")
Back to Journals » Cancer Management and Research » Volume 11
Predictive value of preoperative neutrophil-to-lymphocyte ratio in non-metastatic papillary renal cell carcinoma patients after receiving curative surgery
Authors Tu X, Wang F , Chang T, Zhang C, Zhang M, Liu Z , Qiu S, Yang L , Wei Q
Received 10 April 2019
Accepted for publication 28 July 2019
Published 7 August 2019 Volume 2019:11 Pages 7515—7524
DOI https://doi.org/10.2147/CMAR.S211727
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Xiang Tu,1,* Fan Wang,1,* Tiancong Chang,2,* Chichen Zhang,2 Mengni Zhang,3 Zhenhua Liu,1 Shi Qiu,1 Lu Yang,1 Qiang Wei1
1Department of Urology, Institute of Urology, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 2West China School of Clinical Medicine, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 3Department of Pathology and Laboratory of Pathology, State Key Laboratory of Biotherapy, West China Hospital, West China Medical School, Sichuan University, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Objective: To determine the predictive value of preoperative neutrophil-to-lymphocyte ratio (NLR) for disease-free survival (DFS) in non-metastatic papillary renal cell carcinoma (pRCC) patients following partial or radical nephrectomy.
Methods: We retrospectively analyzed 315 non-clear cell RCC patients who received curative surgery in our hospital from 2013 to 2018, from which 76 pRCC patients without metastasis (T1-3N0M0) were selected. The receiver operating characteristics (ROC) curve was drawn and an NLR cut-off of 2.5 was set to achieve maximum diagnostic accuracy for predicting DFS. Kaplan-Meier method and the Cox regression model was used to determine the relationship of NLR with DFS.
Results: During a median follow-up of 28.0 months (IQR 15.9–42.1, mean 31.4), disease recurred in 12 patients (15.8%) recording a median duration of 14.4 months (IQR 8.6–22.9, mean 16.6). The 5-year DFS was 85.5% and 61.6% for the low (<2.5) and high (≥2.5) NLR groups respectively. According to Kaplan-Meier analysis, DFS was significantly lower in the high NLR group compared with that in the low NLR group (p=0.03). Univariate analysis revealed that high NLR level (HR 3.3, p=0.041), advanced pathological T stage (HR 10.1, p<0.001), larger tumor size (HR 1.2, p=0.008) and radical nephrectomy (HR 5.7, p=0.025) were associated with poor DFS, while multivariate analysis indicated that only advanced pathological T stage (HR 6.9, p=0.010) and high NLR level (HR 3.8, p=0.028) remained as the independent prognostic factors for poor DFS.
Conclusion: A high preoperative NLR level was an independent prognostic marker for DFS in the patients of non-metastatic pRCC (pT1-3N0M0) following curative surgery. This can be used as an adjuvant tool to select patients for clinical trials or more frequent follow-up strategies.
Keywords: neutrophil-to-lymphocyte ratio, papillary renal cell carcinoma, prognostic factor, renal cell cancer
Introduction
Renal cell carcinoma (RCC) accounts for nearly 3% of all human cancers and they occur more frequently in men.1 It comprises of different subtypes based on specific histopathological and genetic characteristics. Papillary RCC (pRCC) is the second most common type, accounting for 10–15% of all cases, which can be further subdivided into type I (60–70%) and type II (30–40%).2
Currently, no adjuvant treatment can decrease the risk of RCC disease recurrence (10–20%) for patients receiving curative surgery, and regular surveillance is the standard of care.3,4 To better evaluate prognosis and optimize individualized surveillance strategy for RCC patients, several preoperative and postoperative nomograms were identified.5,6 However, these risk models have been established entirely or largely based on clear cell RCC, which lead to a lack of accurate and suitable tools for non-clear cell histology. Moreover, increasing evidence has raised concerns about prognostic value for those conventional factors, such as tumor subtypes or Fuhrman grading system in pRCC.7,8 Thus, more feasible and accurate prognostic factors are warranted.
Systemic inflammation has been revealed involving in the process of tumorigenesis and cancer development.9 Since a routine blood test can reflect inflammation status and is broadly available in many institutions, these indicators could be used as ideal parameters in predicting prognosis. It has been reported that the neutrophil-to-lymphocyte ratio (NLR) can serve as an independent predictor of survival in many human cancers, including RCC.10 However, all or the overwhelming majority of participants in these validated studies harbored clear cell RCC.11,12 Compared with clear cell RCC, pRCC exhibits a relatively lower frequency of incidence, different biological pathways, different prognostic factors, and more favorable prognosis which may yield different associations.13 Hence, our study was designed to investigate the predictive value of preoperative NLR in patients of non-metastatic pRCC (T1-3N0M0) who remained disease-free after curative surgery.
Materials and methods
Patient selection
This retrospective study was approved by the Research Ethics Committee of our hospital. All data are anonymous, and the requirement of written informed consent was therefore waived. We retrospectively reviewed 315 consecutive patients with non-clear cell RCC who underwent radical or partial nephrectomy between January 2013 and January 2018. A total of 91 eligible patients of pRCC following curative surgery were screened. Patients were excluded if they had inflammatory disease, chronic leukemia/lymphoma, other concurrent tumors, pathological T4 stage, positive lymph node histologically, or concurrent distant metastasis. This figure was further narrowed down to 76 patients (T1-3N0M0) due to the lack of preoperative or follow-up data. Figure 1 shows a flow chart of patients who met our inclusion criteria.
