")
Back to Journals » OncoTargets and Therapy » Volume 9
Positive association between CD44 gene rs13347 C>T polymorphism and risk of cancer in Asians: a systemic review and meta-analysis
Authors Shi J, Duan Y, Pan L, Zhou X
Received 21 January 2016
Accepted for publication 13 April 2016
Published 13 June 2016 Volume 2016:9 Pages 3493—3500
DOI https://doi.org/10.2147/OTT.S104734
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Li
Jinan Shi,1 Yin Duan,2 Lei Pan,2 Xiaoxi Zhou3
1Department of Medical Oncology, Zhejiang Hospital, 2Department of Breast Surgery, Zhejiang Provincial Traditional Chinese Medical Hospital, 3Department of Respiratory Medicine, Zhejiang Hospital, Hangzhou, Zhejiang Province, People’s Republic of China
Background: Cluster of differentiation 44 (CD44) is an important surface marker of cancer stem cells in a variety of tumors. A number of previous studies have been conducted to investigate the association between CD44 gene rs13347 C>T polymorphism and cancer risk in humans; nevertheless, the results remain controversial. We therefore performed this meta-analysis to confirm the role of this polymorphism in susceptibility to human cancer.
Materials and methods: The studies published up to December 2015 were searched in PubMed, Web of Science, and China National Knowledge Infrastructure databases. Twelve eligible case–control studies were identified, involving a total of 6,982 cases and 7,430 controls. Pooled odds ratio (OR) and corresponding 95% confidence interval (CI) were calculated using a fixed or random-effect model to estimate the strength of the association.
Results: The results of the overall analyses indicated that CD44 gene rs13347 polymorphism was significantly associated with cancer risk in Asians (CT vs CC: OR =1.35, 95% CI =1.12–1.62; TT vs CC: OR =1.99, 95% CI =1.52–2.60; TT + CT vs CC: OR =1.41, 95% CI =1.16–1.71; and TT vs CC + CT: OR =1.74, 95% CI =1.41–2.14), especially in Chinese population (CT vs CC: OR =1.42, 95% CI =1.16–1.75; TT vs CC: OR =2.13, 95% CI =1.58–2.86; TT + CT vs CC: OR =1.50, 95% CI =1.21–1.87; and TT vs CC + CT: OR =1.80, 95% CI =1.43–2.26). In stratified analyses by cancer types, there was evidence for an association between this polymorphism and nasopharyngeal cancer and breast cancer, respectively.
Conclusion: The results of this meta-analysis suggest that the CD44 gene rs13347 C>T polymorphism is associated with elevated risk of human cancer in Asians, especially in Chinese population. Further well-designed studies on a larger population covering other ethnicities should be carried out to validate our results.
Keywords: cancer, CD44, polymorphism, meta-analysis
Background
Cancer is currently a serious public health burden in the world, which results from interactions between accumulations of genetic mutation and environmental risk factors.1,2 In recent years, a small subgroup of cancer cells, called cancer stem cells (CSCs), have been proved to be responsible for tumor initiation, progression, metastasis, recurrence, and drug resistance and cause cancer heterogeneity.3 Thus, eliminating CSCs is considered to be efficient and critical in cancer therapy.4 Several cell surface markers have been found to identify CSCs, and overexpression of these markers, such as cluster of differentiation 44 (CD44), CD24, CD133, CD166, and ALDH1A1, indicates severe clinical features and poor prognosis in a number of cancers.5–10 Among these cell surface markers, CD44 is one of the most frequently reported markers, which was utilized to isolate CSCs from other cancer cells.11–13
CD44, a transmembrane glycoprotein, is ubiquitously expressed in many cell types.14 As a cell surface receptor for hyaluronate and osteopontin, CD44 is involved in many biological and physiological processes including cell migration, hematopoiesis, lymphocyte homing, embryonal development, and apoptosis.14,15 Besides its regulation of cellular processes, CD44 plays a critical role in tumor cell proliferation, differentiation, invasion, and migration, which contributes to the progression and metastasis of tumors.16–19 Therefore, overexpression of CD44 leads to the development of tumors and poor prognosis of several human malignancies.20–22 In addition, it has been reported that CD44+ cancer cells represent enhanced resistance to chemotherapy in the nude mice-engrafted tumor model.23,24 Recent studies have revealed that the genetic variants of CD44 gene could influence tumor cell growth and migration,25,26 which were associated with the risk prediction and prognosis of various human cancers.27–29
The gene encoding CD44 is located on chromosome 11p13.30 A growing number of studies have been carried out to investigate the effects of several CD44 gene single nucleotide polymorphisms (SNPs) on cancer risk. Among them, the rs13347 C>T polymorphism, located on the 3′-untranslated region (3′-UTR) of CD44 gene, is the most frequently studied.20,31,32 This SNP might influence the CD44 gene expression, since it has been reported that subjects carrying TT and CT genotypes had remarkably higher levels of CD44 protein than those carrying CC genotype in breast cancer, nasopharyngeal carcinoma, and acute myeloid leukemia.28,31,33
To date, a number of case–control studies have been conducted to evaluate the role of CD44 gene rs13347 polymorphism in predisposition to several human cancers.28,29,32–35 Nevertheless, the results from different articles remain controversial. To clarify the association between CD44 gene rs13347 polymorphism and risk of cancer, we performed this meta-analysis by integrating data from eligible published studies.
