")
Back to Journals » Journal of Pain Research » Volume 14
Possible Neuropathic Pain in Patients with Osteoarthritis of the Knee Before and After Total Knee Arthroplasty
Authors Hasegawa M, Tone S, Naito Y, Sudo A
Received 18 July 2021
Accepted for publication 3 September 2021
Published 23 September 2021 Volume 2021:14 Pages 3011—3015
DOI https://doi.org/10.2147/JPR.S330091
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael Schatman
Masahiro Hasegawa, Shine Tone, Yohei Naito, Akihiro Sudo
Department of Orthopaedic Surgery, Mie University Graduate School of Medicine, Tsu City, Mie, 514-8507, Japan
Correspondence: Masahiro Hasegawa
Department of Orthopaedic Surgery, Mie University Graduate School of Medicine, 2-174 Edobashi, Tsu City, Mie, 514-8507, Japan
Tel +81-59-231-5022
Fax +81-59-231-5211
Email [email protected]
Purpose: Although the pain of osteoarthritis (OA) is traditionally considered to be nociceptive, some patients also have neuropathic pain. The objective of this study was to evaluate the presence of neuropathic pain in the knees of OA patients using the painDETECT questionnaire (PDQ).
Methods: A total of 180 knees in 158 consecutive patients who underwent total knee arthroplasty (TKA) were enrolled prospectively. The prevalence of neuropathic pain, unclear pain, and nociceptive pain in the knee was determined before and after TKA using a numerical rating scale (NRS). All patients were evaluated preoperatively and 6 months postoperatively. Neuropathic pain and unclear pain were grouped together as possible neuropathic pain. The relationship between possible neuropathic pain and pain intensity was evaluated.
Results: Before TKA, neuropathic pain and unclear pain were found in 10 and 30 knees, respectively. The remaining 140 knees were categorized as nociceptive pain. After TKA, the numbers of knees with neuropathic and unclear pain decreased to one and five, respectively. The prevalence of possible neuropathic pain decreased significantly from 22.2% to 3.3% after surgery. Among the six knees with possible neuropathic pain postoperatively, four had possible neuropathic pain preoperatively as well, while the remaining two patients had been classified as nociceptive pain preoperatively. Knees with possible neuropathic pain postoperatively had higher postoperative NRS scores than those with nociceptive pain.
Conclusion: Although the prevalence of possible neuropathic pain decreased significantly after TKA, the preoperative presence of possible neuropathic pain might be associated with the development of persistent postoperative pain following TKA.
Keywords: neuropathic pain, nociceptive pain, osteoarthritis, total knee arthroplasty, persistent postoperative pain
Introduction
Pain is a major symptom in patients with osteoarthritis (OA), and persistent pain is a frequent and often disabling complication following total knee arthroplasty (TKA) for OA. The proportion of patients with persistent pain outcomes after TKA ranges from 8% to 27%.1 Chronic pain is classified as nociceptive pain and neuropathic pain. However, not all pain can be clearly distinguished into these pain types, and many patients have unclear pain which cannot be clearly classified as either of these pain types. Nociceptive pain is caused by stimulation of nociceptors through chronic inflammation,2 while neuropathic pain is defined as “pain arising as a direct consequence of a lesion or disease affecting the somatosensory system” by the International Association for the Study of Pain (IASP).3 Although OA pain is traditionally considered to be nociceptive in nature, some patients describe aspects of their pain as burning or shooting. Such characteristics suggest common mechanisms with neuropathic pain.4,5 In fact, neuropathic pain has repeatedly been proposed as a major cause of persistent pain after TKA.4,5 Reportedly, the painDETECT questionnaire (PDQ) can be used to determine whether the pain after TKA is nociceptive or neuropathic pain.6–8 This questionnaire was previously validated in a multicenter study with both neuropathic and nociceptive pain.
