")
Back to Journals » Cancer Management and Research » Volume 12
Postoperative Radiotherapy for Thoracic Esophageal Carcinoma with Upfront R0 Esophagectomy
Received 10 October 2020
Accepted for publication 10 December 2020
Published 18 December 2020 Volume 2020:12 Pages 13023—13032
DOI https://doi.org/10.2147/CMAR.S286074
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Eileen O'Reilly
Yichun Wang, Fan Wang
Department of Radiation Oncology, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, People’s Republic of China
Correspondence: Yichun Wang Department of Radiation Oncology
The First Affiliated Hospital of Anhui Medical University, No. 218, Jixi Road, Hefei, 230022 Anhui, People’s Republic of China
Tel +86-18019979312
Email [email protected]
Abstract: Multidisciplinary therapies can improve the survival of patients with locally advanced esophageal carcinoma. However, the determination of the optimal modality is still a controversial subject. Many randomized controlled trials in the late 20th century showed that there was no survival benefit when postoperative radiotherapy was added to surgery for esophageal carcinoma. As a result, the treatment modality shifted thereafter to neoadjuvant therapies. Even so, these trials are criticized for many limitations and an increasing number of studies (mainly nonrandomized controlled trials) has indicated that postoperative radiotherapy/chemoradiotherapy can improve the survival of patients with a poor prognosis after R0 esophagectomy. Additionally, a large number of patients with locally advanced esophageal carcinoma still choose upfront surgery in the clinical practice due to many reasons. Therefore, postoperative radiotherapy seems to be a feasible treatment for these patients with a poor prognosis, particularly in the new era of conformal radiotherapy. Here, we review published studies on postoperative radiotherapy/chemoradiotherapy, and we discuss the clinical issues related to postoperative radiotherapy, such as the indication, target volume, total radiation dosage, time interval and complications of postoperative radiotherapy with or without chemotherapy, to make recommendations of postoperative radiotherapy for both current practice and future research in esophageal carcinoma.
Keywords: esophageal neoplasm, postoperative radiotherapy, survival, clinical target volume
Introduction
Esophageal carcinoma (EC) is the sixth most common cause of cancer-related death worldwide and contributes to a major global health burden.1 Surgery is the cornerstone of treatment for resectable EC; unfortunately, survival is very poor for patients who undergo surgery alone (SA).2 To improve survival, multidisciplinary therapies have been studied worldwide. Due to the unsuccessful or even poor results in the trials of the late 20th century,3–7 postoperative radiotherapy (PORT) is therefore not recommended for patients with negative margin diseases after esophagectomy and the multidisciplinary approach shifts to neoadjuvant therapies.2 However, surgery is still the first choice for a large number of patients due to many reasons in the real world, particularly in many underdeveloped or developing countries.8,9 Both locoregional recurrence and distant organ metastasis represent common treatment failures for patients with SA.10–13 Therefore, in the opinion of most physicians, upfront SA is thought to be insufficient for diseased patients who have a poor prognosis (such as pT3/4 or pN+). Despite the lack of more randomized controlled trials (RCTs), many published studies have suggested that postoperative radiotherapy/chemoradiotherapy can improve survival in many patients with locally advanced EC.14–16
