")
Back to Journals » OncoTargets and Therapy » Volume 11
Positioning error and expanding margins of planning target volume with kilovoltage cone beam computed tomography for prostate cancer radiotherapy
Authors Wang G, Wang WL, Liu YQ, Dong HM, Hu YX
Received 29 September 2017
Accepted for publication 18 December 2017
Published 6 April 2018 Volume 2018:11 Pages 1981—1988
DOI https://doi.org/10.2147/OTT.S152915
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ingrid Espinoza
Gang Wang, Wen-Ling Wang, Yi-Qun Liu, Hong-Min Dong, Yin-Xiang Hu
Department of Abdominal Oncology, Affiliated Hospital of Guizhou Medical University, Guizhou Cancer Hospital, Guiyang, People’s Republic of China
Objective: In this study, prostate cancer patients were treated with image-guided radiotherapy (IGRT). The translational positioning errors were discussed to provide the basis for determining margins of the planning target volume (PTV).
Methods: Thirty prostate cancer patients were treated with radical radiotherapy using the IGRT system. Patients were placed in the supine position and underwent kilovoltage cone beam computed tomography (KVCBCT) scans before radiotherapy. A total of 447 images were acquired. The translational positioning errors were obtained in three linear directions which were X (left-to-right), Y (superior-to-inferior) and Z (anterior-to-posterior) axes (denoted as Lx, Ly and Lz) through the contrast between images adjusted with gray and manual registrations and the planning CT images. Rotational errors were denoted as Rx, Ry and Rz.
Results: Uncorrected translational errors Lx, Ly and Lz in the 251 positioning images were all higher than those after correction, and the differences were all statistically significant (P=0.000, 0.037 and 0.004, respectively). For rotational errors Rx, Ry and Rz, only Rx had a significant difference before and after correction (P=0.044). Before correction, PTV margins in the X, Y and Z directions were 0.61, 0.78 and 0.41 cm, respectively; after correction, these were 0.17, 0.12 and 0.17 cm, respectively.
Conclusion: KVCBCT can be applied to measure positioning errors in prostate cancer radiotherapy and correct these errors in real time through the 6° robotic patient positioning system, in order to improve patient positioning accuracy. The application of IGRT with KVCBCT may reduce PTV margins.
Keywords: prostate cancer, image-guided radiotherapy, kilovoltage cone beam CT, positioning error, planning target volume
Introduction
Radiotherapy is one of the radical treatments for prostate cancer. In recent years, with the development of intensity-modulated radiation therapy, the dose and effect of radiotherapy for prostate cancer have been further improved. Accurate radiotherapy technology requires the reduction of the influence of positioning errors. However, positioning error remains as one of the obstacles in further improving the accuracy of treatment. External error size is an important factor of clinical target volume (CTV)-to-planning target volume (PTV) margins (MPTV) in radiotherapy. At present, MPTV is usually 10 mm in the absence of corrective measures.1
In recent years, with the extensive use of image-guided radiotherapy (IGRT) technology in clinics, related clinical studies have revealed significant differences in positioning errors in different directions.2 The rate of error for ≥6 mm in the anterior-to-posterior direction was 42%, and the rates were 17% and 22% in the upper-to-lower and right-to-left directions. In addition, Palombarini et al3 revealed that in IGRT treatment for prostate cancer patients, except the backward direction, margins in other directions were significantly reduced. Based on significant differences in positioning errors in different directions and the significant reduction of positioning errors on the basis of the application of IGRT,3 it remains to be determined whether it is reasonable to uniformly expand the CTV-to-PTV margins in all directions by 10 mm in the radical radiotherapy for prostate cancer. This is a question that is worth discussing.
