")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Predictors for the Longevity of People with Diabetes in Buno Bedele and Illubabor Zones, South-west Ethiopia
Authors Tadege M , Misganaw A, Truneh Z, Tegegne AS
Received 21 January 2023
Accepted for publication 15 May 2023
Published 18 May 2023 Volume 2023:16 Pages 1449—1457
DOI https://doi.org/10.2147/DMSO.S403556
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Konstantinos Tziomalos
Melaku Tadege,1 Azmeraw Misganaw,2 Zemenay Truneh,1 Awoke Seyoum Tegegne3
1Department of Statistics, Injibara University, Injibara, Amhara, Ethiopia; 2Department of Statistics, Mettu University, Mettu, Oromia, Ethiopia; 3Department of Bio-Statistics, Bahir Dar University, Bahir Dar, Ethiopia
Correspondence: Awoke Seyoum Tegegne, Email [email protected]
Introduction: Currently, diabetes is a global health problem and it affects many people, especially in the developing continents. As patients’ living conditions improve and the science of medicine advances, the longevity of such patients has increased greatly. Therefore, the purpose of this study was to identify predictors for the association of the longevity of people with diabetes in Buno Bedele and Illubabor Zones, South-west Ethiopia.
Methods: The study applied a retrospective cohort study design approach. In particular, long rank tests for longevity experience and Cox semi-parametric regression were implemented to compare and investigate the predictors associated with the longevity of patients with diabetes.
Results: Among all the patients who participated in this study, 56.9% were females and the rest were males. From the Cox regression result, age (AHR = 1.0550, 95% CI: (1.0250, 1.0860), p-value = 0.001), female patients (AHR = 0.2200, 95% CI: (0.0390, 0.5290)), rural patients (AHR = 0.2200, 95% CI: (0.1000, 0.4890), p-value = 0.001), the existence of fasting blood glucose complication (AHR = 1.2040, 95% CI: (1.0930, 1.4460), p-value = 0.001), the existence of blood pressure (AHR = 1.2480, 95% CI: (1.1390, 1.5999), p-value = 0.0180), treatment type, Sulfonylureas (AHR = 4.9970, 95% CI: (1.4140, 17.6550), p-value = 0.0120), treatment type, Sulfonylurea and Metformin (AHR = 5.7200, 95% CI: (1.7780, 18.3990), p-value = 0.0030) were significantly affected the longevity of people with diabetes.
Conclusion: The findings of the current study showed that the patient’s age, sex of patients, residence area, the existence of complications, existence of pressure, and treatment type were major risk factors related to the longevity of people with diabetes. Hence, health-related education should be given to patients who come to take treatment to have better longevity for people with diabetes. More attention should be given to aged patients, male and urban patients, patients under complication treatment, and patients under treatment with single-treatment medication.
Keywords: DMD, mortality, Log rank, Cox proportional hazards model, longevity
Introduction
Non-communicable diseases (NCDs) are the leading cause of death worldwide and present a huge threat to health and development, particularly in developing continents. The diseases kill about 41 million people and account for 74% of all deaths each year, and about 17 million people die from an NCD before age 70 which leads to 86% of premature deaths occurring in developing continents. The diseases consist of cardiovascular diseases, cancers, chronic respiratory diseases, and diabetes. All these four groups account for over 80% of all premature non-communicable deaths.
Diabetes consists of three major groups, namely, T1DM, T2DM, and gestational diabetes mellitus.1 In T2DM, the pancreas makes less insulin than it used to, and the body becomes resistant to insulin while in T1DM, the body’s system damages the cells that discharge insulin, eventually removing insulin fabrication from the body.2 On the other hand, gestational diabetes is well defined as the amount of glucose intolerance with onset or first gratitude throughout pregnancy.3 T1DM is a hereditary complaint that existed in individuals at a young age life. On the other hand, T2DM is mainly developed over time.4 Hence, an individual with high blood glucose levels can lead to serious health complications, whether an individual has T1DM or T2DM.5 So if an individual has either condition, he/she needs to take the right steps to manage it.
