")
Back to Journals » Clinical Ophthalmology » Volume 14
Potential Role and Significance of Ocular Demodicosis in Patients with Concomitant Refractory Herpetic Keratitis
Authors Hung KH , Lan YH, Lin JY, Kang EYC, Tan HY, Chen HC , Hsiao CH, Yeh LK
Received 15 September 2020
Accepted for publication 27 November 2020
Published 23 December 2020 Volume 2020:14 Pages 4469—4482
DOI https://doi.org/10.2147/OPTH.S282059
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kuo-Hsuan Hung,1– 3 Yu-Hsiang Lan,2,4 Jui-Yen Lin,1,2 Eugene Yu-Chuan Kang,1,2 Hsin-Yuan Tan,1,2 Hung-Chi Chen,1,2 Ching-Hsi Hsiao,1,2 Lung-Kun Yeh1,2
1Department of Ophthalmology, Chang Gung Memorial Hospital, Linkou, Taoyuan, 333, Taiwan; 2Chang-Gung University, College of Medicine, Taoyuan 333, Taiwan; 3Institute of Clinical Medicine, National Yang-Ming University, Taipei City 112, Taiwan; 4Department of Medicine, Chang Gung University, Taoyuan 333, Taiwan
Correspondence: Lung-Kun Yeh
Department of Ophthalmology, Chang Gung Memorial Hospital, Linkou, No 5, Fusing St., Taoyuan 333, Taiwan
Tel +886-3-3281200, ext. 8666
Fax +886-3-3287798
Email [email protected]
Purpose: To evaluate the role of Demodex infestation of the eyelids in patients with recurrent herpetic keratitis.
Patients and Methods: This is a retrospective and noncomparative case series. Twenty-seven patients with ocular demodicosis and recurrent herpetic keratitis under conventional treatments were enrolled. Demographic data and clinical photographs were collected. Ocular demodicosis was confirmed by eyelash examination under a microscope. Eyelid scrub was initiated in these patients after proving Demodex infestation. Response after treatment was reviewed.
Results: Herpetic keratitis was characterized by epithelial defect, including dendritic lesions (seven eyes, 25.9%), geographic ulcer (three eyes, 11.1%), and neurotrophic ulcer (two eyes, 7.4%), associated with stromal involvement in 12 cases. Six cases with stromal reactivation, including disciform keratitis (two eyes, 7.4%), immune ring (three eyes, 11.1%), and ghost vessel (one eye, 3.7%), presented no epithelial defect. Active anterior uveitis with keratic precipitates was found in 15 cases. Demodex blepharitis was diagnosed with cylindrical dandruff along their lashes in all patients. Other ocular findings include meibomian gland dysfunction (15 eyes, 55.6%), mal-aligned lashes (eight eyes, 29.6%), telangiectasia (14 eyes, 51.9%), conjunctivitis (18 eyes, 66.7%), and ocular rosacea (three eyes, 11.1%). Initial unstable clinical presentations showed deterioration of corneal melting into descemetocele, corneal perforation, recalcitrant stromal infiltration/uveitis, and uncontrollable IOP, despite antiherpetic medication. After treatment of Demodex blepharitis, infestation was under control, followed by subjective improvement of ocular symptoms and a stable clinical outcome.
Conclusion: Ocular demodicosis should be considered in patients with unstable recurrent herpetic keratitis. A prompt diagnosis and appropriate treatment may curb the progression of herpetic corneal infection.
Keywords: blepharitis, Demodex mites, herpetic keratitis, ocular demodicosis
Introduction
Herpetic keratitis is one of the leading infectious cause of visual loss in developed countries.1 Herpes simplex keratitis (HSK) can be classified into epithelial, stromal, endothelial, and keratouveitis type. Although primary herpes simplex virus (HSV) infection often recovers spontaneously, all the HSV carriers are subsequently at risk of reactivation. Recurrence rate of HSK is 19% during the period of oral antiviral therapy according to the Herpetic Eye Disease Study;1 moreover, risk of corneal scarring and visual impairment increases with each subsequent episode. Susceptibility of ocular HSV infection depends on the host immune status; thus, immunocompromise is regarded as a risk factor of HSV infection and recurrence.2–5 Furthermore, reactivation can be attributed to external and internal medical conditions.6–8
Herpes zoster ophthalmicus (HZO), accounting for 10–20% of herpes zoster infection, occurs when lesions involve ophthalmic division of the trigeminal nerve by varicella zoster virus (VZV).9,10 Of the HZO cases, 13–75% develop acute keratitis, and may affect all layers of the cornea.11 Other than herpes infection, human eyelids can be affected by two species of Demodex mites, D. brevis and D. folliculorum, whose infestation rate is highly age-dependent.12 Several risk factors predispose people to develop ocular demodicosis, including immunocompromise, diabetes mellitus, rosacea, stress, and smoking.13–15 Once facial demodicosis develops, Demodex mites tend to migrate and flourish around the eyes.
The pathogenesis of ocular demodicosis is still under debate since it also occurs in asymptomatic individuals. However, there is increasing evidence suggesting that ocular demodicosis is a potential cause of refractory ocular discomfort, conjunctivitis, pediatric blepharoconjunctivitis, meibomian gland dysfunction, chalazion, eyelid basal cell carcinoma, pterygium, rosacea, and sight-threatening keratitis.13,–16–24 To the best of our knowledge, the interaction between Demodex infestation and HSK/herpes zoster keratitis (HZK) has not been mentioned before. Herein, we reported 27 patients with recurrent herpetic keratitis combined with ocular demodicosis to investigate whether Demodex infestation plays a pathogenic role in herpetic keratitis.
Patients and Methods
This study was approved by the Institutional Review Board of Chang Gung Memorial Hospital, Linkou (No. 201801086B0), to retrospectively review the medical records of 250 patients from 2010 and 2018. Twenty-seven patients with herpetic keratitis and combined ocular demodicosis were enrolled. All patients had signed informed consent for publication of clinical data and images and this study was conducted in accordance with the Declaration of Helsinki. Inclusion criteria in this study were patients from 15–90 years old with a diagnosis of refractory HSK/HZK and blepharitis from ocular demodicosis. Refractory keratitis was defined as conditions resistant to oral or topical anti-viral agents, recurrent keratitis more than three times per year, and no response to regular medical treatment. Subtypes of herpetic keratitis, including HSV stromal keratitis with or without uveitis, atopic dermatitis with herpetic keratitis, and herpetic zoster ophthalmicus, were enrolled. Treatments used in our patients were oral famciclovir or topical acyclovir ointment, combined with topical 0.1% dexamethasone or 0.1% betamethasone, and lubricants. Patients with other combined ocular surface diseases, negative findings of Demodex mites, and loss of follow-up were excluded. Demodex infestation was confirmed by microscopic examination. A thorough ophthalmologic examination and photography were performed.
