")
Back to Journals » Journal of Pain Research » Volume 12
Postoperative analgesic effects of various quadratus lumborum block approaches following cesarean section: a randomized controlled trial
Authors Kang W, Lu D, Yang X, Zhou Z, Chen X, Chen K, Zhou X, Feng X
Received 27 January 2019
Accepted for publication 24 June 2019
Published 25 July 2019 Volume 2019:12 Pages 2305—2312
DOI https://doi.org/10.2147/JPR.S202772
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Erica Wegrzyn
Wenbin Kang,1 Dihan Lu,1 Xiaoyu Yang,1 Zhibin Zhou,1 Xi Chen,2 Keyu Chen,1 Xue Zhou,1 Xia Feng1
1Department of Anesthesiology, First Affiliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong Province, People’s Republic of China; 2Department of Anesthesiology, Tianjin Medical University Cancer Institute and Hospital, Tianjin, People’s Republic of China
Purpose: Quadratus lumborum block (QLB) is shown to be effective on analgesia following cesarean section. This study aimed to compare the effects of three practical QLB approaches and classic epidural analgesia (EA) for cesarean section under spinal anesthesia.
Patients and methods: Parturients undergoing elective cesarean section were randomized as group 1 (QLB type 2), group 2 (QLB type 3), group 3 (QLB type 2+3) and group 4 (EA). The block was performed at the end of the operation, and the epidural group was given a single epidural bolus. All subjects were provided with intravenous patient-controlled analgesia under identical settings. In addition, the postoperative pain severity was assessed by the VAS, which together with the morphine consumption at specific time intervals, was recorded within 48 hrs after surgery. Data were collected from December 2017 to June 2018.
Results: A total of 94 parturients had completed the study. At almost all postoperative time points, the VAS scores at rest and with movement in QLB type 2+3 group were lower than those in QLB type 2 or 3 group. The mean additional morphine consumption in QLB type 2+3 group (2.7 mg) was lower than that in QLB type 2 or 3 group (6.1 mg and 5.7 mg, respectively) within 48 h after surgery (P<0.001). Besides, the total morphine consumption in EA group (1.3 mg) was lower than that in any other QLB group (P<0.001).
Conclusions: The analgesic effect of QLB is highly dependent on the injection position of local anesthetic. Besides, the ultrasound-guided QLB type 2+3 can provide superior analgesic effect following cesarean section to that of QLB type 2 or 3 block. However, it remains to be further validated about whether the combination of QLB type 2 and 3 is the best approach.
Keywords: nerve block, cesarean section, postoperative pain
Introduction
It is vital to apply adequate postoperative analgesia following cesarean section (C-section), since it will affect the distinct surgical recovery requirements of the parturients.1 Epidural administration of opioids remains the most effective approach for postoperative analgesia; nonetheless, it is associated with troublesome side effects.2,3 Moreover, some parturients may fail to receive epidural anesthesia as a result of contraindications or unsuccessful epidural catheter placement. Therefore, alternative analgesia, such as peripheral nerve block, is required to relieve the acute pain from the incisions.
The ultrasound-guided quadratus lumborum block (QLB), first introduced by Blanco R. in 2007, has been recognized as an effective abdominal wall block approach, in which local anesthetic injected from the posterior abdomen will spread around the quadratus lumborum muscle and block the intermuscular nerves.4 In addition, such block is also closely related to multiple sympathetic fibers and is connected to the thoracic paravertebral space.5 Typically, QLB is found to be effective, which can provide satisfactory analgesic effect.6–10
QLB type 1 has been once considered as a kind of transversus abdominis plane (TAP) block at the triangle of Petit, which can be ascribed to its similar injection points and liquid spread paths.11,12 Moreover, QLB type 1 is reported to be an anterolateral approach, which can lead to less dispersion of local anesthetic, as observed in magnetic resonance study.13 Notably, there are other two types of QLB according to previous studies.14 Among them, the standard way to conduct QLB type 2 is to set the injection point at the site posterior to the quadratus lumborum muscle from the posterior abdominal wall.13 QLB type 3, also referred to as transmuscular quadratus lumborum block (TM-QLB), has employed the “Shamrock Sign” to identify muscles and aimed at the anterior border of quadratus lumborum and posterior to psoas major, so that the anesthetic can spread to the thoracic paravertebral space (Figure 1).14 Additionally, it is suggested in a randomized controlled study that QLB type 2 can remarkably relieve pain following C-section.13 However, the effects of other major QLB approaches or their combination on cesarean section have never been compared.
