")
Back to Journals » Vascular Health and Risk Management » Volume 19
Possible Clinical Benefits of Cardio-Ankle Vascular Index Measurement in Urological Diseases
Authors Bulbul E , Ozilhan MO, Sezer A , Yetisen M, Ilki FY
Received 31 December 2022
Accepted for publication 7 March 2023
Published 9 March 2023 Volume 2023:19 Pages 127—132
DOI https://doi.org/10.2147/VHRM.S384937
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
Emre Bulbul,1 Murat Oguz Ozilhan,2 Ali Sezer,3 Mustafa Yetisen,4 Fahri Yavuz Ilki5
1Department of Urology, Trabzon Vakfıkebir State Hospital, Trabzon, Turkey; 2Department of Cardiology, Ankara City Hospital, Ankara, Turkey; 3Department of Urology, Konya City Hospital, Konya, Turkey; 4Department of Cardiology, Erzurum Oltu State Hospital, Erzurum, Turkey; 5Department of Urology, Gulhane Training and Research Hospital, Ankara, Turkey
Correspondence: Emre Bulbul, Department of Urology, Trabzon Vakfıkebir State Hospital, Trabzon, 61400, Turkey, Tel +90 536 390 06 11, Fax +90 462 841 35 50, Email [email protected]
Abstract: Many factors are considered to affect vascular physiology. It is known that one of the reasons for many diseases is a pathology at the microvascular level. Therefore, the relationship between endothelial dysfunction and many diseases is currently being investigated. The clinical evaluations of arterial stiffness have made it possible to perform necessary risk assessment regarding cardiovascular diseases. In this way, protective measures can be taken against microvascular pathologies in many organs. In this paper, we present a review of studies investigating the relationship between urological conditions and the cardio-ankle vascular index (CAVI), a marker of arterial stiffness. As with erectile dysfunction, some studies have shown that conditions such as lower urinary tract symptoms, overactive bladder, and chronic kidney disease are also associated with an elevated CAVI. The association of erectile dysfunction and chronic kidney disease with vascular pathologies has been clearly demonstrated. In addition, lower urinary tract symptoms may be the first sign of silent vascular dysfunction. Assessing arterial stiffness with CAVI can help prevent future cardiovascular events in these patients.
Keywords: arterial stiffness, cardio-ankle vascular index, cardiovascular disease, erectile dysfunction, lower urinary tract symptoms, overactive bladder
Plain Language Summary
- Erectile dysfunction and cardiovascular disease can be seen together with systemic vascular pathologies.
- The cardio-ankle vascular index is higher in patients with erectile dysfunction and overactive bladder than in healthy people.
- The risk of cardiovascular disease in patients with chronic kidney disease is much higher than in the general population.
- Lower urinary tract symptoms are associated with increased arterial stiffness.
Introduction
The human body has a unique vascular anatomy, and many factors are consider to affect vascular physiology. It is known that one of the components of many diseases is a pathology at the microvascular level.1–3 Therefore, the relationship between endothelial dysfunction and many diseases is currently being investigated.4,5
Erectile dysfunction (ED) may be the first sign of cardiovascular disease (CVD) risk. The luminal diameter of the penile artery is smaller than that of the coronary arteries, and the erection mechanism is affected earlier by microvascular pathologies. Therefore, ED may be a marker of systemic microvascular pathologies. Furthermore, ED and CVD can be seen together with systemic vascular pathologies.6 The European Association of Urology guidelines recommend that patients with ED be evaluated in detail regarding CVD risk.7 In the literature, it has been stated that urological diseases, such as overactive bladder (OAB) and benign prostatic enlargement (BPE) are also associated with vascular pathologies.8,9 It has been noted that as the local atherosclerosis of the prostatic artery increases, the prostate volume also increases. It has also been reported that oxidative stress markers are effective in the mechanism of BPE.10 CVD risk has been found to be higher in patients with OAB. In addition, bladder neck perfusion is low on Doppler ultrasonography. As the severity of OAB increases, the Framingham risk score also increases.11
In the literature, it has been reported that endothelial dysfunction is associated with many urological diseases, including ED, OAB, and BPE.12–14 In clinical studies, many markers, such as brachial flow-mediated dilatation, pulse wave velocity (PWV), cardio-ankle vascular index (CAVI), and intima-media thickness have been used to measure endothelial dysfunction.15–18
Vascular age can be determined non-invasively by measuring arterial stiffness. PWV and CAVI are indicators of arterial stiffness.19,20 Carotid-femoral measurement is generally used to evaluate arterial stiffness with PWV. Age, rheumatological diseases and blood pressure are parameters that affect PWV independently.21 The CAVI can also assess arterial stiffness independent of blood pressure.22
With the clinical evaluations of arterial stiffness, necessary risk assessment can be made regarding cardiovascular diseases (Table 1). In this way, protective measures can be taken against microvascular pathologies in many organs. In this paper, we present a review of studies investigating the relationship between urological conditions and CAVI, a marker of arterial stiffness.
