")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
Post hoc analyses of asenapine treatment in pediatric patients with bipolar I disorder: efficacy related to mixed or manic episode, stage of illness, and body weight
Authors Findling RL , Earley W, Suppes T, Patel M , Wu X, Chang CT, McIntyre RS
Received 16 February 2018
Accepted for publication 6 June 2018
Published 2 August 2018 Volume 2018:14 Pages 1941—1952
DOI https://doi.org/10.2147/NDT.S165743
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Robert L Findling,1 Willie Earley,2 Trisha Suppes,3,4 Mehul Patel,2 Xiao Wu,2 Cheng-Tao Chang,2 Roger S McIntyre5
1Johns Hopkins University and the Kennedy Krieger Institute, Baltimore, MD, USA; 2Allergan, Madison, NJ, USA; 3VA Palo Alto Health Care System, Palo Alto, CA, USA; 4Department of Psychiatry and Behavioral Sciences, Stanford University School of Medicine, Stanford, CA, USA; 5Toronto Western Research Institute, Toronto, ON, Canada
Background: Patient characteristics and disease progression may affect response to pharmacologic intervention in bipolar I disorder. Asenapine is approved for acute treatment of manic/mixed episodes of bipolar I disorder in patients 10–17 years old. Post hoc analyses assessed asenapine efficacy in pediatric patients by current manic or mixed episode, number of lifetime episodes, and baseline body mass index (BMI).
Patients and methods: Data were obtained from a 3-week, randomized, double-blind, placebo-controlled, parallel-group trial of asenapine 2.5, 5.0, or 10.0 mg twice daily (BID) in male or female patients (10–17 years) with bipolar I disorder (NCT01244815). Patients were stratified by current episode type (Diagnostic and Statistical Manual of Mental Disorders, fourth edition – defined mixed/manic), number of lifetime episodes (<3, 3–5, >5), and baseline BMI tertile. Changes from baseline to day 21 in Young Mania Rating Scale (YMRS) total score and Clinical Global Impressions Scale for use in Bipolar Illness (CGI-BP) were assessed in asenapine subgroups vs placebo.
Results: In patients with mixed episodes, differences in YMRS and CGI-BP scores were statistically significant for each asenapine dose vs placebo (P<0.001) at day 21; in patients with manic episodes, significant differences vs placebo were seen in all groups (P<0.05) except 2.5 mg BID on the YMRS. In patients with <3 previous mixed/manic episodes, significant differences in YMRS and CGI-BP scores were observed for all asenapine doses vs placebo (P<0.05). In patients with 3–5 or >5 previous episodes, asenapine 10 mg BID was significantly different than placebo (P<0.05) on both scales; differences vs placebo varied for lower doses. Baseline body weight or BMI did not appear to influence the efficacy of asenapine.
Conclusion: Asenapine was effective in the treatment of pediatric patients with bipolar I disorder. Efficacy did not appear to be influenced by the type of current episode, stage of disease progression, or baseline body weight/BMI.
Keywords: asenapine, child, adolescent, bipolar disorder, atypical antipsychotic, second-generation antipsychotic
Introduction
Onset of bipolar disorder in childhood and adolescence is common, with large retrospective studies estimating that between 50% and 66% of adults had onset of bipolar illness before the age of 19; even earlier onset of illness (before the age of 13) was reported for 15%–28% of adults.1,2 Early onset of illness and delay to first pharmacologic treatment are associated with high levels of dysfunction, decreased quality of life, and poor overall outcomes as patients mature.3–5 Monotherapy with an atypical antipsychotic or a mood stabilizer, such as lithium, is recommended as a first-line treatment for pediatric patients with bipolar mania.6 Given the wide range and dynamic nature of illness characteristics and body weight in children and adolescents, the possibility of tailoring the efficacy of antipsychotic treatment to individual patient characteristics is appealing.
Interest in factors associated with response to treatment in bipolar disorder increased with the discovery that the efficacy of lithium differed by baseline characteristics in adults.7,8 Evidence in adult patients suggests that worse treatment response may be related to factors such as more advanced disease progression, characterized by the number of previous mixed or manic episodes,9,10 and the type of current episode (mixed vs pure mania).11 Specifically, mixed states may be associated with worse outcomes and prognosis, including elevated relapse rates, suicide, comorbidity, and treatment resistance.12,13 However, in several subgroup analyses of atypical antipsychotics, no evidence of differential efficacy has been observed in groups defined by factors including sex, age, race, presenting syndromal characteristics, disease history, and comorbidity, with efficacy consistently being demonstrated in favor of drug vs placebo. Although evidence in support of differential efficacy for antipsychotics in adult patients with bipolar I mania may be confined to specific factors, characteristics that influence response to treatment in young patients have not been well studied14 and deserve to be investigated to enhance best practices in this developing and maturing patient population.
Asenapine is a sublingual atypical antipsychotic approved as monotherapy for the acute treatment of manic or mixed episodes associated with bipolar I disorder in pediatric patients aged 10–17 years. In a randomized, double-blind, placebo-controlled trial in pediatric patients with acute manic or mixed episodes associated with bipolar I disorder,15 asenapine 2.5, 5.0, and 10.0 mg twice daily (BID) were more effective than placebo on the Young Mania Rating Scale (YMRS)16 total score, Clinical Global Impressions Scale for use in Bipolar Illness (CGI-BP),17 and Children’s Global Assessment Scale (CGAS).18 Furthermore, differential efficacy based on several baseline characteristics was evaluated in patient subgroups defined by characteristics relevant to this patient population. Of note, asenapine was more effective than placebo in subgroups of patients with or without attention-deficit hyperactivity disorder (ADHD), with or without concomitant stimulant use, and without respect to age of onset (<11 years vs >11 years), or sex.
Although several pharmacologic treatment options for bipolar mania are available, efficacy varies in pediatric patients,19,20 with greater treatment resistance reported for young patients than for adult patients.14 To further characterize the efficacy profile of asenapine in pediatric patients, we conducted post hoc analyses to evaluate the efficacy of asenapine vs placebo in additional subgroups of pediatric patients from the prospective outcome study. Relevant to our interest in improving patient outcomes, we evaluated whether episode type (manic or mixed) or the stage of bipolar disorder (indicated by the number of previous mixed or manic episodes) affected the efficacy of asenapine in young patients. Additionally, as growth and development result in continuous changes that could influence drug effect in pediatric patients, we also conducted analyses in subgroups defined by the dynamic characteristics of weight and body mass index (BMI) to see if a weight-based dosing strategy could be beneficial for asenapine. Collectively with the prospective subgroup analyses, these results may provide a more complete clinical profile that could better inform clinicians about the efficacy of asenapine in pediatric patients.
