")
Back to Journals » Journal of Pain Research » Volume 12
Postural counseling represents a novel option in pain management of fibromyalgia patients
Authors Galvani C, Caramaschi P, Mura P, Paladini A, Piroli A, Arnaudo E , De Franceschi L, Evangelista M , Pari A, Ongaro G, Finco G , Ciannameo A, Carletto A, Varrassi G , Biasi D
Received 6 February 2018
Accepted for publication 21 September 2018
Published 11 January 2019 Volume 2019:12 Pages 327—337
DOI https://doi.org/10.2147/JPR.S164714
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Carla Galvani,1 Paola Caramaschi,1 Paolo Mura,2 Antonella Paladini,3 Alba Piroli,3 Elisa Arnaudo,4 Lucia De Franceschi,5 Maurizio Evangelista,6 Alice Pari,4 Giovanna Ongaro,1 Gabriele Finco,2 Anna Ciannameo,4 Antonio Carletto,1 Giustino Varrassi,3,7 Domenico Biasi1
1Rheumatology Unit, Department of Medicine, University of Verona, Verona, Italy; 2Anesthesia, Intensive Care and Pain Therapy Unit, Department of Medical Science “M. Aresu”, University of Cagliari, Cagliari, Italy; 3Department of MESVA, University of L’Aquila, L’Aquila, Italy; 4Department of Internal Medicine, University of Bologna, Bologna, Italy; 5Internal Medicine Unit, Department of Medicine, University of Verona, Verona, Italy; 6Emergency Department, Institute of Anesthesia, Resuscitation and Pain Medicine, Catholic University of Sacred Heart, Rome, Italy; 7Paolo Procacci Foundation, Rome, Italy
Background: Chronic pain is a key symptom in fibromyalgia (FM), and its management is still challenging for rheumatologists in daily practice. FM patients show psychological and psychiatric manifestations, going from mood and emotional disorders to depression and alexithymia that negatively impact their quality of life, limiting their daily activities. Since pharmacological strategies have a limited efficacy in FM pain, alternative or complementary non-pharmacological approaches have been introduced in the clinical management of FM.
Patients and methods: This is a retrospective study on FM patients (n=52) treated with a novel integrated postural counseling (PC) rehabilitation program carried out by a counselor physiotherapist. The clinical impact of PC was evaluated by 1) a semi-structured interview using an ad hoc modified questionnaire McGill Illness Narrative Interview (MINI) 1 to obtain data on pain management by highlighting everyday experience of living with pain and 2) an FM impact questionnaire (FIQ) total score.
Results: Two main structures of narrative emplotment of FM illness were recognized: 1) the cumulative life narrative structure (46.15%) and 2) the broken life (53.85%) narrative structure. Baseline FIQ score was 77.38±7.77, and it was significantly reduced after PC to 39.12±13.27 (P<0.0001). Although well-being still requires further definition as outcome in pain management, it is important for FM patients, dealing with pain-related sensations, thoughts and feelings and limiting their daily activities. In our study, 87.5% of interviewed FM patients reported an improvement in their well-being after PC.
Conclusion: Our data suggest that an integrated PC program positively impacts chronic pain and fatigue based on self-management strategies. PC allows FM patients to resume their own life and regenerate their own image. Finally, we propose the introduction of the evaluation of the ability to resume daily activities as the target of rehabilitation programs in FM.
Keywords: self-management, sense of self, fatigue, serotonin–norepinephrine reuptake inhibitors, tricyclic drugs, anticonvulsants, NSAIDs
Erratum for this paper has been published.
Introduction
Fibromyalgia (FM) is an invalidating chronic disorder characterized by widespread pain often associated with fatigue, paresthesia, mood alterations such as anxiety and/or depression, sleep disturbance and functional bowel abnormalities. FM is frequently diagnosed in subjects with a history of disorders, in which the symptom pain is predominant such as headache, dysmenorrhea, irritable bowel syndrome, temporomandibular joint disorders or other regional pain syndromes.1,2 Although pathophysiology of FM is still largely unknown, recent studies have identified different factors involved in FM pathogenesis3 such as 1) gene implicated in regulation of pain sensitivity-modulating neurotransmitters; 2) environmental events such as infections, triggering FM; and 3) physical traumas and psychological stresses. Collectively, these factors promote a general alteration of stress regulatory systems and centralized pain state.4 In addition, impaired mechanisms of neurotransmission may also negatively reflect on sleep, mood, memory and cognitive performance.2,5–7
Chronic pain is the main symptom reported by all FM patients.3,8–13 The classical therapeutic approach to chronic pain management in FM subjects is a multimodal analgesia based on drugs with different mechanisms of action such as non-steroidal anti-inflammatory drugs (NSAIDs) combined with serotonin–norepinephrine reuptake inhibitors (SNRIs), low-dose tricyclic compounds or anticonvulsants (ie, duloxetine, amitriptyline and pregabalin). Although this strategy has improved chronic pain management in FM, patients still feel undertreated and frequently autonomously withdraw from prescribed analgesic drugs. Since chronic pain is a deep personal experience, it affects life stories, generating fatigue, anxiety and anger with existential crisis.16–20 Indeed, FM patients show psychological and psychiatric manifestations going from mood and emotional disorders to depression and alexithymia, which negatively impact FM patients’ quality of life, limiting their daily activities.21–23 Alternative or complementary non-pharmacological approaches have been introduced in the clinical management of chronic pain in FM patients. Among them, acupuncture, cognitive behavior therapy (CBT) and exercise strength training10–13 have been related to good outcomes in FM subjects.24,25 This in combination with programs of health education and a patient-centered approach positively impact FM pain.2,14,15,24,25 Recently, the acceptance and commitment therapy (ACT), using the psychological flexibility model, has been tested in patients with either chronic pain of different origins or with FM.26,27 Yu et al26 showed that the acceptance of chronic disease and the restoration of the sense of self positively impact the daily life of FM subjects. The importance to restore the sense of self is further supported by anthropological studies in other chronic diseases, using integrated model for pain management that includes biomedical aspects (disease) and patients’ illness experience.1,20,28 Thus, patients’ ill narratives have been suggested to be a key factor in supporting the process of pain acceptance related to functioning during rehabilitation programs in chronic diseases.7
In this study, we aimed to understand whether an integrated postural counseling (PC) program might impact FM chronic pain and FM patients’ ability to resume previous daily activities. We used the narrative emplotment of illness to profile FM patients. The impact of PC was evaluated by semi-structured interview using a modified questionnaire McGill Illness Narrative Interview (MINI) to obtain data on pain management and individual perception by highlighting everyday experience of living with pain. In FM subjects, the improvement in chronic pain and fatigue based on self-management strategies allowed FM patients to resume their own life and regenerate their own image.
Methods
This is a retrospective study on a cohort of 52 out of 120 patients with FM, referring to the Rheumatology Unit, University of Verona, during the 4-year period (2010–2013). These 52 patients were available to explore integrated PC program in the context of rehabilitation procedures for FM. FM was diagnosed based on the following criteria: a history of chronic widespread pain plus tenderness in 11 or more of 18 specific point sites (tender points) on digital pressure according to the American College of Rheumatology 1990 criteria classification of FM.29 The study was carried out according to the guidelines of the local ethics committee (Comitato Etico, AOUI-Verona, Italy). Each patient was informed, and the written informed consent was obtained. Data were anonymously collected. FM patients were recruited in outpatient clinic by two rheumatologists dedicated to FM care after the failure of standard program of rehabilitation, which was mainly based on aerobic exercise adapted to functional level of FM patients. PC was performed by two counselor physiotherapists, who were full-time dedicated to rheumatologic patients as part of the multidisciplinary rheumatologic medical team.