PORT has the advantage of providing reasonable treatment according to the accurate pathological stage. On the one hand, many patients with inaccurately staged early EC can avoid overtreatment, and on the other hand, PORT can be chosen for many clinical early-stage EC cases with pathological upstaged diseases. Moreover, the pathological results provide an important clue for the design of the target volume, which may be a feasible method of individualized PORT. However, there is little consensus on the optimal populations, target volume, dosage, time interval and combined approach for PORT of EC. The aim of this paper is to review previous studies, to detail the clinical issues and to make recommendations of PORT for both current practice and future EC research.
Literature Review
Identification of Studies
Electronic databases, including PubMed, Scopus, EMBASE, Web of Science, and the Cochrane Library were searched for relevant studies until June 2020. The following key words were searched: (“esophageal” OR “oesophageal” OR “esophagus” OR “oesophagus”) AND (“cancer” OR “carcinoma” OR “tumor” OR “neoplasm”) AND (“adjuvant” OR “postoperative” OR “post” OR “perioperative” OR “peri”) AND (“radiotherapy” OR “chemoradiotherapy”). All the retrieved studies were screened in Endnote X8.1. The reference lists of the included studies, meta-analyses and systematic reviews were also manually searched to identify any eligible studies that reported the efficacy of surgery followed by radiotherapy (S+RT) or chemoradiotherapy (S+CRT).
S+RT or S+CRT versus SA
Eight RCTs compared the survival differences between S+RT and SA for EC.3–7,17–19 As shown in Table 1, five RCTs were conducted in the late 20th century3–7 and five RCTs were conducted in China.5,6,17–19 All patients in these studies had esophageal squamous cell carcinoma (ESCC) except one study that enrolled patients with cardia adenocarcinoma.5 The 100% R0 resection rate was recorded in four studies4,17–19 and two studies included patients with positive M1a nodes.4,7 There was no survival difference between S+RT and SA in six studies.3,4,6,7,17,19 In one study, the S+RT group had poor survival compared to the SA group (P<0.05).6 Wang and colleagues found that S+RT improved not only disease-free survival (DFS) (34.9% vs.11.3%, P <0.001) but also 5-year overall survival (OS) (48.1% vs 30.2%, P=0.007) compared to SA in pT2N0M0 ESCC patients with high Ku80 expression.18 Although there was no OS difference in the study of Xiao and colleagues, subgroup analysis showed that S+RT can improve the 5-year OS from 13.1% to 35.1% for patients with stage III ESCC (P=0.027) and from 14.7% to 29.2% for patients with positive lymph nodes (P=0.0698).17 In the latest RCT, S+RT improved the 3-year DFS from 58.7% to 75.1% (P=0.03) and decreased the locoregional recurrence rate from 32.5% to 10.0% (P=0.001) in patients with pT2-3N0M0 ESCC.19
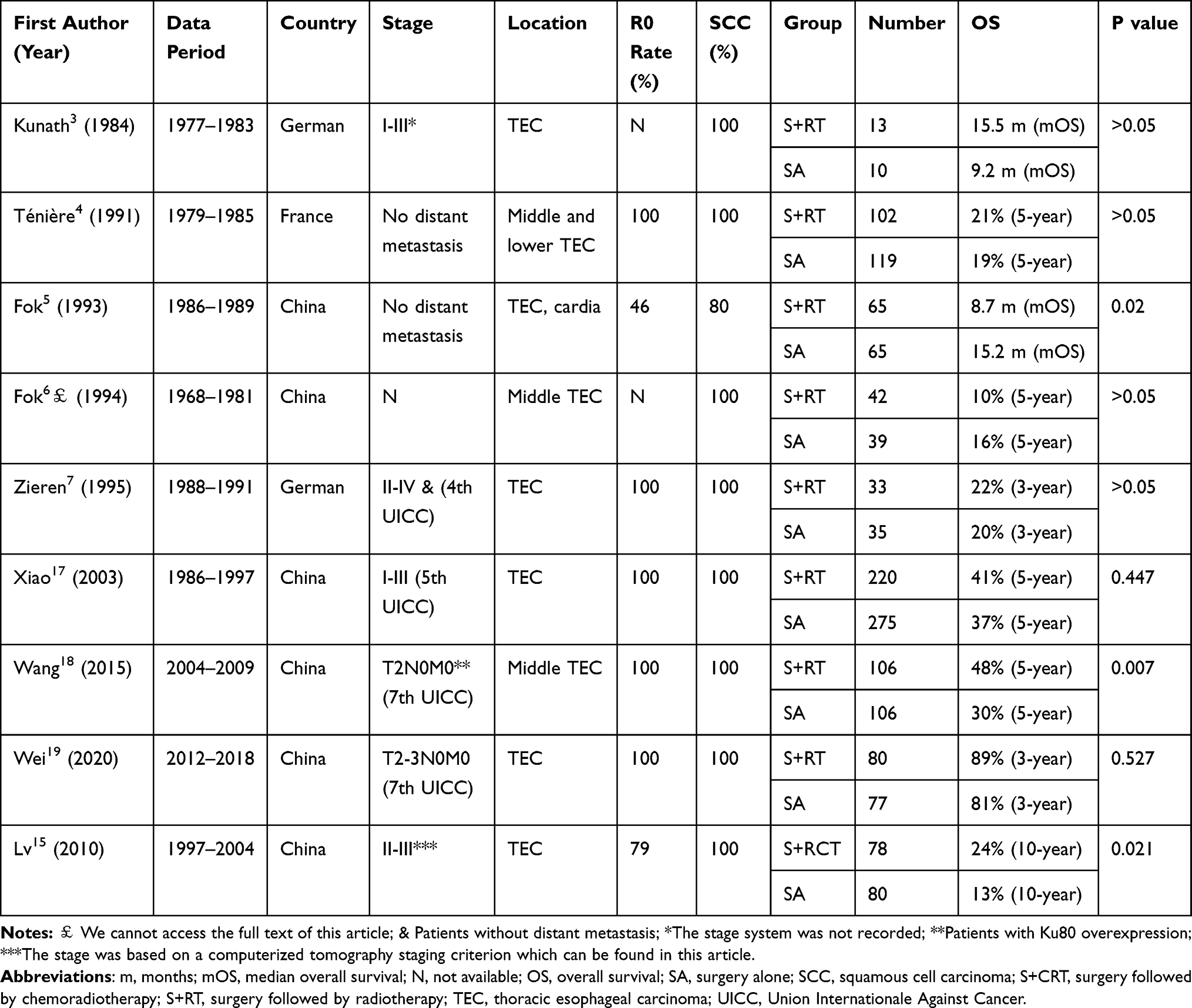 |
Table 1 RCTs Compared S+RT/S+RCT with SA for EC |
Only one RCT compared the survival differences between S+CRT and SA for stage II–III ESCC15 (Table 1). In this study, 78 patients were in the S+CRT group and 80 patients were in the SA group. There were significant differences in the 3-, 5-, and 10-year DFS (61.1%, 37.2%,17.8% vs 49.3%, 25.9%, 6.2%, P<0.05) and in the 3-, 5-, and 10-year OS (62.8%, 42.3%, 24.4% vs 51.3%, 33.8%, 12.5%, P<0.05). The local recurrence rates in the S+CRT group and the SA group were 14.1% and 35%, respectively (P<0.05). No significant differences were detected when comparing complications.
