")
Back to Journals » International Journal of Women's Health » Volume 13
Precancerous Cervical Lesions Among HIV-Infected Women Attending HIV Care and Treatment Clinics in Southwest Ethiopia: A Cross-Sectional Study
Authors Lemu LG , Woldu BF, Eshetu Teke N, Bogale ND, Wondimenew EA
Received 1 December 2020
Accepted for publication 4 February 2021
Published 3 March 2021 Volume 2021:13 Pages 297—303
DOI https://doi.org/10.2147/IJWH.S295137
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Lidiya Gutema Lemu,1 Biruktawit Fekade Woldu,2 Natnael Eshetu Teke,3 Nardos Delelegn Bogale,1 Ermias Ayalew Wondimenew4
1Department of Midwifery, College of Health Science, Mizan Tepi University, Mizan-Aman, Ethiopia; 2Department of Midwifery, College of Medicine and Health Science, Wachemo University, Hossana, Ethiopia; 3Department of Midwifery, College of Medicine and Health Science, Wolkite University, Wolkite, Ethiopia; 4Department of Nursing, College of Health Science, Mizan Tepi University, Mizan-Aman, Ethiopia
Correspondence: Lidiya Gutema Lemu
Mizan Tepi University, Mizan-Aman, Ethiopia
Email [email protected]
Background: Despite being one of the few cancers that can be prevented with simple testing, cervical cancer is the fourth most common cancer in women. HIV-positive women showed a median three-fold higher incidence of cervical lesions.
Aim: This study aims to assess the prevalence and factors associated with precancerous cervical lesions among HIV-infected women attending care and treatment clinic in selected hospitals of Southwestern Ethiopia.
Methods: Institution-based cross-sectional study was conducted from February 1 to July 30, 2018. A systematic random sampling technique was employed to select 454 HIV-infected women. Pretested interviewer-administered questionnaire and medical record review were used for data collection. Visual inspection with Acetic acid was done for participants to detect precancerous cervical lesions. Data were analyzed by SPSS version 20. Binary and multiple logistic regression analyses were done. The presence and strength of association were determined using AOR with its 95% CI. Variables with a P value of less than 0.05 were considered as statistically significant.
Results: The prevalence of precancerous cervical lesion was 18.7% [95% CI; (15.1– 22.4%)]. Currently, not being on highly active antiretroviral treatment [AOR= 2.31, 95% CI: 1.23– 4.39], age (20– 29 years) [AOR= 0.185, 95% CI: 0.036,0.939], has no history of sexually transmitted infection [AOR=0.026, 95% CI: 0.006– 0.116], has no history of genital wart [AOR= 0.261, 95% CI: 0.073– 0.934] and having one lifetime sexual partner [AOR=0.133, 95% CI: 0.024– 0.726] were found to be significantly associated with precancerous cervical lesion.
Conclusion: The prevalence of Precancerous Cervical lesion was found to be high in this study. Expansion of screening services and undertaking preventive measures against sexually transmitted infection need to be emphasized.
Keywords: precancerous cervical lesion, HIV positive, prevalence, factors, Ethiopia
Introduction
In 2018, cervical cancer was the fourth most common cancer in women and the ninth overall, with an estimated 569,847 new cases. There were an estimated 311,365 deaths from cervical cancer worldwide. Nine out of ten (90%) cervical cancer deaths occur in low- and middle-income countries.1 This can be explained by a lack of access to effective screening services that facilitate early detection and treatment.2 In Ethiopia, cervical cancer was the second leading cancer diagnosis among adult women, with an estimated 6,294 new cases and 4,844 deaths annually.3
Despite being one of the few cancers that can be prevented with simple testing, cervical cancer is affecting women in the prime of their lives, causing suffering and death in a critically important segment of the world’s population.4 In urban populations at increased risk for both diseases, cervical cancer is a crucial Acquired Immuno Deficiency Syndrome (AIDS)-defining illness and maybe the most common AIDS-related malignancy in women.5 Women infected with the Human Immunodeficiency Virus (HIV) showed a median three-fold higher incidence of cervical lesions than uninfected women.6 Different studies in Africa indicated the varied prevalence of Precancerous Cervical Lesions (PCCL) among HIV-infected women, ranging between 4.4%-42.4%.7–13 Similarly, the various prevalence of PCCL among HIV-infected women were reported on limited studies conducted in Ethiopia, such as 22.1% in southern Ethiopia,14 20.2% in northwest15 and 9.9% in Amhara Regional State.16
Invasive cervical cancers are usually preceded by a long phase of the preinvasive disease, which can be detected early with different screening techniques. The screening techniques include cervical cytology, Visual Inspection, or Human Papillomavirus(HPV) Testing.17 In low- and middle-income countries, because of the required resources, skilled personnel, need for referral to distant health facilities for diagnostic and treatment services, and the long waiting times before cytology, the “Screen-and-treat” approach is an alternative approach. In such approach, the treatment decision is based on a screening test, and treatment is provided soon or, ideally, immediately after a positive screening test.18 Currently, this single-visit approach is being applied in the study area. However, data on the prevalence of precancerous cervical lesion lack especially among the high-risk group, HIV infected women. Therefore, this study aimed at assessing the prevalence and factors associated with PCCL among HIV infected women attending care and treatment clinics in selected hospitals of Southwestern Ethiopia.