The impact of PC was evaluated by the clinical team, using FM impact questionnaire (FIQ; total score range 1–100) before the first section and after the last section of PC program. Based on previous studies, we considered FM patients as responders who experienced >30% improvement in FIQ total score compared to baseline.30,31
Life story collection and PC program
All patients underwent a PC program at 1–3 months after the first evaluation. PC was monthly scheduled. Each visit was divided into three steps: 1) illness narratives; 2) PC; and 3) exercise program based on the FM patients’ life experience.
Illness narratives
The FM patients were requested to tell 1) their illness experience; 2) their life settings; 3) the trigger(s) worsening their chronic pain and 4) the strategy to control pain different from analgesic medication(s). In the meantime, the postural counselor evaluated FM patients’ sitting posture and their breathing during narration.
PC
FM patients were backward and helped to identify muscular tensions defined as pressure perceived in the contact areas supporting the body compared to noncontact areas. These data were used to generate a map of FM patients’ muscular tensions. To increase muscular relaxation, FM patients were then placed with both legs flexed, using a static support. In this position, FM patients were requested 1) to listen to their own breathing comparing inspiration vs the expiration time; 2) to detect whether any pause might be present between the two phases of breathing; and 3) to identify whether they use either thoracic or diaphragmatic breathing or both. Since diaphragm relaxation affects breathing frequency and respiration load,32 the postural counselor asked FM patients 1) to prolong the breathing expiration time and 2) to feel the movement of their lumbar spine, which is outward during breathing inspiration, while the fixed head is held on the ground. The postural counselor then verified the state of muscular passive permanent contractions on the neck, the shoulders and in the upper part of the thorax, helping FM patients to localize them. This step was followed by a deep massage of the abovementioned areas to induce muscular relaxation, asking the FM patients to realize the differences in the muscular tensions before and after manipulation carried out by the postural counselor. FM patients visualized the muscular and skeletal districts involved in muscular tension using anatomic tables with the help of the postural counselor.
Exercise program based on FM patients’ day life
Postural counselor trained FM patients to the auto-massage of the muscular districts affected by muscular tension. Each day, FM patients were asked to 1) evaluate their breathing: inspiration vs expiration time, prolonging the expiration time; 2) relax shoulders during expiration time, trying to maintain them relaxed; 3) stretch the posterior muscular chains in grounding position during 10 separated prolonged breathing at least five times during the same day; 4) to perform “cat stretching” at waking-up time; 5) correct ergonomic posture during day life; 6) auto-massage of the muscular contracted districts; and 7) listen to their emotion(s) during the day life.
Individual narrative interview
The qualitative study was based of semi-structured interview submitted between May 2013 and June 2013 to FM patients involved in the study. This study was aimed at eliciting individual narrations of the PC experience, particularly in relation to the reduction in the acquired pain and pain self-management skills.33 Each interview lasted about 45 minutes and was audio-taped and verbatim transcribed from the interviewers. Patient interviews were conducted in Italian. The translation to English was done by a professional translator for the manuscript preparation. At the beginning of each interview, the researcher explained the context and the purpose of the study and reminded the interviewer of the right to stop it or ask explanation at any point. The questionnaire was generated to investigate patients’ experiences with PC program as semi-structured interview with open questions aimed at eliciting spontaneous narratives (Box 1). Our questionnaire was based on MINI 1, which investigates lived experience of illness and activates a process of meaning production based on the patients’ reorganization of the illness experience.34 At the same time, this allows the interviewer to access the representations of typical reality of sick people in a wider framework considering the illness as concerning all the aspects of individual existence.35
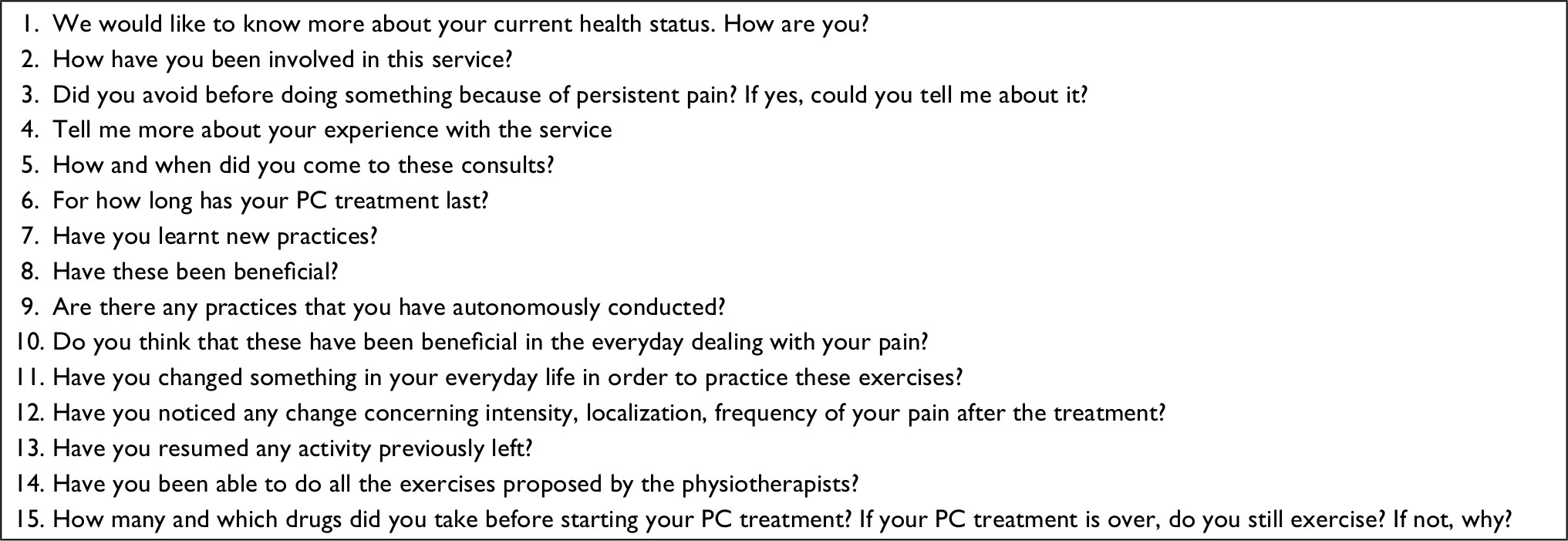 | Box 1 Predetermined questions of semi-structured interview of FM patients after PC Note: Patient interviews were conducted in Italian. The translation to English was done by a professional translator for the manuscript preparation. Abbreviations: FM, fibromyalgia; PC, postural counseling. |
Our questionnaire was driven to obtain data on pain management and individual perception of her/his own condition by highlighting everyday experience of living with pain. This was assessed focusing on the execution of daily activities.
Statistical analyses
The statistical analysis on FIQ was performed comparing data at baseline and after the PC. Gaussian distribution was tested with D’Agostino and Pearson omnibus normality test, and parametric or nonparametric statistics were implemented as appropriate. Basic clinical and sociodemographic data were compared to Student’s t-test or Mann–Whitney U-test (for non-normal distributed variables) for continuous variables and Fischer’s exact test for categorical variables. The evaluation of treatment’s efficacy was performed using a two-tailed t-test for paired data on the whole sample and separately for patients with the different narrative structures. Percentage of responders of the two identified narrative structures was compared using Fischer’s exact test. A P-value of <0.05 on a two-tailed test was considered statistically significant. Descriptive statistics were reported in terms of mean ± SD or median and interquartile range for quantitative variables and in terms of absolute frequencies and percentages for qualitative variables. Statistical analysis was performed using GraphPad Prism® for Windows, version 6.01 (GraphPad Software, Inc., La Jolla, CA, USA).