A large number of retrospective studies have suggested that S+RT or S+CRT can improve survival for patients with poor prognostic factors, such as node-positive disease, stage III/IV disease, large tumors, and advanced T stage.8,9,16,20–27 A meta-analysis based on four RCTs and eight non-RCTs suggested that PORT was promising in improving 3-year OS and reducing the locoregional recurrence rate.28 Another meta-analysis based on thirteen published studies confirmed that S+CRT yielded a significant survival benefit and improved local-regional control with tolerable toxicity for EC.14
S+CRT versus S+RT
There was no RCT comparing the efficacy between S+CRT and S+RT. Five retrospective studies, including two in China, two in America and one in Japan, were found after a systematic search (Table 2). Of them, four studies confirmed that S+CRT can improve survival compared with S+RT.8,24,29,30 The Japanese study showed that there was no survival difference between S+CRT and S+RT. However, this study was criticized for a low sample size (only 19 patients in each group).31
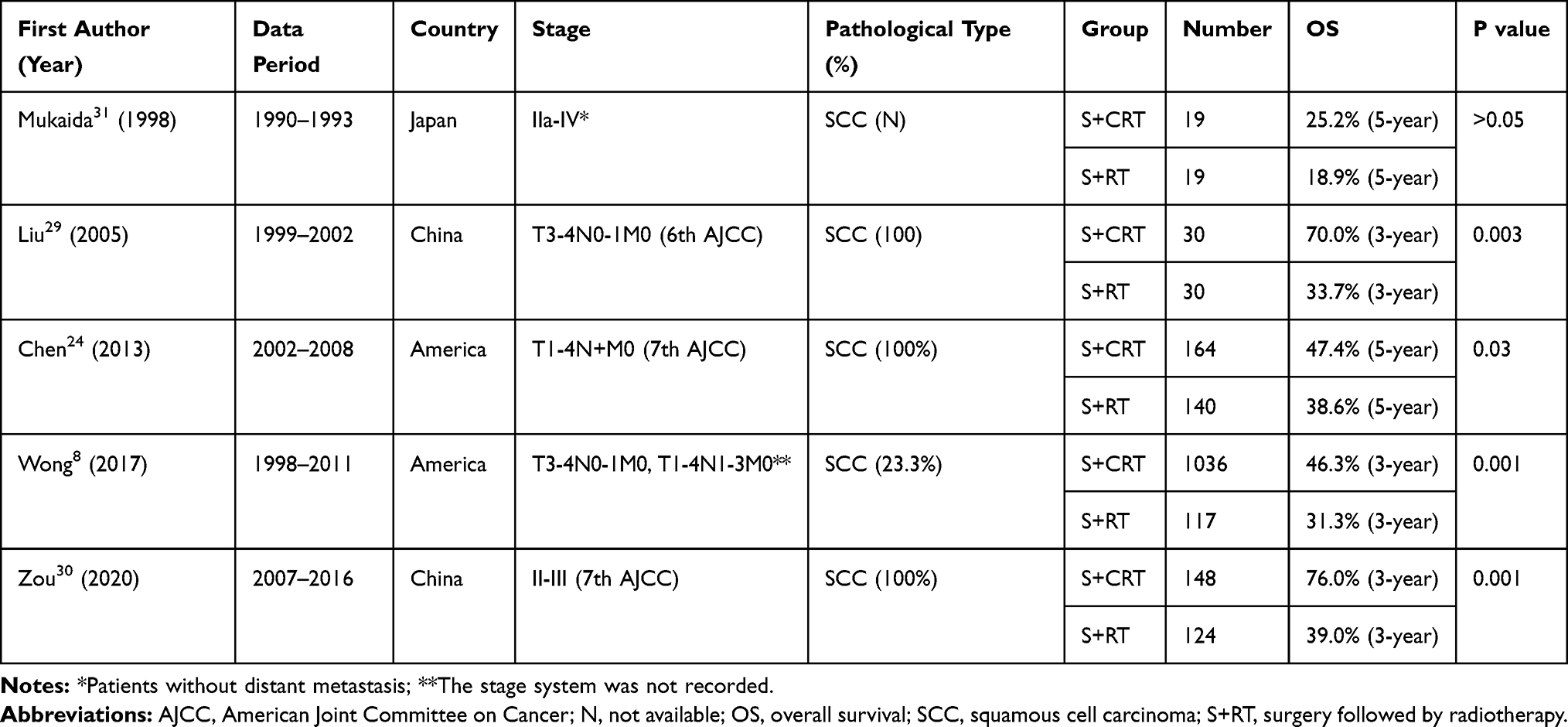 |
Table 2 Retrospective Studies Compared S+CRT with S+RT for EC |
S+CRT versus Neoadjuvant Chemoradiotherapy Followed by Surgery (CRT+S)
Two prospective RCTs15,32 and six retrospective control studies33–38 compared S+CRT with CRT+S directly. Their characteristics are presented in Table 3. Most studies were conducted in Asian countries, including three in China,15,32,36 one in Taiwan37 and one in Iran.38 Most retrospective studies33–38 and published RCTs15 suggested that there were no significant differences in OS between CRT+S and S+CRT. However, most studies showed a trend toward survival benefits in the CRT+S group, except for one study.38 Only one study showed significant survival benefits in the CRT+S group.32
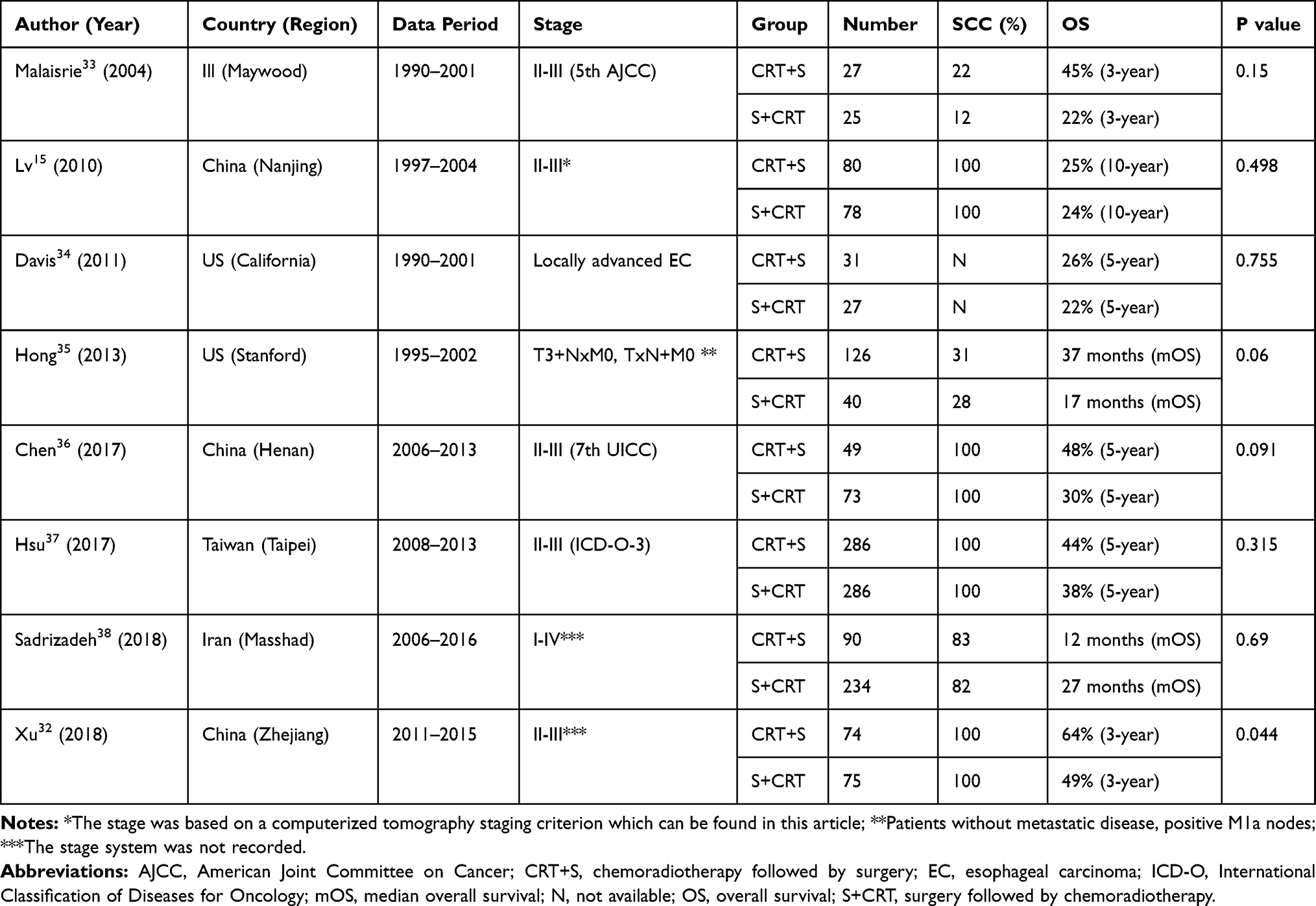 |
Table 3 Studies Compared S+CRT with CRT+S for EC |
Controversies of Clinical Issues
Indications
In the NCCN guidelines, surveillance is recommended for clinical T1-2N0M0 EC patients with negative margins (R0 resection) after radical surgery regardless of the pathological stage (p Any T, Any N) and CRT+S is recommended for patients with resectable clinical T3-4N0M0 or T1-4N+M0 diseases. However, there is no recommendation for patients with pathological T3-4N0M0 or T1-4N+M0 diseases who do not receive any preoperative therapies. It is assumed that upfront SA may not be insufficient for patients with poor prognostic factors. According to the results of Xiao’s RCT17 and a large number of retrospective studies,8,20,22,24–27 PORT is associated with improved survival for patients with node-positive disease. Therefore, in the latest Guideline of the Chinese Society of Clinical Oncology (CSCO), it is suggested that S+RT or S+CRT may be chosen for patients with node-positive disease in the annotations. Although there was no recommendation in all guidelines, PORT can also improve the survival of patients with stage III EC according to the results of Xiao’s RCT17 and many retrospective studies.9,16,20,39 For patients with pT3N0M0 EC, adjuvant conformal radiotherapy may also be associated with improved survival.23 Although CRT+S is now recommended for resectable locally advanced EC, there are few RCTs comparing CRT+S and S+CRT directly and most studies showed that there was no survival difference (Table 3). The optimal timing of chemoradiation combined with surgery will continue to be debated. To these points, S+RT or S+CRT should also be considered for EC, particularly clinical early-stage EC with pathological upstaged diseases and locally advanced EC without preoperative therapies. However, more multicenter RCTs are needed to confirm these findings.
