")
Back to Journals » Risk Management and Healthcare Policy » Volume 12
Pre-operative depression predicted longer hospital length of stay among patients undergoing coronary artery bypass graft surgery
Authors AbuRuz ME
Received 13 October 2018
Accepted for publication 12 April 2019
Published 13 May 2019 Volume 2019:12 Pages 75—83
DOI https://doi.org/10.2147/RMHP.S190511
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kent Rondeau
Mohannad Eid AbuRuz
Clinical Nursing Department, Faculty of Nursing, Applied Science Private University, Amman, Jordan
Purpose: Coronary artery bypass graft surgery (CABG) is a common and remarkably effective treatment for coronary heart disease, improving health status and enhancing quality of life. However, some outcomes after surgery remain unexplained, including psychological factors such as depression. The prevalence rates of pre- and post-operative depression among CABG patients are high, which is associated with negative short- and long-term outcomes. This study explores the impacts of pre-operative depressive symptoms on post-operative hospital length of stay (LOS) among patients undergoing CABG in Jordan.
Patients and methods: This was a non-experimental, prospective observational study among 227 CABG patients recruited from 5 hospitals in Amman, Jordan. Depression was measured within an average of two weeks prior and one month after the operation using the Hospital Anxiety and Depression Scale. Length of stay was abstracted from medical records after discharge.
Results: The average post-operative LOS was 11.40±10.41 days. The average pre-operative depression level was moderate; 12.76±6.80 and 42.47% complained of varying levels of depressive symptoms. The average post-operative depression level was moderate; 11.11±6.78 and 40.53% complained of varying levels of depressive symptoms. In stepwise regression models, depression scores and female gender were independent predictors that increased post-operative LOS. On the other hand, high income (≥1501$/month) and use of statins had protective effects and decreased post-operative LOS. The model explained 22.4% of the total variance regarding LOS.
Conclusion: Pre-operative depressive symptoms increased post CABG LOS. Application of policies and depression assessment protocols prior to CABG by health care providers can identify high-risk groups (eg, females), so appropriate interventions can be designed and implemented to decrease morbidity and mortality.
Keywords: depression, length of hospital stay, coronary artery bypass graft, Jordan
Introduction
Coronary artery bypass graft surgery (CABG) is a remarkable treatment for coronary heart disease worldwide, including in both developed and developing countries.1–4 CABG is a very common performed procedure, with 371,000 operations performed in 2017 in the US alone.1 In 2007, over 800,000 CABG operations were conducted worldwide.4 CABG usually improves health status, functional status, prolongs life, decreases symptoms and disability, and enhances quality of life.2,3,5,6 However, some outcomes after surgery are still unexplained.2,4,7,8 For instance, approximately 35% of the patients complain of anginal pain, and 40% have activity limitation a year after surgery.7 Therefore, identifying modifiable causative agents contributing to these negative outcomes might improve patients’ response after CABG.
It has been shown that recovery from acute cardiac events (ie acute myocardial infarction) depends more on psychological factors and retrieval than physical function.9–12 One of the most prevalent psychological factors that might affect this status is depression. The prevalence rates of pre-operative depression among CABG patients have been found to range from 14% to 60%,5,6,13–15 while post-operative depression rates are near-ubiquitous at 97.9%.4,16 Despite this endemic prevalence, more than 50% of the patients undergoing CABG are not screened for depressive symptoms by their health care providers.4,17 Moreover, health care providers still face challenges in the early identification and management of the negative outcomes during the early phase of post-CABG treatment.4,17
Different studies have shown negative effects of depression on outcomes among CABG patients. Pre-operative depression increases anginal pain, rehospitalization rates, occurrence of delirium, postoperative length of stay (LOS), mortality,2–6,18 and predicts higher levels of post-operative depression.3,19 Pre-operative depression has been associated with higher levels of cholesterol, C-reactive protein and inflammatory markers, including IL-6 and IL-8.4,5 These high levels of inflammatory markers are associated with greater rates of inflammation, lower immunity, and poor wound healing in the post-operative period.4,5 With regard to long-term outcomes, pre-operative depression increases psychosocial morbidity up to five years after the operation, augments the development of new cardiac events, and decreases quality of life 2–5 years following surgery.6,20
Similarly, post-operative depression has its own negative consequences after CABG. Usually, patients with high post-operative depression suffer from impaired quality of life, lack of adherence to medication, and lifestyle changes.2,4 Additionally, post-operative depression increases hospital readmissions and LOS, while reducing ability to walk and wound healing.2,3,15,21
A newly investigated indicator of outcomes between depression and CABG is the LOS, which is considered as an important marker of surgical recovery,5,6 a proxy measure of acute physical recovery, and a vital indicator of long-term recovery.5,6 Post-operative LOS has been connected with postoperative depression,4 re-admissions,22 and recurrent cardiac events.23 Patients who developed complications and have poor recovery after CABG are expected to stay longer in hospital. Recently, post-CABG LOS has decreased significantly due to efforts seeking to reduce the burden placed on health systems by hospital-based post-operative care.5,6 For instance, one day of post-CABG care in the ICU costs approximately $1300.5,6 For these reasons, most health care institutions implement policies to discharge patients as soon as possible, usually within 5–7 days.5,6
A few studies have checked the effect of pre-operative depression on the LOS among patients undergoing CABG.5,6,13 Poole et al5 showed that patients with high depressive symptoms prior to CABG had 3.51 times greater risk to stay in hospital more than seven days, and this relationship was mediated by high levels of C-reactive protein. In another study by the same authors,6 high levels of pre-operative depressive symptoms were associated with longer LOS, even after controlling of covariates. There was an interaction effect between high depression levels with economically disadvantaged levels, whereby patients with high levels of depression and low socioeconomic status had the longest post-operative LOS. Oxald et al13 showed that high pre-operative depression and low PTSD were responsible for 4.4% of the variance with regard to longer post-operative LOS.