Materials and methods
Search strategy
Relevant reports were retrieved by searching the electronic databases: PubMed, Web of Science, and China National Knowledge Infrastructure (CNKI; from inception to December 20, 2015), using the following keywords: (“CD44”) and (“tumor” or “cancer” or “carcinoma” or “neoplasm” or “malignancy”) and (“polymorphism” or “polymorphisms” or “SNP” or “variant” or “variation”). The search was filtered to English-language journals in PubMed. Besides, we also performed a manual search among the references of the relevant publications and related articles. The studies with overlapping data by the same investigators or based on the same population were checked prudently, and the most recent articles covering the largest numbers of cases and controls would be included.
Inclusion and exclusion criteria
The eligible studies in this meta-analysis were required to strictly follow the predetermined criteria: 1) use a case–control study design, 2) evaluate the association between CD44 rs13347 C>T polymorphism and risk of cancer, and 3) report an estimation of odds ratio (OR) and 95% confidence interval (CI), or sufficient data to allow calculation of these two statistics. The main exclusion criteria were studies 1) that did not use a case–control design (eg, case reports, letters, animal studies, reviews, and editorials), 2) that are duplicate of previous publications, 3) that involve inherited cancers, 4) with sample size of cases or controls <100, and 5) in which genotype distribution of controls is not in agreement with the Hardy–Weinberg equilibrium.
Data extraction
All the eligible studies were reviewed by two authors independently to extract useful data. The following information were collected: the name of the first author, the year of publication, the ethnicity of study population, the country of origin, sample size of cases and controls, source of controls (hospital based or population based), genotyping method, and genotype distributions of cases and controls. The disagreements in this step were solved by rechecking the original data to reach a consensus.
Statistical analysis
Hardy–Weinberg equilibrium was estimated by the goodness-of-fit test based on the chi-square test in the control group of each study.36 Pooled analysis was conducted to estimate the strength of the association between CD44 rs13347 C>T polymorphism and cancer risk, using an OR with a corresponding 95% CI. The pooled ORs were calculated by comparisons with a codominant model (CT vs CC and TT vs CC), a dominant model (TT + CT vs CC), and a recessive model (TT vs CC + CT). The values of the pooled ORs were tested by the Z-test.37 Stratified analyses were further performed based on country (People’s Republic of China or India), specific cancer types (nasopharyngeal cancer, gallbladder cancer, or breast cancer), source of controls (hospital based or population based), and genotyping method (TaqMan or matrix-assisted laser desorption/ionization time-of-flight). Heterogeneity among the included studies was evaluated by the chi-square-based Q-test.38 Pooled ORs were calculated using a fixed (Mantel–Haenszel method39) or a random (DerSimonian–Laird method40) effective model, according to the absence (P>0.10 and I2<50%) or presence (P<0.10 or I2>50%) of heterogeneity. Sensitivity analyses were performed by omitting one study each time to evaluate the stability of the results. The potential publication bias of the included studies was assessed by Begg’s funnel plots graphically and Egger’s test quantitatively.41
