")
Back to Journals » Clinical Interventions in Aging » Volume 15
Potentially Inappropriate Prescriptions in Ambulatory Elderly Patients Living in Rural Areas of Romania Using STOPP/START (Version 2) Criteria
Authors Buda V , Prelipcean A, Andor M , Dehelean L, Dalleur O, Buda S, Spatar L, Mabda MC, Suciu M, Danciu C, Tudor A , Petrescu L, Cristescu C
Received 3 October 2019
Accepted for publication 29 January 2020
Published 19 March 2020 Volume 2020:15 Pages 407—417
DOI https://doi.org/10.2147/CIA.S233270
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Valentina Buda,1,* Andreea Prelipcean,2,* Minodora Andor,3,* Liana Dehelean,4,* Olivia Dalleur,5 Simona Buda,2 Lavinia Spatar,2 Maria Cristiana Mabda,1 Maria Suciu,1 Corina Danciu,6 Anca Tudor,7 Lucian Petrescu,8,9 Carmen Cristescu1
1Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, “Victor Babeş” University of Medicine and Pharmacy, Timisoara, Romania; 2“Victor Babeş” University of Medicine and Pharmacy, Timisoara, Romania; 3Department of Medical Semiotics, Faculty of Medicine, “Victor Babeş” University of Medicine and Pharmacy, Timisoara, Romania; 4Discipline of Psychiatry, Department of Neurosciences, Faculty of Medicine, “Victor Babeş” University of Medicine and Pharmacy, Timisoara, Romania; 5Clinical Pharmacy Research Group, Louvain Drug Research Institute, Université catholique de Louvain UCLouvain, Bruxelles, Belgium; 6Department of Pharmacognosy, Faculty of Pharmacy, “Victor Babeş” University of Medicine and Pharmacy, Timisoara, Romania; 7Department of Statistics and Biomedical Informatics, Faculty of Pharmacy, “Victor Babeş” University of Medicine and Pharmacy, Timisoara, Romania; 8Department of Cardiology VI, Faculty of Medicine, “Victor Babeş” University of Medicine and Pharmacy, Timisoara, Romania; 9Cardiovascular Diseases Institute, Timisoara, Romania
*These authors contributed equally to this work
Correspondence: Valentina Buda
Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, “Victor Babeş” University of Medicine and Pharmacy, 2 Eftimie Murgu Street, Timisoara 300041, Romania
Tel/Fax +40-256-494-604
Email [email protected]
Background: Rational use of medications and monitoring of prescriptions in elderly patients is important to decrease the number and duration of hospitalizations, emergency medical consultations, mortality, as well as medical costs.
Purpose: To identify potentially inappropriate medications (PIMs) and potential prescription omissions (PPOs), and determine their prevalence based on the Screening Tool of Older Persons’ potentially inappropriate Prescriptions (STOPP) v2 criteria and Screening Tool to Alert doctors to Right Treatment (START) v2 criteria for patients aged > 65 years.
Methods: This cross-sectional study was conducted in two rural counties in Romania based on electronic prescriptions for chronic conditions (EPCCs) issued from 30 days to 90 days by a specialist or general practitioner. Collected EPCCs were evaluated by an interdisciplinary team of specialists based on 26 STOPP v2 criteria and 10 START v2 criteria.
Results: PIM prevalence was 25.80% and PPO prevalence was 41.72% for 646 EPCCs. The mean age of patients was 75 years and the mean number of drugs per EPCC was four. The most frequently identified PIMs were treatment duration (6.65%), theophylline administration (5.72%), drug indication (4.64%), cyclo-oxygenase-2 non-steroidal anti-inflammatory drugs (1.39%), and zopiclone prescription (0.77%). Statins (24.76%), beta-blockers (8.04%), and beta-2 agonist/antimuscarinic bronchodilators (5.88%) were the most frequently identified PPOs.
Conclusion: PPOs were more prevalent than PIMs for elderly populations living in the two rural counties in Romania we studied. Health practitioners (family physicians, specialists, and pharmacists) should focus on prophylactic and curative considerations when prescribing agents to decrease the morbidity and mortality of elderly rural Romanian patients.
Keywords: Romanian elderly, rural zones, chronic prescriptions, STOPP, START
Introduction
In 2019, the number of Romanians aged >65 years represented ~18.2% of the country’s total population.1
The Eurostat (Brussels, Belgium) predictions for 2100 estimate a significant increase in the number, but also in the complexity of the pharmacotherapeutic approaches for the elderly (secondary to increased life expectancy and migration). Therefore, aged people will represent ~31.3% of the total population in the European Union, compared with 19.8% in 2018.1 Moreover, life expectancy will increase by ~7.8 years for men (from 78.3 in 2016 to 86.1 in 2070) and 6.6 years for women (from 83.7 in 2016 to 90.3 in 2070).2
Comorbidities and polymedication, together with the pharmacokinetic and pharmacodynamic particularities of drugs administered to the elderly, increase the risk of adverse reactions and potentially dangerous drug interactions by up to ~30%.3–5 This scenario leads to an increase in the number and duration of hospitalizations, emergency medical consultations, mortality, as well as medical costs in the elderly population.6–8 Therefore, it is very important to monitor prescriptions and to pursue rational utilization of drugs in this population. Appropriate prescribing of drugs will require special attention (age-centered and age-integrated new challenges) of health professionals: guidelines for appropriate prescription and higher-education programs for patients, as well as for medical practitioners.9,10
Primejdie et al assessed inappropriate prescribing in Romania. They showed disparities between community-dwelling and institutionalized patients regarding the prevalence of inappropriate prescribing in urban settings.11 Differences in the prevalence of inappropriate prescribing are also expected between urban and rural settings.12 Indeed, patients from rural areas have little access to specialist physicians for several reasons: high costs, infrastructure problems, patients’ level of education and awareness of the importance of being evaluated by a specialist.13 Also, some general practitioners (GPs) from rural areas (mostly over 50–60 years of age) prefer to prescribe their own treatment, without insisting that the patient should also be evaluated by a specialist. In addition, many patients from the countryside are treated by a GP for a lifetime, and reach a specialist or the hospital only if their chronic conditions worsen or decompensate.14 Therefore, a problem which will have to be solved in the future, due to the increasing number of elderly people,1 is to ease their access to specialized medical services to keep their diseases under control. Romania is currently confronted with an acute lack of specialist physicians in rural areas.14
In recent years, the concerns of medical specialists have been geared towards finding and applying appropriate criteria for prescribing drugs for each patient. Therefore, Screening Tool of Older Persons’ potentially inappropriate Prescriptions (STOPP) and Screening Tool to Alert doctors to Right Treatment (START) were designed to detect risk or inadequate prescriptions for elderly patients to optimize their pharmacotherapy.15 STOPP detects potentially inappropriate prescribing whereas START identifies necessary (but omitted) drugs that increase the efficiency of pharmacotherapy and prevent complications. STOPP/START criteria are suitable for hospitalized and community-dwelling patients.16,17
The main objective of our study was to identify and determine the prevalence of potentially inappropriate medications (PIMs) and potential prescription omissions (PPOs) based on STOPP/START v2 criteria for patients aged >65 years. The secondary objectives (not detected by STOPP/START v2 and not involved in PIMs or PPOs) of our study were identification of: (i) the most common chronic drug indications and prescribed drugs; (ii) prescribing errors (drugs prescribed at too low/too high a dose, diagnostic codes, number of erroneous day administrations); (iii) differences in prescription habits between the rural areas of two counties in Romania: Arad and Timis.