To our knowledge, only one study was conducted in Jordan to check the prevalence of depression and its associated factors post CABG, in which the authors used a cross-sectional design with a convenience sample of 143 participants (76 men and 67 women).4 Their mean age was 64 years, and approximately 40% were employed. Depression was measured one time during the early recovery period (1–2 weeks post-operatively) using the self-rating depression scale. The results indicated that: the total level of post-operative depression was moderate (62.7±5.6) on a 0–100 scale; 2.1% of the sample were depression-free; 31.2% had mild depression; 60.1% had moderate depression; and 5.6% had severe depression. In terms of demographic variables, higher levels of depression were reported among female, unemployed, low-income, and older patients, while in clinical terms it was more prevalent among patients who did not receive education from nurses, and who stayed longer in the cardiac intensive care unit. The model explained 54.7% of the depression variance. The authors concluded that the incidence of depression post CABG is high, especially for females, the unemployed, and who did not receive education from nurses. However, this study4 used a cross-sectional design with a relatively small convenience sample. Moreover, depression was measured one time only during the post-operative period. This design did not assess depression levels over time (ie, longitudinally) and was particularly lacking in consideration of the pre-operative period.
Therefore, the general purpose of the current study was to check the effect of pre-operative depressive symptoms on post-operative hospital LOS among patients undergoing CABG in Jordan. Research hypotheses: (1) Patients with moderate to severe pre-operative depression levels will have longer post-operative LOS compared to other patients (2) Pre- and post-operative depression will be high (≥8) among patients undergoing CABG (3) Pre-operative depression will be higher than post-operative depression among patients undergoing CABG (4) Pre- and post-operative depression for female patients will be higher than for male patients; and (5) Female patients will have longer post-operative LOS compared to male patients.
Materials and methods
Design, sample, and setting
This was a non-experimental, prospective observational study. Research assistants used a consecutive recruitment method at the cardiology clinics of five hospitals (1 governmental, 1 teaching, and 3 private), in Amman, Jordan. The inclusion criteria were: (a) aged 18 years or older, (b) not having an emergency operation, (c) not diagnosed with any psychiatric disease, (d) not on anti-depressant medications, (e) able to read and write Arabic, and (f) capable and willing to sign informed consent. A total of 227 participants were included in the final analyses (Figure 1).
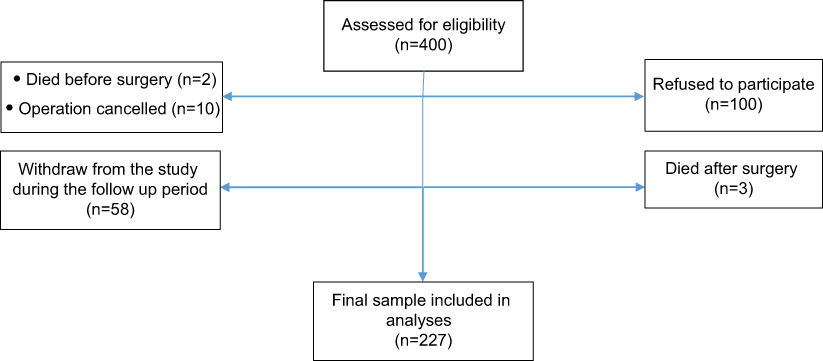 | Figure 1 Flow diagram of participants. |
Ethical considerations
The principal investigator presented the study to the Institutional Review Board (IRB) Committee at the Applied Science Private University, Amman, Jordan. The Committee approved the study and issued the IRB approval letter, which is officially accepted by institutions at Jordan. The medical directors of the selected hospitals acknowledged this IRB and delivered their permission to start data collection. The research team explained the study in full to all potential participants when inviting them to voluntarily participate in this study and those who agreed signed an informed consent form prior to data collection. They were fully informed of their right to withdraw from the study at any time without this affecting the care they received or their statutory rights. They were also given an opportunity to ask any questions if they wished. All data were kept in locked cabinet with access only by the principal investigator, and aggregate data were used for publication purposes.
