")
Back to Journals » ImmunoTargets and Therapy » Volume 12
Predictive Nomogram for Hyperprogressive Disease During Anti-PD-1/PD-L1 Treatment in Patients with Advanced Non-Small Cell Lung Cancer
Authors Wang X , Guo Z , Wu X, Chen D, Wang F, Yang L, Luo M, Wu S, Yang C, Huang L, Fu L
Received 18 May 2022
Accepted for publication 29 July 2022
Published 4 January 2023 Volume 2023:12 Pages 1—16
DOI https://doi.org/10.2147/ITT.S373866
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Shurin
Xueping Wang, Zhixing Guo, Xingping Wu, Da Chen, Fang Wang, Lewei Yang, Min Luo, Shaocong Wu, Chuan Yang, Lamei Huang, Liwu Fu
State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine; Guangdong Esophageal Cancer Institute; Cancer Center, Sun Yat-sen University, Guangzhou, 510060, People’s Republic of China
Correspondence: Liwu Fu, State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine; Guangdong Esophageal Cancer Institute; Cancer Center, Sun Yat-sen University, 651 Dongfengdong Road, Guangzhou, 510060, People’s Republic of China, Email [email protected]
Introduction: Various studies have reported that anti-PD-1/PD-L1 treatment may lead to the rapid development of tumors called hyperprogressive disease (HPD). A nomogram for HPD prediction in NSCLC patients is urgently needed.
Methods: This retrospective cohort study included 176 cases for establishing a model of HPD prediction and 85 cases for validation in advanced NSCLC patients treated with PD-1/PD-L1 inhibitors. HPD was defined as tumor growth rate (TGR, ≥ 2), tumor growth kinetics (TGK, ≥ 2) or time to treatment failure (TTF, ≤ 2 months). Univariate and multivariate logistic regression were used to estimate the specified factors associated with HPD. Then, the nomogram was developed and validated.
Results: Anti-PD-1/PD-L1 therapy resulted in a 9.66% (17/176) incidence of HPD in advanced NSCLC. The overall survival (OS) and progression-free survival (PFS) in patients with HPD were significantly shorter than those in patients without HPD (OS: 7.00 vs 12.00 months, P< 0.01; PFS: 2.00 vs 5.00 months, P< 0.001, respectively). The HPD prediction nomogram included APTT (P< 0.01), CD4+ CD25+ CD127-low cells (Treg cells) (P< 0.01), the presence of liver metastasis (P< 0.05), and more than two metastatic sites (P< 0.05). Then, patients were divided into two groups by the “HPD score” calculated by the nomogram. The C-index was 0.845, while the area under the curve (AUC) was 0.830 (sensitivity 75.00%, specificity 91.70%). The calibration plot of HPD probability showed an optimal agreement between the actual observation and prediction by the nomogram. In the validation cohort, the AUC was up to 0.960 (sensitivity 88.70%, specificity 89.80%).
Conclusions: The nomogram was constructed with the presence of liver metastasis, more than two metastatic sites, lengthened APTT and a high level of Treg cells, which could be used to predict HPD risk.
Keywords: PD-1/PD-L1 inhibitors, hyperprogressive disease, non-small cell lung cancer, nomogram
Introduction
Immune checkpoint inhibitors (ICIs) in cancer treatment have become one of the most important advances in the medical field in recent years and are based on inhibiting the interaction of immune checkpoint receptors on immune cells and immune checkpoint ligands on tumor cells.1 ICIs involving the programmed cell death 1 (PD-1) and programmed cell death ligand 1 (PD-L1) pathways have revolutionized the management of various types of malignancies with more effect and less toxicity than conventional chemotherapy or targeted therapies, such as in melanoma,2,3 non-small cell lung cancer (NSCLC),4,5 advanced urothelial carcinoma,6,7 head and neck squamous cell carcinoma8 and so on.
As the most common malignancy, lung cancer (LC) is still the main cause of cancer morbidity and mortality worldwide and is divided into non-small cell lung cancer (NSCLC, 80%) and small cell lung cancer (SCLC, 20%).9 For stages I and II NSCLC, surgery is considered to be a curable treatment. However, 75% of NSCLC is diagnosed in the advanced stage as III or IV with a high likelihood of mortality and impossible resection.10 Systemic therapy, including chemotherapy, targeted therapy and immunotherapy, is involved. As a monotherapy or in combination with other therapies, ICIs have shown significant survival benefits for NSCLC patients.11–13 However, during the treatment of anti-PD-1/PD-L1, the long-term response rate does not exceed 20% in NSCLC patients,14 especially with an unexpected accelerated tumor volume and rate during treatment associated with clinical deterioration, which has been defined as hyperprogressive disease (HPD). HPD was defined by the following conditions: tumor growth rate (TGR, ≥ 2), tumor growth kinetics (TGK, ≥ 2) or time to treatment failure (TTF, ≤ 2 months).15 Many studies indicate that patients undergoing ICI treatment with HPD experience a poor prognosis, including a faster decline in overall survival (OS) and progression-free survival (PFS) than those treated with conventional therapies.16,17 Early identification of patients who are susceptible to HPD could allow them to avoid ICI treatment, and those in good clinical condition could be re-estimated early and switched to another potentially effective treatment, such as chemotherapy or targeted therapy. However, the mechanism and features of HPD in patients during anti-PD-1/PD-L1 therapy remain unclear. There is an urgent need to look for clinical features in HPD prediction.
Here, a retrospective study was performed to analyze the association between HPD, treatment outcomes, clinicopathologic variables and hematological biomarkers in advanced NSCLC patients before ICI treatment18. Based on these factors, a nomogram was developed and validated, which was used to predict HPD before anti-PD-1/PD-L1 therapy to assist in individualized medicine.
Materials and Methods
Ethics Statement
The Institute Research Ethics Committee of the Sun Yat-Sen University Cancer Center, Guangzhou, China approved this study (IRB No. YB2020-006-01). Written informed consent was exempted because of retrospective analysis. This study was conducted in accordance with the Declaration of Helsinki and patient confidentiality is guaranteed.
Patients
A retrospective study enrolled 176 patients with advanced NSCLC who were treated with anti-PD-1/PD-L1 therapy between January 1, 2016, and September 31, 2019, at Sun Yat-sen University Cancer Center. All patients met the following inclusion criteria: (1) histologically confirmed as advanced NSCLC (stage III or IV); (2) patients over 18 years of age; (3) patients who received ICI therapy (nivolumab, pembrolizumab, or atezolizumab); and (4) baseline assessments were performed with a computed tomography scan (CT scan) of the chest and abdomen within 2 weeks before treatment, and then the oncological outcomes were assessed every 2 cycles of treatment. The tumor responses to ICI were determined by the response evaluation criteria in solid tumors (RECIST) version 1.1.19 The clinicopathological information was obtained from the electronic medical record system (EMR) at the beginning of treatment, while hematological features were also measured at the time of ICI therapy treatment initiation. The independent validation cohort included 85 consecutive NSCLC patients with the same inclusion and exclusion criteria as those in the primary cohort from October 1, 2019, to September 31, 2020, at Sun Yat-sen University Cancer Center.
Laboratory Measurements
Serum/plasma samples were collected at room temperature before treatment initiation (baseline visit) and then centrifuged at 3500 r/min for 10 min. All biomarkers were detected using a commercially available flow cytometry assay according to the manufacturer’s instructions. Routine Blood Test was estimated by Sysmex XN 2000 (Japan), Coagulation Test was estimated by Sysmex XN 5100 (Japan), Liver Function Test, Renal Function Test, Blood Lipid Test and Inflammation Test were estimated by Hitachi 008 (Japan), Thyroid Function Test was estimated by Roche 602 (Germany), Lymphocyte Subsets Exam was estimated by BD FACS Canto II (USA). LMR was calculated by the lymphocyte-monocyte ratio, NLR was calculated by the neutrophil–lymphocyte ratio, and dNLR was defined by neutrophils/[leukocytes minus neutrophils].