Methods
Study Design, Setting, and Participants
An institution-based cross-sectional study was conducted from February to July 2018 in randomly selected hospitals of Southwestern Ethiopia. The selected hospitals were Mizan-Tepi University Teaching Hospital, G/tsadik Shewo Memorial Hospital, and Tepi General Hospital, found in Bench Maji, Keffa, and Sheka zone, respectively. The hospitals apply a single visit approach and offer VIA screening for all voluntary eligible women free of charge. All HIV-infected women aged 18 years and above attending care and treatment clinic during the study period were eligible for enrollment. However, women with prior total hysterectomy, who has a history of Cervical cancer, and pregnant women were excluded.
Sample Size and Sampling Technique
Sample size was calculated using single population proportion formula by taking account of the proportion of precancerous cervical lesion, P=22.1%,14 CI=95%, margin of error =4% and non-response rate=10%. A total of 454 HIV-infected women attending HIV care and treatment clinic at selected hospitals during the study period were invited to participate. A systematic random sampling technique was employed to select study participants. The total number of women who visit CTC (N) was estimated by considering the immediate previous six-month record. Lottery method was used to select the first participant (the first sampling unit). Then, after every 2nd unit included until the required sample reached. The sample size for each institution was distributed proportionally.
Data Collection Tool and Procedures
Data on participants’ demographic, reproductive, behavioral, and HIV-related care were collected using pretested, interviewer-administered structured questionnaires, and reviewing medical records. VIA was done for all participants for the detection of precancerous cervical lesion. Trained midwives working in the screening and treatment center collect the data and conduct the screening procedure supervised by three BSc midwives. Before the actual data collection, a pretest was done on 5% of women in another hospital, and necessary corrections were made accordingly. After informed consent was obtained, relevant obstetric and gynecological history was obtained and recorded. Women were reassured that the procedure was painless. A step-by-step procedure for cervical screening using VIA was applied based on A Practical Manual on Visual Screening for Cervical Neoplasia. Results of VIA were classified according to the International Agency for Research Against Cancer Manual19 and recorded after each test. Women with confirmed VIA positive results eligible for cryotherapy were treated with cryotherapy. A patient with a cervix suspicious for cancer or PCCL ineligible for cold coagulation referred to the gynecology clinic.
Data Analysis
Data were analyzed by SPSS version 20. Descriptive statistics were computed. Binary logistic regression analysis was done, and all explanatory variables with a p-value less than 0.2 were entered into multiple logistic regression model. The second analytical step used a stepwise backward model. Then, association was assessed using AOR and its 95% CI. And p-value of <0.05 was considered statistically significant. The goodness of model fitness was tested by using Hosmer and Lemeshow test.
Results
Sociodemographic Characteristics
Data were analyzed from 444 women making a response rate of 97.8%. The mean age of the participants was 34 (SD±5.72). Around three fourth (73.2%) of respondents were urban residents. Near to half (42.6%) were married, self-employed (34.2%), and attend primary education 189 (42.6%) (Table 1).