Procedure
Five trained research assistants approached all participants at the cardiology clinic and explained the study in details, including its benefits and risks, as explained earlier. Participants answered the Arabic version of the Hospital Anxiety and Depression (HADS) within an average of 16 days before surgery, along with socio-demographic questions about age, gender, marital status, working status, and monthly income. One month after surgery, participants were asked to answer HADS another time. All other required information was collected from medical records after discharge, including post-operative hospital LOS, history of hypertension, diabetes mellitus (DM), previous angina, previous myocardial infarction, Body Mass Index (BMI) (kg/m2), and statins use (yes/no). Data collection was conducted during the period from August 2017 to March 2018.
Measurement of variables
Depression
The Arabic version of the HADS was used to measure depression at both time points. This version is valid and reliable, with a Cronbach’s α of 0.87.9,24 It is a self-reported questionnaire commonly used in clinical settings.9,24 Only the 7-items depression sub-scale was used. Each item has scores from 0 to 3, with higher scores indicating higher symptoms frequency and severity. The total score ranges from 0 to 21, with scores of 0 to 7 indicating normal; 8 to 10 mild; 11 to 14 moderate; and 15 to 21 severe depression.9,24
Post-operative LOS
This was abstracted from the medical records after discharge, reported in days.
Data analysis
SPSS version 21 was used to analyze the data. All test results were considered statistically significant at P<0.05. To test the associations between pre-operative depression and the covariates, Pearson correlation was used for continuous variables, and Spearman rho for categorical variables. For this test only, the statistical significance was set at P<0.1 (to be more conservative when we used the covariates later in the regression analysis). The general purpose of this study was checked by stepwise multiple regression to control for the effects of covariates. The independent variables entered in the models were age, gender, marital status, and monthly income in block one; history of hypertension, DM, previous myocardial infarction, previous angina, BMI, and use of statins in block two; and pre-operative depression scores in block three. Hypothesis one was checked by ANOVA with post hoc test. Depression scores were transformed into levels as the flowing: 0–7 normal, 8–10 mild, 11–21 moderate to severe. Hypothesis two was tested by descriptive statistics (mean±SD). Hypothesis three was tested by paired t-test. Hypotheses four and five were tested using independent t-test.