Patients and methods
Study design
Data were obtained from the positive 3-week, randomized, double-blind, placebo-controlled, parallel-group trial of asenapine in pediatric patients with bipolar I disorder (NCT01244815). Detailed methods of the study have been published previously.15 Briefly, the trial included a 2- to 14-day screening/tapering period followed by a 21-day double-blind treatment period. Patients were randomized 1:1:1:1 to sublingual placebo or asenapine 2.5, 5.0, and 10.0 mg BID. Asenapine doses were up-titrated during the first week for patients in the 5.0 and 10.0 mg BID treatment groups. The primary and key secondary efficacy parameters were change from baseline to day 21 in YMRS total score and CGI-BP assessed at screening, baseline, and on days 4, 7, 14, and 21. Additional secondary parameters included the CGAS (screening, baseline, and day 21) and the Children’s Depressive Rating Scale-Revised (CDRS-R)21 (baseline and days 7, 14, and 21). The trial was conducted in accordance with Good Clinical Practice standards and applicable country and/or local statutes regarding ethical committee review, informed consent, and protection of human subjects participating in biomedical research. Independent ethics committees (listed in Supplementary material) reviewed and approved the protocol and applicable amendments; written informed consent and subject assent were obtained at screening, and additional informed consent was signed if a participant turned 18 years old during the trial.
Patients
Male and female pediatric patients (10–17 years, inclusive) with a primary diagnosis of bipolar I disorder according to the Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (DSM-IV-TR)22 and a current manic (296.4x) or mixed (296.6x) episode with or without psychotic features were included. The diagnosis was confirmed by the Schedule for Affective Disorders and Schizophrenia for School-Aged Children-Present and Lifetime Version.23 The clinical measures required for inclusion were YMRS total score ≥20 and CGI-BP overall score ≥4. Additionally, patients were required to have at least one mania-specific symptom (ie, elation, grandiosity, flight of ideas/racing thoughts, decreased need for sleep, hypersexuality). Criteria for exclusion were typical of clinical studies in pediatric patients with bipolar disorder and included the presence of a pervasive development disorder, schizophrenia, schizoaffective disorder, posttraumatic stress disorder, obsessive-compulsive disorder, or psychosis due to a medical condition or prohibited concomitant medication. The presence of an uncontrolled, unstable, clinically significant medical condition was also exclusionary. Some concomitant medications were allowed during the study, including agents for agitation, irritability, restlessness, insomnia, and hostility (short-acting benzodiazepines such as lorazepam), ADHD (atomoxetine, methylphenidate, amphetamine, guanfacine), extrapyramidal symptoms (anticholinergics and short-acting benzodiazepines), and hormonal birth control.
Post hoc analyses
Post hoc analyses were conducted to evaluate the relationship between efficacy and the type of current episode (mixed or manic), number of previous mixed or manic episodes (<3, 3–5, or >5), and baseline body weight and BMI stratified by tertile. We hypothesized that asenapine would be effective vs placebo regardless of episode type (manic or mixed), the number of previous manic or mixed episodes, and baseline BMI in pediatric patients. The primary and secondary efficacy parameters from the clinical study (YMRS total score and CGI-BP overall score) were used as the measures for post hoc evaluation of patient subgroups. The all-patients-as-treated set consisted of all randomized patients who received at least one dose of study medication. All patients who received at least one dose of study drug and had a baseline and at least one postbaseline efficacy assessment were included in the analyses (full analysis set).
Change from baseline to day 21 in YMRS total score and CGI-BP score was analyzed for each asenapine dose (2.5, 5.0, and 10 mg BID) vs placebo in the patient subgroups. Analyses were conducted using a mixed model for repeated measures (MMRM) for change from baseline values. The model for subgroup analyses by episode type and previous number of episodes included pooled site, treatment, visit, and treatment-by-visit interaction as factors, and baseline, episode group, baseline-by-visit interaction, treatment-by-episode group interaction, and treatment-by-episode group-by-visit as covariates. The model for subgroup analyses by BMI included pooled site, treatment, visit, and treatment-by-visit interaction as factors, and baseline, baseline-by-visit interaction, age, BMI, and treatment-by-BMI as covariates. Unstructured matrix was assumed for the repeated-measures variance–covariance and the model parameters were estimated using restricted maximum likelihood. In addition to analyses of efficacy within baseline BMI subgroups, the relationship between efficacy and baseline body weight, BMI, or BMI percentile was assessed by including the following continuous variables in separate MMRM models as covariates: 1) age, sex, baseline body weight, and the body weight-by-treatment interaction; 2) BMI, age, sex, and the BMI-by-treatment interaction; and 3) BMI percentile (for age and sex) and the BMI percentile interaction-by-treatment. Statistical tests were two-sided and conducted at the 0.05 level of significance.
Results
A total of 403 patients were randomized and treated in the trial. Detailed demographic information has been previously published;15 patient populations and baseline characteristics that are relevant to our post hoc analyses are presented in Table 1. The majority of patients (68.2%) were white with a mean age of 13.8 years. The percentage of females in each treatment group varied from 62 for the placebo group to 41 for the asenapine 10.0 mg BID group. The overall mean (SD) age of onset of bipolar I disorder was 11.0 (2.9) years. Based on standardized medical and psychiatric history intake questionnaires at screening, the most common comorbid Axis I disorder was ADHD, which was reported in 54.6% of patients overall. Baseline YMRS total and CGI-BP scores were similar between treatment groups (Table 1).