Patients and Methods
This cross-sectional study was conducted in Arad and Timis. The study included the analysis of the chronic treatment of patients based on electronic prescriptions for chronic conditions (EPCCs) issued over a period of 30, 60, or 90 days by specialist physicians or GPs. We included only EPCCs to have an overview of the main and predominant treatments taken by the elderly which could induce (due to the long administration period) major adverse events.
EPCC collection was done from eight rural community pharmacies. The analyzed prescriptions were reimbursed by the County Health Insurance Agency of Arad and Timis.
Data of the EPCCs were collected in the pharmacies within a 5-month period (November 2017 to March 2018). Duplicate EPCCs of the same patient, but at different times, were excluded.
EPCCs were gathered based on the following criteria: age of patient ≥65 years; living at home; chronic drug treatment (already taken for >3 months).
In Romania, the electronic prescription form can contain a maximum of seven drugs prescribed on the basis of the international drug name (IDN) or trade name; in the present study, most prescriptions were written in the IDN.18 They included only approved medications to be settled by health-insurance agencies, with over-the-counter (OTC) drugs and dietary supplements not being part of the reimbursement system.
The drugs included in the psychotropic list (eg, barbiturates, benzodiazepines, zolpidem – Table III) and narcotic list (eg, opioids – Table II) are released on the basis of a secured non-electronic prescription form, which is imposed by Romanian legislation.19 Hence, these types of prescriptions were not included in our study. Importantly, in Romania, zopiclone is not included in the psychotropic list and, therefore, can be prescribed on an electronic prescription.
All the collected EPCCs were evaluated (face-to-face meetings) by an interdisciplinary team of specialists (cardiologist, psychiatrist, neurologist, pulmonologist, rheumatologist, and gastroenterologist) as well as one family physician, three clinical pharmacists, one pharmacist, and two students of clinical pharmacy, based on a selection of STOPP/STARTv2 criteria.
Twenty-six STOPP criteria and 10 START criteria (Addendum Table A) could be applied to the database of this study based on the medication classes and medical conditions for which data were available (though the STOPP/START v2 criteria contain 80 STOPP criteria and 34 START criteria).15 The collected EPCCs did not contain all the required clinical data of patients (eg, glomerular filtration rate, potential hydro-electrolyte imbalances, cardiac frequency). Another impediment was that, based on the prescribing form, the diagnostic codes used did not provide additional data regarding the characteristics of the disease (eg, heart failure with maintained systolic ventricular function, type of arrhythmia) or its severity (eg, moderate, severe hypertension). Moreover, some of the comorbidities of the patients were identified based on diagnostic codes found in the EPCCs.
The secondary outcomes were identified based on the prevalence of the diagnostic codes from EPCCs (drug indications) and drug leaflets (prescribing errors). Another objective was to identify possible prescribing differences between the two counties because the municipality of Timis, Timisoara, is a prestigious university center going back more than 50 years.
Moreover, we verified if the age and sex of patients, number of drugs, and days of treatment were associated with the prevalence of PIMs and PPOs based on STOPP/START v2 criteria.
The present study was approved by the Ethics Committee of the “Victor Babes” University of Medicine and Pharmacy of Timisoara, Romania.
Statistical Analyses
Quantitative data are the mean ± standard deviation. Qualitative data are described using percentages. SPSS v17 (IBM, Armonk, NY, USA) was used to process data. Differences between the study groups represented by numerical independent data were obtained using the Mann–Whitney test. Differences between categorical data were obtained using the chi-squared test; p<0.05 was considered significant. Logistic regression was applied to see if age, number of drugs, days of treatment, and sex of patients were associated with the prevalence of PIMs and PPOs based on STOPP and START criteria. In this way, STOPP/START were considered dependent variables and the remainder of the variables were considered independent variables).
Results
A total of 982 EPCCs were included initially, from which 336 were excluded because they were duplicate EPCCs for the same patient at different periods of time. As a result, 646 EPCCs of 646 patients were gathered and analyzed. Of these, 221 EPCCs (34.21%) were from Arad and 425 EPCCs (65.79%) were from Timis.
Of the total number of EPCCs evaluated, 65% of them were written for female patients. The mean age of patients was 75–76 years.
We compared the collected data from the two study regions to ascertain if there were major differences in prescription habits between the counties.
Table 1 shows the demographic data for the EPCCs. There was no significant difference with regard to age between the two counties. Life expectancy is significantly higher for females than for males in both counties.20 Indeed, there were more EPCCs for females’ prescriptions (>50% of the total number of EPCCs evaluated) compared with those for males.
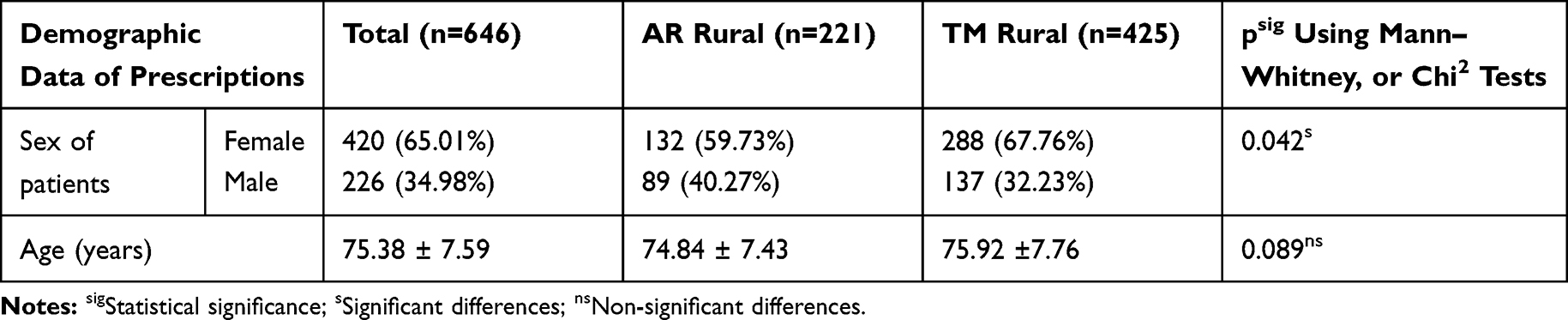 |
Table 1 Demographic Data of Prescriptions |
From the EPCCs collected, 97.21% were released by a GP (in Arad all the collected EPCCs were released by a GP). The mean number of medications contained on an EPCC was four, with the drugs usually being prescribed for 30 days (Table 2).