PD-L1 expression was assessed by IHC staining. Formalin-fixed paraffin-embedded (FFPE, 3-µm thickness) sections were used for deparaffinization and rehydration. PD-L1 (a rabbit monoclonal anti-human antibody, E1L3 N™, Cell Signaling Technology, Danvers, MA) was selected for staining PD-L1 by Bond Max Microsystems. Two pathologists blinded to clinical information independently assessed the expression of PD-L1. The staining results were recorded with an H-score (giving a range of 0–300), which corresponded to an overall staining intensity score (giving a range of 0–3) as follows: 0, absent; 1, weak; 2, moderate; and 3, strong. Tumor cells with more than 10% PD-L1 expression, which were defined as having an H-score ≥ 5, were used as the cutoff for PD-L1 positivity and were considered to be positive.20
HPD Definition
At least 2 CT scans were required for radiological evaluation, including the baseline CT scan (performed up to 7 days before treatment initiation) and the first CT scan for response assessment (within 6 weeks after initiating treatment and a minimum of 2 weeks after treatment initiation). Even CT scans performed between 3 months and 2 weeks prior to the baseline CT scan were also reviewed. CT scans were reviewed by Dr. Lizhi Liu.
All analyses regarding tumor growth dynamics were based on serial CT scans. TGR and TGK were defined according to previous reports.16,21,22 The TGR was measured as the percentage increased change in the tumor volumes for the target lesions according to RECIST 1.1 criteria per month. Similarly, TGK was reported as the percentage increase in the sum of the longest diameters (SLDs) of the target lesions according to RECIST 1.1 criteria per month. TTF was defined as the time from the start of ICI therapy to the interruption with no reason within 2 months (TTF ≤ 2 months).23 The definition of HPD is based on TGR, TGK or TTF.
Statistical Analysis
The flowchart of our research program is presented in Figure 1. NSCLC patients were divided into HPD and non-HPD groups. Associations between HPD and non-HPD patients of clinicopathological variables and baseline hematological features were evaluated using Fisher’s exact test for categorical variables and Student’s test or the Mann–Whitney U-test for continuous variables. SPSS 16.0 (IBM, Chicago, IL, USA) was used for the above statistical analysis. Overall survival (OS) was defined as the interval time between the initiation time of anti-PD-1/PD-L1 therapy and the time of death from any cause. Progression-free survival (PFS) was estimated from the time of anti-PD-1/PD-L1 therapy to the date of disease progression or death due to any cause. The Kaplan–Meier method was used to estimate OS and PFS, which were compared using the Log rank test. A logistic regression model was applied to estimate the association of specified variables HPD, with odds ratios (OR) and 95% confidence intervals (CI). Specified factors identified in the logistic regression analysis were applied to develop a diagnostic model for HPD. The nomogram was constructed for predicting HPD before ICI therapy. To quantify the discrimination performance of the nomogram, Harrell’s C-index and ROC curve were evaluated. In brief, a C-index value greater than 0.75 was considered to indicate a relatively good degree of discrimination.24 Calibration was performed by observing survival probability with Kaplan–Meier estimation. The decision curve was plotted for the nomogram model. A two-tailed P value < 0.05 was considered as statistically significant. R software (version 3.1.4; http://www.Rproject.org) was used for the above statistical analysis.
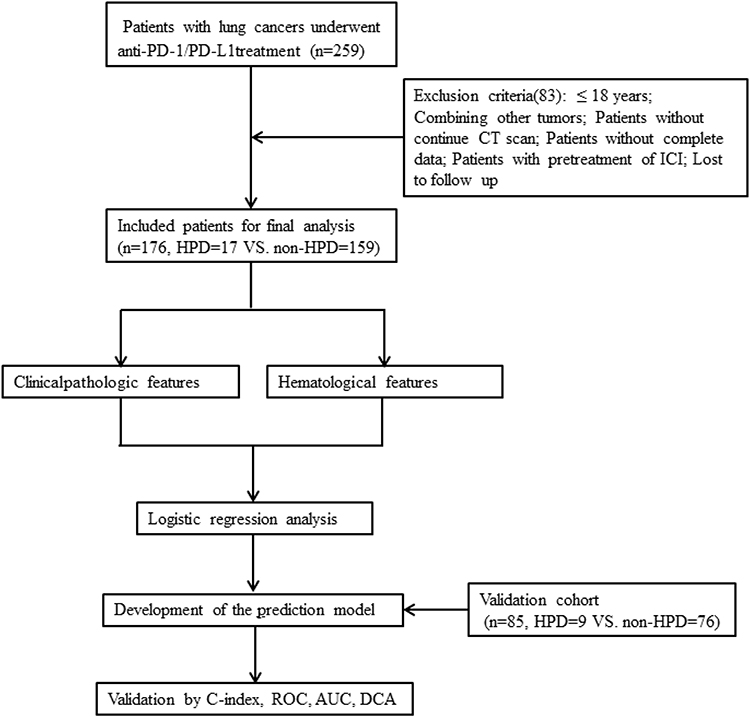 |
Figure 1 Flowchart of our study. |
Results
Patient Characteristics
Overall, our study enrolled 261 patients with advanced NSCLC treated with ICIs, and patients were divided into primary and validation sets by time sequence. There were 17 (9.66%) and 9 (10.59%) patients with HPD in the two cohorts, respectively. In the primary cohort, 7 (20.9%), 5 (20.5%), and 5 (37.3%) patients experienced HPD as defined according to TGR, TGK, and TTF, respectively. In the validation cohort, 4 (44.44%), 2 (22.22%), and 3 (33.33%) patients experienced HPD. There were no differences in terms of age, sex, the constituents of adenocarcinoma, squamous and sarcomatoid, metastasis site including brain and liver and numbers, HPD occurrence rate and so on between the two cohorts. The main characteristics of the patient cohort are listed in Table 1. In the primary cohort, the median OS was 12.00 months (IQR, 7–20 months), and the median PFS was 4.00 months (IQR, 2–13.75 months). The response of patients to ICI treatment was classified into partial response (PR, 22 patients), stable disease (SD, 71 patients), and progressive disease (PD, 83 patients); furthermore, 17 (9.66%) patients met the HPD criteria. In the validation cohort, there were 19 patients with PR, 19 patients with SD, and 47 patients with PD; furthermore, 9 patients met the HPD criteria. The serum biomarkers of the primary cohort before ICI therapy are summarized in Table 2.
