")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Practice and Attitude Towards COVID-19 Prevention and Divine Belief Among Residents in Ethiopia: Cross-Sectional Survey
Authors Melese Ayele W
Received 17 December 2020
Accepted for publication 12 February 2021
Published 10 March 2021 Volume 2021:14 Pages 987—995
DOI https://doi.org/10.2147/RMHP.S297846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Wolde Melese Ayele
Department of Epidemiology and Biostatistics, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia
Correspondence: Wolde Melese Ayele Email [email protected]
Purpose: Coronavirus disease-2019 is an emerging disease that threatens the world. With the absence of successful treatment precipitated by the lack of health infrastructures in developing countries including Ethiopia, efforts to enhance the attitudes and practice of people are critical for managing the pandemic. Hence, this study aimed to assess the practice, attitude towards COVID-19, and divine belief among residents in Ethiopia.
Patients and Methods: A community-based cross-sectional study combining qualitative design was conducted in August 2020. The qualitative design was employed to explore the respondents’ divine belief towards the COVID-19 pandemic. Chi-square analysis was computed to identify factors associated with practice against COVID-19 prevention measures. The calculated chi-square greater than the tabulated value at a degree of freedom ((row total-1) * (column total)) and P-value < 0.05 were considered statistically significant.
Results: In this study, a total of 508 respondents participated. The mean age of the participants was 38.4 ± 11.2 (SD) years. The overall practice of prevention measures and attitude towards COVID-19 was 53.3% (95% CI: 49.0– 57.6%) and 49.6% (95% CI: 45.3– 53.9%), respectively. Age, residency, educational status, monthly income of the household, having a child, and attitude towards COVID-19 were statistically significant predictors of COVID-19 prevention measures (P< 0.05).
Conclusion: As the global threat of COVID-19 continues, it is critical to improving the respondents’ practice and attitude towards the precautionary measures, especially some religious followers.
Keywords: COVID-19, practice, attitudes, divine belief, Ethiopia
Introduction
In Wuhan, China, a cluster of pneumonia cases caused by a novel coronavirus was identified as β-coronavirus on December 2019.1,2 On 11 February 2020, the WHO officially named the disease coronavirus disease 2019 (COVID-19) and declared the pandemic on March 12th, 2020.3–5
Severe Acute Respiratory Syndrome Corona Virus 2 (SARS-CoV-2), a cause for COVID-19, is the seventh member of the family of coronavirus.6 Like in Middle East respiratory syndrome coronavirus (MERS-CoV) and SARS-CoV cases; fever, fatigue, and dry cough are the most commonly observed symptoms among COVID-19 patients. The serious symptoms are difficulty or shortness of breathing, chest pain or pressure, and loss of speech or movement.7–9
Although the intermediate animal host between a bat reservoir and humans is still unknown, recent research reported that SARS‐CoV‐2 is likely originated in bats.8–10 The major mode of transmission is through human‐to‐human transmission. COVID-19 primarily conveys through the respiratory tract by droplets, respiratory secretions, and direct contact.11,12 A molecular and serological study in China found that SARS-CoV-2 is present in fecal swabs, blood, and even in sewages indicating the possibility of multiple routes of transmission.13–15
According to a recent study in China and the WHO report, about 80% of patients present with mild illness.16,17 The community occupants are the most vulnerable groups affected by health problems easily. To halt the COVID-19 pandemic, community members play the front-line practicing precautionary measures such as staying at home, physical distancing, appropriate utilization of personal protective equipment, and social assisting.11,18,19
Although the virus is an emerging phenomenon, there is a wide gap in prevention practice, especially in Ethiopia. Currently, Ethiopia is the fifth in Africa and the first in the Horn of Africa by confirmed SARS-CoV-2 cases. As of January 10, 2021, a total of 128,316 confirmed COVID-19 cases and 1,994 deaths were recorded in the country. For example, the number of new cases on Epi-week 23, 2020 was 848; while on Epi-week 35 were 10,451.20,21 This implies that the severity of the pandemic is becoming catastrophic. As well, some sub-populations have a divine belief towards the emergence of COVID-19. That might be an obstacle to the effective control of the pandemic in the area. But there is no study conducted that explores the practice, attitude, and divine belief towards COVID-19 in Ethiopia. A good prevention practice and attitude might result in decreased morbidity, mortality, and delayed spread of the disease. Therefore, this study aimed to assess the prevention practice, attitude, and exploring participants’ divine belief toward COVID-19 in Ethiopia. The finding will help responsible authorities to organize the necessary interventional programs to the right population group at the right time. Similarly, it will be a noble opportunity for the government to make a linkage with religious institutions for the attitude change of the followers. Finally, the finding will give a starting point to the government about the populations’ divine belief towards any future epidemic occurrence.
Patients and Methods
Study Design and Period
A community-based cross-sectional study was conducted in Northeastern Ethiopia in August 2020. And interviewer-administered structured questionnaire was used to collect the data. The participants were selected using a random method. The objective of the study was explained clearly to the participants at the beginning of the survey. The divine belief of respondents was collected using an interview guide questions. The participants of the qualitative part were 48 people from three religions in the study area. According to the 2007 National census, the study area has 58.62% Orthodox Christian, 39.92% Islam, and 1.15% Protestant religion composition.22 Sixteen eligible equal genders from Orthodox Christian, Muslim, and Protestant followers were included in the study.