Results
Table 1 describes the characteristics of the participants. The mean age was around 66 years, and approximately three-quarters of participants were males. More than half of the sample was married, and the majority had previous history of angina. The average post-operative LOS was 11.40 days. Pre-operative depression increased with non-working status (t(225)=3.54, P<0.001) and higher BMI (r=0.178, P<0.01), and decreased with the use of statins (t(225)=−2.37, P<0.05).
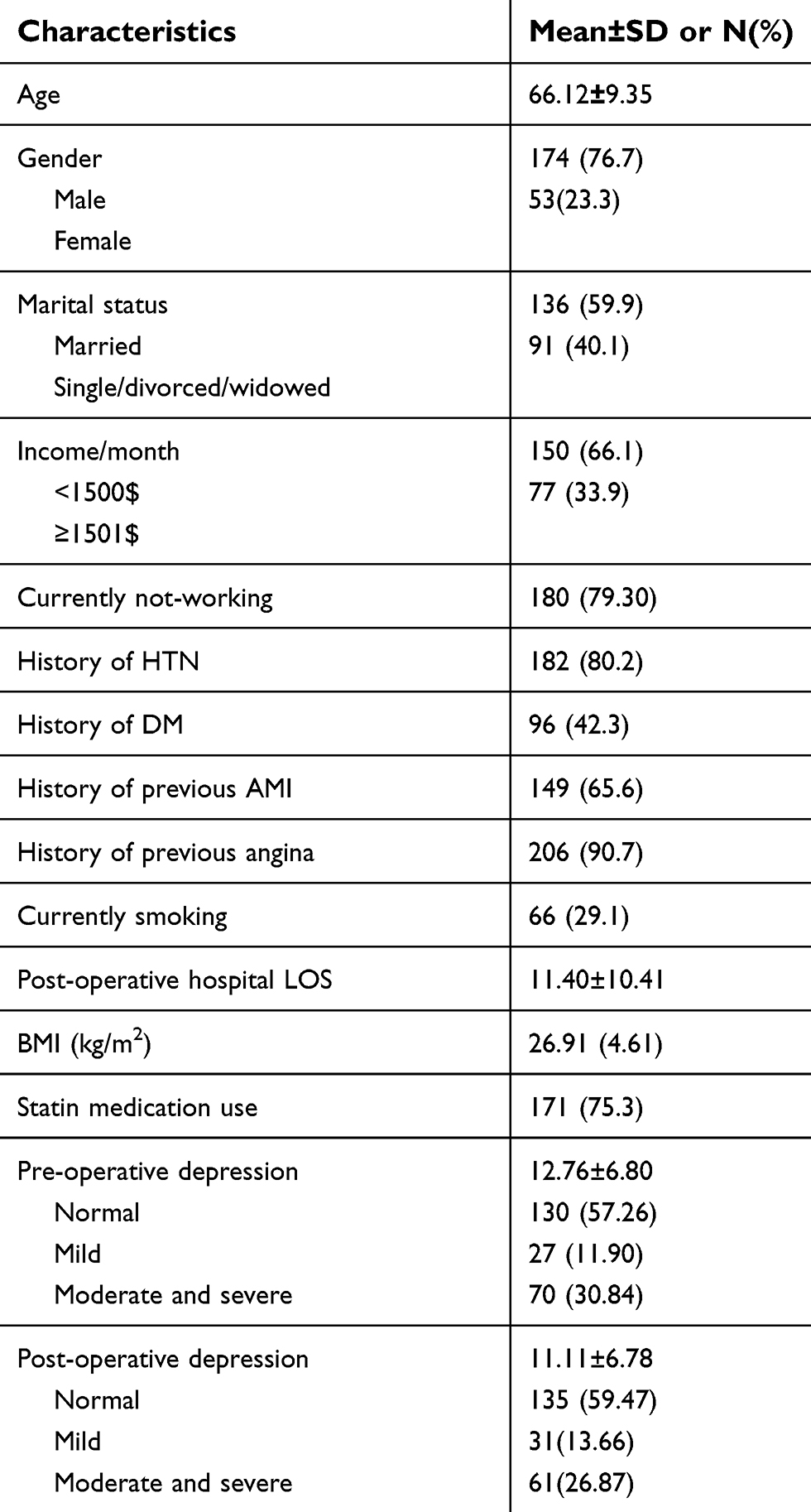 | Table 1 Clinical and sociodemographic characteristics (N=227) |
The general purpose of the study: pre-operative depression with post-operative LOS
Table 2 shows the results of stepwise regression models. Among all independent variables that were entered in the three blocks, depression scores and female gender were independent predictors that increased post-operative LOS. Every unit increase in depression was associated with an increase of 0.4 days in post-operative LOS. Being female increased post-operative LOS by 0.26 days. On the other hand, high income (≥$1501/month) and use of statins had protective effects and decreased post-operative LOS.
 | Table 2 Stepwise regression analyses for predictors of the post-operative hospital LOS (N=227) |
Hypotheses testing
Hypothesis one: patients with moderate and severe pre-operative depression levels will have longer post-operative LOS compared to other patients
ANOVA test showed that there was a significant difference in the post-operative LOS based on the depression levels (F(2,225)=21.77, p<0.001). Bonferroni post hoc test showed that moderate to severe depression were responsible for the main effect. They have longer post-operative LOS (M±SD; 15.11±12.52) compared to normal (M±SD; 5.59±5.12) and mild depression (M±SD; 7.09±5.62) (Table 3).
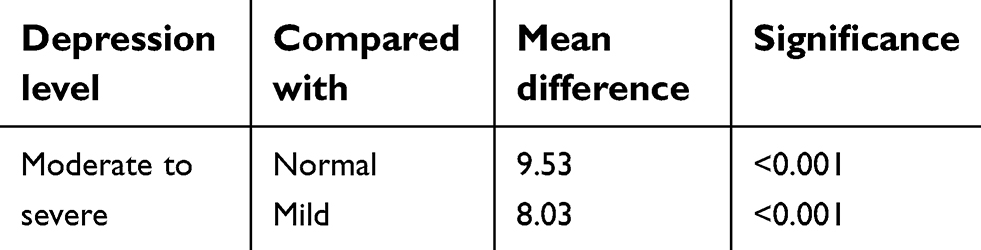 | Table 3 Post hoc Bonferroni test for differences of post-operative hospital LOS based on depression levels (N=227) |
Hypothesis two: pre- and post-operative depression will be high (≥8) among patients undergoing CABG
Descriptive statistics showed that pre- and post-operative depression levels were moderate (M±SD; 12.76±6.80) and (M±SD; 11.11±6.78) respectively.
Hypothesis three: pre-operative depression will be higher than post-operative depression among patients undergoing CABG
Paired t-test showed that there was a significant difference between the two depression levels (mean [SD], 12.76 [6.80] vs 11.11[6.78], t=7.21, p<0.001).