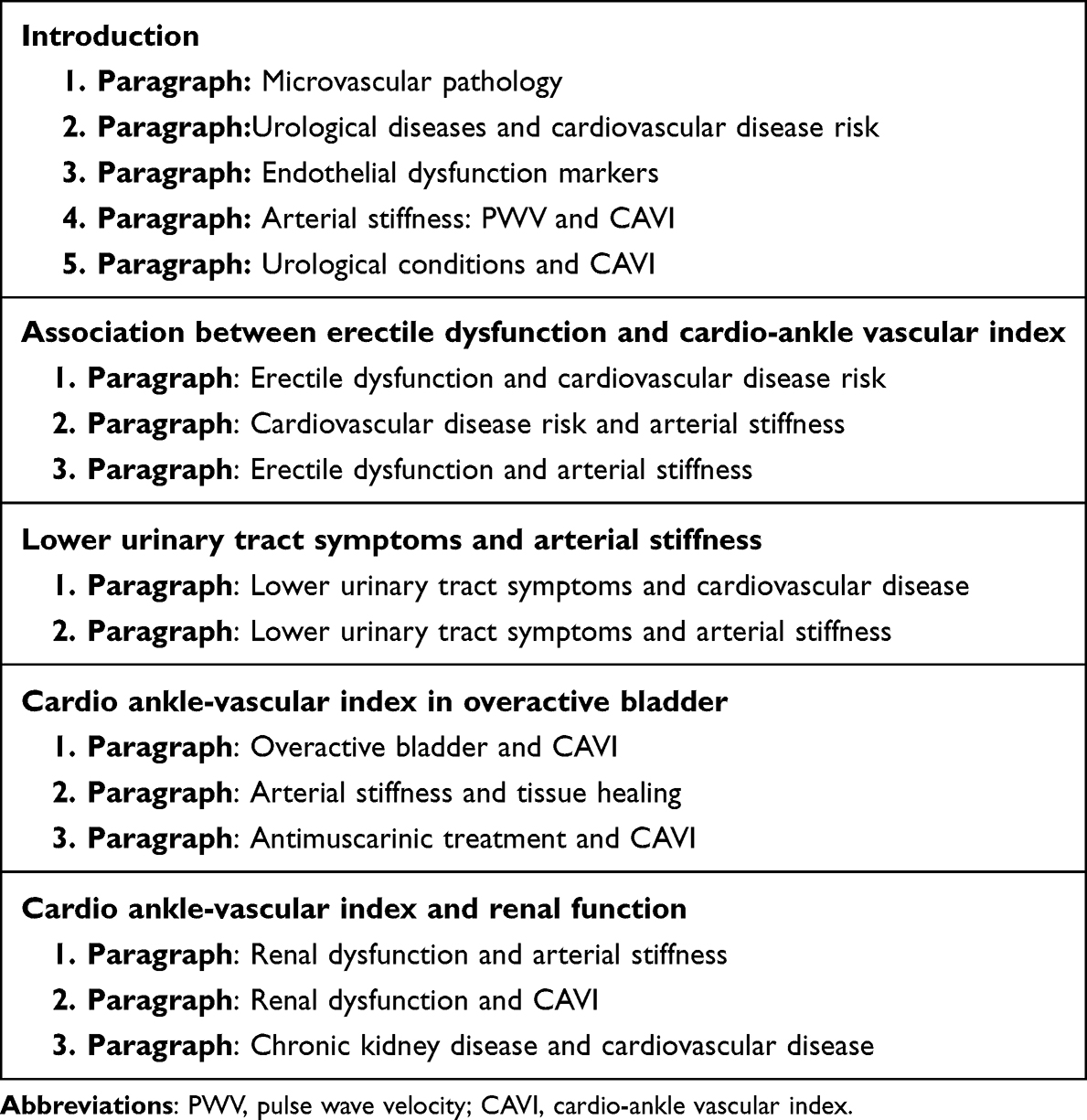 |
Table 1 The Principal Finding of Each Paragraph |
Association Between Erectile Dysfunction and Cardio-Ankle Vascular Index
The relationship between ED and CVD has been known for a long time. Patients with ED, especially those without a history of CVD may be unaware of the possibility of developing associated cardiological pathologies in future. In patients with ED, urologists usually perform a routine metabolic evaluation (body mass index, fasting blood glucose, triglyceride, cholesterol, etc.). However, other than routine blood pressure measurement, no assessment is made regarding vascular physiology. Only local vascular functions can be evaluated with penile Doppler ultrasonography. Investigating vascular dysfunction, an essential component of ED pathophysiology, in the whole body can provide significant benefits. Therefore, there is a need for non-invasive markers to show vascular dysfunction.