Diabetes is the most serious metabolic disease in the world as many people with diabetes are unaware that they are living with diabetes or not may be for up to a decade before diagnosis.6 Hence, hyperglycemia over a long period of time is strongly associated with the development of diabetic complications.7 Diabetic complications lead to damage of tiny vessels like neuropathy, nephropathy, retinopathy, and enormous blood vessels as in cardiovascular diseases.8
It is well known and established that in diabetes, long-term complications result from abnormal regulation of glucose metabolism, and all manifestations of cardiovascular disease, coronary heart disease, stroke, and peripheral vascular disease are substantially more common in patients with diabetes than in normal people.9 Patients with diabetes have a two-to-four-fold increased risk of fatal and nonfatal coronary events.10
Previous studies indicate that there are various mechanisms for preventing and treating diabetes. Screening of a person with pre-diabetes reveals a chance to detect those individuals who are at high risk for emerging diabetes and at high risk of developing cardiovascular disease (CVD).11 Identifying people with pre-diabetes to condemn the progression at an early stage has several advantages.12 Such interventions may be categorized as primordial, primary, secondary, or tertiary-level strategies, based on the pathophysiological stage at which they are being targeted.13 Primordial interventions are activities of an individual such as reduction of fat or salt intake, increased physical activity, and weight loss and belong to the whole population.14 The primary intervention is a strategy that belongs to the prevention of type 2 diabetes progressions.15 This would include the use of pharmacological agents and lifestyle modification.16 Prevention for the development of diabetic complications belongs to secondary prevention, and tertiary prevention includes the handling of specific diabetic complications, to prevent excess amount of morbidity and mortality.17
Therefore, diabetes is highly prevalent with an increasing incidence globally.18 World Health Organization (WHO) declared that about 90% of the people in the world who suffered from diabetes belong to T2DM.19 It is an epidemic in many low- and middle-income countries with many people in younger age groups.20 The latest International Diabetes Federation (IDF) report declared that the global prevalence of diabetes mellitus was estimated to be 3.3% of adults, with total cases of diabetes in adults as 1,920,000 and this will be increased to 55 million by 2045.21
Some of the African countries with the highest number of people living with diabetes are Nigeria (3.9 million), South Africa (2.6 million), Ethiopia (1.9 million), and Tanzania (1.7 million).22 One of the previous systematic reviews of diabetes conducted in 2011 in sub-Saharan Africa (SSA) indicates that about 12.1 million people are living with diabetes in Africa and if the condition continues in this trend, by 2030, about 23.9 million people will be expected to live with diabetes.23
International Diabetes Federation (IDF) indicates that Ethiopia is one of the 48 countries in African regions where 24 million people are living with diabetes.24 Another study indicates that Ethiopia is one of the top five countries with the highest number of people living with diabetes in sub-Saharan Africa.25 Some hospital-based statistical data evidence showed that the prevalence of the occurrence of diabetes and associated death are increasing,26 and this is why the authors are initiated to investigate the situation to identify the risk factor associated with the longevity of people with diabetes. There is a scarcity of such research or investigations associated with risk factors for the longevity of people with diabetes in the study area. Longevity is the long waiting time of people with diabetes or people with diabetes that cannot be cured in a short time. It is the hazard/risk of people living with diabetes.
Materials and Methods
Study Area
The current study was done in Buno Bedele and Illu Aba Bora zones, Oromia Region, Ethiopia. Buno Bedele and Illu Aba Bora zones are located in the south-west part of Ethiopia.
Data
An institution-based cohort study design was conducted in the current study. The data collection was conducted by health professionals and the investigators strictly followed the data quality at Buno, Bedele, and Illubabor zones. Data were analyzed by using SAS software version 9.2.
Sample Size and Selection Method
The study was conducted in two senior hospitals and five health centers. The two hospitals were Illubabor General Hospital and Buno Bedele Specialized Hospitals, selected based on the service they gave and the number of people served in the health institution. Health centers were selected randomly. The systematic random sample selection technique was applied to select patients, considering their id number as code. The study was conducted in a period from September 2008 to January 2018. All people with diabetes who were under treatment in the study period were considered the target population. The sample size was determined using single population proportions’ sample size calculation, considering a 95% confidence level, 4% degree of precision, and 33% proportion of TB/HIV co-infection.27 A stratified random sampling method was used for selecting a representative sample from each of the two hospitals in the study area. Hence, the sample size was allocated proportionally based on the number of patients followed up at each hospital. Patients were selected randomly using their ART unique identification number. The study considered all people living with diabetes and under treatment fulfilled inclusion criteria, regardless of their treatment category during the study period. Hence, a total of 444 randomly selected patients were considered for the current investigation.
Study Variables
The response variable for this study was longevity/long waiting time for people with diabetes. The predictor variables included in the study were gender (male, female), age of the patients, residence area (rural, urban), marital status, fasting blood sugar, the existence of complications (yes, no), patients with hypertension (yes, no), type of medication (treatment type), and type of diabetes mellitus.
Data Collection Procedures and Their Quality
All the relevant information about the patient’s health-related issue was taken from the patient’s chart in the hospital records, repeated questioning of the patient at different visits, and the relationship of the onset to well-known historical events. During data collection, all participants had completed the physical examination. Laboratory examination results like patients’ blood glucose, weight, and blood pressure were recorded at each visiting time.
The long-term complications of diabetes were also categorized based on WHO Report.28 Blood glucose was usually measured by the glucose oxidase method with Dextrostix and an Eyestone reflectance meter. Urine was examined for protein content by precipitation with 20% Sulfosalicylic acid.29
Methods of Data Analysis
Non-Parametric Methods
The Kaplan–Meier, Nelson-Aalen, and Life Tables were used to estimate the longevity of people living with diabetes and hazard functions.