All the statistical calculations were carried out with Stata/SE software Version 12.0 (StataCorp LP, College Station, TX, USA), using two-sided P-values, and P<0.05 was considered to be significant.
Results
Literature search and characteristics of eligible studies
A total of 890 potential relevant records were retrieved through the search strategy described previously. Eight hundred and seventy records were excluded after title or abstract scanning. After full-text reviewing, eight studies were excluded. Finally, 12 studies were eligible for pooled analysis. The flow process of detailed literature search and study selection is shown in Figure 1.
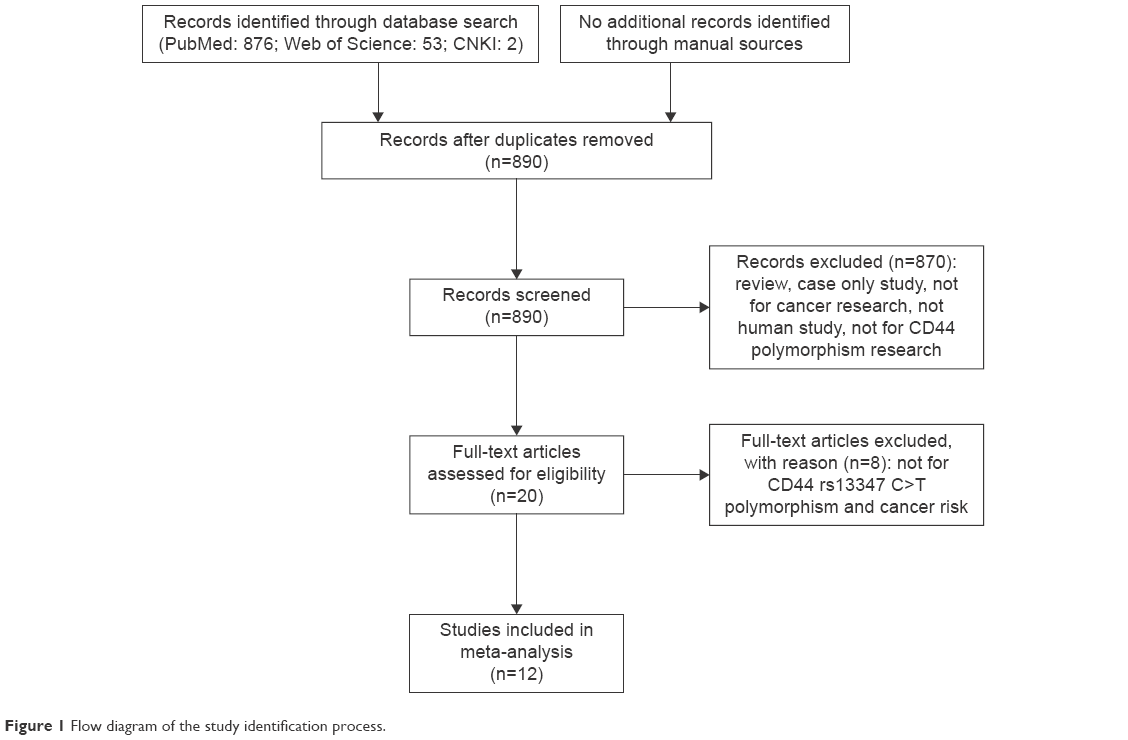 | Figure 1 Flow diagram of the study identification process. |
There were 12 case–control studies included in this meta-analysis,28,29,31–35,42–46 involving a total of 6,982 cases and 7,430 controls. All the studies were conducted on an Asian population. Among them, nine originated from the People’s Republic of China and the other three from India. There was no study conducted on Caucasians or Africans. Cancer types included bladder cancer, non-small-cell lung cancer, gallbladder cancer, colorectal cancer, nasopharyngeal cancer, hepatocellular carcinoma, oral cancer, breast cancer, and acute myeloid leukemia. The distribution of genotypes in all the control groups was in agreement with Hardy–Weinberg equilibrium. The characteristics of each eligible study are listed in Table 1.
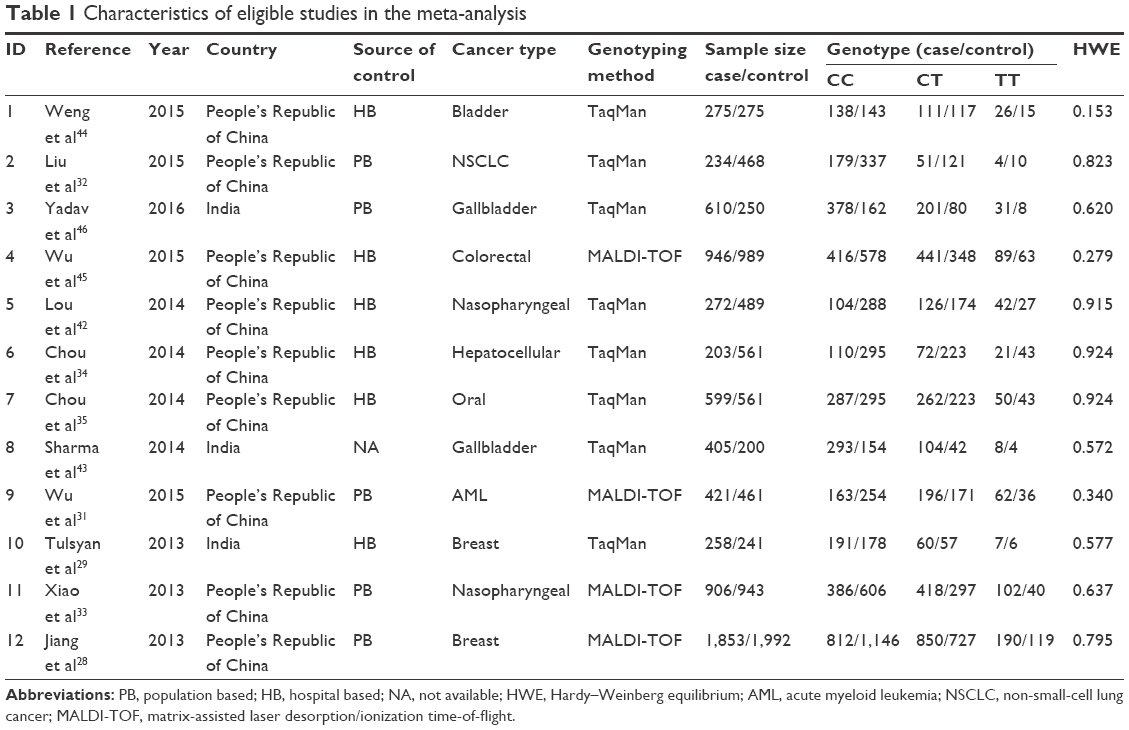 | Table 1 Characteristics of eligible studies in the meta-analysis |
Quantitative synthesis
The pooled results of the present meta-analysis are shown in Table 2 and Figure 2. There was an association between CD44 gene rs13347 polymorphism and risk of cancer in the overall analyses. Significantly elevated cancer risk was revealed in the codominant genetic model (CT vs CC: OR =1.35, 95% CI =1.12–1.62 and TT vs CC: OR =1.99, 95% CI =1.52–2.60), dominant model (TT + CT vs CC: OR =1.41, 95% CI =1.16–1.71), and recessive model (TT vs CC + CT: OR =1.74, 95% CI =1.41–2.14). In the subgroup analyses stratified by country, there was evidence in Chinese population for an association between this SNP and cancer risk (CT vs CC: OR =1.42, 95% CI =1.16–1.75; TT vs CC: OR =2.13, 95% CI =1.58–2.86; TT + CT vs CC: OR =1.50, 95% CI =1.21–1.87; and TT vs CC + CT: OR =1.80, 95% CI =1.43–2.26). According to the source of control, both population based and hospital based subgroups were linked to cancer risk. For specific cancer types, increased risk among studies of nasopharyngeal cancer and breast cancer was observed in several genetic models.