The patients can be evaluated regarding CVD risk using arterial stiffness measurement. Hayashi et al developed the ß formula for this assessment. In their study including 18 cadavers, the authors comprehensively measured vascular wall stiffness and reported that arterial stiffness increased with age. They also stated that increased arterial stiffness played a role in the development of cerebrovascular disease.23 Later, PWV was used as a marker for measuring arterial stiffness. However, the blood pressure value at the time of measurement affects the PWV value.24 Therefore, in 2006, Shirai et al developed a new method for the measurement of arterial stiffness. In a study they conducted with hemodialysis patients, the authors reported that CAVI was higher in those with signs of atherosclerotic disease than those patients without these signs. In addition, they noted that the correlation of CAVI with blood pressure was weaker compared to that of PWV with blood pressure.25
Arterial stiffness assessment in patients with ED can help identify those at risk of CVD.26 In a screening study of healthy Japanese men, Imai et al reported that arterial stiffness was higher among those with ED.27 In another study, Demirelli et al determined that arterial stiffness increased as ED severity increased.28 The literature also suggests that phosphodiesterase-5 inhibitor therapy reduces arterial stiffness in patients with ED.29,30 Bulbul et al compared CAVI between the patients with ED and healthy men and found a significantly higher value in the former. In addition, the authors reported that as the severity of ED increased, CAVI increased proportionally.31 In a 2016 study, Motil et al used a device they developed for low-intensity shockwave therapy in the treatment of vasculogenic ED. In that study, patients with vasculogenic ED were successfully identified by measuring CAVI.32
Lower Urinary Tract Symptoms and Arterial Stiffness
While the cause of lower urinary tract symptoms (LUTS) is mostly BPE in men, the etiology is not yet clear in women. The development of LUTS increases with age and has a multifactorial origin. In the literature, it has been suggested that LUTS may be associated with chronic ischemia. Increased reactive oxygen radicals in the bladder due to chronic ischemia may damage the bladder wall, causing the detrusor to work excessively or be underactive.33 It has been reported that there is a relationship between nocturia and CVD. Tikkinen et al found that the incidence of nocturia increased threefold in patients with CVD.34
The role of vascular dysfunction in the etiology of LUTS is still being investigated. Uzun et al evaluated arterial stiffness and carotid intima–media thickness in male and female patients with LUTS and detected higher values in the patient group compared to the control group. The authors concluded that LUTS was associated with vascular dysfunction in both men and women.35 Yabe et al performed robot-assisted laparoscopic radical prostatectomy on 80 male patients with prostate cancer. They divided these patients into the atherosclerotic group (CAVI ≥ 9.0) and the control group (CAVI < 9.0). The voiding and international prostate symptom scores were significantly higher in the atherosclerosis group than in the control group at the postoperative third month. There was no significant difference between the two groups regarding the voiding and international prostate symptom scores at six months, but the maximum flow rate was significantly lower in the atherosclerosis group. It was concluded that the increase in arterial stiffness determined by CAVI adversely affected the reduction of LUTS in the early period after robot-assisted laparoscopic radical prostatectomy.36 In a study conducted with 12 healthy men in 2011, 4 mg of doxazosin, an alpha 1 adrenergic receptor blocker, was administered to the patients, and it was determined that CAVI significantly decreased after doxazosin administration compared to the pre-treatment value.37
Cardio Ankle-Vascular Index in Overactive Bladder
It has been stated that OAB occurs due to sympathetic autonomic dysfunction. Shimizu et al evaluated patients with OAB or an idiopathic large post-void residual volume (>100 mL) using CAVI and carotid intima-media thickness measurements. The CAVI values were significantly higher in the OAB group than in the control group. However, no significant difference was observed between the two groups regarding the carotid intima-media thickness. Furthermore, there was no significant difference in vascular function between the patients with a large post-void residual volume and the control group. The authors suggested that a large post-void residual volume might be associated with local factors, and the autonomic dysfunction of the bladder might be related to systemic vascular pathologies.38