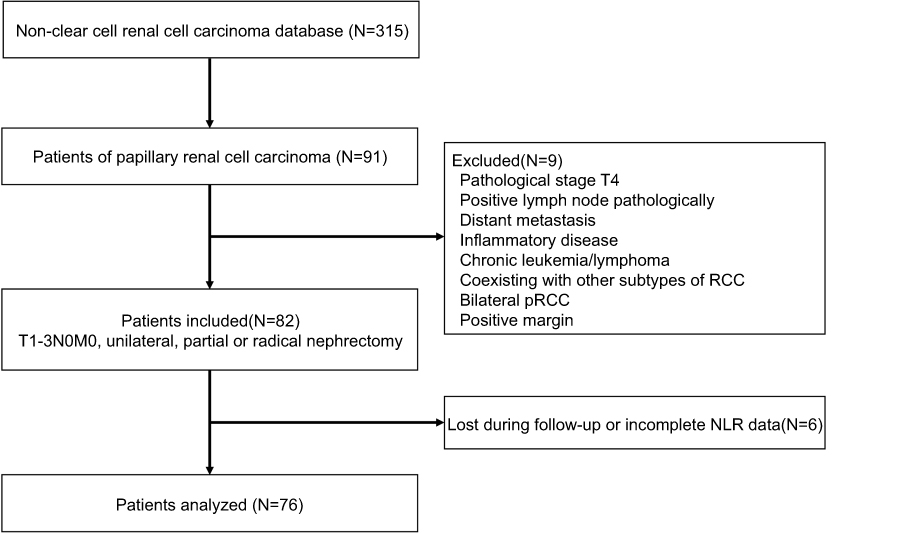 |
Figure 1 Flow chart of patient selection.Abbreviations: RCC, renal cell carcinoma; pRCC, papillary renal cell carcinoma; NLR, neutrophil-to-lymphocyte ratio. |
Data collection
Baseline characteristics and clinicopathologic data including age, sex, Eastern Cooperative Oncology Group performance status (ECOG PS), and other factors, such as smoking status, hypertension (systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg), hyperglycemia (fasting blood glucose ≥7.0 mmol/L or diabetes mellitus history), dyslipidemia (serum cholesterol ≥6.3 mmol/L and/or low density lipoprotein ≥4.2 mmol/L and/or triglyceride ≥1.7 mmol/L), hematuria (≥3 red blood cell per high-power field) and anemia (hemoglobin <120 g/L for male and <110 g/L for female) were extracted from the hospital information system. NLR was defined as the absolute neutrophil count divided by absolute lymphocyte count. Preoperative NLR was collected within 30 days before surgery, and the most recent value was selected if multiple preoperative data were available. Tumor size was defined as the maximum diameter of the tumor (pathologically). And the surgical type was divided into radical/partial or open/minimally invasive procedure. T, N and M stage was assigned based on the 2010 AJCC TNM classification.14 T, N stages were assigned pathologically, and M stage was assigned clinically. Patients with positive lymph nodes on imaging underwent lymph node dissection. Histological differentiation was graded according to Fuhrman’s nuclear grading system.15,16
Follow-up strategy
All patients were considered disease-free after surgery. Patients were followed up postoperatively every 6 months for the first 2 years and annually thereafter. Medical history, physical examination, laboratory blood tests, routine urinalysis, chest imaging and abdominal ultrasound were obtained conventionally. Computed tomography (CT) of chest, abdomen and bone scans were obtained depending on the follow-up strategy (ultrasound or CT of urinary system was undertaken alternatively), or in cases of suspicious disease recurrence or progression. For patients with disease progression between follow-up intervals, we consulted their medical records in our hospital information system and set any recurrence/progression sign recorded on radiography as the disease-progressing point. Progression/recurrence status was defined as local relapse, lymph-node metastasis, or distant metastasis. Follow-up terminated in January 2019.
Statistical analysis
Data were presented as mean ± standard deviation (SD) or median (interquartile, IQR) for continuous variables, and as frequency or percentage for categorical variables. Differences in continuous and categorical variables were analyzed by Student’s t-test and chi-squared test respectively. The primary outcome of this study was disease-free survival (DFS), which was calculated from the date of surgery to the date of disease recurrence/progression. Patients who did not experience recurrence were ceased at the date of the last follow-up. The receiver operating characteristics (ROC) curve analysis was performed to evaluate the optimal NLR cutoff value in predicting DFS based on the maximum sensitivity and specificity points. DFS functions were estimated with the Kaplan-Meier method, and differences between the high and low NLR groups were determined with the log rank test. Univariate and multivariate Cox proportional hazards regression models were used to identify independent predictors of DFS. Risk factors with p<0.1 in univariate analysis were selected for multivariate analyses, and hazard ratios (HRs) with 95% confidence intervals (CIs) were chosen to evaluate the strength of individual variables. All statistical analyses were performed using statistical software packages R (http://www.R-project.org, The R Foundation) and EmpowerStats (http://www.empowerstats.com, X & Y Solutions, Inc., Boston, MA). A 2-tailed P<0.05 was considered as statistically significant.