We hypothesized that the occurrence of neuropathic pain in the knees of OA patients might decrease after surgery. To prove our hypothesis, we used the PDQ to evaluate the prevalence of neuropathic pain preoperatively and postoperatively in the knees of OA patients undergoing TKA, and evaluated the relationship between neuropathic pain, pain intensity and stage of OA using the Kellgren-Lawrence (KL) system.9
Materials and Methods
Patients
We enrolled 158 consecutive patients with OA (180 knees; female, n = 129 [145 knees] male, n = 29 [35 knees]; mean age, 74 [54–87] years; mean body mass index [BMI], 26.1 [17.8–44.1] kg/m2) who underwent TKA from 2016 to 2017 prospectively. All the procedures were performed under general anesthesia by a single surgeon (MH) using the mid-vastus approach to TKA. Posterior-stabilized type knee prostheses were used in all knees. All the prosthetic knees had a fixed-bearing design, and all tibial, femoral and patellar components were cemented. The operating surgeon (MH) screened the patients for medical testing for OA before surgery. Exclusion criteria consisted of severe knee deformity requiring a constrained implant (femoro-tibial angle <155º or >200º), as determined using preoperative radiographs. Patients with knee OA who had severe spinal cord-related pain preoperatively were not indicated for TKA.
Pain Phenotype
Knee pain was evaluated using a numerical rating scale (NRS) ranging from 0 (no pain) to 10 (severe pain). Pain phenotype was assessed using the self-reporting PDQ, which includes nine questions regarding the intensity and quality of pain.6,7 The scores related to the pain course pattern and presence of radiating pain (maximum score of 3) and the gradation of pain (maximum score of 35) were summed up to obtain a maximum PDQ end score of 38. Neuropathic pain was considered unlikely (nociceptive pain group) when PDQ scores ranged between 0 and 12, whereas scores of 19 to 38 indicated neuropathic pain. Scores of 13 to 18 indicated unclear pain (including nociceptive and neuropathic components).
The prevalence of neuropathic pain, unclear pain and nociceptive pain before and after TKA were determined. All patients were evaluated preoperatively and 6 months postoperatively. Neuropathic pain and unclear pain were grouped together as possible neuropathic pain, and NRS scores were compared between the possible neuropathic pain and nociceptive pain groups before and after TKA. We also evaluated the relationship between preoperative pain type and the severity of OA using the KL system.10 The institutional review board of Mie University approved this study, and all patients provided written, informed consent to participate. This study was conducted in accordance with the Declaration of Helsinki.
Statistical Analyses
Preoperative NRS scores, age, BMI and flexion angle were compared between knees with preoperative possible neuropathic pain and nociceptive pain using Mann–Whitney U-tests. Sex and KL grade were compared using Chi-squared tests. The prevalence of possible neuropathic pain and nociceptive pain before and after TKA was compared using Chi-squared tests. Postoperative NRS scores were compared between knees with postoperative possible neuropathic pain and nociceptive pain using Mann–Whitney U-tests. Correlations between NRS and PDQ scores before and after TKA were determined using Spearman correlation coefficient. Changes in pain type before and after TKA were evaluated using Fisher’s test. Power analysis was performed before conducting this study to determine the appropriate sample size. A previous study demonstrated that the incidence of possible neuropathic pain was 21%.10 Based on the results of that study and a two-sided test with a type I error of 0.05, we determined that a sample size of at least 25 patients would be required to achieve a power of 0.8. Statistical significance was set at p < 0.05. Data were statistically analyzed using SPSS version 22 (SPSS Inc., Chicago, IL, USA).
Results
Before TKA, neuropathic pain and unclear pain were found in 10 and 30 knees, respectively. The remaining 140 knees were categorized as nociceptive pain. After TKA, the numbers of knees with neuropathic and unclear pain decreased to one and five, respectively. Nociceptive pain was found in 174 knees after TKA (Table 1). The prevalence of possible neuropathic pain decreased significantly from 22.2% preoperatively to 3.3% postoperatively (p < 0.001). Preoperative and postoperative NRS scores were not significantly different between the preoperative possible neuropathic pain group and nociceptive pain group. There were no differences in preoperative pain in relation to sex, age, BMI, KL grade, and preoperative flexion angle (Table 2). There was a positive correlation between preoperative NRS and PDQ scores (r = 0.385, p < 0.001). Similarly, there was a positive correlation between postoperative NRS and PDQ scores (r = 0.365, p < 0.001). Knees with postoperative possible neuropathic pain had higher postoperative NRS scores than those with nociceptive pain (p = 0.011). Among the six knees with possible neuropathic pain postoperatively, four had possible neuropathic pain preoperatively as well, while the remaining two patients had been classified as nociceptive pain preoperatively (p = 0.021).
