")
Back to Journals » Nature and Science of Sleep » Volume 13
Post-Operative Sleep Endoscopy with Target-Controlled Infusion After Palatopharyngoplasty for Obstructive Sleep Apnea: Anatomical and Polysomnographic Outcomes
Authors Chiu FH , Chang Y, Liao WW, Yeh YL, Lin CM, Jacobowitz O, Hsu YS
Received 22 March 2021
Accepted for publication 7 July 2021
Published 20 July 2021 Volume 2021:13 Pages 1181—1193
DOI https://doi.org/10.2147/NSS.S311702
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ahmed BaHammam
Feng-Hsiang Chiu,1,2 Yi Chang,3 Wen-Wei Liao,3 Yu-Ling Yeh,3 Chia-Mo Lin,4– 6 Ofer Jacobowitz,7 Ying-Shuo Hsu8,9
1Department of Otolaryngology, Head and Neck Surgery, Tri-service General Hospital, Taipei, Taiwan; 2National Defense Medical Center, Taipei City, Taiwan; 3Department of Anesthesiology, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan; 4Division of Chest Medicine, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan; 5Department of Chemistry, Fu-Jen Catholic University, New Taipei City, Taiwan; 6Graduate Institute of Biomedical and Pharmaceutical Science, Fu Jen Catholic University, New Taipei City, Taiwan; 7ENT & Allergy Associates, New York, NY, USA; 8Department of Otolaryngology, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan; 9School of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan
Correspondence: Ofer Jacobowitz
ENT & Allergy Associates, New York, NY, USA
Tel +1 646 868-4300
Email [email protected]
Ying-Shuo Hsu
Department of Otolaryngology, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan
Tel +1-886-2-28332211 ext.2551
Email [email protected]
Introduction: The findings of drug-induced sleep endoscopy (DISE) are not always correlated with the outcome of upper airway surgery for obstructive sleep apnea (OSA), and whether multilevel surgery is truly required in treating multilevel obstruction identified in preoperative DISE remains an issue. We attempted to compare DISE findings before and after palatopharyngoplasty in patients with OSA because changes in DISE may be beneficial to better understand polysomnographic and anatomical outcomes.
Methods: This was a prospective cohort study for 34 patients with moderate to severe OSA who underwent palatopharyngoplasty at a tertiary care center from 2016 to 2018. We recorded the patients’ demographic characteristics, procedures, and surgical outcomes and compared the preoperative and postoperative DISE staging patterns.
Results: The apnea-hypopnea index (AHI) values of 34 adults improved significantly after surgery (40.6 ± 23.3 versus 25.6 ± 20.6, P < 0.001). The majority of patients, 26/34, had preoperative complete concentric collapse at the velum, and for most (20/26, 77%) there was a change of the collapse pattern into anteroposterior collapse postoperatively. Patients with postoperative velar collapse had higher follow-up AHI values than those who without (27.8 ± 21.9 versus 15.2 ± 7.7, P = 0.023). Patients with preoperative complete tongue base collapse had higher follow-up AHI values than did those with no or partial collapse (40.6 ± 21.0 versus 21.0 ± 18.6, P = 0.017). Patients with postoperative complete tongue base collapse also had higher follow-up AHI values than the others (42.7 ± 22.1 versus 18.5 ± 15.4, P = 0.001).
Conclusion: Palatopharyngoplasty could change the collapse pattern at the velum in most patients. Preoperative and postoperative complete tongue base collapse and postoperative velar collapse identified in TCI-DISE were associated with relatively poor outcomes.
Keywords: obstructive sleep apnea, drug-induced sleep endoscopy, palatopharyngoplasty, postoperative, complete concentric collapse, tongue base collapse
Plain Language Summary
To patients with obstructive sleep apnea (OSA) who are not compliant to conservative therapy, upper airway surgery is an alternative. However, because of the complex nature of upper airway, it is hard for surgeons to do surgical decision making. Drug induced sleep endoscopy (DISE) is an accessible tool for surgeons to see which part of upper airway collapse when OSA patients are asleep, however, the surgical decision making according to those findings did not always achieve better surgical outcome. For example, Hsu and Jacobowitz described that for OSA patients with multiple obstruction sites or only one obstruction site in DISE, single surgery to one of the obstruction sites contributed to similar postoperative sleep apnea improvements. One reason for the surprising result was that doing DISE with manual injection of propofol may cause unsteady sleep and excessive collapse in upper airway, especially tongue base.
To clarify whether multiple surgeries are necessary to multiple obstructions in DISE, we did a study of DISE with target-controlled infusion (TCI-DISE) before and after single surgery. TCI-DISE is a better way to control the sleep depth by using drug injection machine.
In this study of 34 patients, we found that there were significant associations between TCI-DISE findings and surgical outcomes, especially preoperative and postoperative complete tongue base collapse and postoperative velar collapse. Our results indicate that multiple surgeries should be considered in OSA patients with multiple obstructions in TCI-DISE. Furthermore, revision surgery may be also needed if there is persistent collapse at velum in postoperative TCI-DISE.
Introduction
Obstructive sleep apnea (OSA) is a highly prevalent disorder. Benjafield et al1 estimated that 425 million adults have moderate to severe OSA globally. This disorder also poses a considerable threat to public health because it has been associated with excessive daytime sleepiness,2 increased risk of sudden cardiac death,3 hypertension,4 cerebrovascular incidents,5 and type 2 diabetes.6 Although continuous positive airway pressure (CPAP) therapy is typically used as the first-line treatment,7 upper airway surgery is considered an alternative therapy because long-term adherence to CPAP therapy is often suboptimal.8
Uvulopalatopharyngoplasty (UPPP) is commonly applied to patients with OSA for whom CPAP therapy failed. In a review the short-term and long-term success rate of this procedure alone ranged from 35% to 65% and from 28.6% to 55%, respectively.9,10 To improve outcomes and avoid complications,11 advanced procedures have been advocated to increase the intraluminal space of the pharynx during sleep; these procedures include lateral pharyngoplasty (LP), expansion sphincter pharyngoplasty, barbed reposition pharyngoplasty, and suspension palatoplasty (SP).12–15 LP is performed to expand the lateral pharyngeal airway by cutting and repositioning the lateral pharyngeal musculature, such as the palatopharyngeus and superior constrictor. SP is applied to enlarge the anterior-posterior velopharyngeal dimension by pulling the soft palate forward and anchoring it to the pterygomandibular raphe. These procedures involve less soft palate excision than does traditional UPPP, preventing scar formation and stenosis.16 However, the effects of these surgical procedures on the staging or pattern of upper airway obstruction identified in drug-induced sleep endoscopy (DISE) have not been well investigated.17
To target the sites and structures of upper airway obstruction before surgery, sleep endoscopy was first advocated by Croft and Pringle in the 1990s.18 Kezirian renamed this technique “DISE”19 and developed the velum, oropharyngeal lateral walls, tongue base, and epiglottis (VOTE) classification system.20 Because this procedure offers a real-time and dynamic image to identify the sites where upper airway obstruction occurs in simulated sleep, it has been widely adopted as a potentially useful tool to help surgeons customize their surgical plan for each patient with OSA.21 In addition, multilevel upper airway obstruction occurs in many patients with OSA,22 but the assessment in awake state does not predict tongue base collapse in sleep.23 Thus, DISE could potentially be used to guide surgical decision-making.