Results
Patient characteristics
Seventy-six patients (61 male and 15 female) with complete follow-up data were included in our final analysis. Median age at surgery was 59.0 years (IQR 50.8–66.0, mean 57.5). Partial and radical nephrectomy was performed in 39 (51.3%) and 37 (48.7%) patients respectively. The mean tumor size was 4.7±2.7 centimeters (cm). The demographic and clinicopathologic characteristics of the patients are shown in Table 1.
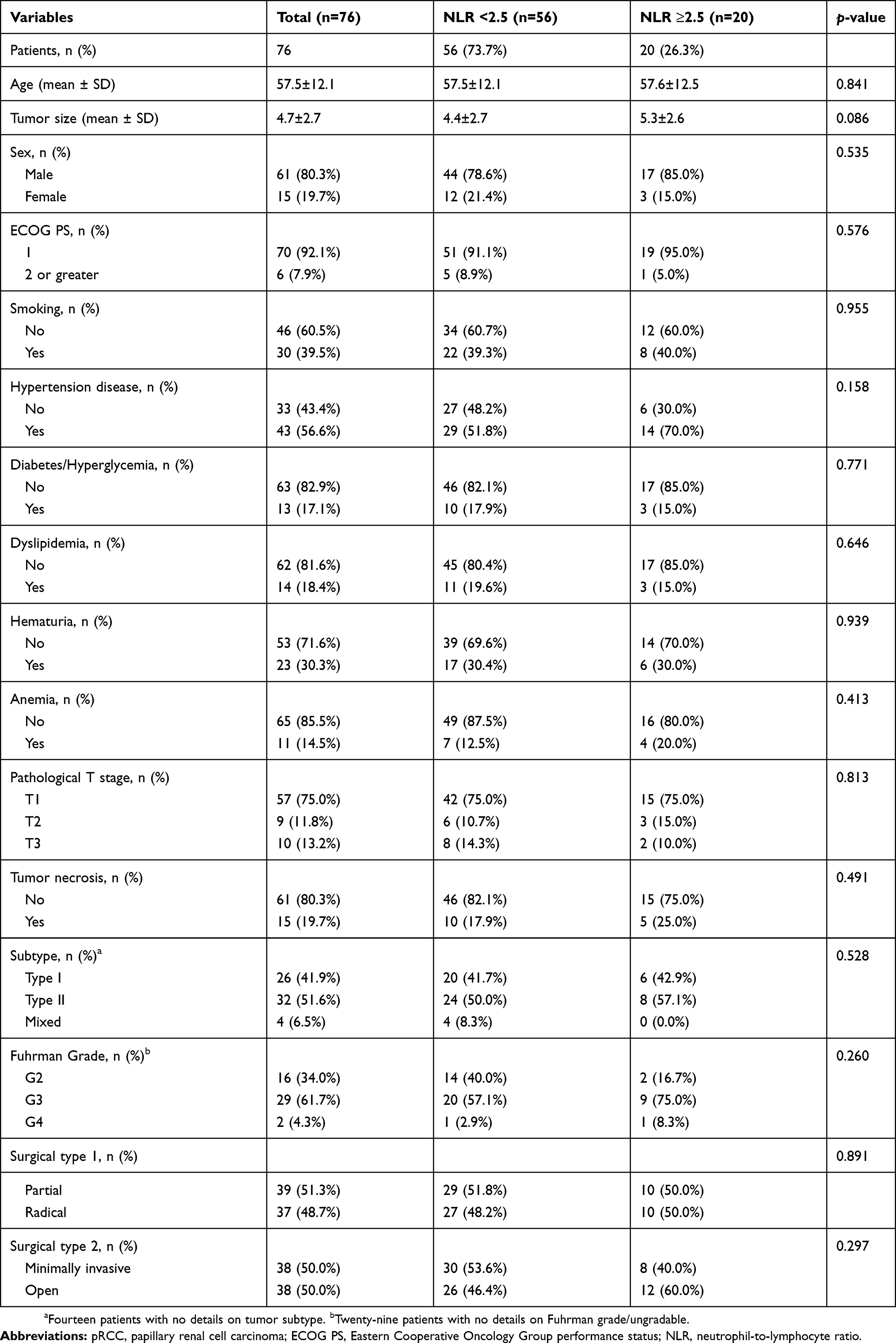 |
Table 1 Demographic and clinicopathologic characteristics of patients with non-metastatic pRCC after partial or radical nephrectomy |
NLR in association with clinical and pathological characteristics
The median preoperative neutrophil count, lymphocyte count and NLR were 3.3 (IQR 2.8–4.3), 1.8 (IQR 1.4–2.2) and 1.8 (IQR 1.4–2.6) respectively. We used the ROC curve analysis to identify suitable cutoff for visualizing survival curves, and the optimal cutoff for NLR was set to be 2.5 to achieve maximum diagnostic accuracy. On basis of the threshold of NLR, we categorized 56 patients (73.7%) into the low NLR (<2.5) group and the other 20 patients (26.3%) into the high NLR (≥2.5) group. There is a trend that patients in the high NLR group have larger tumor size (5.3±2.6 cm vs 4.4±2.7 cm) but with no significant difference (p=0.086). There were no significant differences between the two groups with regard to age, sex, pathological stages, tumor subtype, Fuhrman grade and other factors (Table 1).