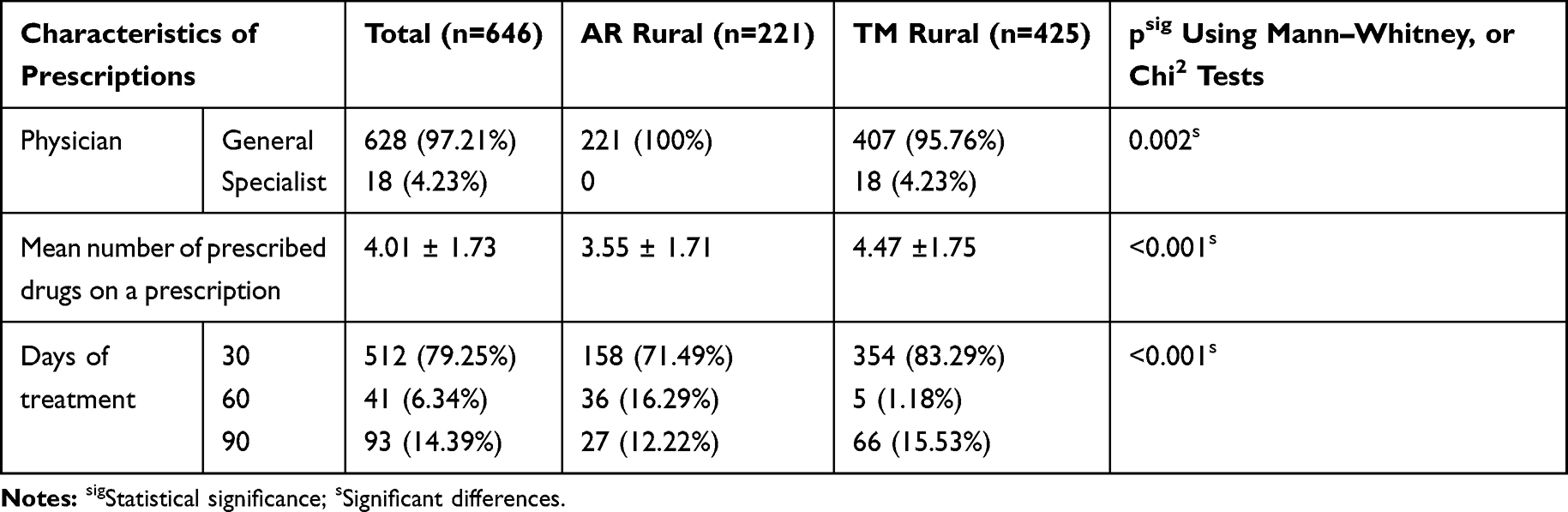 |
Table 2 Characteristics of Prescriptions |
Table 3 lists the most common diagnostic codes for the analyzed EPCCs. Cardiovascular diseases were the most common: essential hypertension (>70% of all EPCCs in both counties), chronic ischemic heart disease (24% in Arad versus 46% in Timis), dyslipidemia (23% versus 16%), and peripheral circulatory disorders (varicose veins of lower limbs, 8% versus 3%). Also, digestive disorders, such as gastritis and duodenitis (12% in Arad versus 20% in Timis), as well as chronic obstructive pulmonary disease (COPD, 4% versus 10%), and diseases of the prostate gland (~7% of all EPCCs in both counties) had important roles in the pyramid of diseases in these two counties.
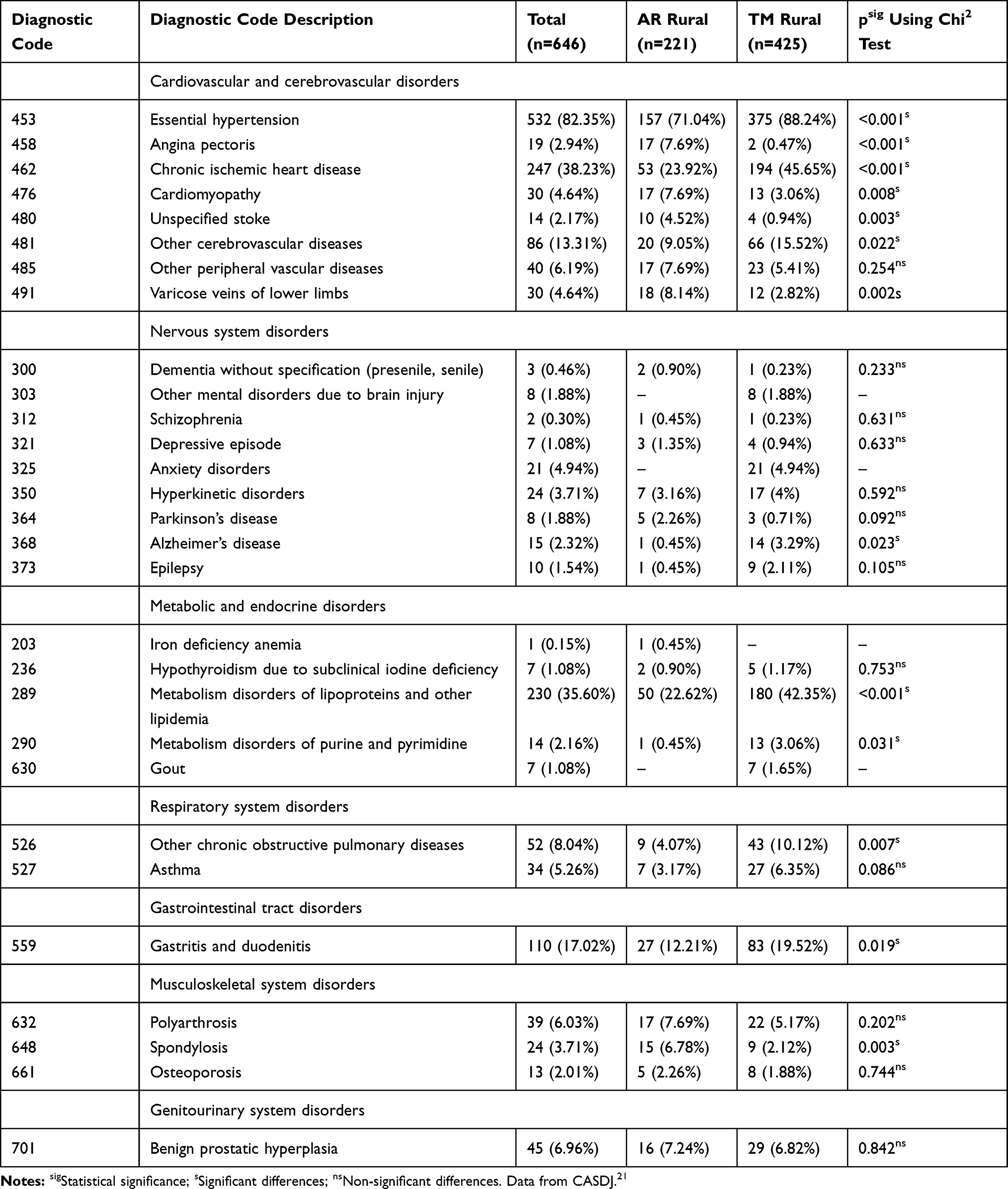 |
Table 3 The Most Used Diagnostic Codes as Indications for Prescriptions |
The most frequently prescribed drugs were beta-blockers (48% in Timis versus 38.46% in Arad), angiotensin-converting enzyme inhibitors (ACEIs) (47.76% versus 30.32%), statins (42.82% versus 28.96%), thiazide-like diuretics and calcium-channel blockers (Addendum Table B). Given that in Romania the prevalence of cardiovascular diseases is the highest, these data are not surprising.22
Compared with Arad, in Timis central-acting antihypertensive drugs were prescribed significantly more often (p=0.004), which was also seen for statins (p<0.001), antiepileptic drugs (p=0.039), theophylline (p=0.022), and allopurinol (p=0.003) (Addendum Table B).