Blepharitis was diagnosed by inspection of morphology of lid margin, such as telangiectasia, irregular lid margin, or abnormal meibomian gland. The diagnostic criteria of ocular demodicosis are summarized as follows:17 1) Slit-lamp finding of typical cylindrical dandruff (CD) at the root of lashes. 2) Microscopic confirmation by direct visualization of Demodex mites on epilated lashes. Briefly, six lashes with prominent CD were epilated from bilateral eyelids. Positive results presented at least one mite on one lash. Alcohol (75–100%) was applied to dissolve CD, allowing embedded mites to migrate out. 3) Highly suspected clinical history and symptoms such as blepharitis, recurrent trichiasis, frequent madarosis, conjunctivitis, keratitis in adult individuals or blepharoconjunctivitis or frequently recurred chalazion in young individuals, refractory to antiviral agents and steroid. Ocular demodicosis was majorly treated with commercialized lid scrub (OcuSOFT®; Lid Scrub PLUS, USA), containing 1,2-Octanediol after warm compress.
Results
Twenty-seven patients of ocular demodicosis and herpetic keratitis were enrolled. The patients’ demographic data are summarized in Table 1. Twenty-one males and six females (male/female ratio: 21/6) with a mean age of 56.9±17.4 (range=15–88) years were included. Average duration of follow-up was 18.8±16.2 months. Clinical manifestation of herpetic keratitis is listed in Table 2. Stromal keratitis with epithelial defect, including dendritic (seven eyes, 25.9%), geographic (three eyes, 11.1%), and neurotrophic ulcer (two eyes, 7.4%), were found in 12 cases, of whom two ended up with corneal perforation. Six cases presented stromal involvement without epithelial defect, including immune ring (three eyes, 11.1%), disciform keratitis (two eyes, 7.4%), and ghost vessel (one eye, 3.7%). Culture of the corneal lesions showed co-infection of Staphylococcus epidermidis (two eyes), and Pseudomonas aeruginosa (one eye). Fifteen patients presented active anterior uveitis with KPs.
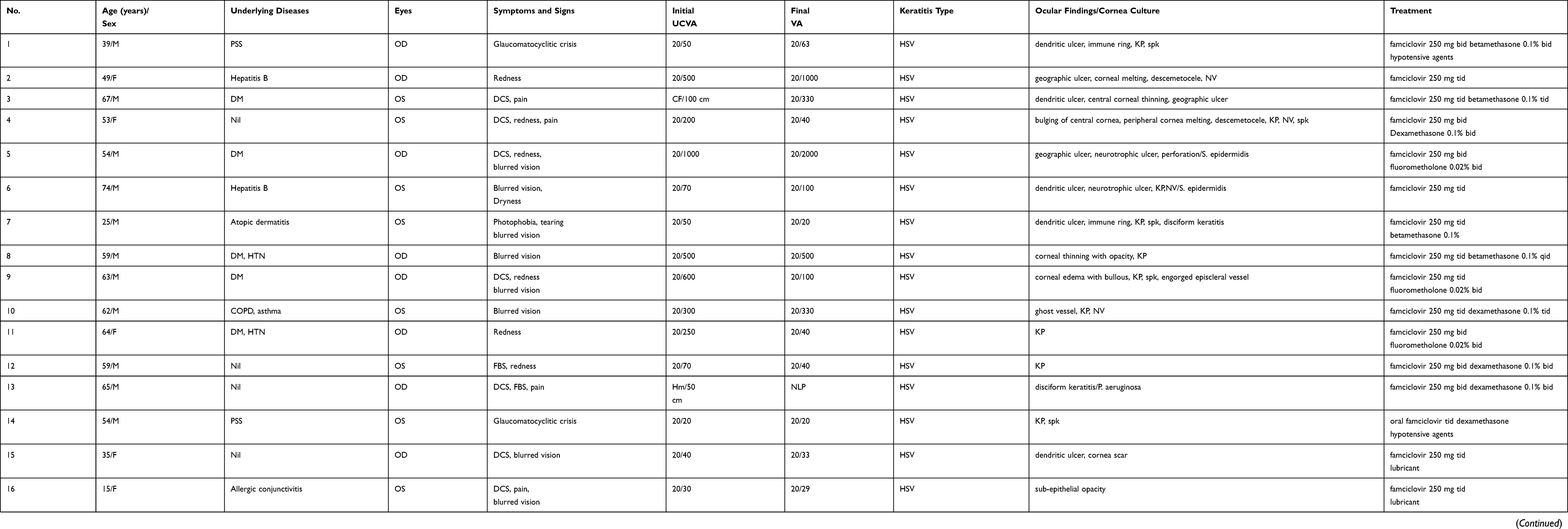 |
Table 1 Demographic Data of Patients with Herpetic Keratitis and Demodex Blepharitis |
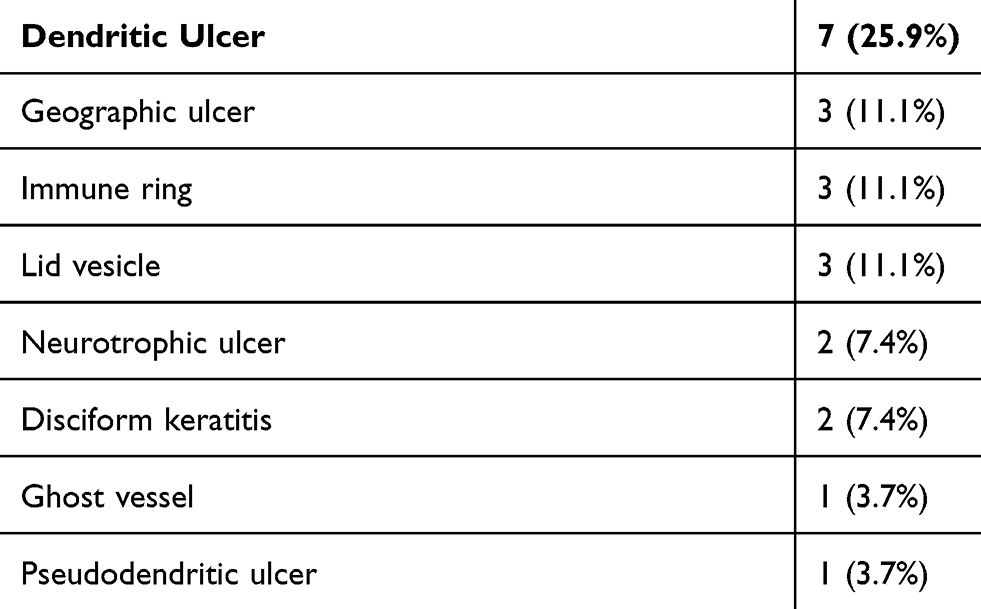 |
Table 2 Ocular Findings in Our Herpetic Keratitis Patients (n=27) |
When diagnosed with keratitis, nearly all of the patients were symptomatic, including blurred vision (18 eyes, 66.7%), redness (nine eyes, 33.3%), decreased cornea sensation (nine eyes, 33.3%), pain (six eyes, 22.2%), dryness (six eyes, 22.2%), foreign body sensation (three eyes, 11.1%), and photophobia (one eye, 3.7%). Manifestations of ocular demodicosis at the time of diagnosis are shown in Table 3. All the patients had CD on lashes, with 21 diffuse type and six sporadic type. Other associated findings include meibomian gland dysfunction (MGD) (15 eyes, 55.6%), telangiectasia (14 eyes, 51.9%), conjunctivitis (18 eyes, 66.7%), mal-aligned lashes (eight eyes, 29.6%), and ocular rosacea (three eyes, 11.1%). Their clinical courses were unstable and presented progressive corneal melting to descemetocele, corneal perforation, recalcitrant uveitis, stromal infiltration, and uncontrollable IOP, despite the antiherpetic treatment being administered. After initiating lid scrub for lid hygiene, ocular demodicosis was controlled with reduced symptoms, followed by more stable clinical conditions. Here, we show representative cases in our study.