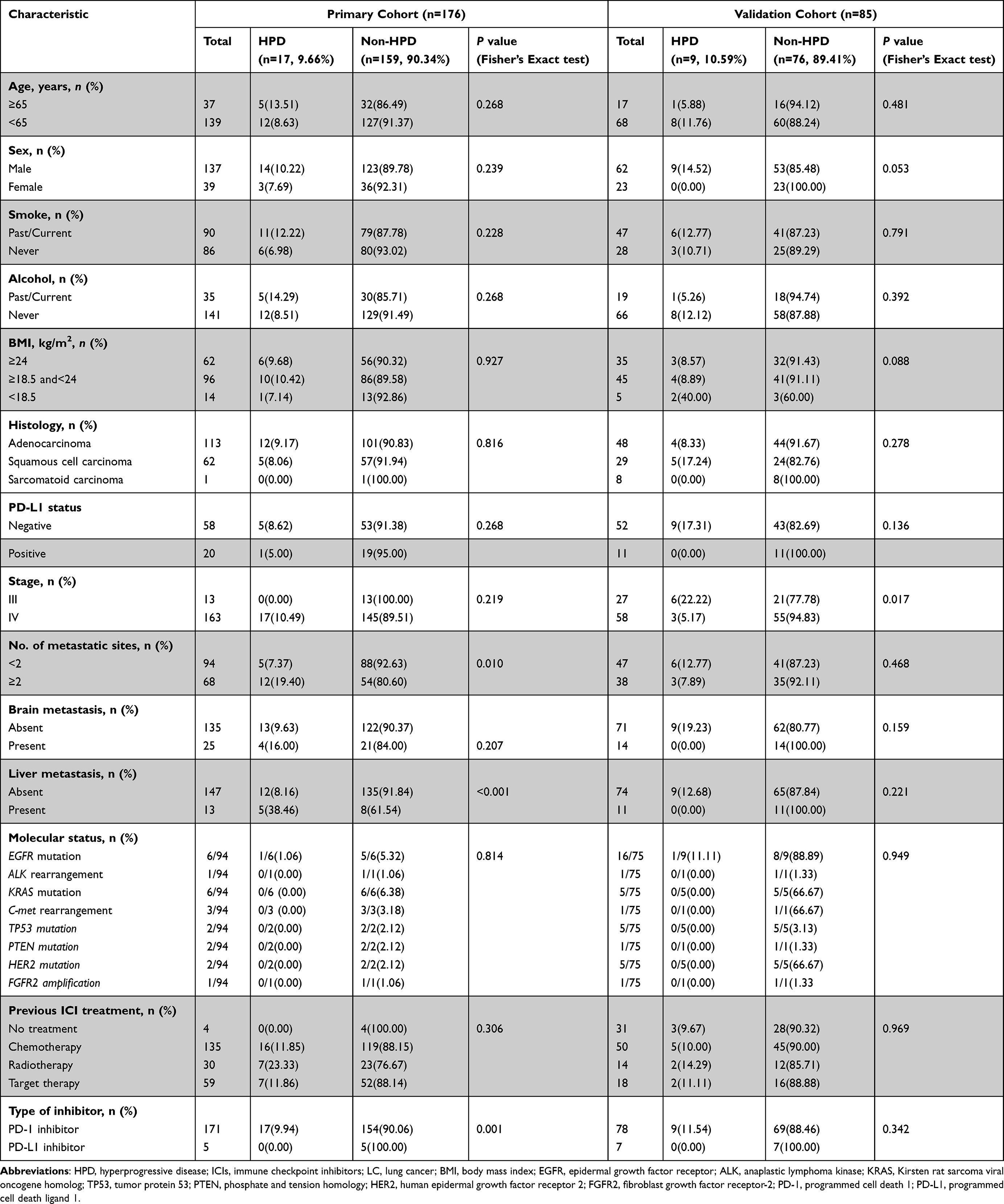 |
Table 1 Baseline Clinical Features of LC Patients with ICI Therapy |
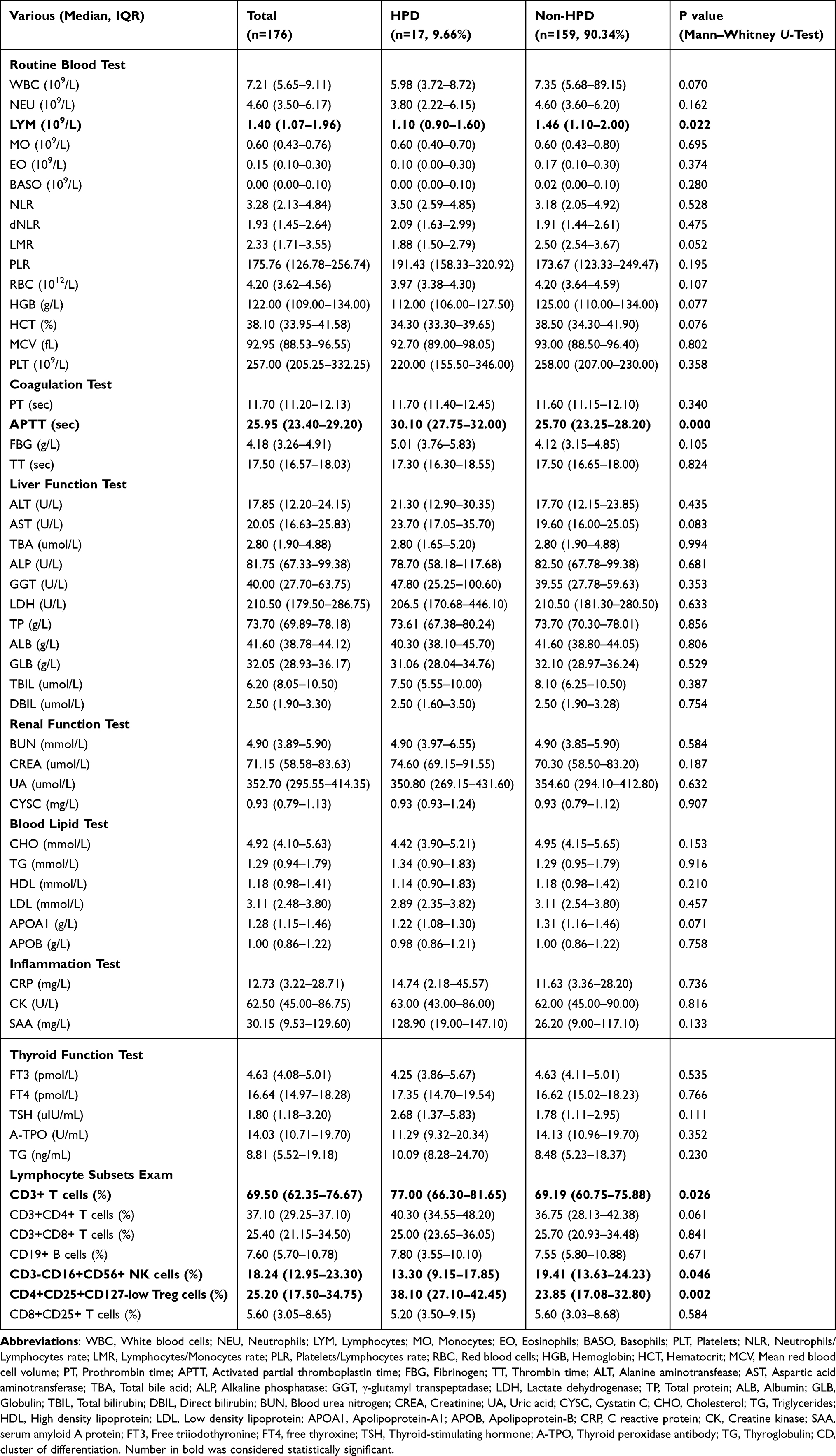 |
Table 2 Hematological Examination Biomarkers of LC Patients with ICI Therapy in the Primary Cohort |
Association Between HPD Status and Clinicopathologic Variables
To evaluate the incidence of HPD, we analyzed the kinetics of tumor growth by comparing CT scans in the reference period and the experimental period as well as the time from treatment initiation to discontinuation. Among them, 17 (9.66%) NSCLC patients were initially grouped into HPD in the primary cohort. The median OS of patients with HPD was significantly shorter than that of patients without HPD (7.00 months [IQR, 2.00–14.50 months] vs 12.00 months [IQR, 8.00–21.00 months], P<0.01, Figure 2A), while the median PFS of patients with HPD was also significantly shorter than that of patients without HPD (2.00 months [IQR, 2.00–3.00 months] vs 5.00 months [IQR, 2.00–16.00 months], P<0.001, Figure 2B). Furthermore, we categorized responses to the treatment according to the following categories: PR, SD, PD without HPD, and HPD. Both OS and PFS showed clear separation in patients with different responses (Figure 2C and D). The OS in patients with HPD was significantly shorter than that in PD patients alone (OS: 7.00 months [IQR, 2.00–14.50 months] vs 11.00 months [IQR, 6.00–16.00 months], P<0.039), while there was no significant difference in PFS between HPD and PD patients (2.00 months [IQR, 2.00–3.00 months] vs 2.00 months [IQR, 2.00–3.00 months], P=0.509). To identify the potential biomarkers of HPD, the clinicopathologic (Table 1) and hematological variables (Table 2) were compared between HPD and non-HPD NSCLC patients. There were significant differences between HPD and non-HPD patients in more than two metastatic sites (P<0.01), presence of liver metastasis (P<0.001), type of inhibitor (P<0.01), lymphocyte count (LYM, P<0.01), activated partial prothrombin time (APTT, P<0.001), CD3+ T cells (P<0.01), CD3-CD16+CD56+ NK cells (P<0.01), and CD4+CD25+ CD127-low cells Treg cells (P<0.01). Then, multivariate logistic regression analysis was performed to identify factors for HPD prediction: APTT (P<0.01) and Treg cells (P<0.01), more than two metastatic sites (P<0.05), and the presence of liver metastasis (P<0.05) (Table 3, Figures 3 and 4).
