")
Back to Journals » Local and Regional Anesthesia » Volume 13
Postoperative “Rescue” Use of Erector Spinae Plane Block After Lumbar Spine Fusion: A Report of 2 Cases
Authors Kianpour DN , Gundy JT, Nadler JW , Lindenmuth DM
Received 2 July 2020
Accepted for publication 31 July 2020
Published 13 August 2020 Volume 2020:13 Pages 95—98
DOI https://doi.org/10.2147/LRA.S268973
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Stefan Wirz
Daniel N Kianpour, Joseph T Gundy, Jacob W Nadler, Danielle M Lindenmuth
Department of Anesthesiology and Perioperative Medicine, University of Rochester Medical Center, Rochester, NY, USA
Correspondence: Daniel N Kianpour
Department of Anesthesiology and Perioperative Medicine, University of Rochester, 601 Elmwood Drive, Box 604, Rochester, NY 14642, USA
Tel +1 214-803-0475
Email [email protected]
Abstract: Pain after lumbar spine fusion surgery is often difficult to control in the immediate postoperative period. Historically, opioids have been the mainstay of treatment, but are associated with many unwanted side effects as well as increased hospital length of stay. The ultrasound-guided erector spinae plane block (ESP) is a relatively safe and simple regional option for the management of acute postoperative pain after spine surgery without the technical difficulty or complications noted with paravertebral injection (eg, pneumothorax, hematoma). To date, there have been reports of preoperative placement of ESP block prior to spine surgery with some success. We present a report of two cases that highlight the efficacy of the ESP block as an early postoperative “rescue” regional anesthetic technique in lumbar spine surgery. These cases demonstrate the potential effectiveness of a “rescue” use of the ESP block in patients having uncontrolled or poorly controlled pain in the early postoperative period with no evidence of significant side effects.
Keywords: erector spinae plane block, acute perioperative pain, lumbar spine surgery
Introduction
The erector spinae plane (ESP) block is a paraspinal myofascial plane block first described in 2016 by Forero as an alternative technique to treat thoracic neuropathic pain. It is theorized to function by blocking ventral, dorsal, and rami communicans of spinal nerves as they exit the lateral neuraxis along with possible diffusion into the paravertebral space.1,2 Before its description, paravertebral injection was the regional anesthetic technique of choice for truncal coverage if one wished to avoid thoracic epidural injection. The ESP block has advantages over paravertebral blocks owing to technically easier and reproducible placement as well as a lower risk of complications such as pneumothorax, nerve damage, or bleeding. Since its first description, the ESP block has been increasingly used to manage perioperative pain in diverse surgical settings (eg, thoracic, breast, abdominal).3–5
More recent investigations have examined the utility of this block for treating acute pain from lumbosacral spine surgery with promising results.6–8 In these studies, the ESP blocks were placed preoperatively or after the induction of general anesthesia, but before surgical incision. We present two cases of early postoperative “rescue” use of bilateral, low thoracic, single-shot ESP blocks to enhance analgesia for spinal fusion surgery. To our knowledge, there are no published case reports of “rescue” ESP blocks after spinal surgery in the early postoperative period.
Materials and Methods
Written informed consent was obtained prior to block placement. Single-shot blocks were performed bilaterally in the sitting position at the T10 level using a 22 gauge 3 1/8th inch echogenic needle (Braun Medical Inc., Bethlehem, PA, USA). Needle placement was confirmed using in-plane ultrasound guidance with a GE Logiq E series ultrasound (GE Healthcare, Arlington Heights, IL, USA) and 12L-RS high-frequency linear probe from a superior to inferior approach. See Figure 1. Patients were continuously monitored for side effects and toxicity with pulse oximetry, non-invasive blood pressure, and ECG in the post-anesthesia care unit for at least 60 minutes after block placement per institutional guidelines.