 |
Table 1 Prevalence of the Different Pain Phenotypes in Patients with Osteoarthritis of the Knee |
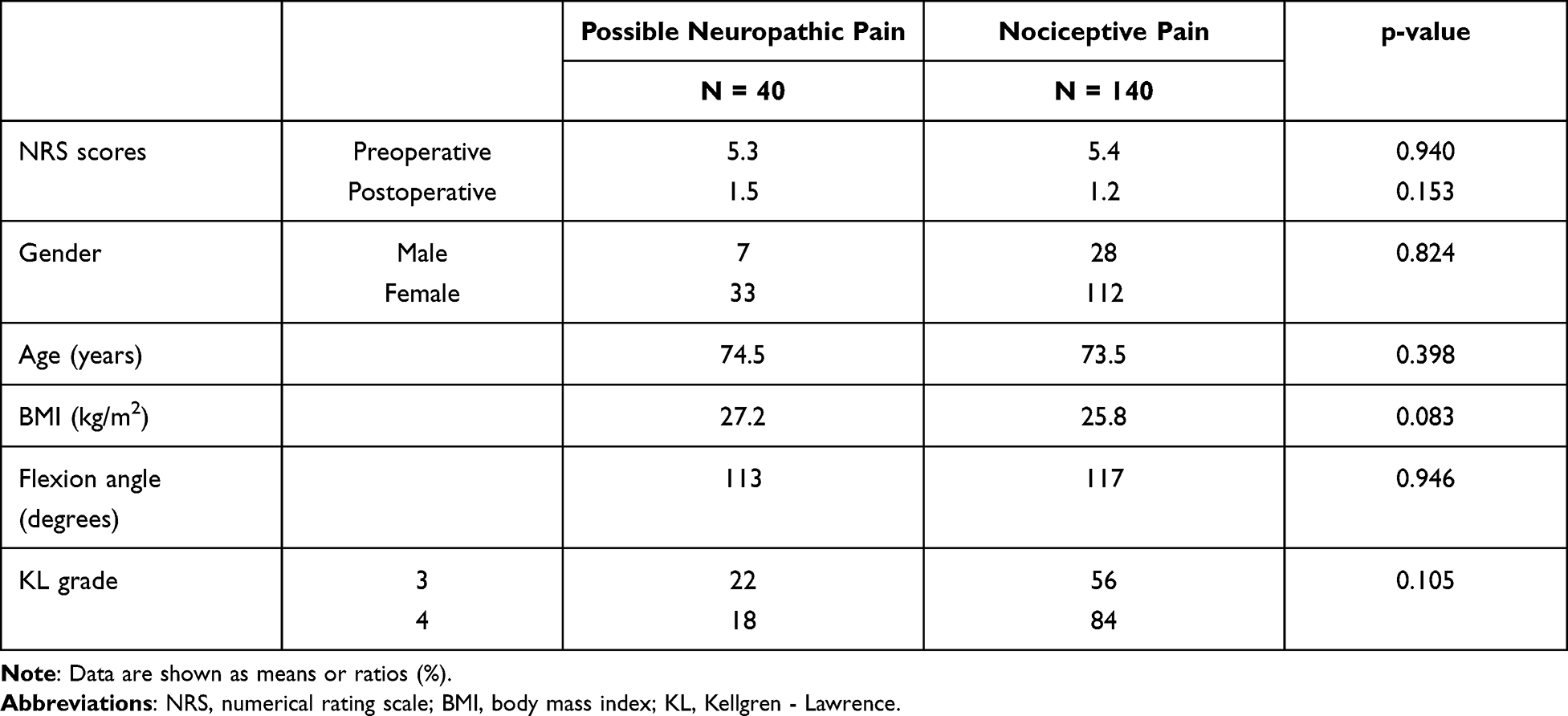 |
Table 2 Comparison Between Patients with the Preoperative Pain Phenotypes of Possible Neuropathic Pain (Neuropathic Pain or Unclear Pain) versus Those with Nociceptive Pain |
Discussion
A growing amount of evidence suggests that OA pain has a neuropathic component in some patients. Deeper understanding of the likely multiple mechanisms of OA pain has led to the use of centrally acting drugs to alleviate osteoarthritic pain.11
Several animal studies supported the hypothesis that neuropathic pain might occur due to the pathogenetic mechanisms of OA.12,13 Histologic assessment of the morphology of nerves in an animal model of knee OA by sodium monoiodoacetate (MIA) injection showed changes in nerves suggestive of neuropathic pain. Such changes include reduced nerve fiber density, and expression of activation transcription factor-3 (ATF-3, a marker of nerve damage) in the spinal cord.12 The presence of lysophosphatidic acid (LPA) in joint synovium has been found to correlate with myelin thickness and ATF-3 in an OA model of MIA injection.13 However, these hypotheses have not been proven in human OA subjects.