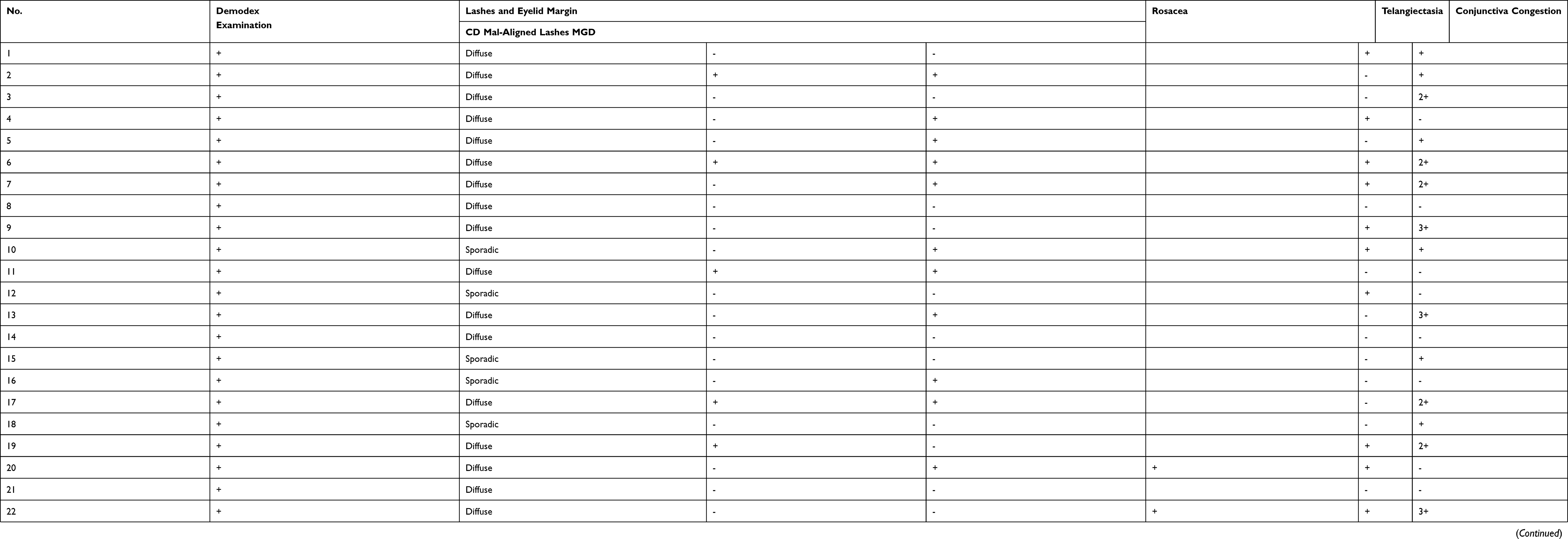 |
Table 3 Clinical Manifestations of Ocular Demodicosis in Our 27 Patients |
Case Series of HSV Stromal Keratitis with Ocular Demodicosis
Case No. 2
A 49-year-old female with unilateral HSV stromal keratitis in her right eye was regularly followed up. Initially, her UCVA were 20/500 OD and 20/25 OS. Progressive central corneal melting, opacity, neovascularization, and congested conjunctiva were found in her right eye. MGD, mal-aligned lashes, and blepharitis were also noted on bilateral lid margins with positive findings of Demodex mites (Figure 1A). Recurrent HSV stromal keratitis and ocular demodicosis were diagnosed. Unfortunately, corneal melting progressed to descemetocele 13 months later, followed by geographic corneal lesion in her right eye (Figure 1B), even after intensive management of antiviral agents, steroid, lubricants, and lid scrub. Hence, triple surgery as penetrating keratoplasty (PK) with extracapsular cataract extraction (ECCE) and posterior chamber intraocular lens (PCIOL) implantation was performed (Figure 1C) for impending corneal perforation and mature cataract. Neither recurrent HSV keratitis nor ocular demodicosis was noted during the following 5 months when lid hygiene was maintained.
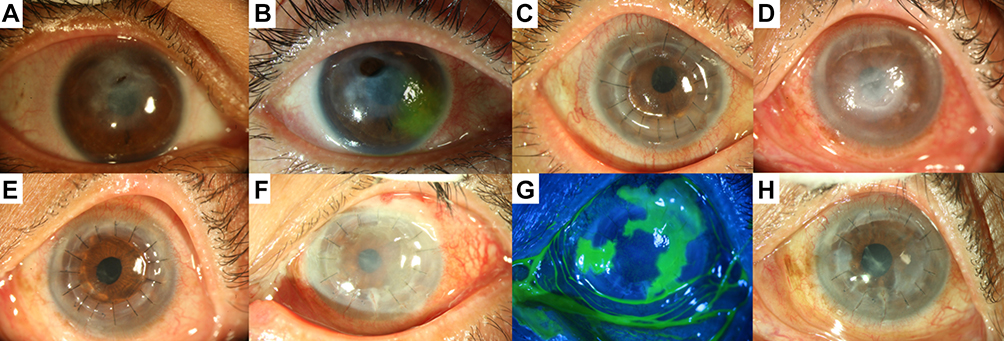 |
Figure 1 HSV stromal keratitis with ocular demodicosis ends in penetrating keratoplasty and unstable course. Central corneal melting, corneal opacity, and blepharitis with meibomian gland dysfunction were noted in the right eye of case No.2 (A). Stromal melting progressed to descemetocele later, complicated with geographic ulcer (B). Triple procedure (PK, ECCE, PCIOL) was performed (C) for impending corneal perforation and mature cataract. Neurotrophic keratitis was observed in the left eye of case No.3 (D). Triple procedure (PK, ECCE, PCIOL) was performed for persistent epithelial defect and his poor vision (E). Post-PK graft rejection with recurrent geographic ulcer developed 3 years later (F and G). Graft edema persisted for 7 months and resolved dramatically after initiating mite-eradicating therapy (H). |
Case No. 3
Herpetic keratitis is one of the common ocular conditions associated with neurotrophic keratitis. A 67-year-old male with diabetes mellitus (DM) was diagnosed as neurotrophic keratitis with persistent corneal defect in his left eye for several months (Figure 1D), which improved after amniotic membrane transplantation (AMT). Improved UCVA from counting finger (CF) at 100 cm to 20/100 was noted in his left eye after triple procedure (Figure 1E). Unfortunately, graft rejection with recurrent geographic ulcer (Figure 1F-G) developed in the same eye 3 years later. Furthermore, the lesions did not respond well to antiviral agents, steroid, and artificial tears for 7 months until ocular demodicosis was identified and intensively treated (Figure 1H). Neither recurrent HSV keratitis nor corneal epithelial defect were noted after ocular demodicosis was controlled.