To further determine the reasonable expanding range of CTV-to-PTV margins in IGRT treatment for prostate cancer, the Department of Abdominal Tumor in our hospital adopted kilovoltage cone beam computed tomography (KVCBCT)-guided three-dimensional conformal intensity-modulated radiotherapy to treat 30 prostate cancer patients using the Elekta Synergy System. At the same time, the expanding margins were calculated according to the formula for MPTV (MPTV=2.5Σ+0.7δ) and through positioning errors before and after correction, to provide a theoretical basis for clinically determining reasonable expanding margins.4
Patients and methods
General information
Data of 30 prostate cancer patients, who underwent radical radiotherapy in the Department of Peritoneal Tumor of the Cancer Hospital of Guizhou Province from April 2012 to December 2015, were collected. Sample supplementary clinical data are as follows: the median age of these patients was 74 years (52–85 years), and the median Gleason score was 7 points (5–10 points). Before treatment, the median level of prostate-specific antigen was 14.23 ng/mL (9.37–259.20 ng/mL). The pathological types were all adenocarcinomas. Staging was carried out according to the 7th edition of the American Joint Committee on Cancer (AJCC) staging in 2010: 11 cases were Stage II, 17 cases were Stage III and two cases were Stage IV. This study was conducted in accordance with the Declaration of Helsinki. This study was approved by the ethics committee of Guizhou Cancer Hospital. Written informed consent was obtained from all participants.
CT simulation positioning
Patients were placed in the supine position and fixed on the frame composed of thermoplastic film. Each patient underwent CT scans with a thickness of 5 mm, when the rectum was empty and the bladder was fully filled. The acquired images were used for the outline of the radiotherapy target area and the design of the radiotherapy program, as well as in planning CT images in a rectangular coordinate system, in which the centers were also the tumor centers.
Acquisition of KVCBCT images and positioning errors
Patients were placed in a position and status the same as that used during the simulation positioning. Before each treatment, KVCBCT scanning started from 180.1° and ended at 180°. Hence, a 359.9° scan was completed to obtain the pretreatment KVCBCT image.
By matching the pretreatment KVCBCT images with the planning CT images, translational positioning errors in the X (left-to-right), Y (superior-to-inferior) and Z (anterior-to-posterior) axes (denoted as Lx, Ly and Lz) and rotational errors Rx, Ry and Rz (with central axes located at the X, Y and Z axes, respectively) were acquired. Correction standard was set at a translational error of <3 mm and a rotational error of <2°. When errors exceeded the correction standard, the position was corrected by a 6° robotic patient positioning system. After correction, the aforementioned procedures were repeated to acquire the posttreatment KVCBCT images. Then, the corrected positioning errors were obtained by comparing these images with the planning CT images. Treatment was carried out until the errors met the standard. Pre- and posttreatment KVCBCT images were matched with the planning CT images using gray and manual registrations: KVCBCT images and planning CT images were concentrically matched using the gray registration pattern provided by the IGRT system. Then, the anatomical structure that inosculated best between the two kinds of images in three dimensions was determined. If the inosculation was not satisfied, manual adjustments were performed until maximum inosculation was achieved. The whole setup procedure is shown in Figure 1.