Polysomnographic outcomes after DISE-guided upper airway surgery are not always satisfactory.21,24–28 Concentric velum collapse, total anteroposterior tongue base obstruction, retrolingual lateral pharyngeal wall collapse, and supraglottic laryngeal collapse identified in preoperative DISE have been reported to predict surgical failure.25,26,28 Preoperative DISE findings are not necessarily helpful either: Meraj et al27 revealed that such findings are not correlated with surgical success after multilevel surgery combined with transoral robotic tongue base resection. These studies have raised some questions. The first question relates to whether multilevel surgery is truly effective in treating multilevel obstruction identified in DISE. The second question relates to whether multilevel surgery is required for every patient with multilevel obstruction revealed through preoperative DISE. In our previous study,28 we found that in patients treated with palatopharyngoplasty alone, surgical outcomes for multilevel and unilevel obstructions identified in DISE were similar. To further clarify these questions, postoperative DISE analysis may be very useful. More reliable DISE techniques are also required for the identification of collapse patterns in stable sleep and to achieve that, target-controlled infusion (TCI) is a suitable choice.29,30
In this study, we analyzed the staging patterns of preoperative and postoperative DISE in patients with moderate to severe OSA after advanced palatopharyngoplasty. We used TCI techniques in this DISE study (henceforth TCI-DISE) because it could engender more stable sleep throughout the examination. This technique enabled us to possibly obtain more reliable results.29,30
Methods
Study Subjects
This prospective study assessed 34 patients with moderate to severe OSA who underwent palatopharyngoplasty; we performed DISE before and at least 3 months after surgery. The operations were all performed by a single surgeon (Dr. Ying-Shuo Hsu) from 2016 to 2018 at a tertiary referral hospital (Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan). Inclusion criteria were as follows: (1) having a baseline AHI or respiratory event index of >15 events/h, as revealed by a polysomnogram (PSG, [Compumedics Grael Compumedics Limited, Abbotsford, Victoria, Australia]) or home sleep apnea test (HST, [ApneaLink Air, Resmed Ltd, NSW, Australia]); (2) having received a follow-up sleep study and sleep endoscopy at least 3 months after upper airway surgery; (3) having no prior upper airway surgery other than nasal surgery; (4) being unwilling to accept CPAP therapy or nonadherent to CPAP therapy under the care of a board-certified sleep medicine specialist; (5) having no significant nasal obstruction or receiving treatment for it at the same time; and (6) having no habitual use of sedatives, antipsychotics, melatonin and alcohol abuse. We performed an overnight standard PSG and conducted the corresponding scoring in accordance with the American Academy of Sleep Medicine’s 2012 definitions,31 using the same scoring criteria for the relevant patients’ preoperative and postoperative studies. Specifically, hypopnea is scored when the peak signal excursions drop by ≥ 30% of pre-event baseline using nasal pressure, for ≥10 seconds in association with either ≥ 3% arterial oxygen desaturation or an arousal. Studies were interpreted by a board-certified sleep physician.
The study protocol (IRB Number: 20161002R) was approved by the institutional review board of Shin Kong Wu-Ho-Su Memorial Hospital, Taipei, Taiwan. All patients provided written informed consents prior to participation, and this study complied with the Declaration of Helsinki.
TCI-DISE System
DISE was performed in the supine position in an outpatient clinic setting in the bronchoscopy room before and at least 3 months after palatopharyngoplasty. Oxymetazoline-soaked pledgets were applied to both nostrils for vasoconstriction of the nasal mucosa before the procedure. To control the depth of sleep throughout the examination, a TCI system (Fresenius Kabi Injectomat TIVA Agilia, Bad Homburg, Germany) was used to achieve a target level of anesthesia of absent arousal to loud verbal stimulation and maintain the bispectral index (BIS) at 50 to 70.29,30 In short, the Schnider model32 was used to administer propofol at a starting dose of 3.0 mcg/mL and subsequent increments of 0.1 to 0.3 mcg/mL until a new cerebral concentration was reached. Compared with conventional bolus injection techniques,19 TCI-DISE could provide greater accuracy, stability, and safety. When the BIS level was achieved, a flexible endoscope was passed through the nasal passage, nasopharynx, velum, oropharynx, tongue base, epiglottis, and larynx to assess the obstruction sites. The DISE procedure lasted at least 2 minutes long or 2 to 3 repeat cycles of snoring, hypoxia, obstruction with apnea and breakthrough with snoring again to ensure reproducible and reliable assessment.33 All examinations were video recorded, and the degree of obstruction at each anatomic site was determined by 2 experienced sleep doctors, one of whom (Dr Chiu) was blinded to the type of surgery and postoperative polysomnographic outcome. In case of disagreement in scoring, the reviewers will discuss it to meet the consensus.
Every patient enrolled in the study underwent preoperative DISE, and postoperative DISE was also performed at least 3 months after surgery. All the DISE findings were scored using the VOTE classification system.27,34
Palatopharyngoplasty and Surgical Success Definition
All patients underwent palatopharyngoplasty for retropalatal collapse identified in DISE. For each patient, we used a 70° rigid endoscope to examine the velopharyngeal space through the nose during the procedure in order to ensure sufficient velopharyngeal space enlargement.
The palatopharyngoplasty procedure we performed for the participants was originated from the conventional SP15 with the incorporation of some LP elements. Briefly, after tonsillectomy, we removed the submucosal fat tissue in the semilunar-shaped supratonsillar area, with careful preservation of the palatopharyngeus muscle and pillar mucosa. The supratonsillar mucosa was elevated laterally to expose the pterygomandibular raphe, where the upper palatopharyngeus muscle was secured with 2-0 Vicryl sutures. We partially lysed the palatopharyngeus inferiorly before suspending it to the pterygomandibular raphe. We also shortened the uvula to 1 cm in length if required. Furthermore, we performed vertical posterior wall-releasing incisions if horizontal tension bands were present.
We defined surgical success as a ≥50% decrease in the AHI relative to the baseline value and a postoperative AHI of <20 events/h.
Statistical Analysis
We observed several zero cells in a cross-table of preoperative × postoperative sleep endoscopy staging patterns; therefore, the change from preoperative to postoperative patterns was evaluated using the exact and Monte Carlo symmetry tests for paired contingency tables. The Monte Carlo symmetry test is equivalent to uncorrected McNemar and McNemar-Bowker tests when there are no zeros in critical cells.35 We applied an independent-sample t test to compare continuous surgical outcomes (ie, follow-up AHI values) between patients with and without complete obstruction after surgery. Moreover, we used a one-way analysis of variance to compare continuous surgical outcomes between patients with no collapse, partial collapse, and complete collapse postoperatively. We employed the Fisher exact test to compare surgical success rates in patients with different staging patterns. A 2-sided P value of <0.05 was considered statistically significant. The Monte Carlo symmetry test was conducted using R version 3.6.3 (R Development Core Team) with the “rcompanion” package (Version 2.3.26 updated on November 5, 2020). Other data analyses were done by using SPSS 25 (IBM SPSS Inc, Chicago, IL, USA).
Results
Baseline Characteristics and Surgical Outcomes
A total of 60 patients underwent palatopharyngoplasty from 2016 to 2018, with lost follow-up sleep studies or unwilling to have post-op DISE in 26 patients. Overall, 34 patients who underwent palatopharyngoplasty from May 2016 to September 2018 with post-op DISE were finally included in this study. Men constituted a predominant portion of all patients (82.4%; 28/34). The average age was 45.5 ± 11.4 years. We conducted the follow-up sleep study at least 3 months after upper airway surgery. We also analyzed the patients’ baseline characteristics and surgical outcomes.
Table 1 presents the changes in body mass index (BMI), AHI, and oxygen saturation (SaO2) before and after surgery. The surgical AHI success rate in all participants was 29.4% (10/34). The AHI and minimal SaO2 values were significantly improved after surgery.