Increased arterial stiffness may affect tissue healing by causing vascular dysfunction. Koguchi et al cross-sectionally examined OAB symptoms in patients who underwent robot-assisted laparoscopic radical prostatectomy for prostate cancer. They divided the patients into two groups according to their arterial stiffness values as the atherosclerotic group (CAVI ≥ 9.0) and the control group (CAVI < 9.0). At the postoperative third month, de novo OAB development was higher in the atherosclerotic group than in the control group. At nine and 12 months, voided volume was significantly lower in the atherosclerotic group than in the control group. The increase in arterial stiffness adversely affected the improvement of storage symptoms after robot-assisted laparoscopic radical prostatectomy.39
Care should be taken regarding the cardiac side effects of antimuscarinic and sympathomimetic agents used in the treatment of OAB. The risks of triggering antimuscarinic autonomic dysfunction and increasing the pulse rate of sympathomimetics should be considered. Hsiao et al investigated the cardiovascular effects of 25 mg mirabegron (beta-3 sympathomimetic) and 5 mg solifenacin in women. After 12 weeks of treatment, blood pressure significantly decreased in the patients that received solifenacin, and the pulse rate significantly increased in those treated with mirabegron. There was no significant difference in CAVI between the two groups after treatment.40 In a study evaluating female patients with OAB, the effects of antimuscarinic drugs were compared. After 12 weeks of treatment, CAVI was significantly reduced in patients that received 5 mg tolterodine. However, CAVI did not significantly differ after 12 weeks of 4 mg solifenacin treatment compared to the pre-treatment values. It was concluded that in the treatment of OAB caused by sympathetic autonomic dysfunction, the use of tolterodine was beneficial to help recover vascular function.41
Cardio Ankle-Vascular Index and Renal Function
Albuminuria is one of the early indicators of renal dysfunction. The albumin/creatinine ratio in urine is used as a marker for albuminuria. If the albumin/creatinine ratio in the urine is ≥ 30 mg/g, it is considered to indicate pathological albuminuria. Jiang et al reported that arterial stiffness was independently associated with pathological albuminuria.42 Latif et al investigated factors affecting mortality in 5827 hemodialysis patients from six countries and found that high serum uric acid levels (>8.2 mg/dl) reduced mortality due to CVD.43 Harada et al examined the serum uric acid and CAVI values of 48 hemodialysis patients without CVD. Interestingly, they found an inverse correlation between these two parameters.44
The increase in arterial stiffness measured by CAVI is a marker of deterioration in renal function.45 The use of intravenous contrast agents in imaging can lead to acute deterioration in renal function. Sahinkus et al performed the CAVI evaluation of 126 patients who underwent contrast-enhanced coronary angiography. CAVI was determined to be significantly higher in the patients who developed contrast-induced nephropathy compared to those without nephropathy.46
The risk of CVD and mortality due to CVD are much higher in patients with chronic kidney disease (CKD) than in the general population.47 Vascular changes in patients with CKD cause an increase in arterial stiffness.48 Blacher et al evaluated the arterial stiffness of 241 patients with end-stage CKD. They reported that increased arterial stiffness resulted in an increase in overall and CVD-related mortality.49 In another study, arterial stiffness was found to increase as CKD increased.50 Ishimura et al measured CAVI in 107 kidney transplant patients and detected significantly lower CAVI values in those that received everolimus compared to the remaining patients. The authors suggested that everolimus treatment might have a protective effect against the development of atherosclerosis after kidney transplantation.51
Conclusions
In addition to ED, elevated CAVI values have been reported in studies evaluating patients with LUTS, OAB, and CKD have been. The association of ED and CKD with vascular pathologies is well established. LUTS may also be the first sign of silent vascular dysfunction. Assessing arterial stiffness with CAVI can help prevent future cardiovascular events in these patients.
Disclosure
The authors report no conflicts of interest concerning this work.