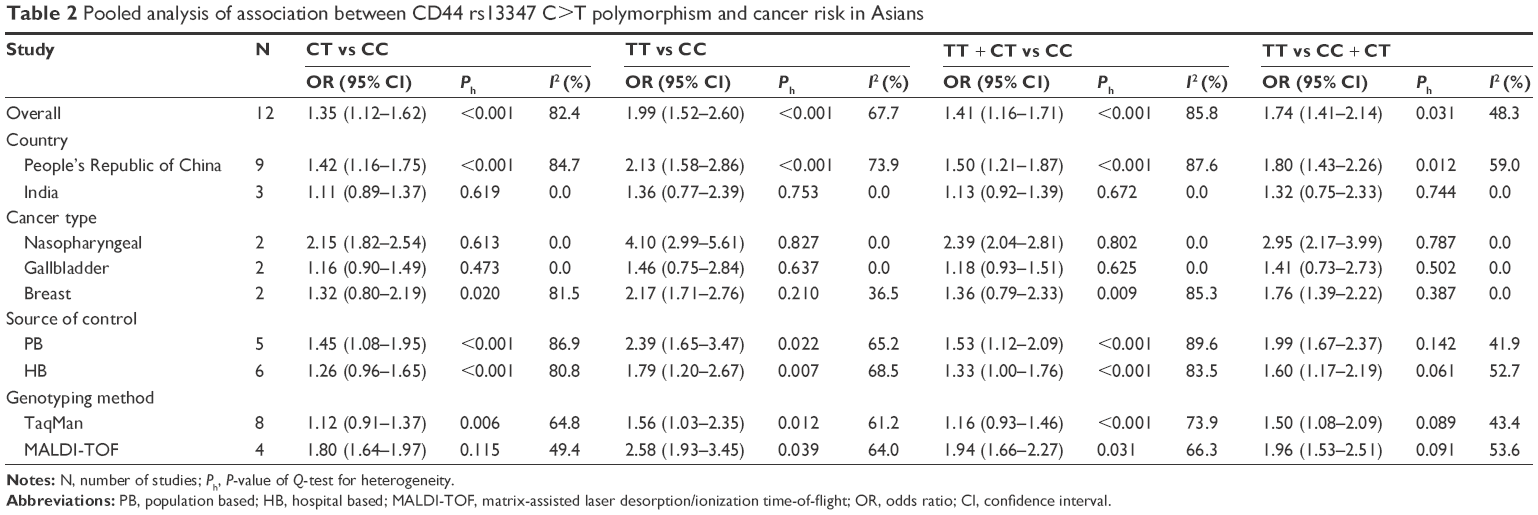 | Table 2 Pooled analysis of association between CD44 rs13347 C>T polymorphism and cancer risk in Asians |
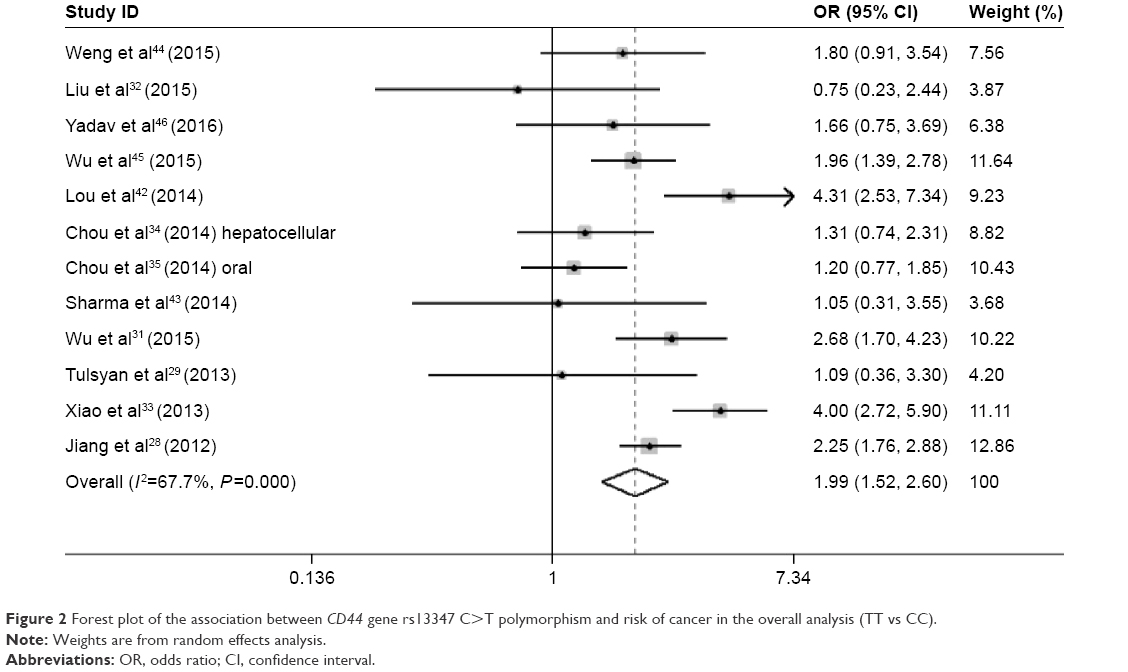 | Figure 2 Forest plot of the association between CD44 gene rs13347 C>T polymorphism and risk of cancer in the overall analysis (TT vs CC). |
Test for heterogeneity and sensitivity analysis
There was significant heterogeneity in the overall comparisons under all the genetic models (CT vs CC: P<0.001 and I2=82.4% for heterogeneity, TT vs CC: P<0.001 and I2=67.7% for heterogeneity, TT + CT vs CC: P<0.001 and I2=85.8% for heterogeneity, and TT vs CC + CT: P=0.031 and I2=48.3% for heterogeneity; Table 2). The source of heterogeneity was investigated by covariates, such as country, cancer type, source of control, and genotype method. According to subgroup analyses, country and cancer type might be the source of heterogeneity. To explore the main origin of heterogeneity, a meta-regression analysis was performed in the comparison TT vs CC, which indicated that cancer type contributed to the most proportion in heterogeneity. Moreover, two