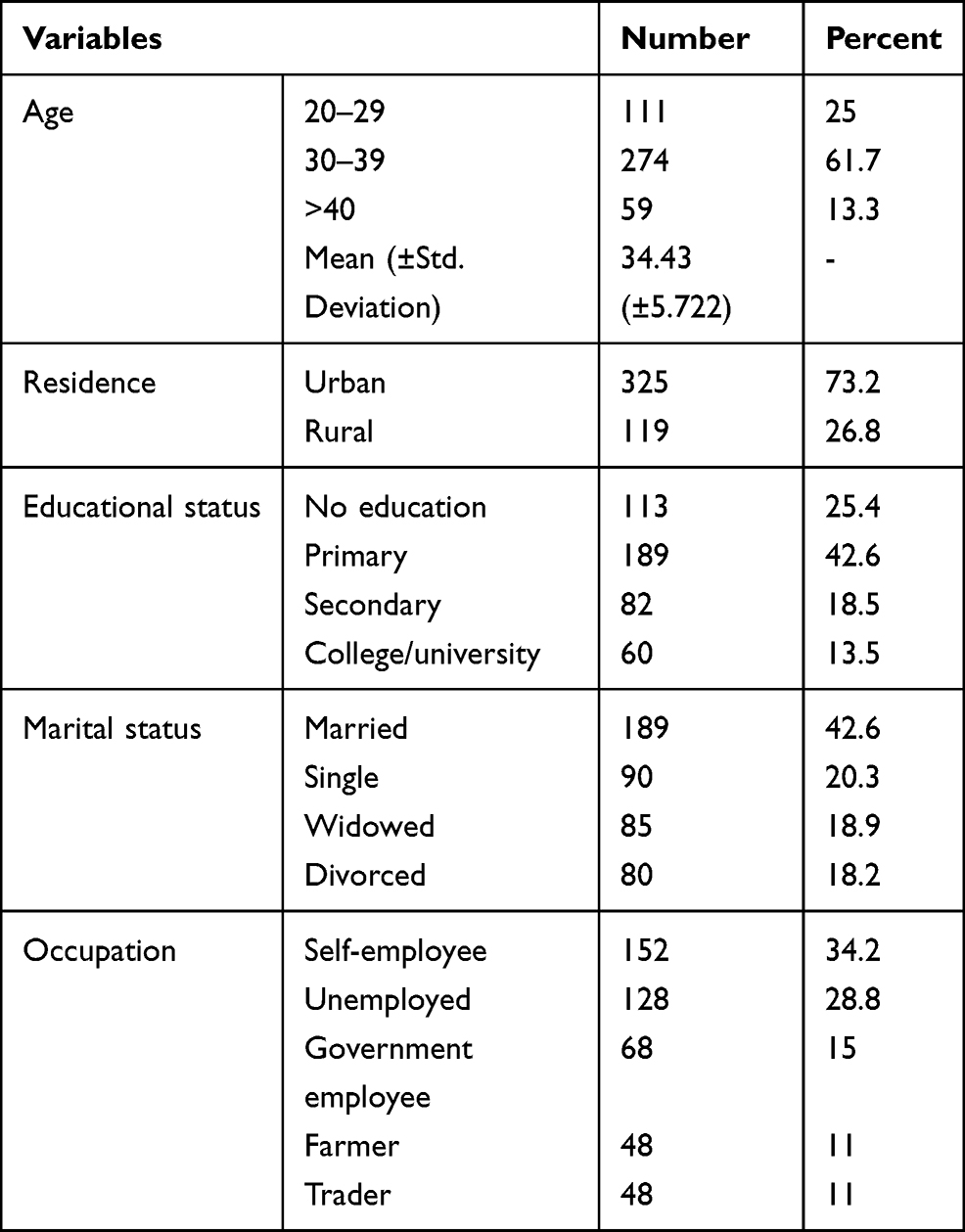 |
Table 1 Sociodemographic Characteristics of HIV-Infected Women Attending HIV Care and Treatment Clinics in Selected Hospitals of Southwest Ethiopia; 2018 (n=444) |
Sexual and Reproductive Characteristics
The mean age at first sexual intercourse was 15.24 years (SD±1.437). More than half (52.7%) of participants had their first sexual intercourse before 15 years. The mean age at first pregnancy was 19.99 (SD±3.102) years. Two-third (68%) of participants had more than a one-lifetime sexual partner. Around three-forth of the participants had given birth at least once (71.2%) and ever used oral contraceptives (72.7%). Nearly two-thirds (64.1%) of the participants had no history of abortion. More than a quarter of women (30.2%) had a history of sexually transmitted infection (STI) (Table 2).