Study Population and Instrument
A community-based cross-sectional survey was conducted with a total of 508 Ethiopian respondents to evaluate the prevention practice, attitudes towards COVID-19, and divine belief about the emergence of the pandemic. The data collection tool was developed in the English language after a thorough search of the recent literatures and based on the most recently available information from the World Health Organization on emerging respiratory viruses, COVID-19. The questionnaire was pre-tested on 50 randomly selected community residents to assess its consistency. As required, necessary modifications were made to facilitate better comprehension and to organize the questions before the actual survey was conducted. The data was collected by twelve diploma nurses and supervised by six BSc in public health graduates. The qualitative data were collected using guiding questions. The respondents were probed to explore their divine belief towards the emergence of COVIID-19.
As shown in Supplementary Material, the questionnaire consisted of closed-ended questions with responses based on yes/no/I do not know formats. This survey tool is divided into three main sections to assess the participants’ practice and attitude towards COVID-19. The first section covered socio-demographic characteristics of the participants such as age, gender, religion, residence (rural/urban), marital status, presence of children, and monthly income. The second section consists of the practice of self-protection measures (six items). Those were staying at home, physical distancing, wearing a mask, washing hands at least for 20 seconds in every object touch, applying sanitizer during every object touch, and self-isolation if self-suspecting of COVID-19. The score was computed for each study participant by assigning a value of one to each corrected response. The total score was changed and presented in a percent form. The last section comprises eleven items that assess participants’ attitudes towards COVID-19 prevention. Similarly, the score was present in a percentage form.
Respondents who answered more than 50% of the eleven questions provided were classified as having a positive attitude on COVID-19. Similarly, six questions related to the practices of COVID-19 prevention were provided to respondents, and respondents who answered above 50% correctly were designated as having a good prevention practice against COVID-19.