Combination with Chemotherapy
There is a high occurrence of distant organ metastasis for EC. In the CROSS trial, blood metastasis occurred in 47.8% of patients with SA,12 which was similar to finding in other studies.10,13 Chemotherapy can not only decrease distant recurrence but also be a radiotherapy sensitizer when concurrent chemoradiotherapy is used. Therefore, it should be another important part of multimodality therapy for EC. The RTOG 85–01 trial confirmed that combined chemotherapy and radiotherapy increased the survival of patients with T1-3N0-1M0 ESCC compared with radiotherapy alone40 and chemotherapy or chemoradiotherapy is recommended as the standard neoadjuvant treatment for locally advanced EC.2 For adjuvant therapies, the combination of chemotherapy and radiotherapy can also improve survival compared with adjuvant radiotherapy alone according to many retrospective studies8,24,29,30 (Table 2) and a meta-analysis.41 Above all, the addition of chemotherapy should provide better survival than adjuvant radiotherapy alone.
In EC, neoadjuvant or definitive concurrent chemoradiotherapy is recommended.42,43 However, it remains unclear whether concurrent chemoradiotherapy or sequential setting is more beneficial for postoperative treatment. Wang AT and colleagues analyzed 4893 patients in the National Cancer Data Base (NCDB) from 1998 to 2011 and found that postoperative chemoradiation (either sequentially or concomitantly) after surgery was associated with improved OS for patients with node-positive disease or positive margins, and sequential setting was associated with the best survival (P<0.001).8 The presumable reason may be the lower toxicity in the sequential group due to the poor performance status after esophagectomy. Similar results were found in the adjuvant therapies for locally advanced or incompletely resected non-small-cell lung cancer.44 However, the concurrent chemoradiotherapy group was associated with improved 1-year, 3-year and 5-year OS tolerable toxicity compared to the nonconcurrent chemoradiotherapy group in a meta-analysis.14 Therefore, more studies should be conducted to identify the optimal sequencing of the addition of chemotherapy.
Target Volume
Due to the complex lymphatic drainage system,45 it is always challenging to design an appropriate target volume for preoperative, postoperative, or definitive radiotherapy in EC. Many target volumes have been used in past decades for PORT of EC, including: (1) a 3 to 5 cm margin at both the cephalad and caudal ends and a 1 to 2 cm margin around the initial tumor;5,46 (2) the supraclavicular areas and whole mediastinum with or without celiac areas (left gastric or/and paracardiac lymph nodes);4,15,17,47 (3): the supraclavicular areas and part of the mediastinum (from the cricothyroid membrane to 3 cm below the carina for proximal diseases and from the T1 vertebra to 3 cm below the primary tumor bed for middle and lower diseases);19,48 (4) a T-shaped field that includes only the bilateral supraclavicular area, upper and middle mediastinum, and primary tumor bed (from the upper edge of the sixth cervical vertebra to 3 cm below the carina for proximal diseases to the lower edge of the primary gross tumor for middle and lower diseases);24 (5): the bilateral supraclavicular areas and upper mediastinum;18,49 and (6) others.3,7,39 The irradiation fields of PORT used in the RCTs are shown in Table 4.