Results
Integrated PC in FM patients and patients’ life story collection
Main demographic and clinical characteristics of the 52 FM patients are reported in Table 1. Mean age of the patients was 51.40±12.65 years (range 18–78 years), 47 females and five males. All of them were Caucasian. The duration of clinical symptomatology ranged between 1 and 30 years, with a median of 3.5 years (2–8.25). Median number of tender points was 17 (15–18). Pharmacological treatment at the first visit site for PC, educational level and work status are reported in Table 1. The tree diagram of the study is shown in Figure 1. In the same visit site, the collection of patient’s life story was combined with PC as described in the “Patients and methods” section.11,14,36–39 Two main structures of narrative emplotment of FM illness were recognized in the 52 FM patients: the cumulative life narrative structure and the broken life narrative structure were identified in 24 (46.15%) and 28 (53.85%) cases, respectively (Table 2 ). Broken narrative structured patients were older, with a mean age of 55.64±11.98 years, vs a mean age of 46.46±11.79 years for cumulative ones (P<0.05). The median FM disease duration was 3.5 years (2–10 years) for patients with broken life narrative structure and 3.5 years (2–7.5 years) for patients with cumulative life narrative structure.
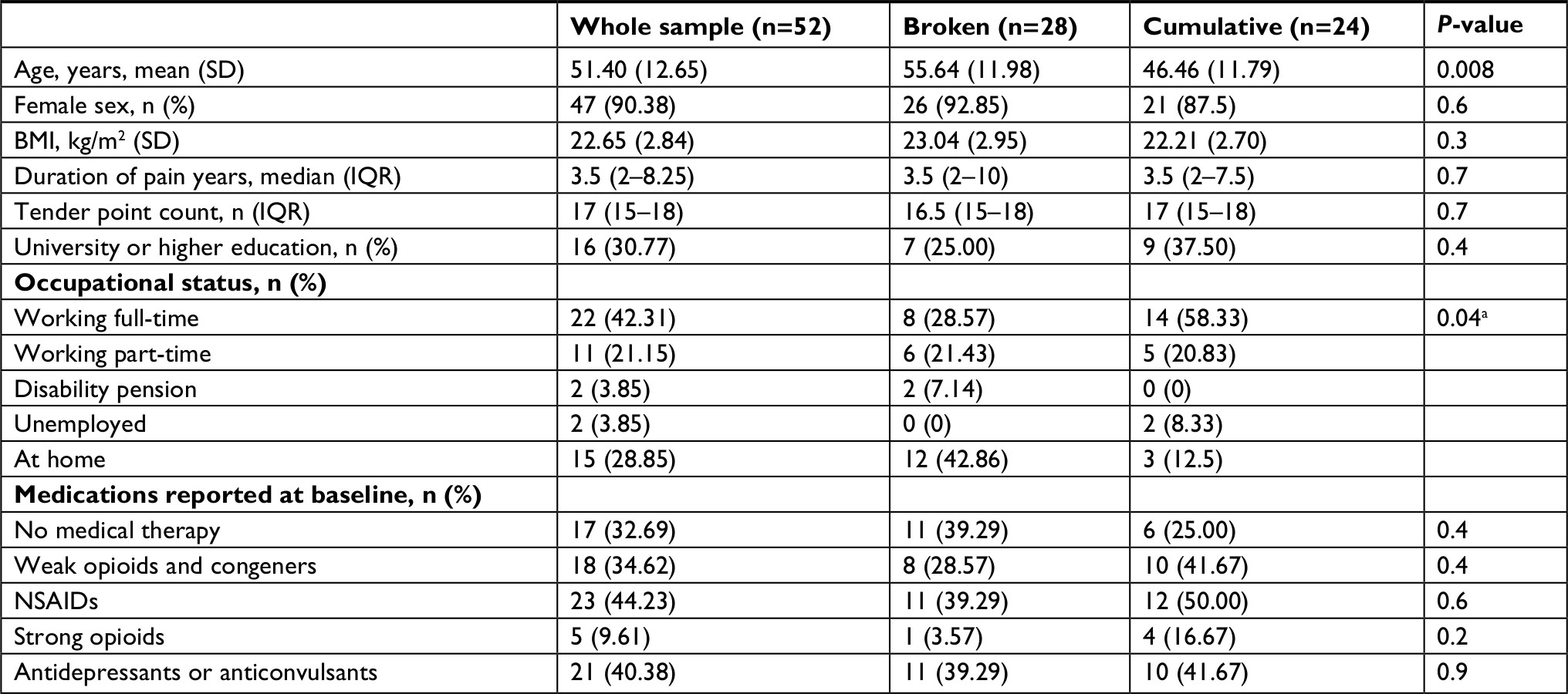 | Table 1 Demographic and clinical characteristics of FM patients treated with PC Note: aWorking (full-time plus part-time) vs not working. Abbreviations: BMI, body max index; FM, fibromyalgia; IQR, interquartile range; NSAIDs, non-steroidal anti-inflammatory drugs; PC, postural counseling. |
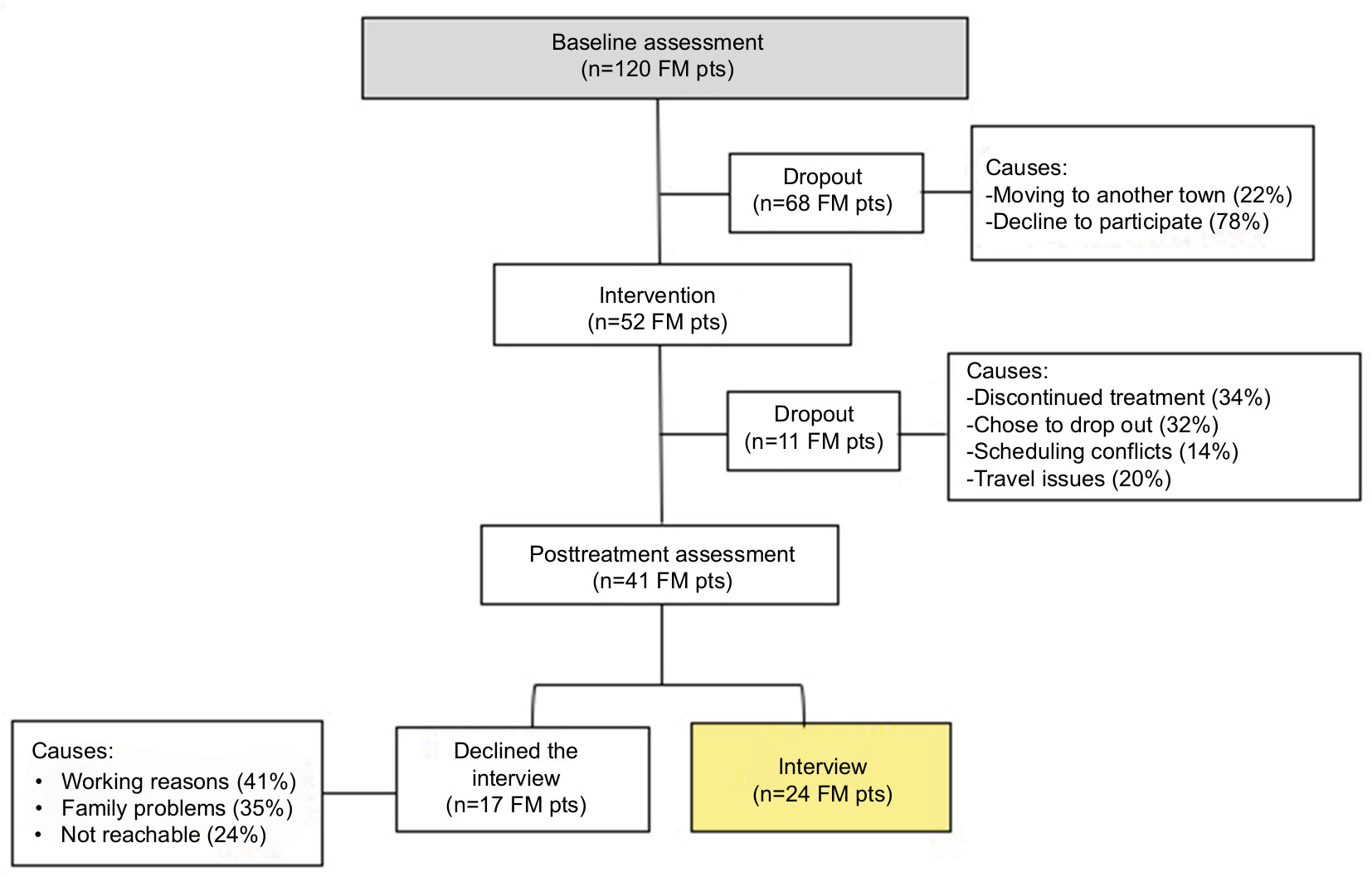 | Figure 1 Tree diagram of the study involving pts with FM treated with integrated PC. Abbreviations: FM, fibromyalgia; PC, postural counseling; pts, patients. |
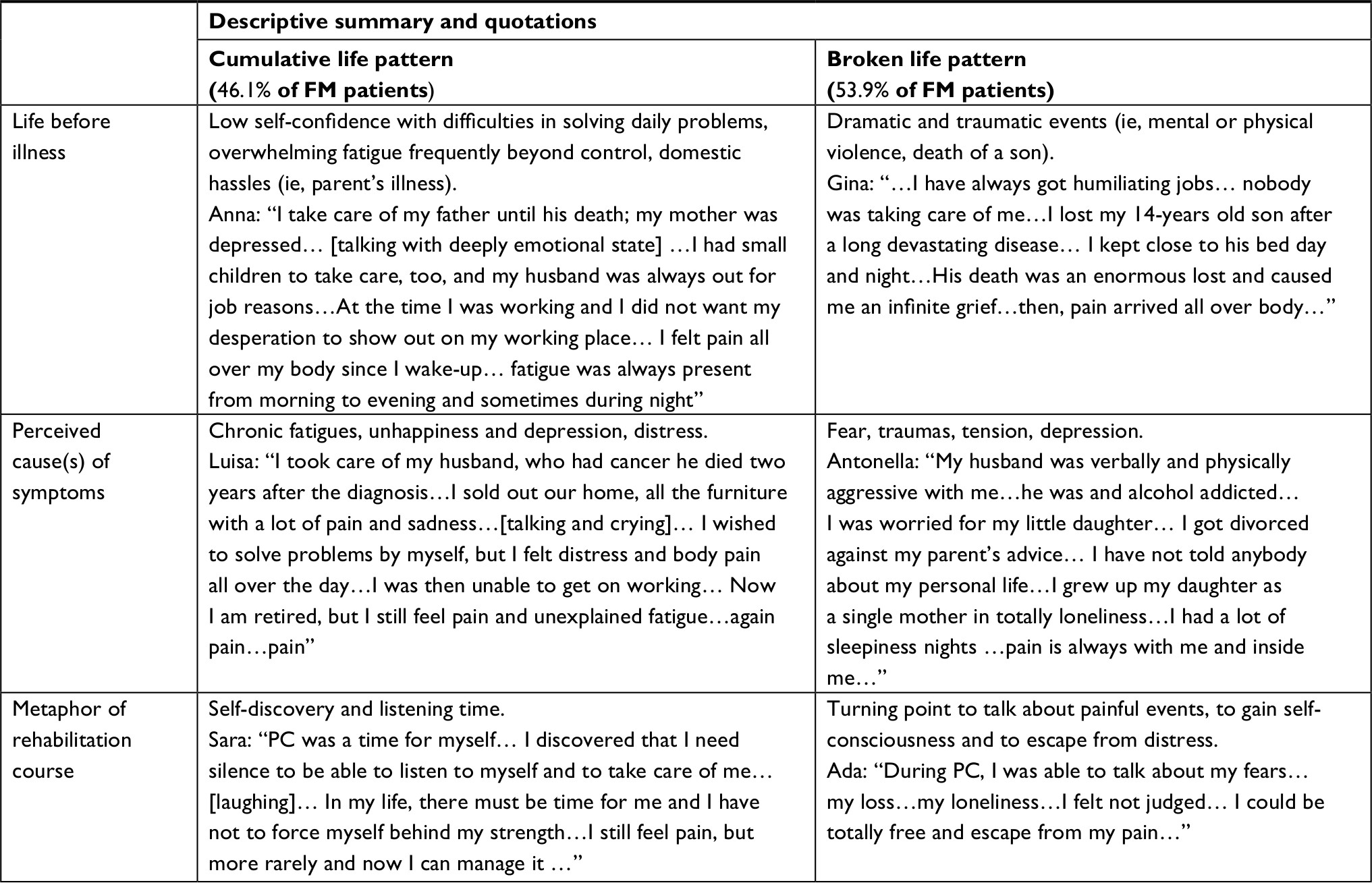 | Table 2 Narrative pattern of FM patients’ life story collected during PC Notes: The names shown in the table do not refer to patients’ real names. Patient interviews were conducted in Italian. The translation to English was done by a professional translator for the manuscript preparation. Abbreviations: FM, fibromyalgia; PC, postural counseling. |