Data Analysis
The data was coded, validated, and analyzed using SPSS version 21. The frequency measures and mean with standard deviation were computed for categorical and continuous variables, respectively. A chi-square test was used to identify the statistical association of independent variables with the practice of COVID-19 prevention. A calculated chi-square value of more than the tabulated value with respective degree of freedom (df=(row total-1) * (column total)) was considered the cut-off level for the presence of statistical significance.
The qualitative data presented here were the only variables that were different from the quantitative data. The data were present in themes based on the nature of the data from each Focus Group Discussion (FGD). Samples of the ideas explored by the discussion members were presented under quotation Italics.
Results
Socio-Demographic Characteristics of Participants
Five hundred and eight community members participated in this community-based survey. Three hundred sixty (70.9%) of 508 participants were females with a mean ± SD of 33.2±11.4 years of age. More than half 342 (67.3%) of the participants were from the urban setting. Around three fourth, 306 (60.2%) of the participants were married, and 369 (53%) had children. The Socio-demographic characteristic is presented in Table 1.
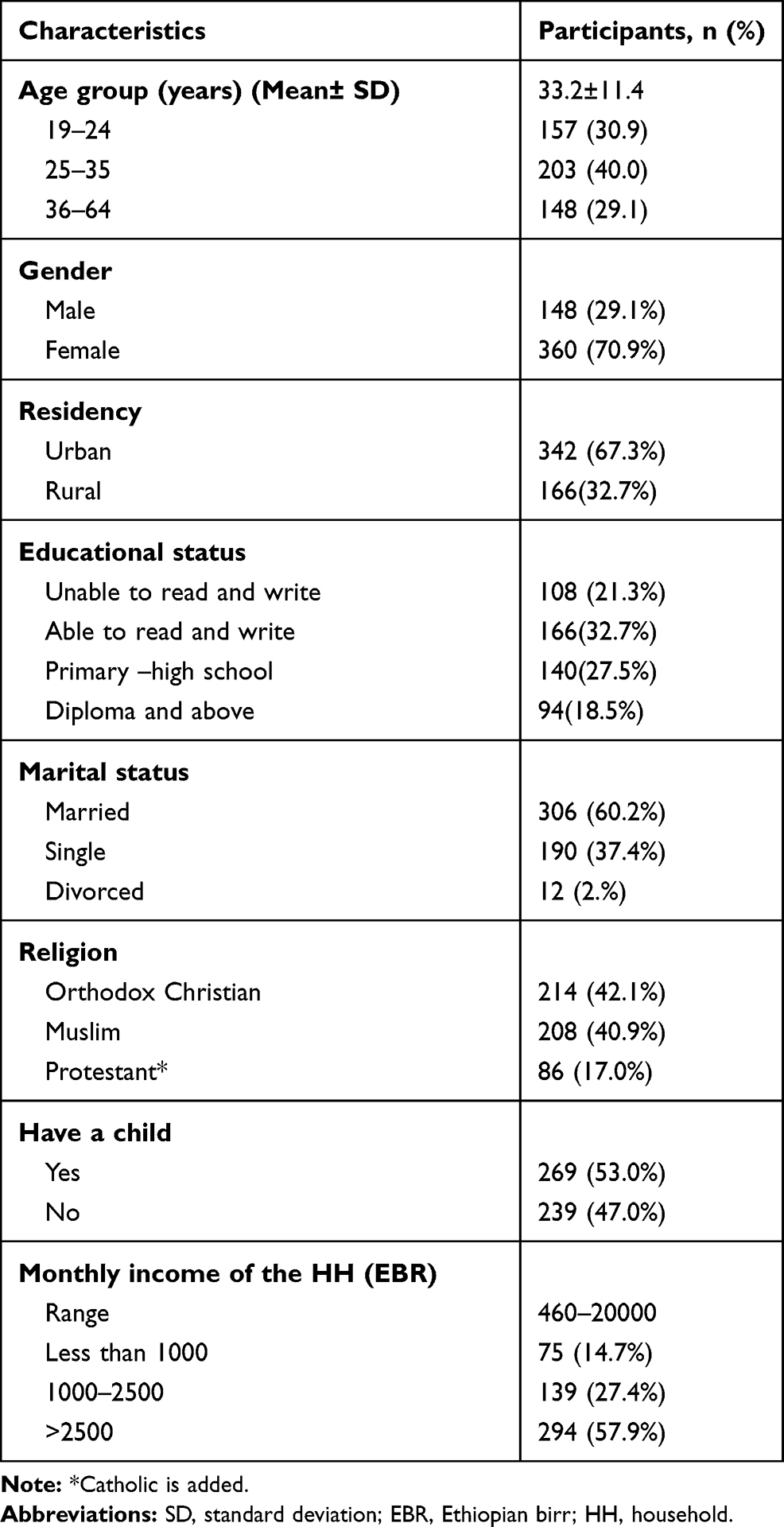 |
Table 1 Sociodemographic Characteristics of the Participants (n=508) |
Participants Attitude Towards COVID-19
The participants’ attitude was addressed by computing the summary score of all the questions. The overall prevalence of participants’ agreement towards COVID-19 was 49.6% (95% CI: 45.3–53.9%). The majority of the participants 402 (95.8%) agreed that COVID-19 is a grim health issue for the whole community members. They believed that the cure rate of COVID-19 is high 212 (41.7%). Likewise, almost all of the participants agreed that elders with comorbidity are more at risk of dying from COVID-19 than younger people. Three hundred sixty-eight (72.4%) of 508 participants believe that adult populations have fewer odds of being infected by SARS-CoV-2 compared to the elders