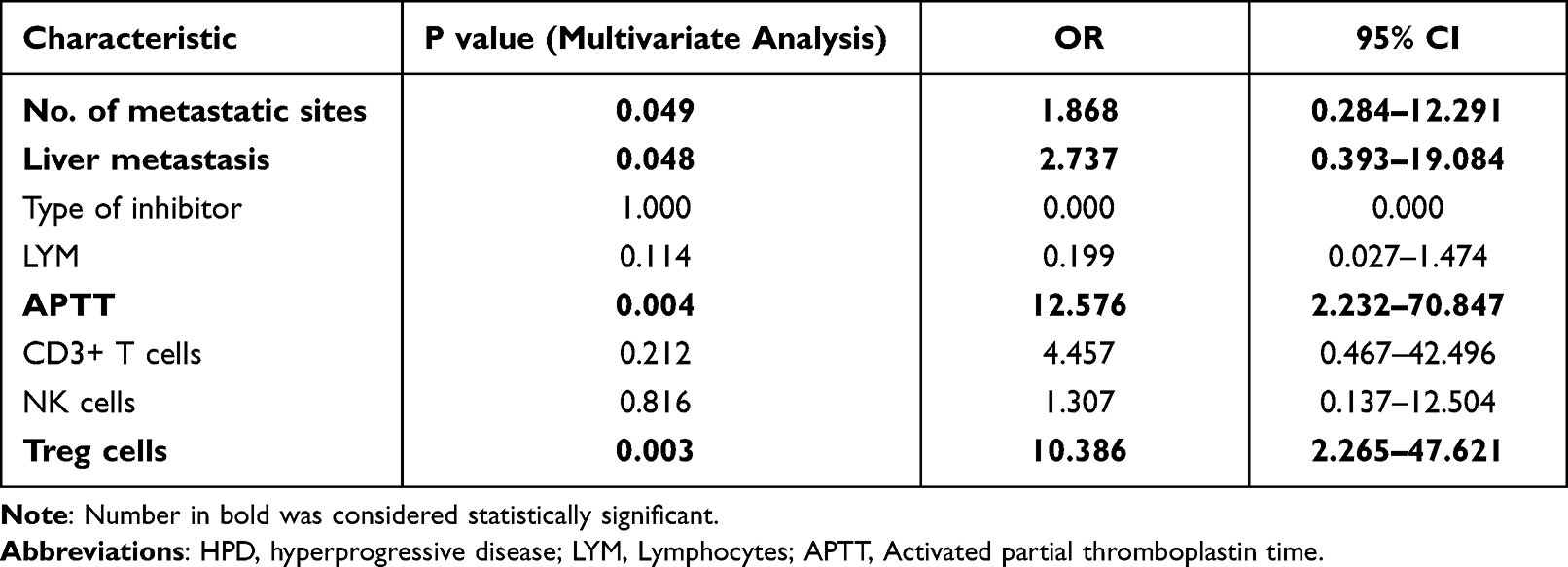 |
Table 3 Multivariate Logistic Regression Analysis Between Features and HPD in Advanced NSCLC |
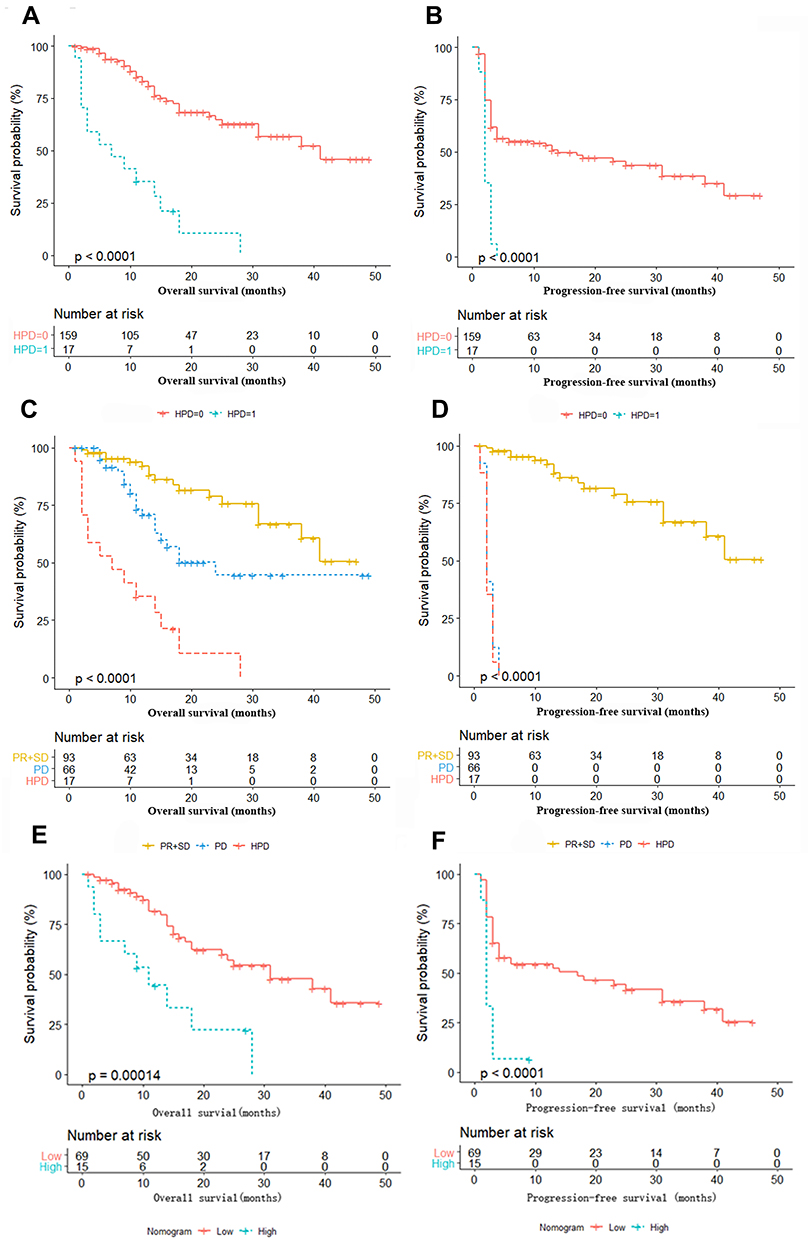 |
Figure 2 Kaplan–Meier survival curves in NSCLC patients according to HPD status, response categories and nomogram. (A) OS according to HPD. (B) PFS according to HPD. (C) OS according to response categories. (D) PFS according to response categories. (E) OS according to the nomogram. (F). PFS according to the nomogram. “HPD=0” indicates patients without HPD, while “HPD=1” indicates patients with HPD. “SD” indicates patients with stable disease, “PR” indicates patients with partial reaction, “PD” indicates patients with progressive disease but no HPD, and “HPD” indicates patients with hyperprogressive disease. “Low” indicates patients in the low-risk group according to the nomogram, while “High” indicates patients in the high-risk group according to the nomogram. |
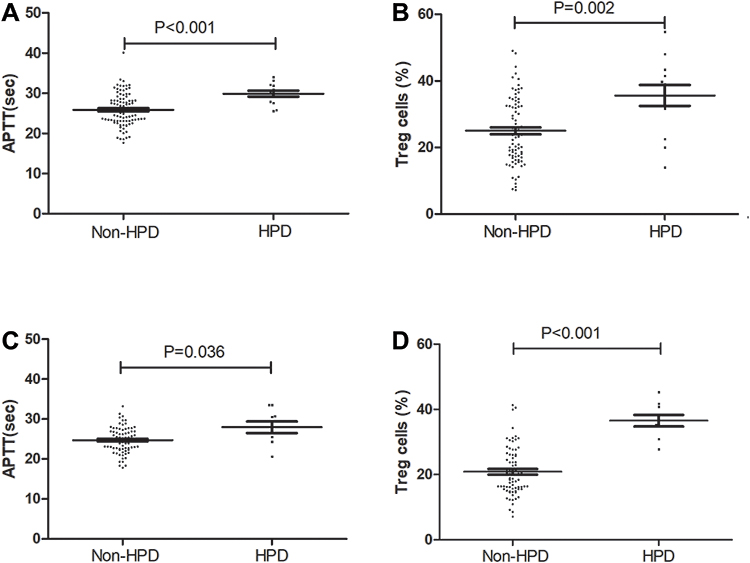 |
Figure 3 Pretherapy levels of APTT and Treg cells between HPD and non-HPD NSCLC patients. (A) The difference in serum levels of APTT in the primary cohort. (B) The difference in the levels of Treg cells in the primary cohort. (C) The difference in serum levels of APTT in the validation cohort. (D) The difference in the levels of Treg cells in the validation cohort. |
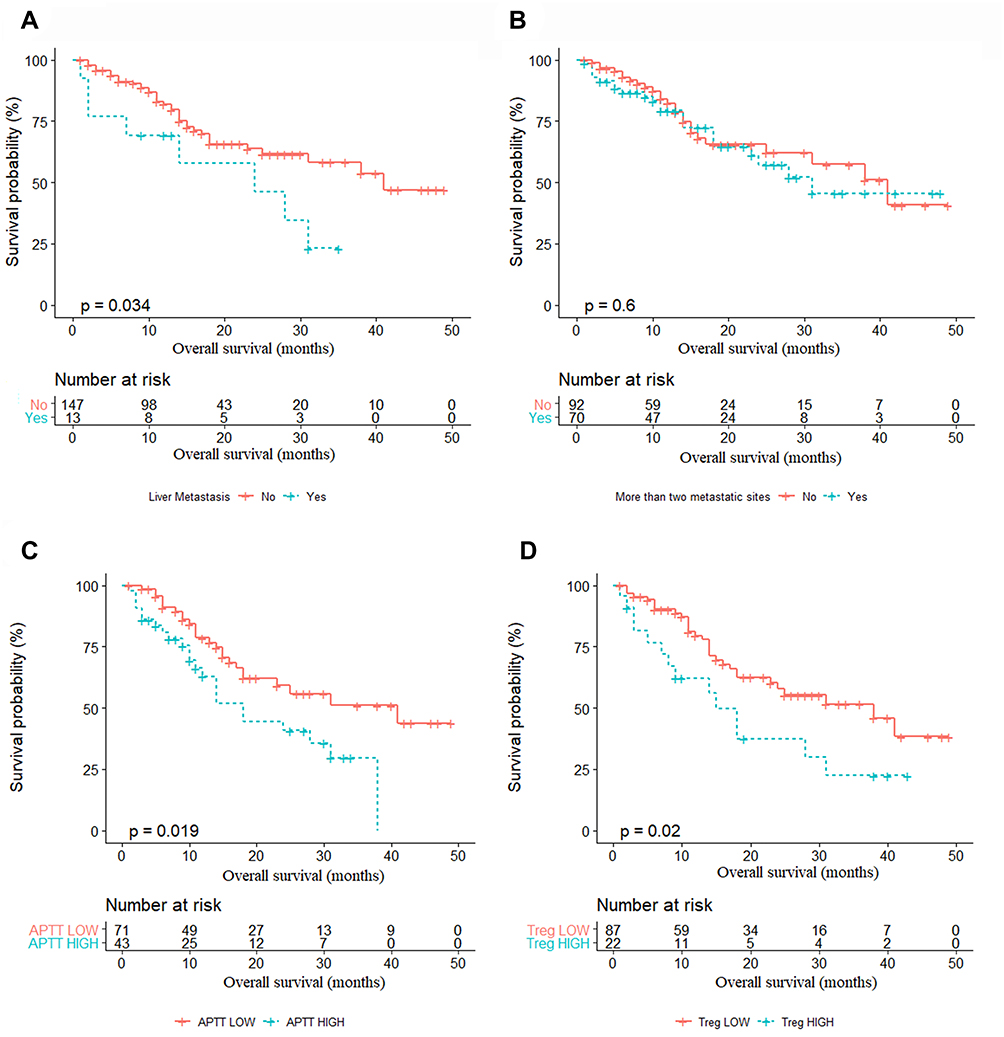 |
Figure 4 Kaplan–Meier survival curves in NSCLC patients according to the factors in the nomogram. (A) OS according to liver metastasis (P<0.05). (B) OS according to more than two metastatic sites (P>0.05). (C) OS according to APTT (P<0.05). (D) OS according to Treg cells (P<0.05). |
Development and Validation of the Prediction Model