The Product-Limit estimator with all information about uncensored and censored observations was used for estimates of the survival function.30 The observed data were used to estimate the conditional probability which is used to estimate the overall survival function.
The Log rank test was used for comparing two or more survival curves (longevity of people with diabetes) in the case that the distribution is right-skewed and censored data sets. On the other hand, the Wilcoxon test was used when there is no censoring in the data set. Log rank test was computed at 5% level of significance to compare the survival experience between different categories to all categorical predictors.
Semi-Parametric Models
The Cox-Proportional Hazard Model was used for estimating time-varying, time-independent, continuous, and discrete covariates. Kaplan–Meier estimate and Log rank test were also used for all categorical variables to know if there is a significant difference among the categories of each predictor variable.
Kaplan–Meier Estimation
The well-known study method for the estimator of the survival function, proposed by (Kaplan and Meier, 1995) is the Product-Limit estimator. This estimator technique incorporates information from all observations included in the study, both uncensored (event) and censored estimates. This considers survival at any point in time as a series of steps defined at the observed and censored times. The observed data were used to estimate the conditional probability of established longevity at each observed time for people living with complications and then multiply them to obtain an estimate of the overall survival function.
Log Rank Test
The most frequently used nonparametric test is a Log rank test, sometimes called the Co-Mantel or Mantel test. The Log rank statistic is approximately standard normal; it can be viewed as time-stratified. It is a nonparametric test for comparing two or more survival curves, and it is more powerful than Wilcoxon’s other non-parametric tests. Because the Log rank test considers right skewed and censoring data sets, whereas the Wilcoxon test is used when there is no censoring in the data set.
Semi-Parametric Models
The Cox-Proportional Hazard Model
The usual statistical model used for survival data is the proportional hazards (PH) model, which is known as the Cox regression model. This model has certain assumptions to conduct a given research but with no assumption on particular form of a probability distribution for the survival times. The Cox proportional hazard model is popular because of its flexibility in selecting covariates. The two other issues that make it popular are it does not make any assumption about the underlying survival distribution and does not require estimation of the baseline hazard rate, to estimate the regression parameters. It is a multiple regression method and is used to evaluate the effect of multiple covariates on the hazard.25 It is a semi-parametric model for the hazard function that allows the addition of covariates while keeping the baseline hazards unspecified, and we can take only positive values.25
Results
There were 444 patients in the cohort study, of which 61 (13.7%) were dead. Of the total number of people with diabetes, 206 (46.4%) of them were females and 238 (53.6%) were males. The majority of patients, 194 (47.7%) of them were unmarried. Among all the patients, 296 (66.7%) of them were urban patients, and others were rural patients. Of all the people with diabetes, about 288 (64.9%) of them were type 2, and 156 (35.1%) of them were type 1. About 159 (35.8%) of them were living with fasting glucose complications. Of all the patients, 186 (41.9%) were hypertensive (Refer to Table 1).