NLR in association with DFS
During a median follow-up of 28.0 months (IQR 15.9–42.1, mean 31.4), disease recurred in 12 patients (15.8%) within a median duration of 14.4 months (IQR 8.6–22.9, mean 16.6). The 5-year DFS was 85.5% and 61.6% in the low and high NLR groups respectively. By Kaplan-Meier analysis, the DFS was significantly lower in the high NLR group compared with that in the low NLR group (p=0.03) (Figure 2). Univariate analysis revealed that a high NLR level (HR 3.3, p=0.041), advanced pathological T stage (HR 10.1, p<0.001), larger tumor size (HR 1.2, p=0.008) and radical nephrectomy (HR 5.7, p=0.025) were associated with a poor DFS. On multivariate analysis, advanced pathological T stage and a high NLR level remained as the independent prognostic factors for a poor DFS (HR 6.9, p=0.010) (HR 3.8, p=0.028). In addition, after adjusting according to age, sex, tumor size, surgical type, pathological T stage, and other conventional parameters, such as ECOG PS and tumor necrosis, high NLR level was still associated with a poor prognosis (HR 4.1, p=0.024) (Table 2). The characteristics of the patients who suffered relapsing after surgery were summarized in Table S1.
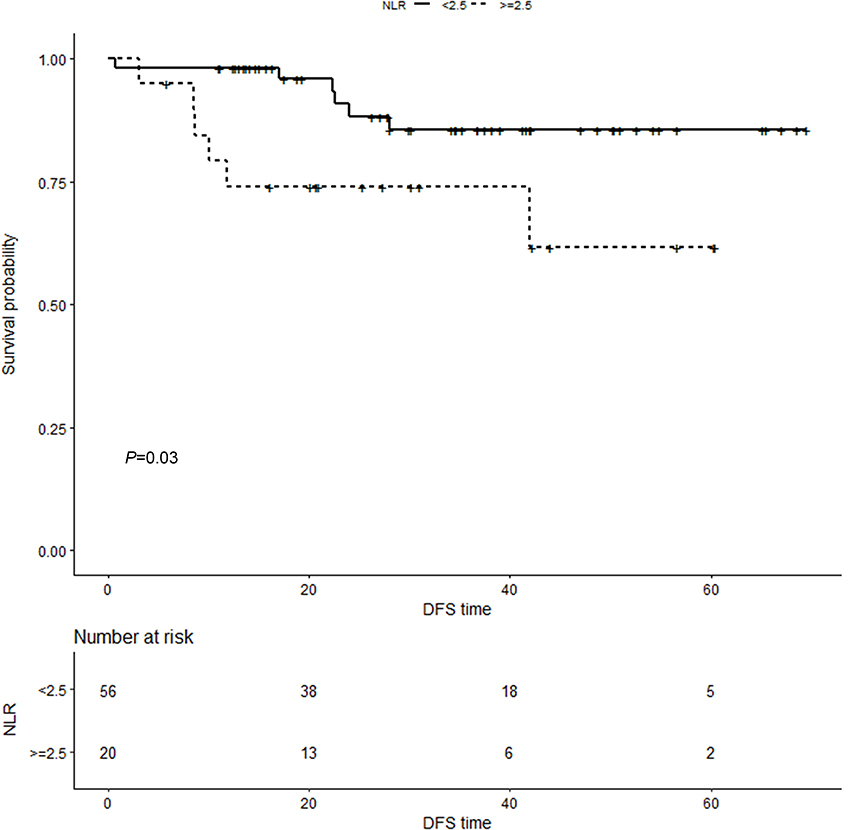 |
Figure 2 Kaplan-Meier curves and log-rank test showing patients with high NLR level (≥2.5) had worse DFS compared with those with low NLR level (<2.5) (p=0.03).Abbreviations: NLR, neutrophil-to-lymphocyte ratio; DFS, disease-free survival. |
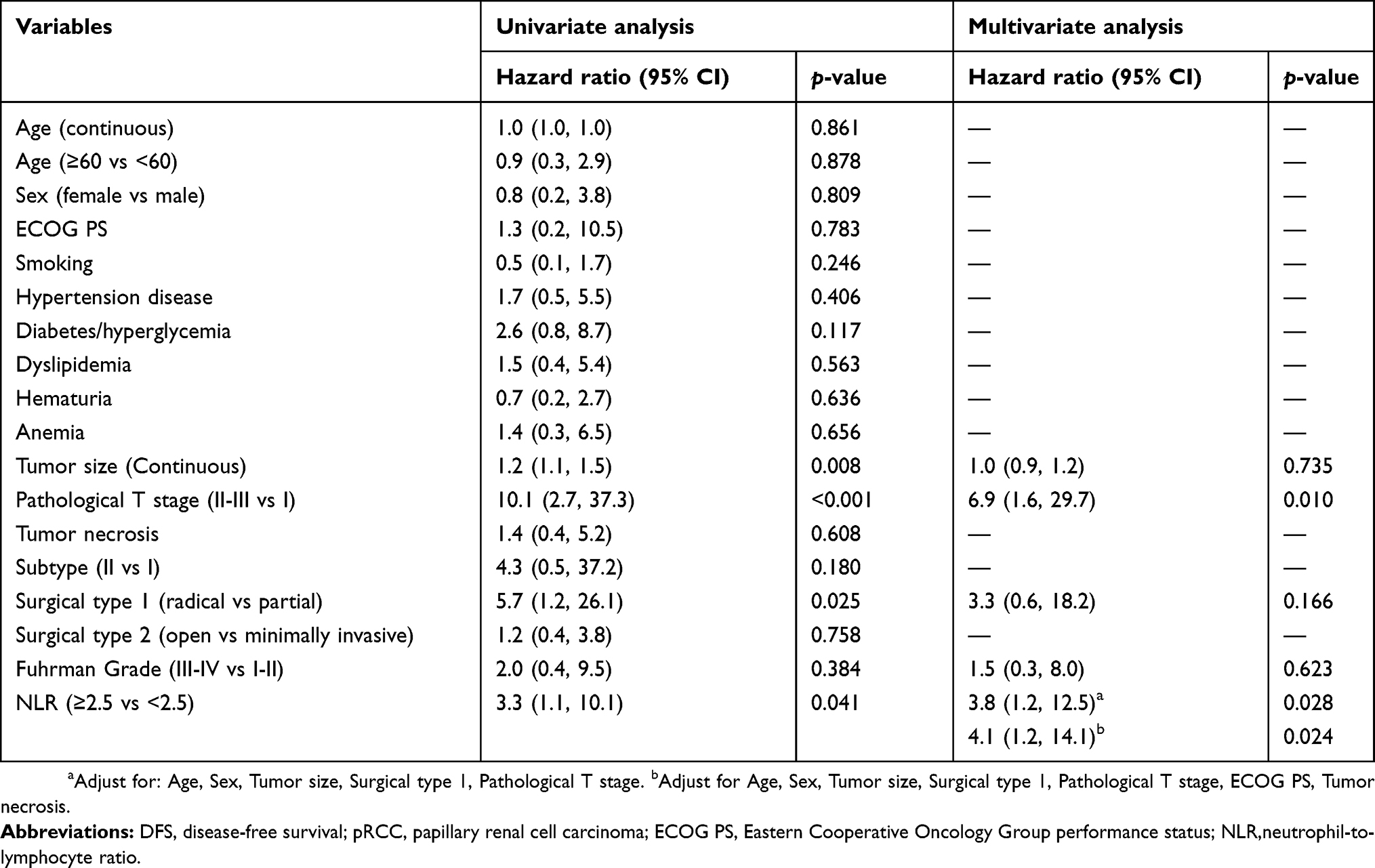 |
Table 2 Univariate and multivariate Cox regression models to predict DFS for patients of non-metastatic pRCC (T1-3N0M0) |
Discussion
In this retrospective study, we investigated the predictive value of the preoperative NLR in patients with non-metastatic pRCC (pT1-3N0M0) following radical or partial nephrectomy. The results revealed that besides conventional clinicopathological predictors, such as advanced pathological T stage, high preoperative NLR level is an independent prognostic marker which is significantly associated with a poor DFS.