Hypothesis four: pre- and post-operative depression for female patients will be higher than for male patients
Independent t tests showed that there were statistically significant differences between females and males in regard to pre- and post-operative depression levels: (mean [SD], 16.57 [6.26] vs 11.60 [6.54], t=4.89, p<0.001) and (mean [SD], 13.15 [7.22] vs 10.49 [6.53], t=2.53, p<0.05), respectively.
Hypothesis five: female patients will have longer post-operative LOS compared to male patients
Independent t-tests showed that there were statistically significant differences between females and males in regard to post-operative LOS (mean [SD], 17.34 [12.62] vs 8.81[7.23], t=5.01, p<0.001).
Discussion
This was the first study specifically designed to check the effect of pre-operative depressive symptoms on post-operative hospital LOS among patients undergoing CABG in Jordan. The results showed that higher depressive symptoms independently increased the post-operative hospital LOS. Furthermore, there was a dose–response relationship between depression levels and post-operative hospital LOS, as evidenced by patients with moderate to severe depression levels exhibiting the longest post-operative hospital LOS. These results are consistent with previous studies.5,6,13
The results of this study showed pre-operative depressive symptoms among 42.74% of the patients, in line with previous studies reporting rates between 14% and 60%.5,6,13–15 Different explanations have been proffered to explain the divergence in reported prevalence, including (a) the use of diverse methods to assess depressive symptoms among researchers; (b) different published norms and cut-off points for these instruments; (c) timing of depression measurement during the study period; (d) differences in the inclusion and exclusion criteria of the study participants; and (e) the lack of control for the use of anti-depressant medications in some studies. Furthermore, the increasing use of lipid-lowering agents (ie, statins) in cardiology since the 1980s has been demonstrated by longitudinal studies to have protective effects against depression.6,25,26 Consistent with these results, our study showed that the use of statins decreased post-operative LOS.
There is no formal policy for discharging patients following CABG surgery in Jordan.4 However, due to the economic burden of health expenditure, all hospitals seek to discharge patients as soon as possible. In this study, the average post-operative LOS was (11.40±10.41) days. This rate is within the range of post-operative LOS among 10 European countries with 66,587 patients, from 9 days in Finland and Sweden to 17 in Ireland and Spain.27 Moreover, the rate in the study is similar to that of post-operative LOS among 19,522 CABG patients in the UK (12.48±10.94).27 On the other hand, our patients stayed longer in the hospital postoperatively compared to the 310 patients studied by Poole et al study.6 The reason behind these results is that our sample had higher percentages of moderately and severely depressed patients. As shown by the results of this study, depressive symptoms are associated with increased post-operative LOS.
The results of this study also showed that patients had high levels of depressive symptoms pre-operatively, which subsequently declined after surgery; during the recovery period (first month duration), but did not get to a remission. This conclusion is similar to the conclusion drawn by Ravven et al3 from a systematic synthesis and meta-analysis on depression and depressive symptoms from 39 prospective studies, which found that pre-operative depression is associated with a reduction of symptoms relief and faster return of these symptoms. Moreover, it is associated with higher rates of re-hospitalization and mortality immediately post-operatively.3,28,29 Post-operative depression is also associated with delayed wound healing, and higher levels of pain, infection rates, and acute myocardial infarction.14,18 The presence of such type of persistent depression might decrease compliance with cardiac rehabilitation and life modification programs. It is noteworthy that 52.9% of the participants in this study reported persistent depression.
In this study, post-operative depression was moderate, which is in line with the Jordanian study done by Hiweidi et al.4 This level of depression is attributed to the nature of the CABG surgery being a stressful and life-threatening event. However, the percentage of participants who had moderate to severe depression in the current study was lower. A possible explanation for this difference is the timing of depression measurement, which was done one month after surgery in the current study, while it was done in the telemetry unit one week after surgery in the previous study.4 Post-CABG patients usually start to improve more rapidly when they are discharged and return home, which might decrease their depression levels.
Exploring mechanisms linking depression to poor outcomes suggests three major pathways: biological, social, and behavioral. Biologically, depression acts on hypothalamic pituitary adrenal access, modulating immune functions and affecting immune cells that dysregulate the secretion of pro-inflammatory cytokines.5,14 Moreover, it has been shown that CRP mediated the relationship between depression and post-operative hospital LOS, suggesting a link between depression and inflammation.5,6,30 This inflammation is responsible for the negative outcomes after surgery. Socially and behaviorally, socioeconomically disadvantaged patients and those who lack sufficient sleep have poorer post-operative outcomes.4,6,31 Moreover, depressed patients demonstrate adverse behavioral changes as poor hygiene, altered nutrition, and lack of adherence to medication, all of which exacerbate negative outcomes.6,14 Therefore, appropriate management of pre- and post-operative depression is necessary.