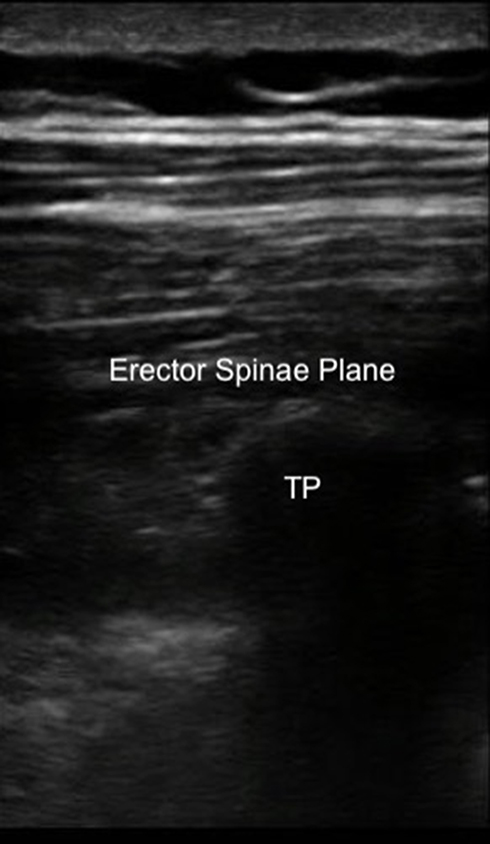 |
Figure 1 Sagittal ultrasound image with target erector spinae plane labeled. Note the acoustic shadow from the transverse process (TP) as the key landmark for this block. |
Case Series
Case 1
A 53-year-old 98-kg male with a history significant for obesity and obstructive sleep apnea underwent L4-5 laminectomy and fusion. Preoperatively he was on no chronic opioids and received acetaminophen 1000mg PO. During the 217-minute case, he received hydromorphone 2mg IV and fentanyl 100mcg IV. Despite 1.5mg of additional hydromorphone IV in PACU, pain NRS remained 8/10 in intensity. Next, bilateral T10 ESP blocks were performed (30cc 0.375% bupivacaine deposited per side). Pain NRS decreased to 2/10 following blocks, and he received no additional opioids in PACU. Pain NRS was documented as 2/10 or less over the next 24 hours on the floor, with an additional hydromorphone 1.4mg IV (via PCA), oxycodone 10mg PO, and non-opioid adjuncts administered over that time. By 24 hours post block, his documented pain scores increased to an average of 7.5/10 for the subsequent 24-hour period. Following the block, there was no documented hypotension and initial lower extremity motor score was 4/5 bilaterally which improved to 5/5 by 5 hours post block placement.
Case 2
A 57-year-old 121-kg male also with obesity and obstructive sleep apnea underwent revision laminectomy and L4-S1 posterior fusion. Preoperatively he was on no chronic opioids and received acetaminophen 1000mg PO and gabapentin 800mg PO. During the 362-minute case, he was administered fentanyl 100mcg IV, hydromorphone 3mg IV, and ketamine infused at 0.5mg/kg/hr. Initially, pain NRS in PACU was 7/10 intensity. Next, bilateral ESP blocks were performed (30cc 0.375% bupivacaine plus dexamethasone 4mg deposited per side). Following the blocks, he reported subjectively improved analgesia. Pain NRS decreased to 5/10 or less over the next 15 hours, with 3.8mg hydromorphone IV (via PCA) and non-opioid adjuncts administered over that time. Following that 15-hour period, his pain scores again increased to a documented average of 7 over the next 24 hours. There were no episodes of hypotension and his lower extremity motor score was documented as 5/5 bilaterally following the block placement and throughout the hospitalization.
Discussion
Chronic back pain has been identified as a leading cause of disability-adjusted life years lost worldwide.9 The national volume of spine surgeries has also been increasing. A retrospective examination of the Agency for Healthcare Research and Quality’s National Inpatient Sample demonstrates from 2004 to 2015 the number of elective lumbar fusion operations performed in the United States increased from 122679 to 199140. Correspondingly, the hospital costs associated with lumbar spine fusion increased from $3.7 billion dollars in 2004 to $10.2 billion dollars in 2015 or an increase of 177.2%.10 Increasing use of parenteral opioids prolongs hospital length of stay as well as unwanted side effects such as nausea, vomiting, respiratory depression, and pruritus which in turn increases overall health-care costs.11 This has focused attention on alternatives to parenteral opioid administration for control of postoperative pain after spine fusion surgery. Historically, the focus was on oral multimodal analgesic regimens which included medications such as acetaminophen, gabapentinoids, and anticonvulsants.12 There has also been investigation into postoperative epidural analgesia’s efficacy in spine surgery with limited surgeon acceptance and complications, notably infection, hematoma, unpredictable spread, and postoperative motor block.13,14 With increasing knowledge, paraspinal truncal blocks offer a new regional alternative to assess in postoperative analgesia after spine surgery.