Forty-three EPCCs revealed a problem regarding treatment duration. We identified 18 EPCCs (8.14%) in Arad versus 25 EPCCs (5.88%) in Timis in which drugs were prescribed for a long time (>2 weeks for non-steroidal anti-inflammatory drugs (NSAIDs) and >8 weeks for proton pump inhibitors (PPIs)). There was a tendency to prescribe PPIs and NSAIDs for long-term management of diseases, with NSAIDs ranked first in both counties (17% in Arad versus 20% in Timis) (Table 4).
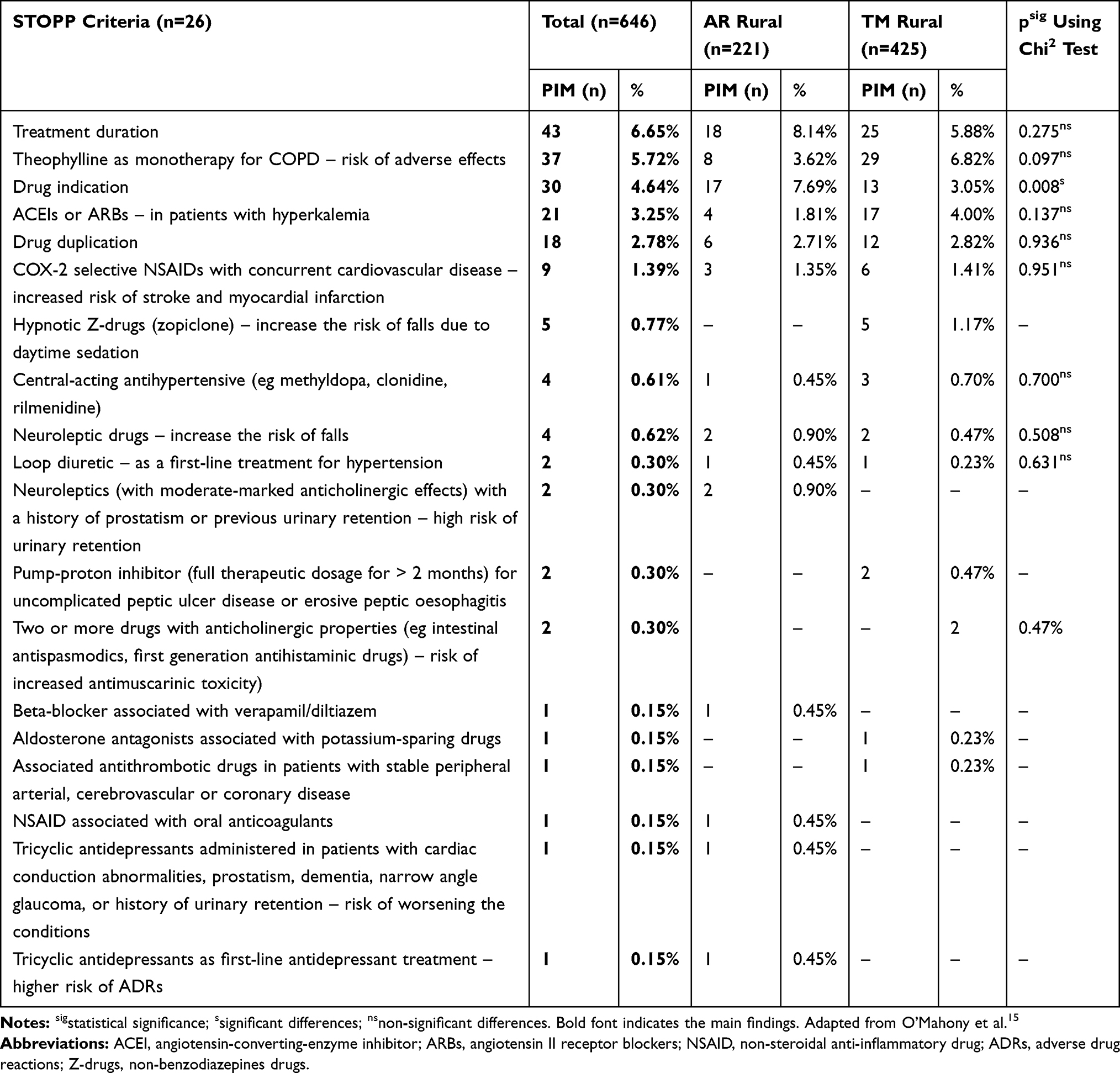 |
Table 4 STOPP Criteria Detected in Study Population |
Theophylline was prescribed as monotherapy in a high proportion of patients with COPD, most of whom were in Timis (6.62% versus 3.62%). Cyclooxygenase (COX)-2-selective NSAIDs were also prescribed in patients with cardiovascular problems (Table 4).
Altogether, 30 EPCCs had no valid drug indication. In Arad, the main problems related to the indication of drugs were dextromethorphan prescribed for bronchitis; trazodone for dementia; theophylline/gabapentin/desloratadine for chronic ischemic heart disease; furosemide for angina pectoris; first-generation antipsychotics for depressive episodes; trimetazidine for hypertension. In Timis, the PIMs identified were PPIs prescribed for bronchitis; beta-blockers for spondylosis; tramadol for lipidemia; propafenone/nitrate derivatives/trimetazidine for hypertension; tamsulosin for gastritis and duodenitis; alphacalcidol for arterial disease. Some of these problems could be the consequence of an error in typing the diagnostic code for the prescribed drug (Table 4).
