")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Predictors for Severity of SARS-CoV-2 Infection Among Healthcare Workers
Authors El-Raey F, Alboraie M , Youssef N , Yousef A, Abdelmoaty AA, Hassan E, Hassany SM , Abd-Elsalam S, Elsharkawy R, Farrag K, Elbadry M, Tag-Adeen M , Abdeen N, Elshaarawy O , Haydara T, Ahmed Hassan A, El-Sayed M, Fouad Y, Abdel Baki A , Zaky S
Received 27 August 2021
Accepted for publication 1 October 2021
Published 25 October 2021 Volume 2021:14 Pages 2973—2981
DOI https://doi.org/10.2147/JMDH.S335226
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Fathiya El-Raey,1 Mohamed Alboraie,2 Naglaa Youssef,3,4 Ahmed Yousef,5 Ahmed A Abdelmoaty,6 Essam Hassan,7 Sahar M Hassany,8 Sherief Abd-Elsalam,9 Ramy Elsharkawy,10 Khaled Farrag,11 Mohamed Elbadry,12 Mohammed Tag-Adeen,13 Nermeen Abdeen,14 Omar Elshaarawy,15 Tamer Haydara,16 Adel Ahmed Hassan,17 Marwa El-Sayed,18 Yasser Fouad,19 Amin Abdel Baki,20 Samy Zaky21
1Department of Hepatogastroenterology and Infectious Diseases, Al-Azhar University, Damietta, Egypt; 2Department of Internal Medicine, Al-Azhar University, Cairo, Egypt; 3Medical-surgical Nursing department, Faculty of Nursing, Cairo University, Cairo, Egypt; 4Medical-surgical Nursing department, College of Nursing, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia; 5Department of Public Health and Community Medicine, Damietta Faculty of Medicine, Al-Azhar University, Damietta, Egypt; 6Tropical Medicine Department, Zagazig University, Zagazig, Egypt; 7Department of Tropical Medicine, Fayoum University, Fayoum, Egypt; 8Department of Tropical Medicine and Gastroenterology, Assiut University, Assiut, Egypt; 9Tropical Medicine and Infectious Diseases Department, Tanta University, Tanta, Egypt; 10Department of Tropical Medicine and Gastroenterology, Sohag University, Sohag, Egypt; 11Department of Tropical Medicine and Hygiene, National Medical Institute of Damanhour, Damanhour, Egypt; 12Endemic Medicine Department, Helwan University, Cairo, Egypt; 13Department of Internal Medicine, South Valley University, Qena Faculty of Medicine, Qena, Egypt; 14Department of Tropical Medicine, Alexandria University, Alexandria, Egypt; 15Department of Hepatology, Gastroenterology and Liver Transplantation, National Liver Institute, Menoufia University, Menoufia, Egypt; 16Department of Internal medicine, Gastroenterology & Hepatology Unit, Kafrelsheikh University, Kafr el-Sheikh, Egypt; 17Infectious and Endemic Disease Department, Suez Canal University, Ismailia, Egypt; 18Department of Microbiology and Immunology, Faculty of Medicine, South Valley University, Qena, 83523, Egypt; 19Department of Endemic Medicine, Faculty of Medicine, Minia University, Minia, Egypt; 20Department: Hepatology, Gastroenterology and Infectious Diseases Department, National Hepatology and Tropical Medicine Research Institute (NHTMRI), Cairo, Egypt; 21Department of Hepatogastroenterology and Infectious Diseases, Al-Azhar University, Cairo, Egypt
Correspondence: Marwa El-Sayed
Department of Microbiology and Immunology, Faculty of Medicine, South Valley University, Qena, 83523, Egypt
Tel +20 1003717916
Fax +20 963216128
Email [email protected]
Mohamed Alboraie
Department of internal medicine, faculty of medicine, Al-Azhar University, Nasr City, Cairo, 11884, Egypt
Tel +20 222602687
Fax +20 224020184
Email [email protected]
Background: Healthcare workers (HCWs) are still at higher risk of acquiring severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections than the general population. Identifying risk factors associated with severe SARS-CoV-2 infections is of paramount importance to protect HCWs and the non-infected patients attending different healthcare facilities.
Purpose: To recognize the predictors for severity of SARS-CoV2 infection among HCWs working in either COVID-19 or non-COVID-19 healthcare settings. Also, to assess compliance of HCW to standard precautions of infection control and explore the possible risk factors for SARS-CoV-2 infection among HCWs.
Methods: A cross-sectional study was conducted among HCWs with suspected or confirmed SARS-CoV-2 infection, from different Egyptian governorates. They were asked to fill in a web-based self-reporting questionnaire. The questionnaire assessed the demographic and socio-economic characteristics of participants, compliance of HCWs to standard precautions of infection control and COVID-19 presentation.
Results: Our study enrolled 204 HCWs (52.3% physicians). Infection of SARS-CoV-2 was confirmed in 61.3% by RT- PCR; 35.8% were admitted to hospital, and of these, 3.9% were admitted to the intensive care unit. While 30.4% had mild disease, 48.5% had moderate disease, 17.2% had severe disease and 3.9% had critical disease. Regression analysis for variables predicting COVID-19 severity among study healthcare workers showed that associated chronic diseases and management at home were the main independent variables predicting severity of their SARS-COV-2 infection, while the variables age, sex, residence, occupation or drug history of immunosuppressives had no role in severity prediction.