Until recently, there has been no easily performed and reliable regional anesthetic option for acute pain related to spine surgery that avoided the direct neuraxis.6 The ultrasound-guided ESP block could offer a safe and technically reproducible option for management of perioperative thoracolumbar spine pain. Our case series is unique in demonstrating the potential of a “rescue” use of the ESP block for analgesia after spine fusion surgery in the immediate postoperative period. Since these blocks were performed postoperatively, we chose the T10 vertebral level for injection as this location is distant from the site of surgical tissue disruption and has been used effectively in prior reports of analgesia for lumbar spine surgery with ESP block.6,8 Despite injecting post laminectomy, we did not see evidence of significant epidural local anesthetic spread such as dense motor block or hemodynamic changes. Relatively high volume bilateral injections (30cc of 0.375% bupivacaine per side) were used primarily to aid in caudal spread along the myofascial plane from the thoracic to lumbar region. It is important to note, there have been case reports of local anesthetic toxicity (LAST) after high volume injection in the erector spinae plane.15,16 Special attention was made to ensure our total bupivacaine dose was less than the recommended maximum dose of 3mg/kg and no signs of LAST were noted during the monitoring period such as tinnitus, vertigo, disorientation, or seizures.17 Most reports with respect to analgesia after spine surgery use injectate volumes of 20–30cc per side with concentrations of bupivacaine or ropivacaine ranging from 0.2% to 0.5%. If indicated, the variables of local anesthetic concentration and volume can be adjusted based on patient characteristics (eg, low lean body weight, extremes of age) to reduce the risk of LAST.
One of the difficulties in studying postoperative pain is defining a clinically significant reduction in pain. Rowbotham discusses this dilemma and concludes that a 2 point decrease on 0–10 scale should be considered “clinically meaningful”.18 In Case 1, our patient was in severe pain in the PACU with a NRS of 8/10 and appeared in significant discomfort. Following the ESP block, his pain NRS quickly decreased to 2/10 and remained below that level for the clinical duration of the block (15 hours). The patient in Case 2 was also having uncontrolled pain the PACU which was not improving with standard parenteral opioid therapy. His pain NRS score had a clinically meaningful decrease from 7/10 to 5/10 post block with a significant subjective improvement.
Conclusion
These cases further highlight the potential for the ESP block to be used as a “rescue” analgesic technique to manage otherwise uncontrolled acute postoperative pain from spinal fusion surgery. In our cases, we noted clinically meaningful improvements in pain without evidence of major side effects. Some limitations of our observations include small sample size, non-standardized perioperative analgesic regimen, as well as inconsistent documentation of pain numerical rating scores. Further prospective studies are needed to better assess the value of this regional technique in the setting of spine surgery.
Consent for Publication
Written informed consent was obtained from the patients for publication of this case series including the associated image. Institutional review is not required for case reports or case series publication per the University of Rochester Medical Center’s Research Subjects Review Board guidelines.
Disclosure
The authors declare there are no conflicts of interest or support that may cause bias in this work. A prior condensed and non-peer-reviewed version of this case series was submitted and accepted as an abstract at ASRA’s virtual 2020 Regional Anesthesia and Pain Medicine meeting.