Previous studies demonstrated that neuropathic pain localized to the knees, assessed using the PDQ, affected 5% to 32% of patients.4,10,14–17 Possible neuropathic pain has been variously reported in 21% to 50% of cases (Table 3).4,10,14–17 The present study demonstrated preoperative neuropathic pain and possible neuropathic pain in 5.6% and 22.2% of the study subjects, respectively. Although this prevalence was lower than in many previous studies, it was similar to a Japanese report by Ohtori et al.10 However, previous studies did not evaluate the outcomes after TKA in patients with neuropathic pain. The present study demonstrated the key role of preoperative possible neuropathic pain on postoperative pain. Using the Self-administered Leeds Assessment of Neuropathic Symptoms and Signs (S-LANSS) scale, Fitzsimmons et al18 reported that suspected neuropathic pain was present in 35.5% of pre-TKA patients, and in 23.6% of OA patients at 6 months post-TKA. In their study, patients scoring 12 or greater on the scale were defined as having suspected neuropathic pain.18 They suggested that in patients with possible neuropathic pain before TKA, careful evaluation, including of spinal disease, is needed to avoid chronic postoperative knee pain. A recent study demonstrated that possible neuropathic pain with end-stage hip and knee OA was more strongly associated with pain at rest than pain on activity.19 This indicates that the clinical presentation of pain at rest might warrant more thorough evaluation for potential neuropathic pain.
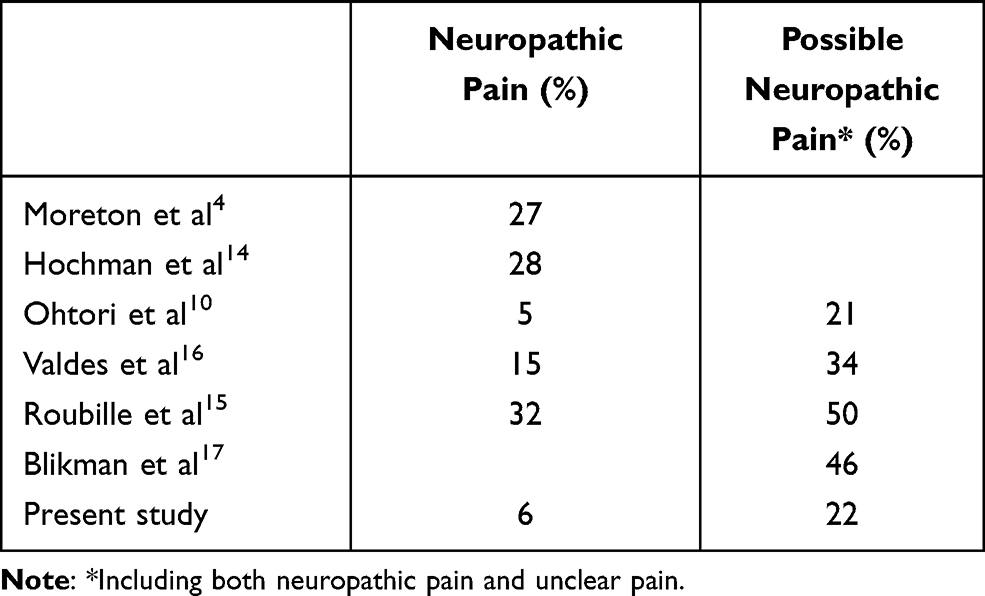 |
Table 3 Prevalence of Neuropathic Pain in Knee Osteoarthritis Patients in the Literature Assessed Using the painDETECT Questionnaire (PDQ) |
Using S-LANSS, Razmjou et al20 showed that the prevalence of neuropathic pain was 14% at an average of 5 years after TKA. They also showed that patients with neuropathic pain (S-LANSS score of 12 or greater) remained more disabled, and with a higher level of depression and less surgical satisfaction. Moreton et al4 evaluated PDQ and S-LANSS to determine agreement between the two assessment methods, and found that agreement between the PDQ and S-LANSS for pain classification was low, and it currently remains unknown which tool might best predict treatment outcomes. The PDQ assesses pain quality associated with augmented central pain processing in patients with OA. Although developed as a screening questionnaire, the PDQ might also function as a measure of characteristics that indicate augmented central pain processing. However, it should be noted that one important problem with the PDQ is that patients with no pain are classified in the nociceptive pain group, since a score of zero on the PDQ is considered nociceptive pain.