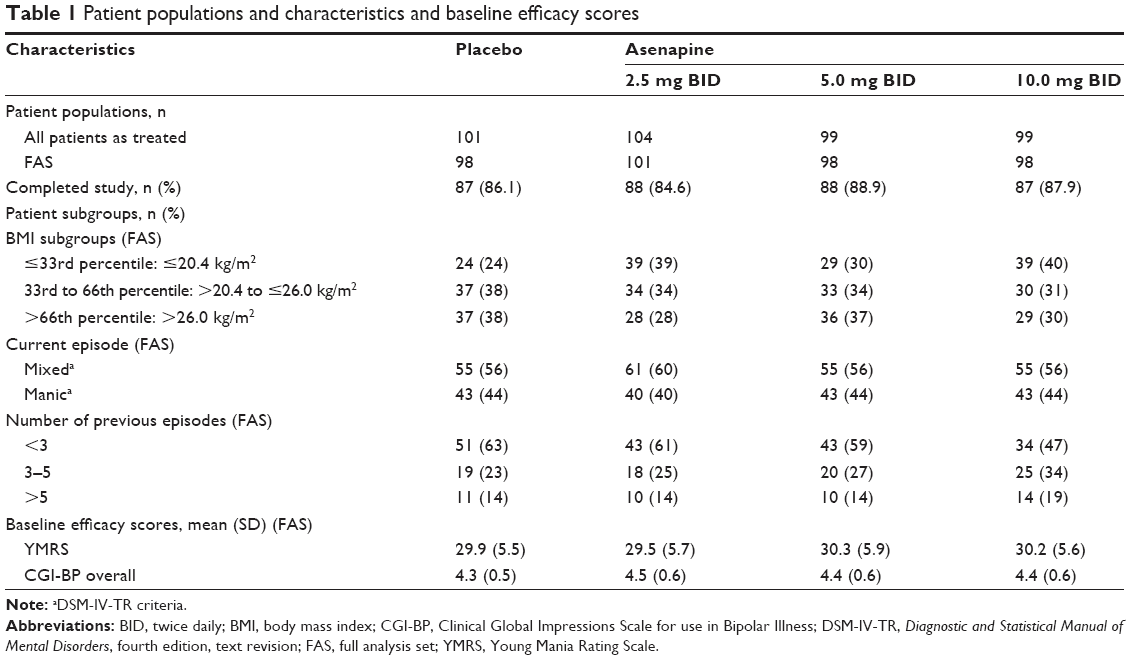 | Table 1 Patient populations and characteristics and baseline efficacy scores |
In prespecified analyses from the clinical study,15 the least squares mean difference (LSMD) in change from baseline to day 21 was statistically significant in favor of all asenapine doses vs placebo in YMRS total score (2.5 mg BID, −3.2; 5.0 mg BID, −5.3; 10.0 mg BID, −6.2; all P<0.01 [adjusted]), CGI-BP overall score (2.5 mg BID, −0.6; 5.0 mg BID, −0.7; 10.0 mg BID, −0.7; all P<0.001 [adjusted]), and CGAS total score (2.5 mg BID, 4.3; 5.0 mg BID, 7.0; 10.0 mg BID, 5.1; all P<0.01). The LSMD for asenapine vs placebo on the CDRS-R at day 21 was only statistically significant for the 5.0 mg BID dose group (−2.2, P<0.05).
Post hoc efficacy outcomes
Efficacy by type of current episode (mixed or manic)
Baseline YMRS total scores were generally similar in patients with a current manic vs mixed episode (placebo, 29.4 vs 30.3; asenapine 2.5–10.0 mg BID, 30.6–31.3 vs 28.8–29.8). Baseline CGI-BP scores were also similar in patients with a current manic vs mixed episode (placebo, 4.4 vs 4.3; asenapine 2.5–10.0 mg BID, 4.4–4.6 vs 4.3–4.4). At baseline, 58% of patients overall were diagnosed with a current mixed episode according to DSM-IV-TR criteria. In patients currently experiencing a mixed episode, differences in total score change on the YMRS and CGI-BP were significantly greater for each asenapine dose group (2.5, 5.0, and 10.0 mg BID) compared to placebo, starting on day 7 and continuing to day 21 (Figure 1A and B). In patients currently experiencing a manic episode, the difference in YMRS total score was statistically significant in favor of asenapine 5.0 and 10.0 mg BID vs placebo starting at day 14; no statistically significant difference from placebo was observed on the YMRS for patients with a current manic episode in the asenapine 2.5 mg BID group (Figure 1C). In patients experiencing a manic episode, the difference in CGI-BP overall scores was statistically significant for all asenapine doses vs placebo at day 21 (Figure 1D).
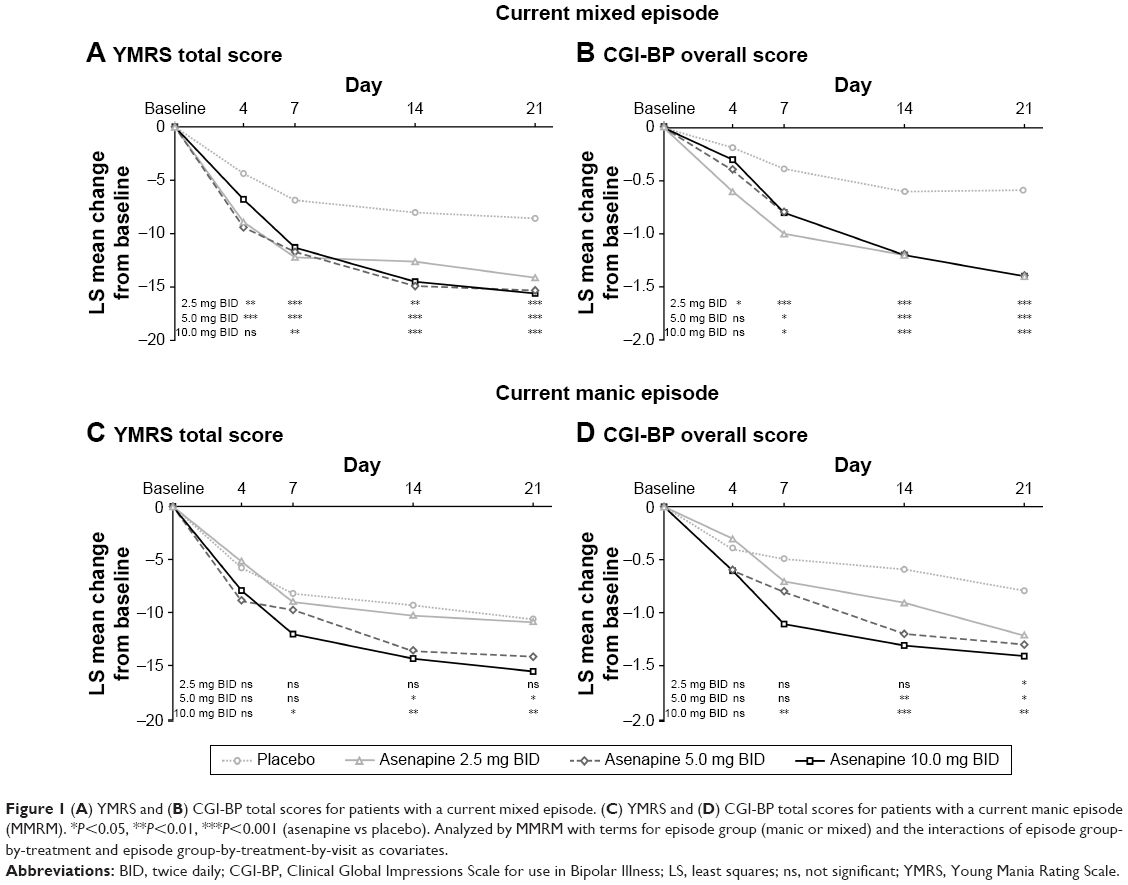 | Figure 1 (A) YMRS and (B) CGI-BP total scores for patients with a current mixed episode. (C) YMRS and (D) CGI-BP total scores for patients with a current manic episode (MMRM). *P<0.05, **P<0.01, ***P<0.001 (asenapine vs placebo). Analyzed by MMRM with terms for episode group (manic or mixed) and the interactions of episode group-by-treatment and episode group-by-treatment-by-visit as covariates. |
Efficacy by number of previous episodes
The majority of patients experienced <3 previous manic or mixed episodes (Table 1). The LSMD in YMRS total score change was significantly different for all asenapine doses vs placebo in patients with <3 prior episodes (2.5 mg BID, −3.8; 5.0 mg BID, −3.9; 10.0 mg BID, −4.7 [P<0.05 for all doses]). In patients with 3–5 prior episodes, the LSMD vs placebo was significant for patients in the asenapine 5.0 and 10.0 mg BID dose groups (5.0 mg BID, −10.2; 10.0 mg BID, −7.7 [P<0.01 for both doses]); in patients with >5 prior episodes, the LSMD vs placebo was significant for the 2.5 and 10.0 mg BID dose groups (2.5 mg BID, −8.4; 10.0 mg BID, −11.6 [P<0.05 for both doses]; Figure 2A).