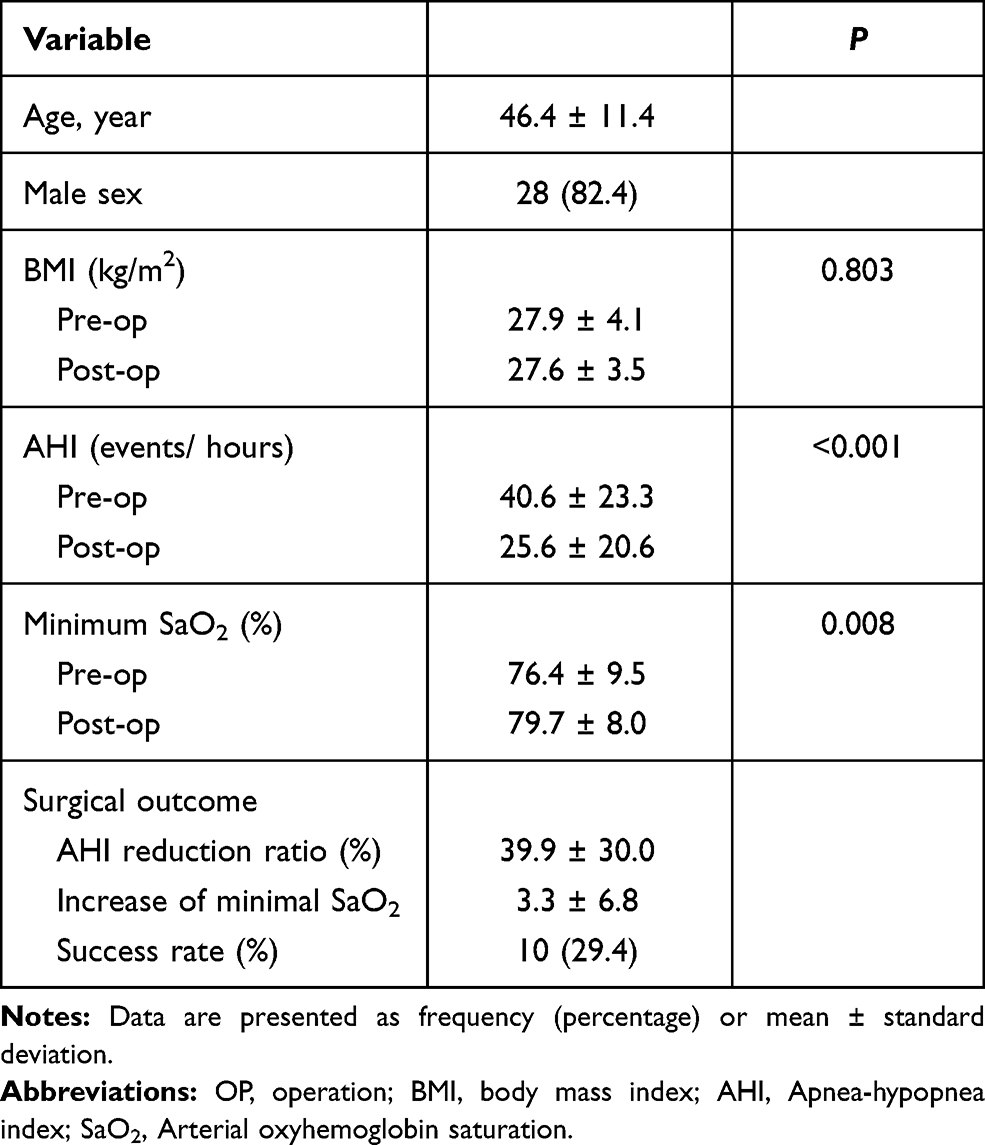 |
Table 1 Baseline Characteristics and Changes After Surgery (N = 34) |
Sleep Endoscopy Staging Patterns: Velum
Preoperatively, all patients presented complete collapse at the velum level: 6 patients presented anteroposterior collapse (APC), 2 presented lateral collapse (LC), and the remaining 26 presented complete concentric collapse (CCC). Among the 26 patients with preoperative CCC (Figure 1A and B), postoperative sleep endoscopy demonstrated APC (Figure 1C and D) in 20 (complete: 18; partial: 2), persistent CCC in 3, and total CCC resolution in the remaining 3. Among the 6 patients with preoperative complete APC at the velum, total resolution was achieved in 2 but complete APC remained in the remaining 4 after surgery. For the 2 patients with preoperative LC, postoperative sleep endoscopy demonstrated total resolution of LC at the velum (P <0.001; Figure 2). Sleep endoscopy in our study demonstrated an obvious transformation from preoperative CCC to postoperative APC.
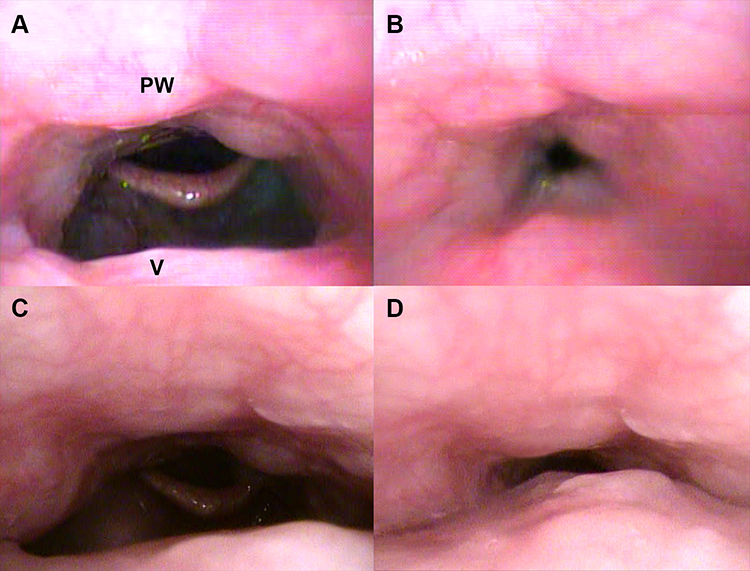 |
Figure 1 Demonstration of the collapse pattern at the velum before and after surgery from the same patient during TCI-DISE. (A) Preoperative expiration view, and CCC was revealed on inspiration (B). (C) Postoperative expiration view, and APC was revealed on inspiration (D). Abbreviations: CCC, complete concentric collapse; APC, anteroposterior collapse; PW, pharyngeal wall; V, velum. |
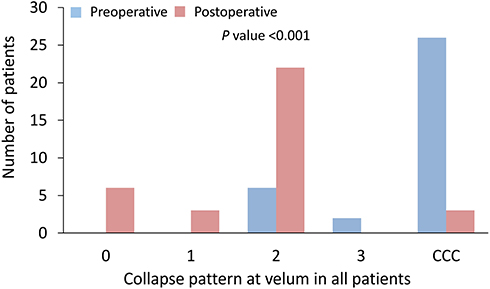 |
Figure 2 Detailed different collapse patterns at the velum before and after surgery for all 34 patients. The numbers “0,” “1,” “2,” and “3” indicate no collapse, partial anteroposterior collapse, total anteroposterior collapse, and total lateral collapse, respectively. Abbreviation: CCC, complete concentric collapse. |
Sleep Endoscopy Staging Pattern: Tongue Base
A total of 12 patients presented tongue base collapse preoperatively: 8 with complete collapse and 4 with partial collapse. 16 patients presented tongue base collapse postoperatively: 10 with complete collapse and 6 with partial collapse. Among the 8 patients with preoperative complete tongue base collapse, 5, 2, and 1 presented complete, partial, and total resolution of tongue base collapse postoperatively, respectively (Figure 3A–D). Of the 22 patients without tongue base collapse, 7 presented prominent tongue base collapse (complete: 4; partial: 3) after palatopharyngoplasty (Figure 4A and B). Noticeably, no significant differences before and after operation were observed. Furthermore, either preoperative or postoperative complete collapse at tongue base was not correlated with the collapse at velum (data not shown).