Case No. 5
Necrotizing stromal keratitis, the most severe form of herpetic keratitis, tends to recur easily with an inflammatory reaction. It will severely damage the corneal structure and potentially lead to corneal perforation. A 54-year-old male with diabetes complained of pain, redness, and gradually decreasing vision in his right eye for weeks. At first, visual acuity was 20/1000 in his right eye with geographic ulcer, melting stroma (Figure 2A), and hypoesthesia. Necrotizing HSV stromal keratitis was impressed with secondary S. epidermidis co-infection. Healing epithelium was observed after treatments of anti-herpetic and antibiotic agents at first (Figure 2B). Unfortunately, corneal ulcer exacerbated to perforation (Figure 2C) with worsened UCVA to CF at 30 cm in the right eye, despite administering intensive treatments with antiviral agent, antibiotics, 20% auto-serum, and lubricant ointment. Simultaneously, bilateral blepharitis with diffuse CDs and MGD were noted. Stabilized corneal stroma and healed epithelial defect with scar (Figure 2D) were observed over the following 6 months after addressing ocular demodicosis. His UCVA improved to 20/500 in the right eye 2 weeks after cataract surgery. No recurrent HSV keratitis was found during the following 17 months.
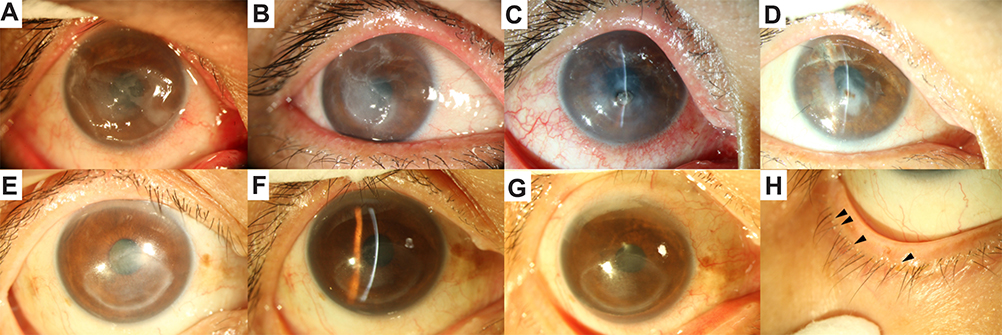 |
Figure 2 Clinical presentation of HSV stromal keratitis with ocular demodicosis. Geographic corneal ulcer with stromal melting was found in the right eye of case No. 5. (A) Healing epithelial defect under treatment was noted at first (B). Unfortunately, stromal melting progressed to perforation (C); meanwhile, ocular demodicosis was found. More stable condition was established after proper treatment for ocular demodicosis (D). Corneal opacity, cornea thinning, and mutton fat keratic precipitates were shown in the right eye of case No. 8 (E and F). Good response to mite-eradicating therapy with improved visual acuity and clinical appearance was noted (G). Diffuse cylindrical dandruff over the root of eyelashes was identified (black arrowhead) (H). |
Case No. 8
A 59-year-old male with diabetes and hypertension complained of blurry vision for weeks in the right eye. Corneal opacity with thinning and mutton-fat KPs (Figure 2E-F) were found. His UCVA was 20/500 OD due to HSV stromal keratitis with uveitis. Corneal transparency and KPs improved 2 weeks after anti-herpetic treatment; however, a decrease in response led to gradually decreased vision (20/1000 OD) within 2 months. He lost follow-up since then, and returned to our clinic with severe bilateral blepharitis 7 months later. His UCVA deteriorated to 20/2000 in the right eye. Bilateral lid margins showed diffuse CDs with confirmed ocular demodicosis on epilated lashes (Figure 2H). Warm compress and mite-eradicating lid scrub were prescribed immediately. After 3 weeks of antiherpetic and anti-Demodex treatment, the ocular surface condition became stable (Figure 2G) and his UCVA improved to 20/350.
Case No. 9
A 63-year-old male with diabetes complained of redness in the right eye. UCVA at presentation were 20/600 OD and 20/500 OS. Corneal stromal infiltration with a localized circumferential opaque ring at the supero-nasal area of the right cornea, superficial punctate keratitis, KPs, and corneal hypoesthesia (Figure 3A) were revealed. Meanwhile, the conjunctiva was severely injected with engorged episcleral vessels. Initial impression was HSV stromal keratitis with uveitis; therefore, oral antiviral and topical steroid agents were initiated. The cornea cleared up (Figure 3B) soon within three weeks and his UCVA improved to 20/25 OD. However, recurrent HSV keratitis at the same quadrant of the cornea was noted, complicated with ocular demodicosis 25 months later (Figure 3C–F). Warm compress and mite-eradiating lid scrub were started after diagnosis. Decreased CDs on the eyelashes and clear-up of the cornea were noted 2 weeks later (Figure 3G and H). No recurrent HSV infection was found during the following 6 months.