Drug duplications were approximately identical in both counties (2.71% in Arad versus 2.82% in Timis). The main frequently duplicated pharmacologic classes/drugs were diuretics, beta-blockers, timolol (ophthalmic use), and NSAIDs (prescribed in two pharmacologic products for the same patients) (Table 4).
Three EPCCs contained a molecule from the central-antihypertensive class of drugs as first-line treatment. In 17 (4.00%) EPCCs, the patient was at risk of hyperkalemia due to the associations of drugs.
Overall, 25.80% of the analyzed EPCCs had at least one PIM. Timis had the most prescribing problems according to STOPP criteria (Table 5).
 |
Table 5 STOPP Prevalence (PIM – Potentially Inappropriate Medication) |
The prevalence of PPOs in our study population was 41.72%, with no significant difference between the two counties (though it was higher in Arad: 23.53%) (Table 6).
 |
Table 6 START Prevalence (PPO – Potentially Prescription Omissions) |
Table 7 presents the START criteria that were applied to the EPCCs included in our study. In the two rural areas studied, statins were poorly prescribed as prophylactic or curative drugs. The Romanian population presents a high cardiovascular risk22 and, in both counties, approximately 23–25% of EPCCs required co-administration of a statin. In addition, beta-blockers should be prescribed more often (especially in Arad), as well as beta-2 adrenergic or anticholinergic bronchodilators (especially in Timis). A first-line antihypertensive drug with proven efficacy over time (as recommended in international guidelines) should be prescribed more frequently, especially in Arad.
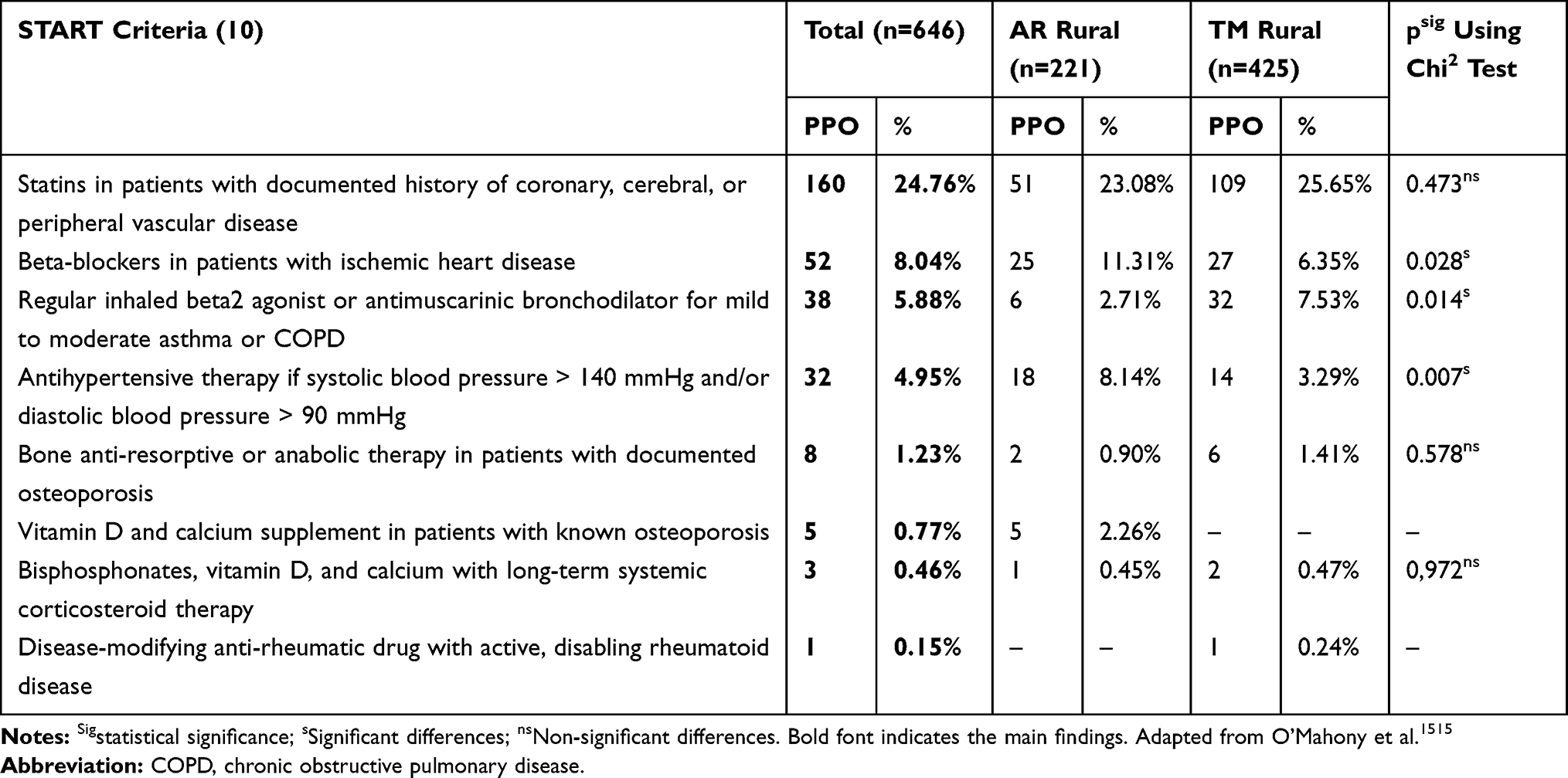 |
Table 7 The Applied START Criteria |
Only age and the number of drugs were significant predictors associated with the prevalence of PIMs and PPOs using STOPP and START v2 criteria (p<0.001 for both using logistic regression) (Tables 8 and 9).