and children of under-five age. A too-small proportion of the participants believed that they refrain from going to overcrowded sites such as a religious place to escape from COVID-19 pandemic. Similar to this, roughly half, 243 (47.8%) of the respondents believed that COVID-19 is emerged because of the sin of human beings. Attitude towards COVID-19 is shown in Table 2.
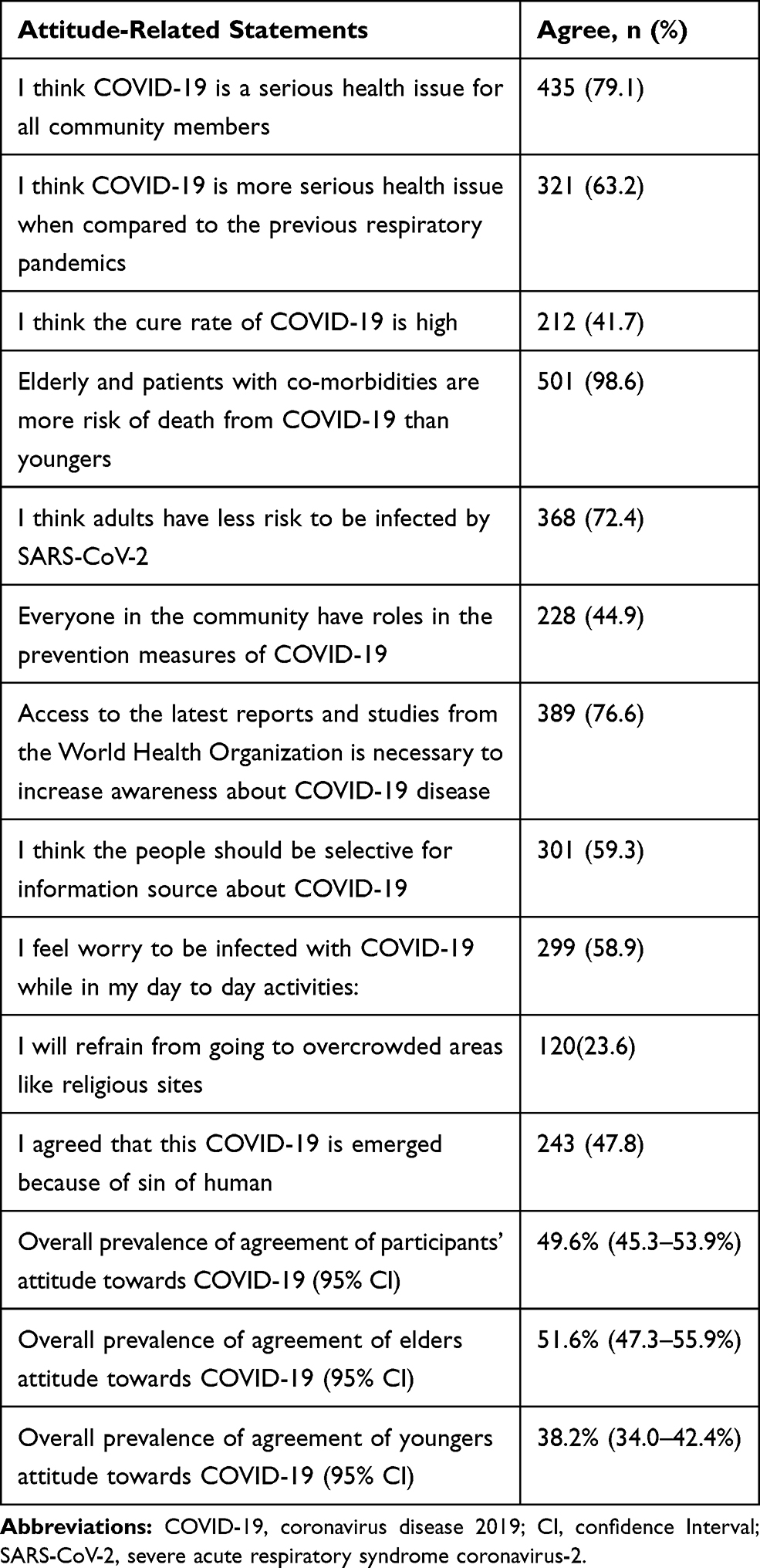 |
Table 2 The Frequency of Participants’ Attitude Towards COVID-19 (N= 508) |
Participants Practice Against COVID-19 Prevention
This study revealed the indications of staying at home unless a must to leave the house. Less than half, 248 (48.8%) of the participants reported that they stay at home. But they leave from home if there is an obligation to get out. Furthermore, the prevalence of physical distancing, wear a mask, wash hands at least for 20 seconds in every object touch, and apply sanitizer during every object touch were 108 (21.3%), 206 (40.6%), 52 (10.2%), 143 (28.2%), respectively. The overall prevalence of the indication for practice in prevention measures of COVID-19 was 53.3% (95% CI: 49.0–57.6%)). The practices of prevention against COVID-19 are shown in Table 3.
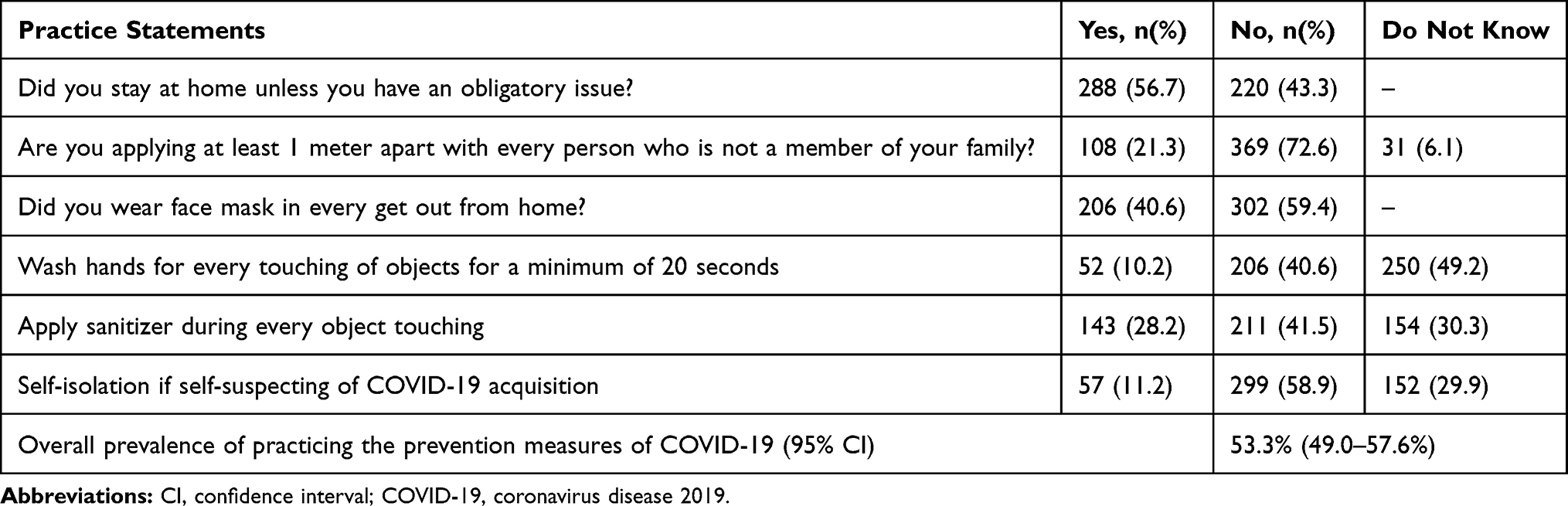 |
Table 3 Participants Practices of the Prevention Measures of COVID-19 (n=508) |
Factors Associated with Practice of COVID-19 Prevention Measures
Using the Chi-Square analysis, this study found that age, residency, educational status, marital status, having a child, income, and attitude towards COVID-19 were factors associated with the practice of protective measures against COVID-19.
This study revealed that there was enough evidence to support the claim that the practice of COVID-19 prevention measure is dependent on age (x2= 37.5; p=0.005) that adults and elders differ in their prevention practice against COVID-19.
Regarding residency, there was a shred of evidence to support the practice of the participants against COVID-19 prevention measures associated with their setting. This note indicates that there was a difference in practicing COVID-19 prevention measures among rural and urban residents.
As depicted in Table 4 below, participants had an opportunity to implement the precautionary measures of COVID-19 depending on their educational status.