A variety of preoperative and postoperative nomogram tools have been identified to predict the prognosis of patients with RCC.5,6 However, these risk models have been entirely or largely limited to the clear cell subtype which led to a lack of predictive tools for non-clear cell histology, pRCC for example. In 2010, Klatte T et al developed a predictive tool for pRCC using basic clinical and pathologic information (T stage, M stage, vascular invasion and tumor necrosis), which had an accuracy of 94.2% for predicting disease specific survival after surgery.17 A more recent study identified symptoms at presentation, and that 2010 TNM stage group and the modified Fuhrman grade system were independently associated with death from pRCC.18 Other potential factors, including age, tumor grade and pRCC type, however, were not consistently associated with prognosis.19 Issues relating to the prognostic role of tumor subtypes were debated since their introduction in 1990s.16 And the standpoint of poorer prognosis for type II pRCC was recently challenged by data showing similar oncologic outcomes in both subtypes.7,20 The Fuhrman grading system, which was firstly introduced in 1982 and thereafter widely adopted in clinical practice,15 has also come under question with the rapid expansion of RCC subtypes. Studies have indicated that Fuhrman grading may be inappropriate for non-clear cell RCC due to the inherent nuclear atypia of chromophobe RCC and large portion of ungradable pRCC.8,21 The four-tiered WHO/ISUP grading system which showed a better association with patient outcome may become a potential alternative for Fuhrman grade system in the future.22
In the last decade, increasing evidence has indicated the potential role of systematic inflammation in tumorigenesis and cancer progression. Neutrophils can be evoked by cytokines involved in cancer-related inflammation (IL-6 and tumor necrosis factor) and may help produce pro-angiogenic factors to promote proliferation, invasion and metastasis cancer cells.23,24 On the other hand, lymphocytopenia reflects a low level of CD4+ T-helper lymphocytes, which may impair cancer immune surveillance.25 NLR combined prognostic information of neutrophil and lymphocytopenia which may serve as a potential indicator. A relatively high NLR level has been identified as an independent prognostic factor for several different human cancers, including RCC.10 However, the majority of participants in these validated studies were diagnosed with clear cell RCC,11,12,26 leaving the prognostic role of NLR in non-clear cell RCC yet to be revealed.