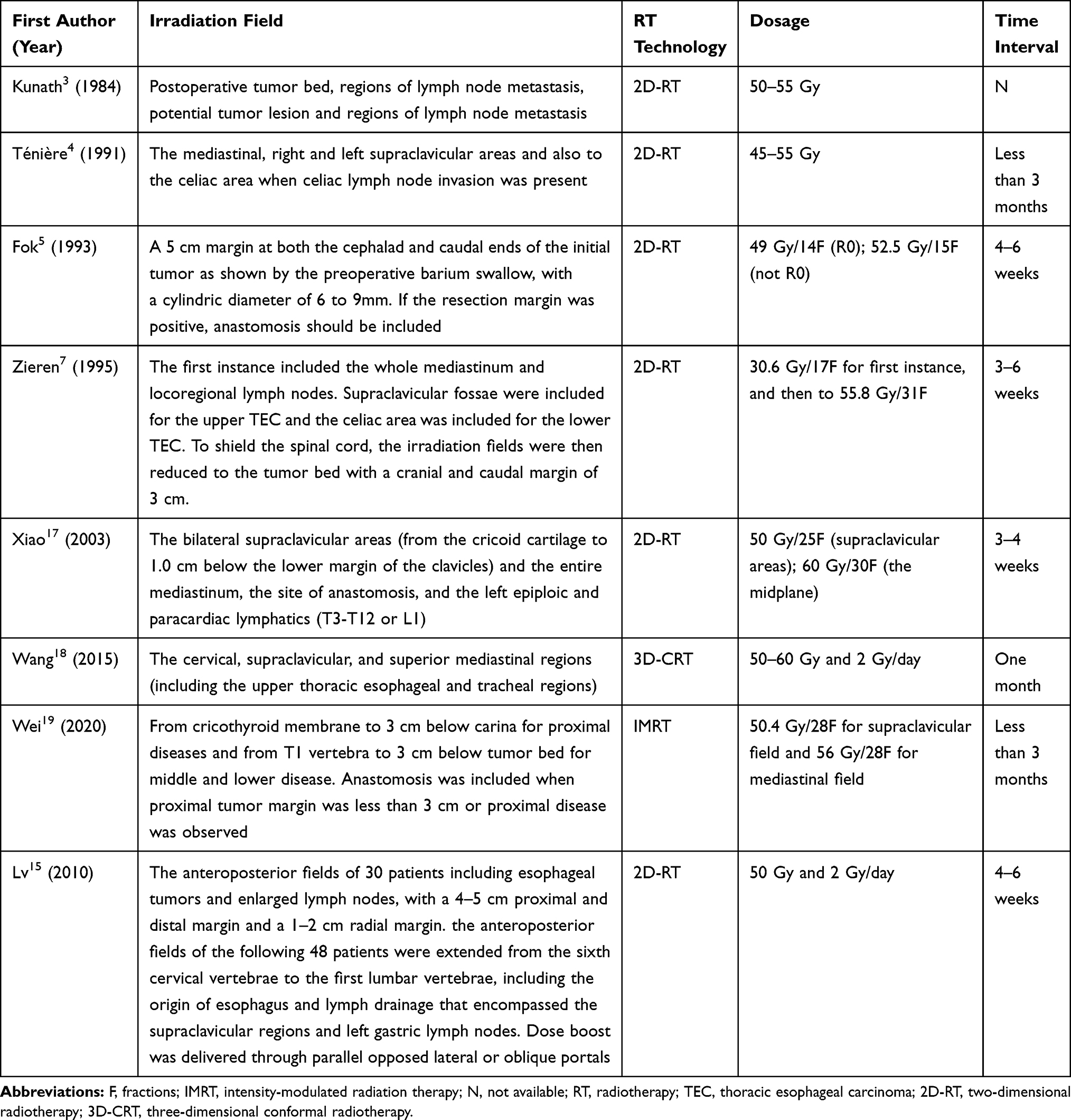 |
Table 4 Methods of PORT in the RCTs |
An appropriate target volume may not only decrease recurrence but also decrease radiotherapy-related complications. There are at least three important factors affecting the delineation of the lymph node target volume of PORT in EC. The first factor is the characteristics of the lymphatic drainage of the esophagus, which we reviewed elsewhere.45 Because of direct drainage to many important extramural lymph nodes from submucosal vessels and bidirectional drainage, lymph node metastasis is frequently present in many important extramural lymph nodes in the lower neck, upper mediastinum, and perigastric areas for all thoracic ECs, even for early-stage diseases. As a result, lymph node metastasis of EC is fairly unpredictable, characterized by wide-range, bidirectional and skipping metastasis. The second factor is the surgical procedure. Two-field lymphadenectomy (2FL) or three-field lymphadenectomy (3FL) are both used in clinical practice. The standard 2FL consists of intrathoracic lymph node dissection from the subcarinal space down to the hiatus and upper abdominal lymph node dissection. Extended 2FL and 3FL may increase the chance of complete resection of positive lymph nodes. However, regardless of whether 2FL or 3FL is used, the cervical, upper mediastinal and paraaortic lymph nodes are usually not resected or not completely resected because of the complex anatomical structures in these regions and the limitations of the surgery itself. The third factor is the recurrence pattern after upfront surgery. A large number of published studies have suggested that locoregional recurrence, particularly lymph node recurrence in the cervical, upper mediastinal and paraaortic regions, is a common relapse after surgery.10–13,50–52 Above all, the cervical, upper mediastinal and paraaortic regions should be the major regions for PORT of thoracic EC.
Additionally, the tumor bed and anastomosis have been taken into consideration for PORT in various tumors.53,54 In fact, the tumor bed was commonly included in the target volume of PORT in previous studies in EC.3,5,7,15,19 However, according to many retrospective studies, the recurrence rate of the tumor bed is very low in patients with EC after radical surgery,50 even in patients with pT3-4 stages.55,56 The recurrence rate of the anastomotic site is usually less than 5.0% (2.8–8.7%).10,12,57–59 To these points, these sites may not be necessary in the clinical target volume (CTV) of PORT for thoracic EC. However, the sites of recurrence can be affected by various factors, such as the tumor itself (TNM stage, histological subtype, differentiation, tumor location, region of positive lymph node, etc.), the operation method, the extent of lymphadenectomy, among others. Therefore, personalized target volume should be considered in clinical practice.
Total Radiation Dose (TRD)
As shown in Table 4, the TRD of PORT is 45 to 60 Gy and the single fractional dose is usually 1.8 or 2 Gy for EC in the RCTs. The determination of the optimal TRD for treating EC is still controversial. A retrospective study analyzed the effect of TRD on the outcome in patients with PORT for ESCC.46 In this study, 54 patients were classified into two groups based on TRD delivery: the low group (less than 50 Gy) and the high group (at least 50 Gy). Although the high group was marginally significant for improved OS (hazard ratio (HR)=0.559, P=0.066), it was statistically significant for improved DFS (HR=0.398, P=0.011), and locoregional recurrence-free survival (HR=0.165, P=0.001) with acceptable complications. It has also been found that the 90% plus control point is 50 Gy for both squamous cell carcinomas of the upper respiratory and digestive tracts and adenocarcinomas of the breast.60 Therefore, it is recommended that the TRD should be at least 50 Gy in PORT for EC. However, there is no RCT to confirm this result. Moreover, it is questionable whether the TRD should decrease when chemotherapy is added to PORT.
Time Interval After Surgery
PORT should start within 6 weeks after surgery; two RCTs specified within 3 months (Table 4). However, there is no direct evidence concerning the optimal time interval between surgery and PORT. Yamada S and colleagues found that there was no survival difference between patients with a waiting period of 30 to 39 days and patients with a waiting period of less than 30 days, and between patients with a waiting period of 40 to 49 days and patients with a waiting period of 50 or more days. However, the survival of patients with a waiting period of 30 to 39 days was significantly higher than that of patients with a waiting period of 40 to 49 days (P<0.01).61 Therefore, PORT should be started within 40 days after radical resection in this study. Another multicenter retrospective study also assessed the effect of PORT delay on survival for 316 patients.62 In this study, the waiting period after surgery varied from 12 days to over 60 days (median, 26 days). Patients with a particularly long waiting period (≥42 days) demonstrated a detrimental impact on OS (P=0.021) but not PFS (P=0.580). Therefore, it was recommended that PORT should be started within six weeks in this study. However, there is no RCT to confirm these results and it is also questionable whether the time interval can be prolonged when sequential chemotherapy is added before PORT.
