")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Prediction of Health Risk Preventative Behavior of Amateur Marathon Runners: A Cross-Sectional Study
Authors Zuo Y , Zhang M, Si Y , Wu X, Ren Z
Received 7 April 2021
Accepted for publication 17 June 2021
Published 12 July 2021 Volume 2021:14 Pages 2929—2944
DOI https://doi.org/10.2147/RMHP.S305937
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Kent Rondeau
Yifan Zuo,1,2 Mu Zhang,2 Yuqi Si,2 Xiaoyuan Wu,3 Zhanbing Ren3
1School of Management, Jinan University, Guangzhou, 510632, People’s Republic of China; 2Shenzhen Tourism College, Jinan University, Shenzhen, 518053, People’s Republic of China; 3Department of Physical Education, Shenzhen University, Shenzhen, 518061, People’s Republic of China
Correspondence: Zhanbing Ren
Department of Physical Education, Shenzhen University, 3688 Nanhai Avenue, Nanshan District, Shenzhen, Guangdong Province, People’s Republic of China
Tel +86755-26534772
Fax +860755-26534772
Email [email protected]
Introduction: Prevention of the health risk of amateur marathon runners is of great significance for the sustainable development of marathon. To reduce the psychological burden of amateur marathon runners and improve the participation experience, the current study used the health belief model to study the relationship among health beliefs, attitude to preventative behavior, self-efficacy, and health values of amateur marathon runners.
Methods: A total of 342 data were collected, and using the PROCESS (analytical procedures developed for mediating and moderating effects tests based on SPSS and SAS). A series of multiple linear regression models were established to study the relationship between variables, and the bootstrap confidence interval was selected to test the mediating and moderating effect.
Results: The results showed that perceived health threat (b = 0.463, p < 0.05), health behavior expectations (b = 0.373, p < 0.001), self-efficacy (b = 0.322, p < 0.001), and behavioral attitudes (b = 0.230, p < 0.001) can be regarded as antecedent variables for predicting preventative behaviors. In addition, the results also show that health behavior expectations, self-efficacy, and behavioral attitudes play chain-mediating role between perceived health threat and preventative behaviors. Health values appear to play a moderating role in the direct/indirect effects of perceived health threat on preventive behavior through a number of mediating variables.
Discussion: This study emphasizes that the amateur marathon runners must improve their health concept and take effective preventive measures before participating in the competition. According to this research, it is the responsibility of the event parties, public health officials and relevant departments of the host city to provide rich health information and risk education to amateur marathon runners. More public service advertisements or educational materials are needed to be placed on runners to enhance their awareness of the necessity and importance of taking preventive measures.
Keywords: health belief model, perceived health threat, health behavior expectation, self-efficacy, behavioral attitude, health values
Introduction
Marathons are a very popular event in the world. However, today’s popular marathons differ from the “classic” marathon. The “classic” marathon race has severe requirements. Participants can participate in the competition only after physical indicators have reached the standard,1 and at present, the popular marathon is primarily geared towards the general public. Compared to the typical marathon events, the mass marathon places more emphasis on entertainment, and the rules of the competition are relatively loose. The participants’ goals are primarily to enhance their physical fitness, enrich their leisure life, emotional wellbeing, and to challenge themselves.2 However, amateur marathon runners need to bear a certain degree of risk and uncertainty in the process of participation, similar to sports injuries during or after physical activity and public health risks.3
As part of the event, health risks are very likely to endanger the health and even life of runners.4 With yearly incidence rates for injury reported to be as high as 90% in those training for marathons,5 as well as the cognitive popularization of diseases such as knee patellar osteochondrosis and friction syndrome. Thus, health risks have become the main concern of amateur marathon runners because of increases in safety awareness.6 A large number of previous studies have examined sports injury and consequences of amateur marathons; however, less attention has been paid to public health risks.7 Due to the characteristics of marathon events such as being large-scale, involving a large number of people, long gathering times, amateur marathon events face more public health risks.8 In particular, during the novel coronavirus disease 2019 (COVID-19) pandemic, amateur runners who participate in marathon events will face greater health risks, which may be due to the lack of continuous exercise during the pandemic period, resulting in deterioration of physical function.9 Alternatively, if they participate in mass gatherings, public health risks are caused by mass migration.10
Previous studies have shown that the health risk management of amateur marathon runners is related to health belief and health risk prevention behaviors.11 The health belief model (HBM) is a health education model that changes individual behavior by intervening in perceptions, attitudes, and beliefs, as well as being the most prominent social behavior model with which a series of health risks can be avoided.12 Specifically, it is the individual’s belief in the perceived susceptibility and severity of the health problems that will be encountered, encouraging people to adopt health protection and preventative behaviors.13 If an individual is afraid of his or her current unhealthy behavior and believes that the benefits of changing the unhealthy behavior are greater than the obstacles, the individual will feel confident and able to change the behavior through long-term efforts.14 Similarly, individuals in sports environments taking measures to protect themselves from exercise-related injuries may depend on their perception of such health threats, such as perceived susceptibility and severity.15 The health risk perception and prevention behaviors of amateur marathon runners may be affected by their health values, especially while experiencing the COVID-19 pandemic, in which people may pay more attention to the importance of health.16 Such a shift can provide a new perspective for the Marathons to improve the experience and satisfaction of participants.
The current study used the HBM to study the relationship among health beliefs, attitude to preventative behavior, self-efficacy, and health values of amateur marathon runners. It attempted to provide useful insights into the public health risk management and event development of marathon events to reduce the psychological burden of amateur marathon runners and improve the participation experience. The results suggested that the most effective way to solve the shortage of public health work in marathon events is to strengthen the amateur marathon runners’ perceived health threats, thereby promoting the production of health risk preventative behaviors; only by making clear the dangers of health risk can participants begin to reduce or even eliminate public health risks in events to the best of their ability.
Related Concepts and Research Hypotheses
Health Risks in Marathons
Researchers have divided the risks of marathon events into amateur runners and professional runners. Amateur runners can be divided into image risk, natural risk, and man-made disaster risk.17 Health risks are included under man-made disaster risks, which includes the risk of injuries and deaths caused by runners who do not understand their physical condition.18 At present, health risks have become the most concerned problem for amateur marathon runners and affect their related behaviors.3 Here, health risk refers to the risk of disease or other health damage (such as knee injury) caused by participating in marathon training and events.5 Marathon is an extreme sport with very long distances that demand high physical stamina. With the “blow-out” development of marathon events, the number of public runners continues to increase, their physical health is uneven, bad running technique and their cognition and prediction of sports risks are insufficient, making it more likely to have sports injuries or even serious sudden deaths during the event.19 Therefore, the importance of research on the health risk of amateur marathon runners is significantly increasing.20
Conceptual Model
Perceived Health Threat
In the HBM, susceptibility and severity of the disease jointly form the perceived health threat.21 Specifically, perceived susceptibility is an individual’s perception of the possibility and probability of a disease and its adverse consequences. The observed variables are generally “whether or not to be ill, the possibility of future disease, the possibility of disease compared with the average person.”22 perceived severity refers to an individual’s perception of the severity of a disease’s adverse effects. The observed variables refer to
worry about the disease, the impact of the disease on daily life, the impact of the disease on interpersonal relationships, and the perception of the severity of the disease.22
At present, there are many perceived health threats related to marathon events, such as sudden cardiac death that can easily arouse widespread attention as to safety risks.
Health Behavior Expectations
In HBM, the recognition of behavioral benefits and the realization or abandonment of behavioral disorders together form health behavior expectation.21 Perceived benefits refer to the individual’s expectation about the benefits brought about by the adoption of health behaviors. These include other’s judgment on whether the risk of disease or the consequences of the disease can be effectively reduced after implementing or giving up a certain behavior, including alleviating the pain and reducing the social impact of the disease. Only when people realize that their actions are effective can they consciously take action. The observed variables include “for the improvement of the disease, early detection of symptoms, and prevention work”.23 Behavioral disorders refer to individuals’ expectations about the resistance instigated by healthy behavior, as well as other’s understanding of the difficulty of taking the action. The observed variables include “time spent, money spent, and life disturbed”.24 In this study, we mainly focused on the perceived benefits of amateur marathon runners.