In our study, more than two metastatic sites (P<0.05), the presence of liver metastasis (P<0.05), pretreatment APTT (P<0.01) and Treg cells (P<0.01) were the confounding factors that were closely related to HPD according to the logistic regression analysis. To explore whether these factors could predict survival outcomes in advanced NSCLC, we compared the OS between patients in the primary cohort classified by the presence of liver metastasis, more than two metastatic sites, APTT and Treg cells. Intriguingly, patients with liver metastasis, longer APTT, and high levels of Treg cells had shorter OS than the other patients (P=0.034, P=0.019, P=0.020, respectively, Figure 4). A model was constructed based on the above results (Figure 5A). According to the regression coefficients of the model, the “risk score” of HPD was calculated by the formula: “HPD score” = 0.8225× presence of liver metastasis + 0.3954 × more than two metastatic sites + 0.2140 × APTT+0.0873 × Treg cells – 11.2476. The value of the formula was as follows: presence of liver metastasis (categorical variable): Yes: 1/No: 0, more than two metastatic sites (categorical variable): Yes: 1/No: 0, APTT (continuous variable): detection value, Treg cells (continuous variable): detection value. The cutoff point of “HPD score” is −1.37; thus, patients could be divided into two groups by “HPD score” as follows: patients with “HPD score” ≥ −1.37 have a high risk of HPD, while patients with “HPD score” < −1.37 have a low risk of HPD. Discrimination was performed by using a concordance index (C-index) and ROC curve. The C-index for the model was 0.845 in our cohort, with an AUC of 0.830 (95% CI: 0.719–0.950, sensitivity 75.00%, specificity 91.70%). The calibration curve of the nomogram for the probability of HPD demonstrated good agreement between prediction and observation in the primary cohort (Figure 5B and C). The Hosmer–Lemeshow test yielded a nonsignificant statistic (P =0.761), which showed that there was no deviation from the perfect fit.