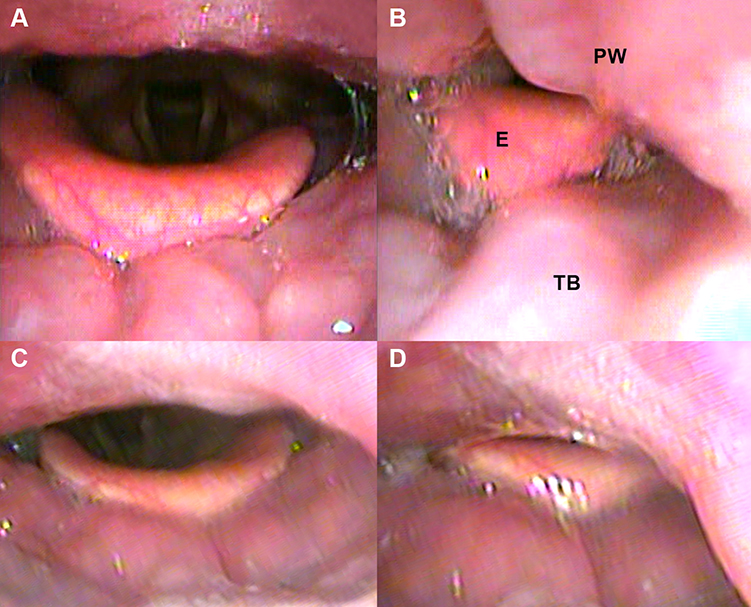 |
Figure 3 Complete tongue base collapse observed in TCI-DISE indicated a relatively poor surgical outcome after palatopharyngoplasty. Hypopharynx in expiration (A) and inspiration (B) preoperatively revealed complete tongue base collapse. Hypopharynx in expiration (C) and inspiration (D) revealed complete tongue base collapse again postoperatively. Abbreviations: E, epiglottis; PW, pharyngeal wall; TB, tongue base. |
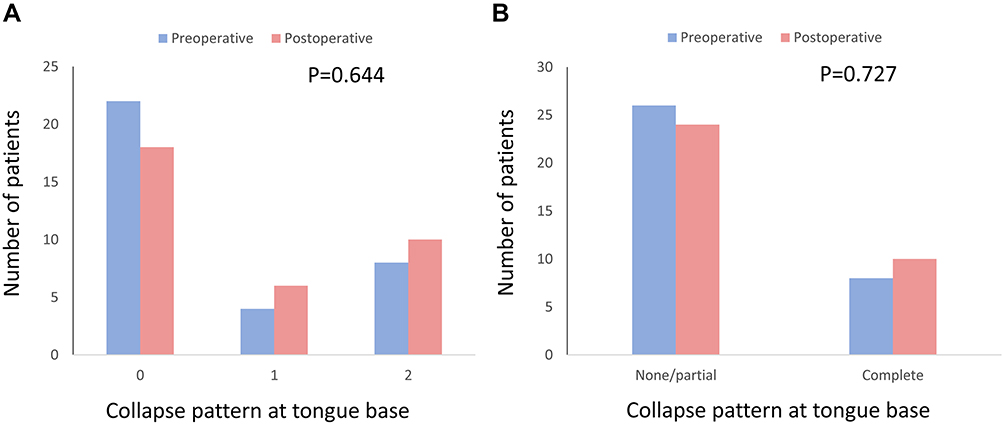 |
Figure 4 Detailed (A) and dichotomized (B) tongue base collapse patterns before and after surgery. The numbers “0,” “1,” and “2,” indicate no collapse, partial collapse, and complete collapse, respectively. |
Relationship Between Sleep Endoscopy Findings and Surgical Outcomes
Among 15 patients in all 34 participants, multilevel collapse was observed in preoperative DISE (15/34, 44.1%). Postoperatively, multilevel collapse remained only in 6 patients (6/34, 17.6%). The results demonstrated that there was significant difference in post-OP AHI between patients with and without complete collapse of ≥2 levels for VOTE. The patients with complete collapse of ≥2 levels had greater post-OP AHI values than the patients who without (38 vs 20.4 event/hour, P = 0.021). Moreover, we conducted an additional analysis to evaluate multilevel collapse for velum and tongue base. The results showed that the post-OP AHI was significantly greater in patients with complete collapse for both velum and tongue base than those who without preoperatively (46 vs 22.1 event/hour, P = 0.014). We have added two supplemental tables (Supplemental Tables 1 and 2) to demonstrate the results.
We stratified the patients into groups depending on whether the postoperative sleep endoscopy findings revealed complete collapse at each upper airway level. The surgical outcomes included the follow-up AHI value, AHI reduction ratio, and surgical success rate. Patients with remaining collapse at velum had greater postoperative AHI values than those without (27.8 vs 15.2 events/hour, P = 0.023) (Table 2). We observed no significant difference in all outcomes between patients with preoperative and postoperative CCC and those without CCC (Table 2), but only 8/34 patients had a non-CCC pattern. Notably, when patients presented complete tongue base collapse as revealed by their preoperative or postoperative TCI-DISE findings, their postoperative AHI values were significantly higher than those of patients with partial or no tongue base collapse in TCI-DISE findings before or after surgery. (Table 3 and Figure 5A and B). Those significance results were even more significant after adjusting for age and preoperative BMI value in the multivariable linear regression analyses (data not shown).