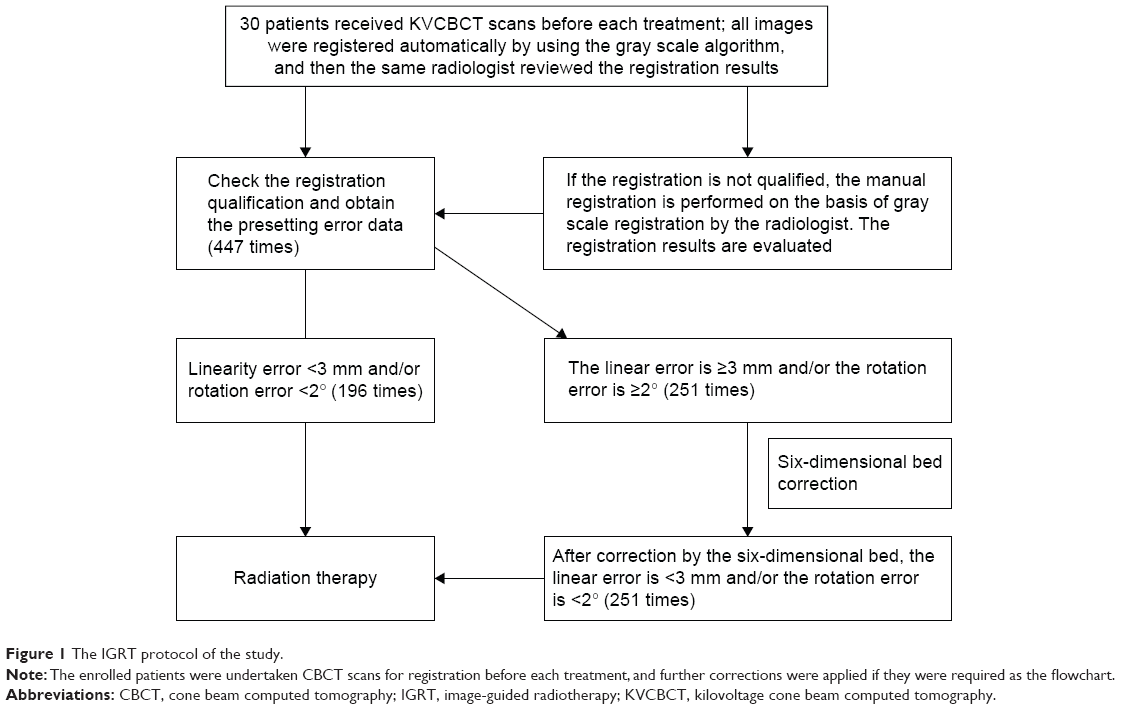 | Figure 1 The IGRT protocol of the study. |
Calculation of CTV-to-PTV margins
The systemic error of positioning for each patient was expressed as the average value  of all positioning errors for this patient, while random error was expressed as the SD of all positioning errors of this patient. Total systematic error was expressed as the average value of systematic errors in all patients (denoted as μ), while total SD was denoted as Σ. Total random error was denoted as δ, which is the square root of the average value of the random errors in all patients.5 The corrected MPTV was calculated according to the formula for CTV-to-PTV margins: MPTV=2.5Σ+0.7δ.
of all positioning errors for this patient, while random error was expressed as the SD of all positioning errors of this patient. Total systematic error was expressed as the average value of systematic errors in all patients (denoted as μ), while total SD was denoted as Σ. Total random error was denoted as δ, which is the square root of the average value of the random errors in all patients.5 The corrected MPTV was calculated according to the formula for CTV-to-PTV margins: MPTV=2.5Σ+0.7δ.
Statistical analysis
Data were analyzed by statistical analysis software SPSS 11.5. Pre- and post-correction data were compared using paired t-test. P<0.05 was considered statistically significant.
Results
- Total positioning errors: The last KVCBCT images of three patients were not registered because they did not complete the full-dose radiotherapy. Therefore, a total of 447 KVCBCT images were acquired from 30 patients through KVCBCT scanning before each treatment, in which 196 images were found to have translational errors <3 mm in three directions and rotational errors <2°. Hence, no correction was required. The other 251 images exceeded the aforementioned range and required correction. This was obtained through the 6° robotic patient positioning system.
- The mean and standard deviation of translational errors in three dimensions and rotational errors for each patient before correction are shown in Table 1. Corrected results are shown in Table 2.
- The mean of the uncorrected translational errors Lx, Ly and Lz in the 251 positioning images were 0.057±0.206, −0.095±0.401 and −0.112±0.259 cm, respectively. After correction, the values were −0.015±0.080, −0.029±0.072 and −0.055±0.069 cm, respectively. Through comparison using paired t-test, it was found that differences in errors in the X, Y and Z axes before and after correction were statistically significant (t=4.59, −2.10 and −2.94; P=0.000, 0.037 and 0.004). Among rotational errors Rx, Ry and Rz, only Rx had a significant difference before and after correction (P=0.044, 0.645 and 0.128; Table 3).