studies on nasopharyngeal cancer33,42 were under suspicion. After omitting these two studies, the pooled OR was not altered (TT vs CC: OR =1.74, 95% CI =1.39–2.16), whereas the heterogeneity remarkably decreased (TT vs CC: P=0.110 and I2=34.7% for heterogeneity).
Sensitivity analysis was performed, and the pooled ORs were not influenced qualitatively in all the genetic models by removing any single study, which indicated that the pooled results of this meta-analysis were statistically stable (Figure 3).
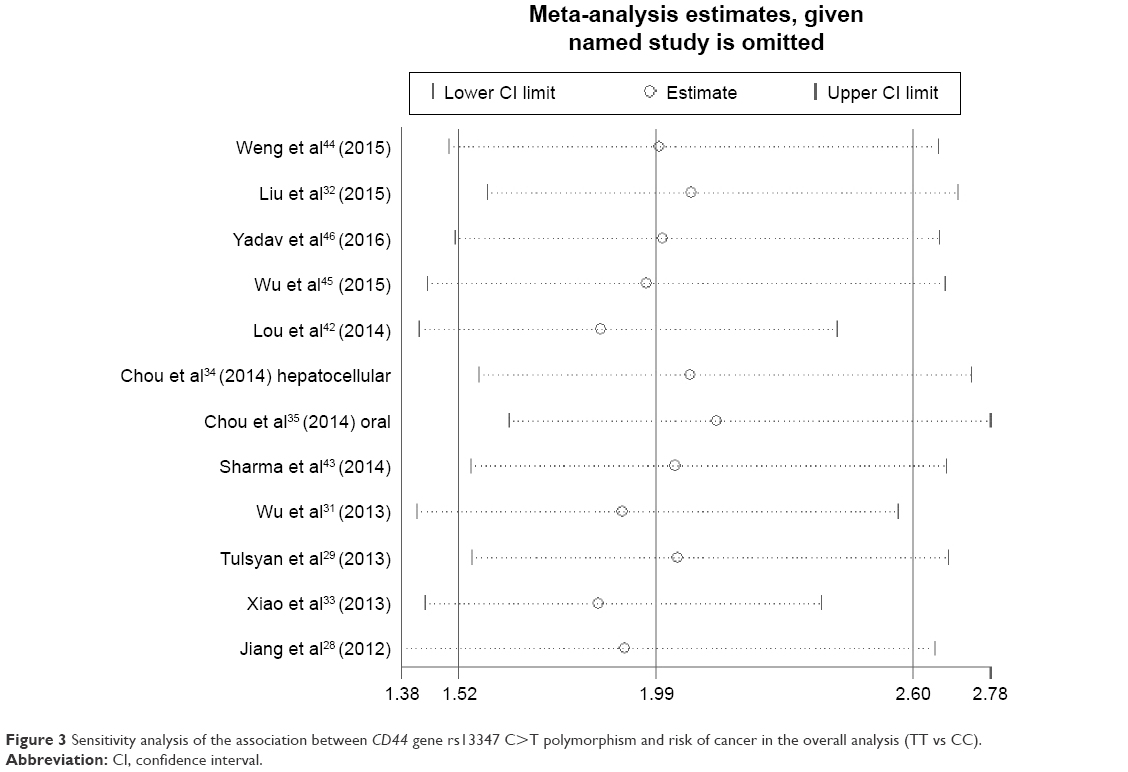 | Figure 3 Sensitivity analysis of the association between CD44 gene rs13347 C>T polymorphism and risk of cancer in the overall analysis (TT vs CC). |
Publication bias
The potential publication bias of the eligible studies was assessed by Begg’s funnel plots graphically and Egger’s test statistically. The shapes of funnel plots in all the genetic models did not indicate any evidence of an obvious asymmetry (Figure 4). Meanwhile, Egger’s test revealed that there was no publication bias either (CT vs CC: P=0.139, TT vs CC: P=0.755, TT + CT vs CC: P=0.186, and TT vs CC + CT: P=0.975).