Self-Efficacy
In the HBM, self-efficacy refers to the individual’s confidence in making changes and adopting healthy behaviors based on their cognition.21 That is to say, a person has a correct evaluation and judgment on his or her behavior ability, and believes that he or she can successfully make an effort and take an action leading to the expected result. The observed variables include “confidence in the improvement of the condition, confidence in maintaining a healthy lifestyle, and the behavior of seeking health information”.24 In previous studies, self-efficacy has been widely used in healthcare, self-management, exercise, and medical issues, diabetes, childhood obesity.21
Attitude to Preventative Behavior
In the Theory of Planned Behavior (TPB), attitude refers to a person’s positive or negative feelings towards the behavior and refers to the psychological disposition formed by the conceptualization of an individual’s evaluation of a particular behavior.25 Attitude can be considered one of the most important factors in emerging behavior and can be subdivided into three components: cognition, emotion, and behavior.26 In previous studies, the attitude has been studied in the context of preventative behavior in a variety of fields, such as medical treatment, lifestyle, and marketing, that are often closely integrated with health behavior.27
Health Risk Preventative Behavior
In TPB, behavior refers to the actual action taken by an individual. It is affected by attitude, subjective norm, perceived behavioral control, and behavioral intentions.28 In HBM, preventative behavior refers to whether people can take preventive measures. According to previous studies, amateur marathon runners display many aspects of health risk preventative behavior, such as improving the physical fitness and well-being, improving self-judgment abilities, treating mild illness and injury, and attaching great importance to pre-event preparations.29
Health Values
Health values are the basic components of the health category, covering the criteria and subjective views of society or individuals on various aspects of health, including physiological, psychological, social, and even ecological values.30 Health value is therefore an important variable in studying people’s participation in health behaviors due to its direct and indirect correlations with health in many studies.31 That is, health values refer to an internal standard and subjective view of the importance of health. It is used to set value goals for the health of the subject and select and implement specific value measures according to their importance to achieve the health of the subject.32 At present, due to the improvement of living conditions, most people are increasingly aware of the importance of physical health, especially after the outbreak of COVID-19, and people should be able to realize the importance of physical health.33 For amateur marathoners, who have different health values, there are some who are overly focused on their personal best, some amateur marathoners are also very conscious of their performance and results. However, the event should promote the idea that fitness is more important than performance.
Model Development, Variables, and Hypotheses
The conceptual model of mediation effect is shown in Figure 1, with relevant hypotheses detailed in the following paragraphs.
 |
Figure 1 Conceptual mediation model and hypotheses. |
In HBM, perceived health threat, health behavior expectation, and self-efficacy are all variables used to evaluate individuals’ health beliefs. The relationship between the three is generally progressive; that is, how people view health and disease. The first is how to recognize the severity and susceptibility of the disease, then understand the effect of preventive measures and the obstacles encountered in taking measures, and finally establish self-confidence in the ability to implement or give up certain behaviors.33 Amateur marathon runners were also the first to recognize the severity and susceptibility of the disease, and to judge the effect of health risk preventative behavior, and affirm the individual’s ability to implement behavior.6 Our hypotheses are therefore as follows:
H1a. Perceived health threat and health behavior expectation are positively correlated. H1b. Perceived health threat and self-efficacy are positively correlated. H2a. Health behavior expectation and self-efficacy are positively correlated.
In TPB, individuals have many beliefs about behavior; however, only a small amount of behavioral beliefs can be acquired in a specific time and environment, and these beliefs are the cognitive and emotional basis of behavioral attitudes, subjective norms, and perceived behavioral control.6 Personal over-influencing behavioral beliefs indirectly affect behavioral attitudes, subjective norms, and perceived behavioral control, and ultimately affect behavioral intentions and behavior.35 For amateur marathon runners, we predict that health beliefs will affect attitudes towards health risk preventative behavior. Therefore, we hypothesize that:
H1c. Perceived health threat and attitude to preventative behavior are positively correlated. H2b. Health behavior expectation and attitude to preventative behavior are positively correlated. H3a. Self-efficacy and attitude to preventative behavior are positively correlated.
Some researchers believe that whether individuals take measures to protect themselves from exercise-related injuries may depend on their perception of the threat of such injuries to health.15 In previous studies, the perceived susceptibility to sports injuries was found to be positively correlated with the length of time of wearing protective equipment.15 Protective equipment commonly used by amateur marathon runners. Such as nipple sticks, patella bands, and intramuscular effect patches. In addition, increased awareness of personal health risks may encourage them to perform appropriate warm-up and stretching exercises.36 At the same time, in the HBM, people will act consciously only when they realize that their actions are effective. Only by having the confidence and will to overcome the obstacles can the relevant actions be completed.34 Amateur marathon runners may therefore take further preventive actions. After having arrived at a correct evaluation and judgment of their behavior ability, corresponding preventive measures will also be taken; meanwhile, attitudes to preventative behavior will eventually affect the behavioral intention and behavior itself. Thus, we hypothesize as follows:
H1d. Perceived health threat and preventative behavior are positively correlated. H2c. Health behavior expectation and preventative behavior are positively correlated. H3b. Self-efficacy and preventative behavior are positively correlated. H4. Attitude to preventative behavior and preventative behavior are positively correlated.
Previous studies have shown significant indirect relationships between health beliefs, attitude to preventative behavior, and preventative behavior in the tourism industry.34 The studies37 above also proposed that perceived risks and benefits are indirectly related to an individual’s food consumption behavior via attitude. Therefore, we predict a direct or indirect relationship between the impact of amateur marathon runners’ health beliefs (perceived health threat, health behavior expectation, and self-efficacy) and attitude on preventative behavior. Thus, we hypothesize that:
H5. Perceived health threat has a direct and indirect positive impact on preventative behavior through health behavior expectation, self-efficacy, and attitude.
In the HBM, individual behavior changes based on an individual’s feeling that a disease or disability can be prevented or avoided, realizing that it can be avoided by taking the recommended measures, and being confident that he or she can successfully change this behavior.34 However, as a behavioral change model of psychology, it does not consider the influence of other factors on people’s behavior, such as health values. Health values are the driving force for individuals to adopt healthy behaviors, which is directly related to the implementation of healthy behaviors.30 Some studies have found a connection between physical activity and health, but due to differences in health values, people have different health values.38 Amateur marathon runners may also have different values, which may similarly lead to low health values of amateur marathon runners despite having a high perceived health threat. Thus, we hypothesize that:
H6a. The indirect relationship between amateur marathon runners’ perceived health threat and health risk preventative behavior through health behavior expectations is moderated by health values. H6b. The indirect relationship between amateur marathon runners’ perceived health threat and health risk preventative behavior through self-efficacy is moderated by health values. H6c. The indirect relationship between amateur marathon runners’ perceived health threat and health risk preventative behavior through attitude is moderated by health values. H6d Direct relationship between amateur marathon runners’ perceived health threat and their health risk preventative behavior is moderated by amateur marathon runners’ level of health values.
Methodology
Sampling and Procedure
This study was conducted in September 7–15 2020. The current study used a survey design to test the hypotheses stated above. Researchers used nonprobability sampling questionnaire survey and, at the same time, used the Internet for distribution (https://www.wjx.cn/). Questionnaires were distributed through social media and consisted of 34 questions. An electronic informed consent form was provided to obtain the participants’ consent at the beginning of the questionnaire. At the same time, participants were informed on the first page of the questionnaire that the survey is anonymous and is for research purposes only. All study procedures were approved by the Ethics Committee of Shenzhen University (Protocol Registration No. PN-2021-006), and that it was conducted in accordance with the Declaration of Helsinki. We collected responses from 395 participants from 29 Chinese provinces. We determined that 53 respondents’ data did not meet the criteria and were removed from further analysis, resulting in 342 collected surveys with a recovery rate of 86.58%. In this study, amateur marathon runners were screened by three subjective questions, (a) whether they were amateur marathon runners, (b) whether they had trained professionally for a long time, and (c) whether they were registered athletes. Information about the respondents’ gender, age, household income, education level, employment status, number of marathon events, and running age were recorded. As shown in Table 1, The majority of the respondents were male (55.6%), aged 18–25 years (62.0%), had a household income of 100,000–200,000 RMB, Chinese yuan (47.7%), held a bachelor’s degree (49.1%), were employed (64.0%), participated in 1–2 marathon events (60.8%) and running age of 1–2 years (35.1%). The number of sample data collected in each region is consistent with the number of marathon events held in each region, with more in the eastern region than in the western region and more in the southern region than in the northern region,39 indicating that the sample is somewhat representative.