- In the X, Y and Z axes, the calculated CTV-to-PTV margins, MPTV, before and after correction were 0.61, 0.78 and 0.41 cm, respectively, and 0.17, 0.12 and 0.17 cm, respectively. The margin differences of before and after correction were 0.44, 0.66, and 0.24 cm, respectively, corresponding to 72%, 85% and 56% of the margins before correction, respectively (Table 4).
 | Table 1 System and random errors in three dimensions and rotational directions for 30 patients before correction |
 denotes the average value of all positioning errors for each patient. Lx, Ly and Lz denote translational positioning errors in the X, Y and Z axes, respectively. Rx, Ry and Rz denote rotational errors with central axes located at the X, Y and Z axes, respectively.
denotes the average value of all positioning errors for each patient. Lx, Ly and Lz denote translational positioning errors in the X, Y and Z axes, respectively. Rx, Ry and Rz denote rotational errors with central axes located at the X, Y and Z axes, respectively.
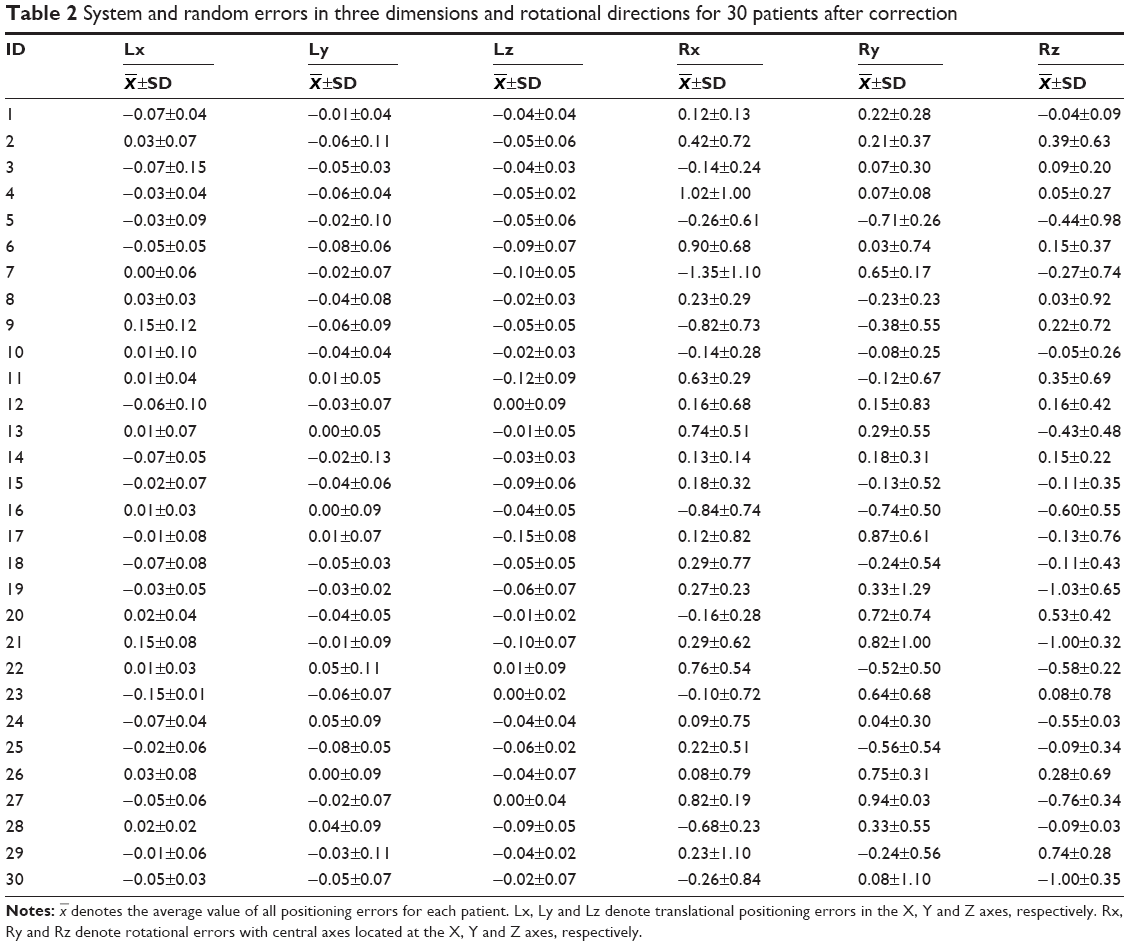 | Table 2 System and random errors in three dimensions and rotational directions for 30 patients after correction |
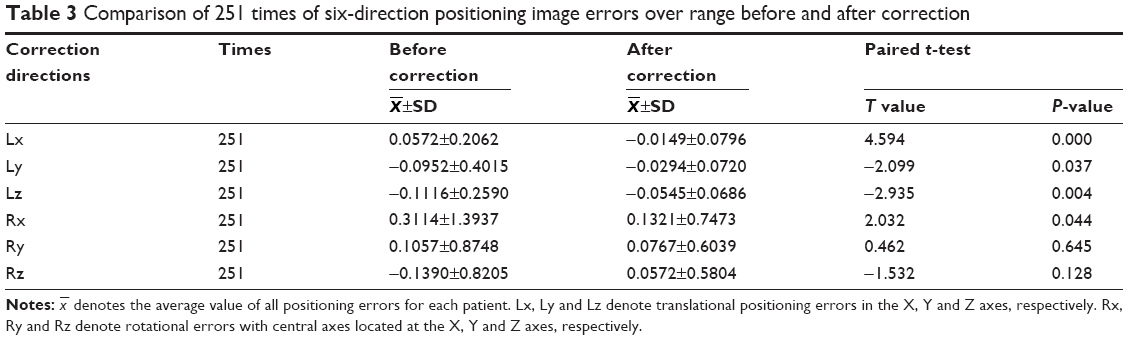 | Table 3 Comparison of 251 times of six-direction positioning image errors over range before and after correction |
 | Table 4 Comparison of the calculated margins before and after correction |
Discussion
Determining a method for reducing positioning errors in radiotherapy and determining how to reduce the influence of positioning errors on radiotherapy have become the focus of studies and have also been a challenge for doctors, radiation therapists and technicians in conducting studies of cancer radiotherapy. To compensate the effects of positioning errors on the dose of radiotherapy, radiotherapy doctors must make PTV by expanding certain margins based on CTV. If the positioning errors are large, larger expanding margins can guarantee that the CTV of the radiotherapy can acquire an adequate prescription dose. However, larger expanding margins can bring greater radiation damage to normal tissues and organs and also limit the increase in dosage in PTV.6 To effectively reduce positioning errors in stepwise radiotherapy, a study revealed that thermoplastic film somatic fixation was more accurate than other fixation methods.7 At the same time, to more accurately measure the positioning errors, for both accurately measuring positioning errors and reducing damage to normal tissues, cone beam computed tomography (CBCT) is superior to the electronic portal imaging device (EPID).8,9 According to the abovementioned research results, this study was designed to investigate the difference in position errors before and after correction and its impact on PTV margins when patients were fixed by thermoplastic film, and positioning errors were measured by CBCT.