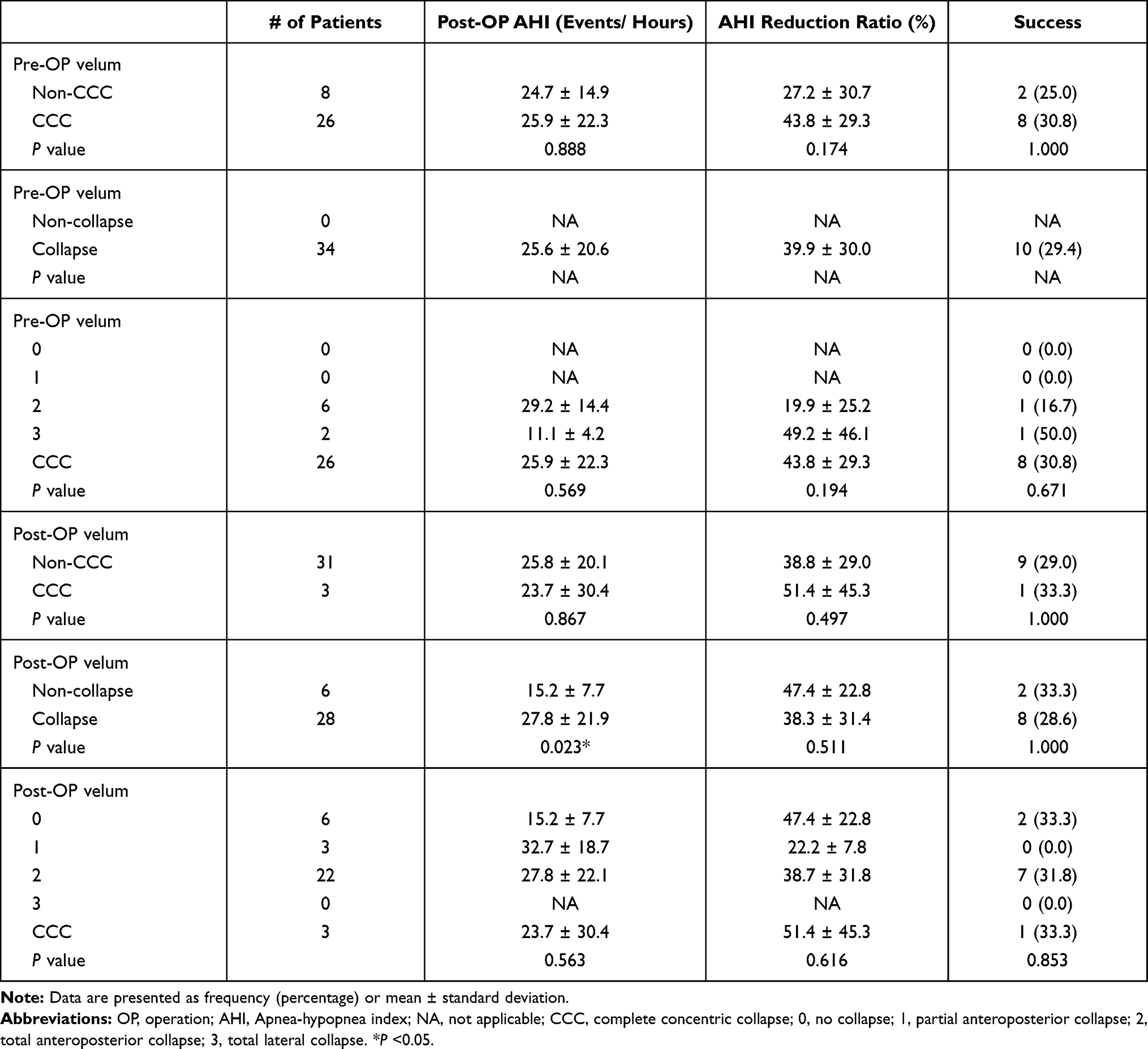 |
Table 2 Outcomes According to Preoperative and Postoperative Status at the Velum |
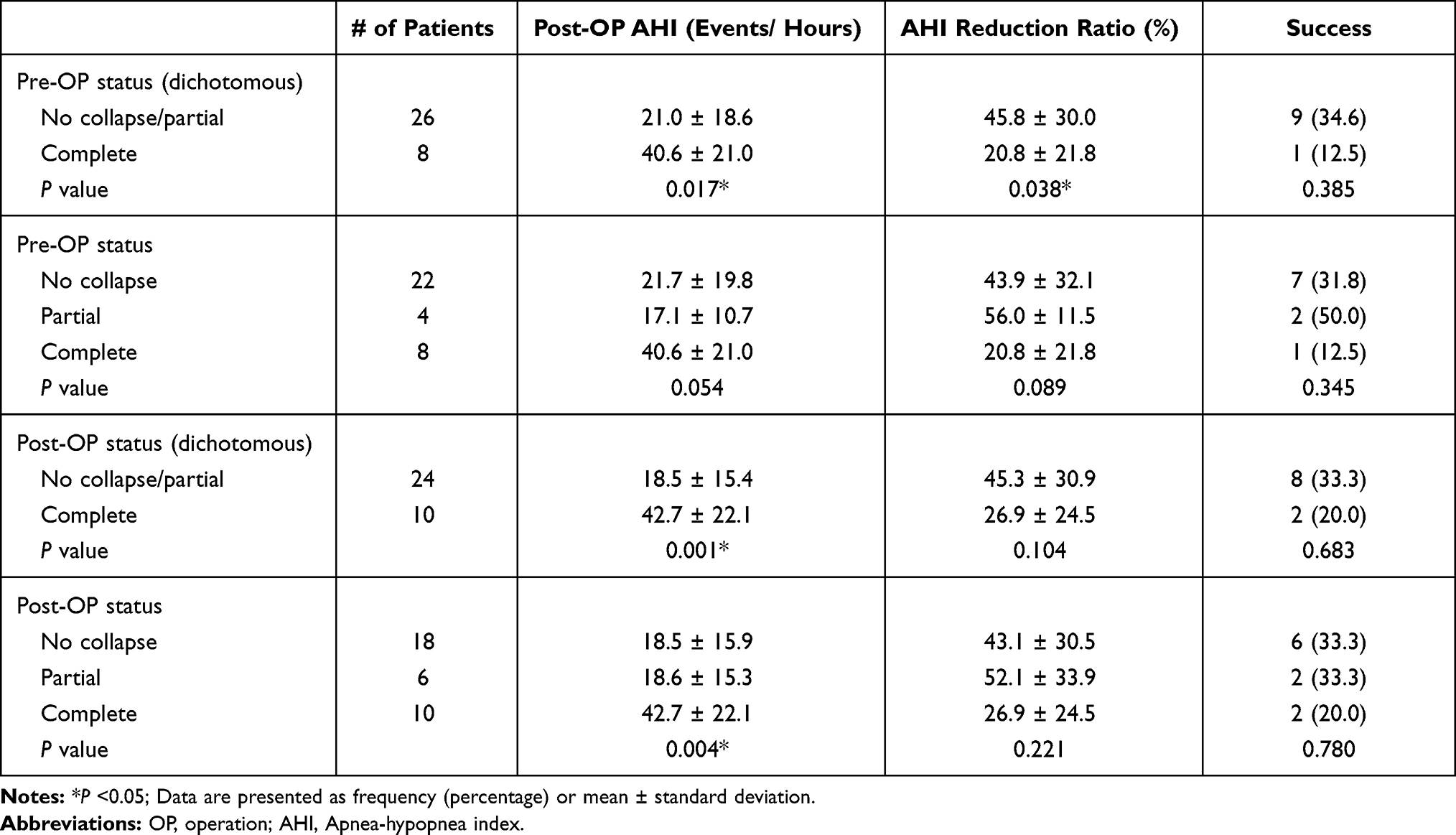 |
Table 3 Outcomes According to Preoperative and Postoperative Status at the Tongue Base |
 |
Figure 5 Follow-up AHI values of the 34 patients with detailed (A) and dichotomized (B) tongue base collapse patterns after surgery. Abbreviation: AHI, Apnea-hypopnea index. |
The sleep endoscopy staging patterns for the oropharynx and epiglottis are listed. We observed no significant differences in all outcomes between patients with and without complete obstruction at the oropharynx or at the epiglottis (Table 4).
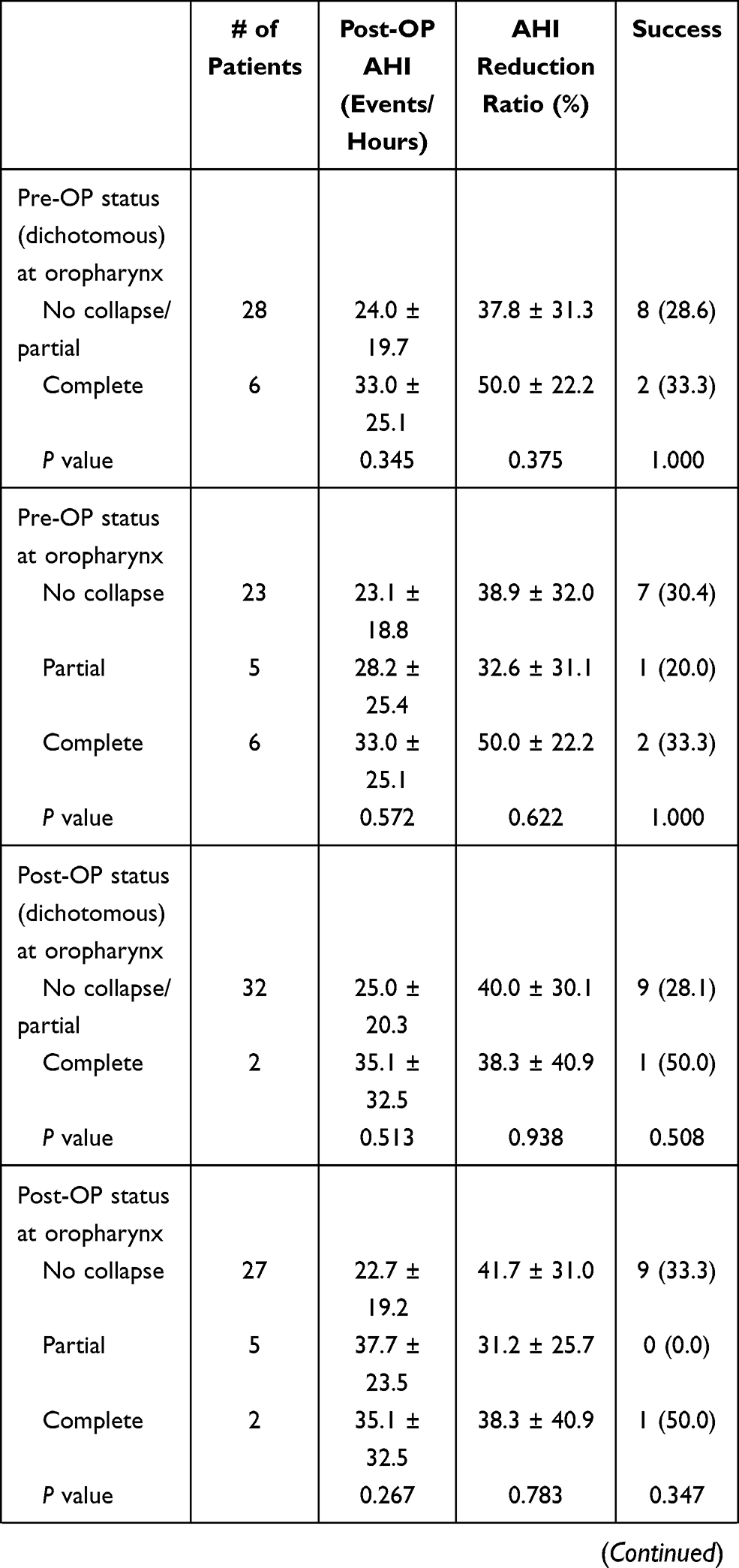 |
Table 4 Outcome According to Pre-OP and Post-OP Status at Oropharynx and Epiglottis |
Discussion
According to our review of the literature, this is the first study to prospectively collect preoperative and postoperative TCI-DISE and sleep study data in patients with moderate to severe OSA who underwent palatopharyngoplasty. AHI values were significantly reduced, and the minimal SaO2 value was significantly elevated postoperatively. TCI-DISE demonstrated that most patients’ CCC at the velum level shifted to anteroposterior collapse after palatopharyngoplasty. However, these changes were not significantly associated with the AHI. Relatively poor surgical outcomes after palatopharyngoplasty were significantly related to multilevel collapse identified preoperatively and tongue base collapse in either preoperative or postoperative TCI-DISE. Because tongue base collapse significantly contributes to relatively poor surgical results, multilevel surgery to treat the tongue base may be necessary when tongue base collapse is observed in TCI-DISE. Furthermore, our results demonstrated that patients with remaining collapse at velum had greater residual AHI values after palatopharyngoplasty. A persistent collapse at the level of the velum may need further treatment, as upstream persistent collapse could mediate downstream collapse.