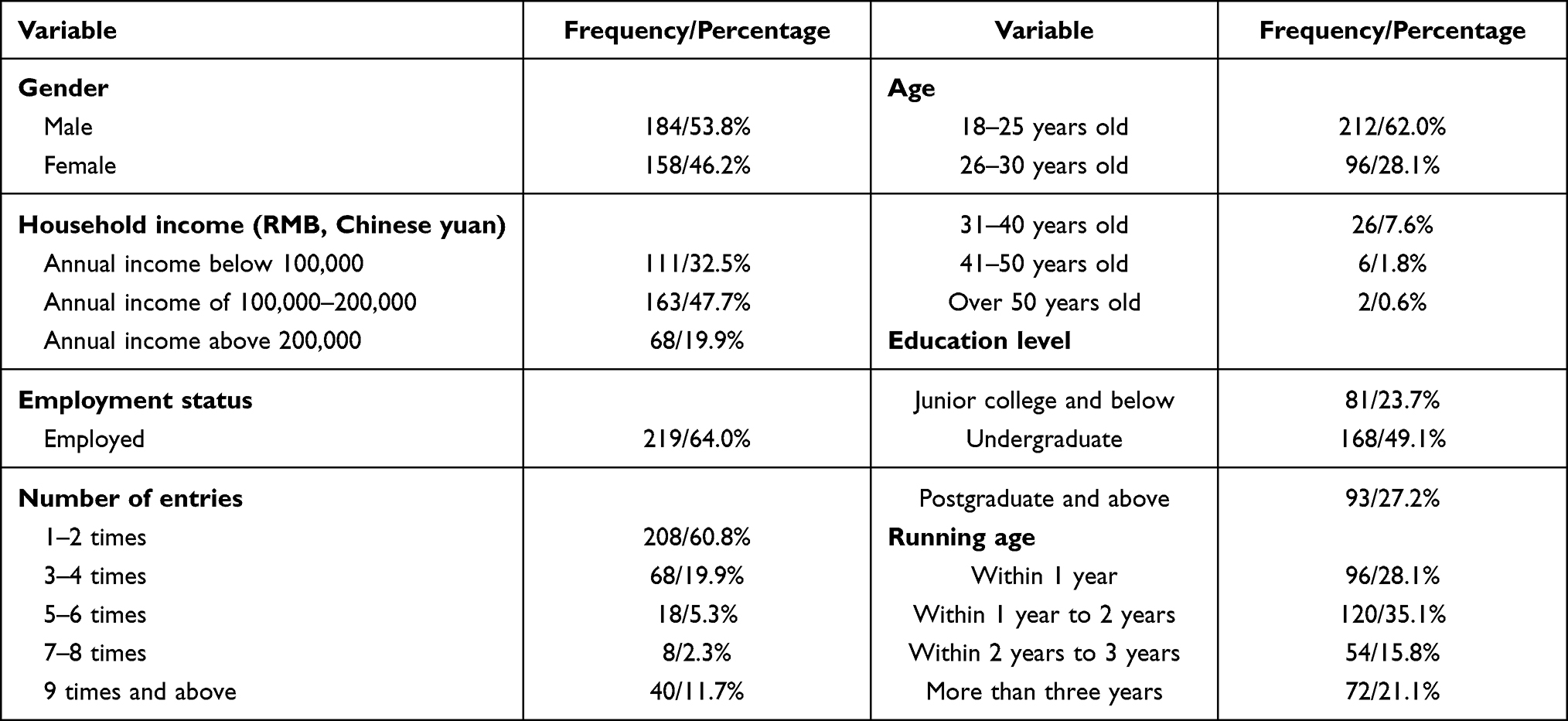 |
Table 1 Descriptive Statistical Results of Demographic Characteristics |
Measures
Based on previous experience, this study developed a scale survey process by standardized procedures. Since the survey was conducted in China, the scale was translated into Chinese by the reverse translation procedure.40 The content validity of the items in the scale for measuring each construct was evaluated by three scholars and two research assistants. They evaluated the content and comprehensibility of the measurement items and then proposed items that required re-editing and improvement to enhance clarity, readability, and content effectiveness. The team also determined whether there was redundancy between items and proposed improvements to the quota entries of each construct. To test the tool, a pilot study was first carried out on a group of 50 social media platform users between the ages of 18 and 50 years old. The purpose of the pre-survey was to try to improve the problem, delete indeterminate or unclear items, refine the survey content and structure, and initially verify the reliability and validity of the scale.
This study is based on the previous health risk of marathon runners3 and the experience of several interviews with amateur marathon runners, combined with the current international COVID-19 pandemic situation4041 and air quality problems.42 We identified three main risks of health: (a) Exercise diseases, such as knee joint injury and muscle strain;5 (b) Respiratory diseases, such as new coronary pneumonia and respiratory disorders (caused by smog);43,44 and (c) Blood circulatory diseases, such as arrhythmia, myocardial fibrosis, and sudden cardiac death.45
According to previous research,28 the measurement of perceived susceptibility and severity in the health risk preventative behavior questionnaires resulted in the determination of the measurement items of the amateur marathon runner’s perceived health threat. Perceived susceptibility was measured by estimating the potential risks of amateur marathon runners participating in the event. The scale includes items “After the outbreak of COVID-19, do you think [insert risk] are likely to happen before you run the marathon?” on a 5-point Likert-type scale ranging from 1(completely impossible) to 5 (very possible) for three different risks. Perceived severity referred to an amateur marathon runner’s perception of the potential impact of health risk on exercise diseases, respiratory diseases, and blood circulatory diseases. The scale includes items “After the epidemic, do you think [insert risk] will affect your participation seriously before you run the marathon?” on a 5-point Likert-type scale ranging from 1(not serious at all) to 5 (very serious) for three different risks. According to scholars’ definitions of health behavior expectation21 and health risk preventative behavior questionnaire,28 the measurement items of health behavior expectation of amateur marathon runners were determined. The scale includes items “What do you think of the effects of prevention measures in reducing [insert risk]?” on a 5-point Likert-type scale ranging from 1(no effect at all) to 5 (very effective) for three different risks.
To measure the self-efficacy, the attitude, and the preventative behavior of amateur marathon runners on preventative behavior, the scale developed by Freimuth46 and revised by Huang28 was adopted. Self-efficacy was measured with the item, “Before running a marathon, how confident are you that you can take precautions to reduce [insert risk]? ” on a 5-point Likert-type scale ranging from 1(not all confident) to 5 (very confident) for three different risks. The attitude of amateur marathon runners to preventative behavior was measured using adjectives such as wise, correct, necessary, effective, and satisfactory. The scale includes items “I think it’s wise to take preventive measures before I run marathon”, “I think it’s right to take precautions before I run marathon”, “It is very necessary for me to take preventive measures ahead of time”, “The precautionary measures I made for this marathon can effectively reduce risks”, and “I am satisfied with the precautions I made for this marathon” on a 5-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree). The preventative behavior was measured with the item, “How well did you prepare for [insert risk] before running a marathon?” on a 5-point Likert-type scale ranging from 1 (no prevention at all) to 5 (very sufficient prevention).
To measure the health values of amateur marathon runners, this study used the health values scale, aimed at measuring the importance that respondents attach to health.47 The scale includes the following items: “If you don’t have your health you don’t have anything”, “There are many things I care about more than my health”, “ Good health is of only minor importance in a happy life”, and “There are few things more important than good health ”on a 5-point Likert-type scale ranging from 1 (strongly disagree) to 5 (strongly agree). More details can be found in the Supplementary Materials.
Data Analysis
Data were analyzed using SPSS 24.0 (SPSS Inc., Chicago, IL, USA, 2019), and the PROCESS plug-in in SPSS was used, PROCESS is a plug-in for mediating and moderating effects in SPSS software, traditional SPSS does mediating and conditioning effects requires stepwise or hierarchical regression, but PROCESS is a one-step.48 We first examined the descriptive statistics of the sample (Mean and Standard Deviation) and then used Cronbach’s alpha to check the internal consistency of each construct. The results showed that the reliability was acceptable Subsequently, the criterion validity of all constructs was verified, and the value of the result corrected item-total correlation (CITC) obtained from the current data was determined. Then, confirmatory factor analysis was used to determine the validity of aggregation, and finally, the score information of each construct was counted. To test the main effect of the model, a series of multiple regression analyses was carried out.
Results
Assessment of the Psychometric Properties of the Measures
Table 2 shows that Cronbach’s alpha values range from 0.759 to 0.879, and all constructs exceed the threshold value of 0.75, indicating that the internal consistency between each scale is acceptable.49 The fitting indexes of the final confirmatory factor analysis model were better, χ2 = 405.028, df = 237, χ2/df = 1.709, RMSEA = 0.046, GFI = 0.915, NFI = 0.939, IFI = 0.974, TLI = 0.969, CFI = 0.974. The CR values for all the constructs ranged from 0.747 to 0.881, which exceeded the threshold value of 0.70.50 The standardized factor load of each item was greater than 0.5 and less than 0.9. Also, the AVE values from all constructs ranged from 0.500 to 0.712, which exceeded the minimum criterion of 0.50.51 This shows that there is a better convergent validity.