First, many studies have revealed that in the implementation of radiotherapy, positioning errors vary in different translational directions in different batches of radiotherapy.10–13 Differences in positioning errors were most significant in the Y and Z axes among the three linear directions in all these studies. Khosa et al12 reported that regardless of whether the reference was an implanted marker or bone marker, displacement was most significant in the direction of the Y axis, followed by the direction of the Z axis. Osei et al13 reported that when an implanted marker was set as reference, displacement in the Z axis was the most significant, followed by that in the Y axis. Furthermore, when the reference was a bone marker, displacement was most significant in the Y axis, followed by the Z axis. In this study, patients were fixed with thermoplastic film in the supine position; and positioning errors before correction in the X, Y and Z axes were 0.057±0.206, −0.095±0.401 and −0.112±0.259 cm, respectively. Displacements in the directions of Y and Z axes were the most significant, which were consistent with the results of the abovementioned studies. The main reason why the displacement in the Y axis was most significant was that the stability of the somatic thermoplastic film fixation in the head–foot direction was the worst, and other reasons were the influence from the filled bladder above. The reason that the displacement in the Z axis was significant may be that the influence of the filled rectum was significant. Previous related studies have also considered that the filled bladder and rectum were the main factors for positioning errors.4,14 After correction by the 6° robotic patient positioning system, the positioning errors in the X, Y and Z axes were −0.015±0.080, −0.029±0.072 and −0.055±0.069, respectively, which were significantly different from those before correction (P=0.000, 0.037 and 0.004, respectively).
Second, in addition to linear displacement, the rotational error of the prostate is inevitable in the process of radiotherapy. Tehrani et al15 reported that based on the iterative closest point (ICP) algorithm, rotational errors of the prostate, in which the central axes were the X, Y and Z axes, were 2.3°, 0.89° and 0.72°, respectively. Graf et al16 reported that the rotational errors of these three axes are −0.01°±3.95°, 0.09°±2.01° and 0.52°±2.30°, respectively.
The aforementioned two studies on rotational error revealed that the rotational error with the central axis located at the X axis was the most significant among the three axis directions. In this study, rotational errors in these three axis directions were 0.31°±1.39°, 0.11°±0.87° and −0.14°±0.82°, respectively. These were consistent with the results of the previous two studies, in which the rotational error in the X axis was the most significant. The reasons remain possibly correlated with the filling status of the rectum and bladder. In this study, rotational errors in these three axes after correction by the 6° robotic patient positioning system were 0.13°±0.75°, 0.78°±0.60° and −0.06°±0.58°, respectively, and only the reduction rate in the X axis was statistically significant compared with those before correction (P=0.044). The reason for this result is that the rotational error in the X axis is more prone to influence factors for translational errors, and the significant differences in these two kinds of errors may be related to the filling status of the bladder and rectum. Results of this analysis can be further verified by evaluating the correlation between the filling status of the rectum and bladder and positioning errors.