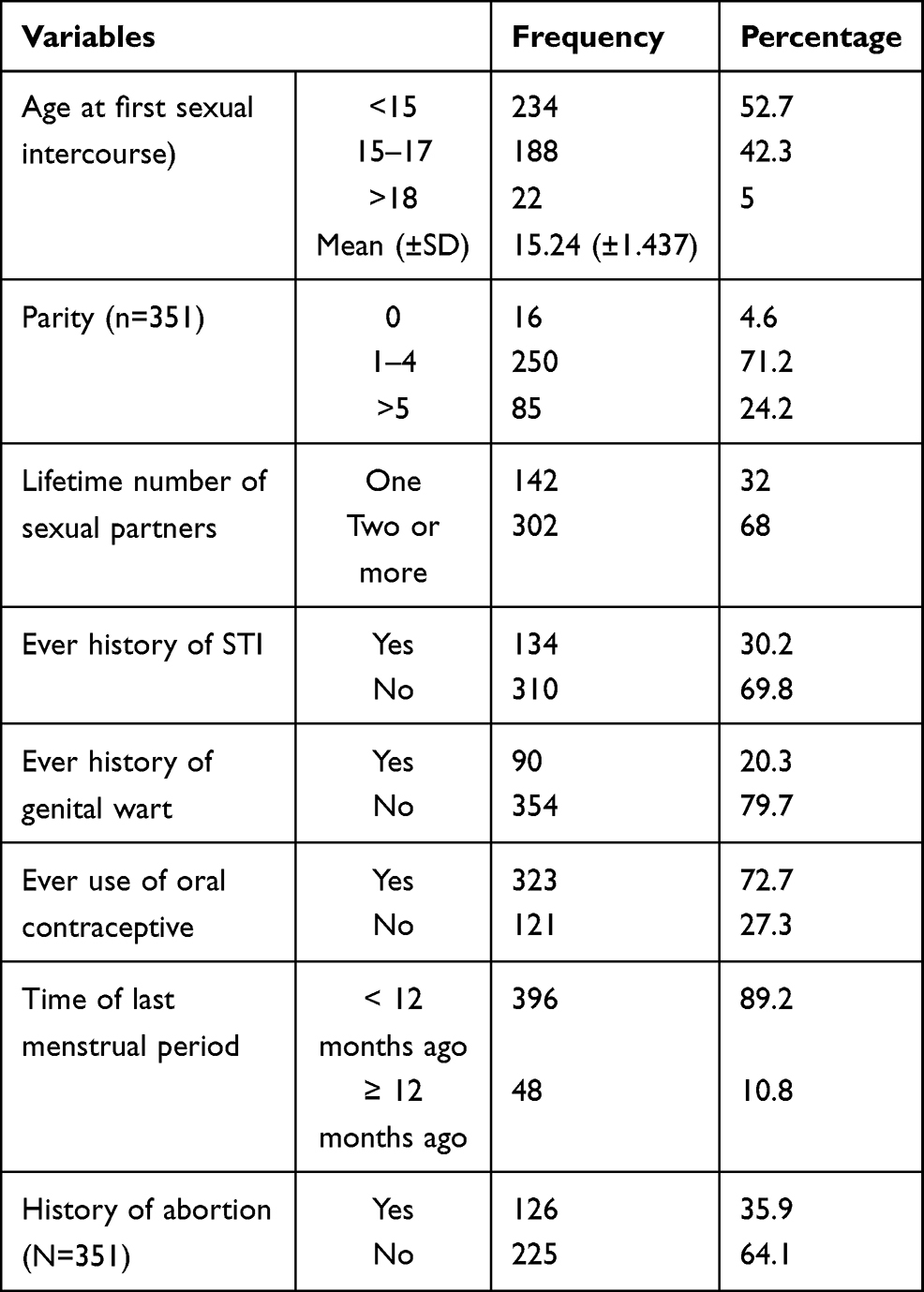 |
Table 2 Reproductive Health Characteristics of HIV-Infected Women Attending Care and Treatment Clinics in Selected Hospitals of Southwest Ethiopia; 2018 (n=444) |
Immunological and Behavioral Characteristics
More than two-thirds of the study participants (63%) were on Highly Active Antiretroviral Treatment (HAART). The mean baseline CD4 count of the participants while initiating HAART was 130.9 copies/mm3 (SD±52.4), and the recent mean CD4 count was 312.93 copies/mm3 (SD±219.38). Only 32 (7.2%) participants had a history of cigarette smoking (Table 3).