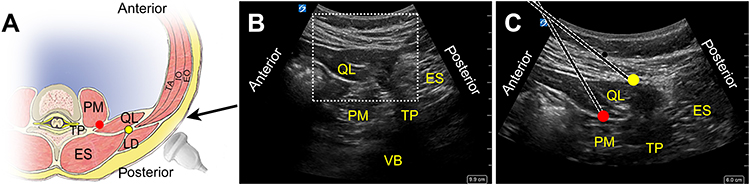 |
Figure 1 Approaches of QL block conducted with subjects in supine position. (A) Schematic diagram showing the direction of needle (black arrow) and the site of injection in QL2 (yellow dot) and QL3 (red dot). (B) Ultrasonogram detecting deep tissues to identify the Shamrock sign. The image with low depth in dotted box was acquired (C) for procedure. (C) Needle approaches and the injection points of QL2 (yellow dot) and QL3 (red dot). Abbreviations: TP, transverse process; PM, psoas major; QL, quadratus lumborum muscle; ES, erector spinae; LD, latissimus dorsi; EO, external oblique muscle; IO, internal oblique muscle; TA, transversus abdominis muscle; VB, vertebral body. |
This study aimed to observe the effects of three practical QLB approaches, including type 2 and 3, as well as their combination. Typically, their effects were compared with the classic epidural analgesia (EA) on C-section under the single-blind randomized controlled trial. We hypothesized that combination of QLB type 2 and 3 was superior to type 2 or 3 alone in relieving postoperative pain following C-section.
Materials and methods
This is a prospective, single-blind, randomized controlled trial. The Ethics Committee for Clinical Research and Animal Trials of the First Affiliated Hospital of Sun Yat-sen University approved the research protocol (No. [2016]123). The trial was conducted in accordance with the Declaration of Helsinki and was registered at ClinicalTrials.gov (identifier NCT03333902) on November 2, 2017. All efforts were made to avoid iatrogenic injury to participants. In each case, written informed consent was obtained, and the parturients who were scheduled for elective cesarean delivery via a Pfannenstiel incision under spinal anesthesia were enrolled in the study. Inclusion criteria were American Society of Anesthesiologists (ASA) physical status I or II, age from 24 to 40 years old, weight from 50 to 70 kg and a normal singleton pregnancy with a gestation of at least 37 weeks. We excluded patients who had congenital coagulopathy, anatomic abnormalities and localized infection and who were incapable of comprehending or using the verbal rating pain scoring system or patient-controlled analgesia (PCA) pump.
Parturients were labeled by her enrolled sequence. W. Kang generated the random allocation sequence using a software (Microsoft Excel, Version 2013, USA, http://www.microsoft.com) and allocated them into four groups as follows (equal sample size in each group): the QLB type 2 (QL2 group), QLB type 3 (QL3 group), QLB type 2+3 (QL2+3 group) and EA group. Parturients were blinded to the treatments or block techniques until study completion.
Treatments
A 16-gauge intravenous cannula pathway was established in the non-dominant hand or arm in the operation unit. All parturients with standard monitoring including electrocardiogram, pulse arterial oxygen saturation, respiratory rate and non invasive blood pressure (NIBP) were performed combined with spinal and epidural anesthesia before C-section in the left lateral position and peripheral nerve block at the end of surgery by an experienced doctor. The epidural needle was inserted into the lumbar epidural space at the level of L2-3 intervertebral space. After finding the epidural space using loss of resistance to saline technique, the tip of a spinal needle was passed through the epidural needle. To achieve a sensory block height to the level of the sixth thoracic dermatome, every parturient received intrathecal anesthesia of 0.75% bupivacaine (Zhaohui Co., Shanghai, China) 1.3–1.7 mL. Then, we withdrew the needle and then inserted an epidural catheter through the epidural needle in case the failure of intrathecal anesthesia. All surgical treatments were performed successfully in the usual manner.
Immediately after surgery, all subjects were transferred to the post-anesthesia care unit (PACU) and administered pre determined analgesia, which was concealed by the doctor conducting the randomization until the end of the operation. All parturients were in the supine position, tilting 45 degrees to the opposed side in order to place the low-frequency convex probe properly and see the sonography clearly. Bilateral QLB was performed by either of two investigators (X. Feng and X. Zhou) using the atraumatic needle (22-G, 120-mm needle for peripheral nerve blocks, B. Braun Melsungen AG, Germany) advanced in-plane under the guidance of an ultrasound machine (X-Porte, Sonosite Ltd, USA). The ultrasonogram of the abdominal wall could be displayed clearly through probe moving or tilting. Pillows could help to relieve the tension along the abdominal wall of parturients. The whole procedure was performed strictly according to clinical protocol.