No significant difference was found for educational degree in the two narrative structures (P=0.4), with a higher percentage (37.50% vs 25.00%) of highly educated patients (master degree or higher) among the cumulative life narrative structured patients. A significant difference was found for the occupational status, with 79.17% employed among cumulative life narrative and 50.00% in the broken group (P=0.04). Eleven (21%) patients dropped out of the study; the main causes were as follows: refusal of self-management program (63.6%), working-related time restriction(s) (9.1%), unexpected family duties (18.2%) and long distance between home and hospital (9.1%). It is of interest to note that the dropped-out FM patients were mainly from the broken life narrative structure subgroup: seven out of 28 patients (25%) vs four out of 24 cases (16.6%) in the cumulative one. This datum reflects the overwhelming fatigue in performing a rehabilitation program that requires a self-management approach by subjects characterized by the broken life narrative structure; these patients felt a loss of control over their lives, which generates a constant fear and requires frequent contacts with the rheumatologists in charge.
Twenty (71.4%) patients with the broken life narrative structure were under major antidepressive treatment in respect to six subjects (25%) with cumulative life narrative structure (P<0.05).
Pain was present in both narrative structures as the leading element of FM patients’ life stories.
In 46.16% of FM patients, PC was focused on deep muscle manipulation and muscle stretching of the upper limb and neck areas combined with education on listening to breathing cycles. In 42.30% of FM patients, PC was based on the revision of their fixed postures, mainly related to job context (ie, computer working and long time on car driving) or habits. This involved working out with antigravity muscles (ie, stretching and postural variation). In 11.53% of FM patients, PC targeted lower limbs and lumbar back areas to stretch superficial and deep muscle system and reduce pain in long-time standing position related to patients’ job duties.