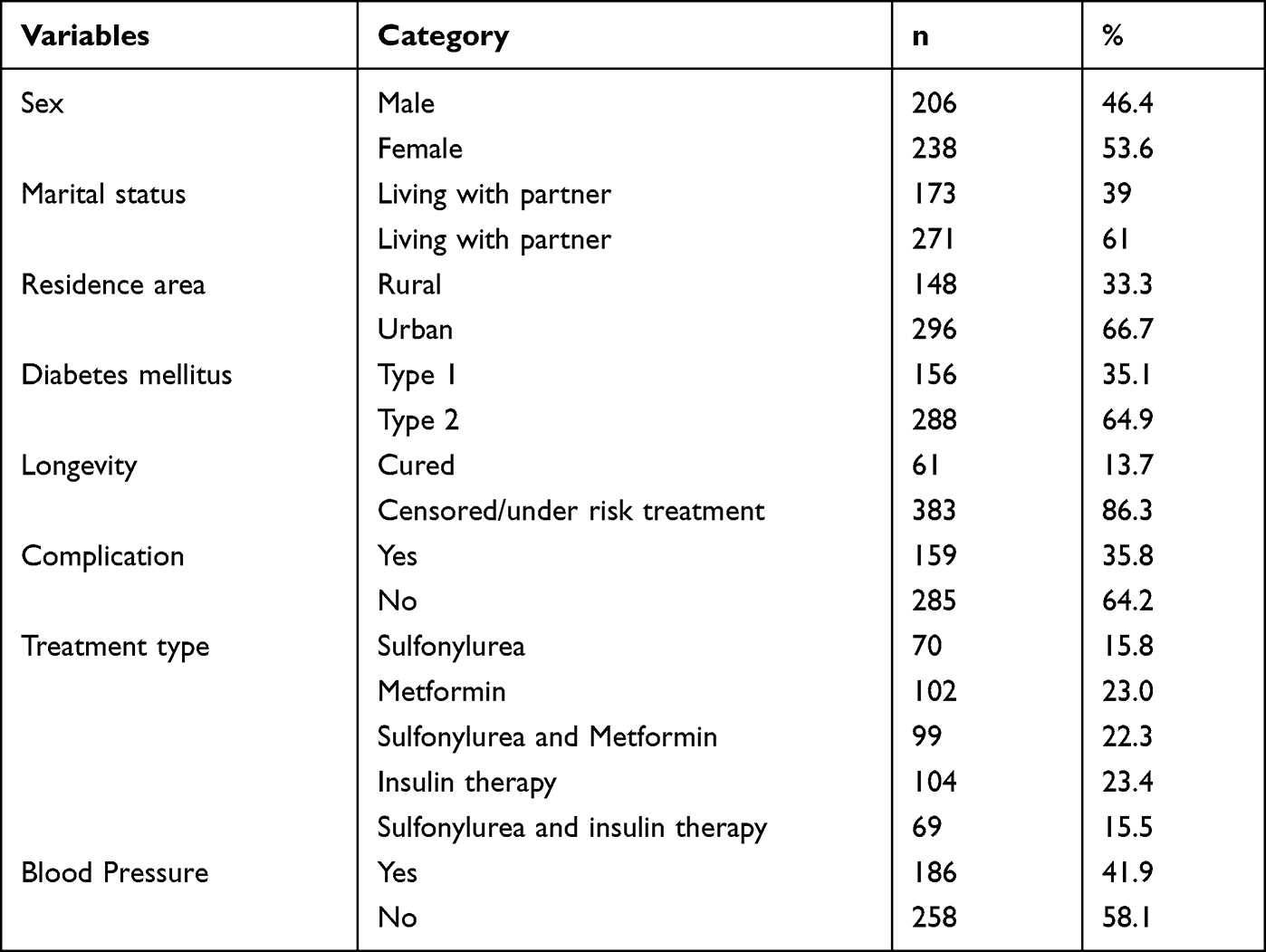 |
Table 1 Descriptive Statistical Analysis |
Longevity of People with Diabetes/Log Rank Survival Estimate
From the Log rank test, the survival practice of patients related to profession and diabetes mellitus type, marital status, residence area, treatment type, and hypertensive status had a significant difference in the longevity of people with diabetes under the complicated risk stage at a 5% statistically significant level (Refer to Table 2). Hence, Table 2 indicates that the expected waiting time (longevity) of married people to be cured of the disease was significantly shorter than that of separated and never married people with diabetes (p-value < 0.01). Similarly, the expected waiting time of people with diabetes tocure from the disease was significantly shorter than urban patients (p-value = 0.010). In the same way, complication status and hypertensive status had significant differences with their counterparts.
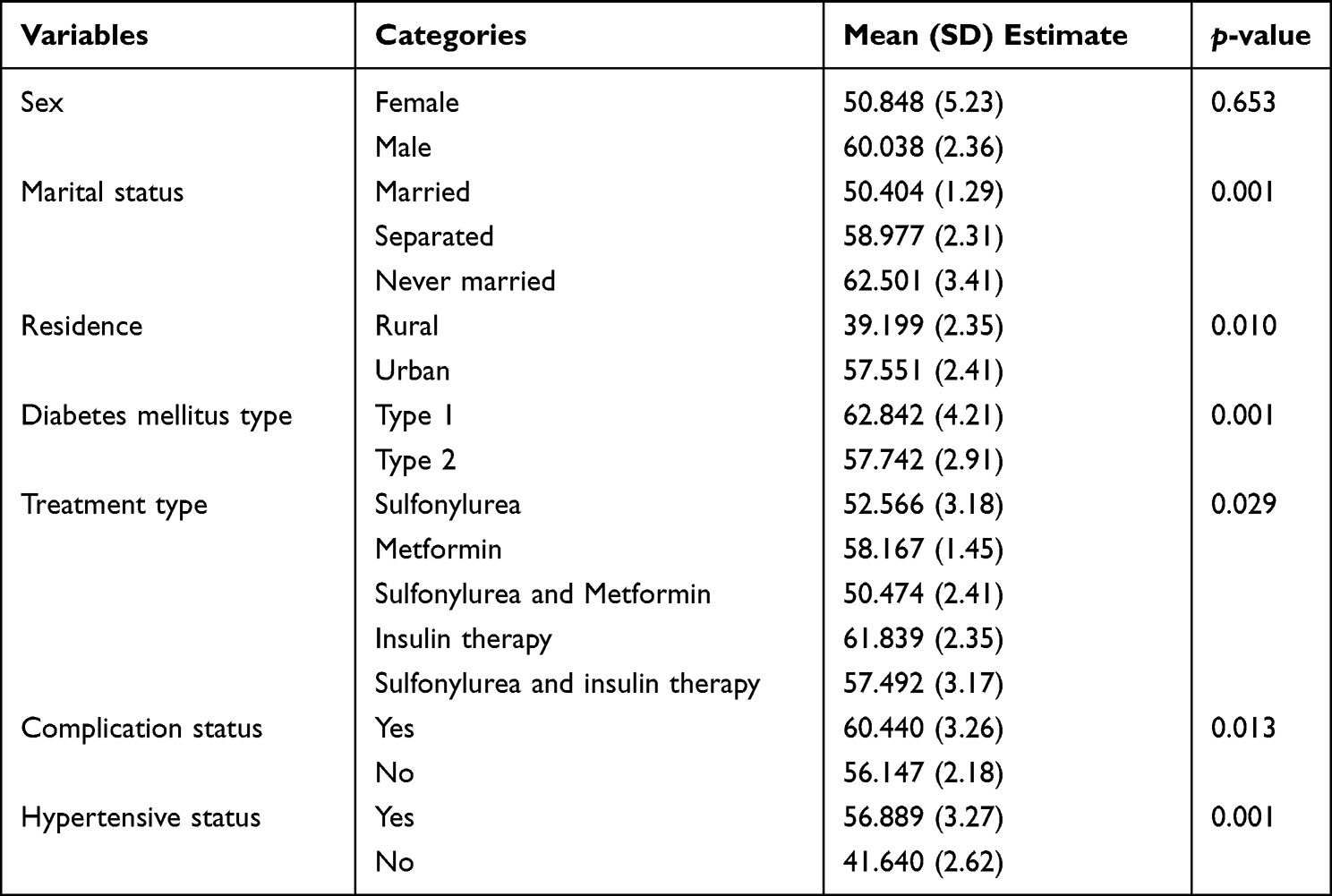 |
Table 2 The Long Rank Test Result |
Cox Proportional Hazard Model Results
The Cox proportional hazard model in Table 3 indicates that as age increased by one year, the expected hazard/risk of the longevity of people living with diabetes was increased by 5.5% (AHR = 1.055, CI (1.025, 1.086), p-value ≤ 0.001), given that the other covariates are constant.
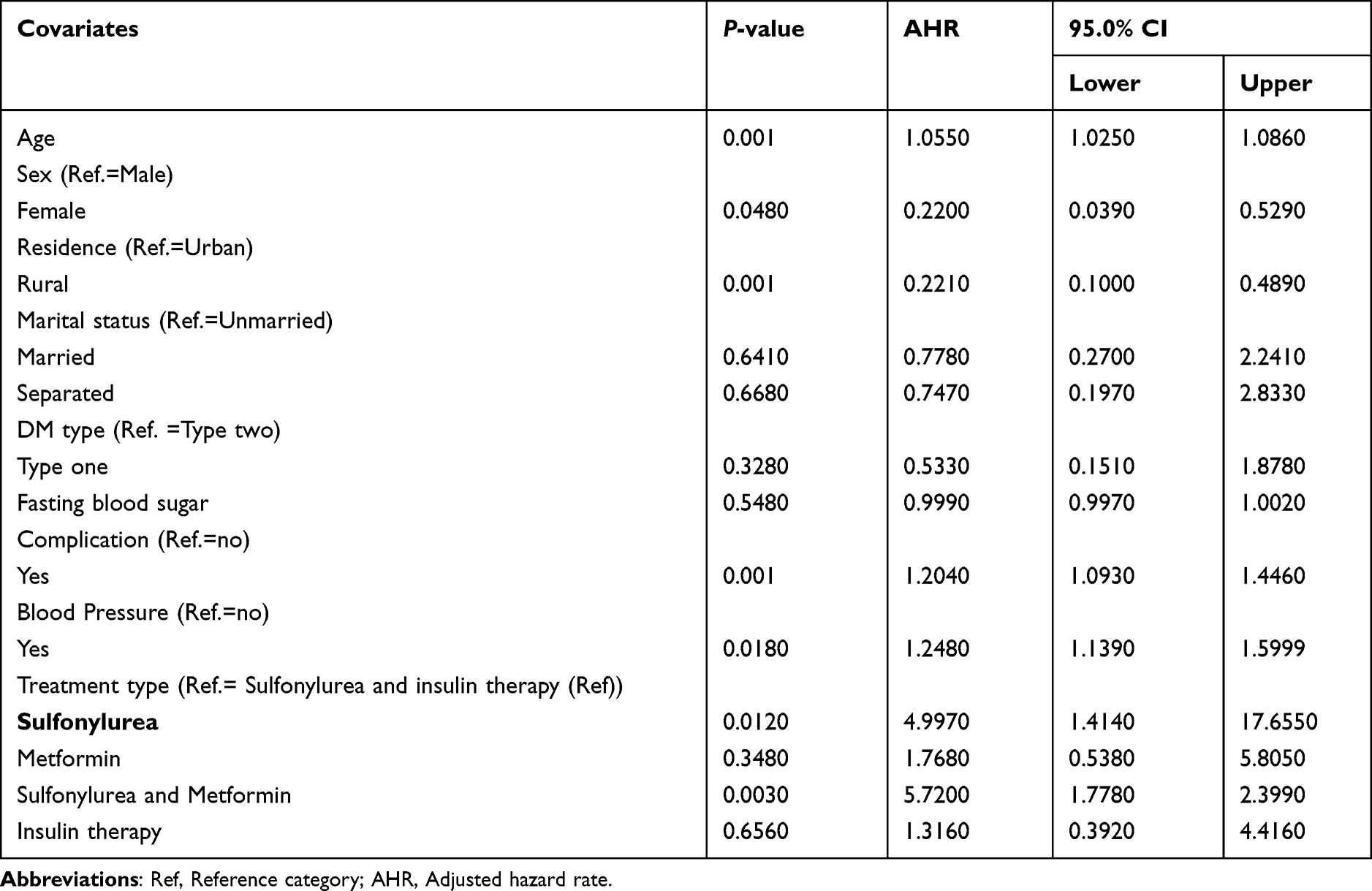 |
Table 3 Multivariable Analysis of Cox Proportional Hazard Model |
Comparing rural patients with urban, the expected hazard of the longevity of people living with diabetes for rural patients was decreased by 78.1% as compared to urban patients (AHR = 0.2210, 95% CI: (0.1000, 0.4890), p-value < 0.01), given the other conditions constant.