Conclusion: Associated chronic diseases and management at home were the main independent variables predicting severity of SARS-COV-2 infection among HCWs. So, HCWs with chronic diseases should not work in COVID-19 designated hospitals, and there should be a screening strategy for their infection with SARS-COV-2. HCWs must not be negligent in adhering to strict precautions of infection control. HCWs infected with SARS-COV-2 must be managed in hospital not at home.
Keywords: health care providers, SARS-CoV-2, COVID-19, delivery of health care, infection control introduction
Introduction
By the end of December 2019, new-coronavirus 19 (SARS-CoV-2) was identified as the main cause of a cluster of pneumonia cases in Wuhan.1 It rapidly spread throughout China resulting in an epidemic, followed by rapid global expansion throughout the world. The World Health Organization (WHO) designated the disease caused by SARS-Cov-2 to be named as coronavirus 19 (COVID-19).2 In mid-February 2020, Egypt reported its first COVID-19 case in a contact of an infected case returning from China and it was confirmed by laboratory analysis for the virus.3 Few published data are available about the prevalence of SARS-CoV-2 infections in HWs.4 Lanher et al. described their experience of a teaching hospital in central Italy to assess SARS-CoV-2 infection rate amongst HWs and the diagnostic performance of SARS-CoV-2 serology as an index test in comparison with the SARS-CoV-2 RNA PCR assay as a reference standard; they demonstrated a low prevalence of SARS-CoV-2 infection amongst HWs, but higher than in the general population.5 That study did not investigate which control measures were accomplished or the compliance of HCWs to standard precautions.
Human-to-human transmission among close contacts of infected persons has been documented, with high risk of transmission to health care workers (HCWs) given their close and direct interactions with confirmed cases as well as shortage of personal protective equipment (PPE) in some healthcare facilities.6 According to the definition of the WHO, HCWs are all people engaged in actions whose primary intent is to enhance health. This includes physicians, nurses, midwives, paramedical staff, hospital managers, support staff and community workers, all of whom now face the occupational risk of acquiring SARS-CoV-2 infection, and at worst, even death.7
Compliance of HCWs to standards of infection control is crucial, however protecting HCWs remains a challenge for most countries due to shortages of recommended PPE and due to limited testing availability, which prevent early identification and isolation of SARS-CoV-2 cases.8 It was reported that 95% of SARS-CoV-2 infections among HCWs occurred in a non-COVID-19 designated facility and 72% of these infections were linked to exposure to a coworker or patient as the source of infection. Most of these infections were attributed to non-adherence to prescribed PPE in non- COVID-19 settings, non-adherence to strict infection control precautions, and asymptomatic infections among patients and coworkers.9
Although HCWs in certain specialties may be considered at high risk, the risk to other specialties must not be underestimated.10 Advanced age, comorbidities and elevated inflammatory markers are predictive factors of COVID-19 severity among the general population.11,12
In this study we aimed to investigate the predictors for severity of SARS-CoV-2 infection among HCWs working in either COVID-19 or non-COVID-19 healthcare settings. We aimed also to assess compliance of HCW to standard precautions of infection control and explore the possible risk factors for SARS-CoV-2 infection among HCWs.
Patients and Methods
Study Design and Subjects
This cross-sectional survey study was conducted among HCWs with suspected or confirmed COVID-19, from different Egyptian governorates. All HCWs (physicians, nurses, technicians, administrative clerks, and hospital managers) with confirmed or suspected COVID-19 completed the survey according to the study protocol. The survey was distributed to HCWs working in either COVID-19 or non-COVID-19 healthcare settings through an appropriate, web-based self-reporting questionnaire.
Defining a COVID-19 Severity Spectrum
Adults with SARS-CoV-2 infection were grouped into the following categories according to the severity of illness:
Asymptomatic or Presymptomatic Infection: Individuals who test positive for SARS-CoV-2 using a virologic test (i.e., a nucleic acid amplification test or an antigen test) but who have no symptoms that are consistent with COVID-19.
Mild Illness: Individuals who have any of the various signs and symptoms of COVID-19 (e.g., fever, cough, sore throat, malaise, headache, muscle pain, nausea, vomiting, diarrhea, loss of taste and smell) but who do not have shortness of breath, dyspnea, or abnormal chest imaging.
Moderate Illness: Individuals who show evidence of lower respiratory disease during clinical assessment or imaging and who have saturation of oxygen (SpO2) ≥94% in room air at sea level.
Severe Illness: Individuals who have SpO2 30 breaths/min, or lung infiltrates >50%.
Critical Illness: Individuals who have respiratory failure, septic shock, and/or multiple organ dysfunction.13
Sample Size Calculation
The minimum sample size required was 204 according to Rao soft sample size calculator based on 95% confidence level, 6.86% margin of error, anticipated response of 50% and total target population size of 82,160 physicians, 197,600 nurses (0.79 physicians/1000 population)14 (1.9 nurses/1000 population)15 according to 2017 estimate.
Data Collection and Questionnaire Validation
An Arabic questionnaire was created to identify risk variables for COVID-19 infection severity among HCWs. Curfew and social distance measures were applied until we reached the necessary sample size and met the inclusion requirements, thus a web-based questionnaire was designed for wider and faster dissemination and to minimize any personal contact. According to WHO and Egyptian Ministry of Health [MOH] standards, it was written in Arabic.16,17 The questions were authenticated and validated in terms of relevance, simplicity, and importance by a group of multidisciplinary professionals in relevant disciplines (pulmonology, internal medicine, epidemiology, infection control experts). A pilot study was done on 25 people of various ages and genders to evaluate the survey’s validity and make any necessary changes, and the questionnaire was finished following a series of group talks. The pilot data were not included in the final study. In this study, the scale showed good internal consistency with Cronbach’s alpha of 0.793.