To our knowledge, only few studies reported the prognostic role of NLR in non-clear cell RCC. The first study was conducted by de Matino et al in 2012. Their cohort included 281 patients (185 papillary and 96 chromophobe) of localized non-clear cell RCC. The five-year DFS was 88.1%. They found that an increased preoperative NLR was independently associated with DFS on a multivariable analysis (HR 1.17, p=0.022).27 The first study of NLR focusing on pRCC was conducted by Huang et al in 2015.28 Their multivariate analysis identified that a high NLR level was an independent prognostic factor for recurrence-free survival (HR 4.01, p=0.018). Regarding other even rare non-clear cell RCC, Agizamhan et al recruited 82 Xp11.2 translocation/TFE3 RCC patients and identified that high NLR levels (above 2.45) were associated with poorer DFS (HR 4.25, p=0.026).29 And Taguchi et al studied 11 patients and revealed that a high NLR level was associated with poor cancer-specific survival for collecting duct carcinoma.30
Our study was the first study that strictly recruited patients of non-metastatic pRCC (T1-3N0M0) and investigated the association between NLR and DFS for these patients who all achieved disease-free after surgery. The optimal NLR cut-off value of 2.5 is slightly lower than the two previous studies,27,28 however, de Martino et al analyzed mixed non-clear cell RCCs (papillary and chromophobe) as one group, while Huang et al simply set the same cut-off value in consistency with the former study. Moreover, the strict inclusion criteria for patients of non-metastatic status (T1-3N0M0) and the small sample size of our study may also contribute to the variety. Nevertheless, our study revealed that patients with a high preoperative NLR level has a significantly poor DFS, validating that NLR could be a prognostic factor in association with the prognosis of pRCC. This widely available, inexpensive biomarker may be used as a meaningful adjuvant with conventional prognostic factors to identify high-risk patients, who might be candidates for adjuvant clinical trials or more frequent follow-up strategies.
Our study has several limitations. Besides our single-center and retrospective design, the low incidence of pRCC and the strict inclusion criteria concurrently led to the limited sample size of our study. Though significant association between NLR and DFS was revealed, however, the interpretation of our results should be cautioned (only 12 relapses in total), and an external validation from large-scale and multicenter-design studies are warranted. And the relatively low mortality of pRCC urged us and current studies to use a surrogate parameter, DFS rather than overall survival (OS) or cancer-specific survival (CSS), to evaluate prognostic features.27,28 We assumed that longer follow-up and larger sample size may enable researchers to elucidate the relationship between potential prognostic factors and OS/CSS. Secondly, we did not exclude patients with recurrent disease within the first 6 months postoperatively. However, their preoperative staging for lymph node and distant metastasis were both negative, thus disease-free status instead of micrometastatic disease at surgery should be considered after the full resection procedure. Thirdly, six patients (7.3%) without full follow-up information were excluded from the final analysis which may introduce a potential bias. Finally, some other prognostic factors, such as microvascular invasion have not been evaluated in this study. And due to the limited available data for tumor subtype and Fuhrman grade, our study can not fully evaluate their prognostic roles in non-metastatic pRCC. Nevertheless, the role of subtype and Fuhrman grade system as prognostic factors in pRCC is still in debate.8,20 In addition, whether the four-tiered WHO/ISUP grading system is associated with better patient outcomes than the Fuhrman grade system should be prospectively investigated in the future.
Conclusion
A high preoperative NLR level is an independent prognostic marker for DFS in the patients with non-metastatic pRCC (T1-3N0M0) following curative surgery. This widely available, inexpensive biomarker may be used as an adjuvant with standard prognostic factors to identify high-risk patients, who might be candidates in adjuvant clinical trials or more frequent follow-up strategies.
Ethnical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This study was approved by the Research Ethics Committee of West China Hospital. All data are anonymous and retrospectively collected, and the requirement of written informed consent was therefore waived.