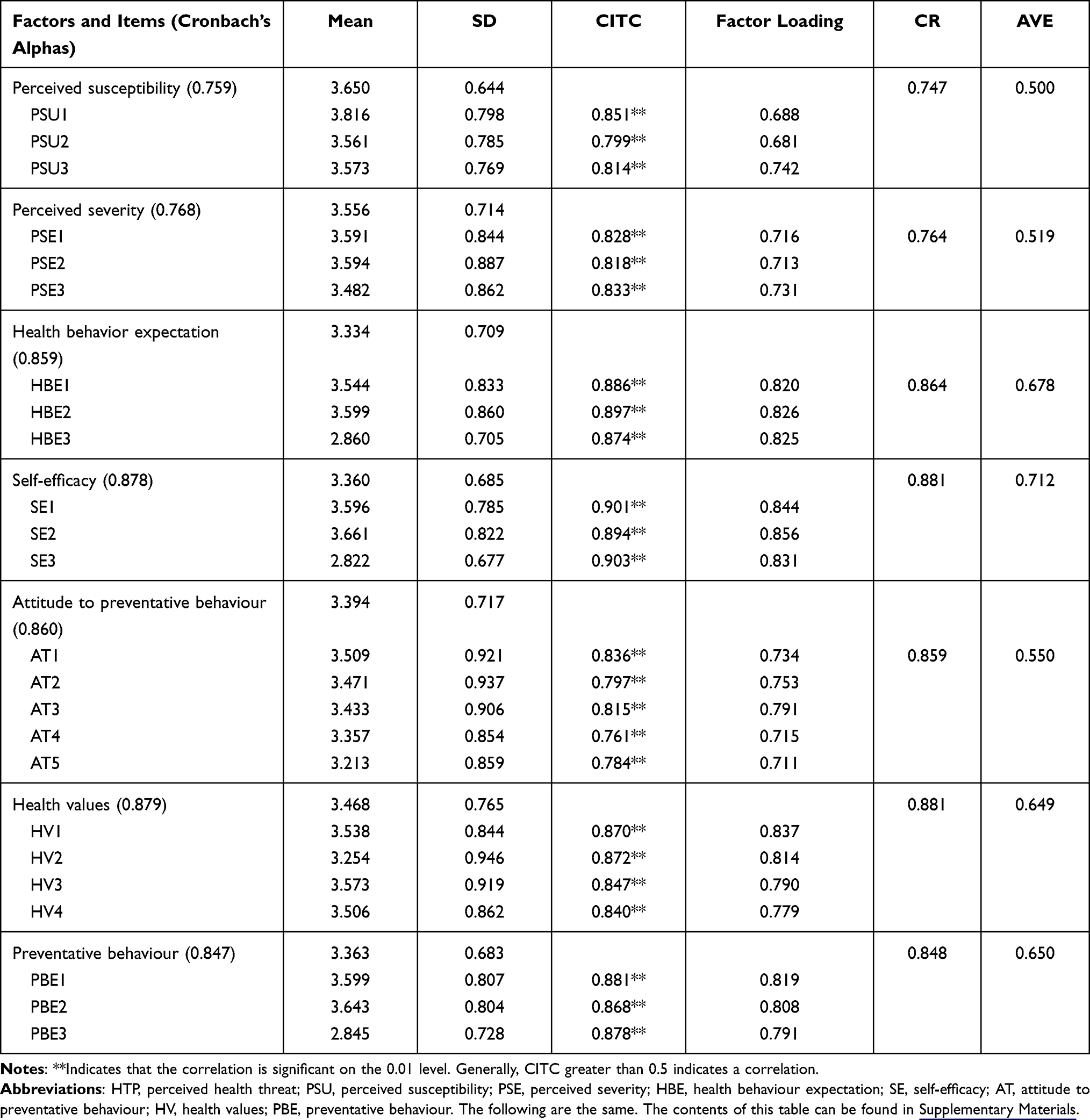 |
Table 2 Reliability Analysis Results of Each Item in the Scale |
Hypothesis Testing
Main Effects
As presented in Table 3, amateur marathon runners’ health behaviour expectation, self-efficacy and attitude significantly predicted their levels of health risk preventative behaviour, after controlling for perceived health threat variable. The results show that there is a significant positive correlation between attitude to preventative behaviour and preventative behaviour (b = 0.230, p <0.001), a significant positive correlation between self-efficacy and preventative behaviour (b = 0.322, p <0.001), and a significant positive correlation between health behaviour expectation and preventative behaviour (b = 0.373, p <0.001). These results provide support for H2c, H3b, and H4.
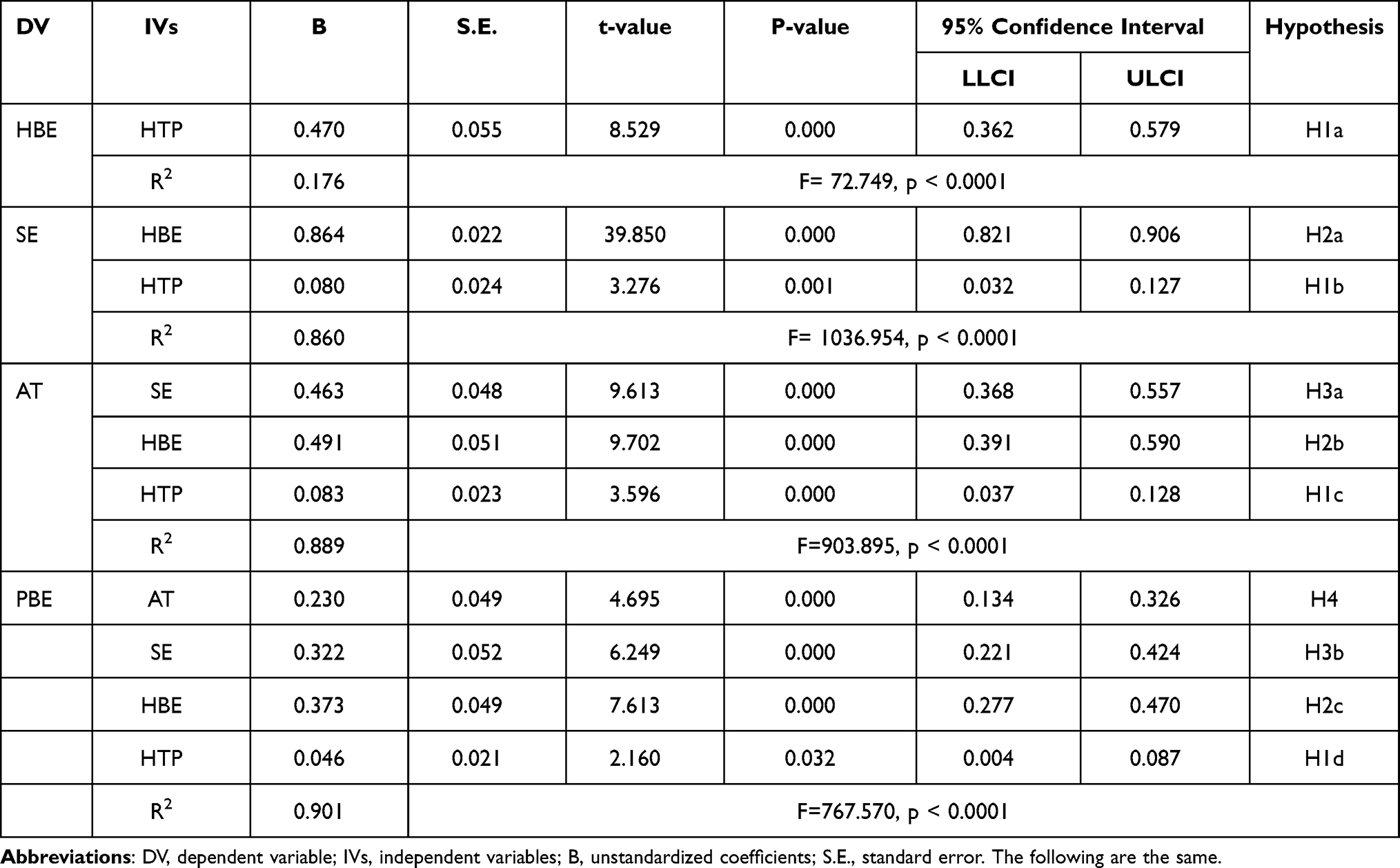 |
Table 3 Regressions Analyses |
Health behaviour expectation significantly influenced the formation of self-efficacy in a positive fashion (b = 0.864, p < 0.001), while it affected their attitude to preventative behaviour in a positive way (b = 0.491, p < 0.001). On the other hand, self-efficacy predicted an increased attitude to preventative behaviour (b = 0.463, p < 0.001). The results provide support for all hypotheses 2a, 2b and 3.