The questionnaire was composed of three domains with multiple choice questions. The first domain described the demographic and socio-economic characteristics of participating HCWs. Also, it collected data about number and type of work setting and in which department SARS-CoV-2 infection may have been acquired. This domain also collected data about history of drugs that may modulate immunity. The second domain assessed compliance of HCWs to standard precautions of infection control. It collected data about recent and previous training on standard precautions of infection control especially proper hand washing and adherence to prescribed PPE in clinical practice. Also, it collected data about compliance of HCWs to these precautions. The third domain characterized COVID-19 among HCWs. It collected data about clinical presentation, diagnostic method and prescribed medications for COVID-19 among HCWs. Additionally, it collected data about duration of illnesses and relation to close family member infection.
Statistical Methods
Analysis was done using Statistical Package for Social Sciences [SPSS], version 23 [SPSS Inc., Chicago, USA]. Qualitative data including multiple response variables were presented in frequency and percentage distribution, while quantitative data were presented as mean [for central tendency] ± standard deviations [SD; for dispersion]. Chi-square goodness-of-fit test was used for single categorical variable with multiple choices. Hierarchical regression analysis was used to predict the possible independent variables which may predict the severity of the COVID-19 in HCWs as an independent variable. P value < 0.05 was considered statistically significant.
Results
In this study, 204 HCWs with confirmed or suspected COVID-19 were enrolled; their mean age (± SD) was 37 ± 11.5 and their mean body mass index was 29.7 ± 10.6. The majority (53.9%) were females, and most (49.5%) of them resided in the Delta region in Egypt. Physicians and nurses represented 52.3% and 35.3% respectively of the participating HCWs. The majority of the studied HCWs (60.8%) worked in two healthcare facilities, while only 5.4% worked in one facility. Out of 270 facilities attended by study