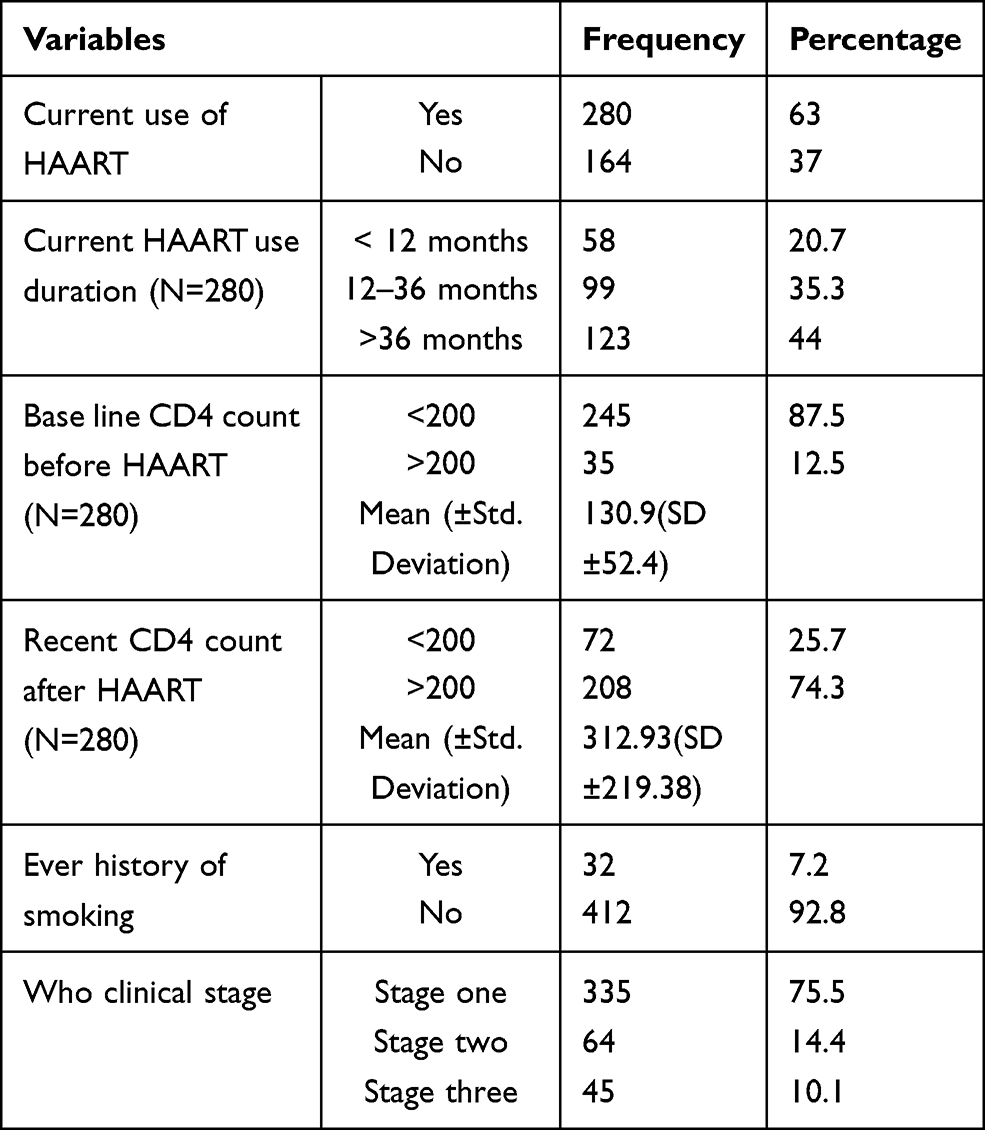 |
Table 3 Immunological Characteristics of HIV-Infected Women in Three Screening Centers, Southwest Ethiopia, 2018 (N=444) |
Prevalence of PCCL
Among 444 HIV-infected women screened for precancerous cervical lesions, 83 (18.7%) were found to be positive. Two women had suspicious invasive cervical cancer and sent to a gynecologic clinic.
Factors Associated with Precancerous Cervical Lesion
Age of participant, being on HAART, history of STI, number of lifetime sexual partner, and history of genital wart was significantly associated with PCCL.
Younger women aged 20–29 years were 81.5% less likely to be positive for PCCL than older women (>40 yrs) [AOR=0.185, 95% CI: 0.036–0.939]. Women who were not on HAART were about 2.31 times more likely to develop PCCL [AOR= 2.31, 95% CI: 1.23–4.39]. Those women who had one-lifetime sexual partner were 86.67% less likely to be positive for PCCL [AOR=0.133, 95% CI: 0.024–0.726]. HIV-infected women with no prior history of genital wart were 73.9% less likely to develop PCCL [AOR= 0.261, 95% CI: 0.073–0.934]. Also, those women who had no STI history were 97.4% less likely to be positive for PCCL [AOR=0.026, 95% CI: 0.006,0.116] (Table 4).