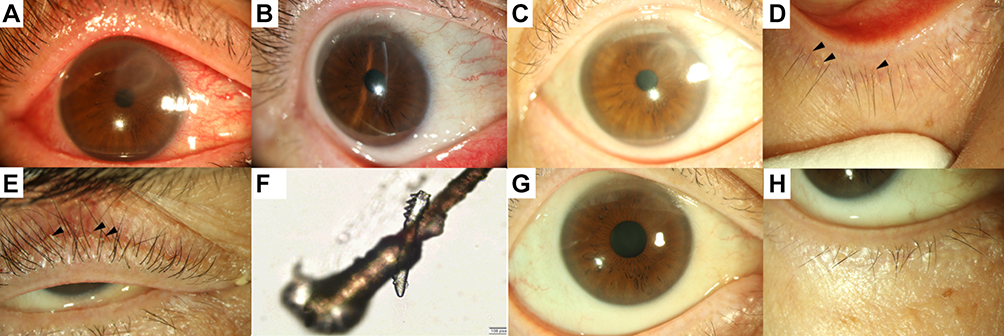 |
Figure 3 Recurrent localized HSV stromal keratitis complicated with ocular demodicosis. Stromal edema with localized circumferential opaque ring at superonasal area in the right eye of case No.9. (A) The lesion cleared up after anti-herpetic agents. (B) Recurrent HSV episode at the same area of the cornea was found, complicated with ocular demodicosis (black arrowheads; D,E) (C–F). No recurrence of herpes simplex keratitis was noted after proper treatment of ocular demodicosis (G and H). |
Case Series of HSV Stromal Keratitis and Uveitis with Ocular Demodicosis
Case No. 1
A 39-year-old man with glaucomatocyclitic crisis visited our clinic for poorly controlled intraocular pressure (IOP). At presentation, his UCVA were 20/50 OD and 20/25 OS. Slit-lamp examination showed dendritic corneal lesions, which resolved in 2 weeks after antiviral agents. However, 8 months later, KPs and recurrent HSV stromal keratitis with immune ring from 7 to 9 o’clock developed in the right eye (Figure 4A and B). IOP escalated to 33 mmHg OD and 27 mmHg OS. Immune ring (Figure 4C) resolved after initiating antiviral agent and topical steroid; however, soaring IOP was refractory to the aforementioned treatment. Simultaneously, blepharitis with CDs was found (Figure 4D). Since Demodex mites infestation was confirmed, mite-eradicating lid scrub and warm compress were initiated for ocular demodicosis. No episode of ocular hypertension was noted during the following 5 months.
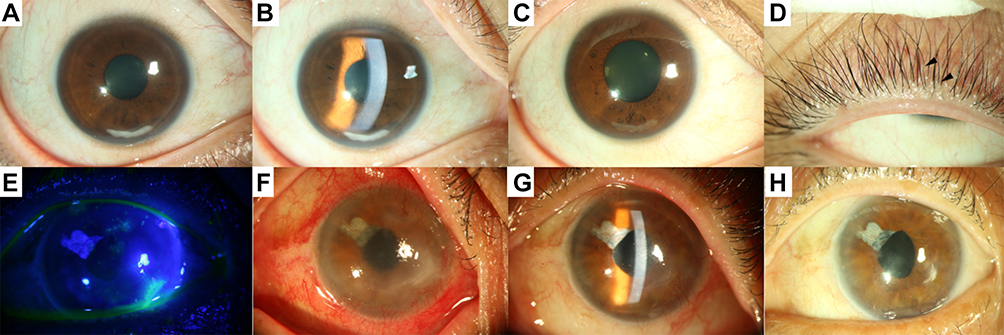 |
Figure 4 HSV stromal keratitis with refractory uveitis was controlled after initiating mite eradicating agents. Circumferential immune ring and keratic precipitates were found in the right eye of case No. 1 (A and B). Corneal condition improved after anti-herpetic treatment (C). However, elevated intraocular pressure persisted and did not resolve until initiating mite-eradicating eyelid scrub. Cylindrical dandruff was found over the root of the eyelashes (black arrowheads) (D). Corneal dendritic ulcer and peripheral pannus was noted at temporo-inferior area in the left eye of patient No. 6 (E). Neurotrophic keratitis developed later (F) and five episodes of HSV uveitis with keratic precipitates (G) occurred in the following 2 years. No recurrent HSV infection was noted after managing the Demodex infestation (H). |
Case No. 6
A 74-year-old male with hepatitis B presented with blurry vision in his left eye. He had a cataract surgery in the left eye 1 year earlier. At presentation, ocular examination revealed dendritic ulcer in the left eye (Figure 4E), which resolved within 1 week after anti-herpetic treatment. Seven weeks later, an episode of neurotrophic HSV keratitis with superimposed S. epidermidis infection (Figure 4F) developed in the left eye. The stroma reduced thinning with a clear-up appearance within 8 weeks after intensive treatment. However, the clinical condition of the cornea was still unstable. Five episodes of HSV uveitis with KPs (Figure 4G) waxed and waned during the following 2 years. At the same time, lid margin showed meibomian gland dysfunction, telangiectasia, and CDs over the lash root in both eyes. Ocular demodicosis was microscopically confirmed. No recurrent HSV infection (Figure 4H) was noted during the 6-month follow-up after treatment of ocular demodicosis.
Case No. 11
A 64-year-old female with diabetes and hypertension presented with a congested right eye for 2 days. Her UCVA were 20/250 OD and 20/70 OS, accompanied with sectoral episcleritis in the right eye (Figure 5A) and anterior chamber inflammation with KPs in both eyes. Initial diagnosis was uveitis secondary to HSV, which responded well to the therapy. However, uveitis flared up with poor response later. Simultaneously, bilateral blepharitis with CDs was noted (Figure 5C) with confirmed ocular demodicosis (Figure 5D). After controlling ocular demodicosis, no recurrence of uveitis was noted during the following 5 months (Figure 5B).