 |
Figure 5 Development and validation of the prediction nomogram in the primary cohort. (A) Nomogram to predict HPD in patients with ICI therapy. The nomogram is valued to obtain the probability of HPD by adding up the points identified on the points scale for each variable, which included the presence of liver metastasis, more than two metastatic sites, APTT and Treg cells. Each patient has a different score due to different indicator points and is then divided into different risk groups. (B) Calibration curve of our nomogram. (C) The AUC of our nomogram was 0.845 (95% CI: 0.719–0.950, P<0.001). (D) The results of decision curve analysis. Decision curve analysis for the nomogram and other previously reported variables. The gray line represents the assumption that all patients have HPD. The thin black line represents the assumption that no patients have HPD. |
Validation of the Predictive Accuracy of the Nomogram for HPD
In the validation cohort, the C-index for HPD prediction was up to 0.960. The AUC was 0.960 (95% CI: 0.874–0.987), with a sensitivity of 88.70%, specificity of 89.80%, PPV of 89.69%, and NPV of 88.82%. The calibration plot for HPD prediction after anti-PD-1/PD-L1 treatment showed optimal agreement between the prediction by the nomogram and the actual observation (Figure 6A and B).
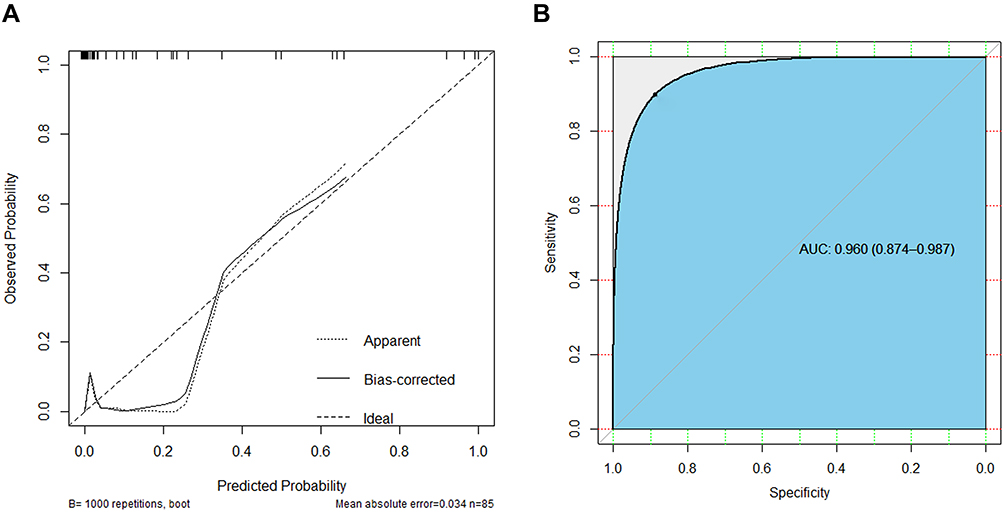 |
Figure 6 Discrimination of the nomogram was performed by using a concordance index (C-index) and ROC curve in the validation cohort. (A) Calibration curve of the nomogram in the validation cohort. (B) The AUC of our nomogram was 0.960 (95% CI: 0.874–0.987, P<0.001) in the validation cohort. |
Clinical Use
The decision curve analysis of the nomogram for HPD is presented in Figure 5D, which shows that if the threshold probability of a patient is > 10%, the developed nomogram in predicting HPD will be more beneficial to patients receiving ICI treatment. According to the nomogram in this range, the net benefit was comparable. Furthermore, the nomogram in predicting HPD is more advantageous than the reported biomarkers (including PD-L1, number of metastases, age≥65) in predicting HPD.15 Based on the nomogram we developed in this study, patients were subdivided into a low-risk group and a high-risk group, which showed good classification for NSCLC patients in the primary cohort. The Kaplan–Meier method was used to estimate OS and PFS, which were compared using the Log rank test. The median OS between the two risk groups was 16 (IQR: 8.5–29) months and 9 (IQR: 3–14) months (p =0.009), and the median PFS between the two risk groups was 6 (IQR: 3–24) months and 2 (IQR: 2–3) months (p<0.001) (Figure 2E–F).
Discussion
In this study, HPD was observed in 9.66% (17/176) of patients with advanced NSCLC during PD-1/PD-L1 inhibitor treatment in the primary cohort, which was assessed by TGR, TGK or TTF. In the validation cohort, there were 10.59% (9/85) HPD patients. Our results for the HPD rate are consistent with previous studies in various cancer types (9–29%).16,22 Ferrara et al17 suggested that HPD occurred in 13.8% (56/406) of advanced NSCLC patients with single-agent chemotherapy according to TGR. Kim et al25 observed that HPD occurred in 20.9% (55/263), 20.5% (54/263), and 37.3% (98/263) of NSCLC patients according to the TGK, TGR, and TTF. Lo et al26 reported that HPD occurred in 25.7% (39/152) of NSCLC patients according to the TGR and TTF. Furthermore, HPD was related to the survival outcome. NSCLC patients with HPD had shorter OS and PFS than those with non-HPD, as previously reported.
At present, there are no credible and easy-to-use biomarkers that could be used to predict HPD. Clinical indicators (including regional recurrence, more than two metastatic sites, age≥65 and high level ANC/CRP), tumor microenvironment biomarkers (including Treg cells, exhausted T cells, M2 tumor-associated macrophages and so on.), and tumor cell biomarkers (including MDM2 amplification and EGFR mutation) were reported to be associated with HPD,15 but not all of the above biomarkers were significantly different between HPD and non-HPD patients, except for two biomarkers (more than two metastatic sites and Treg cells). The difference in HPD prediction biomarkers among various studies is attributed to the following reasons: different types of tumors, various definitions of HPD, different types of anti-PD-1/PD-L1 agents, different regions and populations and so on. The prolongation of APTT may be the manifestation and sensitive indicator of the most common side effects of cancer immunotherapy. Prolonged APTT was observed in advanced cancer patients treated with interleukin-2 (IL-2) alone,27,28 the combination of ex vivo anti-CD3-stimulated T-killer cells and IL-2,29 and the combination of IL-2 and alpha-interferon.30 Furthermore, the patients received treatment with chimeric antigen receptor T-cell (CAR-T) therapies after tisagenlecleucel therapy in 137 patients with relapsed or refractory B-cell acute lymphoblastic leukemia from the ELIANA and ENSIGN trials. Although hypofibrinogenemia was the most clinically significant coagulopathy, some patients also developed prolonged prothrombin time and activated partial thromboplastin time.31 Recently, Patel et al found a more than 10% incidence rate of prolonged APTT in patients treated with immune checkpoint inhibitors (ICIs).32,33 Interestingly, lengthened APTT was also a poor prognostic factor for overall survival (OS) in patients with NSCLC,34 gallbladder cancer,35 multiple myeloma,36 gastric cancer,37 breast cancer,38 and even COVID-1939. Importantly, we are the first to report that APTT is a key biomarker for predicting HPD triggered by ICI therapy. Therefore, further studies are needed to identify better biomarkers for HPD screening before anti-PD-1/PD-L1 therapy.