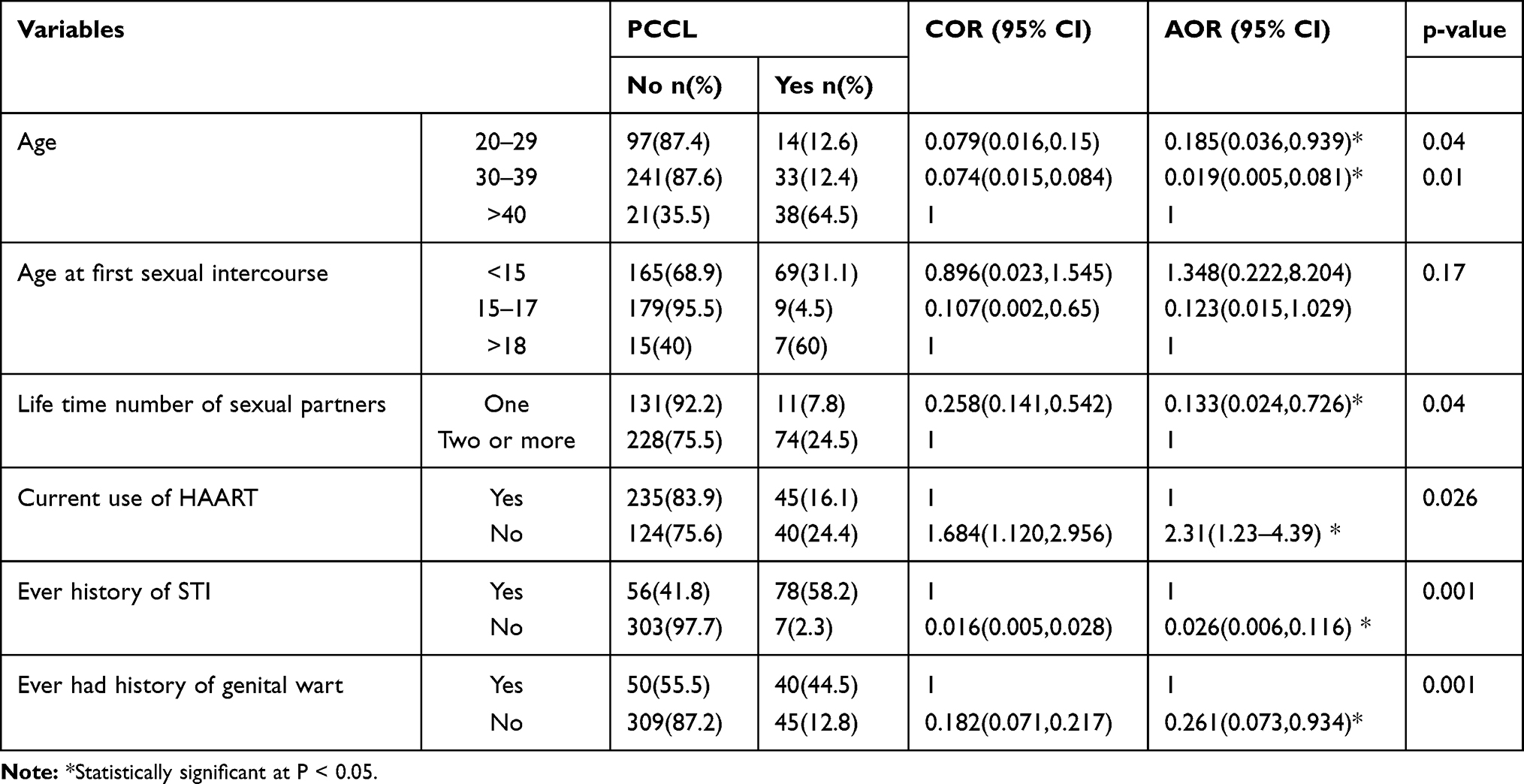 |
Table 4 Logistic Regression Analysis of Factors Associated with PCCL in a Selected Hospital, Southwest Ethiopia, 2018 |
Discussion
Various studies have shown a high prevalence of PCCL, indicating Cervical cancer and HIV infection are major public health problems facing women in developing counties like Ethiopia. This study aimed to assess the prevalence and factors associated with PCCL at three selected hospitals in Southwest Ethiopia. In this study, the prevalence of PCCL among HIV positive women was 18.7% (95% CI: 15.1–22.4). This finding is comparable with a study in southern Ethiopia.14 However, it is lower than a study in Tanzania (26.8%).7 This might be due to the difference in the sexual characteristics of participants. In such study, the participants had a higher number of lifetime sexual partners.8 That might increase their exposure to HPV infection, the predominant cause of PCCL. The prevalence of PCCL in this study was also found to be lower than a study in Kenya.8 This can be due to variation in the WHO clinical stage of participants. The majority of participants in kenya were on stage III & IV. The advanced stage of HIV might increase their risk of PCCL.20 The prevalence of PCCL in this study is higher than a study in Northern Ethiopia.16 It is also higher than a study in cote d'Ivoire (9.0%)12 and in Uganda (3%).21 The variation can be possibly explained by the difference in characteristics of study participants. The higher prevalence of PCCL in this study highlights the need to expand the screening service throughout the health service facilities in the region and provision of health education regarding cervical cancer and its screening for the vulnerable community.