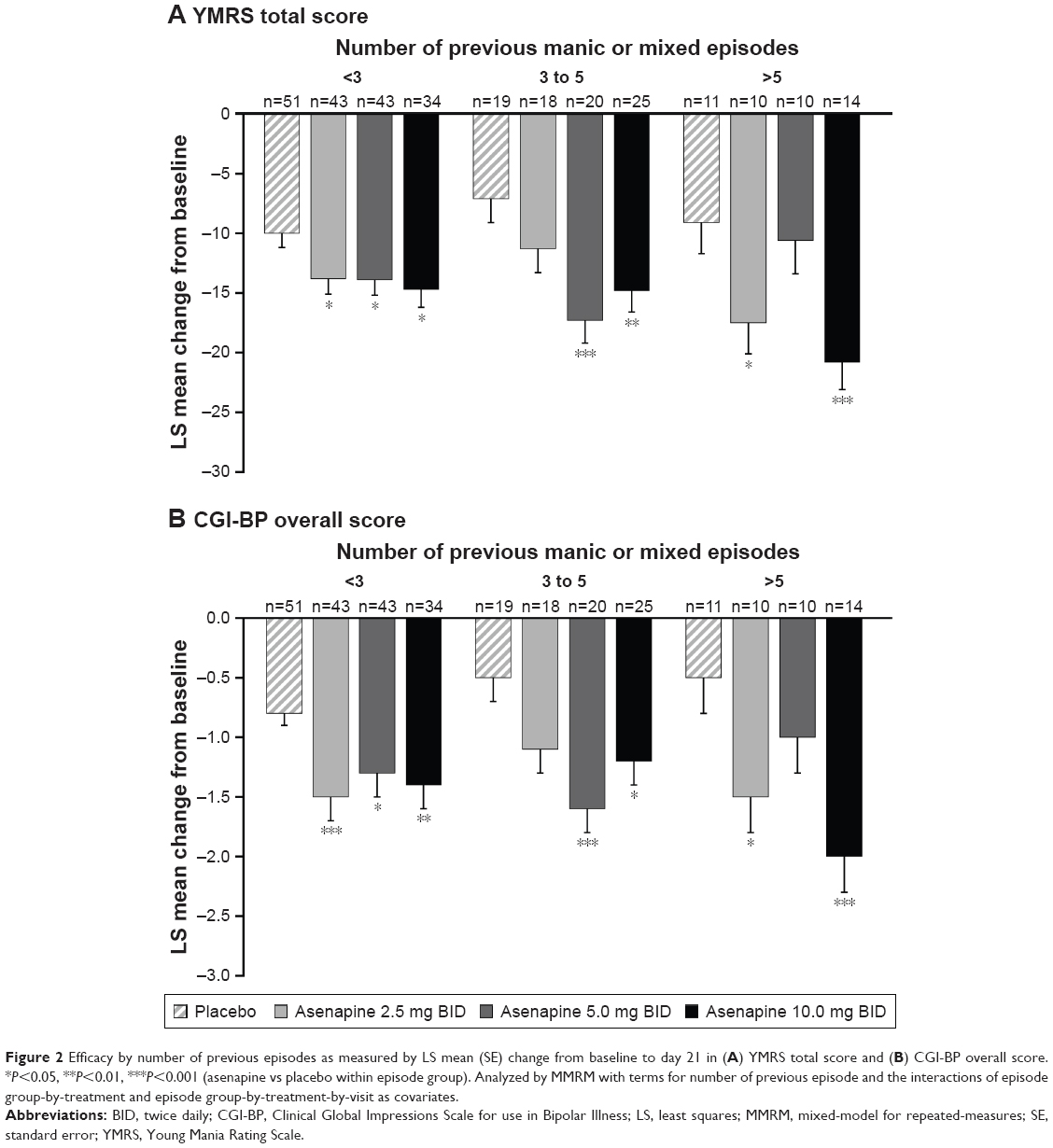 | Figure 2 Efficacy by number of previous episodes as measured by LS mean (SE) change from baseline to day 21 in (A) YMRS total score and (B) CGI-BP overall score. *P<0.05, **P<0.01, ***P<0.001 (asenapine vs placebo within episode group). Analyzed by MMRM with terms for number of previous episode and the interactions of episode group-by-treatment and episode group-by-treatment-by-visit as covariates. |
At day 21, the LSMDs were statistically significant in favor of asenapine vs placebo for change from baseline in CGI-BP overall score for all doses in pediatric patients with <3 prior episodes (2.5 mg BID, −0.7; 5.0 mg BID, −0.5; 10.0 mg BID, −0.6 [P<0.05 all doses]), for the two higher doses in patients with 3–5 prior episodes (5.0 mg BID, −1.1; 10.0 mg BID, −0.7 [P<0.05 for both doses]), and for the 2.5 and 10.0 mg BID in those with >5 prior episodes (2.5 mg BID, −1.0; 10.0 mg BID, −1.5 [P<0.05 for both doses]; Figure 2B).