The sex of patients was one of the other significant covariates affecting the longevity of people living with diabetes. Hence, comparing female patients with males, the expected risk of the longevity of female people living with diabetes was decreased by 88% as compared to male patients (AHR = 0.2200, 95% CI: (0.0390, 0.5290), p-value= 0.0480), keep the other conditions constant.
Fasting blood glucose complications also significantly affected the risk of longevity of people living with diabetes. Comparing those people with diabetes who had also fasting blood glucose complications with people free from fasting blood glucose complications, the expected risk of longevity of people living with diabetes for those who had also fasting blood glucose complications was increased by 20.4% as compared to those without blood glucose complication (AHR = 1.2040, 95% CI: (1.0930, 1.4460), p-value < 0.01), considering the other covariates constant.
Blood pressure also significantly affected the dependent variable. Hence, the expected risk of the longevity of people with diabetes who had also blood pressure was increased by 24.8% as compared to people with diabetes but with no blood pressure (AHR = 1.2480, 95% CI: (1.1390, 1.5990), p-value = 0.0180), given the other things constant.
Treatment type also affected the study variables. Comparing those people with diabetes with treatment type Sulfonylurea and insulin therapy, the expected risk of people living a long time whose treatment type Sulfonylurea was 4.997 times that of people living with diabetes whose treatment type Sulfonylurea and insulin therapy (AHR = 4.9970, 95% CI: (1.4140, 17.6550), p-value= 0.0120), given the other conditions constant (Refer to Table 3).
Discussions
The significant variables that affected the study variable are discussed as follows. The age of people with diabetes significantly affects the long life of people under the risk conditions. Hence, as age increased, the complication of the risk of treatment for diabetes also increased and this further leads to taking a long time to be cured of the disease. The potential reason for this might be the fact that aged people have a small number of white blood cells, used to fight diseases, and such people may be exposed to additional diseases. This result was consistent with another previously conducted study.27
The sex of people with diabetes also plays a significant role in the variation of the risk of longevity of such patients. One of the mechanisms of preventing and treating diabetes is doing physical exercises. Most of the time females are busy at home managing children and cooking food and this leads to a reduction in blood glucose. Hence, females are less likely to be exposed to the risk of living with diabetes under treatment as compared to males. This result was similar to one of the other previously conducted research29 but contradicted another study.30 The potential reason for the contradiction might be the study area, sample size, and study period.
Comparing rural patients with urban, rural people are always engaged in physical exercises for daily livelihood activities and this leads to reduction of fats and blood glucose. Hence, people with diabetes can cure from diabetes in a short time with simple treatment as compared to urban people with diabetes.31
Fasting blood glucose complications also significantly affected the risk of longevity of people living with diabetes. Comparing those people with fasting blood glucose complications with people free from fasting blood glucose complications, the people without fasting blood complications need a short time to be free from the disease, assuming that the other conditions remain constant. This result is supported by one of the studies conducted previously.31
Blood pressure also affects the dependent variable. The duration of time for curing diabetes for people who have blood pressure is short as compared to people with blood pressure in addition to diabetes. The possible reason for this might be the interaction effect of the two treatments given for diabetes and blood pressure. This result is supported by other studies.32
Treatment type also affects the study variables. Comparing those people with diabetes with treatment type Sulfonylurea and insulin therapy, people with diabetes whose treatment type Sulfonylurea need a long time period to be free from as compared to those people with diabetes with treatment type Sulfonylurea and insulin therapy. This result is contradicted by another study conducted previously,33 and this needs further investigation for the result to be coherent and consistent.