participants, 44.4% were university hospitals and 3% were primary healthcare facilities (Table 1). About 27.9% of HCWs had chronic disease and 8.3% of them received immunosuppressant drugs regularly. Hypertension (HTN) and diabetes mellitus (DM) as associated comorbidities were reported in 41.9% and 24.3% of HCWs, respectively (Figure 1A).
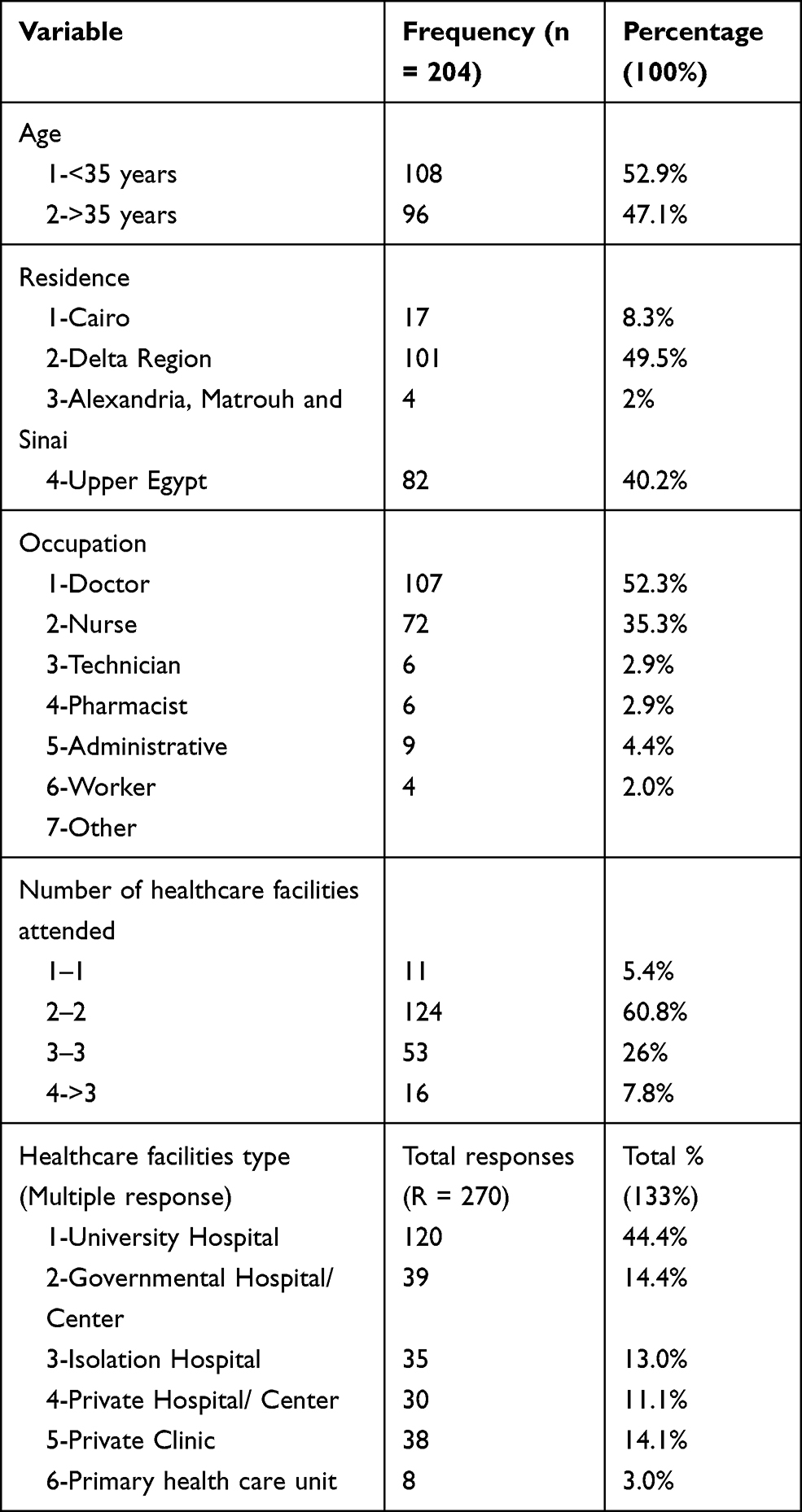 |
Table 1 General Characteristics of the HCWs who Participated in the Study |
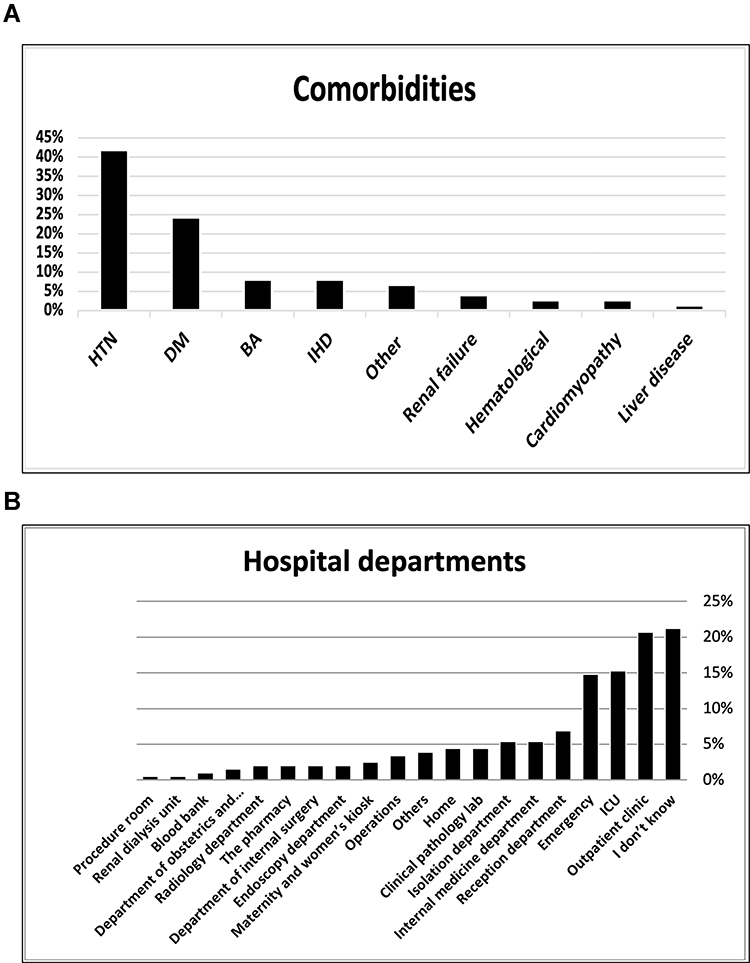 |
Figure 1 (A) Associated comorbidities in the studied group of HCWs. (B) Departments of the hospital in which SARS-COV-2 might be acquired. |
About one fifth (20.7%) of the study HCWs with COVID-19 thought that they had acquired infection in the outpatient clinic, 15.3% thought they may have got infected during their work in intensive care unit (ICU) and 14.8% of them in emergency department. On the other hand, about (21.2%) of them did not know exactly where they might have caught the COVID-19 infection (Figure 1B). Among the studied HCWs, 45.1% reported recent training on standard infection control measures, 70.6% had received training on standard hand washing and 86.8% washed their hands frequently before and after handling the patients. Only 52.5% of participant HCWs had been specially trained in how to properly put on and take off PPE. 30.9% of HCWs mentioned that PPE provided by their employer was appropriate to protect them from exposure to COVID-19, while 46.6% registered that PPE provided by their employer was adequate to protect them from exposure to COVID-19. 61.3% of HCWs had occupational safety concerns at workplace. 55.9% of HCWs were not compliant with standard recommendations for proper use of provided PPE during all work time and 53.9% removed their PPE in settings with coworkers outside patient wards (Table 2, Figure 2). More than half (53.9%) of included HCWs reported close contact (less than 6 feet distance) with SARS-CoV-2 infected patients, while only 2.7% denied contact or exposure to SARS-CoV-2 infected patients. Only 7.8% were working in a specialized COVID-19 healthcare facility and 9.8% did not know if they were exposed to patients or not (Supplementary Table 1).