This study revealed that women who were not on HAART were about 2.31 times morelikely to develop PCCL. This is consistent with the study done in Kenya,8 Tanzania11 and Southern Ethiopia.14 This attributes to the reason that being on HAART boosts women’s immunity and reduce the tendency to develop PCCL. It can also be explained by the fact that HAART lowers HPV acquisition, and increases clearance via immune reconstitution.22 This finding supports the current practice of early initiation of HAART for all HIV positive individuals regardless of CD4 count and WHO clinical stage. Those women who had no history of STI were 97.4% less likely to be positive for VIA screening test. This finding is similar to a study conducted in Tanzania,23 North Uganda21 and Southern Ethiopia.14 This can be explained by the fact that HPV infection is more prevalent in STI patients due to its sexually transmitted nature.24 However, a contradicting finding was reported on a study in Mekelle, which indicated that STI’s history was not significantly associated with PCCL.25 In this study, those women who had one-lifetime sexual partner were less likely to be positive for PCCL. It is supported by different studies.7,14,25,26 The increased number of sexual partners increases the chance of acquiring HPV infection, the predominant cause of PCCL.3 A significant association was obtained between PCCLand age; older women were more likely to acquire precancerous cervical cancer lesion than younger ones. Similar results were found in the study done in China.27 This might attribute to the quality of life of the youth and the time required for a cervical precancerous lesion to develop. Women with no history of genital warts were less likely to develop precancerous cervical lesion. This finding goes with a study conducted in Tanzania.23
Limitations
In this study, the prevalence of PCCL was assessed by VIA result only as a result, visually inapparent PCCL could have been missed due to its limited sensitivity and specificity. The results may not be generalizable to HIV negative women.
Conclusions
The prevalence of precancerous cervical lesion was found to be high in this study. Preventive measures against sexually transmitted infection are required. Further studies which address large population regardless of their HIV status using highly sensitive and specificity screening techniques are needed.
Data Sharing Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. Ethical clearance obtained from Mizan-Tepi University research and community support officers. Before this survey, a formal letter was submitted to heads of the respective zonal health offices and health facilities. The study’s objective, benefit, and risks were explained to the participants before data collection and obtained written informed consent from all respondents. The study participants were assured of the attainment of confidentiality, and the information they give us will not be used for any purpose other than the study.
Acknowledgments
We are grateful to Research Directorate Office, Mizan-Tepiuniversity, for the grants. We want to thank Mizan-Tepi university teaching hospital, G/Tsadik Shawo general hospital, and Tepi general hospital administration and ART clinic staffs for their marvelous collaboration. Finally, we want to thank data collectors and all women who participated in this research.
Author Contributions
All authors made a significant contribution to the work reported. Whether in the conception, study design, execution, acquisition of data, analysis, interpretation, or in all these areas. They took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Mizan-Tepi university research directorate office. This paper’s content is solely the responsibility of the authors and does not necessarily represent the official views of the University.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Anorlu RI. Cervical cancer: the sub-Saharan African perspective. Reprod Health Matters. 2008;16(32):41–49. doi:10.1016/S0968-8080(08)32415-X
3. Ting J, Kruzikas DT, Smith JS. A global review of age-specific and overall prevalence of cervical lesions. Int J Gynecol Cancer. 2010;20(7):1244–1249. doi:10.1111/IGC.0b013e3181f16c5f
4. Denny L, Anorlu R. Cervical cancer in Africa. Cancer Epidemiol Biomarkers Prev. 2012;21(9):1434–1438. doi:10.1158/1055-9965.EPI-12-0334
5. Maiman M, Fruchter RG, Clark M, Arrastia CD, Matthews R, Gates EJ. Cervical cancer as an AIDS-defining illness. Obstet Gynecol. 1997;89(1):76–80. doi:10.1016/S0029-7844(96)00378-X
6. Denslow SA, Rositch AF, Firnhaber C, Ting J, Smith JS. Incidence and progression of cervical lesions in women with HIV: a systematic global review. Int J STD AIDS. 2014;25(3):163–177. doi:10.1177/0956462413491735
7. Kafuruki L, Rambau PF, Massinde A, Masalu N. Prevalence and predictors of cervical intraepithelial neoplasia among HIV infected women at Bugando Medical Centre, Mwanza-Tanzania. Infect Agent Cancer. 2013;8(1):45. doi:10.1186/1750-9378-8-45
8. Memiah P, Mbuthia W, Kiiru G, et al. Prevalence and risk factors associated with precancerous cervical cancer lesions among HIV-infected women in resource-limited settings. AIDS Res Treat. 2012;2012. doi:10.1155/2012/953743
9. Sanad AS, Kamel HH, Hasan MM. Prevalence of cervical intraepithelial neoplasia (CIN) in patients attending Minia Maternity University Hospital. Arch Gynecol Obstet. 2014;289(6):1211–1217. doi:10.1007/s00404-013-3109-0
10. Jaquet A, Horo A, Ekouevi DK, et al. Risk factors for cervical intraepithelial neoplasia in HIV-infected women on antiretroviral treatment in Cote d’Ivoire, West Africa. PLoS One. 2014;9:3. doi:10.1371/journal.pone.0090625
11. Mugabe K. Prevalence and factors associated with precancerous cervical lesions among HIV-positive women attending Mulago Hospital, Uganda. 2013.