Individual biomarkers are used to assess only one part of HPD. There is an urgent need to select a tool for HPD prediction that covers different aspects of patients. Hence, we aimed to generate and validate a nomogram to predict HPD and thus guide treatment in NSCLC patients with ICI therapy. In the primary cohort, patients with liver metastasis, more than two metastatic sites, longer APTT and a high level of Treg cells on the baseline examination before ICI therapy had a high risk of HPD; thus, we developed and validated a nomogram for HPD personalized prediction for NSCLC patients. The nomogram performed well in predicting HPD, and formulas of “HPD score” were established with adequate discrimination in the primary cohort (C-index, 0.845; AUC: 0.830, 95% CI: 0.719–0.950, with sensitivity 75.00%, specificity 91.70%). Thus, patients could be divided into two groups by “HPD score” point as −1.37 (patients with “HPD score” ≥ −1.37 have a high risk of HPD, while patients with “HPD score” < −1.37 have a low risk of HPD). In the validation cohort, the AUC was up to 0.960 (95% CI: 0.874–0.987), with a sensitivity of 88.70%, specificity of 89.80%, PPV of 89.69%, and NPV of 88.82%. Furthermore, the Hosmer–Lemeshow test showed that the nomogram had an optimal agreement in HPD prediction with the actual observation. DCA was also used to evaluate the nomogram, which showed that the nomogram had a higher net clinical benefit across a wider range of threshold probabilities than the previous biomarkers in both the primary and validation cohorts. Thus, the nomogram, which is composed of the clinical and hematological biomarkers we already have before ICI therapy, could be used as a more convenient biomarker for HPD prediction and treatment strategy guidance for NSCLC. Based on the nomogram, the first horizontal line represents the point values for each variable in the vertical line, and then all the corresponding points are summed to obtain the total points. Finally, from the total points, we obtained the risk point of HPD.
In this study, we added liver metastasis and more than two metastatic sites to the nomogram with hematological biomarkers that are easily available pretreatment, which has the ability to generate an individual probability of HPD and divide patients into two risk groups. Both physicians and patients could perform a pretreatment individualized prediction of the risk of HPD with this easy-to-use scoring system, which is in line with the current trend toward personalized medicine. The most important and final argument for using a nomogram is based on the need to interpret the individual need for other treatments or care. Patients with high risk scores of HPD should suspend further ICI treatment, and those in good clinical condition should be re-estimated as soon as possible and switched to another potentially effective treatment, such as chemotherapy.
Limitations
There are also some limitations in our study. First, due to rapid deterioration, the existence and definition of HPD still need to be further explored, with the search for valid predictive markers also becoming an urgent problem. To date, no consensus HPD definition has been proposed. The definition is as follows: TTF≤2 months, TGR≥2; and/or TGK≥2. Although some previous reports have concluded that a ΔTGR greater than 100 is the best definition, additional studies on larger groups of patients are necessary to confirm the accuracy and validate this proposed definition.40,41 We should assess HPD as early as possible and quickly switch to new chemotherapy regimens before or at the onset of HPD. Second, various characteristics that were clinically related to OS and PFS were not included in our study. Tumor mutational burden (TMB) was not provided because it was not mandatory and routinely estimated.42 Immune-related adverse events (irAEs) were not included due to the rapid progression time and severity of HPD.43 Third, as a respective analysis, our nomogram was created based on a single data source. The validation of the nomogram in a multicenter study of HPD remains an unmet need. Future studies that prospectively evaluate blood samples of HPD patients before and during treatment will help clarify the mechanism behind this phenomenon and its causal relationship with treatment.
Conclusions
In conclusion, 17 (9.66%) patients and 9 (10.59%) with advanced NSCLC treated with PD-1/PD-L1 inhibitors met the HPD criteria in the primary and validation cohorts, respectively.
HPD was associated with poor survival. Furthermore, we developed and validated a nomogram to predict HPD. The proposed nomogram in this study provided statistically significant discrimination, and it offered a credible, easy-to-use and noninvasive tool for HPD assessment pretreatment of ICI, which could be used to identify and guide reasonable management of patients with HPD.
Acknowledgments
We are grateful to all the participants who made this research possible.
Funding
This project was supported by the National Natural Science Foundation of China (No. 81473233) and the Science and Technology Program of Guangzhou (No. 201504010038, 201604020079, 201601010008).
Disclosure
The authenticity of this article has been validated by uploading the key raw data onto the Research Data Deposit public platform (www.researchdata.org.cn), with the approval RDD number RDDA2020001591. There are no conflicts of interest.
References
1. Topalian SL, Taube JM, Anders RA, Pardoll DM. Mechanism-driven biomarkers to guide immune checkpoint blockade in cancer therapy. Nat Rev Cancer. 2016;16(5):275–287. doi:10.1038/nrc.2016.36
2. Schachter J, Ribas A, Long GV, et al. Pembrolizumab versus ipilimumab for advanced melanoma: final overall survival results of a multicentre, randomised, open-label Phase 3 study (KEYNOTE-006). Lancet. 2017;390(10105):1853–1862. doi:10.1016/S0140-6736(17)31601-X
3. Betof WA, Palmer JS, Shoushtari AN, et al. Long-Term outcomes and responses to retreatment in patients with melanoma treated with PD-1 blockade. J Clin Oncol. 2020;38(15):1655–1663. doi:10.1200/JCO.19.01464
4. Socinski MA, Jotte RM, Cappuzzo F, et al. Atezolizumab for First-Line treatment of metastatic nonsquamous NSCLC. N Engl J Med. 2018;378(24):2288–2301. doi:10.1056/NEJMoa1716948
5. Rittmeyer A, Barlesi F, Waterkamp D, et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet. 2017;389(10066):255–265. doi:10.1016/S0140-6736(16)32517-X
6. Bellmunt J, de Wit R, Vaughn DJ, et al. Pembrolizumab as Second-Line therapy for advanced urothelial carcinoma. N Engl J Med. 2017;376(11):1015–1026. doi:10.1056/NEJMoa1613683
7. Powles T, Duran I, van der Heijden MS, et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): a multicentre, open-label, phase 3 randomised controlled trial. Lancet. 2018;391(10122):748–757. doi:10.1016/S0140-6736(17)33297-X
8. Harrington KJ, Ferris RL, Blumenschein GJ, et al. Nivolumab versus standard, single-agent therapy of investigator’s choice in recurrent or metastatic squamous cell carcinoma of the head and neck (CheckMate 141): health-related quality-of-life results from a randomised, phase 3 trial. Lancet Oncol. 2017;18(8):1104–1115. doi:10.1016/S1470-2045(17)30421-7
9. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30. doi:10.3322/caac.21590
10. Dawe DE, Harlos CH, Juergens RA. Immuno-oncology—the new paradigm of lung cancer treatment. Curr Oncol. 2020;27(Suppl 12):S78–S86. doi:10.3747/co.27.5183