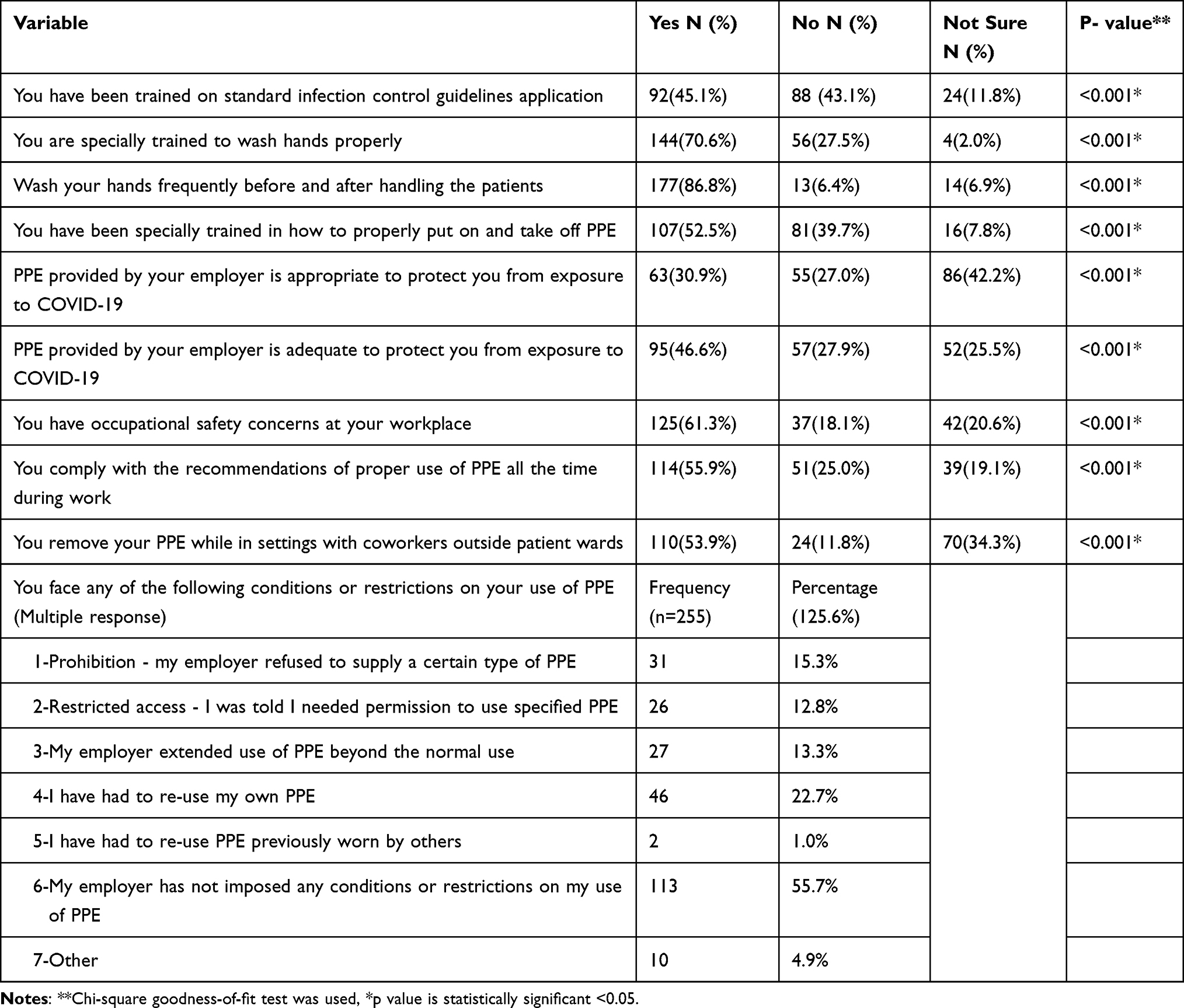 |
Table 2 Compliance of HCWs to Infection Control Measures |
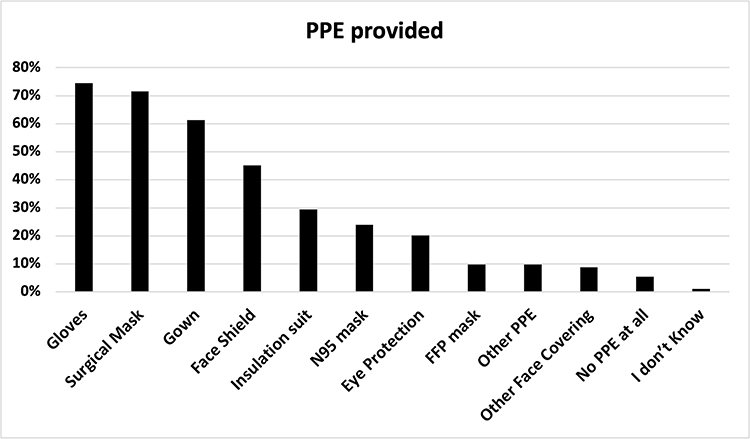 |
Figure 2 PPE that has been provided to HCWs during the COVID-19 outbreak. |
Infection of SARS-CoV-2 was confirmed in 61.3% of the studied HCWs by real time- polymerase chain reaction (RT-PCR); while only 1.0% was suspected to have COVID-19 based on their clinical presentation. Most of these HCWs (63.2%) presented with constitutional symptoms like fever, headache, fatigue and body aches and 62.7% of them presented with upper respiratory tract manifestations (sore throat, anosmia, loss of taste, sneezing and rhinorrhea). About 57.8% of infected HCWs sought medical advice in hospitals or clinics after onset of symptoms, while 28.4% were managed at home. A total of 51% and 77.5% of HCWs received hydroxychloroquine and azithromycin, respectively. Severity of COVID-19 varied among HCWs; 30.4% had mild disease, 48.5% had moderate disease, 17.2% had severe disease and 3.9% had critical disease. The majority (64.2%) of the study HCWs received treatment at home, 35.8% were admitted to hospital, and 3.9% were admitted to ICU. The average duration of disease among them was 18.99 days. The majority (53.9%) of HCWs who got COVID-19 quarantined at home as a work policy and around 13.7% were tracked by the hospital they worked at for symptom progression. Only 8.3% continued working in spite of their infection. 79.9% of infected HCWs were fully recovered, 18.6% still under treatment while 0.5% died. Near to one third (29.9%) of the family members of the COVID-19 infected HCWs were diagnosed after diagnosis of their related HCWs while 23% of them were diagnosed before the diagnosis of their related HCWs (Supplementary Table 2, Supplementary Figure 1).
