disease in the acquired immunodeficiency syndrome in North Central Nigeria. Niger J Med. 2003;12:120–125.
8. Anyabolu EN, Chukwuonye II, Arodiwe E, Ijoma CK, Ulasi I. Prevalence and predictors of chronic kidney disease in newly diagnosed human immunodeficiency virus patients in Owerri, Nigeria. Ind J Nephrol. 2016;26(1):10–15. doi:10.4103/0971-4065.156115
9. Umeizudike T, Mabayoje M, Okany C, Abdulkareem F, Adeyomoye A, Okubadejo N. Okpechi prevalence of chronic kidney disease in HIV positive patients in Lagos, South-west Nigeria. Nephrol Rev. 2012;4:22–26. doi:10.4081/nr.2012.e5
10. Lucas GM, Lau B, Atta MG, Fine DM, Keruly J, Moore RD. Chronic kidney disease incidence, and progression to end-stage renal disease, in HIV-infected individuals: a tale of two races. J Infect Dis. 2008;197(11):1548–1557. doi:10.1086/587994
11. Szczech LA, Gupta SK, Habash R, et al. The clinical epidemiology and course of the spectrum of renal diseases associated with HIV infection. Kidney Int. 2004;66:1145–1152. doi:10.1111/j.1523-1755.2004.00865.x
12. Gerntholtz TE, Goetsch SJ, Katz I. HIV-related nephropathy: a South African perspective. Kidney Int. 2006;69:1885–1891. doi:10.1038/sj.ki.5000351
13. Estrella M, Fine DM, Gallant JE, et al. HIV type 1 RNA level as a clinical indicator of renal pathology in HIV-infected patients. Clin Infect Dis. 2006;43:377–3380. doi:10.1086/505497
14. Shahinian V, Rajaraman S, Borucki M, Grady J, Hollander WM, Ahuja TS. Prevalence of HIV-associated nephropathy in autopsies of HIV-infected patients. Am J Kidney Dis. 2000;35:884–888. doi:10.1016/S0272-6386(00)70259-9
15. D’Agati V, Suh JI, Carbone L, Cheng JT, Appel G. Pathology of HIV-associated nephropathy: a detailed morphologic and comparative study. Kidney Int. 1989;35:1358–1370. doi:10.1038/ki.1989.135
16. Rao TK, Friedman EA, Nicastri AD. The types of renal disease in the acquired immunodeficiency syndrome. N Engl J Med. 1987;316:1062–1068. doi:10.1056/NEJM198704233161705
17. Laradi A, Mallet A, Beaufils H, Allouache M, Martinez F. HIV-associated nephropathy: outcome and prognosis factors. Groupe d’ Etudes Nephrologiques d’Ile de France. J Am Soc Nephrol. 1998;9:2327–2335.
18.
19. Ahuja TS, Grady J, Khan S. Changing trends in the survival of dialysis patients with human immunodeficiency virus in the United States. J Am Soc Nephrol. 2002;13:1889–1893.
20. Lucas GM, Eustace JA, Sozio S, Mentari EK, Appiah KA, Moore RD. Highly active antiretroviral therapy and the incidence of HIV-1-associated nephropathy: a 12-year cohort study. Aids. 2004;18:541–546.
21. Winston J, Deray G, Hawkins T, Szczech L, Wyatt C, Young B. Kidney disease in patients with HIV infection and AIDS. Clin Infect Dis. 2008;47:1449–1457. doi:10.1086/593099
22. Röling J, Schmid H, Fischereder M, Draenert R, Goebel F. HIV-associated renal diseases and highly active antiretroviral therapy-induced nephropathy. Clin Infect Dis. 2006;42:1488–1495. doi:10.1086/503566
23. Ravasi G, Lauriola M, Tinelic C, Brandolini M, Uglietti A, Maserati R. Comparism of glomerulae filtration rate estimate vs. 24-h creatinine clearance in HIV-positive patients. HIV Med. 2009;10(4):219–228. doi:10.1111/j.1468-1293.2008.00673.x
24.
25. Adedeji TA, Adedeji ON, Adebisi SA, Idowu AA, Fawale MB, Jimoh KA. Prevalence and pattern of chronic kidney disease in antiretroviral-naive patients with HIV/AIDS. J Int Assoc Provid AIDS Care. 2015;14(5):434–440. doi:10.1177/2325957415587570
26. Mocroft A, Kirk O, Gatell J, et al. Chronic renal failure among HIV-1-infected patients. Aids. 2007;21:1119–1127. doi:10.1097/QAD.0b013e3280f774ee
27. Crum-Cianflone N, Ganesan A, Teneza-Mora N, et al. Prevalence and factors associated with renal dysfunction among HIV-infected patients. AIDS Patient Care STDS. 2010;24:353–360. doi:10.1089/apc.2009.0326
28. Overton ET, Nurutdinova D, Freeman J, Seyfried W, Mondy KE. Factors associated with renal dysfunction within an urban HIV-infected cohort in the era of highly active antiretroviral therapy. HIV Med. 2009;10:343–350. doi:10.1111/j.1468-1293.2009.00693.x
29. Szczech LA, Gange SJ, van der Horst C, et al. Predictors of proteinuria and renal failure among women with HIV infection. Kidney Int. 2002;61:195–202. doi:10.1046/j.1523-1755.2002.00094.x
30. Reid A, Stöhr W, Walker AS, et al. Severe renal dysfunction and risk factors associated with renal impairment in HIV-infected adults in Africa initiating antiretroviral therapy. Clin Infect Dis. 2008;46:1271–1281. doi:10.1086/533468
31. Fux CA, Simcock M, Wolbers M, et al. Tenofovir use is associated with a reduction in calculated glomerular filtration rates in the Swiss HIV Cohort Study. Antivir Ther. 2007;12(8):1165–1173.
32. Horberg M, Tang B, Towner W, et al. Impact of tenofovir on renal function in HIV-infected, antiretroviral-naive patients. J Acquir Immune Defic Syndr. 2010;53(1):62–69. doi:10.1097/QAI.0b013e3181be6be2
33. Laprise C, Baril J-G, Dufresne S, Trottier H. Association between tenofovir exposure and reduced kidney function in a cohort of HIV-positive patients: results from 10 years of follow-up. Clin Infect Dis. 2013;56(4):567–575. doi:10.1093/cid/cis937
34. Brennan A, Evans D, Maskew M, et al. Relationship between renal dysfunction, nephrotoxicity and death among HIV adults on tenofovir. Aids. 2011;25(13):1603–1609. doi:10.1097/QAD.0b013e328343443b
35. Mulenga L, Musonda P, Mwango A, et al. Effect of baseline renal function on tenofovir-containing antiretroviral therapy outcomes in Zambia. Clin Infect Dis. 2014;58(10):1473–1480. doi:10.1093/cid/ciu117
36. Shemesh O, Golbetz H, Kriss JP, Myers BD. Limitations of creatinine as a filtration marker in glomerulopathic patients. Kidney Int. 1985;28:830–838. doi:10.1038/ki.1985.205
37. Agbaji OO, Onu A, Agaba PE, Muazu MA, Falang KD, Idoko JA. Predictors of impaired renal function among HIV infected patients commencing highly active antiretroviral therapy in Jos, Nigeria. Niger Med J. 2011;52:182–185.
38. Cheung CY, Wong KM, Lee MP, et al. Prevalence of chronic kidney disease in Chinese HIV-infected patients. Nephrol Dial Transplant. 2007;22:3186–3190. doi:10.1093/ndt/gfm350
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.