Most patients (26/34, 76.5%) had preoperative CCC of the velum, 20 presented APC (20/26, 76.9%), as revealed by the postoperative DISE. This transformation has also been addressed in related studies.36,37 Although Hasselbacher et al36 and Liu et al37 described that collapse pattern changed at velopharynx among 15 and 12 patients after palatopharyngoplasty respectively, the correlations between postoperative DISE and surgical outcome were not investigated fully, and those studies were done by manual injection of propofol. Besides, the change of collapse pattern in DISE at lower levels (tongue base, oropharynx and epiglottis) were not addressed in detail. Our results might provide novel information as below: (1) Presentation of the postoperative change of collapse pattern in TCI-DISE in the whole upper airway (velopharynx, oropharynx, tongue base and epiglottis) after unilevel palatopharyngoplasty; (2) Correlation of the surgical outcome preoperatively and postoperatively with TCI-DISE; (3) Clarification that when tongue base collapse and multilevel obstruction are presented in TCI-DISE, they are poor prognostic factors to unilevel palatopharyngoplasty. (4) Absence of velar collapse in postoperative TCI-DISE correlate to better surgical outcome. We believed that those TCI-DISE results are going to help sleep surgeons to do precision medicine when treating OSA patients.
CCC is considered a contraindication to upper airway stimulation (UAS).38 In our study, most CCC cases were resolved after palatopharyngoplasty; thus, more future treatment options are available for patients originally excluded because of UAS selection criteria. Among the 26 patients with preoperative CCC, 3 demonstrated total resolution (3/26, 11.5%). This finding indicates that retropalatal obstruction could be completely ameliorated by palatopharyngoplasty in some patients. Other factors may also play a critical role in CCC. For example, the tongue body may push back against the soft palate at the velopharyngeal level.39 The probability of CCC is associated with higher BMI and AHI values.40 Consistent postoperative CCC could also be attributed to older age, overweight, severe OSA with high collapsibility.36
CCC identified in preoperative DISE is considered a poor prognostic factor for surgical outcomes.28,41 Because most of the patients in our study presented CCC on DISE, the lower surgical success rate (10/34, 29.4%) in our study is similar to that in related reports9,10,14,28 and could be anticipated, especially considering that we performed single-level surgery in patients with moderate to severe OSA. However, whether CCC after palatopharyngoplasty is related to poor surgical outcomes is unclear. In our study, the AHI success rate, AHI reduction ratio, and increase in minimal SaO2 in the 3 patients with postoperative CCC were not significantly different from those in the remaining patients. Additional lines of evidence are required to clarify whether persistent CCC after palatopharyngoplasty is indicative of poor surgical outcomes. Another important point is that AASM 2012 hypopnea definition is more inclusive and residual AHI may be higher for this reason.
Probability of tongue base collapse is associated with higher AHI values and positional OSA.42 However, whether tongue base collapse in DISE is a poor prognostic factor to palatopharyngoplasty remains unclear in literature review.25,28 Hsu and Jacobowitz described that in DISE with manual injection of propofol, OSA patients with multilevel obstruction (retropalatal and tongue base collapse) and unilevel obstruction (only retropalatal collapse) presented similar postoperative AHI values after unilevel palatopharyngoplasty, so only palatopharyngoplasty may also achieve good results to multilevel obstruction with less complication.43 To clarify this issue, better propofol injection method like TCI-DISE and postoperative DISE after palatopharyngoplasty are necessary to evaluate residual collapse in upper airway.
Our data demonstrate that both preoperative and postoperative tongue base collapse identified in TCI-DISE significantly affected surgical outcome. In the future, since we found that most patients with tongue base obstruction in TCI-DISE did not achieve good results and tongue base obstruction remained the same in postoperative TCI-DISE, we could be more confident to do tongue base surgery and use TCI-DISE as a tool to decide whether multilevel surgery is necessary. Studies of postoperative TCI-DISE after multilevel surgery should also be done in the future to compare the surgical outcome with unilevel surgery.
This finding implies that if tongue base collapse is not noted preoperatively in TCI-DISE, practitioners can more confidently recommend single-level or single-stage procedures first, such as LP or SP, even for a patient with a large tongue, because multilevel surgery still involves a greater risk of complications than does single-level surgery.43 By contrast, if tongue base collapse is identified in TCI-DISE preoperatively, practitioners can also more confidently recommend tongue base procedures to the relevant patients. Another important interpretation is that residual AP velar collapse is also a problem. Tongue base collapse may be a sign of greater collapsibility still and the palatopharyngeal musculature may also need to be stabilized with a revision procedure. In our study, persistent complete collapse at the level of the velum after palatopharyngoplasty potentially contributes to higher residual AHI as well. Hence, for patients with complete tongue base collapse in TCI-DISE after palatopharyngoplasty, hypopharyngeal surgery or revision palatopharyngoplasty is reasonable.
Because we performed only palatopharyngoplasty in the patients, we expected the tongue base obstruction pattern in TCI-DISE to be the same after surgery. However, 8 patients (8/34, 23.5%) presented exacerbated tongue base collapse in postoperative TCI-DISE. Nevertheless, the follow-up AHI and surgical success rate in these 8 patients were not significantly different from those of the remaining patients. A possible explanation for this unexpected finding is that the amelioration of upper- level obstruction facilitated the observation of lower level obstruction. Because postoperative tongue base obstruction in TCI-DISE was significantly associated with relatively poor surgical outcomes in this study, follow-up TCI-DISE is recommended in patients after upper airway surgery, especially in those with poor outcomes.