Regression analysis for variables predicting COVID-19 severity among study healthcare workers showed that associated chronic diseases and management at home were the main independent variables predicting severity of SARS-COV-2 infection among HCWs, while the variables age, sex, residence, occupation or drug history of immunosuppressives had no role in severity prediction (Table 3).
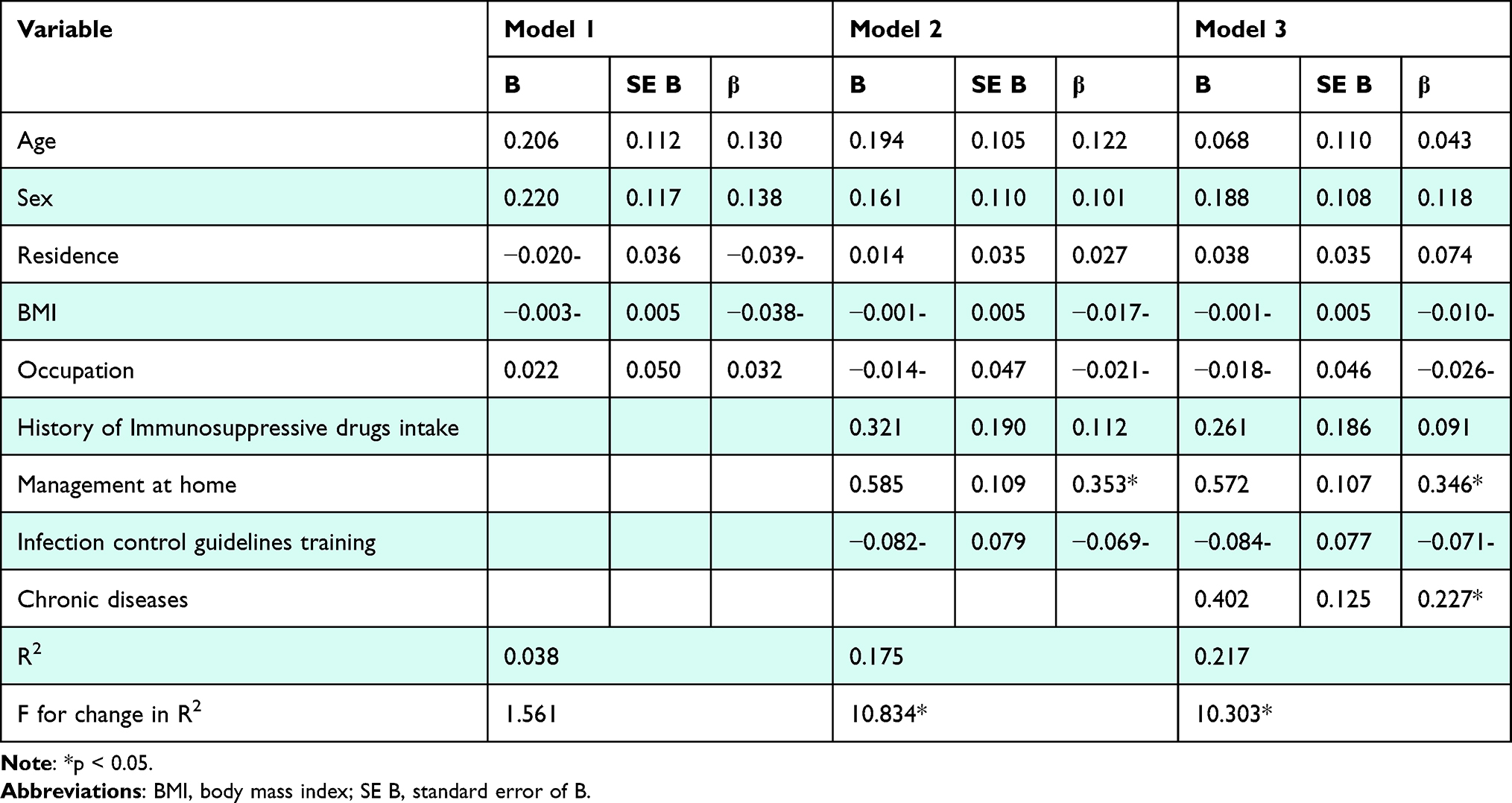 |
Table 3 Summary of Hierarchical Regression Analysis for Variables Predicting COVID-19 Severity Among Study Healthcare Workers |
Discussion
Worldwide, as well as in Egypt, the COVID-19 pandemic has significantly affected HCWs. There is increased risk for COVID-19 infection among HCWs compared with the general population. Healthcare workers are at increased risk of getting severe COVID-19 that needs hospital admission. Good understanding of SARS-CoV-2 in this special population is crucial to plan and implement proper measures for infection control, early diagnosis and treatment to ensure that HCWs who fight against COVID-19 are continually protected.18 So, we designed this study to recognize the predictors for severity of SARS-CoV-2 infection among HCWs. Also, to assess compliance of HCW to standard precautions of infection control and explore the possible risk factors for SARS-CoV-2 infection among HCWs.