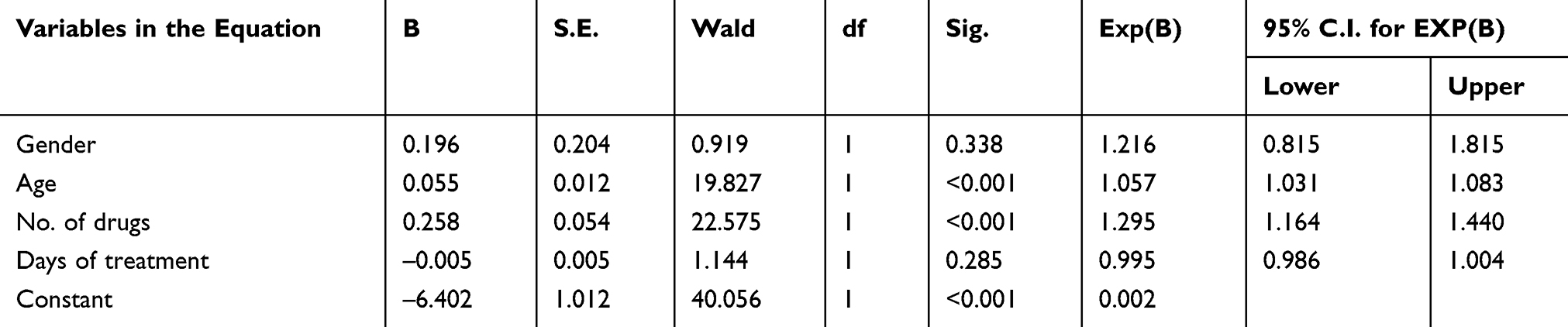 |
Table 8 Variables Associated with STOPP Prevalence |
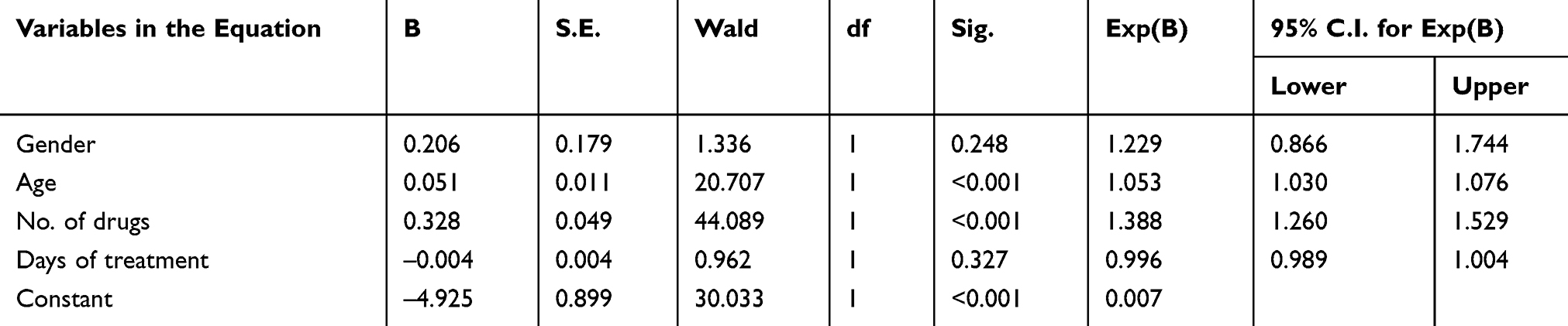 |
Table 9 Variables Associated with START Prevalence |
With regard to prescription errors (Table 10), the main problems were medications prescribed at too high a dose, and the number of administrations within 24 h.
 |
Table 10 The Prescription Errors Observed |
In Arad, 5.43% of EPCCs were prescribed at too low a dose based on the drug leaflet. For example, dextromethorphan (20 mg), pentoxifylline (400 mg), trimebutine (200 mg), nitrate derivatives, betahistine, and vincamine were prescribed only once a day. In Timis, the number of EPCCs containing drugs prescribed at too low a dose was lower (3.52%). For example, diosmin, nitrate derivatives, trimebutine, fenspiride, vincamine, nicergoline, and pramiracetam were prescribed only once a day. They were not considered PIMs.
The medications prescribed at too high a dose most often were beta-blockers, ACEIs, and dihydropyridines, which, in general, were prescribed at a maximum dose twice daily (a problem observed particularly in Arad).
Discussion
We evaluated EPCCs issued in two rural areas in Romania to people over 65 years of age. We found that 25.80% of patients had PIMs and 41.72% had PPOs according to STOPP and START v2 criteria. The most common PIMs were related to treatment duration (6.65%), theophylline administration (5.72%), drug indication (4.64%), COX-2-selective NSAIDs (1.39%), and zopiclone prescription (0.77%). The most frequent PPOs were statins (24.76%), beta-blockers (8.04%), and beta-2 agonist/antimuscarinic bronchodilators (5.88%).
Moreover, we conducted a separate analysis in the two counties to ascertain if there were major differences in prescribing habits. We found minor differences between the two counties with regard to potentially inappropriate prescribing.
Compared with the study undertaken by Primejdie et al in 2016, we found a lower prevalence of PIMs in these two rural areas compared with 34.49% reported for urban areas.11
In 2018, O’Riordan et al looked at PIMs in elderly people living in urban and rural settings in Ireland, Switzerland, and the Netherlands. They found that the highest percentage of PIMs was in elderly patients in Switzerland (16.7%), the Netherlands (12.5%), and Ireland (8.7%). With respect to START criteria, the prevalence of PPOs was lower for the elderly in Ireland (14%) compared with those in the Netherlands (24%) and Switzerland (25.3%).23 Our results show that for elderly people living in two rural counties of Romania, the prevalence of PIMs and PPOs was higher.
Other studies conducted in the ambulatory setting showed the prevalence of PIMs to vary from 27.3% (Serbia) to 57% (Ireland) and for the prevalence of PPOs to vary from 40.5% (Spain) to 73.3% (Turkey). In those studies, the most frequent PIMs were represented by PPIs, drugs without an indication, NSAIDs, and benzodiazepines, whereas PPOs were represented by statins, antiplatelet agents, calcium, and vitamin D.24–27
The most prevalent PIMs observed in our study are in accordance with those from other studies.28–32 A study in Romania by Primejdie et al in 2016 using the STOPP/START criteria of 2008 showed that the drug class with the highest percentage of use was NSAIDs (56.66% of outpatients and 35.63% of hospitalized patients), followed by benzodiazepines. That study did not assess PPOs.11 In our study, NSAIDs were the most prevalent drugs prescribed for >2 weeks. NSAIDs are recommended for use with caution in elderly patients for a short period of time and at a minimal therapeutic dose due to: (i) their side effects; (ii) an increased risk of falls and stroke.33
Regarding PPOs, we observed poor management for the prophylaxis of cerebrovascular or cardiovascular complications (acute myocardial infarction (AMI) or stroke) in elderly patients diagnosed with hypertension and/or coronary artery disease. Indeed, under-prescription of statins attested to this phenomenon. This poor management translates to a high prevalence of AMI or stroke, as reported by Eurostat as well as in Romania.22 Kovačeic et al also reported the under-prescription of cardiovascular drugs in Serbian patients with coronary, cerebral, or peripheral vascular disease.26 Moreover, for a country with a high prevalence of cardiovascular disease and cardiovascular events, apart from statins, beta-blockers should be prescribed for ischemic heart disease. Theophylline should be avoided in patients with cardiovascular complications, and beta-2 agonists/antimuscarinic bronchodilators should be first-line treatment.