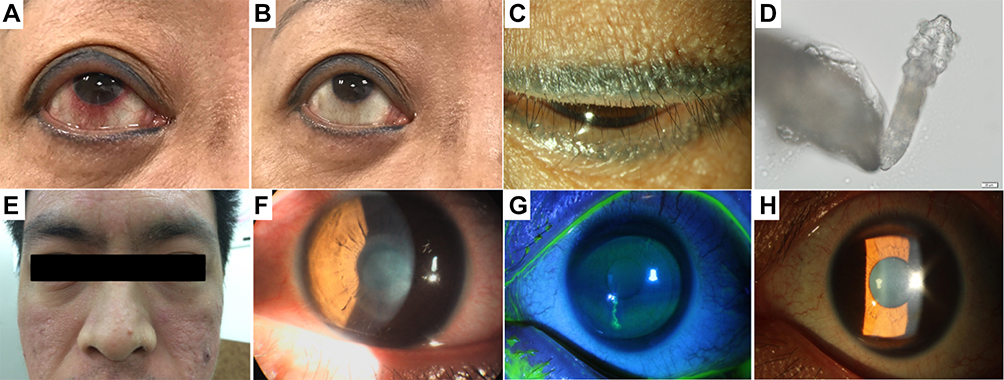 |
Figure 5 Demodex blepharitis demonstrated in patients with episcleritis/uveitis or atopy. Episcleritis in the right eye and uveitis in both eyes were found in patient No.11 (A). Uveitis frequently flared up and did not resolve until treatment of Demodex blepharitis which is confirmed under microscopic examination (B–D). External appearance of patient No. 7 with atopic dermatitis (E). Disciform keratitis in the left eye was shown at presentation (F). Several episodes of recurrent herpes simplex keratitis with branching dendritic lesions were recorded (G), and keratic precipitates (H) were noted during follow-up examination. |
Atopic Dermatitis Associated with Herpetic Virus Infection and Ocular Demodicosis
Case No. 7
Atopy is viewed as one of the factors causing reactivation of herpes virus. A 25-year-old male complained of photophobia with blurry vision and tearing in his left eye. Atopic dermatitis had been diagnosed before (Figure 5E). His UCVA were 20/40 OD and 20/50 OS; meanwhile, slit-lamp examination revealed circle-shaped corneal edema with superficial punctate keratitis. The adjacent conjunctiva showed inflammation due to atopic conjunctivitis (Figure 5F). Herpetic disciform keratitis with stromal edema improved 1 week after treatment. However, several episodes of recurrent HSV keratitis were noted with a persistent circumferential immune ring, branching dendritic lesions (Figure 5G), and endothelial KPs (Figure 5H) during follow-up. Severe dermatitis and blepharitis due to atopic dermatitis were discovered simultaneously. Lid margin showed diffuse CDs, MGD, and telangiectasia in both eyes, followed by confirmation of ocular demodicosis.
Evidence of Herpetic Zoster Ophthalmicus Complicated with Demodex Infestation
Case No. 22
An 88-year-old male, with phymatous rosacea (Figure 6A), asthma, and congestive obstructive pulmonary disease (COPD), suffered from herpes zoster infection. His UCVA were 20/100 OD and 20/300 OS. His left eye presented decreased cornea sensation, pseudodendritic ulcer, and cornea edema. The cornea cleared up in 3 weeks after oral antiviral agent for HZO. One recurrent episode of herpes zoster keratitis with neovascularization, KPs, and soared IOP developed in the left eye 1 year later (Figure 6B). Blepharitis with CDs, telangiectasia, and associated conjunctivitis occurred on bilateral lid margin before identification of Demodex mites (Figure 6C). Clinical presentation improved after antiherpetic treatment and controlling ocular demodicosis.
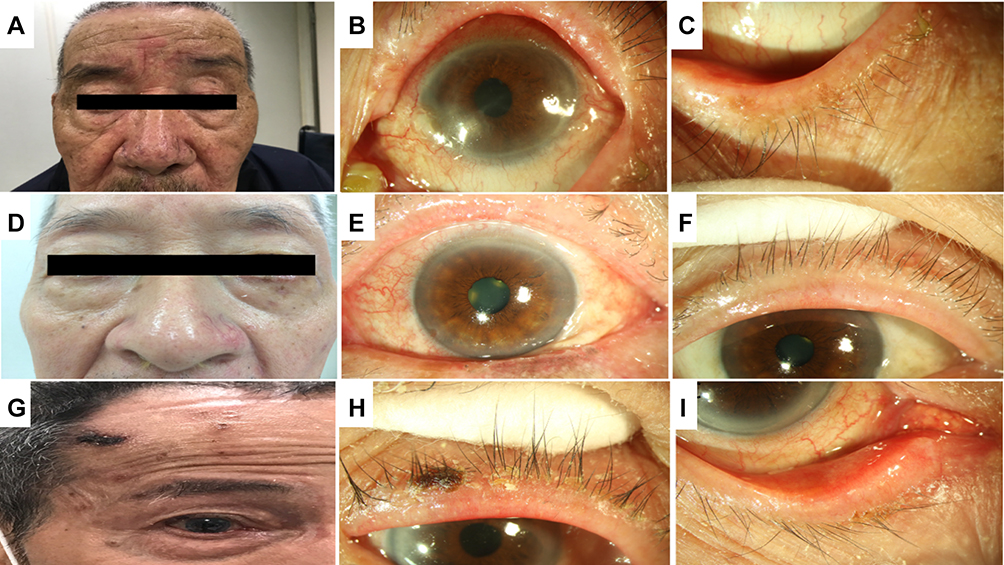 |
Figure 6 Patterns of herpes zoster ophthalmicus with comorbidity of ocular demodicosis. Phymatous rosacea and herpes zoster ophthalmicus were found in patient No. 22 (A). At the same time, herpes zoster keratitis (B) complicated with Demodex infestation showing cylindrical dandruff and telangiectasia over lid margin, was presented (C). Appearance of herpes zoster infection in patient No. 23 (D). Typical meibomian gland dysfunction, telangiectasia, and blepharitis over lid margin were noticed (E and F). Appearance of herpes zoster infection over forehead and periorbita of patient No. 24 (G). Demodex blepharitis with cylindrical dandruff and telangiectasia was revealed over lid margin (H and I). |
Case No. 23
A 67-year-old male with HZO (Figure 6D), ocular rosacea, and ocular demodicosis complained of a congested left eye for 2 days. UCVA at presentation were 20/30 OD and 20/70 OS. Ocular examination revealed meibomian gland dysfunction, telangiectasia, and blepharitis over bilateral lid margin (Figure 6E and F). The presence of Demodex mites was found on eyelashes. The patient responded well to the antiviral agent and mite-eradicating therapy with improved clinical appearance.
Case No. 24
An 80-year-old male presented with redness and blurred vision in the right eye. He had hepatitis B and herpes zoster infection with vesicular eruption over his right forehead (Figure 6G). His UCVA were 20/30 OD and 20/100 OS, combined with central superficial punctate keratitis, corneal edema, and KPs. Diffuse CDs on eyelashes and telangiectatic lid margin were noted as well (Figure 6H and I), with microscopically confirmed Demodex mites. HZO complicated with ocular demodicosis was diagnosed. The patient started oral antiviral agent, topical steroid, and mite-eradicating eyelid scrub. Improvement of clinical appearance was noted within 2 weeks.
Discussion
Demodex infestation is a common but often overlooked condition in ocular surface and corneal diseases.17 The prevalence rate of Demodex infestation increases with age,17,25 by contrast, the age range in our patients were from 15–88 years, with the majority (70%) under 65 years old. Two patients were even younger than 25 years old (Table 1). Male gender was predominant in our enrolled patients (male:female = 21:6), which may be due to less care on lid hygiene and no need of frequent removing make-up, compared to females. Corneal manifestation of ocular demodicosis, including superficial corneal opacity, corneal vascularization, marginal corneal infiltration, phlyctenule-like lesion, and corneal scar, was first reported by Kheirkhah et al.26 We recently identified ocular demodicosis in 27 patients with a diagnosis of herpetic keratitis. Their clinical courses, including progressive corneal melting to descemetocele (case 2), prolonged resolution of rejected corneal graft (case 3), corneal perforation (case 5), recalcitrant uveitis (case 6), recalcitrant stromal infiltration (case 9), and uncontrollable IOP, were refractory to antiherpetic treatments. After initiating mite-eradicating therapeutics, warm compress, and maintenance of lid hygiene, ocular demodicosis was under control and the ocular symptoms improved, followed by more stable corneal condition.