In this study, QL2 or QL3 were conducted through an anterolateral approach with the supine position as mentioned earlier (Sato et al, 2017).15 The ultrasound transducer was placed transversely on both flanks at the horizontal level of L2-3 and adjusted until the “Shamrock sign” formed of QL muscle, psoas major and erector spinae was visualized, with imaging depth set between 0 and 9.9 cm (Figure 1B). Needles were penetrated in an anterolateral to posteromedial direction. Local anesthetic was injected posterior to QL muscle in QL2, while in QL3, it was located between QL muscle and psoas major. QL2+3 block could be conducted in the same plane with only one puncture on each side (Figure 1C). QL2 and QL3 groups received 0.2% ropivacaine (AstraZeneca, Södertälje, Sweden) at 30 mL at the sites mentioned above in each side for a total of 60 mL. For QL2+3 group, they were given the 0.2% ropivacaine 15 mL at each point of injection with the needle inserting only once in each side. The solution was injected after negative aspiration to exclude vascular puncture. As for the EA group, we used a single bolus of 6-mL saline solution containing 9 mg ropivacaine (0.15%) and 2 mg morphine via the epidural catheter as postoperative analgesia, and meanwhile, they received a procedure like QL2, but only saline was injected as placebo.
Epidural catheters were detached from all parturients after the procedure mentioned above. Parturients were prescribed a standard postoperative analgesic regime of regular oral paracetamol 1.0 g 6 hourly. A PCA pump of 0.5 mg/mL morphine (1 mg bolus with a 5-min lockout) was connected to the intravenous line and was removed 48 hrs postoperatively, including the EA group. They were educated to press the button on the pump when feeling pain before leaving PACU.
The primary outcome measures of the study were the values assessed with visual analogue scale (VAS, 0–100 mm) pain scores at rest and with movement at 0, 4, 6, 12, 24 and 48 hrs postoperatively and the total morphine consumption in predetermined time intervals after surgery. The secondary outcomes included complications such as nausea and vomiting, pruritus, urinary retention, lower-limb weakness, infection and hematoma. The following vital signs were recorded including heart rate, respiratory rate, oxygen saturation and NIBP.
Sample size
The sample size was calculated by the Power Analysis and Sample Size software (PASS version 11.0.7; NCSS, Kaysville, Utah, USA), based on VAS at 5 postoperative time points in our pilot test with 5 subjects admitted in each group. Tests for two means in a repeated design were adopted. A maximal sample size of 16 subjects in each of 4 groups calculated would be appropriate to have an α =0.0083 corrected by Bonferroni method and an 80% power to detect a mean difference of 10 (mm) in VAS, with an SD of 18 (mm) from the pilot test. We recruited an additional six to seven patients per group in case of 30% dropouts.
Statistical analysis
A standard statistical program IBM SPSS Statistics (Version 23, IBM Corporation, Armonk, NY, USA) was used. ANOVA for repeated measures was used to analyze VAS data, on which Mauchly’s test of sphericity was performed first. Shapiro–Wilk test was used to determine the normality of data. Nonparametric tests like Kruskal–Wallis test were used to analyze the non-normally distributed data. Multiple comparisons would be performed if the ANOVA test was significant and Bonferroni method was used in the correction. Categorical data were analyzed using χ2 or Fisher’s exact test as appropriate. Normally distributed data are presented as mean SD, non-normally distributed data are presented as median IQR, and categorical data are presented as frequencies. The α level for all analyses was set as P<0.05.
Results
From December 2017 to June 2018, a total of 102 parturients were enrolled in the study, of which 94 parturients were included in the analysis (Figure 2). All groups were comparable in age, weight, height and gestation (Table 1). The occurrence of some complications including postoperative nausea and vomiting (PONV), pruritus, lower-limb weakness and the total number of subjects with complications were recorded and compared using Fisher’s exact test (Table 2). We noticed that the total number of subjects in EA group with complications was higher than the rest of groups; however, no statistical differences were found among groups (P>0.05). Catheter displacement or cutting off, local infection or hematoma, organ injuries, low blood pressure and headache were not observed during the trial.