Related studies revealed that in intensity-modulated radiotherapy for prostate cancer, PTV derived from even external expansion by 10 mm on the basis of CTV was inferior to PTV that formed from the reduction of margins after IGRT correction in the following two aspects: target motion sensitivity and reduction of irradiation dose on risk organs.17,18 Under the condition of IGRT guided by CBCT, the results of this study revealed that the correction of overstandard displacement using the 6° robotic patient positioning system could effectively reduce translational errors. To further discuss the influence of positioning error reduction on margins, we calculated PTV based on the formula: MPTV=2.5Σ+0.7δ, which was proposed by van Herk et al.4 This formula is based on the cumulative dose distribution and minimum CTV cumulative dose in population-based patients, which avoids the interference of tumor diameter, considers the influence of both system error and random error on the dose and guarantees that the minimum cumulative dose of CTV can reach at least 95% of the prescribed dose in 90% of patients. Hence, it was calculated that before correction, MPTV values in the X, Y and Z directions were 0.61, 0.78 and 0.41 cm, respectively. Furthermore, after correction, MPTV values in the three directions were 0.17, 0.12 and 0.17 cm, respectively. Therefore, it is obvious that the MPTV margins were reduced significantly from the difference of before and after corrections, 0.44, 0.66 and 0.24 cm, respectively; and the reduction rates were 72%, 85% and 56%, respectively. The number of studies in which prostate cancer PTV margins were calculated based on this formula is large. Furthermore, a number of studies revealed that before positioning errors were corrected in the X, Y and Z axes, MPTV values were 0.14–0.93, 0.40–1.2 and 0.47–1.05 cm, respectively.19–21 Studies conducted by Skarsgard et al22 and Rudat et al23 revealed that PTV margins were significantly reduced through image guidance and positioning error correction, even though the margins in every day IGRT did not significantly decline. In the former study, MPTV values before and after error correction in the X, Y and Z axes were 0.57, 0.79 and 0.77 cm and 0.36, 0.37, 0.37 cm, respectively. In the latter study, error correction was conducted every 2 days, and MPTV values before and after correction in the X, Y and Z axes were 0.82, 1.14 and 1.15 cm and 0.41, 0.81 and 0.66 cm, respectively. The results of the aforementioned studies revealed that although the same formula was used, the conditions of different radiotherapy institutions were different, systemic positioning errors were different and the final calculated MPTV also had significant differences. The consistency is that PTV margins could be reduced by the correction of positioning errors. In summary, in the course of radiotherapy, the conditions in different institutions differ, and systemic positioning errors and PTV margins also differ.
Conclusion
To improve the accuracy of radiotherapy and reduce the irradiated volume of normal tissues and risk organs as far as possible, reasonable PTV margins should differ based on different radiotherapy conditions in different agencies. In the present study, the PTV margins obtained through calculating with the data obtained before and after correction of positioning error using IGRT, which was based on the formula: MPTV=2.5Σ+0.7δ, were significantly different. After correction, the PTV margins decreased by 72%, 85% and 56% in the three linear directions of X, Y and Z, respectively. But these values are only analog values, which require further verification online. In this study, the calculated PTV margins were based on positioning systematic errors, which are just simulation values. Hence, further online verifications are required.
Disclosure
The authors report no conflicts of interest in this work.
References
Nijkamp J, Pos FJ, Nuver TT, et al. Adaptive radiotherapy for prostate cancer using kilovoltage cone-beam computed tomography: first clinical results. Int J Radiat Oncol Biol Phys. 2008;70(1):75–82. | ||
Wong JR, Gao Z, Uematsu M, et al. Interfractional prostate shifts: review of 1870 computed tomography (CT) scans obtained during image-guided radiotherapy using CT-on-rails for the treatment of prostate cancer. Int J Radiat Oncol Biol Phys. 2008;72(5):1396–1401. | ||
Palombarini M, Mengoli S, Fantazzini P, Cadioli C, Degli Esposti C, Frezza GP. Analysis of inter-fraction setup errors and organ motion by daily kilovoltage cone beam computed tomography in intensity modulated radiotherapy of prostate cancer. Radiat Oncol. 2012;7:56. | ||