The research results show that the higher the degree of amateur marathon runners’ perceived health threat, the higher the significant increase the health behaviour expectation brings (b = 0.470, p <0.001). It also significantly increased self-efficacy (b = 0.080, p <0.005), and also significantly improved attitude to preventative behaviour (b = 0.083, p <0.001). Similarly, there was also a positive correlation between amateur marathon runners’ perceived health threat and preventative behaviour (b = 0.463, p <0.05). In addition, the results show that amateur marathon runners’ perceived health threat is an important prediction index of their preventative behaviour, thereby controlling for the effects of multiple mediators. Approximately 90.1% of the variance in support was explained by the variables included in the model. These results provide support for H1a, H1b, H1c, and H1d.
Mediation Effects
Relationship between amateur marathon runners’ perceived health threat and preventative behaviour was hypothesized to be partially mediated by health behaviour expectation, self-efficacy and attitude to preventative behaviour. To test the effects of multiple mediators on health risk preventative behaviour, a serial mediation analysis was conducted using Hayes’ Model 6 with a bootstrap method.48 Table 4 lists the results of all paths.
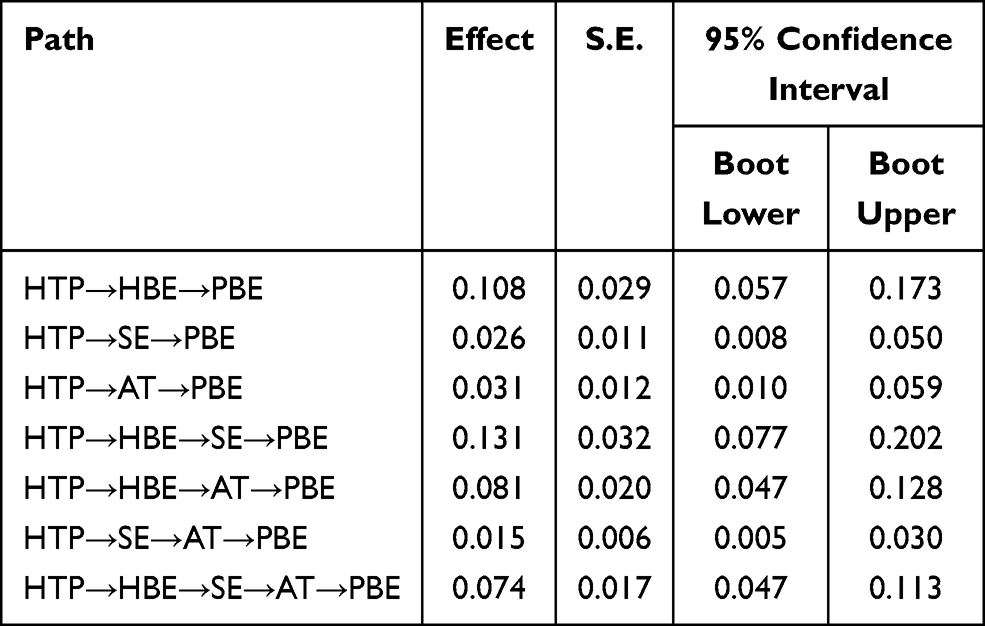 |
Table 4 Regression Coefficients of Serial Mediation Models Estimated Using PROCESS |
Amateur marathon runners’ perceived health threat was found to be a critical predictor of their health risk preventative behaviour with a total effect of 0.465 (95% CI: [0.355, 0.566]). The results also revealed a significant effect of amateur marathon runners’ perceived health threat on their health risk preventative behaviour both directly (b = 0.046, 95% CI: [0.004, 0.087]) and indirectly (b = 0.419, 95% CI: [0.309, 0.479]). Therefore, the existence of a direct relationship between amateur marathon runners’ perceived health threat and their health risk preventative behaviour was confirmed. More importantly, the indirect effect of perceived health threat on preventative behaviour was qualified by significant mediations through health behaviour expectation, self-efficacy and attitude to preventative behaviour paths, with a point estimate of 0.108, (95% CI: [0.057, 0.173]), 0.026 (95% CI: [0.008, 0.050]), and 0.031 (95% CI: [0.010, 0.059]), respectively for health behaviour expectation, self-efficacy and attitude to preventative behaviour.
Since this research model is a chain-type multiple mediation model, involving two or more intermediary variables, there is an interaction relationship between them. Multiple mediating variables show sequential characteristics and form a mediating chain, so it needs to be further explored and verified. Serial mediation through the multiple-process of appraisal was further investigated. The mediating chain through health behaviour expectation and experiencing self-efficacy (b=0.131, 95% CI: [0.077, 0.202]) had a significant impact. The mediating chain through health behaviour expectation and experiencing attitude to preventative behaviour (b=0.081, 95% CI: [0.047, 0.128]) also had a significant impact. Similarly, indirect effect of perceived health threat on preventative behaviour that sequentially went through self-efficacy and attitude to preventative behaviour was significant but trivial (b=0.015, 95% CI: [0.005, 0.030]). However, the indirect effect of perceived health threat on preventative behaviour that sequentially went through health behaviour expectation, self-efficacy and attitude to preventative behaviour had an obvious mediating effect in the mediating chain of the three (b=0.074, 95% CI: [0.047, 0.113]).
All in all, amateur marathon runners who have a high perception of health threat will treat health risk issues in a positive way and carry out effective preventative. More importantly, during this process, the expected effect of amateur marathon runners on health risk preventative behaviour will be greatly improved. At the same time, they will also believe that they can reduce their health risk through preventive measures. Therefore, in addition, there is a correct attitude towards preventive measures. These results provide support for Hypothesis H5.
Moderation Effects
Taken the proposed mediation (H5) and moderation effects (H6a, H6b, H6c, H6d) as a set, these hypotheses suggest that although amateur marathon runners’ health behaviour expectation, self-efficacy and attitude to preventative behaviour mediate the effects of perceived health threat on preventative behaviour, health values moderates those mediation effects. Thus, a moderated mediation analysis (Model 8 in PROCESS) with a bootstrap method was conducted to test the moderating effects of health values.48 The results are shown in Table 5:
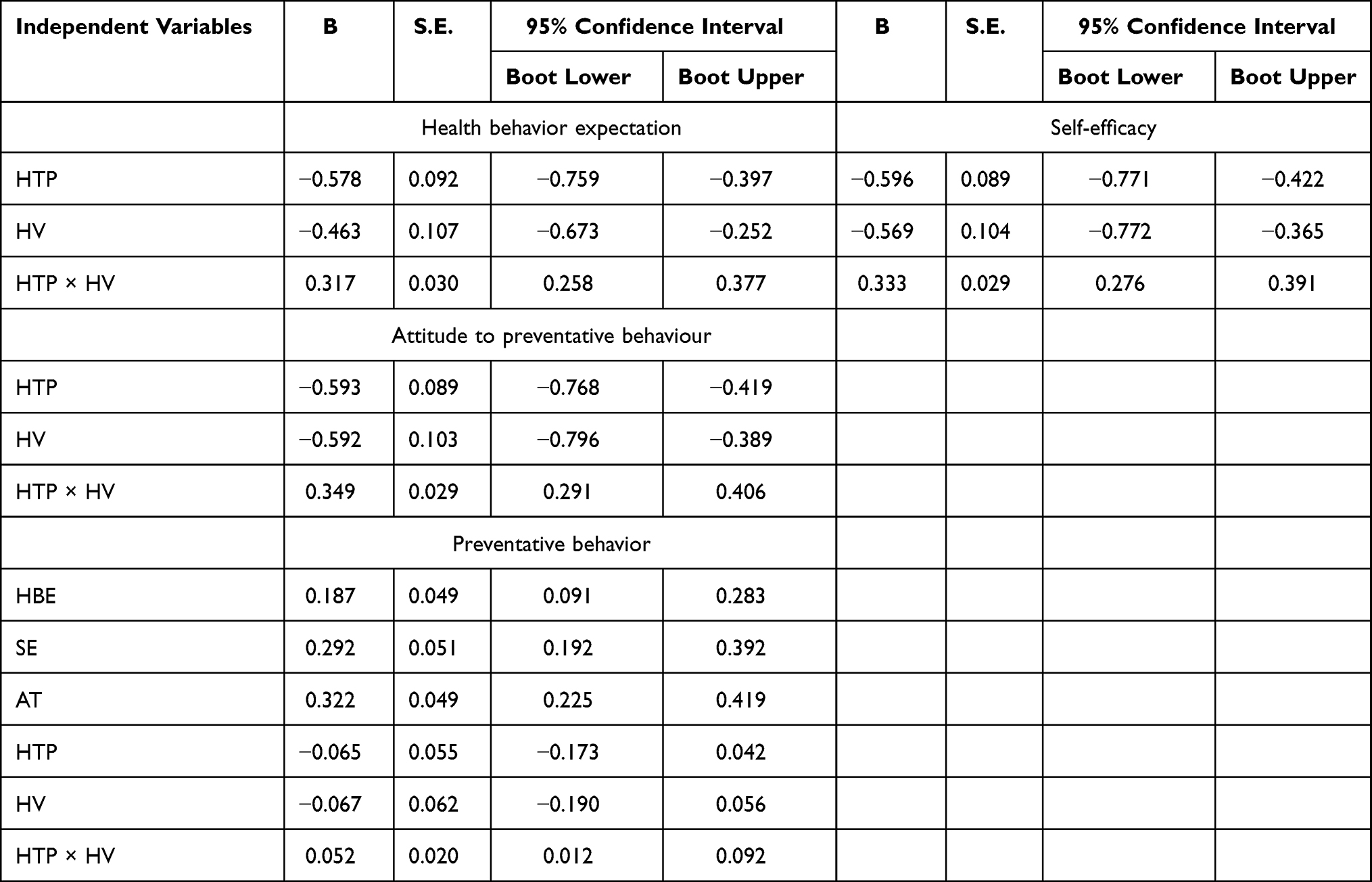 |
Table 5 Regression Coefficients of Moderated Mediation Models Estimated Using PROCESS |
As presented in Table 5. The results revealed that the strength of the relationship between amateur marathon runners’ perceived health threat and their health behaviour expectation, self-efficacy, as well as their attitude to preventative behaviour vary significantly across different levels of health values. Specifically, amateur marathon runners’ health values enhance their health behaviour expectation (b=0.317, 95% CI: [0.258, 0.377]), self-efficacy (b=0.333, 95% CI: [0.276, 0.391]) and attitude to preventative behaviour (b=0.349, 95% CI: [0.291, 0.406]), which weakens the health risk preventative behaviour and shows a positive interaction effect. The findings also provided support for the moderation effect of health values on the indirect relationship between perceived health threat and preventative behaviour, as the interaction with health values was found to be significant (b = 0.052, CI: [0.012, 0.092]). These findings suggest that health values have a moderating effect on the relationship between perceived health threat, health behaviour expectation, self-efficacy, attitude to preventative behaviour, and preventative behaviour.