Complications and Toxicities
Six of the nine RCTs reported complications or toxicity.5–7,15,17,19 In Fok’s study,5 lesions in the intrathoracic stomach (gastritis, gastric ulcer, bleeding gastric ulcer, penetrating gastric ulcer and fistula to trachea) were found in 34 patients (37%) in the S+RT group and four patients in the SA group (6%) (P<0.001). The major reason should be that the substitute organ was placed either orthotopically or in the thoracic cavity within the target volume. Furthermore, the fractional radiation dose was 3.5 Gy which may lead to increased mortality in the S+RT group. As a result, the median OS was actually worse in the S+RT group (8.7 months vs 15.2 months, P=0.02). Additionally, 6 patients in both the S+RT group and the SA group had anastomotic strictures. In another study, respiratory symptoms in 25 patients, postoperative death in 3 patients and leaks in 11 patients were observed in the S+RT group (42 patients) while respiratory symptoms in 15 patients, postoperative death in 3 patients and leaks in 7 patients were observed in the SA group (39 patients).6 In other RCTs,7,15,17,19 severe radiotherapy-related adverse events were not found in the S+RT group compared with the SA group. The commonly reported adverse events were anastomotic strictures, nausea, anorexia, weakness, leukopenia, anemia, and others.
The addition of chemotherapy to PORT may increase adverse events. Many studies have indicated that the incidence of grade 3 or more hematological toxicity,24,29,30 radiation esophagitis,24 and gastrointestinal reactions24,30 was higher in the S+CRT group than in the S+R group, but patients could tolerate chemoradiotherapy. In a meta-analysis, it was found that the most common prevalent severe complications (grade 3–4) were leukocytopenia (0–36.8%), hypohemoglobinemia (0–16.7%), thrombocytopenia (0–10.5%), nausea/vomiting (0–18.4%), and stomatitis (0–5.3%) in the S+CRT group. However, S+CRT did not increase the risk of pneumonitis, anastomotic stenosis or severe hematologic toxicities compared to the S+RT group.14
Radiation-based adverse events can be affected by the performance status, the methods of surgery, the methods of radiotherapy (technology, irradiation field, and TRD), the combined therapy, etc. In the past, it was always thought that PORT is difficult for patients to endure after radical surgery, and radiotherapy is often not fully delivered. However, this idea is not in accordance with the results of published studies. Additionally, with the rapid development of operation methods, precise radiotherapy using optimal target volume and dosage, and new chemotherapy drugs with low toxicity, it should be acceptable for postoperative radiotherapy or chemoradiotherapy. For example, postoperative conformal radiotherapy, which enables a superior delineation of target volume and planning, is associated with improved survival and tolerable toxicities for patients with pT3N0M0 EC.23
Conclusions
Previous RCTs mainly conducted in the late 20th century showed that PORT was not associated with improved survival (even a poor outcome in one RCT). However, these studies had many limitations, such as low sample size, two-dimensional radiotherapy technology, defects in the irradiation field, and inappropriate fractional and total irradiation dosages. Many studies included patients with paraaortic lymph node metastasis or cardiac adenocarcinoma. An increasing number of studies, mainly non-RCTs, have indicated that PORT with or without chemotherapy can improve survival for patients with a poor prognosis (i.e., positive nodal disease, stage III/IV disease) after upfront surgery. Additionally, almost all the non-RCTs and the published RCT compared CRT+S and S+CRT directly showed that there was no survival difference between these two groups. Both CRT+S and S+CRT have their own advantages and disadvantages, and therefore can be chosen for locally advanced EC in the clinical practice. There is a great dispute on the indication, target volume, TRD, time interval and complications of PORT with or without chemotherapy. Future studies will be needed to address the optimal subgroup populations for different treatment methods and to reevaluate the role of PORT for EC in the new era of conformal radiotherapy.
Ethics approval
This study was approved by the institutional review board of the First Affiliated Hospital of Anhui Medical University.
Consent for Publication
All the authors have consented to the publication of this manuscript.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
No funding was provided in the generation of this work.
Disclosure
The authors declare that they have no competing interests.
References
1. Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424.
2. Lagergren J, Smyth E, Cunningham D, et al. Oesophageal cancer. Lancet. 2017;390:2383–2396. doi:10.1016/S0140-6736(17)31462-9
3. Kunath U, Fischer P. [Radical nature and life expectancy in the surgical treatment of esophageal and cardial carcinoma]. Deutsche Medizinische Wochenschrift (1946). 1984;109:450–453. German. doi:10.1055/s-2008-1069212
4. Ténière P, Hay JM, Fingerhut A, et al. Postoperative radiation therapy does not increase survival after curative resection for squamous cell carcinoma of the middle and lower esophagus as shown by a multicenter controlled trial. French University Association for Surgical Research. Surg Gynecol Obstet. 1991;173:123–130.
5. Fok M, Sham JS, Choy D, et al. Postoperative radiotherapy for carcinoma of the esophagus: a prospective, randomized controlled study. Surgery. 1993;113:138–147.
6. Fok M, McShane J, Law SYK, et al. Prospective randomised study on radiotherapy and surgery in the treatment of oesophageal carcinoma. Asian J Surg. 1994;17:223.