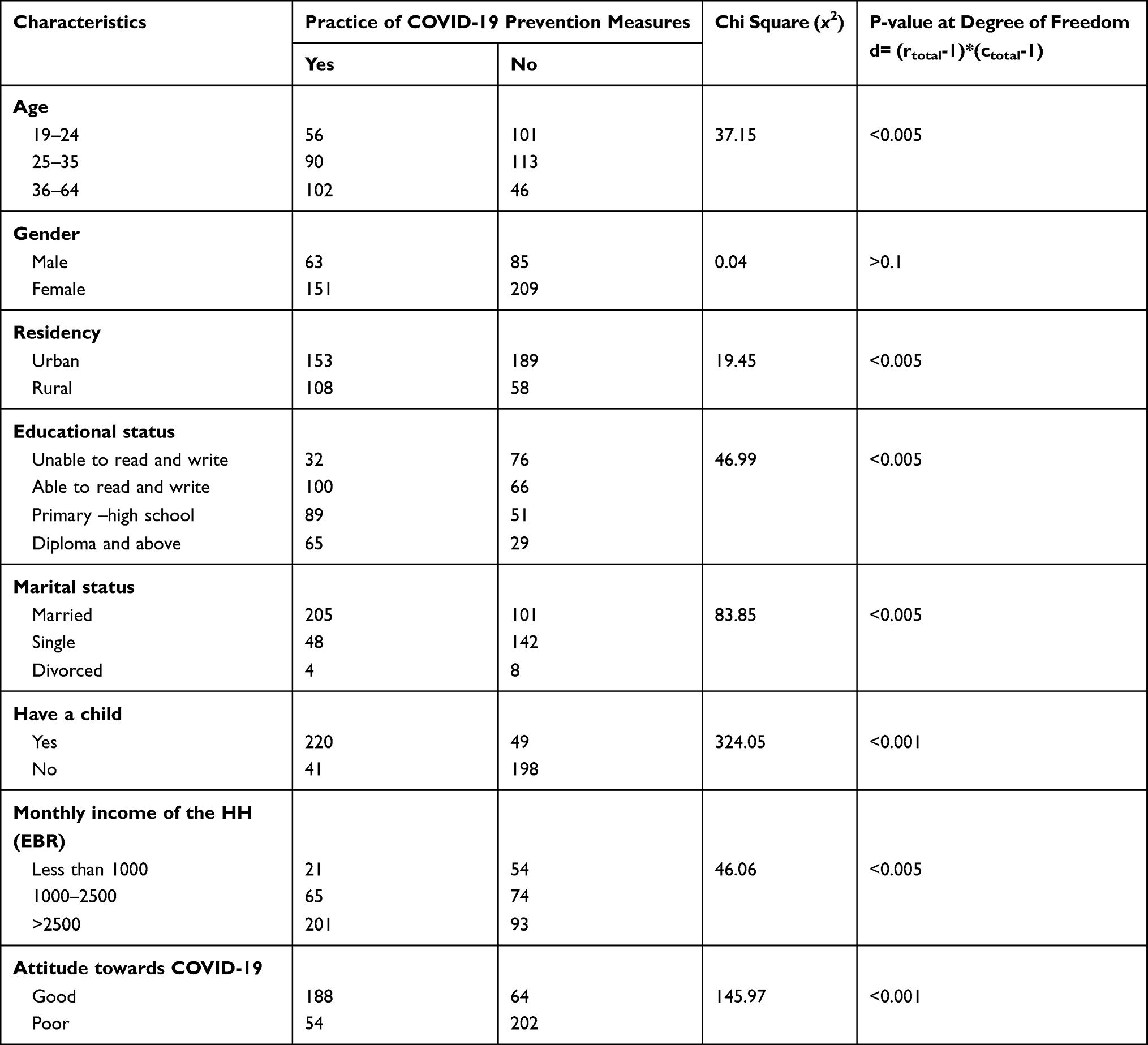 |
Table 4 Factors Associated with Participants Practice of COVID-19 Prevention Measures |
Moreover, there was a difference in the practice of COVID-19 prevention measures among the different marital statuses, number of children, level of monthly income, and attitude towards COVID-19. Factors associated with the practices of prevention against COVID-19 are shown in Table 4.
Factors Explored by FGD
Two focus group discussions were conducted among the participants of this study. The arrangement of the groups was formed based on the participants’ practice for COVID-19 prevention methods. One group comprises participants practicing the six prevention measures used in this study, while the other group comprised of those who did not practice. The group formation was; participants practicing the six prevention measures completely (g1n1=12) and participants who did not practice the prevention measures (g2n2=10). The two groups contain equal numbers by gender.
The mean age of males was 36, while the female was 29 years of age.
Eight of group 1 and seven of group 2 participants were married during the discussion. Regarding religion, four, six, and two from group 1 and four, four, and two from group 2 are Muslims, Orthodox Christians, and Protestants.
According to the group discussions, divine belief, economic problem, reluctance, and small numbers of visible COVID-19 cases/deaths in Ethiopia compared to the rest of the world are the main factors explored.
Most respondents reported that they believe COVID-19 emerged because of the extreme sins of the population. People are doing activities that are forbidden or not allowed by God.
Nowadays, I think we human beings are being non-spiritual. We forgot the presence of God. We are putting ourselves in the place of God. We have a shortage of knowledge to differentiate our responsibility from God’s responsibility. We took everything that we did are holy works. Hence, I believe that this COVID-19 pandemic has emerged to punish us. (g1, p4)
G2, p10 said,
I shared the divine belief of this pandemic occurrence. Of course, God did not catastrophically punish people, but it is happened due to our sin. There are also people who believe like me.