Efficacy by baseline BMI
When results were stratified by baseline BMI, LS mean changes in YMRS total score significantly favored all asenapine doses within the middle tertile and the highest doses of asenapine within the highest tertile (Figure 3A). LS mean changes in CGI-BP score significantly favored all asenapine doses within the middle tertile (Figure 3B). Overall, however, no systematic patterns across BMI strata were evident.
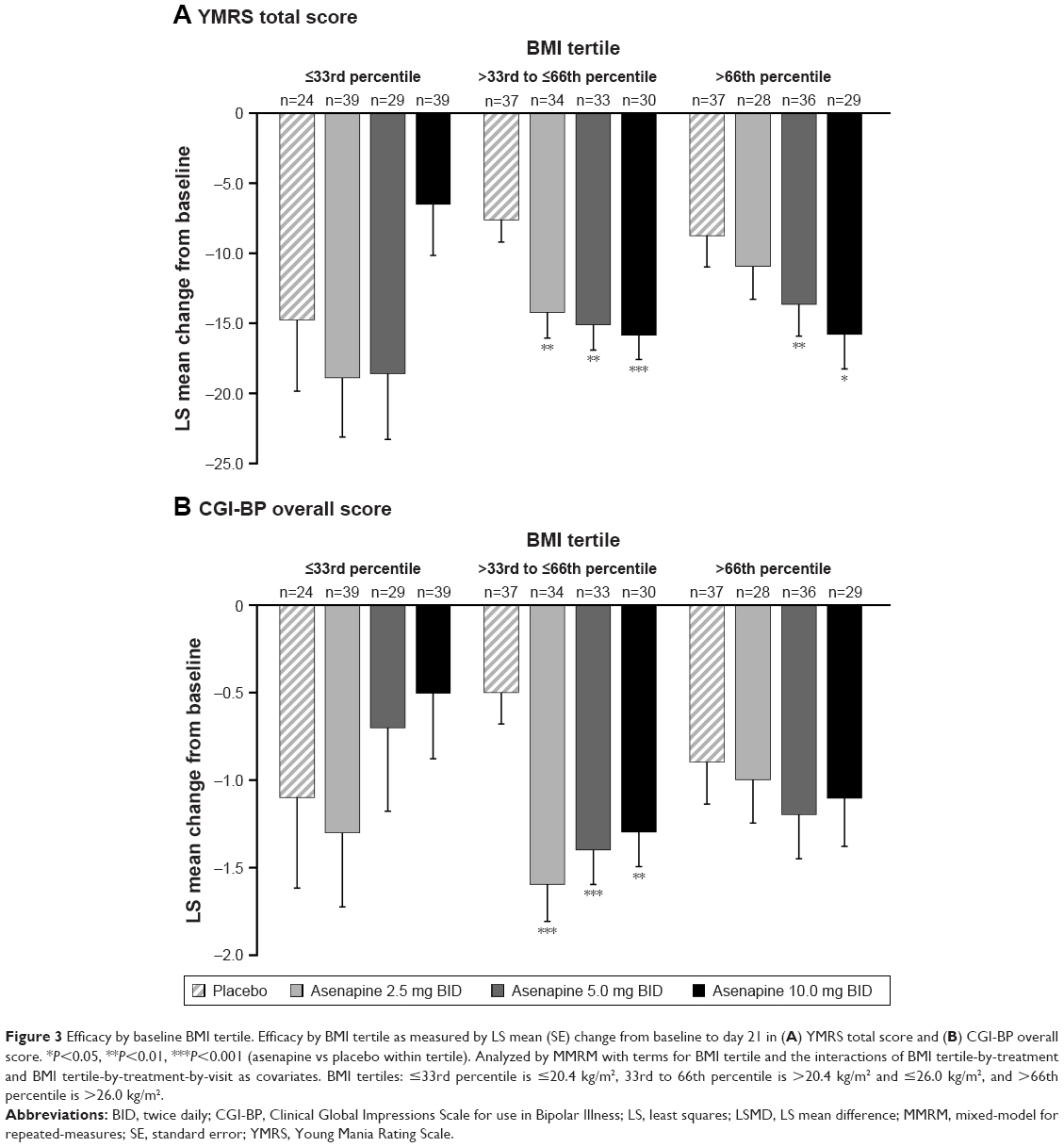 | Figure 3 Efficacy by baseline BMI tertile. Efficacy by BMI tertile as measured by LS mean (SE) change from baseline to day 21 in (A) YMRS total score and (B) CGI-BP overall score. *P<0.05, **P<0.01, ***P<0.001 (asenapine vs placebo within tertile). Analyzed by MMRM with terms for BMI tertile and the interactions of BMI tertile-by-treatment and BMI tertile-by-treatment-by-visit as covariates. BMI tertiles: ≤33rd percentile is ≤20.4 kg/m2, 33rd to 66th percentile is >20.4 kg/m2 and ≤26.0 kg/m2, and >66th percentile is >26.0 kg/m2. |
In analyses using continuous variables instead of subgroups, there were no statistically significant effects on efficacy for the continuous variables of baseline body weight, BMI, BMI percentile, or the interactions of dose with these variables (P>0.10 in all cases).
Discussion
In these post hoc analyses, consistent efficacy was noted for asenapine vs placebo in the treatment of pediatric patients with bipolar I disorder regardless of the type of episode (mixed or manic) or the number of previous episodes. In patients experiencing a mixed episode, changes in YMRS and CGI-BP total score were significantly greater for each asenapine dose group compared to placebo starting on day 7 and continuing to day 21. In patients experiencing a current manic episode, the difference in YMRS total score was statistically significant in favor of asenapine 5.0 and 10.0 mg BID vs placebo starting at day 14, but no significant difference from placebo was observed in the asenapine 2.5 mg BID group, suggesting that higher asenapine doses may be the most beneficial in patients with solely manic symptoms. Significant improvement vs placebo in CGI-BP overall scores was also seen for all asenapine doses at day 21 in patients with a current manic episode.
Additionally, when efficacy by number of prior manic or mixed episodes was evaluated, significantly greater changes in YMRS total score and CGI-BP overall score, indicating symptomatic and global improvement, were seen for all asenapine doses vs placebo in patients with <3 prior episodes. Data were less consistent in patients with ≥3 prior mixed or manic episodes, which may have been due to small sample sizes in these subgroups. In patients with 3–5 prior episodes, change in YMRS total score and CGI-BP overall score was significantly greater for asenapine 5.0 and 10.0 mg BID than for placebo, but in patients with >5 prior episodes, YMRS total score and CGI-BP overall score changes were significantly greater than placebo for asenapine 2.5 and 10.0 mg BID.