Limitations
This study is not without limitations. One of the limitations is that the study was done in only two zones and including that more health institutions may give additional information about the predictor variables. Since the data were secondary, some important variables such as doing physical exercise or not, job type, and others may also reveal additional information. Authors recommend this for future research including more variables and additional health institutions.
Conclusion
Important significant predictors for the variable of interest were identified for proper intervention to the program. Hence, the age of patients, the sex of patients, the residence area of patients, the existence of complications, and the existence of blood pressure, diabetes type, and treatment type significantly affected the longevity of people with diabetes to wait a long time under risk treatment.
The study recommends that zonal health institutions and the Ministry of Health should give more attention to those people who were in a long time under treatment to be cured of the disease. Health professionals should care for patients of older age, living with complications, and living in urban. The result obtained in the current study would be used as a baseline for future researchers, managers, and policymakers.
Abbreviations
T1DM, Type one diabetes patients; T2DM, Type two diabetes patients; SSA, Sub-Saharan African; AHR, adjusted hazard rate; CI, confidence Interval; NCDs, Non-communicable diseases; DMD, Diabetes mellitus disease.
Data Sharing Statement
The data used in the current study are available under the corresponding author and can be attached on request.
Ethics Approval and Consent to Participate
The study was carried out after receiving an ethical clearance endorsement letter from Mettu University Research Technical and Ethical Review Board and permission was obtained from the health office of the Buno Bedele and Illubabor zone. This study used secondary data from medical case records and patients were not contacted by investigators, and consent to participate was not taken from respondents. During data analysis, the authors used only the id number of each patient to be confidential.
Consent for Publication
This manuscript was not published or is not under consideration for publication by other journals.
Acknowledgments
The authors need to forward their acknowledgement for all the health staffs at the two hospitals. Data collectors shall also owe our heartfelt thanks for their cooperation for the success of this research work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no agent/institution that funded this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nagaraj P, P D, Mansour RF, et al. Artificial flora algorithm-based feature selection with gradient boosted tree model for diabetes classification. Diabetes Metab Syndr Obes. 2021;14:2789. doi:10.2147/DMSO.S312787
2. Mukhtar Y, Galalain A, Yunusa U. A modern overview on diabetes mellitus: a chronic endocrine disorder. Eur J Biol. 2020;5(2):1–14. doi:10.47672/ejb.409
3. Radzicka S, Pietryga M, Iciek R, Brązert J. et al. The role of visfatin in pathogenesis of gestational diabetes (GDM). Ginekol Pol. 2018;89(9):518–521. doi:10.5603/GP.a2018.0088
4. Chowdhury NH, Reaz MBI, Ali SHM, et al. Nomogram-based chronic kidney disease prediction model for type 1 diabetes mellitus patients using routine pathological data. J Pers Med. 2022;12(9):1507. doi:10.3390/jpm12091507
5. Chaudhury A, Duvoor C, Reddy Dendi VS, et al. Clinical review of antidiabetic drugs: implications for type 2 diabetes mellitus management. Front Endocrinol. 2017;8:6. doi:10.3389/fendo.2017.00006
6. Glovaci D, Fan W, Wong ND. Epidemiology of diabetes mellitus and cardiovascular disease. Curr Cardiol Rep. 2019;21:1–8.
7. Chawla A, Chawla R, Jaggi S. Microvascular and macrovascular complications in diabetes mellitus: distinct or continuum? Indian J Endocrinol Metab. 2016;20(4):546. doi:10.4103/2230-8210.183480