Acknowledgments
This study was supported by the National Key Research and Development Program of China (grant no. SQ2017YFSF090096), Programs from Science and Technology Department of Sichuan Province (grant no. 2017HH0063) and Young Investigator Award of Sichuan University 2017. We thank R. D. T Rajaguru for reviewing and editing the manuscript.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Moch H, Cubilla AL, Humphrey PA, Reuter VE, Ulbright TM. The 2016 WHO classification of tumours of the urinary system and male genital organs-part A: renal, penile, and testicular tumours. Eur Urol. 2016;70(1):93–105. doi:10.1016/j.eururo.2016.02.029
3. Park YH, Baik KD, Lee YJ, Ku JH, Kim HH, Kwak C. Late recurrence of renal cell carcinoma >5 years after surgery: clinicopathological characteristics and prognosis. BJU Int. 2012;110(11 Pt B):E553–E558. doi:10.1111/j.1464-410X.2012.11246.x
4. Ljungberg B, Albiges L, Abu-Ghanem Y, et al. European association of urology guidelines on renal cell carcinoma: the 2019 update. Eur Urol. 2019;75(5):799–810. doi:10.1016/j.eururo.2019.02.011
5. Frank I, Blute ML, Cheville JC, Lohse CM, Weaver AL, Zincke H. An outcome prediction model for patients with clear cell renal cell carcinoma treated with radical nephrectomy based on tumor stage, size, grade and necrosis: the SSIGN score. J Urol. 2002;168(6):2395–2400. doi:10.1097/01.ju.0000035885.91935.d5
6. Karakiewicz PI, Suardi N, Capitanio U, et al. A preoperative prognostic model for patients treated with nephrectomy for renal cell carcinoma. Eur Urol. 2009;55(2):287–295. doi:10.1016/j.eururo.2008.07.037
7. Ledezma RA, Negron E, Paner GP, et al. Clinically localized type 1 and 2 papillary renal cell carcinomas have similar survival outcomes following surgery. World J Urol. 2016;34(5):687–693. doi:10.1007/s00345-015-1692-3
8. Delahunt B, Egevad L, Srigley JR, Samaratunga H. Fuhrman grading is inappropriate for papillary renal cell carcinoma. World J Urol. 2018;36(8):1335–1336. doi:10.1007/s00345-017-2153-y
9. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–674. doi:10.1016/j.cell.2011.02.013
10. Roxburgh CS, McMillan DC. Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol. 2010;6(1):149–163. doi:10.2217/fon.09.136
11. Ohno Y, Nakashima J, Ohori M, Hatano T, Tachibana M. Pretreatment neutrophil-to-lymphocyte ratio as an independent predictor of recurrence in patients with nonmetastatic renal cell carcinoma. J Urol. 2010;184(3):873–878. doi:10.1016/j.juro.2010.05.028
12. Pichler M, Hutterer GC, Stoeckigt C, et al. Validation of the pre-treatment neutrophil-lymphocyte ratio as a prognostic factor in a large European cohort of renal cell carcinoma patients. Br J Cancer. 2013;108(4):901–907. doi:10.1038/bjc.2013.28
13. Steffens S, Janssen M, Roos FC, et al. Incidence and long-term prognosis of papillary compared to clear cell renal cell carcinoma–a multicentre study. Eur J cancer. 2012;48(15):2347–2352. doi:10.1016/j.ejca.2012.05.002
14. Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–1474. doi:10.1245/s10434-010-0985-4
15. Fuhrman SA, Lasky LC, Limas C. Prognostic significance of morphologic parameters in renal cell carcinoma. Am J Surg Pathol. 1982;6(7):655–663.
16. Delahunt B, Eble JN. Papillary renal cell carcinoma: a clinicopathologic and immunohistochemical study of 105 tumors. Mod Pathol. 1997;10(6):537–544.