11. Larkin J, Minor D, D’Angelo S, et al. Overall survival in patients with advanced melanoma who received nivolumab versus investigator’s choice chemotherapy in CheckMate 037: a randomized, controlled, Open-Label Phase III trial. J Clin Oncol. 2018;36(4):383–390. doi:10.1200/JCO.2016.71.8023
12. Gray JE, Villegas A, Daniel D, et al. Three-year overall survival with durvalumab after chemoradiotherapy in stage III NSCLC—update from PACIFIC. J Thorac Oncol. 2020;15(2):288–293. doi:10.1016/j.jtho.2019.10.002
13. Chung HC, Piha-Paul SA, Lopez-Martin J, et al. Pembrolizumab after two or more lines of previous therapy in patients with recurrent or metastatic SCLC: results from the KEYNOTE-028 and KEYNOTE-158 studies. J Thorac Oncol. 2020;15(4):618–627. doi:10.1016/j.jtho.2019.12.109
14. Travert C, Barlesi F, Greillier L, Tomasini P. Immune oncology biomarkers in lung cancer: an overview. Curr Oncol Rep. 2020;22(11):107. doi:10.1007/s11912-020-00970-3
15. Wang X, Wang F, Zhong M, Yarden Y, Fu L. The biomarkers of hyperprogressive disease in PD-1/PD-L1 blockage therapy. Mol Cancer. 2020;19(1):81. doi:10.1186/s12943-020-01200-x
16. Champiat S, Dercle L, Ammari S, et al. Hyperprogressive disease is a new pattern of progression in cancer patients treated by Anti-PD-1/PD-L1. Clin Cancer Res. 2017;23(8):1920–1928. doi:10.1158/1078-0432.CCR-16-1741
17. Ferrara R, Mezquita L, Texier M, et al. Hyperprogressive disease in patients with advanced Non-Small cell lung cancer treated with PD-1/PD-L1 inhibitors or with Single-Agent chemotherapy. JAMA Oncol. 2018;4(11):1543–1552. doi:10.1001/jamaoncol.2018.3676
18. Lin Z, Zhang Y, Zhang L. Construction of an integrated prognostic classifier model for predicting the efficacy of immune checkpoint inhibitor therapy in non-small cell lung cancer. Cancer Commun. 2020;40(8):370–373. doi:10.1002/cac2.12070
19. Schwartz LH, Litiere S, de Vries E, et al. RECIST 1.1-Update and clarification: from the RECIST committee. Eur J Cancer. 2016;62:132–137. doi:10.1016/j.ejca.2016.03.081
20. Fang W, Chen Y, Sheng J, et al. Association between PD-L1 expression on tumour-infiltrating lymphocytes and overall survival in patients with gastric cancer. J Cancer. 2017;8(9):1579–1585. doi:10.7150/jca.18729
21. Ferte C, Fernandez M, Hollebecque A, et al. Tumor growth rate is an early indicator of antitumor drug activity in Phase I clinical trials. Clin Cancer Res. 2014;20(1):246–252. doi:10.1158/1078-0432.CCR-13-2098
22. Saada-Bouzid E, Defaucheux C, Karabajakian A, et al. Hyperprogression during anti-PD-1/PD-L1 therapy in patients with recurrent and/or metastatic head and neck squamous cell carcinoma. Ann Oncol. 2017;28(7):1605–1611. doi:10.1093/annonc/mdx178
23. Kato S, Goodman A, Walavalkar V, Barkauskas DA, Sharabi A, Kurzrock R. Hyperprogressors after immunotherapy: analysis of genomic alterations associated with accelerated growth rate. Clin Cancer Res. 2017;23(15):4242–4250. doi:10.1158/1078-0432.CCR-16-3133
24. Wu Q, Xu Y, Zhang KJ, Jiang SM, Zhou Y, Zhao Y. A clinical model for the prediction of acute exacerbation risk in patients with idiopathic pulmonary fibrosis. Biomed Res Int. 2020;2020:8848919. doi:10.1155/2020/8848919
25. Kim CG, Kim KH, Pyo KH, et al. Hyperprogressive disease during PD-1/PD-L1 blockade in patients with non-small-cell lung cancer. Ann Oncol. 2019;30(7):1104–1113. doi:10.1093/annonc/mdz123
26. Lo RG, Moro M, Sommariva M, et al. Antibody-Fc/FcR interaction on macrophages as a mechanism for hyperprogressive disease in non-small cell lung cancer subsequent to PD-1/PD-L1 blockade. Clin Cancer Res. 2019;25(3):989–999. doi:10.1158/1078-0432.CCR-18-1390
27. Locker GJ, Kapiotis S, Veitl M, et al. Activation of endothelium by immunotherapy with interleukin-2 in patients with malignant disorders. Br J Haematol. 1999;105(4):912–919. doi:10.1046/j.1365-2141.1999.01453.x
28. Richard V, Bernier M, Themelin L, Bron D, Sculier JP. Blood coagulation abnormalities during adoptive immunotherapy with interleukin-2 (r-Met Hu IL-2 [ala 125]). Ann Oncol. 1991;2(1):67–68. doi:10.1093/oxfordjournals.annonc.a057827
29. Curti BD, Longo DL, Ochoa AC, et al. Treatment of cancer patients with ex vivo anti-CD3-activated killer cells and interleukin-2. J Clin Oncol. 1993;11(4):652–660. doi:10.1200/JCO.1993.11.4.652
30. Becker JC, Winkler B, Klingert S, Brocker EB. Antiphospholipid syndrome associated with immunotherapy for patients with melanoma. Cancer Am Cancer Soc. 1994;73(6):1621–1624. doi:10.1002/1097-0142(19940315)73:6<1621::aid-cncr2820730613>3.0.co;2-e
31. Buechner J, Grupp SA, Hiramatsu H, et al. Practical guidelines for monitoring and management of coagulopathy following tisagenlecleucel CAR T-cell therapy. Blood Adv. 2021;5(2):593–601. doi:10.1182/bloodadvances.2020002757
32. Tawbi HA, Burgess M, Bolejack V, et al. Pembrolizumab in advanced soft-tissue sarcoma and bone sarcoma (SARC028): a multicentre, two-cohort, single-arm, open-label, Phase 2 trial. Lancet Oncol. 2017;18(11):1493–1501. doi:10.1016/S1470-2045(17)30624-1
33. Kida W, Nakaya M, Ito A, Kozai Y, Bingo M. A case of acquired factor v inhibitor following nivolumab administration. Cureus. 2022;14(1):e21670. doi:10.7759/cureus.21670
34. Abbas M, Kassim SA, Wang ZC, Shi M, Hu Y, Zhu HL. Clinical evaluation of plasma coagulation parameters in patients with advanced-stage non-small cell lung cancer treated with palliative chemotherapy in China. Int J Clin Pract. 2020;74(12):e13619. doi:10.1111/ijcp.13619
35. Shu YJ, Weng H, Bao RF, et al. Clinical and prognostic significance of preoperative plasma hyperfibrinogenemia in gallbladder cancer patients following surgical resection: a retrospective and in vitro study. Bmc Cancer. 2014;14:566. doi:10.1186/1471-2407-14-566
36. Geng C, Yang G, Wang H, Zhang Z, Zhou H, Chen W. The prognostic role of prothrombin time and activated partial thromboplastin time in patients with newly diagnosed multiple myeloma. Biomed Res Int. 2021;2021:6689457. doi:10.1155/2021/6689457
37. Suzuki T, Shimada H, Nanami T, et al. Hyperfibrinogenemia is associated with inflammatory mediators and poor prognosis in patients with gastric cancer. Surg Today. 2016;46(12):1394–1401. doi:10.1007/s00595-016-1339-z
38. Dirix LY, Oeyen S, Buys A, et al. Coagulation/fibrinolysis and circulating tumor cells in patients with advanced breast cancer. Breast Cancer Res Treat. 2022;192(3):583–591. doi:10.1007/s10549-021-06484-1
39. Huang W, Li C, Wang Z, et al. Decreased serum albumin level indicates poor prognosis of COVID-19 patients: hepatic injury analysis from 2,623 hospitalized cases. Sci China Life Sci. 2020;63(11):1678–1687. doi:10.1007/s11427-020-1733-4
40. Kas B, Talbot H, Ferrara R, et al. Clarification of definitions of hyperprogressive disease during immunotherapy for Non-Small cell lung cancer. JAMA Oncol. 2020;6(7):1039–1046. doi:10.1001/jamaoncol.2020.1634
41. Matos I, Martin-Liberal J, Garcia-Ruiz A, et al. Capturing Hyperprogressive disease with immune checkpoint inhibitors using RECIST 1.1 criteria. Clin Cancer Res. 2019. doi:10.1158/1078-0432.CCR-19-2226
42. Klempner SJ, Fabrizio D, Bane S, et al. Tumor mutational burden as a predictive biomarker for response to immune checkpoint inhibitors: a review of current evidence. Oncologist. 2019. doi:10.1634/theoncologist.2019-0244
43. Martins F, Sofiya L, Sykiotis GP, et al. Adverse effects of immune-checkpoint inhibitors: epidemiology, management and surveillance. Nat Rev Clin Oncol. 2019;16(9):563–580. doi:10.1038/s41571-019-0218-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.