In contradiction, a few participants believe that the emergence of COVID-19 is not because of people’s sin. Instead, it is nature.
SARS-CoV-2 is a virus which is created by God during the period when God creates nature. Therefore, I did not believe that the disease was a newly emerged virus. And it is not raised because of our sin. I know that God could not punish us with such a catastrophic disease, but he forgives us when we did sin. (g2, p8)
Regarding the economy, the participants responded as they are not able to buy many face masks daily, sanitizer, and soap for handwashing. This implies that the low economic status of the respondents is the main hindering factor to use COVID-19 prevention measures.
There are so many people who afford to cover their daily prevention materials. They are also capable to help others. But in myself, I am not at a level of covering my daily prevention materials. I have tried to use face masks by using washable masks, but sanitizers and soaps are too costly. (g1, p5)
Although there is an economic problem, the participants did not deny exploring whether there are wealthy and charity-minded people who aid others.
The reluctance of the participants was the other factor explored for the reason that people are not using prevention measures against COVID-19. The majority of the participants (eight from g1, 7 from g2) reported a high level of reluctance to practice the prevention measures of COVID-19.
I was very worried at the beginning of the pandemic. Because of that, I have applied the prevention measures of the disease. Nonetheless, I am not bothering to use the prevention measures now. (G1, p12)
Moreover, the respondents reported that the small numbers of visible COVID-19 cases/deaths in Ethiopia compared with other countries is the main reason that people are not practicing the prevention methods of COVID-19.
We did not see any person acquire COVID-19 or die because of this disease in our setting (some specific area). We only heard by the news that there are people infected, severely ill, and died. Seeing is more witness than hearing. Therefore, we bored to practice those prevention methods of COVID-19 every day. (g2, p6)
In contrast, there were also people strictly practicing prevention measures. G2, P7 said
the disease has a catastrophic effect on people. For example, I saw a person who died who came from the United Arab Emirates. We have heard millions have died in the world. So, I advised everyone should use COVID-19 prevention methods.
Discussion
Currently, Corona Virus Disease 2019 is a pandemic illness causing the deaths of millions in the world. Despite the small number of cases recorded in Ethiopia compared to the rest world, the government took significant measures from the beginning to limit the spread of the disease and reduced the number of cases, which in turn led to a report of small numbers of deaths. Various segments of the people of Ethiopia, especially physicians who are considered the main focus of the medical structures have contributed to this achievement. Likewise, community engagement in the country contributes a vital role in the prevention of COVID-19. Therefore, this study was targeted to assess the attitude and practice of preventive measures among the community members. Presently, the transmission of SARS-CoV-2 occurs primarily via direct contact,16 airborne,23–25 fecal-oral.26 Therefore, the community members must recognize the possible routes of transmission since direct contact with contaminated surfaces and the virus’s ability to stay alive on-air are more vulnerable to them being infected.
This study revealed that the overall unacceptable attitude of the participants towards COVID-19 was high, 49.6% (95% CI: 45.3–53.9%). More than half of the participants believed that adults are less at risk for COVID-19. This finding is similar to the study in Korea27 and a systematic literature review report,28 in which people more than 70 years and children of 1–5 years old are more acquired COVID-19. Although children of all ages can get COVID-19, they appear to be affected less commonly than adults.29,30 The overall attitude of elders towards COVI-19 prevention practice was higher 51.6% (95% CI: 47.3–55.9%) compared with the youngers 38.2% (95% CI: 34.0–42.4%). This might be due to the population believing that elders are more at risk to COVID-19 of unfavorable outcomes. Besides, the difference might be attributed to that elders are more worried about their family than youngers.
Information is a tool that can be a cause for declining or improving any issue in the globe. In the current global crisis, the follow-up of medical information from reliable sources is one of the crucial reasons that helped the community to enhance their good practice and positive attitudes toward COVID-19. However, only 59.3% of the participants agreed that people must be selective in the acquisition of medical information. According to the finding from a study,31 at least 40% of information shared on social media is fake, of which 20% is hazardously fake. This result implies that being selective and cascaded information from the responsible body is mandatory.
Surprisingly, about half, 243 (47.8%) of participants believe that COVID-19 emerged because of the sins of human beings. The finding indicates that there is undone homework for the government and the religious leaders to convince the community that the disease might not be as they believe. Otherwise, morbidity and mortality rates will be projected unexpectedly.
Furthermore, it is crucial for Ethiopians difficult to apply social distancing, prone to increase morbidity and mortality rates. Likewise, in Ethiopia, there is a poor culture to accept new technology/approach or unfamiliar culture (such as face mask), which will rise COVID-19 morbidity. This finding was similar to several studies where they reported that the effective application of prevention measures against COVID-19 could decrease morbidity and mortality rates.1,16,32
To limit the COVID-19 pandemic, prevention at the individual level has a significant role. The current study emphasizes the various critical aspects associated with the selection of different preventive gadgets such as hand hygiene, personal protective equipment that constrain the global speedy spread of CoVID-19 infections. However, it is worthwhile to recognize the population groups who did not know the prevention measures against COVID-19. This study found out that half 250 (49.2%) of 508 participants did not know whether or not they should wash their hands for 20 seconds after they touch the inanimate surface. Similarly, around 154 (30.3%) of the participants did not know about the use of sanitizer for disinfection of hands. This finding contradicted the WHO technical guideline about COVID-19 prevention measures.33 This implies that the government and other responsible bodies have intensive homework to take effective and efficient prevention measures.