7. Zieren HU, Müller JM, Jacobi CA, et al. Adjuvant postoperative radiation therapy after curative resection of squamous cell carcinoma of the thoracic esophagus: a prospective randomized study. World J Surg. 1995;19:444–449. doi:10.1007/BF00299187
8. Wong AT, Shao M, Rineer J, et al. The impact of adjuvant postoperative radiation therapy and chemotherapy on survival after esophagectomy for esophageal carcinoma. Ann Surg. 2017;265:1146–1151. doi:10.1097/SLA.0000000000001825
9. Yu J, Ouyang W, Li Y, et al. Value of radiotherapy in addition to esophagectomy for stage II and III thoracic esophageal squamous cell carcinoma: analysis of surveillance, epidemiology, and end results database. Cancer Med. 2019;8:21–27. doi:10.1002/cam4.1731
10. Cai W-J, Xin P-L. Pattern of relapse in surgical treated patients with thoracic esophageal squamous cell carcinoma and its possible impact on target delineation for postoperative radiotherapy. Radiother Oncol. 2010;96:104–107. doi:10.1016/j.radonc.2010.04.029
11. Boonstra JJ, Kok TC, Wijnhoven BP, et al. Chemotherapy followed by surgery versus surgery alone in patients with resectable oesophageal squamous cell carcinoma: long-term results of a randomized controlled trial. BMC Cancer. 2011;11:181. doi:10.1186/1471-2407-11-181
12. Oppedijk V, van der Gaast A, van Lanschot JJB, et al. Patterns of recurrence after surgery alone versus preoperative chemoradiotherapy and surgery in the CROSS trials. J Clin Oncol. 2014;32:385–391. doi:10.1200/JCO.2013.51.2186
13. Chen J, Pan J, Zheng X, et al. Number and location of positive nodes, postoperative radiotherapy, and survival after esophagectomy with three-field lymph node dissection for thoracic esophageal squamous cell carcinoma. Int J Radiat Oncol Biol Phys. 2012;82:475–482. doi:10.1016/j.ijrobp.2010.08.037
14. Kang J, Chang JY, Sun X, et al. Role of postoperative concurrent chemoradiotherapy for esophageal carcinoma: a meta-analysis of 2165 patients. J Cancer. 2018;9:584–593. doi:10.7150/jca.20940
15. Lv J, Cao XF, Zhu B, et al. Long-term efficacy of perioperative chemoradiotherapy on esophageal squamous cell carcinoma. World J Gastroenterol. 2010;16:1649–1654. doi:10.3748/wjg.v16.i13.1649
16. Schreiber D, Rineer J, Vongtama D, et al. Impact of postoperative radiation after esophagectomy for esophageal cancer. J Thorac Oncol. 2010;5:244–250. doi:10.1097/JTO.0b013e3181c5e34f
17. Xiao ZF, Yang ZY, Liang J, et al. Value of radiotherapy after radical surgery for esophageal carcinoma: a report of 495 patients. Ann Thorac Surg. 2003;75:331–336. doi:10.1016/S0003-4975(02)04401-6
18. Wang S, Wang Z, Yang Z, et al. Postoperative radiotherapy improves survival in stage pT2N0M0 esophageal squamous cell carcinoma with high risk of poor prognosis. Ann Surg Oncol. 2016;23:265–272. doi:10.1245/s10434-015-4622-0
19. Deng W, Yang J, Ni W, et al. Postoperative radiotherapy in pathological T2-3n0m0 thoracic esophageal squamous cell carcinoma: interim report of a prospective, phase iii, randomized controlled study. Oncologist. 2020;25:e701–e8. doi:10.1634/theoncologist.2019-0276
20. Chen J, Zhu J, Pan J, et al. Postoperative radiotherapy improved survival of poor prognostic squamous cell carcinoma esophagus. Ann Thorac Surg. 2010;90:435–442. doi:10.1016/j.athoracsur.2010.04.002
21. Gao HJ, Shang XB, Gong L, et al. Adjuvant radiotherapy for patients with pathologic node-negative esophageal carcinoma: a population based propensity matching analysis. Thorac Cancer. 2020;11:243–252. doi:10.1111/1759-7714.13235
22. Yu S, Zhang W, Ni W, et al. A propensity-score matching analysis comparing long-term survival of surgery alone and postoperative treatment for patients in node positive or stage III esophageal squamous cell carcinoma after R0 esophagectomy. Radiother Oncol. 2019;140:159–166. doi:10.1016/j.radonc.2019.06.020
23. Yang J, Zhang W, Xiao Z, et al. The impact of postoperative conformal radiotherapy after radical surgery on survival and recurrence in pathologic T3N0M0 esophageal carcinoma: a propensity score-matched analysis. J Thorac Oncol. 2017;12:1143–1151. doi:10.1016/j.jtho.2017.03.024
24. Chen J, Pan J, Liu J, et al. Postoperative radiation therapy with or without concurrent chemotherapy for node-positive thoracic esophageal squamous cell carcinoma. Int J Radiat Oncol Biol Phys. 2013;86:671–677.
25. Xu Y, Liu J, Du X, et al. Prognostic impact of postoperative radiation in patients undergoing radical esophagectomy for pathologic lymph node positive esophageal cancer. Radiat Oncol. 2013;8:116. doi:10.1186/1748-717X-8-116
26. Hwang JY, Chen HS, Hsu PK, et al. A propensity-matched analysis comparing survival after esophagectomy followed by adjuvant chemoradiation to surgery alone for esophageal squamous cell carcinoma. Ann Surg. 2016;264:100–106. doi:10.1097/SLA.0000000000001410
27. Luo H, Cui YY, Zhang JG, et al. Meta-analysis of survival benefit with postoperative chemoradiotherapy in patients of lymph node positive esophageal carcinoma. Clin Transl Oncol. 2018;20:889–898. doi:10.1007/s12094-017-1803-2
28. Zhao XH, Wang D, Wang F, et al. Comparison of the effect of postoperative radiotherapy with surgery alone for esophagus squamous cell carcinoma patients: a meta-analysis. Medicine (Baltimore). 2018;97:e13168. doi:10.1097/MD.0000000000013168
29. Liu HC, Hung SK, Huang CJ, et al. Esophagectomy for locally advanced esophageal cancer, followed by chemoradiotherapy and adjuvant chemotherapy. World J Gastroenterol. 2005;11:5367–5372. doi:10.3748/wjg.v11.i34.5367
30. Zou B, Tu Y, Liao D, et al. Radical esophagectomy for stage II and III thoracic esophageal squamous cell carcinoma followed by adjuvant radiotherapy with or without chemotherapy: which is more beneficial? Thorac Cancer. 2020;11:631–639. doi:10.1111/1759-7714.13307
31. Mukaida H, Hirai T, Yamashita Y, et al. Clinical evaluation of adjuvant chemoradiotherapy with CDDP, 5-FU, and VP-16 for advanced esophageal cancer. Jpn J Thorac Cardiovasc Surg. 1998;46:11–17. doi:10.1007/BF03217716
32. Xu Y, Chen Q, Sun X, et al. Phase III randomized study of preoperative versus postoperative chemoradiotherapy in resectable locally advanced esophageal squamous cell carcinoma. Int J Radiat Oncol Biol Phys. 2018;102:S30–S.
33. Malaisrie SC, Untch B, Aranha GV, et al. Neoadjuvant chemoradiotherapy for locally advanced esophageal cancer: experience at a single institution. Arch Surg. 2004;139:
34. Davis CS, Johns JR, Abood GJ, et al. Locally advanced esophageal cancer: actual 5-year survival comparing neoadjuvant and adjuvant chemoradiation. Ann Surg Oncol. 2011;18:S86–S7.