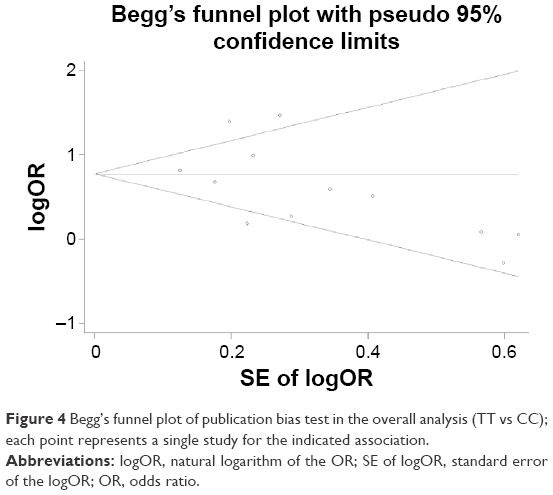 | Figure 4 Begg’s funnel plot of publication bias test in the overall analysis (TT vs CC); each point represents a single study for the indicated association. |
Discussion
Cancer is a group of heterogeneous diseases that result from genetic and environmental factors, as well as their interactions. According to CSC theory, CSCs can drive cancer initiation, progression, and metastasis.3 As an important CSC surface maker in variant tumors, CD44 is reportedly a risk factor and poor prognostic molecular marker in various cancers.47–50 CD44 plays a crucial role in the invasion and migration of cancer cells. In addition, overexpression of CD44 in primary tumors has been revealed to be associated with early metastasis in several human cancers.20,29,51 CD44 gene rs13347 C>T polymorphism is a common genetic variation in the 3′-UTR. It has been proved that the expression of CD44 was modulated by mRNAs, and rs13347 C>T polymorphism could alter has-mir-509-3p-mediated CD44 gene expression activity. Recently, a number of studies have been carried out to evaluate the association between this SNP and risk of cancer; however, the results were conflicting. The possible reason may be that the effects of CD44 on the development of different cancer types are not the same.
To our knowledge, the present meta-analysis, including 6,982 cases and 7,430 controls from 12 case–control studies, is the first comprehensive study to assess the association between CD44 gene rs13347 polymorphism and risk of cancer. We found an association between CD44 gene rs13347 polymorphism and human cancer risk by pooling all the data from eligible studies. The results were robust because the pooled ORs did not alter statistically in sensitivity analyses. Stratified analyses suggested that this association was mainly in a Chinese population. According to specific cancer types, this polymorphism was linked to elevated risk of gallbladder cancer, nasopharyngeal cancer, and breast cancer, the significance of which was limited because there were only two studies for each cancer type. Since there was significant heterogeneity by the Q-test in all the genetic models, a meta-regression analysis was performed to explore the origin of heterogeneity. As a result, different cancer types were considered to be the main source of interstudy variance, especially two studies on nasopharyngeal cancer. By removing these two studies, the heterogeneity significantly decreased but pooled ORs were not altered. However, this kind of heterogeneity was hard to eliminate in the present meta-analysis, because there were only one or two studies for one specific cancer type. Moreover, pooling data from different cancer types might affect the significance of this meta-analysis because different cancer types might give rise to different host responses, and the interactions between different environmental factors and host might also influence the susceptibility to different cancer types.
Some limitations of the present meta-analysis should be pointed out. First, the pooled results were calculated based on unadjusted estimates, which limited us to perform a more precise assessment on adjusted estimates by several important factors such as sex, age, lifestyle, etc. Thus, lack of the baseline information restricted further evaluation of the potential interactions, because malignancy predisposition might be influenced by gene–gene and gene–environment interactions. Second, most of the included studies just focused on the relationship between CD44 gene rs13347 polymorphism and cancer risk, which made it hard to assess the effects of CD44 gene haplotypes composed of different CD44 gene SNPs on carcinogenesis. There was evidence that CD44 gene rs187115 A>G and rs115214213 T>C polymorphisms were associated with cancer risk.35,42,44 Thus, the status of other CD44 gene polymorphisms might cover up the effects of rs13347 T>C polymorphism, which could lead to controversial results among different studies.
Despite these limitations, advantages in this meta-analysis should also be acknowledged. First, the statistical power was remarkably increased since we pooled a substantial number of cases and controls. Second, the quality of all the eligible studies met the inclusion criteria completely and strictly. Third, there was no publication bias observed through Begg’s funnel plots and Egger’s test, which indicated that the pooled outcomes should be unbiased.
Conclusion
The results of the present meta-analysis were robust and credible. The relationship between CD44 gene rs13347 polymorphism and cancer risk was assessed, and this SNP was associated with elevated cancer risk in Asians. To draw a more conclusive result, further studies should be conducted with more detailed information on individuals and environmental factors, concerning the effects of different haplotypes and other SNPs and enrolling properly identified cases and well-matched controls, especially in other ethnicities including Africans and Caucasians, to validate the role of CD44 gene rs13347 C>T polymorphism in carcinogenesis.