van Herk M, Remeijer P, Rasch C, Lebesque JV. The probability of correct target dosage: dose-population histograms for deriving treatment margins in radiotherapy. Int J Radiat Oneol Biol Phys. 2000;47(4):1121–1135. | ||
van Herk M. Errors and margins in radiotherapy. Semin Rodiat Oncol. 2004;14(1):52–64. | ||
Hoskin P. External Beam Therapy. 2nd ed. Oxford: Oxford University Press; 2012. | ||
White P, Yee CK, Shan LC, Chung LW, Man NH, Cheung YS. A comparison of two systems of patient immobilization for prostate radiotherapy. Radiat Oncol. 2014;9:29. | ||
Ost P, De Gersem W, De Potter B, Fonteyne V, De Neve W, De Meerleer G. A comparison of the acute toxicity profile between two-dimensional and three-dimensional image-guided radiotherapy for postoperative prostate cancer. Clin Oncol. 2011;23(5):344–349. | ||
Ung NM, Wee L, Hackett SL, Jones A, Lim TS, Harper CS. Comparison of low-dose, half-rotation, cone-beam CT with electronic portal imaging device for registration of fiducial markers during prostate radiotherapy. J Appl Clin Med Phys. 2013;14(4):4249. | ||
Bylund KC, Bayouth JE, Smith MC, Hass AC, Bhatia SK, Buatti JM. Analysis of interfraction prostate motion using megavoltage cone beam computed tomography. Int J Radiat Oncol Biol Phys. 2008;72(3):949–956. | ||
Cendales R, Torres F, Arbelaez J, Gaitan A, Vasquez J, Bobadilla I. Displacements of fiducial markers in patients with prostate cancer treated with image guided radiotherapy: a single-institution descriptive study. Rep Pract Oncol Radiother. 2014;20(1):38–42. | ||
Khosa R, Nangia S, Chufal KS, Ghosh D, Kaul R, Sharma L. Daily online localization using implanted fiducial markers and its impact on planning target volume for carcinoma prostate. J Cancer Res Ther. 2010;6(2):172–178. | ||
Osei EK, Jiang R, Barnett R, Fleming K, Panjwani D. Evaluation of daily online set-up errors and organ displacement uncertainty during conformal radiation treatment of the prostate. Br J Radiol. 2009;82(973):49–61. | ||
Ten Haken RK, Forman JD, Heimburger DK, et al. Treat-ment planning issues related to prostate movement in response to differential filling of the rectum and bladder. Int J Radiat Oncol Biol Phys. 1991;20(6):1317–1324. | ||
Tehrani JN, O’Brien RT, Poulsen PR, Keall P. Real-time estimation of prostate tumor rotation and translation with a kV imaging system based on an iterative closest point algorithm. Phys Med Biol. 2013;58(23):8517–8533. | ||
Graf R, Boehmer D, Budach V, Wust P. Interfraction rotation of the prostate as evaluated by kilovoltage X-ray fiducial marker imaging in intensity-modulated radiotherapy of localized prostate cancer. Med Dosim. 2012;37(4):396–400. | ||
Góra J, Stock M, Lütgendorf-Caucig C, Georg D. Is there an advantage in designing adapted, patient-specific PTV margins in intensity modulated proton beam therapy for prostate cancer? Int J Radiat Oncol Biol Phys. 2013;85(3):881–888. | ||
Pérez-Romasanta LA, Lozano-Martín E, Velasco-Jiménez J, et al. CTV to PTV margins for prostate irradiation. Three-dimensional quantitative assessment of interfraction uncertainties using portal imaging and serial CT scans. Clin Transl Oncol. 2009;11(9):615–621. | ||
Kliton J, Agoston P, Major T, Polgár C. Patient positioning using in-room kV CT for image-guided radiotherapy (IGRT) of prostate cancer. Magy Onkol. 2012;56(3):193–198. | ||
Ikeda I, Mizowaki T, Sawada Y, et al. Assessment of interfractional prostate motion in patients immobilized in the prone position using a thermoplastic shell. J Radiat Res. 2014;55(1):168–174. | ||
Kanakavelu N, Jebaseelan Samuel J. Determination of patient set-up error and optimal treatment margin for intensity modulated radiotherapy using image guidance system. J BUON. 2016;21(2):505–511. | ||
Skarsgard D, Cadman P, El-Gayed A, et al. Planning target volume margins for prostate radiotherapy using daily electronic portal imaging and implanted fiducial markers. Radiat Oncol. 2010;5:52. | ||
Rudat V, Nour A, Hammoud M, Alaradi A, Mohammed A. Image-guided intensity-modulated radiotherapy of prostate cancer: analysis of interfractional errors and acute toxicity. Strahlenther Onkol. 2016;192(2):109–117. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.