In order to further reveal how amateur marathon runners’ health values regulate the relationship between perceived health threat, health behaviour expectation, self-efficacy, attitude to preventative behaviour, and preventative behaviour, a simple slope test was conducted on amateur marathon runners’ health values, as shown in Figure 2. The results once again confirmed that the interaction between health values and perceived health threat, as well as the existence and promotion of the relationship had a significant effect on health behaviour expectation (gradient of simple slope = 0.280, t-value = 9.219, p-value = 0.000), self-efficacy (gradient of simple slope = 0.305, t-value = 10.974, p-value = 0.000), attitude to preventative behaviour (gradient of simple slope = 0.349, t-value = 12.559, p-value = 0.000) and preventative behaviour (gradient of simple slope = 0.327, t-value = 4.484, p-value = 0.000). In other words, when the level of amateur marathon runners’ health values is high, the perceived health threat shows a relatively obvious upward trend in health behaviour expectation, self-efficacy and attitude to preventative behaviour. When the level of amateur marathon runners’ health values is low, the effects of perceived health threat on health behaviour expectation, self-efficacy and attitude to preventative behaviour all present a relatively gentle upward trend. Therefore, health values can play a catalytic role in the positive predictive role of amateur marathon runners’ perceived health threat on health behaviour expectation, self-efficacy and attitude to preventative behaviour. In the same way, health values can also play a role in promoting the positive predictive effect of amateur marathon runners’ perceived health threat on their preventative behaviour, but the effect is relatively less obvious.
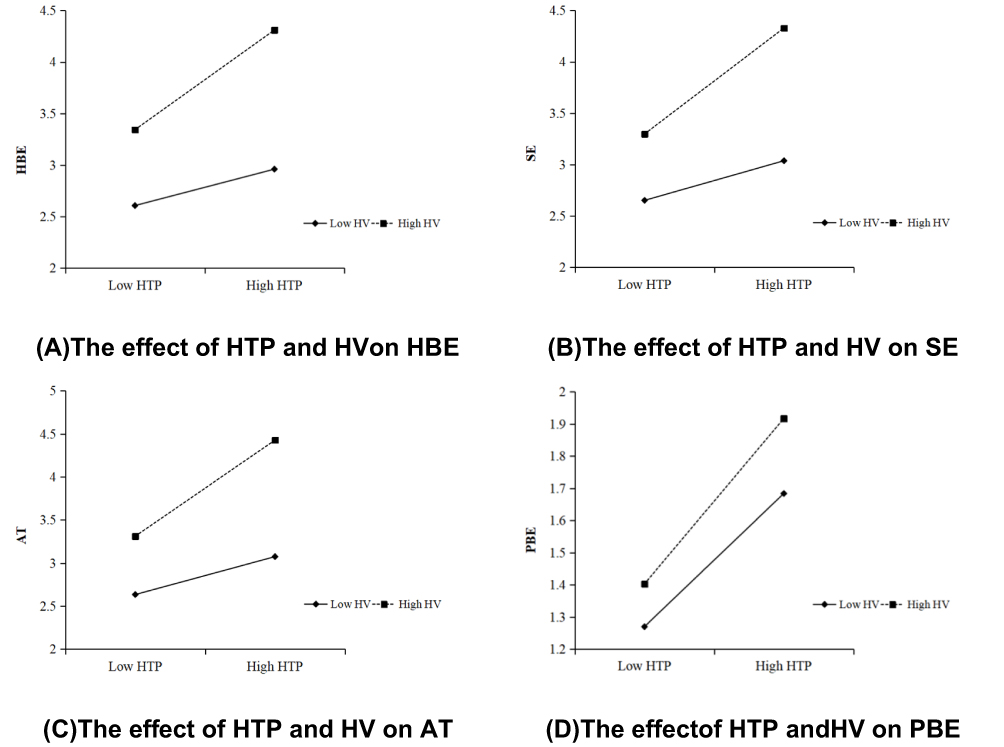 |
Figure 2 Health values simple slope test. The upper figure (A): The Interplay of amateur marathon runners’ perceived health threat, health values and health behaviour expectation; the upper figure (B): The Interplay of amateur marathon runners’ perceived health threat, health values and self-efficacy; the upper figure (C): The Interplay of amateur marathon runners’ perceived health threat, health values and attitude to preventative behaviour; the upper figure (D): The Interplay of amateur marathon runners’ perceived health threat, health values and preventative behaviour. Abbreviations: HTP, perceived health threat; HV, health values; HBE, health behaviour expectation; SE, self-efficacy; AT, attitude to preventative behaviour; PBE, preventative behaviour. |
Discussion
H1a, H1b, and H2a verified the relationship between the three HBM variables: perceived health threat, health behavior expectation, and self-efficacy. The current results show that for amateur marathon runners, it is only after realizing the severity and susceptibility of the three systemic diseases that we can judge the effect of health risk preventive behavior and the individual’s ability to implement behavior.6 Similarly, when individuals think that health risk preventative behavior will be effective, their confidence in the success of individual implementation behavior will also be improved.24
H1c, H2b, and H3a are supported, indicating that health beliefs will affect behavior and attitude, which is an integrated model of TPB and HBM to examine the relationship between health concepts and attitudes toward preventative behavior. As has been confirmed in the study, individuals can directly influence their behavior attitudes by influencing their behavior beliefs, and health beliefs will affect their attitudes towards health risk preventative behavior.5152 The current results show that amateur marathon runners will adjust their attitudes towards health risk preventative behavior because of their perceived threat to three systemic diseases. It also shows that health beliefs are crucial to the attitude and behavior of amateur marathon runners.27
H1d, H2c, H3b, and H4 verified the results of previous studies. As expected, perceived health threat, health behavior expectation, self-efficacy, and attitude to preventative behavior were all positive predictors of preventative behavior. If amateur marathon runners have a more positive attitude towards protective measures, they will be more likely to take preventive measures.28 With the frequent occurrence of sudden death in marathon running in recent years, amateur marathon runners have improved their cognition of three systemic diseases, which will induce amateur marathon running to form health belief, and have a deeper understanding of the health threats of three systemic diseases,12 thus forming the identification of the effect of preventative behavior,53 the confirmation of one’s ability and the adjustment of attitude towards preventative behavior,21 to judge the health risk preventative behavior from all levels.6 All in all, health risk has become the main concern of amateur marathon runners, and risk perception will affect the health risk preventative behavior of amateur marathon runners.