We found a mean number of four drugs per EPCC to be consistent with the average reported in other studies of elderly patients living in Europe.23,27 Moreover, a study conducted in Serbia concluded that utilization of >4 medications prescribed to the elderly could be linked to a higher probability of having a PIM.26 A study conducted in 2016 by a Romanian research team stated that the median number of prescribed medications in elderly patients was three.11
Psychotropic medications were prescribed mostly in Timis. These were represented by new, well-chosen drugs according to international recommendations (most probably as a consequence of being prescribed by specialists).34,35 Conversely, the EPCCs collected in Arad had a lower percentage of psychotropic drugs (probably because most were penned by a GP).
The predominant diseases in Romania are cardiovascular diseases according to Eurostat. These are followed by metabolic and endocrine disorders, diseases of the gastrointestinal tract, respiratory system, and nervous system.22 Use of STOPP and START criteria in rural regions could help rationalize curative and preventive medications for these conditions, along with non-pharmacologic measures (ie, good diet, exercise, smoking cessation, as well as periodic monitoring of body weight, blood pressure, heart rate, lipid/carbohydrate profile, and laboratory investigations36) addressed in concert with a GP and pharmacist.37
Despite limited access to physicians in rural areas, we observed that EPCCs from GPs were, in general for 30 days. Hence, the GP could monitor outcomes and adjust (as appropriate) the treatment regimen and drug dose.
With regard to prescription errors not detected using STOPP and START v2 criteria, the highest share was represented by the prescription of some drugs under the therapeutic dose (which could lead to therapeutic failure), dosing regimen, and an unadjusted dose in accordance with disease stage or based on patients’ characteristics. Calcium-channel blockers were among the medications at which too high a dose was prescribed (the maximum dose used was twice daily).
Our study had three main limitations. First, the frailty of patients was not recorded. Second, we could apply only a subset of STOPP and START v2 criteria because the database available did not cover all the required elements to assess all criteria. The prevalence of PIMs and PPO should, therefore, be interpreted with caution.38 Due to lack of data, we could not identify certain omissions of anticoagulants in chronic atrial fibrillation; Getachew et al noted their absence in 41.2% of elderly patients.39 Third, we did not include data regarding vaccination or OTC medications (eg, aspirin or laxatives). Physicians and pharmacists should monitor the adherence of patients to OTC drugs and cardiovascular aspirin therapy to avoid under-prescribing of such agents.
We also noticed positive aspects that reflect adequate prescription of medications in the elderly. For instance: allopurinol was prescribed for hyperuricemia; topical anti-glaucoma drugs were chosen for glaucomatous disease; second-generation antipsychotics were recommended for psychomotor agitation; second-generation anti-allergic drugs were recommended appropriately.
Access to medical care in rural regions is challenging. More than in other settings, the network of healthcare professionals is important, and the pharmacist can play a key part in detection of inappropriate prescribing. The importance of the pharmacist in identifying potentially inadequate prescriptions based on STOPP/START criteria has been documented.40,41 In 2016, Tommelein et al developed an explicit screening tool which could PIMs in community pharmacies.42 Optimization of drug therapy by a clinical pharmacist can improve the quality of care and lower the costs of polymedication.43
Conclusions
PPOs were more prevalent than PIMs for elderly populations living in the two rural counties in Romania we studied. Health practitioners (family physicians, specialists, and pharmacists) should focus on prophylactic and curative considerations when prescribing agents to decrease the morbidity and mortality of elderly rural Romanian patients.
Disclosure
Dr Liana Dehelean reports personal fees from Johnson and Johnson, Lundbeck, Eli Lilly and Angelini, outside of the submitted work. The authors report no other conflicts of interest in this work.
References
1. Eurostat. Population structure and ageing; 2019. Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Population_structure_and_ageing&oldid=298662.
2. European Commission. The 2018 ageing report: economic and budgetary projections for the EU member states (2016–2070); 2018. Available from: https://ec.europa.eu/info/sites/info/files/economy-finance/ip079_en.pdf.
3. National Institute of Statistics Romania. Health status of the population in Romania (Institutul Naţional de Statistică România. Starea de sănătate a populaţiei din România); 2015:321. Available from: http://www.insse.ro/cms/sites/default/files/com_presa/com_pdf/sanatate2015r_0.pdf.
4. Ruiter R, Visser LE, Rodenburg EM, et al. Adverse drug reaction - Related hospitalizations in persons aged 55 years and over: a population-based study in the Netherlands. Drugs Aging. 2012;29(3):225–232. doi:10.2165/11599430-000000000-00000
5. Sferrazza G, Nicotera G, Pierimarchi P. Suspected adverse drug reactions (ADRs) trends in older Italian patients: an analysis from the National Pharmacovigilance Network. Aging Clin Exp Res. 2019. doi:10.1007/s40520-019-01304-5
6. Bjerre LM, Ramsay T, Cahir C, et al. Assessing potentially inappropriate prescribing (PIP) and predicting patient outcomes in Ontario’s older population: a population-based cohort study applying subsets of the STOPP/START and Beers’ criteria in large health administrative databases. BMJ Open. 2015;5:e010146. doi:10.1136/bmjopen-2015-010146
7. Wauters M, Elseviers M, Vaes B, et al. Too many, too few, or too unsafe? Impact of inappropriate prescribing on mortality, and hospitalization in a cohort of community-dwelling oldest old. Br J Clin Pharmacol. 2016;82(5):1382–1392. doi:10.1111/bcp.13055
8. Moriarty F, Bennett K, Cahir C, Kenny RA, Fahey T. Potentially inappropriate prescribing according to STOPP and START and adverse outcomes in community-dwelling older people: a prospective cohort study. Br J Clin Pharmacol. 2016;82(3):849–857. doi:10.1111/bcp.12995
9. World Health Organization. Global health and ageing; 2011. Available from: https://www.who.int/ageing/publications/global_health.pdf.
10. Miller GE, Sarpong EM, Davidoff AJ, Yang EY, Brandt NJ, Fick DM. Determinants of potentially inappropriate medication use among community-dwelling older adults. Health Serv Res. 2017;52(4):1534–1549. doi:10.1111/1475-6773.12562
11. Primejdie DP, Bojita MT, Popa A. Potentially inappropriate medications in elderly ambulatory and institutionalized patients: an observational study. BMC Pharmacol Toxicol. 2016;17(1):38. doi:10.1186/s40360-016-0081-x
12. Tommelein E, Mehuys E, Petrovic M, Somers A, Colin P, Boussery K. Potentially inappropriate prescribing in community-dwelling older people across Europe: a systematic literature review. Eur J Clin Pharmacol. 2015;71(12):1415–1427. doi:10.1007/s00228-015-1954-4
13. Ursulica ET. The Relationship between health care needs and accessibility to health care services in Botosani County- Romania. Procedia Environ Sci. 2016;32:300–310. doi:10.1016/j.proenv.2016.03.035
14. Albulescu AC, Larion D. An analysis of the proximity based polarisation of the hospital network of Moldavia’s counties. Lucrarile Seminarului Geografic Dimitrie Cantemir. 2018;46(2):3–18. doi:10.15551/lsgdc.v46i2.01
15. O’Mahony D, O’Sullivan D, Byrne S, et al. STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Aging. 2015;44:213–218. doi:10.1093/ageing/afu145
16. Ryan C, O’Mahony D, Kennedy J, Weedle P, Byrne S. Potentially inappropriate prescribing in an Irish elderly population in primary care. Br J Clin Pharmacol. 2009;68(6):936–947. doi:10.1111/j.1365-2125.2009.03531.x
17. Curtain CM, Bindoff IK, Westbury JL, Peterson GM. A comparison of prescribing criteria when applied to older community-based patients. Drugs Aging. 2013;30(11):935–943. doi:10.1007/s40266-013-0116-6