Differential efficacy for antipsychotics in patients with manic vs mixed episodes has been attributed to the presence of depressive features instead of pure mania.11 Our results suggest that asenapine may be an appropriate treatment option for pediatric patients with either manic or mixed episodes, which is consistent with previous efficacy findings in favor of asenapine vs placebo in adult patients with acute manic or mixed episodes.24–26 Of additional interest for asenapine, the presence of depressive symptoms in adult patients with mixed mania did not appear to predict inferior efficacy. In a pooled post hoc analysis of two studies in adults, asenapine was compared with placebo in patients with acute manic or mixed episodes who also met proxy criteria for a moderate-to-severe mixed major depressive episode; olanzapine was used as an active comparator in these studies.24 Asenapine- vs placebo-treated patients had significant improvement in both manic and depressive symptoms as shown by change from baseline in YMRS total score and Montgomery–Åsberg Depression Rating Scale (MADRS) total score;27 no significant differences in manic or depressive symptoms were observed for olanzapine vs placebo in patients meeting mixed criteria.
Improvement in depressive symptoms with asenapine was supported in another pooled post hoc analysis showing significant differences in MADRS total score in favor of asenapine over placebo in adult patients experiencing an acute bipolar manic or mixed episode with clinically relevant depressive symptoms.26 Finally, asenapine findings of efficacy in mixed episodes are in accordance with a meta-analysis investigating second-generation antipsychotic efficacy in the treatment of acute mixed episodes in adult patients with bipolar disorder.28 Antipsychotic monotherapy was significantly more effective than placebo in treating acute mixed episodes, with effect sizes for mixed episodes (0.44) and pure manic episodes (0.56) both in the medium range, suggesting efficacy for these agents in both mixed and manic episodes. Although these findings pertain to adult patients and asenapine is not approved for the treatment of bipolar depression, these results support the effects of asenapine in patients with mixed affective symptoms and may be instructive for clinicians treating mixed affective symptoms in pediatric patients.
Illness progression, defined in our analyses as the number of previous episodes, has also been related to differential efficacy in patients with bipolar mania. Decreased antimanic response to lithium has been noted in association with an increasing number of manic episodes,9 with parallel results observed with at least one atypical antipsychotic. In a pooled analysis that included mania studies with olanzapine in adults, data from individuals categorized as having had 0, 1–5, 6–10, or >10 prior episodes of illness were analyzed.10 Response rates ranged from 52% to 69% for individuals with 1 to 5 previous manic episodes, and from 29% to 59% for individuals with >5 previous episodes. The rate of response was significantly higher for the 1–5 episode group compared to the >5 episode group, with an up to twofold increase in the chance of responding for those with fewer previous episodes.
Alternatively, in pediatric patients in our subgroup analyses, efficacy for asenapine vs placebo was observed at some dose levels regardless of the number of previous episodes. This is an important finding because bipolar disorder may not be immediately recognized and diagnosed in pediatric patients,29 and treatment may be commensurately delayed. In a retrospective review of youths treated in a community mental health outpatient clinic, the mean time from onset of symptoms to a diagnosis of bipolar disorder was 5 years,30 suggesting that delayed diagnosis may be common in pediatric patients with bipolar disorder and efficacy in cases with a greater number of previous episodes may be an important aspect of treatment.
In our post hoc analyses examining efficacy by baseline BMI, changes in YMRS total score were significantly greater for all asenapine doses in the middle BMI tertile (>33rd and ≤66th percentile) and for the highest dose of asenapine in the highest BMI tertile (>66th percentile); no dose was significantly different than placebo in the lowest BMI tertile (≤33rd percentile). Changes in CGI-BP score were also significantly greater for all asenapine doses in the middle BMI tertile, but no significant differences from placebo were noted for any dose in the low or high BMI tertiles. When weight characteristics were analyzed using continuous variables instead of subgroups, there were no statistically significant effects for baseline body weight, BMI, BMI percentile, or the interactions of dose with these variables. In pediatric patients where growth and development are often times changing, the impact of body weight on medication efficacy and safety is an important clinical consideration. As such, weight-based dosing is common in pediatric patients because pharmacokinetic parameters may be affected by several factors such as weight and BMI.31 Consistent with results from our post hoc analyses showing that asenapine was effective across BMI tertiles and irrespective of body weight, a previous population pharmacokinetics study of asenapine found no statistically significant differences or clinically meaningful changes in asenapine exposure when BMI was analyzed as a covariate in the model.32 Together, these findings indicate that no asenapine dose adjustments based on patient weight or BMI are required.
While there is research investigating efficacy and patient characteristics in adults with bipolar disorder, very few studies have investigated whether illness or patient factors are related to efficacy in mixed or manic episodes in young patients with bipolar disorder. A small naturalistic study in children and adolescents with manic or mixed episodes associated with bipolar disorder found that most of the evaluated clinical characteristics (eg, mean age, sex, inpatient vs outpatient, duration of follow-up, manic vs mixed index episode) did not differentiate treatment responders from nonresponders.14 However, the study did find that comorbidity with conduct disorder or ADHD, and higher baseline CGI-Severity score were predictors of nonresponse. This is an interesting finding given that there was a high rate of comorbid baseline ADHD in our pediatric population (55%) but no differences in efficacy were observed in asenapine-treated patients with or without ADHD.15 Collectively, prospective asenapine subgroup analyses in pediatric patients, in conjunction with our post hoc analyses, contribute to the literature on differential response in pediatric patients with bipolar I disorder. Namely, asenapine has been shown to be effective regardless of the type of episode (mixed or manic) and the level of disease progression, without regard to patient BMI and weight, in patients with and without ADHD and without concomitant stimulant use, and regardless of age of onset or sex.
Limitations
Limitations of our analyses include their post hoc nature and the short-term duration of the clinical study. Given the scope of these post hoc investigations, our analyses were limited to factors that we considered salient based on prior results in adult patients or of particular relevance in pediatric patients. As our analyses were exploratory, there is risk for both type I error (false positive findings) due to multiple comparisons and type II errors (false negative findings) due to the small sample size of the subgroups. Additionally, these results may not be generalizable to a wider population of child and adolescent patients with bipolar I disorder beyond the inclusion and exclusion criteria that were used in the clinical study. Finally, patients in the clinical trial were enrolled based on criteria described in the DSM-IV-TR; it is unknown whether efficacy by type of episode (mixed or manic) would have differed had mixed episodes been defined using DSM-V diagnostic criteria.