Individual narrative interview as tool to evaluate the impact of integrated PC on chronic pain in FM patients
Participants were asked to tell about their experiences with PC program according to the predetermined questions (Box 1). Twenty-four FM patients accepted to participate in the semi-structured one-to-one interview (Figure 1). The professional background of the 24 interviewed patients was as follows: employees in different fields such as teaching, office and industrial work (37.5%), housewives (33.3%) and retired (29.1%). The attendance to the PC service was quite variable ranging from 1 year to 6 years. At the interview site, the mean value personalized PC consultations was 15. Seventy percent of the interviewed patients had already completed the PC program, and 87.5% of the interviewed patients were under analgesic or antidepressive treatment before starting the PC program. When interviews took place, 20% of the participants stopped their pain drug treatment(s), while 58.3% of them reduced their dosages. Concerning self-management of chronic pain promoted by PC, 79.1% of the participants learned and regularly practiced the exercise, while 75% of them referred an improved management of their acute pain episodes related to FM through exercise and breath control. Moreover, 87.5% of the interviewed FM patients reported an improvement in their well-being (Table 3, quotation 2.1). For what pain concerns, 75.0% of patients assessed a relevant improvement both as decrease in pain intensity or as a reduction in acute pain episodes already perceived after the second PC visit (Table 3, quotations 2.1 and 2.4).
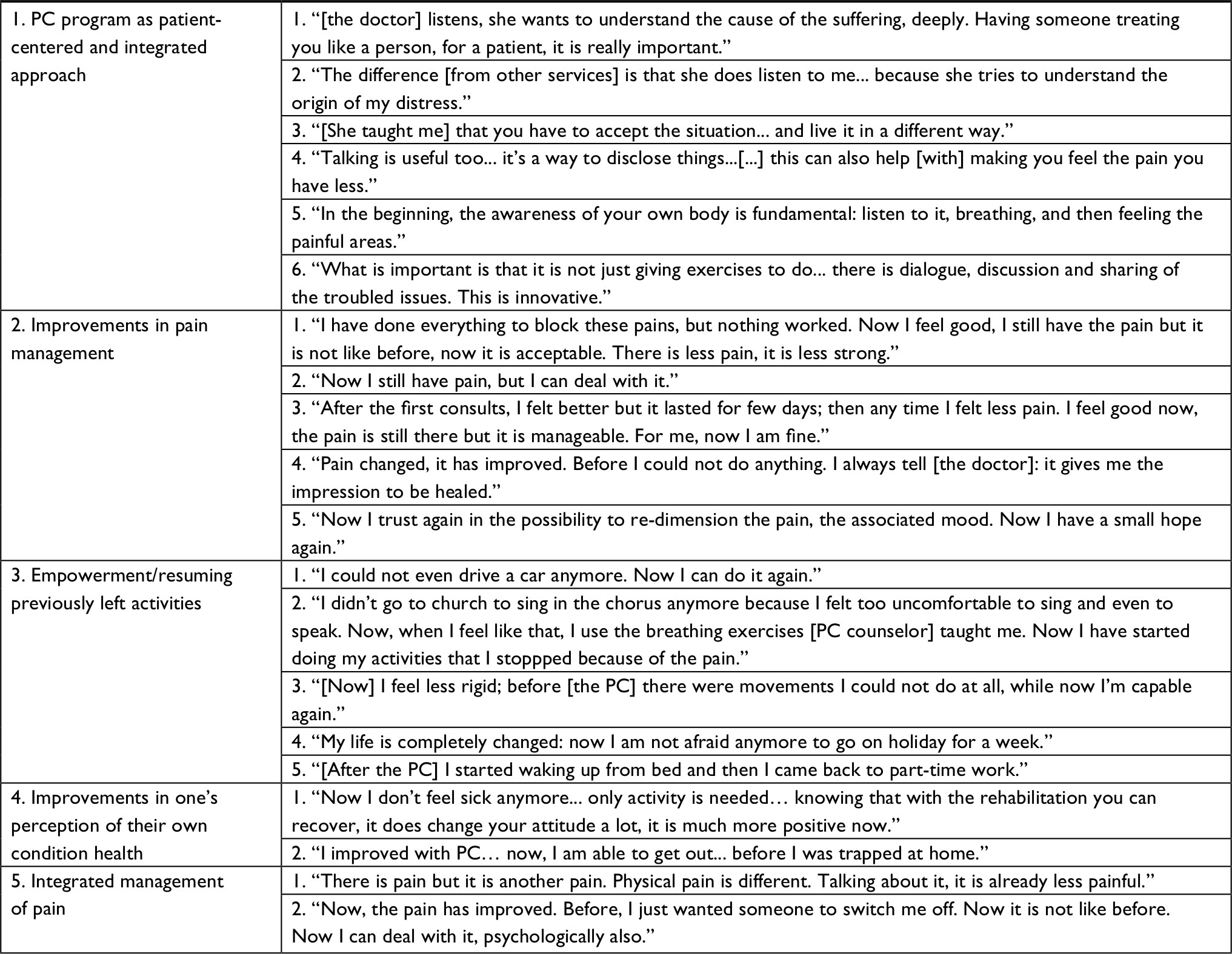 | Table 3 FM patients’ quotations during semi-structured interview after PC Note: Patient interviews were conducted in Italian. The translation to English was done by a professional translator for the manuscript preparation. Abbreviations: FM, fibromyalgia; PC, postural counseling. |
Although pain improvements were not quantified through the interviews, the outcomes of the qualitative interview clearly supported such improvement (ie, ability to handle acute episodes, resuming previously left working activities as described in the “Discussion” section).
A relevant outcome of the interviews concerns the resume of previously left activities due to FM chronic pain. Two-thirds of interviewed FM patients resumed previously left activities, while 33.3% of them were unable to determine any major changes (Table 3, quotations 3.1 and 3.5).
Participants described the integrated PC as a personalized and global care, which associated physical rehabilitation with listening practices, where individual illness narrative is the ground to work on patients’ chronic pain and its management (Table 3, quotation 1).40,41
Evaluation of clinical improvement in FM by FIQ
Baseline FIQ score of studied FM patients was 77.38±7.77, and it was significantly reduced after the integrated PC to 39.12±13.27 (P<0.0001), with a mean difference of 38.27±10.57. We then analyzed the effects of life story profiles on FIQ before and after PC. As shown in Figure 2 that depicts variation in FIQ after treatment for single patients, the absolute mean differences were similar in broken and cumulative structured patients. Considering the patients as responders who witnessed an improvement in FIQ of at least 30% from baseline, we were able to identify 19 out of 20 responders in the cumulative patients (95%) vs 18 out of 21 in the broken ones (85.71%; P=0.6).