Identification of coexisting ocular demodicosis in herpetic keratitis relied on symptoms of blepharitis, microscopic examination, and therapeutic response to mite-eradicating therapy. Demodicosis-related keratitis may also cause vision-threatening ocular surface diseases, and masquerade as herpetic keratitis due to recurrent episodes and its slit-lamp findings.13,24 However, demodicosis-related keratitis responds well to mite-eradicating therapy rather than antiviral agents and steroid.13,24 Evaluation of Demodex infestation has been implicated in ocular diseases, based on several postulated pathogenic mechanisms. Mechanically, Demodex mites block the eyelash follicles and cause direct damage, leading to epithelial hyperplasia and reactive hyperkeratinization. Mites also induce granulomatous reaction via their chitinous exoskeleton. A potential microbial and symbiotic role in Demodex infestation was also disclosed.19 Demodex mites may act as a carrier of bacteria, such as Staphylococci and Streptococci, on its surface. The super antigen on bacteria potentially elicits microbial blepharitis and rosacea. Furthermore, the mites may also harbor Bacillus oleronius and elicit inflammatory cascade by producing pro-inflammatory proteins.17,27
We found blepharitis and CDs on eyelashes in all patients. Other manifestations of infestation, including MGD, telangiectasia, mal-aligned lashes, conjunctival congestion and rosacea are shown in Table 4. The chance of detecting D. folliculorum on lashes is higher than that of D. brevis, because D. folliculorum congregates at the base of the lashes instead of the meibomian and sebaceous glands where D. brevis resides in.19 Interestingly, D. brevis is more often related to corneal involvement and the severity of keratitis is significantly correlated with the number of mites.24,26 One of the reasons is that D. brevis can reach the cornea more easily.19 MGD is another common and relevant condition affecting ocular surface, which may interact and exacerbate ocular demodicosis due to abnormal inflammation and accumulation of debris along the lid margin. There were 15 eyes (55.6%) presenting concomitant MGD in our study. Our treatment plan for ocular demodicosis is a warm compress of eyelids before cleaning the lid with eyelid scrub. The advantage of this strategy is based on temperature-sensitive characteristics of Demodex mites; however, warm compress is also beneficial to improve MGD. If sever MGD is recognized, oral doxycycline 100 mg Q12H will be provided for better control.
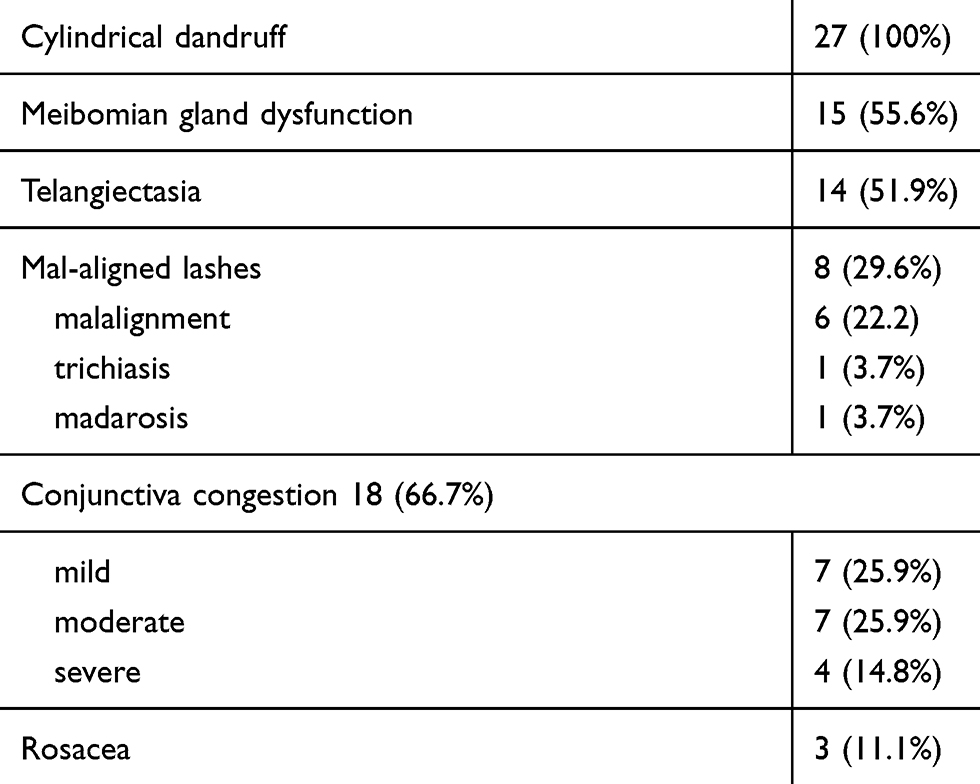 |
Table 4 Patterns of Ocular Demodicosis in Our Patients (n=27) |
The increased incidence of demodicosis in patients with diabetes, hematologic malignancies, AIDS, and UV radiation indicates that immunosuppressed status may play a role in Demodex infestation.13–15 This comorbidity may predispose reactivation of herpes virus. T-cell immunodeficiency, in particular, is a major predisposing factor of Demodex mites invasion. In our case series, it showed a personal history of diabetes in eight cases, hepatitis B in three cases, rosacea in two cases, Posner Schlossman syndrome in two cases, and asthma in two cases. There were three cases who have atopic dermatitis, allergic conjunctivitis, and hyperthyroidism, respectively. Systemic or topical corticosteroid were required to address these conditions, which may predispose patients to develop demodicosis in several reports.13 Additionally, 0.35% of patients with methimazole for hyperthyroidism may develop agranulocytosis. Significantly lower values of CD3+, CD4+, CD8+, CD16+ cells, CD3+/CD20+ ratio, and decreased function of leukocytes in individuals infested by Demodex mites were observed.28
Some limitations existed in our study. First, there was no control group to compare the immune markers between the group of ocular demodicosis with herpetic keratitis and pure herpetic keratitis. Second, neither does our study tell whether a specific species of Demodex is involved in recurrent herpetic keratitis, nor does it show the total numbers of Demodex distribution. To address these questions, a prospective and comparative study in correlating ocular demodicosis with herpetic keratitis to delineate the potential pathogenic role of Demodex mites is required.