12. Horo A, Jaquet A, Ekouevi DK, et al. Cervical cancer screening by visual inspection in Cote d’Ivoire, operational and clinical aspects according to HIV status. BMC Public Health. 2012;12(1):237. doi:10.1186/1471-2458-12-237
13. Makuza JD, Nsanzimana S, Muhimpundu MA, Pace LE, Ntaganira J, Riedel DJ. Prevalence and risk factors for cervical cancer and precancerous lesions in Rwanda. Pan African Medical Journal. 2015;22(1). doi:10.11604/pamj.2015.22.26.7116
14. Gedefaw A, Astatkie A, Tessema GA. The prevalence of precancerous cervical cancer lesion among HIV-infected women in southern Ethiopia: a cross-sectional study. PLoS One. 2013;8(12):e84519. doi:10.1371/journal.pone.0084519
15. Kassa LS, Dile WM, Zenebe GK, Berta AM. Precancerous lesions of cervix among women infected with HIV in Referral Hospitals of Amhara Region, Northwest Ethiopia: a cross sectional study. Afr Health Sci. 2019;19(1):1695–1704. doi:10.4314/ahs.v19i1.46
16. Belayneh T, Mitiku H, Weldegebreal F. Precancerous cervical lesion and associated factors among HIV-infected women on ART in Amhara Regional State, Ethiopia: a hospital-based cross-sectional study. Int J Health Sci. 2019;13(3):4–9.
17. Cancer IAfRo. Planning and implementing cervical cancer prevention and control programs: a manual for managers. 2004.
18. Shiferaw N, Salvador-Davila G, Kassahun K, et al. The single-visit approach as a cervical cancer prevention strategy among women with HIV in Ethiopia: successes and lessons learned. Glob Health Sci Pract. 2016;4(1):87–98. doi:10.9745/GHSP-D-15-00325
19. Sankaranarayanan R, Wesley RS. A Practical Manual on Visual Screening for Cervical Neoplasia. Diamond Pocket Books (P) Ltd; 2003.
20. Patrelli TS, Gizzo S, Peri F, et al. Impact of highly active antiretroviral therapy on the natural history of cervical precancerous lesions: a 17-year institutional longitudinal cohort study. Reprod Sci. 2014;21(7):837–845. doi:10.1177/1933719113512531
21. Izudi J, Adrawa N, Amongin D. Precancerous cervix in human immunodeficiency virus infected women thirty years old and above in Northern Uganda. J Oncol. 2016;2016. doi:10.1155/2016/5473681
22. Liu G, Sharma M, Tan N, Barnabas RV. HIV-positive women have higher risk of human papilloma virus infection, precancerous lesions, and cervical cancer. Aids. 2018;32(6):795–808. doi:10.1097/QAD.0000000000001765
23. Balandya B, Pembe A, Mwakyoma H. Cervical pre-malignant lesions in HIV infected women attending care and treatment centre in a tertiary hospital, Dar es Salaam, Tanzania. East Afr J Public Health. 2011;8(3):185–189.
24. Ciccarese G, Herzum A, Rebora A, Drago F. Prevalence of genital, oral, and anal HPV infection among STI patients in Italy. J Med Virol. 2017;89(6):1121–1124. doi:10.1002/jmv.24746
25. Gessesse Z, Tadesse Z, Alemayehu M, et al. Determinant factors of visual inspection with acetic acid (VIA) positive lesions among HIV positive women in Mekelle Hospital, Northern Ethiopia: a case control study. EMJ. 2015;17–24.
26. Purwaningsih H, Prajatmo H. Risk factors associated with the occurrence of precancerous cervical lesions at health centers of Karanganyar regency. Int J Community Med Public Health. 2016;3(6):1437–1441. doi:10.18203/2394-6040.ijcmph20161607
27. Zhang Q, Xie W, Wang F, et al. Epidemiological investigation and risk factors for cervical lesions: cervical cancer screening among women in rural areas of Henan province China. Med Sci Monit. 2016;22:1858–1865. doi:10.12659/MSM.894663
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.