In our study cohort, most patients (76.5%) presented CCC, a considerably higher proportion than those presented in other reports28,44 (23% to 49%). Possible explanations for an abnormally high percentage of patients with CCC as compared to other previous studies include: (1) patients with CCC may have higher collapsibility of upper airway and they may be more intolerant to CPAP, so they are more willing to undergo alternative therapy, such as surgery; (2) the patients tend to have worse outcome or residual sleep apnea after palatopharyngoplasty, so they may have more motivation to cooperate with doctors and have post-op sleep endoscopy to seek further treatment options. Further studies with larger cohort may be needed to prove these hypotheses.
The low total resolution rate for retropalatal collapse after palatopharyngeal surgery may be attributed to the complexity of the pathophysiology of CCC because the collapse may not originate from the velopharyngeal structure itself. The tongue body may push the palate backward to produce retropalatal APC;39 therefore, it may also produce CCC when the lateral velopharyngeal wall collapses. Although palatopharyngoplasty attenuated lateral pharyngeal wall collapse in our study, the remaining tongue body collapse produced APC in most patients. This hypothesis was supported by positional changes observed in our postoperative DISE. The velopharyngeal collapse in most of the patients was completely resolved when the patients’ heads were placed in a lateral position because their tongue body no longer pushed the palate back (data not shown).
Limitations
This study has some limitations. First, DISE may not demonstrate upper airway obstruction during rapid-eye-movement sleep,45 and the degree of upper airway narrowing could be aggravated by the depth of sedation and length of the procedure.46 Second, the applied DISE scoring system is subjective, and some concerns remain regarding its interobserver reliability.47 Third, propofol is associated with a higher incidence of tongue base collapse when compared with dexmedetomidine.48 Therefore, we used the TCI technique because it enables more stable sleep and the observation of more multilevel obstruction when compared with the conventional bolus technique.29 Furthermore, DISE provides only an intraluminal view. If the skeletal framework is not demonstrated, identifying the real cause of upper airway obstruction is challenging. In addition, without an intraoral view, tongue palate interaction is difficult to determine.39 Finally, most of our study cohort had severe velar collapse characterized by CCC pattern and most of them had residual AP collapse postoperatively. Therefore, it is possible that further treatment of the velar level may be needed by using revision palatopharyngoplasty or transpalatal advancement surgery.
In addition to the limitations associated with DISE, another limitation is that only AHI and SaO2 were reported as surgical outcomes. The oxygen desaturation index (ODI), percentage of total sleep time spent with SaO2 < 90% (T90), Epworth Sleepiness Scale (ESS) and blood indicators were not available for all patients. Indicators related to central obesity, such as neck circumference and waist-to-hip ratio, were not available for all participants either in the research. Considering these limitations, additional studies with larger samples and more comprehensive data must be conducted on changes in DISE patterns after single or multilevel surgical procedures.
Conclusion
Palatopharyngoplasty could change the collapse pattern at the velum in most patients with moderate to severe OSA. Preoperative and postoperative complete tongue base collapse and postoperative velar collapse identified in TCI-DISE were associated with relatively poor outcomes. Tongue base procedures or revision palatopharyngoplasty should be considered in patients with such findings.
Acknowledgments
The authors would like to thank the anonymous reviewers and editors for their comments.
Funding
This study was supported by grants from Shin Kong Wu-Ho-Su Memorial Hospital (2017SKHADR016). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. No additional external funding was received for this study.
Disclosure
The authors declare no conflicts of interest.
References
1. Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687–698. doi:10.1016/S2213-2600(19)30198-5
2. Engleman HM, Douglas NJ. Sleep. 4: sleepiness, cognitive function, and quality of life in obstructive sleep apnoea/hypopnoea syndrome. Thorax. 2004;59(7):618–622. doi:10.1136/thx.2003.015867
3. Gami AS, Olson EJ, Shen WK, et al. Obstructive sleep apnea and the risk of sudden cardiac death: a longitudinal study of 10,701 adults. J Am Coll Cardiol. 2013;62(7):610–616. doi:10.1016/j.jacc.2013.04.080
4. Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342(19):1378–1384. doi:10.1056/NEJM200005113421901
5. Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353(19):2034–2041. doi:10.1056/NEJMoa043104
6. Reichmuth KJ, Austin D, Skatrud JB, Young T. Association of sleep apnea and type II diabetes: a population-based study. Am J Respir Crit Care Med. 2005;172(12):1590–1595. doi:10.1164/rccm.200504-637OC
7. Kushida CA, Littner MR, Hirshkowitz M, et al. Practice parameters for the use of continuous and bilevel positive airway pressure devices to treat adult patients with sleep-related breathing disorders. Sleep. 2006;29(3):375–380. doi:10.1093/sleep/29.3.375
8. Kohler M, Smith D, Tippett V, Stradling JR. Predictors of long-term compliance with continuous positive airway pressure. Thorax. 2010;65(9):829–832. doi:10.1136/thx.2010.135848
9. Stuck BA, Ravesloot MJL, Eschenhagen T, de Vet HCW, Sommer JU. Uvulopalatopharyngoplasty with or without tonsillectomy in the treatment of adult obstructive sleep apnea - A systematic review. Sleep Med. 2018;50:152–165. doi:10.1016/j.sleep.2018.05.004
10. He M, Yin G, Zhan S, et al. Long-term efficacy of uvulopalatopharyngoplasty among adult patients with obstructive sleep apnea: a systematic review and meta-analysis. Otolaryngol Head Neck Surg. 2019;161(3):401–411. doi:10.1177/0194599819840356
11. Hsu YS, Hsu WC, Ko JY, Yeh TH, Lee CH, Kang KT. Readmission after adult uvulopalatopharyngoplasty: a population-based inpatient cohort study in Taiwan. Otolaryngol Head Neck Surg. 2019;160(3):559–566. doi:10.1177/0194599818813337
12. Cahali MB. Lateral pharyngoplasty: a new treatment for obstructive sleep apnea hypopnea syndrome. Laryngoscope. 2003;113(11):1961–1968. doi:10.1097/00005537-200311000-00020
13. Pang K, Woodson B. Expansion sphincter pharyngoplasty: a new technique for the treatment of obstructive sleep apnea. Otolaryngol Head Neck Surg. 2007;137(1):110–114. doi:10.1016/j.otohns.2007.03.014
14. Vicini C, Hendawy E, Campanini A, et al. Barbed reposition pharyngoplasty (BRP) for OSAHS: a feasibility, safety, efficacy and teachability pilot study. “We are on the giant’s shoulders. Eur Arch Otorhinolaryngol. 2015;272(10):3065–3070. doi:10.1007/s00405-015-3628-3
15. Li HY, Lee LA, Kezirian EJ, Nakayama M. Suspension palatoplasty for obstructive sleep apnea- a preliminary study. Sci Rep. 2018;8(1):4224. doi:10.1038/s41598-018-22710-1