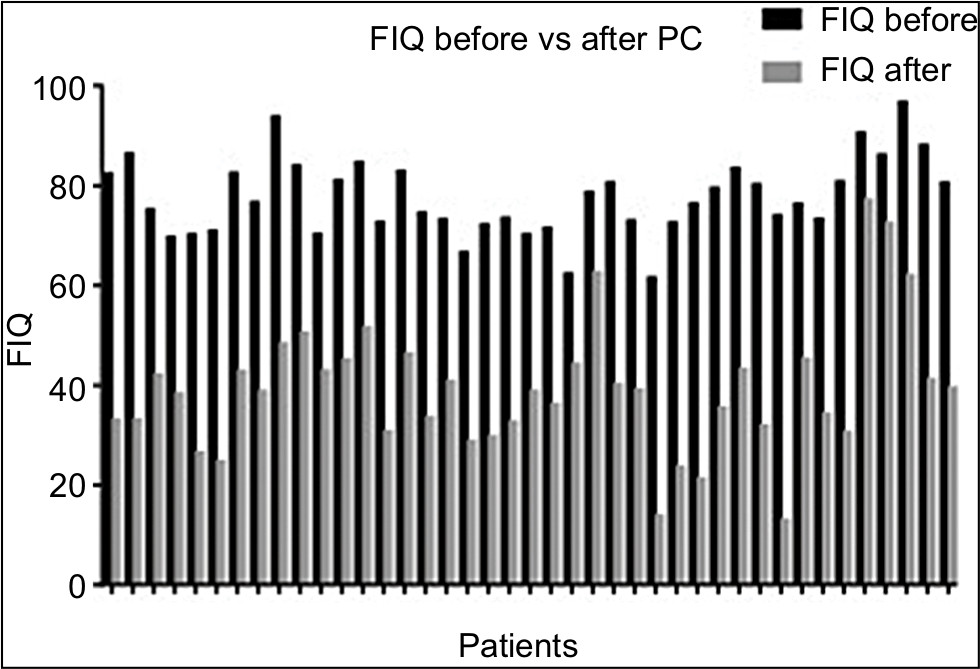 | Figure 2 Histogram depicting individual variations on FIQ score in FM patients who completed the study protocol. Note: FIQ was collected before and after PC program. Abbreviations: FIQ, FM impact questionnaire; FM, fibromyalgia; PC, postural counseling. |
Discussion
In this study, we evaluated the impact of a novel developed integrated PC rehabilitation program on FM patients. We found that combining postural rehabilitation and counseling represents a unique experience of non-pharmacological treatment of pain in FM. PC allowed FM patients to resume their own life and regenerate their own image. We propose to introduce the evaluation of the ability to resume daily activities by FM patients as additional outcome of rehabilitation programs in FM. Since the counselor physiotherapist combined investigating the patients’ illness stories, with listening and postural work in the same visit, we were able to identify two major narrative illness profiles in FM patients: the broken life pattern and the cumulative life pattern (Table 2). We found that FM subjects with broken life pattern dropped out from the PC program earlier and more frequently, compared to FM subjects with cumulative life pattern. The counselor physiotherapist assisted FM patients in the process of transformation from an entrapped victim of pain and chronic fatigue into leading actor of their own life (Table 2). During PC, FM patients felt free to talk about themselves, their fairs and their illness, receiving emotional support (Table 3, quotation 1.2). FM patients referred to PC as “safe harbor” where it was possible to share thoughts without being judged (Table 3, quotation 1.2 and 1.6). Previous studies in other diseases characterized by chronic pain and/or fatigue such as chronic low back pain or rheumatoid arthritis suggest that motivational counseling combined with exercise improves pain and ameliorates patients’ ability to deal with it daily.43–45 However, the integration of counseling and physical rehabilitation seems to be even more effective in chronic pain relief, as reported in patients with myofascial pain related to temporomandibular disorders.46
Using FIQ, we found a higher percentage of responders among the FM cumulative life pattern compared to broken life one, although it did not reach statistical significance (being a retrospective study). This finding is important, suggesting that the early identification of life story pattern might be used in the selection of FM patients for integrated PC program. It is of note that FM patients, who completed the PC program, learned how to experience difficulties related to FM illness without trying to control them (Table 3, quotation 3.4 and 4.1),42 based on a process of recreation of patients’ own body image far from pain, allowing the reconstruction of their own life (Table 2).
In fact, the interviews showed that PC helped FM patients to accept and elaborate their individual illness (Table 3, quotation 1). It is of note that FM patients reported a change in the perception of their own condition after the PC program, feeling less like an ill person (affected by an untreatable condition) and more like a person, who needs rehabilitation (Table 3, quotation 4.1). The ability of PC to tackle the variety and the complexity of individual issues represented for FM subjects the core difference between PC and classical rehabilitation approaches. In particular, the balance between practices acting on self-perception and the perception of their own postures, personal attitudes toward everyday life, allowed them to understand and deal with chronic pain and fatigue as deeply intertwined aspects (Table 3, quotations 1.2 and 1.6).47
This is particularly relevant in FM, since fatigue is one of the most common symptoms and is generally poorly handled by standard therapeutic options. The interviews support an amelioration of the perceived fatigue through both motivational tools and physical exercises learnt during the PC sessions. This allowed FM patients to deal with their daily activities and duties in the right prospective with respect to their own energies.13,48
In our study, 75% of the participants reported an amelioration of pain severity and a reduction in the frequency of acute pain episodes. In addition, the improvement in pain management has been assessed as increased ability of FM subjects to interpret body signals of a forthcoming pain attack and subsequently to better deal with it. This outcome is relevant in FM clinical management.49,50
In fact, FM patients who are more confident in self-management of pain are not entrapped by pain (Table 3, quotation 2).33 This is further supported by the empowerment reported by the large part of FM patients, who resumed previously abandoned activities because of pain and fatigue (Table 3, quotation 3). Up to now, limited data are available on the impact of non-pharmacological treatment on resuming previous activities such as job duties or hobbies in FM patients. The interviews highlighted that 75% of participants resumed previously left everyday activities with a positive impact on individual own image. As summarized in Table 3 (quotation 3.5), women highly committed to their job reported to come back to working after a period of leave or to have learnt to manage their everyday job duties in a more coherent way in relation to their condition. As summarized in Table 3 (quotations 3.1, 3.2, 3.3 and 3.4), FM subjects resume social activities after a period of abandonment due to their pain and, more generally, to difficulties in conciliating those activities with FM. These data suggest that integrated PC program positively impacts chronic pain and fatigue based on self-management strategies grown during PC. This allows FM patients to resume their own life and regenerate their own image. Based on our findings, we propose to introduce the evaluation of the ability to resume daily activities (ie, jobs and hobbies) by FM patients as additional outcome of rehabilitation programs in FM. Last but not least, the withdrawal or the reduction in the pharmacological burden further ameliorates patients’ self-image and strengthens self-confidence in the own ability to manage the disease. The clinical improvement in FM patients after PC program was also supported by FIQ data. Our results agree with recent evidences on the ACT in FM patients, showing that pain acceptance and a stable sense of self beneficially impact the functioning of FM patients in daily life activities.26,27
Implications for practice and/or policy and conclusions
Our data suggest that integrated PC program is an interesting new option as an alternative/complementary treatment for FM since it positively impacts chronic pain and fatigue. Integrated PC program allows FM patients to resume their own life and regenerate their own image. PC helps FM patients 1) to ask for new perspectives on FM, considered as physical illness that requires rehabilitation; 2) to gain new individual perspective on FM, such as recreation of body image and reconstruction of their own life and 3) to improve self-pain management and body perception (Figure 3). The main limitation of the present study is the absence of a control group. However, our data highlight the importance of integrated rehabilitation approaches to FM and generate the rationale to design a large randomized study to fully understand the impact of PC on FM. The evaluation of patients’ ability to resume daily activities may be considered as possible additional outcome of rehabilitation programs in FM as well as in other disorders characterized by chronic pain.