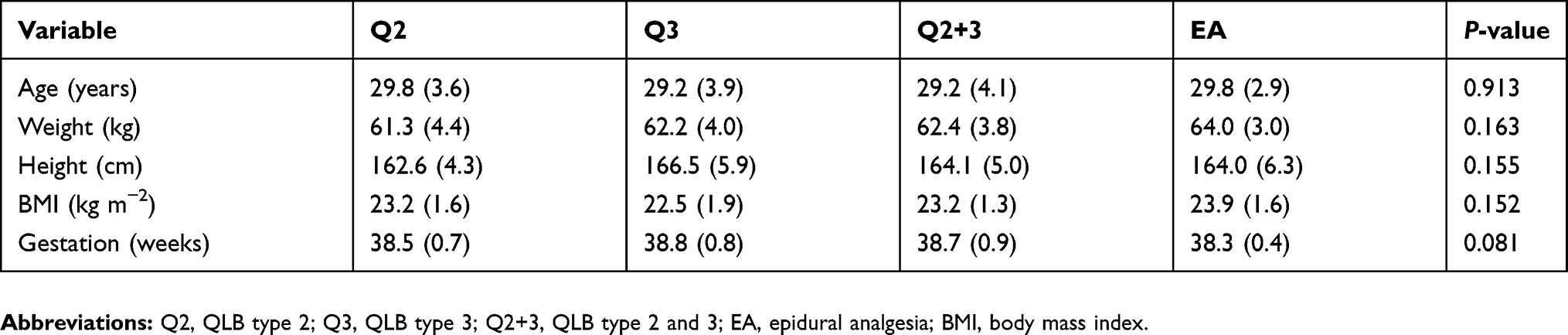 |
Table 1 Baseline characteristics of parturients undergoing cesarean section |
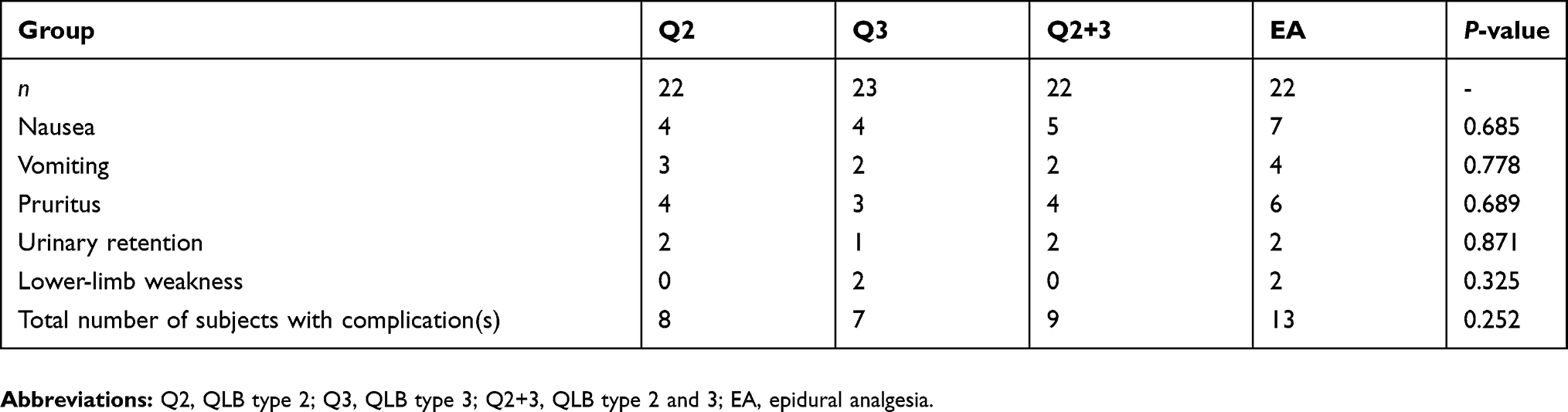 |
Table 2 Complications in 48 hrs after cesarean section |
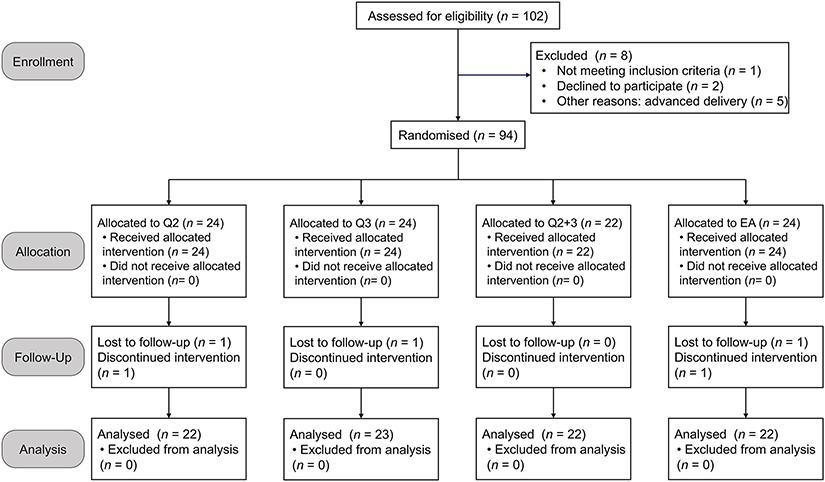 |
Figure 2 Study flow diagram. |
Pain scores
The results of the VAS scores at rest showed significant differences in treatment effect among 4 groups (P<0.001). Multiple comparison tests indicated that the level of VAS scores at rest of each group was different from one another. The order of mean values of each group was as follows (P<0.001, Figure 3A):
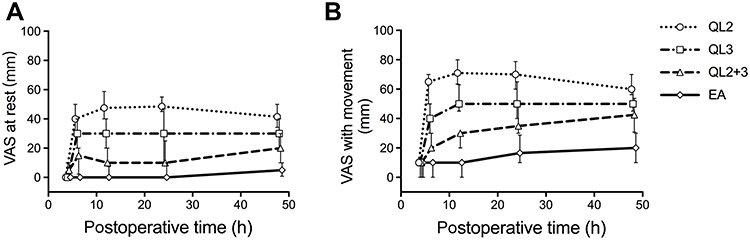 |
Figure 3 Postoperative VAS scores of 4 groups at 5 time points (median and IQR). (A) VAS at rest and (B) with movement at different time points postoperatively. Abbreviations: QL2, QLB type 2; QL3, QLB type 3; QL2+3, QLB type 2 and 3; EA, epidural analgesia. |
Q2 (36.1 mm) > Q3 (24.6 mm) > Q2+3 (13.5 mm) > EA (3.0 mm)
As for VAS scores with movement, the results of treatment effect were similar to VAS scores at rest (P<0.001). The VAS with movement was significantly different when performing all the pairwise comparisons. The order of mean value of VAS scores with movement of each group was as follows (P<0.001, Figure 3B):
Q2 (55.5 mm) > Q3 (42.1 mm) > Q2+3 (27.8 mm) > EA (11.7 mm)
Morphine consumption
The total morphine consumption during postoperative 48 hrs was statistically different among all groups. The mean total morphine consumption of QL2+3 group (2.7 mg) was lower than QL2 (6.1 mg) and QL3 group (5.7 mg) (P<0.001). Besides, the total morphine consumption of each QLB group was statistically higher than the EA group (1.3 mg) (P<0.001, Figure 4A). Differences of morphine consumption among the 4 groups in each time interval are shown in Figure 4B.
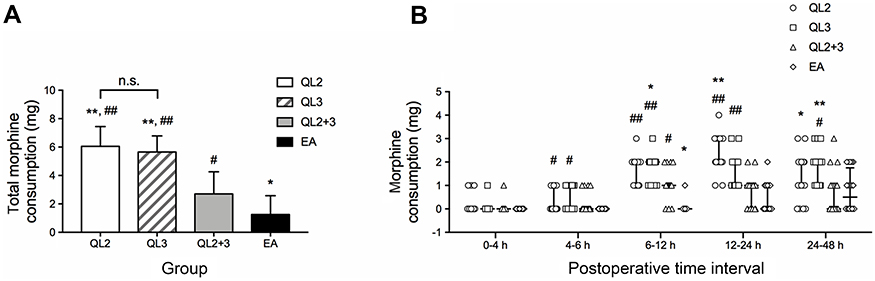 |