18. CNAS. Available from: http://www.cnas.ro/media/pageFiles/Ghid%20prescriere%20Reteta.pdf.
19. CNAS. Available from: http://www.cnas.ro/casamm/post/type/local/regimul-juridic-al-plantelor-substantelor-si-preparatelor-stupefiante-si-psihotrope.html.
20. Eurostat. Mortality and life expectancy statistics; 2019. Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php/Mortality_and_life_expectancy_statistics.
21. CASDJ. Available form: www.casdj.ro/999cod.xls.
22. Eurostat. Cardiovascular diseases statistics; 2018. Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php/Cardiovascular_diseases_statistics#Deaths_from_cardiovascular_diseases.
23. Riordan DO, Aubert CE, Walsh KA. Prevalence of potentially inappropriate prescribing in a subpopulation of older European clinical trial participants: a cross-sectional study. BMJ Open. 2018;8(3):e019003. doi:10.1136/bmjopen-2017-019003
24. Kara Ö, Arık G, Kızılarslanoglu MC, et al. Potentially inappropriate prescribing according to the STOPP/START criteria for older adults. Aging Clin Exp Res. 2016;28(4):761–768. doi:10.1007/s40520-015-0475-4
25. Rodríguez-Blanco R, Álvarez-García M, Villalibre-Calderón C, et al. [Updated report on STOPP-START criteria in primary care]. Semergen. 2019;45(3):180–186. Spanish. doi:10.1016/j.semerg.2018.06.004
26. Vezmar Kovačević S, Simišić M, StojkovRudinski S, et al. Potentially inappropriate prescribing in older primary care patients. PLoS One. 2014;9(4):e95536. doi:10.1371/journal.pone.0095536
27. Moriarty F, Bennett K, Fahey T, Kenny RA, Cahir C. Longitudinal prevalence of potentially inappropriate medicines and potential prescribing omissions in a cohort of community-dwelling older people. Eur J Clin Pharmacol. 2015;71:473–482. doi:10.1007/s00228-015-1815-1
28. Cabassi A, Tedeschi S, Perlini S, et al. Non-steroidal anti-inflammatory drug effects on renal and cardiovascular function: from physiology to clinical practice. Eur J PrevCardiol. 2019;14:2047487319848105. doi:10.1177/2047487319848105
29. Masumoto S, Sato M, Maeno T, Ichinohe Y, Maeno T. Association between potentially inappropriate medications and anxiety in Japanese older patients. Geriatr Gerontol Int. 2017;17(12):2520–2526. doi:10.1111/ggi.13128
30. Davies J, Rae TC, Montagu L. Long-term benzodiazepine and Z-drugs use in England: a survey of general practice [corrected]. Br J Gen Pract. 2017;67(662):e609–e613. doi:10.3399/bjgp17X691865
31. Mo L, Ding D, Pu SY, et al. Patients aged 80 years or older are encountered more potentially inappropriate medication use. Chin Med J (Engl). 2016;129(1):22–27. doi:10.4103/0366-6999.172558
32. Yazdanshenas H, Bazargan M, Smith J, Martins D, Motahari H, Orum G. Pain treatment of underserved older African Americans. J Am Geriatr Soc. 2016;64(10):2116–2121. doi:10.1111/jgs.14302
33. Wongrakpanich S, Wongrakpanich A, Melhado K, Rangaswami J. A comprehensive review of non-steroidal antiinflammatory drug use in the elderly. Aging Dis. 2018;9(1):143–150. doi:10.14336/AD.2017.0306
34. Andor M, Dehelean L, Romosan AM, et al. A novel approach to cardiovascular disturbances in patients with schizophrenia spectrum disorders treated with long-acting injectable medication. Neuropsychiatr Dis Treat. 2019;15:349–355. doi:10.2147/NDT.S186892
35. Dehelean L, Andor M, Romosan AM, Tomescu MC. Pharmacological and disorder associated cardiovascular changes in patients with psychosis. A comparison between olanzapine and risperidone. Farmacia. 2018;66(1):129–134.
36. World Health Organization Regional Office for Europe. Planning healthy and sustainable meetings; 2018. Available from: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/publications/2018/planning-healthy-and-sustainable-meetings-2018.
37. Dalton K, Byrne S. Role of the pharmacist in reducing healthcare costs: current insights. Integr Pharm Res Pract. 2017;6:37–46. doi:10.2147/IPRP.S108047
38. Ryan C, O’Mahony D, O’Donovan DÓ, et al. A comparison of the application of STOPP/START to patients’ drug lists with and without clinical information. Int J Clin Pharm. 2013;35(2):230–235. doi:10.1007/s11096-012-9733-0
39. Getachew H, Bhagavathula AS, Abebe TB, Belachew SA. Inappropriate prescribing of antithrombotic therapy in Ethiopian elderly population using updated 2015 STOPP/START criteria: a cross-sectional study. Clin Interv Aging. 2016;11:819–827. doi:10.2147/CIA.S107394
40. Delgado-Silveira E, Fernández-Villalba EM, García-Mina Freire M, et al. The impact of pharmacy intervention on the treatment of elderly multi-pathological patients. Farm Hosp. 2015;39(4):192–202. doi:10.7399/fh.2015.39.4.8329
41. Cortejoso L, Dietz RA, Hofmann G, Gosch M, Sattler A. Impact of pharmacist interventions in older patients: a prospective study in a tertiary hospital in Germany. Clin Interv Aging. 2016;11:1343–1350. doi:10.2147/CIA.S109048
42. Tommelein E, Petrovic M, Somers A, Mehuys E, van der Cammen T, Boussery K. Older patients’ prescriptions screening in the community pharmacy: development of the Ghent older people’s prescriptions community pharmacy screening (GheOP3S) tool. J Public Health (Oxf). 2016;38(2):e158–70. doi:10.1093/pubmed/fdv090
43. Lin HW, Lin CH, Chang CK, et al. Economic outcome of pharmacist-physician medication therapy management for polypharmacy elderly: a prospective, randomized, controlled trial. J Formos Med Assoc. 2018;117(3):235–243. doi:10.1016/j.jfma.2017.04.017
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.