Diverse strategies can be implemented for this purpose. The AHA recommends the use of Selective Serotonin Re-uptake Inhibitors (SSRIs) prior to the use of any anti-depressant.32,33 Tricyclic antidepressants are not recommended for this population due to their potential cardiac toxicity.34–36 Other strategies might include behavioral and psychological interventions, such as yoga and enhancing perceived control, which have been found to have positive effects on left ventricular ejection fraction, BMI, depression, and blood pressure.18,28,37 Other studies showed that cognitive behavioral therapy and supportive stress management are effective in treating depression among CABG patients.17 It is highly recommended that such holistic interventions be implemented for patients planning to undergo CABG surgery, especially high-risk groups.
Depression is sometimes considered a particularly feminine illness, which causes stigmatization and numerous barriers to effective care, but women do indeed have higher rates compared to males.9 Women also have higher depression rates in different cardiac populations, including heart failure, acute myocardial infarction, and post-CABG.9,38–43 This study reaffirmed that female patients had higher levels of pre- and post-operative depression compared to male patients. This result is in line with the Jordanian study by Hiweidi et al.4 On the other hand, some studies16,44,45 did not find this, which might be due to the same reasons of the difference in depression rates among this population of patients, and the small numbers of females involved in these studies.
After CABG surgery, women have a more difficult recovery compared to men, which cannot be explained by illness severity, pre-surgery health status, or other patient characteristics.39 These results suggesting that an important role may be exerted by the psychological status of patients on their outcomes, with the association being related to different gender roles and expectations.39 In most cultures, including in Jordan, women usually have a greater role in the home and family life (particularly child-rearing), thus they may feel more disruption in their lives and consequently feel more depressed when they cannot resume their former role in full after surgery. This is particularly acute during the recovery period following surgery.39
Rates of depression were associated with women having longer post-operative LOS in this study, and the impact of their socioeconomic status. It has been shown that income interacts with depression and increased post-operative LOS.6 Hweidi et al4 also showed that depression was higher among unemployed and low-income patients. Employment can ensure more monthly income, which is inversely related to depression levels. Higher income permits patients to be safer and less worried after CABG.4 The number of women who had lower income in this study was greater than that of men. Furthermore, in Jordan, women are usually paid less compared to men, even when performing the same job.
Conclusion
Pre- and post-operative depression rates among Jordanian patients undergoing CABG are high. Pre-operative depression increases post-operative LOS. Therefore, the application of policies and depression assessment protocols prior to CABG by health care providers can identify high-risk groups (eg, females) so appropriate interventions can be implemented to decrease morbidity and mortality.
Study limitations
The major limitation of this study was the use of chart review in order to collect some of the data, as we depended on others for such information. Moreover, depression was measured by the HADS, which is a self-reported questionnaire. Albeit this instrument is valid, reliable, and widely used in clinical settings, and it does not contain somatic symptoms, it is recommended that future studies undertake clinical evaluation of depression among patients with the assistance of a psychiatrist, in addition to the HADS, for further confirmation of depressive symptoms.
Acknowledgments
The author is grateful to the Applied Science Private University, Amman, Jordan, for the partial financial support granted to do data collection for this research project.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Benjamin EJ, Virani SS, Callaway CW, et al. Heart disease and stroke statistics-2018 update: a report from the American Heart Association. Circulation. 2018;137(12):e67–e492. doi:10.1161/CIRCULATIONAHA.117.031422
2. Kidd T, Poole L, Leigh E, Ronaldson A, Jahangiri M, Steptoe A. Health-related personal control predicts depression symptoms and quality of life but not health behaviour following coronary artery bypass graft surgery. J Behav Med. 2016;39(1):120–127. doi:10.1007/s10865-016-9713-2
3. Ravven S, Bader C, Azar A, Rudolph JL. Depressive symptoms after CABG surgery: a meta-analysis. Harv Rev Psychiatry. 2013;21(2):59–69. doi:10.1097/HRP.0b013e31828a3612
4. Hweidi IM, Gharaibeh BA, Al-Obeisat S, Al-Smadi A. Prevalence of depression and its associated factors in patients post-coronary artery bypass graft surgery. J Res Nurs. 2018;23(1):76–88. doi:10.1177/1744987117728314
5. Poole L, Kidd T, Leigh E, Ronaldson A, Jahangiri M, Steptoe A. Depression, C-reactive protein and length of post-operative hospital stay in coronary artery bypass graft surgery patients. Brain Behav Immun. 2014;37:115–121. doi:10.1016/j.bbi.2013.11.008
6. Poole L, Leigh E, Kidd T, Ronaldson A, Jahangiri M, Steptoe A. The combined association of depression and socioeconomic status with length of post-operative hospital stay following coronary artery bypass graft surgery: data from a prospective cohort study. J Psychosom Res. 2014;76(1):34–40. doi:10.1016/j.jpsychores.2013.10.019
7. Mallik S, Krumholz HM, Lin ZQ, et al. Patients with depressive symptoms have lower health status benefits after coronary artery bypass surgery. Circulation. 2005;111(3):271–277. doi:10.1161/01.CIR.0000152102.29293.D7
8. Abramov D, Tamariz MG, Fremes SE, et al. Trends in coronary artery bypass surgery results: a recent, 9-year study. Ann Thorac Surg. 2000;70(1):84–90.