Figure 4 Extra morphine consumption during postoperative 48 hrs. (A) Total morphine consumption during postoperative 48 hrs are presented by mean (SD). Mean difference was significant between each group except the one between QL2 and QL3. (B) Data of morphine consumption in different time intervals are showed by scatter dot plot with the vertical bars indicating IQR. *P<0.05 and **P<0.001 compared with QL2+3 group. #P<0.05 and ##P<0.001 compared with EA group. All pairwise comparisons were corrected by Bonferroni method.Abbreviations: QL2, QLB type 2; QL3, QLB type 3; QL2+3, QLB type 2 and 3; EA, epidural analgesia; n.s., not significant. |
Discussion
To date, the goal of optimal post-cesarean analgesia can still hardly be attained. A systematic review has been conducted to summarize the recent advances in modalities, such as opioids, TAP block, wound infiltration/infusion, ketamine, gabapentin and ilioinguinal-iliohypogastric nerve block (II-IH NB).16 Typically, intrathecal or epidural opioids play a vital part in postoperative analgesia, but their side effects have restricted their application, and the optimal dose remains a source of controversy. TAP block has been employed and extensively investigated. According to a meta-analysis, TAP block can provide effective analgesia after C-section. However, a randomized controlled trial by Blanco et al illustrated that QLB type 2 was superior to TAP block.1,17 Moreover, no consensus results can be obtained from studies on wound infiltration with local anesthetics, systemic ketamine or gabapentin and II-IH NB. Therefore, further trials are needed to assess their efficacy. QLB is now performed as one of the perioperative pain management procedures for all generations (including pediatrics and adults) undergoing abdominal surgery.18 However, the best approach of the block is still under debate due to the unclear mechanisms. Consequently, our primary objective was to compare the effects of three practical QLB approaches and classic EA in patients undergoing C-section.