It is not hidden that community members face challenges in their daily life. There are so many social interactions among Ethiopians such as grief sharing, happiness festivals, and aiding the poor. Due to this fact, it is difficult to practice the COVID-19 prevention measures like; social/physical distancing, staying at home, buying and wearing face masks, and sanitizers. Although 288 (56.7%) of the participants were staying at home, less than half, 108 (21.3%), 206 (40.6%), 52 (10.2%), and 143 (28.2%) kept 1 meter apart from others, wear a face mask, wash hands, and apply sanitizer, respectively. The result is similar to a review34 that the critical and current effective prevention methods of COVID-19 transmission are practiced rarely. However, the finding is contradicting the WHO recommendation that physical distancing, hand washing, use of sanitizer, and staying at home are the effective prevention methods of COVID-19.33,35 This difference might be due to the discrepancy between what it is and what it should be.
In this study, some socio-demographic characteristics of participants were found to be statistically associated with infection prevention practice among the Ethiopian residents. These were age, residency, educational status, monthly income of the household, having a child, and attitude towards COVID-19. This finding is consistent with previous studies.33,36–38 In contradiction to the studies,36,38 this study revealed that gender had no association with the practice of COVID-19 prevention.
To the best of my knowledge, this study is the first study in Ethiopia that investigates the practice and divine belief toward the COVID-19 pandemic at the community level. The strength of the study is that the sample size was large enough that increase the generalizability of the findings. However, there are limitations that the investigator noted to the readers. The cross-sectional nature of the design used might lack to ascertain a causal association. Similarly, this study employed a chi-square statistical measure of association, which lacks to explore the direction of the association. Furthermore, the lack of standardized tools to assess attitude and practice was another limitation of this study. Finally, the investigator noticed the future researcher quantifies the factors explored by the qualitative part of this study.
Conclusions
Currently, COVID-19 continues to be a priority public health problem of the globe. The pandemic is exacerbated in the developing world in which poor health infrastructures and medication systems have existed. The outcome of the pandemic in countries like Ethiopia will worsen with the lesser application of prevention measures and the poor attitude of the people towards the COVID-19 pandemic. Therefore, it is critical to implement appropriate and effective practice approach and proactive attitudes toward COVID-19, which will decrease the incidence and mortality rate in Ethiopia. Moreover, the policymakers must combine the participants’ divine belief towards COVID-19 with their religious ideology, which will improve the implementation of prevention methods against the disease.
Ethical Approval and Consent to Participate
Ethical approval was obtained from the Review Committee of College of Medicine and Health Sciences, Wollo University with a reference number of Ref.No/CMHS/301/028/2012. The survey was anonymous to maintain the privacy and confidentiality of all information collected in the study. The ethical committee also approved to use of verbal consent of study participants unless personal identifiers are used. Eligible participants were included voluntarily and were not compensated. Verbal informed consent was ensured from each participant to obtain the necessary data and consent for publication. They were also told their rights in discontinuing or not responding to the interview. All over, the risks, burdens, and benefits that the participants will take were following the Declaration of Helsinki.
Acknowledgments
I am grateful to acknowledge the COVID-19 surveillance system evaluation team members of Wollo University, data collectors, and the study participants.
Funding
There is no funding to report.
Disclosure
The author reports no conflicts of interest for this work.
References
1. Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N Engl J Med. 2020;382(13):1199–1207. doi:10.1056/NEJMoa2001316
2. Tan W, Zhao X, Ma X, et al. A novel coronavirus genome identified in a cluster of pneumonia cases—Wuhan, China 2019− 2020. China CDC Weekly. 2020;2(4):61–62.
3. Adhikari SP, Meng S, Wu Y-J, et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: a scoping review. Infect Dis Poverty. 2020;9(1):1–12.
4. Organization WH. Novel coronavirus—China. 2020. Available from: http://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en.
5. Takian A, Raoofi A, Kazempour-Ardebili SJL. COVID-19 battle during the toughest sanctions against Iran. Lancet. 2020;395(10229):1035. doi:10.1016/S0140-6736(20)30668-1
6. Le Bert N, Tan AT, Kunasegaran K, et al. SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls. Nature. 2020;584(7821):457–462. doi:10.1038/s41586-020-2550-z
7. Wang Y, Wang Y, Chen Y, Qin QJ. Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID‐19) implicate special control measures. J Med Virol. 2020;92(6):568–576. doi:10.1002/jmv.25748
8. Wu A, Peng Y, Huang B, et al. Genome composition and divergence of the novel coronavirus (2019-nCoV) originating in China. Cell Host Microbe. 2020;27(3):325–328. doi:10.1016/j.chom.2020.02.001
9. Liu Y, Gayle AA, Wilder-Smith A, Rocklöv J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J Travel Med. 2020;27(2). doi:10.1093/jtm/taaa021
10. Singla R, Mishra A, Joshi R, et al. Human animal interface of SARS-CoV-2 (COVID-19) transmission: a critical appraisal of scientific evidence. Vet Res Commun. 2020:1–12.