H5 test showed that perceived health threat has direct and indirect positive effects on preventive behavior through health behavior expectation, self-efficacy, and attitude. Once again, the mechanism of action in HBM is verified, and there is a significant indirect relationship between health belief, attitude to preventative behavior, and preventative behavior.28 In terms of the results, the mediating effect of health behavior expectation and the “health behavior expectation—self-efficacy” intermediary chain is the most obvious, which may be due to the close relationship between perceived health threat, health behavior expectation, and self-efficacy, with all belonging to HBM and echoing with H1a, H1b, and H2a. The results show that there is a progressive relationship among the three factors: perceived health threat, health behavior expectation, and self-efficacy, and the order of health behavior expectation should be before self-efficacy. Moreover, although the mediating effect of self-efficacy and “self-efficacy—attitude” intermediary chain is significant, the effect is the worst compared to other intermediary relationships. Therefore, the independence of self-efficacy in HBM is once again verified.23,28
The verification of H6a, b, c, d shows that perceived health threat and preventative behavior of amateur marathon runners are affected by their health values. Judging from the current results, the stimulation of health values on health behavior expectation, self-efficacy, and attitude to preventative behavior by the perceived health threat are obvious. High-level health values can significantly promote the production of preventative behavior, while low-level health values are still positively promoting the production of preventative behavior, but the effect is not obvious. This also validates previous studies that after experiencing the COVID-19 pandemic, people pay more attention to the importance of health, and health values are beneficial to the generation of health beliefs.16 People with high-level health values generally follow healthy behaviors and lifestyles.54 Health values vary from person to person. Amateur marathon runners in different regions have different perceived values in health, which this difference leads to different preventive measures for each runner.38 In addition, this study also found that the moderating effect of health values on preventative behaviour indirectly through health behaviour expectation, self-efficacy and attitude to preventative behaviour was significantly better than that of direct effects. This shows that if amateur marathon runners simply think about the impact of perceived health threat on preventative behaviour without considering other factors, the difference in the role of personal health values will be less obvious. This also indicates that when amateur marathon runners are stimulated by health threat, they will always worry about participating in such gatherings again, and will still encounter the same health threat, and the impact of this perception on behaviour will not be affected by personal health values.55
Conclusion
This study provides empirical evidence that amateur marathon runners’ Perceived Health Threat, Health Behavior Expectation, self-efficacy, and behavioral attitudes while participating in a marathon positively influence their health risk prevention behaviors. This study highlights the importance of health belief education and provides useful insights for risk management and event development for public health in marathons. In addition, this study emphasizes that the amateur marathon runners must improve their health concept and take effective preventive measures before participating in the competition. According to this research, it is the responsibility of the event parties, public health officials and relevant departments of the host city to provide rich health information and risk education to amateur marathon runners. More public service advertisements or educational materials are needed to be placed on runners to enhance their awareness of the necessity and importance of taking preventive measures.
Managerial Implications
When a contestant becomes ill or in danger during the competition, it may bring trouble to the participants, the event parties, and the managers of the sports industry, especially the possibility of a large-scale outbreak of COVID-19 infection.56 Therefore, proper health risk education and management for amateur marathon runners will help to reduce their concerns and bring a better event experience. The competition parties, institutions, and the government have begun to attach importance to the screening of applicants, the popularization of health protection, and the preparation of first aid measures in the competition, while the public has also begun to attach importance to the professional training methods. However, to popularize the health risks and preventive measures related to marathon events, more scholars in the fields of sports management and public health are required to offer insight and empirical evidence.11
To strengthen amateur marathon runners’ awareness of health risks, it is necessary to improve their risk perception levels. For example, the management department should inform the runners who are prone to exercise diseases, respiratory diseases, and blood circulatory diseases through announcements, advertisements, or educational materials about the prevalence and symptoms of these diseases.5 Moreover, health belief education should be strengthened to improve the awareness of the effectiveness of preventive measures, including pre-match adaptive training and pre-match physical and mental preparation can effectively reduce health risks. For example, it is the responsibility of the organizers and relevant experts to convince amateur marathon runners that the risk prevention measures related to running a marathon are reasonable, useful, and effective. Sports management departments and public health experts should also introduce simple and effective protective measures to amateur marathon runners to prevent health risks.
Limitations and Future Research Directions
First, we used the convenience sampling of nonprobability sampling. Although we attempted to expand the geographical area as much as possible, the samples may not have been entirely representative of the population under study, leading to statistical sample or selection bias. Secondly, this study is limited to the inclusion of Chinese participants only, requiring more cross-cultural and international samples to validate the findings.
Finally, the current research mainly focused on health beliefs, attitudes, and preventative behavior. It is not clear whether there is a causal relationship between the perception of obstacles in HBM and behavioral intention, subjective norms, and perceived behavior control in TBP. Future research should address these limitations and establish a more comprehensive model to analyze the risk prevention behavior and competition behavior of amateur marathon runners. Moreover, the health risk prevention behavior prediction model of amateur marathon runners in this study was as comprehensive as possible, but may not have considered all possible risks relevant to marathon-running. For example, skin disease, which is a mild disease risk, makes it difficult for runners to determine whether or not a lesion has occurred.
Our research shows that the health risk preventative behavior prediction model can be applied to psychosocial problems related to amateur marathon runners, and it would be highly fruitful to extend this model to other amateur sports events to determine applicability and wider relevance.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from the Ethics Committee of Shenzhen University (Protocol Registration No. PN-2021-006) and electronic informed consent was obtained from participants by asking them to check on an “I agree to participate button” before having access to the questionnaire. All participants were informed about the purpose of the study, and that it was conducted in accordance with the Declaration of Helsinki. No potential risk had been expected for the study participants.
Acknowledgments
I would like to thank the Management School of Jinan University and the Sports Department of Shenzhen University for their Research Platform, and thank the teachers for their support.
Funding
This research was funded by The National Social Science Fund of China (18BTY033).
Disclosure
No potential conflicts of interest was reported by the authors.
References
1. Noakes TD. Hydration in the marathon. Sports Med. 2007;37(4–5):463–466. doi:10.2165/00007256-200737040-00050
2. Perényi S. The popularisation and expansion of amateur running culture. In: J. Scheerder, K. Breedveld, & J. Borgers (Eds.), Running Across Europe: The Rise and Size of One of the Largest Sport Markets. Basingstoke: Palgrave Macmillan. 2015:163–186.
3. Satterthwaite P, Norton R, Larmer P, Robinson E. Risk factors for injuries and other health problems sustained in a marathon. Br J Sport Med. 1999;33(1):22–26. doi:10.1136/bjsm.33.1.22
4. Hulme A, Nielsen RO, Timpka T, Verhagen E, Finch C. Risk and protective factors for middle-and long-distance running-related injury. Sports Med. 2017;47(5):869–886. doi:10.1007/s40279-016-0636-4
5. Fredericson M, Misra AK. Epidemiology and aetiology of marathon running injuries. Sports Med. 2007;37(4–5):437–439. doi:10.2165/00007256-200737040-00043
6. Stephan Y, Deroche T, Brewer BW, Caudroit J, Le Scanff C. Predictors of perceived susceptibility to sport‐related injury among competitive runners: the role of previous experience, neuroticism, and passion for running. Appl Psychol. 2009;58(4):672–687. doi:10.1111/j.1464-0597.2008.00373.x
7. Van der Worp MP, Ten Haaf DS, van Cingel R, de Wijer A, Nijhuis-van Der Sanden MW, Staal JB. Injuries in runners; a systematic review on risk factors and sex differences. PLoS One. 2015;10(2):e0114937. doi:10.1371/journal.pone.0114937
8. Robson-Ansley P, Howatson G, Tallent J, et al. Prevalence of allergy and upper respiratory tract symptoms in runners of the London marathon. Med Sci Sports Exerc. 2012;44(6):999–1004. doi:10.1249/MSS.0b013e318243253d
9. Lippi G, Henry BM, Sanchis-Gomar F. Physical inactivity and cardiovascular disease at the time of coronavirus disease 2019 (COVID-19). Eur J Prev Cardiol. 2020:2047487320916823.
10. Ebrahim SH, Memish ZA. COVID-19–the role of mass gatherings. Travel Med Infect Dis. 2020;34:101617. doi:10.1016/j.tmaid.2020.101617
11. Burkule N. Marathon running for amateurs: benefits and risks. J Clin Prev Cardiol. 2016;5(4):113. doi:10.4103/2250-3528.192681
12. Janz NK, Becker MH. The health belief model: a decade later. Health Educ Q. 1984;11(1):1–47. doi:10.1177/109019818401100101
13. Aiken LS, Gerend MA, Jackson KM. Perceived Risk and Health Protective Behavior: Cancer Screening and Cancer Prevention Handbook of Health Psychology. Lawrence Erlbaum Associates; 2001:727–746.
14. Shojaei F, Asemi S, Najaf YA, Hosseini F. Self-care behaviors in patients with heart failure. Payesh Journal. 2009;8:361–9.