Our result suggested that, compared with all QLB approaches, epidural morphine could provide the most reliable analgesic effect after C-section. In this study, epidural morphine remained the most effective approach at present due to its lowest VAS scores both at rest and with movement. Besides, the complications mainly induced by spinal anesthesia and morphine use included PONV, pruritus and urinary retention; meanwhile, the total numbers of subjects with these complications were comparable (Table 2). At the same time, catheter displacement or cutting off, local infection or hematoma, low blood pressure and headache were not observed. Differences were observed in pain scores and morphine consumption, and we considered that with the increase in sample size, the incidence of side effects associated with opioid use, which was related to its consumption, might show significant differences. Nevertheless, further studies should be designed to primarily observe the side effects of various QLB approaches.
Our results on the analgesic efficacy of epidural morphine were consistent with those from a systematic review indicating that a single bolus of epidural morphine after cesarean section was effective in reducing pain, but it was associated with adverse effects.19 Typically, the adverse effects were closely related to the use of epidural morphine. It is reported that 1.5 mg of epidural morphine can provide comparable post-cesarean analgesia in the meantime of inducing fewer adverse effects relative to those of 3 mg of epidural morphine.20
Additionally, a case series report supports that QLB may be a promising anesthetic adjuvant treatment for post-cesarean analgesia, but the specific QLB steps are not mentioned.21 By contrast, our study had clearly shown the steps to perform different types of QLB. To be specific, QLB type 1 is an anterolateral approach, which can result in less dispersion of local anesthetic, as observed in magnetic resonance study;13 therefore, QLB type 1 was abandoned in this trial. Our results indicated that ultrasound-guided QL3 or QL2+3 blocks could have superior analgesic effects after C-section relative to that of QL2 block. These results were a little bit different from those of previous studies performed by Blanco et al demonstrating that QL2 block was a superior analgesic technique, which can reduce morphine consumption as well as the demands for postoperative pain relief following cesarean section.13 The following reasons were presented for the differences in outcomes between our study and those previously described.
The analgesic efficacy of QLB is highly dependent on the injection position of the needle tip. A recent cadaver study was performed to compare three types of QLB;22 among them, one of three QL1 blocks and one of three QL2 blocks were misplaced, which could not provide postoperative analgesic effect if administered to patients, even though they were carried out by an expert anesthetist with rich experience in cadaver regional anesthesia.23 In this study, QLB was performed by an anterolateral approach under the present circumstances, because it was quite inconvenient for parturients to lie in the lateral position after surgery. However, we found that this approach was relatively difficult to be performed in parturients, which was considered as the special postural problem among parturients that might lead to a higher needle misplacement rate. Therefore, we assumed that although QL2 might be effective for pain relief, it was an unreliable approach following C-section due to the failure of injection accuracy and the anatomic characteristics. Moreover, it was difficult to guarantee the spread of QL2 block anesthetic even in the presence of accurate injection, since the anatomical configuration of connective tissue and relative resistance to the flow of injection remained unknown in each cadaver, or in the actual patient.22 Our results suggested that the practitioners should be cautious when performing such type of block and thereafter remained vigilant.