11. Chan JF-W, Yuan S, Kok K-H, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet. 2020;395(10223):514–523. doi:10.1016/S0140-6736(20)30154-9
12. Li C, Ji F, Wang L, et al. Asymptomatic and human-to-human transmission of SARS-CoV-2 in a 2-family cluster, Xuzhou, China. Emerg Infect Dis. 2020;26(7):1626.
13. Zhang W, Du R-H, Li B, et al. Molecular and serological investigation of 2019-nCoV infected patients: implication of multiple shedding routes. Emerg Microbes Infect. 2020;9(1):386–389. doi:10.1080/22221751.2020.1729071
14. Kitajima M, Ahmed W, Bibby K, et al. SARS-CoV-2 in wastewater: state of the knowledge and research needs. Sci Total Environ. 2020:139076.
15. Elsamadony M, Fujii M, Miura T, Watanabe T. Possible transmission of viruses from contaminated human feces and sewage: implications for SARS-CoV-2. Sci Total Environ. 2020;755:142575. doi:10.1016/j.scitotenv.2020.142575
16. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323(13):1239–1242. doi:10.1001/jama.2020.2648
17. Rajgor DD, Lee MH, Archuleta S, Bagdasarian N, Quek SC. The many estimates of the COVID-19 case fatality rate. Lancet Infect Dis. 2020;20(7):776–777. doi:10.1016/S1473-3099(20)30244-9
18. Gilmore B, Ndejjo R, Tchetchia A, et al. Community engagement for COVID-19 prevention and control: a rapid evidence synthesis. BMJ Global Health. 2020;5(10):e003188. doi:10.1136/bmjgh-2020-003188
19. Bonell C, Melendez-Torres G, Viner RM, et al. An evidence-based theory of change for reducing SARS-CoV-2 transmission in reopened schools. Health Place. 2020:102398.
20. World Health Organization. Weekly bulletin on outbreak and other emergencies: week 2: 04–10 January 2021. 2021.
21. World Health Organization. Weekly bulletin on outbreak and other emergencies: week 51: 14–20 December 2020. 2020.
22. Seid YM. Innovations in data dissemination at the central statistical agency of Ethiopia. IASSIST Quarterly. 2010;33(3):26. doi:10.29173/iq380
23. Guo Z-D, Wang Z-Y, Zhang S-F, et al. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerg Infect Dis. 2020;26(7):1586.
24. Ding Z, Qian H, Xu B, et al. Toilets dominate environmental detection of SARS-CoV-2 virus in a hospital. MedRxiv. 2020.
25. Chia PY, Coleman KK, Tan YK, et al. Detection of air and surface contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in hospital rooms of infected patients. MedRxiv. 2020.
26. Jiang F, Deng L, Zhang L, Cai Y, Cheung CW, Xia ZJ. Review of the clinical characteristics of coronavirus disease 2019 (COVID-19). J Gen Intern Med. 2020;35:1545–1549.
27. Jung C-Y, Park H, Kim DW, Choi YJ, Kim SW, Chang T. Clinical characteristics of asymptomatic patients with COVID-19: a nationwide cohort study in South Korea. Int J Infect Dis. 2020;99:266–268. doi:10.1016/j.ijid.2020.08.001
28. Ludvigsson JF. Systematic review of COVID‐19 in children shows milder cases and a better prognosis than adults. Acta Paediatrica. 2020;109(6):1088–1095. doi:10.1111/apa.15270
29. Lu X, Zhang L, Du H, et al. SARS-CoV-2 infection in children. N Engl J Med. 2020;382(17):1663–1665. doi:10.1056/NEJMc2005073
30. Zimmermann P, Curtis N. Coronavirus infections in children including COVID-19: an overview of the epidemiology, clinical features, diagnosis, treatment and prevention options in children. Pediatr Infect Dis J. 2020;39(5):355.
31. Waszak PM, Kasprzycka-Waszak W, A K. The spread of medical fake news in social media–the pilot quantitative study. Health Policy Technol. 2018;7(2):115–118. doi:10.1016/j.hlpt.2018.03.002
32. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–1069. doi:10.1001/jama.2020.1585
33. Organization WH. Coronavirus disease 2019 (COVID-19): situation report, 82. 2020.
34. Ferdous MZ, Islam MS, Sikder MT, Mosaddek ASM, Zegarra-Valdivia J, Gozal D. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: an online-based cross-sectional study. PLoS One. 2020;15(10):e0239254. doi:10.1371/journal.pone.0239254
35. World Health Organization. Coronavirus disease (COVID-19): situation report, 185. 2020.
36. Saqlain M, Munir MM, Ur Rehman S, et al. Knowledge, attitude, practice and perceived barriers among healthcare professionals regarding COVID-19: a Cross-sectional survey from Pakistan. J Hosp Infect. 2020;105:419–423.
37. Ivey MF. Global opportunity: pharmacists working together to improve patient care. Am J Health Syst Pharm. 2019;76(12):869–872. doi:10.1093/ajhp/zxz071
38. Hussain R, Hassali MA, Hashmi F, Farooqui M. A qualitative exploration of knowledge, attitudes and practices of hospital pharmacists towards adverse drug reaction reporting system in Lahore, Pakistan. J Pharm Policy Pract. 2018;11(1):16. doi:10.1186/s40545-018-0143-0
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.