9. AbuRuz ME, Alaloul F, Al-Dweik G. Depressive symptoms are associated with in-hospital complications following acute myocardial infarction. Appl Nurs Res. 2018;39:65–70. doi:10.1016/j.apnr.2017.11.001
10. Huffman JC, Smith FA, Blais MA, Januzzi JL, Fricchione GL. Anxiety, independent of depressive symptoms, is associated with in-hospital cardiac complications after acute myocardial infarction. J Psychosom Res. 2008;65(6):557–563. doi:10.1016/j.jpsychores.2008.08.001
11. AbuRuz ME, Masa‘Deh R. Gender differences in anxiety and complications early after acute myocardial infarction. J Cardiovasc Nurs. 2017;32(6):538–543. doi:10.1097/JCN.0000000000000375
12. AbuRuz ME. Perceived control moderates the relationship between anxiety and in-hospital complications after ST segment elevation myocardial infarction. J Multidiscip Healthc. 2018;11:359–365. doi:10.2147/JMDH.S170326
13. Oxlad M, Stubberfield J, Stuklis R, Edwards J, Wade TD. Psychological risk factors for increased post-operative length of hospital stay following coronary artery bypass graft surgery. J Behav Med. 2006;29(2):179–190. doi:10.1007/s10865-005-9043-2
14. Doering LV, Moser DK, Lemankiewicz W, Luper C, Khan S. Depression, healing, and recovery from coronary artery bypass surgery. Am J Crit Care. 2005;14(4):316–324.
15. Tully PJ, Baker RA, Turnbull D, Winefield H. The role of depression and anxiety symptoms in hospital readmissions after cardiac surgery. J Behav Med. 2008;31(4):281–290. doi:10.1007/s10865-008-9153-8
16. Amouzeshi A, Hosseini SM, Javadi A, et al. Depression and associated factors in patients undergoing coronary artery bypass grafting in Imam Reza hospital of Mashhad in 2013. J Surg Trauma. 2016;3(3–4):51–56.
17. Freedland KE, Skala JA, Carney RM, et al. Treatment of depression after coronary artery bypass surgery: a randomized controlled trial. Arch Gen Psychiatry. 2009;66(4):387–396. doi:10.1001/archgenpsychiatry.2009.7
18. Chaudhury S, Saini R, Bakhla AK, Singh J. Depression and anxiety following coronary artery bypass graft: current Indian scenario. Cardiol Res Pract. 2016;2016:2345184. doi:10.1155/2016/2345184
19. Pirraglia PA, Peterson JC, Williams-Russo P, Gorkin L, Charlson ME. Depressive symptomatology in coronary artery bypass graft surgery patients. Int J Geriatr Psychiatry. 1999;14(8):668–680. doi:10.1002/(ISSN)1099-1166
20. Burg MM, Benedetto MC, Rosenberg R, Soufer R. Presurgical depression predicts medical morbidity 6 months after coronary artery bypass graft surgery. Psychosom Med. 2003;65(1):111–118. doi:10.1097/01.PSY.0000038940.33335.09
21. Tully PJ, Baker RA, Knight JL. Anxiety and depression as risk factors for mortality after coronary artery bypass surgery. J Psychosom Res. 2008;64(3):285–290. doi:10.1016/j.jpsychores.2007.09.007
22. Hannan EL, Racz MJ, Walford G, et al. Predictors of readmission for complications of coronary artery bypass graft surgery. Jama. 2003;290(6):773–780. doi:10.1001/jama.290.6.773
23. Connerney I, Shapiro PA, McLaughlin JS, Bagiella E, Sloan RP. Relation between depression after coronary artery bypass surgery and 12-month outcome: a prospective study. Lancet. 2001;358(9295):1766–1771. doi:10.1016/S0140-6736(01)06803-9
24. Abu Ruz ME, Al-Akash HY, Jarrah S. Persistent (Anxiety and depression) affected academic achievement and absenteeism in nursing students. Open Nurs J. 2018;12:171–179. doi:10.2174/1874434601812010171
25. Otte C, Zhao S, Whooley MA. Statin use and risk of depression in patients with coronary heart disease: longitudinal data from the heart and soul study. J Clin Psychiatry. 2012;73(5):610–615. doi:10.4088/JCP.11m07038
26. Stafford L, Berk M. The use of statins after a cardiac intervention is associated with reduced risk of subsequent depression: proof of concept for the inflammatory and oxidative hypotheses of depression? J Clin Psychiatry. 2011;72(9):1229–1235. doi:10.4088/JCP.09m05440blu
27. Gaughan J, Kobel C, Linhart C, Mason A, Street A, Ward P;
28. Gallagher R, McKinley S. Anxiety, depression and perceived control in patients having coronary artery bypass grafts. J Adv Nurs. 2009;65(11):2386–2396. doi:10.1111/j.1365-2648.2008.04937.x
29. McKhann GM, Borowicz LM, Goldsborough MA, Enger C, Selnes OA. Depression and cognitive decline after coronary artery bypass grafting. Lancet. 1997;349(9061):1282–1284.