Compared with QL2 block, QL3 block is much more effective since it is not dependent on the vagaries of connective tissue anatomy. QL3 block can provide a distinct and clear end point, as well as the spread of anesthetic both lateral and posterior to the psoas muscle when the needle tip penetrates through the quadratus lumborum.22 Besides, the spread of anesthetic in QL3 block is mainly posterior to the arcuate ligaments and into the thoracic paravertebral space.24
Furthermore, our study indicated that QL2+3 block could achieve a better analgesic effect than QL3 block. Thus, it was assumed that QL2+3 block, if applied more appropriately, could be utilized to achieve better pain control. There are some points to be taken into consideration when performing the QL3 block. It is important to use ultrasound for QL3 block, the deeper nerve block compared with QL2 block. In this study, sites were identified carefully in case of blood hematoma and organ injuries. Additionally, the QL3 block approach may also block the lumbar nerve roots.22 Theoretically, a spread to the lumbar plexus can cause weakness of the psoas, iliacus and quadriceps muscles, as described in a case report.25 However, the adverse effects of lumbar plexus block were not commonly observed in our patients.
Three limitations should be noted in our study. First, the dermatomal levels were not assessed immediately after QLB because of the persistent effects of spinal anesthesia. To evaluate the analgesic effects of QLB, we focused on morphine consumption and demands. Second, the VAS scores assessed by the parturients were subjective; by contrast, morphine consumption was much more objective. Last but not least, we used a maximum dose of 60 mg ropivacaine at each side in our study, which was generally used in our daily anesthesia for abdominal operation to prevent systemic analgesic effects and the risks of systemic toxicity.26,27 Nevertheless, the questions regarding the ideal dosing, volumes, timing of block and pertinence of catheters and adjuvants (such as adrenaline or dexmedetomidine) remain to be answered.
Conclusion
In conclusion, spinal morphine reduces early pain after cesarean section, and among all the QL blocks, the combination of QL type 2 and 3 blocks can be applied more appropriately to achieve better pain control and have therapeutic value for patients who failed to receive spinal morphine. However, whether the combination of QL type 2 and 3 is the best approach needs further validation and more studies are warranted.
Acknowledgments
The authors would like to thank Professor Lihua Zhou, from the Department of Anatomy, Zhong Shan Medical College, for her detailed instruction of the abdominal anatomy. This work was supported by the National Natural Science Foundation of China (grant numbers 81571032; 81701047).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Blanco R, Ansari T, Riad W, Shetty N. Quadratus lumborum block versus transversus abdominis plane block for postoperative pain after cesarean delivery: a randomized controlled trial. Reg Anaesth Pain Med. 2016;41(6):757–762. doi:10.1097/AAP.0000000000000495
2. Dahl JB, Jeppesen IS, Jorgensen H, Wetterslev J, Moiniche S. Intraoperative and postoperative analgesic efficacy and adverse effects of intrathecal opioids in patients undergoing cesarean section with spinal anesthesia: a qualitative and quantitative systematic review of randomized controlled trials. Anesthesiology. 1999;91(6):1919–1927. doi:10.1097/00000542-199912000-00045
3. Rawal N. Current issues in postoperative pain management. Eur J Anaesthesiol. 2016;33(3):160–171. doi:10.1097/EJA.0000000000000366
4. Blanco R. Tap block under ultrasound guidance: the description of a “nonpopstechnique”. Reg Anaesth Pain Med. 2007;32(suppl 1):130.
5. Willard FH, Vleeming A, Schuenke MD, Danneels L, Schleip R. The thoracolumbar fascia: anatomy, function and clinical considerations. J Anat. 2012;221(6):507–536. doi:10.1111/j.1469-7580.2012.01511.x
6. Chakraborty A, Goswami J, Patro V. Ultrasound-guided continuous quadratus lumborum block for postoperative analgesia in a pediatric patient. A A Case Rep. 2015;4(3):34–36. doi:10.1213/XAA.0000000000000090
7. Corso RM, Piraccini E, Sorbello M, Bellantonio D, Tedesco M. Ultrasound-guided transmuscular quadratus lumborum block for perioperative analgesia in open nephrectomy. Minerva Anestesiol. 2017;83(12):1334–1335. doi:10.23736/S0375-9393.17.12167-X