35. Hong JC, Murphy JD, Wang SJ, et al. Chemoradiotherapy before and after surgery for locally advanced esophageal cancer: a SEER-medicare analysis. Ann Surg Oncol. 2013;20:3999–4007. doi:10.1245/s10434-013-3072-9
36. Chen Y, Hao D, Wu X, et al. Neoadjuvant versus adjuvant chemoradiation for stage II-III esophageal squamous cell carcinoma: a single institution experience. Dis Esophagus. 2017;30:1–7.
37. Hsu PK, Chen HS, Liu CC, et al. Pre- versus postoperative chemoradiotherapy for locally advanced esophageal squamous cell carcinoma. J Thorac Cardiovasc Surg. 2017;154:732–40.e2. doi:10.1016/j.jtcvs.2017.03.038
38. Sadrizadeh A, Bagheri R, Soltani E, et al. The comparison of the advantages of neoadjuvant chemoradiotherapy versus postoperative chemoradiotherapy: outcomes in esophageal cancer patients. J Gastrointest Cancer. 2018;49:50–56. doi:10.1007/s12029-016-9899-0
39. Zou B, Pang J, Liu Y, et al. Postoperative chemoradiotherapy improves survival in patients with stage II-III esophageal squamous cell carcinoma: an analysis of clinical outcomes. Thorac Cancer. 2016;7:515–521.
40. Cooper JS, Guo MD, Herskovic A, et al. Chemoradiotherapy of locally advanced esophageal cancer: long-term follow-up of a prospective randomized trial (RTOG 85-01). Radiation Therapy Oncology Group. JAMA. 1999;281:1623–1627.
41. Li S, Liu H, Diao C, et al. Prognosis of surgery combined with different adjuvant therapies in esophageal cancer treatment: a network meta-analysis. Oncotarget. 2017;8:36339–36353.
42. Li F, Li T, Liu L, et al. Concurrent versus sequential chemoradiotherapy for esophageal cancer among Chinese population: a meta-analysis. Tumori. 2015;101:353–359.
43. Liu B, Bo Y, Wang K, et al. Concurrent neoadjuvant chemoradiotherapy could improve survival outcomes for patients with esophageal cancer: a meta-analysis based on random clinical trials. Oncotarget. 2017;8:20410–20417.
44. Francis S, Orton A, Stoddard G, et al. Sequencing of postoperative radiotherapy and chemotherapy for locally advanced or incompletely resected non-small-cell lung cancer. J Clin Oncol. 2018;36:333–341.
45. Wang Y, Zhu L, Xia W, et al. Anatomy of lymphatic drainage of the esophagus and lymph node metastasis of thoracic esophageal cancer. Cancer Manag Res. 2018;10:6295–6303.
46. Moon S, Kim H, Chie E, et al. Positive impact of radiation dose on disease free survival and locoregional control in postoperative radiotherapy for squamous cell carcinoma of esophagus. Dis Esophagus. 2009;22:298–304.
47. Xiao ZF, Yang ZY, Miao YJ, et al. Influence of number of metastatic lymph nodes on survival of curative resected thoracic esophageal cancer patients and value of radiotherapy: report of 549 cases. Int J Radiat Oncol Biol Phys. 2005;62:82–90.
48. Zhao Y, Chen L, Zhang S, et al. Predictive factors for acute radiation pneumonitis in postoperative intensity modulated radiation therapy and volumetric modulated arc therapy of esophageal cancer. Thorac Cancer. 2015;6:49–57.
49. Chen H, Wang Z, Yang Z, et al. Prospective study of adjuvant radiotherapy on preventing lymph node metastasis after Ivor-lewis esophagectomy in esophageal cancer. Ann Surg Oncol. 2013;20:2721–2726.
50. Zhang X, Yang X, Ni J, et al. Recommendation for the definition of postoperative radiotherapy target volume based on a pooled analysis of patterns of failure after radical surgery among patients with thoracic esophageal squamous cell carcinoma. Radiat Oncol. 2018;13:255.
51. Wang Y, Ye D, Kang M, et al. Risk factors and patterns of abdominal lymph node recurrence after radical surgery for locally advanced thoracic esophageal squamous cell cancer. Cancer Manag Res. 2020;12:3959–3969.
52. Yu J, Ouyang W, Li C, et al. Mapping patterns of metastatic lymph nodes for postoperative radiotherapy in thoracic esophageal squamous cell carcinoma: a recommendation for clinical target volume definition. BMC Cancer. 2019;19:927.
53. Wee CW, Kim IH, Park CK, et al. Postoperative radiotherapy for WHO grade II-III intracranial ependymoma in adults: an intergroup collaborative study (KROG 18-06/KNOG 18-01). Radiother Oncol. 2020;150:4–11.
54. Loganadane G, Truong PT, Taghian AG, et al. Comparison of nodal target volume definition in breast cancer radiation therapy according to RTOG versus ESTRO atlases: a practical review from the TransAtlantic Radiation Oncology Network (TRONE). Int J Radiat Oncol Biol Phys. 2020;107:437–448.
55. Shen WB, Gao HM, Zhu SC, et al. Analysis of the causes of failure after radical surgery in patients with (P)T(3)N(0)M(0) thoracic esophageal squamous cell carcinoma and consideration of postoperative radiotherapy. World J Surg Oncol. 2017;15:192.
56. Zeng Y, Yu W, Liu Q, et al. Difference in failure patterns of pT3-4N0-3M0 esophageal cancer treated by surgery vs surgery plus radiotherapy. World J Gastrointest Oncol. 2019;11:1172–1181.
57. Wang Y, Zhang L, Ye D, et al. A retrospective study of pattern of recurrence after radical surgery for thoracic esophageal carcinoma with or without postoperative radiotherapy. Oncol Lett. 2018;15:4033–4039.
58. Lin G, Liu H, Li J. Pattern of recurrence and prognostic factors in patients with pT1-3 N0 esophageal squamous cell carcinoma after surgery: analysis of a single center experience. J Cardiothorac Surg. 2019;14:58.
59. Liu Q, Cai XW, Wu B, et al. Patterns of failure after radical surgery among patients with thoracic esophageal squamous cell carcinoma: implications for the clinical target volume design of postoperative radiotherapy. PLoS One. 2014;9:e97225.
60. Fletcher GH. Clinical dose-response curves of human malignant epithelial tumours. Br J Radiol. 1973;46:1–12.
61. Yamada S, Takai Y, Nemoto K, et al. Prognostic impact of the period between surgery and postoperative irradiation in esophageal carcinoma. Tohoku J Exp Med. 1994;172:275–282.
62. Wang Y, Guan S, Bi Y, et al. Survival impact of delaying postoperative radiotherapy in patients with esophageal cancer. Transl Oncol. 2018;11:1358–1363.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.