Neuropathic pain is uncommon after TKA surgery.8 In a previous study by Hasegawa et al8 neuropathic pain after TKA was not identified (mean observation period: 4.7 years) among 222 patients with OA. However, unclear pain (including nociceptive and neuropathic pain) was found in 9% of the knees. There was also an association between moderate-to-severe postoperative pain and unclear pain.8 In the present study, the prevalence of neuropathic pain decreased from 5.6% to 0.6% after TKA, and the prevalence of possible neuropathic pain decreased from 22.2% to 3.3% (Table 1), verifying our hypothesis that neuropathic pain might decrease after TKA surgery. However, knees with postoperative possible neuropathic pain had higher postoperative NRS scores than those with nociceptive pain. In addition, higher PDQ scores were associated with severe pain, which might result in worse outcomes and less satisfaction after TKA. Although the causes and factors associated with neuropathic pain warrant further investigation, preoperative assessment, including by the PDQ, might be useful for reducing the prevalence of postoperative chronic knee pain.
Limitations of this study include the absence of evaluations of spinal disease and a short follow-up period of only 6 months.
Conclusion
Preoperative PDQ scores classified 22.2% of OA knee pain as possible neuropathic pain, suggesting that it is important to consider neuropathic pain when planning the treatment of OA knee pain. Furthermore, although the prevalence of possible neuropathic pain decreased to 3.3% after TKA, our results indicate that there might be an association between the preoperative presence of possible neuropathic pain and the occurrence of chronic postoperative pain after TKA.
Acknowledgments
The authors have not received financial support or any other benefits from commercial sources for the work reported in the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Beswick AD, Wylde V, Gooberman-Hill R, Blom A, Dieppe P. What proportion of patients report long-term pain after total hip or knee replacement for osteoarthritis? A systematic review of prospective studies in unselected patients. BMJ Open. 2012;2(1):e000435. doi:10.1136/bmjopen-2011-000435
2. Siddall PJ, McClelland JM, Rutkowski SB, Cousins MJ. A longitudinal study of the prevalence and characteristics of pain in the first 5 years following spinal cord injury. Pain. 2003;103(3):249–257. doi:10.1016/S0304-3959(02)00452-9
3. Treede RD, Jensen TS, Campbell JN, et al. Neuropathic pain: redefinition and a grading system for clinical and research purposes. Neurology. 2008;70(18):1630–1635. doi:10.1212/01.wnl.0000282763.29778.59
4. Moreton BJ, Tew V, Das Nair R, Wheeler M, Walsh DA, Lincoln NB. Pain phenotype in patients with knee osteoarthritis: classification and measurement properties of painDETECT and self-report Leeds assessment of neuropathic symptoms and signs scale in a cross-sectional study. Arthritis Care Res. 2015;67(4):519–528. doi:10.1002/acr.22431
5. Fernandes GS, Valdes AM, Walsh DA, Zhang W, Doherty M. Neuropathic-like knee pain and associated risk factors: a cross-sectional study in a UK community sample. Arthritis Res Ther. 2018;20(1):215. doi:10.1186/s13075-018-1717-6