Conclusion
In these post hoc, exploratory analyses, asenapine 2.5, 5.0, and 10.0 mg BID were more effective than placebo in the treatment of pediatric patients with bipolar I disorder regardless of the type of episode (mixed or manic) or the number of previous mixed or manic episodes. Change from baseline in YMRS and CGI-BP total was significantly greater than placebo for at least one dose of asenapine in each patient subgroup that was evaluated by episode type (mixed or manic) and number of previous episodes; in most cases, multiple asenapine doses were more effective than placebo. Significant differences vs placebo on the YMRS and CGI-BP were not seen in all BMI subgroups; however, when all weight variables were considered, body weight did not appear to influence the efficacy of asenapine, obviating the need for weight-based dosing in this population. Due to small patient subgroup numbers and the vagaries of post hoc analysis, it was not possible to detect specific by-dose patterns of statistical significance vs placebo in most subgroups.
Acknowledgments
Writing assistance and editorial support were provided by Krystina Neuman, PhD, of Prescott Medical Communications Group (Chicago, IL), a contractor of Allergan. The study was sponsored by Merck & Co., Inc. This manuscript was supported by funding from Allergan (Madison, NJ).
Author contributions
Robert L Findling, Willie Earley, Trisha Suppes, Mehul Patel, and Roger S McIntyre contributed to the concept/design of these analyses and data analyses/interpretation. Xiao Wu and Cheng-Tao Chang were involved in the statistical analysis and interpretation of data. All authors contributed toward data analyses/interpretation, drafting and critically revising the paper, and they agree to be responsible for all aspects of the work.
Disclosure
Dr Findling receives or has received research support, acted as a consultant and/or served on a speaker’s bureau for Aevi, Akili, Alcobra, Amerex, American Academy of Child & Adolescent Psychiatry, American Psychiatric Press, Bracket, Epharma Solutions, Forest, Genentech, Guilford Press, Ironshore, Johns Hopkins University Press, KemPharm, Lundbeck, Merck, NIH, Neurim, Nuvelution, Otsuka, PCORI, Pfizer, Physicians Postgraduate Press, Purdue, Roche, Sage, Shire, Sunovion, Supernus Pharmaceuticals, Syneurx, Teva, Tris, TouchPoint, Validus, and WebMD.
Dr Suppes has reported grants from National Institute of Mental Health, VA Cooperative Studies Program, Pathway Genomics, Stanley Medical Research Institute, Elan Pharma International Limited, and Sunovion Pharmaceuticals; consulting fees from A/S H. Lundbeck, Sunovion, Merck & Co., and Astra Zeneca; honoraria from Medscape Education, Global Medical Education, and CMEology; royalties from Jones and Bartlett and UpToDate.
Dr McIntyre has received research grant support from Lundbeck, AstraZeneca, Pfizer, Shire, Otsuka, Bristol-Myers Squibb, National Institute of Mental Health, Stanley Medical Research Institute, Canadian Institutes for Health Research, and The Brain and Behavior Research Foundation. He has also received speaker/consultant fees from Lundbeck, Pfizer, AstraZeneca, Eli Lilly, Janssen Ortho, Sunovion, Takeda, Forest, Otsuka, Bristol-Myers Squibb, and Shire.
Drs Earley and Patel acknowledge potential conflicts of interest as employees of Allergan.
Drs Wu and Chang acknowledge potential conflicts of interest as former employees of Allergan.
The authors report no other conflicts of interest in this work.
References
Lewinsohn PM, Klein DN, Seeley JR. Bipolar disorder during adolescence and young adulthood in a community sample. Bipolar Disord. 2000;2(3 Pt 2):281–293. | ||
Post RM, Kowatch RA. The health care crisis of childhood-onset bipolar illness: some recommendations for its amelioration. J Clin Psychiatry. 2006;67(1):115–125. | ||
Birmaher B, Axelson D, Goldstein B, et al. Four-year longitudinal course of children and adolescents with bipolar spectrum disorders: the Course and Outcome of Bipolar Youth (COBY) study. Am J Psychiatry. 2009;166(7):795–804. | ||
Perlis RH, Dennehy EB, Miklowitz DJ, et al. Retrospective age at onset of bipolar disorder and outcome during two-year follow-up: results from the STEP-BD study. Bipolar Disord. 2009;11(4):391–400. | ||
Post RM, Leverich GS, Kupka RW, et al. Early-onset bipolar disorder and treatment delay are risk factors for poor outcome in adulthood. J Clin Psychiatry. 2010;71(7):864–872. | ||
Mcclellan J, Kowatch R, Findling RL; Work Group on Quality Issues. Practice parameter for the assessment and treatment of children and adolescents with bipolar disorder. J Am Acad Child Adolesc Psychiatry. 2007;46(1):107–125. | ||
Bowden CL. Clinical correlates of therapeutic response in bipolar disorder. J Affect Disord. 2001;67(1–3):257–265. | ||
Swann AC, Bowden CL, Calabrese JR, Dilsaver SC, Morris DD. Differential effect of number of previous episodes of affective disorder on response to lithium or divalproex in acute mania. Am J Psychiatry. 1999;156(8):1264–1266. | ||
Swann AC, Bowden CL, Calabrese JR, Dilsaver SC, Morris DD. Mania: differential effects of previous depressive and manic episodes on response to treatment. Acta Psychiatr Scand. 2000;101(6):444–451. | ||
Berk M, Brnabic A, Dodd S, et al. Does stage of illness impact treatment response in bipolar disorder? Empirical treatment data and their implication for the staging model and early intervention. Bipolar Disord. 2011;13(1):87–98. | ||
González-Pinto A, Aldama A, Mosquera F, González Gómez C, Epidemiology GGC. Epidemiology, diagnosis and management of mixed mania. CNS Drugs. 2007;21(8):611–626. | ||
Rosenblat JD, Mcintyre RS. Treatment of mixed features in bipolar disorder. CNS Spectr. 2017;22(2):141–146. | ||
Swann AC, Lafer B, Perugi G, et al. Bipolar mixed states: an international society for bipolar disorders task force report of symptom structure, course of illness, and diagnosis. Am J Psychiatry. 2013;170(1):31–42. | ||
Masi G, Perugi G, Toni C, et al. Predictors of treatment nonresponse in bipolar children and adolescents with manic or mixed episodes. J Child Adolesc Psychopharmacol. 2004;14(3):395–404. | ||