Similar to several published studies, we reported that frontline (physicians and nurses) healthcare workers constitute the main percentage getting COVID-19 infection among the studied HCWs.19 Human to human transmission of SARS-CoV-2 in hospital settings was documented.20 In this study, most HCWs were working in two healthcare facilities which may increase their risk of exposure to SARS-CoV-2 infection in the workplace. McMichael et al. had described the incidence of COVID-19 among HCWs working in long-term care facilities and showed that the temporal and geographical transmission of the disease was in part due to the movement of HCWs from one facility to another.21 HCWs in certain specialties may be considered at highrisk due to frequent exposure to infected secretions; in this study HCWs dealing with patients in outpatient clinics and ICU were more likely to be infected with COVID-19.22 This may be attributed to the high flow of patients through outpatient clinics and possibility of infection transmission from asymptomatic carrier or during frequent invasive ICU tasks, in addition to lack of sufficient PPE, leading to increased risk of viral transmission.23 Nearly half of the positive HCWs reported no previous exposure to SARS-CoV-2-infected subjects and were diagnosed thanks to the proactive screening strategy.5 About one fifth (21.2%) of participant HCWs did not know where they had been infected with SARS CoV-2 as they had no previous exposure to SARS-CoV-2-infected subjects. This could be due to the fact that COVID‐19 has many atypical clinical manifestations, so the patients may go to different departments for treatment.24 Also, the possibility exists of infection transmission during the incubation period from a symptomatic patient with non-specific and brief illness or may be due to the presence of an asymptomatic carrier.23 Patient-facing HCWs are at increased risk of experiencing severe COVID-19 that needs hospital admission.25
Our study provides evidence that about one fifth (21.1%) of HCWs with COVID-19 had severe and critical disease needing hospital admission with a considerable proportion needing ICU admission. In a study by Sahu et al. the incidence of severe or critical disease in the affected HCWs was 9.9%.26 Outcome of SARS-CoV-2 infection among HCWs was reported in the current study, where a small proportion (0.05%) died. This mortality rate was lower than that reported by Vandercam et al. (0.5%).27 This observation may be related to the younger age of participant HCWs, who were also less likely to have associated comorbidities.21 HCWs may be at increased risk of transmitting SARS-CoV-2 to their household contacts,28 in accordance with our results, nearly one third of the family members of the COVID-19 infected HCWs were diagnosed after diagnosis of their related HCWs. This study clearly identified the link between comorbidities and severity of disease, where a severe level of SARS CoV-2 infection was common in HCWs known to have chronic diseases. Also it was related to type of both treatment received and care setting. Age had no role in severity prediction in this study. This might be due to the younger age of this cohort as compared with that in the study by Chu et al., who reported age was inversely related to the severity of illness.24
Our results revealed that chronic diseases and management at home were associated with severe and critical levels of COVID-19, which was inconsistent with the results of Li et al.29 Regression analysis showed that chronic diseases and management at home were the main independent variables predicting severity of SARS-COV-2 infection among HCWs. Training all HCW on preventive measures of SARS CoV2 including standard hand hygiene and PPE use is a promising policy to reduce viral transmission in healthcare facilities.27 However, more than half of participant HCWs were not compliant to standard precautions of infection control in many ways; first, improper use of provided PPE during all work time. Second, removal of their PPE while in settings with coworkers outside the patient wards. Third, close contact with SARS-CoV-2 infected patients. These results were in agreement with a published study.9
Ongoing awareness, hands-on training, and maintaining adequate supplies are needed to reinforce staff adherence to infection prevention and control practices with regular auditing and feedback from observation of staff workflow.21 Most of the participating healthcare personnel work in non-specialized COVID-19 settings. It was reported that 95% of SARS-CoV-2 infections among HCWs occurred in a non-COVID-19 designated facility and 72% of these infections were linked to exposure to a coworker or patient as the source of infection.9
This study clearly identified the link between comorbidities and severity of disease. This was not commonly reported in most other studies. This study had some limitations, first the small sample size. Second limitation could be non-compliance of Egyptian HCWs to infection control measures, unlike in other developed countries; this might increase hospital-acquired infections in Egypt which cannot be fully generalized to countries with more strict infection control roles.
Conclusion
There is an increased risk of severe COVID-19 among healthcare workers. Chronic diseases and management at home were the main independent variables predicting severity of SARS-COV-2 infection among HCWs. So, HCWs with chronic diseases should not work in COVID-19 designated hospitals, and a screening strategy should be employed. HCWs must not be negligent in adhering to strict precautions of infection control. HCWs infected with SARS-COV-2 must be managed in hospital not at home.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Ethics Approval and Informed Consent
The protocol of the study was firstly approved by Al-Azhar University ethical committee (IRB number 00012367-20-05-006). Participants provided informed consent before their participation. This study was conducted in accordance with the Declaration of Helsinki.
Consent for Publication
All co-authors reviewed and approved the final version of the manuscript.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, agreed to the submitted journal, and agree to be accountable for all aspects of the work.
Funding
This study was not funded.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382:727–733. doi:10.1056/NEJMoa2001017
2. World Health Organization. Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV). Geneva. Available from: https://www.who.int/news/item/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov).
3. Al-Mandhari A, Samhouri D, Abubakar A, Brennan R. Coronavirus disease 2019 outbreak: preparedness and readiness of countries in the Eastern Mediterranean Region. EMHJ. 2020;26(2):136–137. doi:10.26719/2020.26.2.136
4. Chou R, Dana T, Buckley DI, Selph S, Fu R, Totten AM. Epidemiology of and risk factors for coronavirus infection in health care workers: a living rapid review. Ann Intern Med. 2020;M20:1632.