References
1. Lush CW, Kvietys PR. Microvascular dysfunction in sepsis. Microcirculation. 2000;7(2):83–101. doi:10.1038/sj.mn.7300096
2. Namekata T, Suzuki K, Ishizuka N, Shirai K. Establishing baseline criteria of the cardio-ankle vascular index as a new indicator of arteriosclerosis: a cross-sectional study. BMC Cardiovasc Disord. 2011;11(1):1–10. doi:10.1186/1471-2261-11-51
3. Lee MH, Perl DP, Nair G, et al. Microvascular injury in the brains of patients with Covid-19. N Engl J Med. 2021;384(5):481–483. doi:10.1056/NEJMc2033369
4. Gonzalez‐Juanatey C, Llorca J, Miranda‐Filloy JA, et al. Endothelial dysfunction in psoriatic arthritis patients without clinically evident cardiovascular disease or classic atherosclerosis risk factors. Arthritis Care Res. 2007;57(2):287–293. doi:10.1002/art.22530
5. Sari I, Okan T, Akar S, et al. Impaired endothelial function in patients with ankylosing spondylitis. Rheumatology. 2006;45(3):283–286. doi:10.1093/rheumatology/kei145
6. Gandaglia G, Briganti A, Jackson G, et al. A systematic review of the association between erectile dysfunction and cardiovascular disease. Eur Urol. 2014;65(5):968–978. doi:10.1016/j.eururo.2013.08.023
7. Salonia A, Minhas S, Bettocchi C, et al. EAU guidelines. End.
8. Kilinc MF, Yasar E, Aydin HI, Yildiz Y, Doluoglu OG. Association between coronary artery disease severity and overactive bladder in geriatric patients. World J Urol. 2018;36(1):35–40. doi:10.1007/s00345-017-2098-1
9. Andersson KE, De Groat WC, McVary KT, et al. Tadalafil for the treatment of lower urinary tract symptoms secondary to benign prostatic hyperplasia: pathophysiology and mechanism (s) of action. Neurourol Urodyn. 2011;30(3):292–301. doi:10.1002/nau.20999
10. Haga N, Akaihata H, Hata J, et al. The association between local atherosclerosis of the prostatic artery and benign prostatic enlargement in humans: putative mechanism of chronic ischemia for prostatic enlargement. Prostate. 2018;1–12. doi:10.1002/pros.23658
11. Yeniel AO, Ergenoglu AM, Meseri R, et al. Is overactive bladder microvasculature disease a component of systemic atherosclerosis? Neurourol Urodyn. 2017;1–8. doi:10.1002/nau.23452
12. Bivalacqua TJ, Usta MF, Champion HC, Kadowitz PJ, Hellstrom WJ. Endothelial dysfunction in erectile dysfunction: role of the endothelium in erectile physiology and disease. J Androl. 2003;24(S6):S17–S37. doi:10.1002/j.1939-4640.2003.tb02743.x
13. Azadzoi KM, Tarcan T, Kozlowski R, Krane RJ, Siroky MB. Overactivity and structural changes in the chronically ischemic bladder. J Urol. 1999;162(5):1768–1778. doi:10.1016/S0022-5347(05)68236-5
14. Inci M, Sarli B, Davarci M, et al. Relationship between endothelial dysfunction and nocturia with benign prostatic hyperplasia. Scand J Urol. 2013;47(5):384–389. doi:10.3109/21681805.2012.762038
15. Neunteufl T, Heher S, Katzenschlager R, et al. Late prognostic value of flow-mediated dilation in the brachial artery of patients with chest pain. Am J Cardiol. 2000;86(2):207–210. doi:10.1016/S0002-9149(00)00857-2
16. McEniery CM, Wallace S, Mackenzie IS, McDonnell B, Yasmin ND, Wilkinson IB. Endothelial function is associated with pulse pressure, pulse wave velocity, and augmentation index in healthy humans. Hypertension. 2006;48(4):602–608. doi:10.1161/01.HYP.0000239206.64270.5f
17. Nakamura K, Tomaru T, Yamamura S, Miyashita Y, Shirai K, Noike H. Cardio-ankle vascular index is a candidate predictor of coronary atherosclerosis. Circulation J. 2007;72(4):598–604. doi:10.1253/circj.72.598
18. Halcox JP, Donald AE, Ellins E, et al. Endothelial function predicts progression of carotid intima-media thickness. Circulation. 2009;119(7):1005–1012. doi:10.1161/CIRCULATIONAHA.108.765701