30. Kiecolt-Glaser JK, Glaser R. Depression and immune function: central pathways to morbidity and mortality. J Psychosom Res. 2002;53(4):873–876. doi:10.1016/S0022-3999(02)00309-4
31. Gallo LC, Matthews KA. Understanding the association between socioeconomic status and physical health: do negative emotions play a role? Psychol Bull. 2003;129(1):10–51. doi:10.1037/0033-2909.129.1.10
32. Hillis LD, Smith PK, Anderson JL, et al. 2011 ACCF/AHA guideline for coronary artery bypass graft surgery: executive summary: a report of the American college of cardiology foundation/American Heart Association task force on practice guidelines. Circulation. 2011;124(23):2610–2642. doi:10.1161/CIR.0b013e31823b5fee
33. Hillis LD, Smith PK, Anderson JL, et al. 2011 ACCF/AHA guideline for coronary artery bypass graft surgery. A report of the American college of cardiology Foundation/American Heart Association task force on practice guidelines. Developed in collaboration with the American Association for thoracic surgery, society of cardiovascular anesthesiologists, and society of thoracic surgeons. J Am Coll Cardiol. 2011;58(24):e123–210.
34. Tully PJ, Baker RA. Depression, anxiety, and cardiac morbidity outcomes after coronary artery bypass surgery: a contemporary and practical review. J Geriatr Cardiol. 2012;9(2):197–208. doi:10.3724/SP.J.1263.2011.12221
35. Cohen HW, Gibson G, Alderman MH. Excess risk of myocardial infarction in patients treated with antidepressant medications: association with use of tricyclic agents. Am J Med. 2000;108(1):2–8. doi:10.1016/S0002-9343(99)00301-0
36. Ha JH, Wong CK. Pharmacologic treatment of depression in patients with myocardial infarction. J Geriatr Cardiol. 2011;8(2):121–126. doi:10.3724/SP.J.1263.2011.00121
37. Raghuram N, Parachuri VR, Swarnagowri MV, et al. Yoga based cardiac rehabilitation after coronary artery bypass surgery: one-year results on LVEF, lipid profile and psychological states–a randomized controlled study. Indian Heart J. 2014;66(5):490–502. doi:10.1016/j.ihj.2014.08.007
38. Moser DK, Dracup K, Evangelista LS, et al. Comparison of prevalence of symptoms of depression, anxiety, and hostility in elderly patients with heart failure, myocardial infarction, and a coronary artery bypass graft. Heart Lung. 2010;39(5):378–385. doi:10.1016/j.hrtlng.2009.10.017
39. Vaccarino V, Lin ZQ, Kasl SV, et al. Gender differences in recovery after coronary artery bypass surgery. J Am Coll Cardiol. 2003;41(2):307–314. doi:10.1016/S0735-1097(02)02698-0
40. Nemati MH, Astaneh B. The impact of coronary artery bypass graft surgery on depression and anxiety. J Cardiovasc Med. 2011;12(6):401–404. doi:10.2459/JCM.0b013e32834358e9
41. Mitchell RH, Robertson E, Harvey PJ, et al. Sex differences in depression after coronary artery bypass graft surgery. Am Heart J. 2005;150(5):1017–1025. doi:10.1016/j.ahj.2005.05.005
42. McCrone S, Lenz E, Tarzian A, Perkins S. Anxiety and depression: incidence and patterns in patients after coronary artery bypass graft surgery. Appl Nurs Res. 2001;14(3):155–164. doi:10.1053/apnr.2001.24414
43. Duits AA, Duivenvoorden HJ, Boeke S, et al. The course of anxiety and depression in patients undergoing coronary artery bypass graft surgery. J Psychosom Res. 1998;45(2):127–138. doi:10.1016/S0022-3999(97)00307-3
44. Sharif F, Shoul A, Janati M, Kojuri J, Zare N. The effect of cardiac rehabilitation on anxiety and depression in patients undergoing cardiac bypass graft surgery in Iran. BMC Cardiovasc Disord. 2012;12:40. doi:10.1186/1471-2261-12-40
45. Shafiei Z, Babaee S, Nazari A. The effectiveness of massage therapy on depression, anxiety and stress of patients after coronary artery bypass graft surgery. Iran J Surg. 2013;21(1).
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.