5. Lahner E, Dilaghi E, Prestigiacomo C, et al. Prevalence of Sars-Cov-2 infection in Health Workers (HWs) and diagnostic test performance: the experience of a teaching hospital in Central Italy. Int J Environ Res Public Health. 2020;17(12):4417. doi:10.3390/ijerph17124417
6. Zhou P, Huang Z, Xiao Y, Huang X, Fan XG. Protecting Chinese healthcare workers while combating the 2019 novel coronavirus. Infect Control Hosp Epidemiol. 2020;41:745–746. doi:10.1017/ice.2020.60
7. World Health Organization. Health workers: a global profile. Available from: https://www.Who.int/whr/2006/06_chap1_en.Pdf.
8. World Health Organization. Rational use of personal protective equipment for coronavirus disease (COVID-19) and considerations during severe shortages. Available from: https://www.Who.int/publications-detail/rational-use-of-personal-protective-equipmentfor-coronavirus-disease-(covid-19)-and-considerations-duringsevere-shortages.
9. Alajmi J, Jeremijenko AM, Abraham JC, et al. COVID-19 infection among healthcare workers in a national healthcare system: the Qatar experience. Int J Infect Dis. 2020;100:386–389. doi:10.1016/j.ijid.2020.09.027
10. Bandyopadhyay S, Baticulon RE, Kadhum M, et al. Infection and mortality of healthcare workers worldwide from COVID-19: a systematic review. BMJ Global Health. 2020;5:e003097. doi:10.1136/bmjgh-2020-003097
11. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323:1061. doi:10.1001/jama.2020.1585
12. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395:497–506. doi:10.1016/S0140-6736(20)30183-5
13. NIH COVID-19 treatment guidelines. Available from: www.covid19treatmentguidelines.nih.gov.
14. CIA. World fact book, Egypt. Available from: https://www.cia.gov/library/publications/the-world-factbook/fields/359.html.
15. World Bank. Countries indicators/ Egypt/ Nurses and midwives. Available from: https://data.worldbank.org/indicator/SH.MED.NUMW.P3?end=2018&start=1990&view=map.
16. World Health Organization. Health workforce in the COVID-19 response. Available from: https://www.who.int/docs/default-source/nursing/who-healthworkforce-in-the-covid-19response.pdf?sfvrsn=62d228b0_2.
17. Presidency of the Council of Ministers. Center for information and decision support; 2020. Available from: https://www.care.gov.eg/EgyptCare/index.aspx.
18. Kassem AM, Talaat H, Shawky S, et al. SARS-CoV-2 infection among healthcare workers of a gastroenterological service in a tertiary care facility. Arab J Gastroenterol. 2020;21(3):151–155. doi:10.1016/j.ajg.2020.07.005
19. Pouwels KB, House T, Pritchard E, et al. Community prevalence of SARS-CoV-2 in England: results from the ONS Coronavirus Infection Survey. Lancet Public Health. 2021;6:e30–e38. doi:10.1016/S2468-2667(20)30282-6
20. Chan JF, Yuan S, Kok KH, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet. 2020;395(10223):514–523. doi:10.1016/S0140-6736(20)30154-9
21. McMichael TM, Currie DW, Clark S, et al. Epidemiology of Covid-19 in a long-term care facility in King County, Washington. N Engl J Med. 2020;382(21):2005–2011. doi:10.1056/NEJMoa2005412
22. Ing EB, Xu Q, Salimi A, Torun N. Physician deaths from Corona virus (COVID-19) disease. Occup Med (Chic Ill). 2020;70:370–374. doi:10.1093/occmed/kqaa088
23. Callaway E, Cyranoski D. China coronavirus: six questions scientists are asking. Nature. 2020;577(7792):605–607. doi:10.1038/d41586-020-00166-6
24. Chu J, Yang N, Wei Y, et al. Clinical characteristics of 54 medical staff with COVID‐19: a retrospective study in a single center in Wuhan. Chinam J Med Virol. 2020;1–7. doi:10.1002/jmv.25793.
25. Shah ASV, Wood R, Gribben C, et al. Risk of hospital admission with coronavirus disease 2019 in healthcare workers and their households: nationwide linkage cohort study. BMJ. 2020;371:m3582. doi:10.1136/bmj.m3582
26. Sahu AK, Amrithan VT, Mathew R, Aggarwal P, Najer J, Bhoi S. COVID-19 in healthcare workers – a systematic review and meta-analysis. Am J Emerg Med. 2020;38(9):1727–1731. doi:10.1016/j.ajem.2020.05.113
27. Vandercam G, Simon A, Scohy A. Clinical characteristics and humoral immune response in healthcare workers with COVID-19 in a teaching hospital in Belgium. J Hosp Infect. 2020;106(4):713–720. doi:10.1016/j.jhin.2020.09.018
28. Hou R, Dana T, Buckley DI, Selph S, Fu R, Totten AM. Epidemiology of and risk factors for coronavirus infection in health care workers: a living rapid review. Ann Intern Med. 2020;173:120–136. doi:10.7326/M20-1632
29. Li J, He X, Zhang W, et al. Meta-analysis investigating the relationship between clinical features, outcomes, and severity of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pneumonia. Am J Infect Control. 2021;49(1):82–89. doi:10.1016/j.ajic.2020.06.008
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.