References
1. Forero M, Adhikary SD, Lopez H, et al. The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41(5):621–627. doi:10.1097/AAP.0000000000000451
2. Hamilton DL, Manickam B. The erector spinae plane block. Reg Anesth Pain Med. 2017;42(2):276. doi:10.1097/AAP.0000000000000565
3. Chin KJ, Malhas L, Perlas A. The erector spinae plane block provides visceral abdominal analgesia in bariatric surgery: a report of 3 cases. Reg Anesth Pain Med. 2017;42:372–376. doi:10.1097/AAP.0000000000000581
4. Chin KJ, Adhikary S, Sarvani N, et al. The analgesic efficacy of preoperative bilateral erector spinae plane (ESP) blocks in patients having ventral hernia repair. Anaesthesia. 2017;72:452–460. doi:10.1111/anae.13814
5. Adhikary SD, Pruett A, Forero M, Thiruvenkatarajan V. Erector spinae plane block as an alternative to epidural analgesia for post-operative analgesia following video-assisted thoracoscopic surgery: a case study and a literature review on the spread of local anaesthetic in the erector spinae plane. Indian J Anaesth. 2018;62(1):75–78.
6. Singh S, Choudhary NK, Lalin D, et al. Bilateral ultrasound-guided erector spinae plane block for postoperative analgesia in lumbar spine surgery: a randomized control trial. J Neurosurg Anesthesiol. 2019.
7. Ueshima H, Inagaki M, Toyone T, Otake H. Efficacy of the erector spinae plane block for lumbar spinal surgery: a retrospective study. Asian Spine J. 2019;13(2):254–257. doi:10.31616/asj.2018.0114
8. Melvin JP, Schrot RJ, Chu GM, Chin KJ. Low thoracic erector spinae plane block for perioperative analgesia in lumbosacral spine surgery: a case series. Can J Anaesth. 2018;65(9):1057–1065. doi:10.1007/s12630-018-1145-8
9. Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(9995):743–800.
10. Martin BI, Mirza SK, Spina N, Spiker WR, Lawrence B, Brodke DS. Trends in lumbar fusion procedure rates and associated hospital costs for degenerative spinal diseases in the United States, 2004 to 2015. Spine (Phila Pa 1976). 2019;44(5):369–376. doi:10.1097/BRS.0000000000002822
11. Van Boerum DH, Smith JT, Curtin MJ. A comparison of the effects of patient-controlled analgesia with intravenous opioids versus Epidural analgesia on recovery after surgery for idiopathic scoliosis. Spine (Phila Pa 1976). 2000;25(18):2355–2357. doi:10.1097/00007632-200009150-00014
12. Zarei M, Najafi A, Mansouri P, et al. Management of postoperative pain after Lumbar surgery-pregabalin for one day and 14 days-a randomized, triple-blinded, placebo-controlled study. Clin Neurol Neurosurg. 2016;151:37–42. doi:10.1016/j.clineuro.2016.10.007
13. Gottschalk A, Freitag M, Tank S, et al. Quality of postoperative pain using an intraoperatively placed epidural catheter after major lumbar spinal surgery. Anesthesiology. 2004;101(1):175–180. doi:10.1097/00000542-200407000-00027
14. Guay J, Suresh S, Kopp S, Johnson RL. Postoperative epidural analgesia versus systemic analgesia for thoraco-lumbar spine surgery in children. Cochrane Database Syst Rev. 2019;1(1):CD012819. doi:10.1002/14651858.CD005619.pub3
15. Tulgar S, Selvi O, Senturk O, Serifsoy TE, Thomas DT. Ultrasound-guided erector spinae plane block: indications, complications, and effects on acute and chronic pain based on a single-center experience. Cureus. 2019;11(1):e3815.
16. Karaca O, Pinar HU. Is high dose lumbar erector spinae plane block safe? J Clin Anesth. 2020;62:109721. doi:10.1016/j.jclinane.2020.109721
17. Rosenberg PH, Veering BT, Urmey WF. Maximum recommended doses of local anesthetics: a multifactorial concept. Reg Anesth Pain Med. 2004;29(6):564–575. doi:10.1016/j.rapm.2004.08.003
18. Rowbotham MC. What is a “clinically meaningful” reduction in pain? Pain. 2001;94(2):131–132. doi:10.1016/S0304-3959(01)00371-2
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.