Acknowledgment
This work was granted by National Natural Science Foundation of China (grant no 91229104).
Disclosure
The authors report no conflicts of interest in this work.
References
Hoeijmakers JH. Genome maintenance mechanisms for preventing cancer. Nature. 2001;411(6835):366–374. | ||
Bredberg A. Cancer: more of polygenic disease and less of multiple mutations? A quantitative viewpoint. Cancer. 2011;117(3):440–445. | ||
Nguyen LV, Vanner R, Dirks P, Eaves CJ. Cancer stem cells: an evolving concept. Nat Rev Cancer. 2012;12(2):133–143. | ||
Bomken S, Fiser K, Heidenreich O, Vormoor J. Understanding the cancer stem cell. Br J Cancer. 2010;103(4):439–445. | ||
Wang K, Chen X, Zhan Y, et al. Increased expression of ALDH1A1 protein is associated with poor prognosis in clear cell renal cell carcinoma. Med Oncol. 2013;30(2):574. | ||
Mikami S, Mizuno R, Kosaka T, Saya H, Oya M, Okada Y. Expression of TNF-alpha and CD44 is implicated in poor prognosis, cancer cell invasion, metastasis and resistance to the sunitinib treatment in clear cell renal cell carcinomas. Int J Cancer. 2015;136(7):1504–1514. | ||
Kim K, Ihm H, Ro JY, Cho YM. High-level expression of stem cell marker CD133 in clear cell renal cell carcinoma with favorable prognosis. Oncol Lett. 2011;2(6):1095–1100. | ||
Lee JH, Kim SH, Lee ES, Kim YS. CD24 overexpression in cancer development and progression: a meta-analysis. Oncol Rep. 2009;22(5):1149–1156. | ||
Wang K, Xu J, Zhang J, Huang J. Prognostic role of CD133 expression in colorectal cancer: a meta-analysis. BMC Cancer. 2012;12:573. | ||
Ni C, Zhang Z, Zhu X, et al. Prognostic value of CD166 expression in cancers of the digestive system: a systematic review and meta-analysis. PLoS One. 2013;8(8):e70958. | ||
Moon JH, Kwak SS, Park G, et al. Isolation and characterization of multipotent human keloid-derived mesenchymal-like stem cells. Stem Cells Dev. 2008;17(4):713–724. | ||
Cho JS, Park JH, Kang JH, Kim SE, Park IH, Lee HM. Isolation and characterization of multipotent mesenchymal stem cells in nasal polyps. Exp Biol Med. 2015;240(2):185–193. | ||
Al-Hajj M, Wicha MS, Benito-Hernandez A, Morrison SJ, Clarke MF. Prospective identification of tumorigenic breast cancer cells. Proc Natl Acad Sci U S A. 2003;100(7):3983–3988. | ||
Goodison S, Urquidi V, Tarin D. CD44 cell adhesion molecules. Mol Pathol. 1999;52(4):189–196. | ||
Ponta H, Sherman L, Herrlich PA. CD44: from adhesion molecules to signalling regulators. Nat Rev Mol Cell Biol. 2003;4(1):33–45. | ||
Zoller M. CD44: can a cancer-initiating cell profit from an abundantly expressed molecule? Nat Rev Cancer. 2011;11(4):254–267. | ||
Marhaba R, Zoller M. CD44 in cancer progression: adhesion, migration and growth regulation. J Mol Histol. 2004;35(3):211–231. | ||
Hill A, McFarlane S, Johnston PG, Waugh DJ. The emerging role of CD44 in regulating skeletal micrometastasis. Cancer Lett. 2006;237(1):1–9. | ||
Udabage L, Brownlee GR, Nilsson SK, Brown TJ. The over-expression of HAS2, Hyal-2 and CD44 is implicated in the invasiveness of breast cancer. Exp Cell Res. 2005;310(1):205–217. | ||
Luo Z, Wu RR, Lv L, et al. Prognostic value of CD44 expression in non-small cell lung cancer: a systematic review. Int J Clin Exp Pathol. 2014;7(7):3632–3646. | ||
Brown RL, Reinke LM, Damerow MS, et al. CD44 splice isoform switching in human and mouse epithelium is essential for epithelial-mesenchymal transition and breast cancer progression. J Clin Invest. 2011;121(3):1064–1074. | ||
Ozawa M, Ichikawa Y, Zheng YW, et al. Prognostic significance of CD44 variant 2 upregulation in colorectal cancer. Br J Cancer. 2014;111(2):365–374. | ||
Marhaba R, Klingbeil P, Nuebel T, Nazarenko I, Buechler MW, Zoeller M. CD44 and EpCAM: cancer-initiating cell markers. Curr Mol Med. 2008;8(8):784–804. | ||
Wang SJ, Bourguignon LY. Role of hyaluronan-mediated CD44 signaling in head and neck squamous cell carcinoma progression and chemoresistance. Am J Pathol. 2011;178(3):956–963. | ||
Bertaux-Skeirik N, Feng R, Schumacher MA, et al. CD44 plays a functional role in Helicobacter pylori-induced epithelial cell proliferation. PLoS Pathog. 2015;11(2):e1004663. | ||
Dong C, Ye DX, Zhang WB, Pan HY, Zhang ZY, Zhang L. Overexpression of c-fos promotes cell invasion and migration via CD44 pathway in oral squamous cell carcinoma. J Oral Pathol Med. 2015;44(5):353–360. | ||