Findling RL, Landbloom RL, Szegedi A, et al. Asenapine for the Acute Treatment of Pediatric Manic or Mixed Episode of Bipolar I Disorder. J Am Acad Child Adolesc Psychiatry. 2015;54(12):1032–1041. | ||
Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry. 1978;133:429–435. | ||
Spearing MK, Post RM, Leverich GS, Brandt D, Nolen W. Modification of the Clinical Global Impressions (CGI) Scale for use in bipolar illness (BP): the CGI-BP. Psychiatry Res. 1997;73(3):159–171. | ||
Shaffer D, Gould MS, Brasic J, et al. A children’s global assessment scale (CGAS). Arch Gen Psychiatry. 1983;40(11):1228–1231. | ||
Correll CU, Sheridan EM, Delbello MP. Antipsychotic and mood stabilizer efficacy and tolerability in pediatric and adult patients with bipolar I mania: a comparative analysis of acute, randomized, placebo-controlled trials. Bipolar Disord. 2010;12(2):116–141. | ||
Liu HY, Potter MP, Woodworth KY, et al. Pharmacologic treatments for pediatric bipolar disorder: a review and meta-analysis. J Am Acad Child Adolesc Psychiatry. 2011;50(8):749–762.e39. | ||
Jain S, Carmody TJ, Trivedi MH, et al. A psychometric evaluation of the CDRS and MADRS in assessing depressive symptoms in children. J Am Acad Child Adolesc Psychiatry. 2007;46(9):1204–1212. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed, Text Revision. Washington, DC: American Psychiatric Association; 2000. | ||
Kaufman J, Birmaher B, Brent D, et al. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry. 1997;36(7):980–988. | ||
Berk M, Tiller JW, Zhao J, Yatham LN, Malhi GS, Weiller E. Effects of asenapine in bipolar I patients meeting proxy criteria for moderate-to-severe mixed major depressive episodes: a post hoc analysis. J Clin Psychiatry. 2015;76(6):728–734. | ||
Szegedi A, Durgam S, Mackle M, et al. Randomized, Double-Blind, Placebo-Controlled Trial of Asenapine Maintenance Therapy in Adults With an Acute Manic or Mixed Episode Associated With Bipolar I Disorder. Am J Psychiatry. 2018;175(1):71–79. | ||
Szegedi A, Zhao J, van Willigenburg A, Nations KR, Mackle M, Panagides J. Effects of asenapine on depressive symptoms in patients with bipolar I disorder experiencing acute manic or mixed episodes: a post hoc analysis of two 3-week clinical trials. BMC Psychiatry. 2011;11:101. | ||
Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. 1979;134:382–389. | ||
Muralidharan K, Ali M, Silveira LE, et al. Efficacy of second generation antipsychotics in treating acute mixed episodes in bipolar disorder: a meta-analysis of placebo-controlled trials. J Affect Disord. 2013;150(2):408–414. | ||
Hirschfeld RM, Lewis L, Vornik LA. Perceptions and impact of bipolar disorder: how far have we really come? Results of the national depressive and manic-depressive association 2000 survey of individuals with bipolar disorder. J Clin Psychiatry. 2003;64(2):161–174. | ||
Marchand WR, Wirth L, Simon C. Delayed diagnosis of pediatric bipolar disorder in a community mental health setting. J Psychiatr Pract. 2006;12(2):128–133. | ||
Cella M, Knibbe C, Danhof M, della Pasqua O. What is the right dose for children? Br J Clin Pharmacol. 2010;70(4):597–603. | ||
Stepanova E, Grant B, Findling RL. Asenapine Treatment in Pediatric Patients with Bipolar I Disorder or Schizophrenia: A Review. Paediatr Drugs. 2018;20(2):121–134. |
Supplementary material
List of independent ethics committees
- Schulman Associates Institutional Review Board, Inc.
4445 Lake Forest Dr, Suite 300
Cincinnati, OH 45242, USA - Western Institutional Review Board
3535 7th Ave SW
Olympia, WA 98502, USA - Chesapeake Research Review, Inc.
7063 Columbia Gateway Dr, Suite 110
Columbia, MD 21046, USA - Stanford Human Research Protection Program
1501 S. California Ave.
Research Compliance Office
Palo Alto, CA 94304-5579, USA - Office of Institutional Review (UHCMC IRB)
University Hospitals Case Medical Center
11100 Euclid Avenue, Lakeside 1400
Cleveland, OH 44106, USA - UCSF Committee on Human Research
3333 California St., Suite 315
Office of Research
San Francisco, CA 94118, USA - St. Anthony IRB
1000 N. Lee St.
Oklahoma City, OK 73101, USA - Hartford Hospital Cardiac Lab
80 Seymour St.
Hartford, CT 06102, USA - Sharp Healthcare Institutional Review Board
8695 Spectrum Center Blvd
San Diego, CA 92123, USA - New York State Psychiatric IRB
1051 Riverside Drive, Suite 5200
New PI building
New York, NY 10032, USA - Via Christi Medical Center
929 N. St. Francis
Institutional Review Board
Wichita, KS 67214, USA - Howard University IRB
1840 NW 7th St., Suite 309
Washington, DC 20001, USA - Integris Health IRB
3330 NW 56th St., Suite 310
Oklahoma City, OK 73112, USA - North Shore LIJ Institute of Medical Research
350 Community Drive
Manhasset, NY 11030, USA - Kootenai Health IRB
2003 Koonetai Health Way
Coeur d’Alene, ID 83814, USA - Office of Research Integrity
19 Hagood Ave. – Room 601
Harborview Office Tower
Charleston, SC 29425, USA - Office of Research Integrity
Box 800483
University of Virginia IRB
Charlottesville, VA 22908, USA - University of Texas Health Science Center at Houston
6410 Fannin, Suite 1100 IRB
Committee for the Protection of Human Subjects
Houston, TX 77030, USA - Partners Human Research Committee
116 Huntington Ave., Suite 1002
Partners Human Research Office
Boston, MA 02116, USA - Saratov City Clinical Hospital #2 n.a. V.I. Razumovsky
Chernyshevskogo St. 141
Department of Psychiatry
Saratov 410028, Russia - EC at Sverdlovsky Regional Clinical Psychiatry Hospital
8thkm, ulitsa Sibirsky trakt
Ekaterinburg 620030, Russia - IEC at St. Petersburg Research Psychoneurology Institute
3 Bekhtereva St.
Saint Petersburg 192019, Russia - Research-And-Educational Centre of Psychotherapy
Lenina St. 417, build. 3
Stavropol 355000, Russia - IIEC on Ethical Review for Clinical Studies
Leningradsky prospekt, 51
Moscow 125468, Russia - Stavropol Region Psychiatric Hospital #2
84 Koroleva Street
Kochubeev district Stavropol region
Township Tonnelniy 357034, Russia - LEC at Central Clinical Psychiatric Hospital
1, 8 Marta ul.
Moscow 127083, Russia - Russian State Medical University, Faculty of Psychiatry
3 Poteshnaya street
Moscow 107076, Russia
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.