6. Freynhagen R, Baron R, Gockel U, Tölle TR. painDETECT: a new screening questionnaire to identify neuropathic components in patients with back pain. Curry Med Res Opin. 2006;22(10):1911–1920. doi:10.1185/030079906X132488
7. Matsubayashi Y, Takeshita K, Sumitani M, et al. Validity and reliability of the Japanese version of the painDETECT questionnaire: a multicenter observational study. PLoS One. 2013;8(9):e68013. doi:10.1371/journal.pone.0068013
8. Hasegawa M, Tone S, Naito Y, Wakabayashi H, Sudo A. Prevalence of persistent pain after total knee arthroplasty and the impact of neuropathic pain. J Knee Surg. 2019;32(10):1020–1023. doi:10.1055/s-0038-1675415
9. Kellgren JH, Lawrence JS. Radiological assessment of osteoarthrosis. Ann Rheum Dis. 1957;16(4):494–502. doi:10.1136/ard.16.4.494
10. Ohtori S, Orita S, Yamashita M, et al. Existence of a neuropathic pain component in patients with osteoarthritis of the knee. Yonsei Med J. 2012;53(4):801–805. doi:10.3349/ymj.2012.53.4.801
11. Dimitroulas T, Duarte RV, Behura A, Kitas GD, Raphael JH. Neuropathic pain in osteoarthritis: a review of pathophysiological mechanisms and implications for treatment. Semin Arthritis Rheum. 2014;44(2):145–154. doi:10.1016/j.semarthrit.2014.05.011
12. Thakur M, Rahman W, Hobbs C, Dickenson AH, Bennett DL. Characterisation of a peripheral neuropathic component of the rat monoiodoacetate model of osteoarthritis. PLoS One. 2012;7(3):e33730. doi:10.1371/journal.pone.0033730
13. McDougall JJ, Albacete S, Schuelert N, et al. Lysophosphatidic acid provides a missing link between osteoarthritis and joint neuropathic pain. Osteoarthritis Cartilage. 2017;25(6):926–934. doi:10.1016/j.joca.2016.08.016
14. Hochman JR, Gagliese L, Davis AM, Hawker GA. Neuropathic pain symptoms in a community knee OA cohort. Osteoarthritis Cartilage. 2011;19(6):647–654. doi:10.1016/j.joca.2011.03.007
15. Roubille C, Raynauld JP, Abram F, et al. The presence of meniscal lesions is a strong predictor of neuropathic pain in symptomatic knee osteoarthritis: a cross-sectional pilot study. Arthritis Res Ther. 2014;16(6):507. doi:10.1186/s13075-014-0507-z
16. Valdes AM, Suokas AK, Doherty SA, Jenkins W, Doherty M. History of knee surgery is associated with higher prevalence of neuropathic pain-like symptoms in patients with severe osteoarthritis of the knee. Semin Arthritis Rheum. 2014;43(5):588–592. doi:10.1016/j.semarthrit.2013.10.001
17. Blikman T, Rienstra W, van Raay JJAM, et al. Neuropathic-like symptoms and the association with joint-specific function and quality of life in patients with hip and knee osteoarthritis. PLoS One. 2018;13(6):e0199165. doi:10.1371/journal.pone.0199165
18. Fitzsimmons M, Carr E, Woodhouse L, Bostick GP. Development and persistence of suspected neuropathic pain after total knee arthroplasty in individuals with osteoarthritis. PM R. 2018;10(9):903–909. doi:10.1016/j.pmrj.2018.01.010
19. Power JD, Perruccio AV, Gandhi R, et al. Neuropathic pain in end-stage hip and knee osteoarthritis: differential associations with patient-reported pain at rest and pain on activity. Osteoarthritis Cartilage. 2018;26(3):363–369. doi:10.1016/j.joca.2018.01.002
20. Razmjou H, Boljanovic D, Wright S, Murnaghan J, Holtby R. Association between neuropathic pain and reported disability after total knee arthroplasty. Physiother Can. 2015;67(4):311–318. doi:10.3138/ptc.2014-46
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.