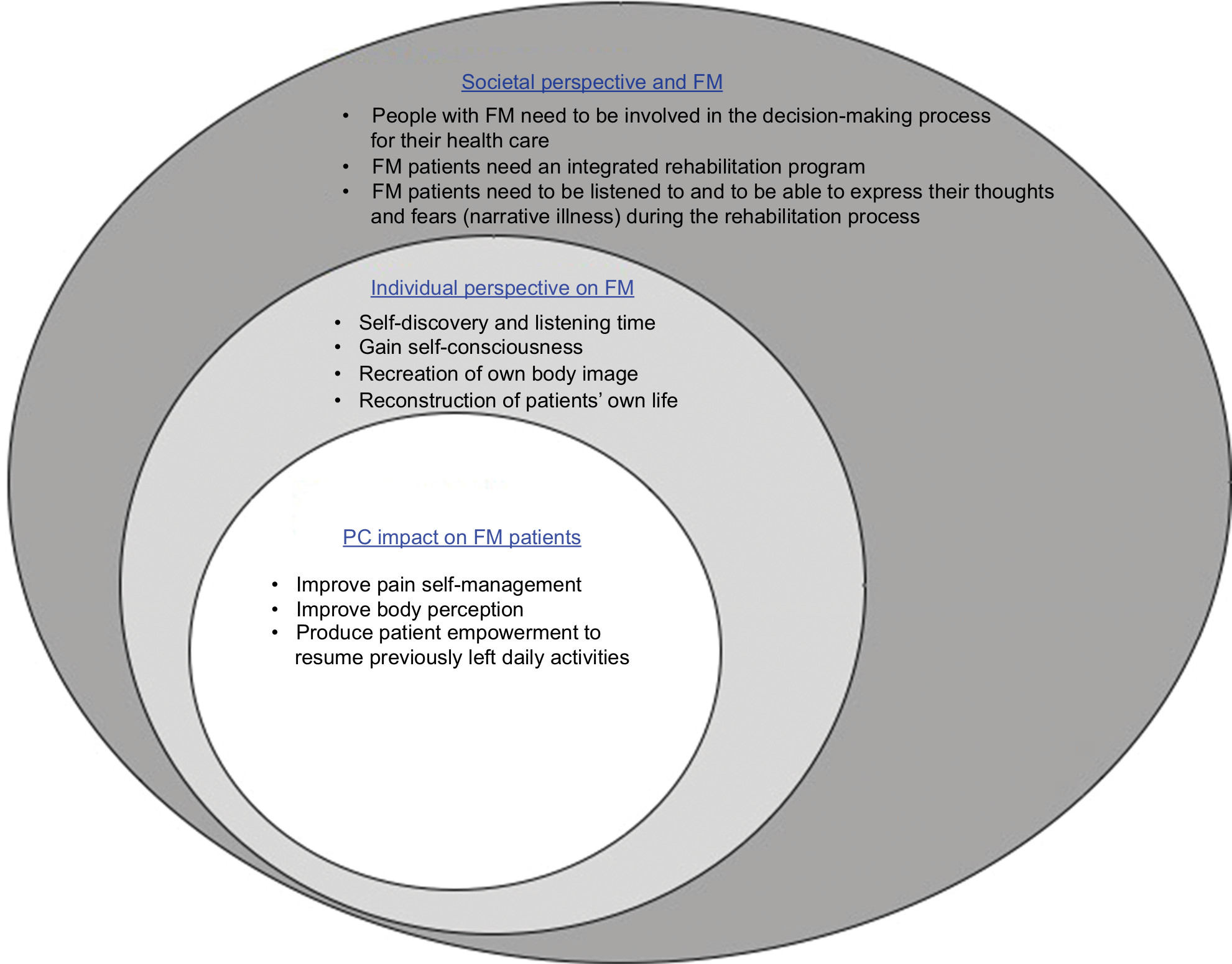 | Figure 3 A clinical model of care in FM patients based on PC program outcomes. Notes: The clinical care in FM should take into account the contextual factor as well as societal and individual perspective in designing a rehabilitation program such as a PC program. This successfully impacts both individual perspective of FM and the ability of patients to deal with FM symptoms, such as pain and fatigue daily. Abbreviations: FM, fibromyalgia; PC, postural counseling. |
Acknowledgment
This study is dedicated to Professor Lisa Maria Bambara who was a pioneer in rheumatologic disorders, combining the scientific and biopsychosocial approaches.
Author contributions
P Caramaschi, D Biasi and A Carletto were the rheumatologists in charge of FM patients, and they collected and analyzed the patients’ data and wrote the paper. C Galvani and G Ongaro were the counselor physiotherapists involved in FM treatment, collected illness narratives, analyzed the data and wrote the paper. L De Franceschi, P Mura, M Evangelista, A Paladini and G Finco analyzed the data and wrote the paper. A Ciannameo, A Piroli and E Arnaudo carried out the interviews, analyzed the data and wrote the paper. A Piroli and G Varrassi wrote and reviewed the paper. All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Clauw DJ. Fibromyalgia: a clinical review. JAMA. 2014;311(15):1547–1555. | ||
Fitzcharles MA, Yunus MB. The clinical concept of fibromyalgia as a changing paradigm in the past 20 years. Pain Res Treat. 2012;2012:184835. | ||
Coaccioli S, Varrassi G, Sabatini C, Marinangeli F, Giuliani M, Puxeddu A. Fibromyalgia: nosography and therapeutic perspectives. Pain Pract. 2008;8(3):190–201. | ||
Varrassi G, Fusco M, Coaccioli S, Paladini A. Chronic pain and neurodegenerative processes in elderly people. Pain Pract. 2015;15(1):1–3. | ||
Chang RW, Semanik PA, Lee J, Feinglass J, Ehrlich-Jones L, Dunlop DD. Improving physical activity in arthritis clinical trial (IMPAACT): study design, rationale, recruitment, and baseline data. Contemp Clin Trials. 2014;39(2):224–235. | ||
Paladini A, Marinangeli F, Coaccioli S, Varrassi G. New perspectives in chronic and neuropathic pain in older population. SOJ Anesthesiol Pain Manag. 2015;2:1–3. | ||
Phillips K, Clauw DJ. Central pain mechanisms in the rheumatic diseases: future directions. Arthritis Rheum. 2013;65(2):291–302. | ||
Crawford BK, Piault EC, Lai C, Bennett RM. Assessing fibromyalgia-related fatigue: content validity and psychometric performance of the Fatigue Visual Analog Scale in adult patients with fibromyalgia. Clin Exp Rheumatol. 2011;29(6 Suppl 69):S34–43. | ||
Okifuji A, Bradshaw DH, Donaldson GW, Turk DC. Sequential analyses of daily symptoms in women with fibromyalgia syndrome. J Pain. 2011;12(1):84–93. | ||
Peñacoba Puente C, Velasco Furlong L, Écija Gallardo C, Cigarán Méndez M, Bedmar Cruz D, Fernández-de-Las-Peñas C. Self-efficacy and affect as mediators between pain dimensions and emotional symptoms and functional limitation in women with fibromyalgia. Pain Manag Nurs. 2015;16(1):60–68. | ||
Umeda M, Corbin LW, Maluf KS. Examination of contraction-induced muscle pain as a behavioral correlate of physical activity in women with and without fibromyalgia. Disabil Rehabil. 2015;37(20):1864–1869. | ||
Ustinova KI, Langenderfer JE. Postural stabilization by gripping a stick with different force levels. Gait Posture. 2013;38(1):97–103. | ||
Vincent A, Benzo RP, Whipple MO, McAllister SJ, Erwin PJ, Saligan LN. Beyond pain in fibromyalgia: insights into the symptom of fatigue. Arthritis Res Ther. 2013;15(6):221. | ||
Ang DC, Kaleth AS, Bigatti S, et al. Research to encourage exercise for fibromyalgia (REEF): use of motivational interviewing, outcomes from a randomized-controlled trial. Clin J Pain. 2013;29(4):296–304. | ||
Fitzcharles MA, Ste-Marie PA, Panopalis P, Ménard H, Shir Y, Wolfe F. The 2010 American college of rheumatology fibromyalgia survey diagnostic criteria and symptom severity scale is a valid and reliable tool in a French speaking fibromyalgia cohort. BMC Musculoskelet Disord. 2012;13:179. | ||
Miró E, Martínez MP, Sánchez AI, Prados G, Medina A. When is pain related to emotional distress and daily functioning in fibromyalgia syndrome? The mediating roles of self-efficacy and sleep quality. Br J Health Psychol. 2011;16(4):799–814. | ||
Sallinen M, Kukkurainen ML, Peltokallio L, Mikkelsson M. Women’s narratives on experiences of work ability and functioning in fibromyalgia. Musculoskeletal Care. 2010;8(1):18–26. | ||
Sallinen M, Kukkurainen ML, Peltokallio L, Mikkelsson M, Anderberg UM. Fatigue, worry, and fear-life events in the narratives of women with fibromyalgia. Health Care Women Int. 2012;33(5):473–494. | ||
Stuifbergen AK, Phillips L, Voelmeck W, Browder R. Illness perceptions and related outcomes among women with fibromyalgia syndrome. Womens Health Issues. 2006;16(6):353–360. | ||
Giordano J, Schatman ME. A crisis in chronic pain care: an ethical analysis. Part three: Toward an integrative, multi-disciplinary pain medicine built around the needs of the patient. Pain Physician. 2008;11(6):775–784. | ||