19. Willum Hansen T, Staessen JA, Torp-Pedersen C, et al. Prognostic value of aortic pulse wave velocity as index of arterial stiffness in the general population. Circulation. 2006;113(5):664–670. doi:10.1161/CIRCULATIONAHA.105.579342
20. Aydın E, Kant A, Yilmaz G. Evaluation of the cardio-ankle vascular index in COVID-19 patients. Revista da Associação Médica Brasileira. 2021;68:73–76. doi:10.1590/1806-9282.20210781
21. Maloberti A, Vallerio P, Triglione N, et al. Vascular aging and disease of the large vessels: role of inflammation. High Blood Pressure Cardiovasc Prev. 2019;26:175–182. doi:10.1007/s40292-019-00318-4
22. Nagayama D, Sugiura T, Choi SY, Shirai K. Various obesity indices and arterial function evaluated with CAVI–is waist circumference adequate to define metabolic syndrome? Vasc Health Risk Manag. 2022;721–733. doi:10.2147/VHRM.S378288
23. Hayashi K, Handa H, Nagasawa S, Okumura A, Moritake K. Stiffness and elastic behavior of human intracranial and extracranial arteries. J Biomech. 1980;13(2):175–184. doi:10.1016/0021-9290(80)90191-8
24. Sutton-Tyrrell K, Najjar SS, Boudreau RM, et al. Elevated aortic pulse wave velocity, a marker of arterial stiffness, predicts cardiovascular events in well-functioning older adults. Circulation. 2005;111(25):3384–3390. doi:10.1161/CIRCULATIONAHA.104.483628
25. Shirai K, Utino J, Otsuka K, Takata M. A novel blood pressure-independent arterial wall stiffness parameter; cardio-ankle vascular index (CAVI). J Atheroscler Thromb. 2006;13(2):101–107. doi:10.5551/jat.13.101
26. Chang ST, Chu CM, Hsu JT, et al. Scrutiny of cardiovascular risk factors by assessing arterial stiffness in erectile dysfunction patients. World J Urol. 2010;28(5):625–630. doi:10.1007/s00345-009-0486-x
27. Imai A, Yamamoto H, Hatakeyama S, et al. Risk factors for erectile dysfunction in healthy Japanese men. Int J Androl. 2010;33(4):569–573. doi:10.1111/j.1365-2605.2009.00974.x
28. Demirelli E, Karagöz A, Öğreden E, et al. The relationship between the severity of erectile dysfunction and aortic stiffness. Andrologia. 2020;52:e13544. doi:10.1111/and.13544
29. Solomon H, Wierzbicki AS, Lumb PJ, Lambert-Hammill M, Jackson G. Cardiovascular risk factors determine erectile and arterial function response to sildenafil. Am J Hypertens. 2006;19(9):915–919. doi:10.1016/j.amjhyper.2006.02.010
30. Shigemura K, Arakawa S, Kamidono S, Nakano Y, Fujisawa M. Effect of sildenafil on arterial stiffness, as assessed by pulse wave velocity, in patients with erectile dysfunction. Int J Urol. 2006;13(7):956–959. doi:10.1111/j.1442-2042.2006.01447.x
31. Bulbul E, Aydin E, Yilmaz E. Evaluation of endothelial dysfunction with cardio-ankle vascular index measurements in patients with erectile dysfunction. Andrology. 2022;10:926–930. doi:10.1111/andr.13191
32. Motil I, Kubis I, Sramkova T. Treatment of vasculogenic erectile dysfunction with Piezowave2 device. Application of low-intensity shockwaves using novel linear shockwave tissue coverage (LSTC-ED®) technique. A prospective, multicentric, placebo-controlled study. Adv Sex Med. 2016;6(02):15. doi:10.4236/asm.2016.62002
33. Yamaguchi O, Nomiya M, Andersson KE. Functional consequences of chronic bladder ischemia. Neurourol Urodyn. 2014;33(1):54–58. doi:10.1002/nau.22517
34. Tikkinen KA, Auvinen A, Johnson TM, et al. A systematic evaluation of factors associated with nocturia: the population-based FINNO Study. Am J Epidemiol. 2009;170:361–368. doi:10.1093/aje/kwp133