Conclusion
Patients with herpetic keratitis should be meticulously examined and routinely screened for concomitant Demodex eyelid infestation, which requires specific treatment modalities to improve long-term visual outcome. If patients fail to respond to antiviral therapy more than 1 week, potential antiviral toxicity, resistance to antiviral therapy, neurotrophic status, poor compliance to treatment, or an alternative diagnosis should be considered. We recommended a complete evaluation of patient’s immune status and a meticulous exploration of symptoms associated with Demodex infestation and cylindrical dandruff, particularly in herpetic keratitis. We highlighted the need to put Demodex infestation into differential diagnosis in immunocompromised patients with herpetic keratitis. A correct diagnosis and appropriate treatment may stop progression of herpetic corneal infection.
Abbreviations
HSK, Herpes simplex keratitis; KPs, keratic precipitates; HZO, Herpes zoster ophthalmicus; HZK, herpes zoster keratitis; CD, cylindrical dandruff; MGD, Meibomian gland dysfunction; PK, penetrating keratoplasty, ECCE, extracapsular cataract extraction; PCIOL, posterior chamber intraocular lens; DM, diabetes mellitus; AMT, amniotic membrane transplantation; CF, counting finger; IOP, intraocular pressure; COPD, congestive obstructive pulmonary disease.
Data Sharing Statement
The dataset used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Institutional Review Board of Chang Gung Memorial Hospital, Linkou (No. 201801086B0), to retrospectively review the medical records of 27 patients with co-existing herpetic keratitis and ocular demodicosis between 2010 and 2018.
Consent for Publication
All patients had signed informed consent.
Author Contributions
Authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Ministry of Science and Technology (MOST; Taiwan) [grant numbers 109-2314-B-182A-021]; and Chang Gung Medical Research Project [grant numbers CMRPG3E1522, CMRPG3H1281, CMRPG3H1282].
Disclosure
The authors report no financial interest or conflict of interests in this study.
References
1. Azher TN, Yin XT, Tajfirouz D, et al. Herpes simplex keratitis: challenges in diagnosis and clinical management. Clin Ophthalmol. 2017;11:185–191.
2. Rowe AM, St Leger AJ, Jeon S, et al. Herpes keratitis. Prog Retin Eye Res. 2013;32:88–101.
3. Kaiserman I, Kaiserman N, Nakar S, et al. Herpetic eye disease in diabetic patients. Ophthalmology. 2005;112:2184–2188.
4. Hodge WG, Margolis TP. Herpes simplex virus keratitis among patients who are positive or negative for human immunodeficiency virus: an epidemiologic study. Ophthalmology. 1997;104:120–124.
5. Papanicolaou GA, Meyers BR, Fuchs WS, et al. Infectious ocular complications in orthotopic liver transplant patients. Clin Infect Dis. 1997;24:1172–1177.
6. Herpetic Eye Disease Study Group. Psychological stress and other potential triggers for recurrences of herpes simplex virus eye infections. Arch Ophthalmol. 2000;118:1617–1625.
7. Herpetic Eye Disease Study Group. Predictors of recurrent herpes simplex virus keratitis. Cornea. 2001;20:123–128.
8. Mucci JJ, Utz VM, Galor A, et al. Recurrence rates of herpes simplex virus keratitis in contact lens and non-contact lens wearers. Eye Contact Lens. 2009;35:185–187.
9. Ragozzino MW, Melton LJ. 3rd, Kurland LT, et al. Population-based study of herpes zoster and its sequelae. Medicine (Baltimore). 1982;61:310–316.
10. Liesegang TJ. Herpes zoster ophthalmicus natural history, risk factors, clinical presentation, and morbidity. Ophthalmology. 2008;115:S3–12.
11. Li JY. Herpes zoster ophthalmicus: acute keratitis. Curr Opin Ophthalmol. 2018;29:328–333.
12. Post CF, Juhlin E. Demodex folliculorum and blepharitis. Arch Dermatol. 1963;88:298–302.
13. Luo X, Li J, Chen C, et al. Ocular demodicosis as a potential cause of ocular surface inflammation. Cornea. 2017;Suppl 1:S9–S14.
14. Sarro RA, Hong JJ, Elgart ML. An unusual demodicidosis manifestation in a patient with AIDS. J Am Acad Dermatol. 1998;38:120–121.
15. Kemal M, Sumer Z, Toker MI, et al. The prevalence of Demodex folliculorum in blepharitis patients and the normal population. Ophthalmic Epidemiol. 2005;12:287–290.
16. Lee SH, Chun YS, Kim JH, et al. The relationship between demodex and ocular discomfort. Invest Ophthalmol Vis Sci. 2010;51:2906–2911.
17. Liu J, Sheha H, Tseng SC. Pathogenic role of Demodex mites in blepharitis. Curr Opin Allergy Clin Immunol. 2010;10:505–510.
18. Liang L, Safran S, Gao Y, et al. Ocular demodicosis as a potential cause of pediatric blepharoconjunctivitis. Cornea. 2010;29:1386–1391.
19. Fromstein SR, Harthan JS, Patel J, et al. Demodex blepharitis: clinical perspectives. Clin Optom (Auckl). 2018;10:57–63.
20. Liang L, Ding X, Tseng SC. High prevalence of demodex brevis infestation in chalazia. Am J Ophthalmol. 2014;157:342–348.
21. Erbagci Z, Erbagci I, Erkilic S. High incidence of demodicidosis in eyelid basal cell carcinomas. Int J Dermatol. 2003;42:567–571.
22. Huang Y, He H, Sheha H, et al. Ocular demodicosis as a risk factor of pterygium recurrence. Ophthalmology. 2013;120:1341–1347.
23. Zhao YE, Wu LP, Peng Y, et al. Retrospective analysis of the association between Demodex infestation and rosacea. Arch Dermatol. 2010;146:896–902.
24. Liang L, Liu Y, Ding X, et al. Significant correlation between meibomian gland dysfunction and keratitis in young patients with Demodex brevis infestation. Br J Ophthalmol. 2018;102:1098–1102.
25. Vargas-Arzola J, Reyes-Velasco L, Segura-Salvador A, et al. Prevalence of Demodex mites in eyelashes among people of Oaxaca, Mexico. Acta Microbiol Immunol Hung. 2012;59:257–262.
26. Kheirkhah A, Blanco G, Casas V, et al. Fluorescein dye improves microscopic evaluation and counting of demodex in blepharitis with cylindrical dandruff. Cornea. 2007;26:697–700.
27. Wolf R, Ophir J, Avigad J, et al. The hair follicle mites (Demodex spp.). Could They Be Vectors of Pathogenic Microorganisms? Acta Derm Venereol. 1988;68:535–537.
28. Akilov OE, Mumcuoglu KY. Immune response in demodicosis. J Eur Acad Dermatol Venereol. 2004;18:440–444.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.