Di Tella M, Castelli L, Colonna F, et al. Theory of mind and emotional functioning in fibromyalgia syndrome: an investigation of the relationship between social cognition and executive function. PLoS One. 2015;10(1):16. | ||
Castelli L, Tesio V. Commentary: Mindfulness training for reducing anger, anxiety, and depression in fibromyalgia patients. Front Psychol. 2016;7:740. | ||
Amutio A, Franco C, Pérez-Fuentes MC, Gázquez JJ, Mercader I. Mindfulness training for reducing anger, anxiety, and depression in fibromyalgia patients. Front Psychol. 2014;5:1572. | ||
Lawson K. Treatment options and patient perspectives in the management of fibromyalgia: future trends. Neuropsychiatr Dis Treat. 2008;4(6):1059–1071. | ||
Perry R, Leach V, Davies P, Penfold C, Ness A, Churchill R. An overview of systematic reviews of complementary and alternative therapies for fibromyalgia using both AMSTAR and ROBIS as quality assessment tools. Syst Rev. 2017;6(1):97. | ||
Yu L, Norton S, Almarzooqi S, McCracken LM. Preliminary investigation of self-as-context in people with fibromyalgia. Br J Pain. 2017;11(3):134–143. | ||
Yu L, Norton S, McCracken LM. Change in “self-as-context” (“Perspective-Taking”) occurs in acceptance and commitment therapy for people with chronic pain and is associated with improved functioning. J Pain. 2017;18(6):664–672. | ||
Kleinman A. Concepts and a model for the comparison of medical systems as cultural systems. Soc Sci Med. 1978;12(2B):85–93. | ||
Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990;33(2):160–172. | ||
Arnold LM, Emir B, Pauer L, Resnick M, Clair A. Time to improvement of pain and sleep quality in clinical trials of pregabalin for the treatment of fibromyalgia. Pain Med. 2015;16(1):176–185. | ||
Larsson A, Palstam A, Löfgren M, et al. Resistance exercise improves muscle strength, health status and pain intensity in fibromyalgia-a randomized controlled trial. Arthritis Res Ther. 2015;17:161. | ||
Coirault C, Chemla D, Lecarpentier Y. Relaxation of diaphragm muscle. J Appl Physiol. 1999;87(4):1243–1252. | ||
Mcmahon L, Murray C, Sanderson J, Daiches A. “Governed by the pain”: narratives of fibromyalgia. Disabil Rehabil. 2012;34(16):1358–1366. | ||
Pelaez Cf CL. The use of McGill illness narrative interview (MINI) in fibromyalgia patients. An experience from Spain. In: 19th European Congress of Psychiatry. 2011;26:1002. | ||
Williams G. The genesis of chronic illness: narrative re-construction. Sociol Health Illn. 1984;6(2):175–200. | ||
Ang D, Kesavalu R, Lydon JR, Lane KA, Bigatti S. Exercise-based motivational interviewing for female patients with fibromyalgia: a case series. Clin Rheumatol. 2007;26(11):1843–1849. | ||
Busch AJ, Webber SC, Richards RS, et al. Resistance exercise training for fibromyalgia. Cochrane Database Syst Rev. 2013;(12):CD010884. | ||
Egeli NA, MacMillan PD. Fibromyalgia: predicting openness to counselling referrals. Psychol Health. 2008;23(5):569–584. | ||
Muto LH, Sauer JF, Yuan SL, Sousa A, Mango PC, Marques AP. Postural control and balance self-efficacy in women with fibromyalgia: are there differences? Eur J Phys Rehabil Med. 2015;51(2):149–154. | ||
Sim J, Madden S. Illness experience in fibromyalgia syndrome: a metasynthesis of qualitative studies. Soc Sci Med. 2008;67(1):57–67. | ||
del Giorno R, Skaper S, Paladini A, Varrassi G, Coaccioli S. Palmitoylethanolamide in fibromyalgia: Results from prospective and retrospective observational studies. Pain Ther. 2015;4(2):169–178. | ||
Sallinen M, Kukkurainen ML, Peltokallio L. Finally heard, believed and accepted-peer support in the narratives of women with fibromyalgia. Patient Educ Couns. 2011;85(2):e126–e130. | ||
Angel S, Jensen LD, Gonge BK, Maribo T, Schiøttz-Christensen B, Buus N. Patients’ interpretations of a counselling intervention for low back pain: a narrative analysis. Int J Nurs Stud. 2012;49(7):784–792. | ||
Buus N, Jensen LD, Maribo T, Gonge BK, Angel S. Low back pain patients’ beliefs about effective/ineffective constituents of a counseling intervention: a follow-up interview study. Disabil Rehabil. 2015;37(11):936–941. | ||
Esbensen BA, Thomsen T, Hetland ML, et al. The efficacy of motivational counseling and SMS-reminders on daily sitting time in patients with rheumatoid arthritis: protocol for a randomized controlled trial. Trials. 2015;16:23. | ||
de Laat A, Stappaerts K, Papy S. Counseling and physical therapy as treatment for myofascial pain of the masticatory system. J Orofac Pain. 2003;17(1):42–49. | ||
Dennis NL, Larkin M, Derbyshire SW. ‘A giant mess’-making sense of complexity in the accounts of people with fibromyalgia. Br J Health Psychol. 2013;18(4):763–781. | ||
Humphrey L, Arbuckle R, Mease P, Williams DA, Samsoe BD, Gilbert C. Fatigue in fibromyalgia: a conceptual model informed by patient interviews. BMC Musculoskelet Disord. 2010;11:216. | ||
Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient Educ Couns. 2002;48(2):177–187. | ||
Kett C, Flint J, Openshaw M, Raza K, Kumar K. Self-management strategies used during flares of rheumatoid arthritis in an ethnically diverse population. Musculoskeletal Care. 2010;8(4):204–214. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.