35. Uzun H, Çiçek Y, Kocaman SA, Durakoğlugil ME, Zorba OÜ. Increased pulse-wave velocity and carotid intima–media thickness in patients with lower urinary tract symptoms. Scand J Urol. 2013;47(5):393–398. doi:10.3109/21681805.2013.780185
36. Yabe M, Haga N, Ogawa S, et al. Atherosclerosis as a predictor of delayed recovery from lower urinary tract dysfunction after robot‐assisted laparoscopic radical prostatectomy. Neurourol Urodyn. 2016;35(8):920–925. doi:10.1002/nau.22824
37. Shirai K, Song M, Suzuki J, et al. Contradictory effects of β1-and α1-aderenergic receptor blockers on cardio-ankle vascular stiffness index (CAVI)—CAVI is independent of blood pressure. J Atheroscler Thromb. 2011;18(1):49–55. doi:10.5551/jat.3582
38. Shimizu A, Sakakibara R, Takahashi O, Tateno F, Aiba Y. Bladder overactivity and post-void residual: which relates more to systemic atherosclerotic markers? Autonom Neurosci. 2020;223:102600. doi:10.1016/j.autneu.2019.102600
39. Koguchi T, Haga N, Matsuoka K, et al. Atherosclerosis as a predictor of transient exacerbation of overactive bladder symptoms after robot‐assisted laparoscopic radical prostatectomy. Int J Urol. 2019;26(2):234–240. doi:10.1111/iju.13848
40. Hsiao SM, Tu FC, Su TC, Wu PC, Lin HH. Impact of mirabegron versus solifenacin on autonomic function and arterial stiffness in female overactive bladder syndrome: a randomized controlled trial. Sci Rep. 2022;12(1):1–8. doi:10.1038/s41598-022-18391-6
41. Hsiao SM, Su TC, Chen CH, Chang TC, Lin HH. Autonomic dysfunction and arterial stiffness in female overactive bladder patients and antimuscarinics related effects. Maturitas. 2014;79(1):65–69. doi:10.1016/j.maturitas.2014.06.001
42. Jiang Y, Fan F, Jia J, et al. Brachial–ankle pulse wave velocity is independently associated with urine albumin-to-creatinine ratio in a Chinese community-based cohort. Int Urol Nephrol. 2020;52(4):713–720. doi:10.1007/s11255-020-02404-2
43. Latif W, Karaboyas A, Tong L, et al. Uric acid levels and all-cause and cardiovascular mortality in the hemodialysis population. Clin J Am Soc Nephrol. 2011;6(10):2470–2477. doi:10.2215/CJN.00670111
44. Harada M, Fujii K, Yamada Y, et al. Relationship between serum uric acid level and vascular injury markers in hemodialysis patients. Int Urol Nephrol. 2020;52(8):1581–1591. doi:10.1007/s11255-020-02531-w
45. Nagayama D, Fujishiro K, Miyoshi T, et al. Predictive ability of arterial stiffness parameters for renal function decline: a retrospective cohort study comparing cardio-ankle vascular index, pulse wave velocity and cardio-ankle vascular index0. J Hypertens. 2022;40(7):1294–1302. doi:10.1097/HJH.0000000000003137
46. Sahinkus S, Aydin E, Aksoy MNM, Akcay C, Eynel E, Yaylaci S. Association between cardio-ankle vascular index and contrast-induced nephropathy. Hypertension. 2020;27(3.3):0–993.
47. Sarnak MJ, Levey AS. Cardiovascular disease and chronic renal disease: a new paradigm. Am J Kidney Dis. 2000;35:S117–S131. doi:10.1016/S0272-6386(00)70239-3
48. Amann K, Tyralla K. Cardiovascular changes in chronic renal failure--pathogenesis and therapy. Clin Nephrol. 2002;58:S62–72.
49. Blacher J, Guerin AP, Pannier B, Marchais SJ, Safar ME, London GM. Impact of aortic stiffness on survival in end-stage renal disease. Circulation. 1999;99:2434–2439. doi:10.1161/01.CIR.99.18.2434
50. Wang MC, Tsai WC, Chen JY, Huang JJ. Stepwise increase in arterial stiffness corresponding with the stages of chronic kidney disease. Am J Kidney Dis. 2005;45(3):494–501. doi:10.1053/j.ajkd.2004.11.011
51. Ishimura T, Endo T, Nishioka S, et al. MP59-19 Anti-atherosclerotic effect of everolimus in kidney-transplanted patients. J Urol. 2020;203(Supplement 4):e888–e888.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.