Ko YH, Won HS, Jeon EK, et al. Prognostic significance of CD44s expression in resected non-small cell lung cancer. BMC Cancer. 2011;11:340. | ||
Jiang L, Deng J, Zhu X, et al. CD44 rs13347 C>T polymorphism predicts breast cancer risk and prognosis in Chinese populations. Breast Cancer Res. 2012;14(4):R105. | ||
Tulsyan S, Agarwal G, Lal P, Agrawal S, Mittal RD, Mittal B. CD44 gene polymorphisms in breast cancer risk and prognosis: a study in North Indian population. PLoS One. 2013;8(8):e71073. | ||
Goodfellow PN, Banting G, Wiles MV, et al. The gene, MIC4, which controls expression of the antigen defined by monoclonal antibody F10.44.2, is on human chromosome 11. Eur J Immunol. 1982;12(8):659–663. | ||
Wu H, Deng J, Zheng J, et al. Functional polymorphisms in the CD44 gene and acute myeloid leukemia cancer risk in a Chinese population. Mol Carcinog. 2015;54(2):102–110. | ||
Liu Y, Qing H, Su X, Wang C, Li Z, Liu S. Association of CD44 gene polymorphism with survival of NSCLC and risk of bone metastasis. Med Sci Monit. 2015;21:2694–2700. | ||
Xiao M, Hu S, Zhang L, Huang J, Jiang H, Cai X. Polymorphisms of CD44 gene and nasopharyngeal carcinoma susceptibility in a Chinese population. Mutagenesis. 2013;28(5):577–582. | ||
Chou YE, Hsieh MJ, Chiou HL, Lee HL, Yang SF, Chen TY. CD44 gene polymorphisms on hepatocellular carcinoma susceptibility and clinicopathologic features. Biomed Res Int. 2014;2014:231474. | ||
Chou YE, Hsieh MJ, Hsin CH, et al. CD44 gene polymorphisms and environmental factors on oral cancer susceptibility in Taiwan. PLoS One. 2014;9(4):e93692. | ||
Haber M. Exact significance levels of goodness-of-fit tests for the Hardy-Weinberg equilibrium. Hum Hered. 1981;31(3):161–166. | ||
Breslow NE, Day NE. Statistical methods in cancer research. Volume II – the design and analysis of cohort studies. IARC Sci Publ. 1987;82:1–406. | ||
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. | ||
Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959;22(4):719–748. | ||
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–188. | ||
Sterne JA, Gavaghan D, Egger M. Publication and related bias in meta-analysis: power of statistical tests and prevalence in the literature. J Clin Epidemiol. 2000;53(11):1119–1129. | ||
Lou F, Ma HN, Xu L, Chen M, Zhu YB. Two polymorphisms of CD44 3′UTR weaken the binding of miRNAs and associate with naso-pharyngeal carcinoma in a Chinese population. Eur Rev Med Pharmacol Sci. 2014;18(17):2444–2452. | ||
Sharma KL, Yadav A, Gupta A, et al. Association of genetic variants of cancer stem cell gene CD44 haplotypes with gallbladder cancer susceptibility in North Indian population. Tumour Biol. 2014;35(3):2583–2589. | ||
Weng WC, Huang YH, Yang SF, et al. Effect of CD44 gene polymorphisms on risk of transitional cell carcinoma of the urinary bladder in Taiwan. Tumour Biol. Epub 2015 Dec 12. | ||
Wu XM, Yang HG, Zheng BA, Cao HF, Hu ZM, Wu WD. Functional genetic variations at the microRNA binding-site in the CD44 gene are associated with risk of colorectal cancer in Chinese populations. PLoS One. 2015;10(5):e0127557. | ||
Yadav A, Gupta A, Rastogi N, et al. Association of cancer stem cell markers genetic variants with gallbladder cancer susceptibility, prognosis, and survival. Tumour Biol. 2016;37(2):1835–1844. | ||
Korski K, Malicka-Durczak A, Breborowicz J. Expression of stem cell marker CD44 in prostate cancer biopsies predicts cancer grade in radical prostatectomy specimens. Pol J Pathol. 2014;65(4):291–295. | ||
Jing F, Kim HJ, Kim CH, Kim YJ, Lee JH, Kim HR. Colon cancer stem cell markers CD44 and CD133 in patients with colorectal cancer and synchronous hepatic metastases. Int J Oncol. 2015;46(4):1582–1588. | ||
Nosrati A, Naghshvar F, Khanari S. Cancer stem cell markers CD44, CD133 in primary gastric adenocarcinoma. Int J Mol Cell Med. 2014;3(4):279–286. | ||
Wang H, Tan M, Zhang S, et al. Expression and significance of CD44, CD47 and c-met in ovarian clear cell carcinoma. Int J Mol Sci. 2015;16(2):3391–3404. | ||
Taira N, Kawabata T, Ichi T, et al. Long-term survival after surgical treatment of metachronous bilateral adrenal metastases of non-small cell lung carcinoma. Am J Case Rep. 2014;15:444–446. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.