8. Ishio J, Komasawa N, Kido H, Minami T. Evaluation of ultrasound-guided posterior quadratus lumborum block for postoperative analgesia after laparoscopic gynecologic surgery. J Clin Anesth. 2017;41:1–4. doi:10.1016/j.jclinane.2017.05.015
9. Johnston DF, Sondekoppam RV. Continuous quadratus lumborum block analgesia for total hip arthroplasty revision. J Clin Anesth. 2016;35:235–237. doi:10.1016/j.jclinane.2016.08.002
10. Kadam VR. Ultrasound guided quadratus lumborum block or posterior transversus abdominis plane block catheter infusion as a postoperative analgesic technique for abdominal surgery. J Anaesthesiol Clin Pharmacol. 2015;31(1):130–131. doi:10.4103/0970-9185.150575
11. Carney J, Finnerty O, Rauf J, Bergin D, Laffey JG, Mc Donnell JG. Studies on the spread of local anaesthetic solution in transversus abdominis plane blocks. Anaesthesia. 2011;66(11):1023–1030. doi:10.1111/j.1365-2044.2011.06855.x
12. El-Boghdadly K, Elsharkawy H, Short A, Chin KJ. Quadratus lumborum block nomenclature and anatomical considerations. Reg Anaesth Pain Med. 2016;41(4):548–549. doi:10.1097/AAP.0000000000000411
13. Blanco R, Ansari T, Girgis E. Quadratus lumborum block for postoperative pain after caesarean section: a randomised controlled trial. Eur J Anaesthesiol. 2015;32(11):812–818. doi:10.1097/EJA.0000000000000299
14. Hansen CK, Dam M, Bendtsen TF, Borglum J. Ultrasound-guided quadratus lumborum blocks: definition of the clinical relevant endpoint of injection and the safest approach. A A Case Rep. 2016;6(2):39. doi:10.1213/XAA.0000000000000270
15. Sato M, Hara M, Uchida O. An antero-lateral approach to ultrasound-guided lumbar plexus block in supine position combined with quadratus lumborum block using single-needle insertion for pediatric hip surgery. Paediatr Anaesth. 2017;27(10):1064–1065. doi:10.1111/pan.13208
16. Kerai S, Saxena KN, Taneja B. Post-caesarean analgesia: what is new? Indian J Anaesth. 2017;61(3):200–214.
17. Champaneria R, Shah L, Wilson MJ, Daniels JP. Clinical effectiveness of transversus abdominis plane (TAP) blocks for pain relief after caesarean section: a meta-analysis. Int J Obstet Anesth. 2016;28:45–60. doi:10.1016/j.ijoa.2016.07.009
18. Ueshima H, Otake H, Lin JA. Ultrasound-guided quadratus lumborum block: an updated review of anatomy and techniques. Biomed Res Int. 2017;2017:2752876. doi:10.1155/2017/2752876
19. Bonnet MP, Mignon A, Mazoit JX, Ozier Y, Marret E. Analgesic efficacy and adverse effects of epidural morphine compared to parenteral opioids after elective caesarean section: a systematic review. Eur J Pain. 2010;14(9):894e1–9. doi:10.1016/j.ejpain.2010.03.003
20. Singh SI, Rehou S, Marmai KL, Jones PM. The efficacy of 2 doses of epidural morphine for postcesarean delivery analgesia: a randomized noninferiority trial. Anesth Analg. 2013;117(3):677–685. doi:10.1213/ANE.0b013e31829cfd21
21. Sebbag I, Qasem F, Dhir S. [Ultrasound guided quadratus lumborum block for analgesia after cesarean delivery: case series]. Rev Bras Anestesiol. 2017;67(4):418–421. doi:10.1016/j.bjan.2017.03.002
22. Carline L, McLeod GA, Lamb C. A cadaver study comparing spread of dye and nerve involvement after three different quadratus lumborum blocks. Br J Anaesth. 2016;117(3):387–394. doi:10.1093/bja/aew224
23. Adhikary SD, El-Boghdadly K, Nasralah Z, Sarwani N, Nixon AM, Chin KJ. A radiologic and anatomic assessment of injectate spread following transmuscular quadratus lumborum block in cadavers. Anaesthesia. 2016;72(1):73–79. doi:10.1111/anae.13647
24. Dam M, Moriggl B, Hansen CK, Hoermann R, Bendtsen TF, Borglum J. The pathway of injectate spread with the transmuscular quadratus lumborum block: a cadaver study. Anesth Analg. 2017;125(1):303–312. doi:10.1213/ANE.0000000000001922
25. Wikner M. Unexpected motor weakness following quadratus lumborum block for gynaecological laparoscopy. Anaesthesia. 2017;72(2):230–232. doi:10.1111/anae.13754
26. Kato N, Fujiwara Y, Harato M, et al. Serum concentration of lidocaine after transversus abdominis plane block. J Anesth. 2009;23(2):298–300. doi:10.1007/s00540-008-0721-4
27. Griffiths JD, Le NV, Grant S, Bjorksten A, Hebbard P, Royse C. Symptomatic local anaesthetic toxicity and plasma ropivacaine concentrations after transversus abdominis plane block for Caesarean section. Br J Anaesth. 2013;110(6):996–1000. doi:10.1093/bja/aet015
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.