16. Jones LM, Guillory VL, Mair EA. Total nasopharyngeal stenosis: treatment with laser excision, nasopharyngeal obturators, and topical Mitomycin-c. Otolaryngol Neck Surg. 2005;133(5):795–798. doi:10.1016/j.otohns.2005.07.005
17. Elzayat S, El Sobki A, El Deeb ME, Moussa HH. Managing obstructive sleep apnea patients with CPAP failure with a novel Lateral Pharyngoplasty as a stand-alone procedure. Am J Otolaryngol. 2020;102500. doi:10.1016/j.amjoto.2020.102500
18. Croft CB, Pringle M. Sleep nasendoscopy: a technique of assessment in snoring and obstructive sleep apnoea. Clin Otolaryngol Allied Sci. 1991;16(5):504–509. doi:10.1111/j.1365-2273.1991.tb01050.x
19. Kezirian EJ. Drug-induced sleep endoscopy. Oper Tech Otolaryngol. 2006;17(4):230–232. doi:10.1016/j.otot.2006.10.005
20. Kezirian EJ, Hohenhorst W, de Vries N. Drug-induced sleep endoscopy: the VOTE classification. Eur Arch Otorhinolaryngol. 2011;268(8):1233–1236. doi:10.1007/s00405-011-1633-8
21. Blumen M, Bequignon E, Chabolle F. Drug-induced sleep endoscopy: a new gold standard for evaluating OSAS? Part II: results. Eur Ann Otorhinolaryngol Head Neck Dis. 2017;134(2):109–115. doi:10.1016/j.anorl.2016.12.004
22. Lin HC, Weaver EM, Lin HS, Friedman M. Multilevel obstructive sleep apnea surgery. Adv Otorhinolaryngol. 2017;80:109–115. doi:10.1159/000470879
23. Lin HY, Lin YC, Hsu YS, et al. Comparison of findings between clinical examinations and drug-induced sleep endoscopy in patients with obstructive sleep apnea syndrome. Int J Environ Res Public Health. 2020;17:6041. doi:10.3390/ijerph17176041
24. Blumen MB, Latournerie V, Bequignon E, Guillere L, Chabolle F. Are the obstruction sites visualized on drug-induced sleep endoscopy reliable? Sleep Breath. 2015;19(3):1021–1026. doi:10.1007/s11325-014-1107-5
25. Koutsourelakis I, Safiruddin F, Ravesloot M, Zakynthinos S, de Vries N. Surgery for obstructive sleep apnea: sleep endoscopy determinants of outcome. Laryngoscope. 2012;122(11):2587–2591. doi:10.1002/lary.23462
26. Soares D, Sinawe H, Folbe AJ, et al. Lateral oropharyngeal wall and supraglottic airway collapse associated with failure in sleep apnea surgery. Laryngoscope. 2012;122(2):473–479. doi:10.1002/lary.22474
27. Meraj TS, Muenz DG, Glazer TA, Harvey RS, Spector ME, Hoff PT. Does drug-induced sleep endoscopy predict surgical success in transoral robotic multilevel surgery in obstructive sleep apnea? Laryngoscope. 2017;127(4):971–976. doi:10.1002/lary.26255
28. Hsu YS, Jacobowitz O. Does sleep endoscopy staging pattern correlate with outcome of advanced palatopharyngoplasty for moderate to severe obstructive sleep apnea? J Clin Sleep Med. 2017;13(10):1137–1144. doi:10.5664/jcsm.6756
29. De Vito A, Agnoletti V, Berrettini S, et al. Drug-induced sleep endoscopy: conventional versus target controlled infusion techniques—a randomized controlled study. Eur Arch Otorhinolaryngol. 2011;268(3):457–462. doi:10.1007/s00405-010-1376-y
30. De Vito A, Agnoletti V, Zani G, et al. The importance of drug-induced sedation endoscopy (D.I.S.E.) techniques in surgical decision making: conventional versus target controlled infusion techniques-a prospective randomized controlled study and a retrospective surgical outcomes analysis. Eur Arch Otorhinolaryngol. 2017;274(5):2307–2317. doi:10.1007/s00405-016-4447-x
31. Berry RB, Budhiraja R, Gottlieb DJ, et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events. Deliberations of the sleep apnea definitions task force of the American academy of sleep medicine. J Clin Sleep Med. 2012;8(5):597–619. doi:10.5664/jcsm.2172
32. Struys MMRF, Sahinovic M, Lichtenbelt BJ, Vereecke HEM, Absalom AR. Optimizing intravenous drug administration by applying pharmacokinetic/pharmacodynamic concepts. Br J Anaesth. 2011;107(1):38–47. doi:10.1093/bja/aer108
33. Kotecha B, De Vito A. Drug induced sleep endoscopy: its role in evaluation of the upper airway obstruction and patient selection for surgical and non-surgical treatment. J Thorac Dis. 2018;10(Suppl 1):S40–S47. doi:10.21037/jtd.2017.10.32
34. Hohenhorst W, Ravesloot MJL, Kezirian EJ, de Vries N. Drug-induced sleep endoscopy in adults with sleep-disordered breathing: technique and the VOTE Classification system. Oper Tech Otolaryngol Head Neck Surg. 2012;23(1):11–18. doi:10.1016/j.otot.2011.06.001
35. Mangiafico S. Summary and Analysis of Extension Program Evaluation in R, Version 1.18.1. New Brunswick, NJ: Rutgers Cooperative Extension; 2016.
36. Hasselbacher K, Seitz A, Abrams N, Wollenberg B, Steffen A. Complete concentric collapse at the soft palate in sleep endoscopy: what change is possible after UPPP in patients with CPAP failure? Sleep Breath. 2018;22(4):933–938. doi:10.1007/s11325-018-1657-z
37. Liu SYC, Hutz MJ, Poomkonsarn S, Chang CP, Awad M, Capasso R. Palatopharyngoplasty resolves concentric collapse in patients ineligible for upper airway stimulation. Laryngoscope. 2020. doi:10.1002/lary.28595
38. Vanderveken OM, Maurer JT, Hohenhorst W, et al. Evaluation of drug-induced sleep endoscopy as a patient selection tool for implanted upper airway stimulation for obstructive sleep apnea. J Clin Sleep Med. 2013. doi:10.5664/jcsm.2658
39. Li HY, Lo YL, Wang CJ, et al. Dynamic drug-induced sleep computed tomography in adults with obstructive sleep apnea. Sci Rep. 2016;6:35849. doi:10.1038/srep35849
40. Vroegop AV, Vanderveken OM, Boudewyns AN, et al. Drug-induced sleep endoscopy in sleep-disordered breathing: report on 1249 cases. Laryngoscope. 2014;124(3):797–802. doi:10.1002/lary.24479
41. Chiu FH, Chen CY, Lee JC, Hsu YS. Effect of modified uvulopalatopharyngoplasty without tonsillectomy on obstructive sleep apnea: polysomnographic outcome and correlation with drug-induced sleep endoscopy. Nat Sci Sleep. 2021;13:11–19. doi:10.2147/NSS.S286203
42. Ravesloot MJL, de Vries N. One hundred consecutive patients undergoing drug-induced sleep endoscopy: results and evaluation. Laryngoscope. 2011;121(12):2710–2716. doi:10.1002/lary.22369
43. Hsu YS, Hsu WC, Ko JY, Yeh TH, Lee CH, Kang KT. Incidence of multilevel surgical procedures and readmissions in uvulopalatopharyngoplasty in Taiwan. JAMA Otolaryngol Head Neck Surg. 2019. doi:10.1001/jamaoto.2019.1656
44. Ong AA, Murphey AW, Nguyen SA, et al. Efficacy of upper airway stimulation on collapse patterns observed during drug-induced sedation endoscopy. Otolaryngol Head Neck Surg. 2016;154(5):970–977. doi:10.1177/0194599816636835
45. Rabelo FAW, Küpper DS, Sander HH, Fernandes RMF, Valera FCP. Polysomnographic evaluation of propofol-induced sleep in patients with respiratory sleep disorders and controls. Laryngoscope. 2013;123(9):2300–2305. doi:10.1002/lary.23664
46. Hong SD, Dhong H-J, Kim HY, et al. Change of obstruction level during drug-induced sleep endoscopy according to sedation depth in obstructive sleep apnea. Laryngoscope. 2013;123(11):2896–2899. doi:10.1002/lary.24045
47. Carrasco Llatas M, Zerpa Zerpa V, Dalmau Galofre J. Reliability of drug-induced sedation endoscopy: interobserver agreement. Sleep Breath. 2017;21(1):173–179. doi:10.1007/s11325-016-1426-9
48. Capasso R, Rosa T, Tsou DYA, et al. Variable findings for drug-induced sleep endoscopy in obstructive sleep apnea with propofol versus dexmedetomidine. Otolaryngol Head Neck Surg. 2016;154(4):765–770. doi:10.1177/0194599815625972
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.