8. Ighodaro O, Adeosun A. Vascular complications in diabetes mellitus. kidney. 2018;4:16–19.
9. Reutrakul S, Van Cauter E. Interactions between sleep, circadian function, and glucose metabolism: implications for risk and severity of diabetes. Ann N Y Acad Sci. 2014;1311(1):151–173. doi:10.1111/nyas.12355
10. Beulens J, Rutters F, Rydén L, et al. Risk and management of pre-diabetes. Eur J Prev Cardiol. 2019;26(2_suppl):47–54. doi:10.1177/2047487319880041
11. Alam DS, Talukder SH, Chowdhury MAH, et al. Overweight and abdominal obesity as determinants of undiagnosed diabetes and pre-diabetes in Bangladesh. BMC Obes. 2016;3:1–12. doi:10.1186/s40608-016-0099-z
12. Burch P, Blakeman T, Bower P, et al. Understanding the diagnosis of pre-diabetes in patients aged over 85 in English primary care: a qualitative study. BMC Fam Pract. 2019;20:1–10. doi:10.1186/s12875-019-0981-0
13. Mechanick JI, Farkouh ME, Newman JD, et al. Cardiometabolic-based chronic disease, addressing knowledge and clinical practice gaps: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75(5):539–555. doi:10.1016/j.jacc.2019.11.046
14. Claas SA, Arnett DK. The role of healthy lifestyle in the primordial prevention of cardiovascular disease. Curr Cardiol Rep. 2016;18:1–8. doi:10.1007/s11886-016-0728-7
15. Ha J, Sherman A. Type 2 diabetes: one disease, many pathways. Am J Physiol Endocrinol Metab. 2020;319(2):E410–E426. doi:10.1152/ajpendo.00512.2019
16. Alsinani TS, Alanazi MD, Alkahtani MA, et al. Lifestyle modifications for hypertension management. Egypt J Hosp Med. 2018;70(12):2152–2156. doi:10.12816/0045044
17. Pearson-Stuttard J, Buckley J, Cicek M, et al. The changing nature of mortality and morbidity in patients with diabetes. Endocrinol Metab Clin. 2021;50(3):357–368. doi:10.1016/j.ecl.2021.05.001
18. Schwartz JI, Guwatudde D, Nugent R, et al. Looking at non-communicable diseases in Uganda through a local lens: an analysis using locally derived data. Global Health. 2014;10:1–9. doi:10.1186/s12992-014-0077-5
19. Alwin Robert A, Abdulaziz Al Dawish M, Braham R, et al. Type 2 diabetes mellitus in Saudi Arabia: major challenges and possible solutions. Curr Diabetes Rev. 2017;13(1):59–64. doi:10.2174/1573399812666160126142605
20. Kar SK, Oyetunji TP, Prakash AJ, et al. Mental health research in the lower-middle-income countries of Africa and Asia during the COVID-19 pandemic: a scoping review. Neurol Psychiatry Brain Res. 2020;38:54–64. doi:10.1016/j.npbr.2020.10.003
21. Robinson S. Priorities for Health Promotion and Public Health: Explaining the Evidence for Disease Prevention and Health Promotion. Routledge; 2021.
22. Chiwanga FS, Njelekela MA, Diamond MB, et al. Urban and rural prevalence of diabetes and pre-diabetes and risk factors associated with diabetes in Tanzania and Uganda. Glob Health Action. 2016;9(1):31440. doi:10.3402/gha.v9.31440
23. Ali RAB, Hannoun Z, Harraqui K, et al. Profile of diabetes and cardiovascular risk factors in adults Anjouan Island (Comoros). Pan Afr Med J. 2019;2019:33.
24. Molalign Takele G, Weharei MA, Kidanu HT, et al. Diabetes self-care practice and associated factors among type 2 diabetic patients in public hospitals of Tigray regional state, Ethiopia: a multicenter study. PLoS One. 2021;16(4):e0250462. doi:10.1371/journal.pone.0250462
25. Alebel A, Wondemagegn AT, Tesema C, et al. Prevalence of diabetes mellitus among tuberculosis patients in Sub-Saharan Africa: a systematic review and meta-analysis of observational studies. BMC Infect Dis. 2019;19(1):1–10. doi:10.1186/s12879-019-3892-8
26. Khan MAB, Hashim MJ, King JK, et al. Epidemiology of type 2 diabetes–global burden of disease and forecasted trends. J Epidemiol Glob Health. 2020;10(1):107. doi:10.2991/jegh.k.191028.001
27. Gezae KE, Abebe HT, Gebretsadik LG. Incidence and predictors of LTFU among adults with TB/HIV co-infection in two governmental hospitals, Mekelle, Ethiopia, 2009–2016: survival model approach. BMC Infect Dis. 2019;19(1):1–9. doi:10.1186/s12879-019-3756-2
28. Group LAR. Effect of a long-term behavioural weight loss intervention on nephropathy in overweight or obese adults with type 2 diabetes: a secondary analysis of the Look AHEAD randomised clinical trial. Lancet Diabetes Endocrinol. 2014;2(10):801–809.
29. Moodley N, Ngxamngxa U, Turzyniecka MJ, et al. Historical perspectives in clinical pathology: a history of glucose measurement. J Clin Pathol. 2015;68(4):258–264. doi:10.1136/jclinpath-2014-202672
30. Prinja S, Gupta N, Verma R. Censoring in clinical trials: review of survival analysis techniques. Indian J Community Med. 2010;35(2):217. doi:10.4103/0970-0218.66859
31. Aroda VR, Bain SC, Cariou B, et al. Efficacy and safety of once-weekly semaglutide versus once-daily insulin glargine as add-on to metformin (with or without sulfonylureas) in insulin-naive patients with type 2 diabetes (SUSTAIN 4): a randomised, open-label, parallel-group, multicentre, multinational, phase 3a trial. Lancet Diabetes Endocrinol. 2017;5(5):355–366.
32. Derks M, Bastiaannet E, van de Water W, et al. Impact of age on breast cancer mortality and competing causes of death at 10 years follow-up in the adjuvant TEAM trial. Eur J Cancer. 2018;99:1–8. doi:10.1016/j.ejca.2018.04.009
33. Macedo AF, Douglas I, Smeeth L, et al. Statins and the risk of type 2 diabetes mellitus: cohort study using the UK clinical practice research datalink. BMC Cardiovasc Disord. 2014;14:1–12. doi:10.1186/1471-2261-14-85
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.