17. Klatte T, Remzi M, Zigeuner RE, et al. Development and external validation of a nomogram predicting disease specific survival after nephrectomy for papillary renal cell carcinoma. J Urol. 2010;184(1):53–58. doi:10.1016/j.juro.2010.03.026
18. Sukov WR, Lohse CM, Leibovich BC, Thompson RH, Cheville JC. Clinical and pathological features associated with prognosis in patients with papillary renal cell carcinoma. J Urol. 2012;187(1):54–59. doi:10.1016/j.juro.2011.09.053
19. Borgmann H, Musquera M, Haferkamp A, et al. Prognostic significance of Fuhrman grade and age for cancer-specific and overall survival in patients with papillary renal cell carcinoma: results of an international multi-institutional study on 2189 patients. World J Urol. 2017;35(12):1891–1897. doi:10.1007/s00345-017-2078-5
20. Polifka I, Agaimy A, Herrmann E, et al. High proliferation rate and TNM stage but not histomorphological subtype are independent prognostic markers for overall survival in papillary renal cell carcinoma. Hum Pathol. 2019;83:212–223. doi:10.1016/j.humpath.2018.08.006
21. Delahunt B, Sika-Paotonu D, Bethwaite PB, et al. Fuhrman grading is not appropriate for chromophobe renal cell carcinoma. Am J Surg Pathol. 2007;31(6):957–960. doi:10.1097/01.pas.0000249446.28713.53
22. Delahunt B, Cheville JC, Martignoni G, et al. The International Society of Urological Pathology (ISUP) grading system for renal cell carcinoma and other prognostic parameters. Am J Surg Pathol. 2013;37(10):1490–1504. doi:10.1097/PAS.0b013e318299f0fb
23. Kusumanto YH, Dam WA, Hospers GA, Meijer C, Mulder NH. Platelets and granulocytes, in particular the neutrophils, form important compartments for circulating vascular endothelial growth factor. Angiogenesis. 2003;6(4):283–287. doi:10.1023/B:AGEN.0000029415.62384.ba
24. Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):e493–e503. doi:10.1016/S1470-2045(14)70263-3
25. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–444. doi:10.1038/nature07205
26. Viers BR, Houston Thompson R, Boorjian SA, Lohse CM, Leibovich BC, Tollefson MK. Preoperative neutrophil-lymphocyte ratio predicts death among patients with localized clear cell renal carcinoma undergoing nephrectomy. Urol Oncol. 2014;32(8):1277–1284. doi:10.1016/j.urolonc.2014.05.014
27. de Martino M, Pantuck AJ, Hofbauer S, et al. Prognostic impact of preoperative neutrophil-to-lymphocyte ratio in localized nonclear cell renal cell carcinoma. J Urol. 2013;190(6):1999–2004. doi:10.1016/j.juro.2013.06.082
28. Huang J, Dahl DM, Dong L, et al. Preoperative neutrophil-to-lymphocyte ratio and neutrophilia are independent predictors of recurrence in patients with localized papillary renal cell carcinoma. Biomed Res Int. 2015;2015:891045. doi:10.1155/2015/891045
29. Agizamhan S, Qu F, Liu N, et al. Preoperative neutrophil-to-lymphocyte ratio predicts the surgical outcome of Xp11.2 translocation/TFE3 renal cell carcinoma patients. BMC Urol. 2018;18(1):60. doi:10.1186/s12894-018-0374-z
30. Taguchi S, Fukuhara H, Miyakawa J, et al. Prognostic significance of neutrophil-to-lymphocyte ratio in collecting duct carcinoma. Jpn J Clin Oncol. 2018;48(7):692–694. doi:10.1093/jjco/hyy076
Supplementary material
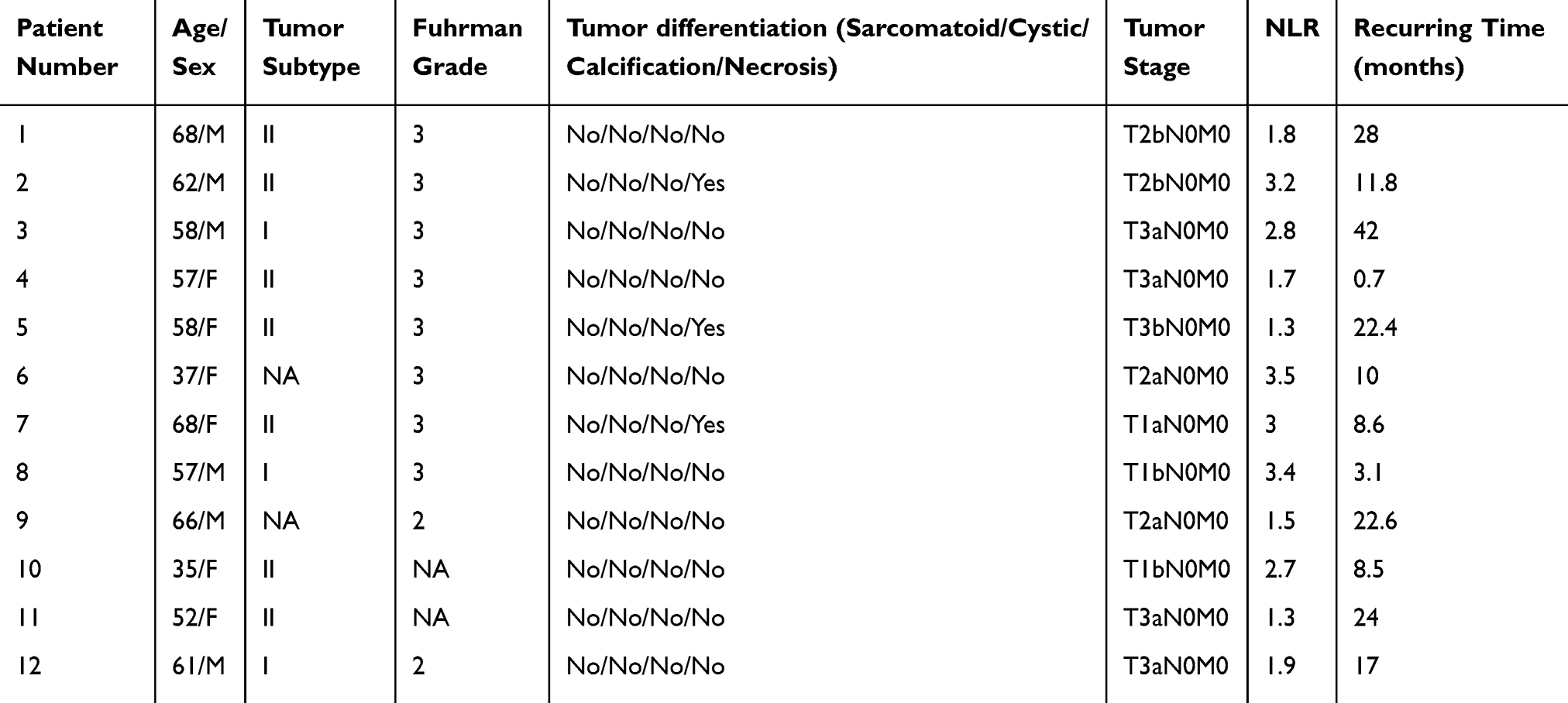 |
Table S1 Patient characteristics who recurred following curative surgery |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.