15. Williams-Avery RM, Mackinnon DP. Injuries and use of protective equipment among college in-line skaters. Accid Anal Prev. 1996;28(6):779–784. doi:10.1016/S0001-4575(96)00040-1
16. Wray A, Fleming J, Gilliland J. The public realm during public health emergencies: exploring local level responses to the COVID-19 pandemic. Cities Health. 2020;1–4. doi:10.1080/23748834.2020.1790260
17. Hall SA, Manning RD, Keiper M, Jenny SE, Allen B. Stakeholders’ perception of critical risks and challenges hosting marathon events: an Exploratory Study. J Contemp Athl. 2019;13(1):11.
18. Xu W, Xie J. A study on risk management of International Marathon Race in Xiamen. J Beijing Sport Univ. 2010;2.
19. Maron BJ, Poliac LC, Roberts WO. Risk for sudden cardiac death associated with marathon running. J Am Coll Cardiol. 1996;28(2):428–431. doi:10.1016/0735-1097(96)00137-4
20. Chalabaev A, Radel R, Ben Mahmoud I, Massiera B, Deroche T, D’Arripe Longueville F. Is motivation for marathon a protective factor or a risk factor of injury? Scand J Med Sci Sport. 2017;27(12):2040–2047. doi:10.1111/sms.12807
21. Tarkang EE, Zotor FB. Application of the health belief model (HBM) in HIV prevention: a literature review. Cent Afr J Public Health. 2015;1(1):1–8.
22. Lo SWS, Chair SY, Lee FK. Factors associated with health-promoting behavior of people with or at high risk of metabolic syndrome: based on the health belief model. Appl Nurs Res. 2015;28(2):197–201. doi:10.1016/j.apnr.2014.11.001
23. Champion VL, Scott CR. Reliability and validity of breast cancer screening belief scales in African American women. Nurs Res. 1997;46(6):331–337. doi:10.1097/00006199-199711000-00006
24. Jacobs LA. Health beliefs of first-degree relatives of individuals with colorectal cancer and participation in health maintenance visits: a population-based survey. Cancer Nurs. 2002;25(4):251–265. doi:10.1097/00002820-200208000-00001
25. Mathieson K. Predicting user intentions: comparing the technology acceptance model with the theory of planned behavior. Inform Syst Res. 1991;2(3):173–191. doi:10.1287/isre.2.3.173
26. Hogg MA, Vaughan GM. Social Psychology: An Introduction. Harvester Wheatsheaf; 1995.
27. Duarte AF, Nagore E, Silva JN, Picoto A, Pereira AC, Correia OJ. Sun protection behaviour and skin cancer literacy among outdoor runners. Eur J Dermatol. 2018;28(6):803–808. doi:10.1684/ejd.2018.3450
28. Huang X, Dai S, Xu H. Predicting tourists’ health risk preventative behaviour and travelling satisfaction in Tibet: combining the theory of planned behaviour and health belief model. Tour Manag Perspect. 2020;33:100589. doi:10.1016/j.tmp.2019.100589
29. Hollman H, Ezzat A, Esculier J, Gustafson P, Scott A. Effects of tailored advice on injury prevention knowledge and behaviours in runners: secondary analysis from a randomised controlled trial. Phys Ther Sport. 2019;37:164–170. doi:10.1016/j.ptsp.2019.04.003
30. Stapleton A, O Connor M, Feerick E, Kerr J, McHugh L. Testing the relationship between health values consistent living and health-related behavior. J Context Behav Sci. 2020;17:17–22. doi:10.1016/j.jcbs.2020.05.002
31. Brassai L, Piko B, Steger MF. A reason to stay healthy: the role of meaning in life in relation to physical activity and healthy eating among adolescents. J Health Psychol. 2015;20(5):473–482. doi:10.1177/1359105315576604
32. Bergin AE. Values and religious issues in psychotherapy and mental health. Am Psychol. 1991;46(4):394. doi:10.1037/0003-066X.46.4.394
33. Maugeri G, Castrogiovanni P, Battaglia G, et al. The impact of physical activity on psychological health during Covid-19 pandemic in Italy. Heliyon. 2020;6(6):e04315. doi:10.1016/j.heliyon.2020.e04315
34. Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the health belief model. Health Educ Q. 1988;15(2):175–183. doi:10.1177/109019818801500203
35. McMillan B, Conner M. Using the theory of planned behaviour to understand alcohol and tobacco use in students. Psychol Health Med. 2003;8(3):317–328. doi:10.1080/1354850031000135759
36. Wedderkopp N, Kaltoft M, Lundgaard B, Rosendahl M, Froberg K. Prevention of injuries in young female players in European team handball. A prospective intervention study. Scand J Med Sci Sport. 1999;9(1):41–47. doi:10.1111/j.1600-0838.1999.tb00205.x
37. Zhang H, Li L, Yang Y, Zhang J. Why do domestic tourists choose to consume local food? The differential and non-monotonic moderating effects of subjective knowledge. J Destin Mark Manag. 2018;10:68–77.
38. Lera-López F, Marco R. Sports participation, physical activity, and health in the European regions. J Sport Sci. 2018;36(15):1784–1791. doi:10.1080/02640414.2017.1418810
39. Zuo Y, Zou L, Zhang M, et al. The temporal and spatial evolution of marathons in China from 2010 to 2018. Int J Environ Res Public Health, 2019, 16(24): 5046. https://doi.org/10.3390/ijerph16245046
40. Brislin RW. Back-translation for cross-cultural research. J Cross Cult Psychol. 1970;1(3):185–216. doi:10.1177/135910457000100301
41. Hall G, Laddu DR, Phillips SA, Lavie CJ, Arena R. A tale of two pandemics: how will COVID-19 and global trends in physical inactivity and sedentary behavior affect one another? Prog Cardiovasc Dis. 2020.
42. Lelieveld J, Evans JS, Fnais M, Giannadaki D, Pozzer A. The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature. 2015;525(7569):367–371. doi:10.1038/nature15371
43. Nguyen TV. Air pollution: a largely neglected risk factor for osteoporosis. Lancet Planet Health. 2017;1(8):e311–e312. doi:10.1016/S2542-5196(17)30143-2
44. Ren Z, Zuo Y, Ma Y, et al. The natural environmental factors influencing the spatial distribution of marathon event: a Case Study from China. Int J Environ Res Public Health. 2020;17(7):2238. doi:10.3390/ijerph17072238
45. Predel H. Marathon run: cardiovascular adaptation and cardiovascular risk. Eur Heart J. 2014;35(44):3091–3098. doi:10.1093/eurheartj/eht502
46. Freimuth VS, Hovick SR. Cognitive and emotional health risk perceptions among people living in poverty. J Health Commun. 2012;17(3):303–318. doi:10.1080/10810730.2011.626505
47. Lau RR, Hartman KA, Ware JE. Health as a value: methodological and theoretical considerations. Health Psychol. 1986;5(1):25–43. doi:10.1037/0278-6133.5.1.25
48. Hayes AF. PROCESS: a versatile computational tool for observed variable mediation, moderation, and conditional process modeling; 2012. Available online: https://www.afhayes.com/public/process2012.pdf. Accessed 15 October, 2020.
49. Christmann A, Van Aelst S. Robust estimation of Cronbach’s alpha. J Multivariate Anal. 2006;97(7):1660–1674. doi:10.1016/j.jmva.2005.05.012
50. Hair JF, Anderson RE, Babin BJ, Black WC. Multivariate Data Analysis: A Global Perspective. Vol. 7. Upper Saddle River, NJ: Pearson; 2010.
51. Fornell C, Larcker DF. Structural Equation Models with Unobservable Variables and Measurement Error: Algebra and Statistics. Los Angeles, CA: Sage Publications Sage CA; 1981.
52. Fishbein M, Ajzen I. Belief, attitude, intention, and behavior: an introduction to theory and research. Philosophy and Rhetoric. 1977;10(2):177–188.
53. Bailey RR. Self-efficacy, self-regulation, social support, and outcomes expectations for daily physical activity in adults with chronic stroke: a descriptive, exploratory study. Occup Ther Health Care. 2019;33(2):129–141. doi:10.1080/07380577.2018.1558326
54. Quah SR. The health belief model and preventive health behaviour in Singapore. Soc Sci Med. 1985;21(3):351–363. doi:10.1016/0277-9536(85)90112-1
55. Day SM, Thompson PD. Cardiac risks associated with marathon running. Sports Health. 2010;2(4):301–306. doi:10.1177/1941738110373066
56. Carmody S, Murray A, Borodina M, Gouttebarge V, Massey A. When Can Professional Sport Recommence Safely During the COVID-19 Pandemic? Risk Assessment and Factors to Consider. BMJ Publishing Group Ltd and British Association of Sport and Exercise Medicine; 2020.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.